
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To assess the efficacy and compliance of early night-time bracing in adolescent idiopathic scoliosis with curve magnitudes between the recently proposed early-intervention threshold (15°) and the traditional treatment threshold (25°) recommended by the Scoliosis Research Society (SRS).
Methods
This dual-center retrospective study included 153 AIS patients (Risser 0-3, Cobb angle 15°-25°) treated with the Dresdner Night-Time Brace (DNTB) between 2002 and 2021. Patient demographics, patient compliance, and radiographic outcomes were analyzed. Treatment success was defined by curve stabilization or regression. Statistical analysis was performed with significance set at P < 0.05.
Results
The DNTB achieved a mean in-brace correction of 60.9%, moderately correlated with the initial Cobb angle. Compliance was high: 72.6% of patients were compliant, 15.0% partially compliant, and 12.4% non-compliant. The in-brace correction angle was associated with compliance but not with age, sex, or initial curve magnitude. Compliance significantly influenced outcomes (P < 0.05). Overall curve progression was 12.5%, but only 2.7% in compliant patients, compared to 30.4% and 47.4% in partially and non-compliant groups, respectively. Surgery was required in 10.5% of non-compliant cases.
Conclusions
Early intervention with the DNTB is an effective and well-tolerated treatment for mild AIS (15°-25°), with treatment success highly dependent on patient compliance. These findings underscore the importance of timely bracing and sustained compliance.
Introduction
Adolescent idiopathic scoliosis (AIS) is a structural, three-dimensional spinal deformity, characterized by a lateral curvature of ≥10° accompanied by vertebral rotation in children aged 10 to 18 years, with no identifiable underlying cause.1,2 The global prevalence of AIS ranges from 0.47% to 5.2%, varying across populations.1,2 Although some spinal curves remain stable, a substantial proportion progress during skeletal growth, potentially resulting in severe deformity, compromised mechanical stability, pulmonary dysfunction, chronic back pain, and reduced quality of life.3-5 Therefore, early conservative intervention is essential to prevent long-term morbidity and avoid surgical correction, 5 which carries significant risks and irreversible loss of spinal mobility. 6
Bracing remains the only non-operative treatment with proven efficacy in slowing curve progression in skeletally immature patients. 7 However, the optimal threshold for initiating brace treatment remains a subject of debate. 6 According to the guidelines of the Scoliosis Research Society (SRS), bracing is recommended for skeletally immature patients with curves between 25° and 45°-50°, while surgical intervention is typically considered for curves exceeding 45°-50°. 8 Recently, an emerging consensus suggests that initiating bracing at earlier stages, beginning at 15° for progressive curves in immature patients, with proposed indications extending up to 60°. 9 Despite this evolving perspective, high-quality evidence supporting early bracing in mild AIS, especially using less burdensome approaches, remains limited.
While Full-time bracing (16-23 hours/day) is effective in preventing curve progression; its prolonged wear time is often associated with poor compliance, social stigma, and reduced quality of life.10-12 Adolescents frequently struggle to maintain compliance, thereby limiting therapeutic efficacy.10,12,13 To overcome these challenges, night-time bracing, typically worn for 8-10 hours during sleep, has emerged as an alternative strategy offering corrective force with a lower psychosocial burden.10,12,13 Due to its improved tolerability, night-time bracing may offer practical advantages in the conservative management of mild AIS. However, its clinical efficacy in patients with curve magnitudes between the recently proposed early-intervention threshold (15°) 9 and the traditional treatment threshold (25°) recommended by the Scoliosis Research Society (SRS) 8 remains insufficiently studied. Moreover, although factors such as Risser stage and curve flexibility have been associated with treatment outcomes, the impact of patient compliance in night-time bracing remains inconclusive. 14 This highlights a critical evidence gap regarding both the effectiveness of night-time bracing in early-stage AIS and the role of compliance in determining treatment success.
To address this gap, the present study evaluated the clinical effectiveness and patient compliance of early intervention using the Dresdner Night-Time Brace (DNTB), a anti-rotational orthosis, in patients with mild AIS. 15 We hypothesized that initiating night-time bracing below the conventional treatment threshold would result in high compliance and a reduced risk of curve progression. By exploring this under-investigated range, our findings aim to inform earlier and more tolerable strategies in the conservative treatment of AIS.
Methods
Study Design
This retrospective, dual-center cohort study analyzed AIS patients treated with the DNTB between 2002 and 2021 at Universitätsklinikum Carl Gustav Carus Dresden and Wirbelsäulenzentrum-Asklepios Fachklinik Hohwald, Neustadt in Sachsen, Germany. Institutional Review Board (IRB) approval was obtained. This project received an exemption from the IRB for informed consent. Treatment followed a standardized protocol managed by an interdisciplinary team comprising orthopedic surgeons, orthopedic technicians, and rehabilitation specialists.
Inclusion and Exclusion Criteria
Inclusion criteria were: age between 10 and 16 years at treatment initiation; baseline Cobb angle between 15°-25°; skeletal immaturity (Risser stage 0-3); no prior treatment; and, for female patients, premenarchal status or ≤1 year post-menarche. 4 Exclusion criteria included: prior scoliosis treatment; primary Cobb angle outside the specified range; neuromuscular scoliosis; congenital spinal deformities; and history of spinal surgery.
Brace Fabrication and Treatment Protocol
Each DNTB was custom-fabricated by Orthopedic and Rehabilitation Technology Dresden GmbH (Dresden, Germany). DNTB was individually manufactured based on corrected plaster casts. Negative casts were converted into plaster positives and remodeled to achieve optimal correction. The braces were thermoformed under vacuum, trimmed, and adjusted during fitting. Specifically, the thoracic plaster cast was obtained in two half-shells with the patient in pre-corrected supine and prone positions, while two technicians applied simultaneous manual corrections during hardening. These half-shells were combined into a solid plaster positive model, which was further refined to reduce pressure zones and add expansion areas, following a three-dimensional correction concept that incorporates elongating and derotating forces. Hot polyethylene was thermoformed over the plaster model under vacuum and solidified. The rigid shell was then cut, windowed, and reinforced. The orthosis was fitted to the patient, with adjustments made to ensure proper pressure distribution. Final steps included reinforcement fixation, addition of closures and corrective pads, and placement of radiographic markers. Standardized photographs were taken upon delivery for follow-up, and radiographic evaluation was conducted with corrective forces adjusted as necessary. The prescribed wear time was restricted to nighttime only, approximately 8 hours per night, to reduce the physical and psychosocial burden on patients’ daily lives.
15
The patients did not receive any other brace during the daytime besides the DNTB. Certified orthotists were responsible for verifying proper brace alignment, function, and tolerability. Patients were instructed to wear the brace exclusively and attend scheduled follow-ups for radiographic and clinical assessment. Bracing efficacy was evaluated based on radiographic changes (Figure 1). (A) Schematic Representation of the Biomechanical Principles Underlying the Dresdner Night-Time Brace (DNTB).
15
(B) Clinical Photograph of an Adolescent Idiopathic Scoliosis (AIS) Patient Wearing the DNTB. (C–E) Serial Radiographic Assessments: (C) Baseline (Pre-treatment), (D) In-Brace Follow-up Showing Early Correction, and (E) Final Post-Brace Follow-up Demonstrating Long-Term Treatment Outcome.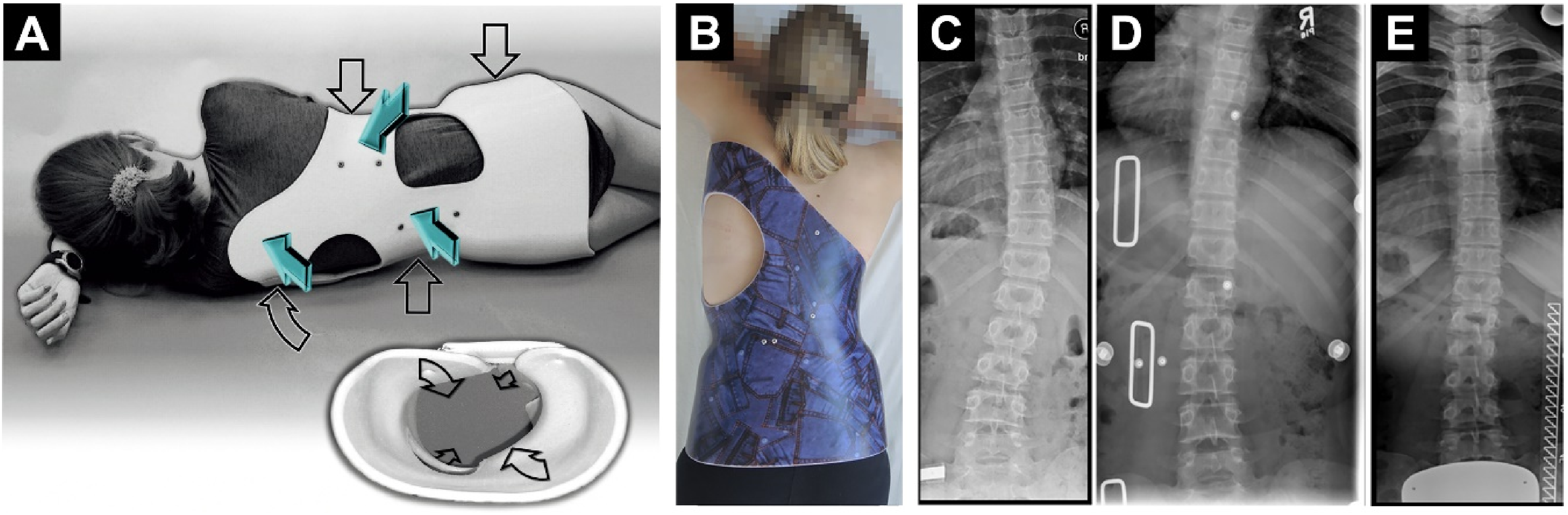
Compliance Assessment
Compliance with brace usage was assessed every 6 months based on self-reports from patients and their families, as well as documentation by orthopedic technicians and physicians during follow-up visits. Based on compliance patterns, patients were categorized into 3 compliance levels 16 : compliant (consistently adhered to the prescribed wear time approximately 8 hours per night), partially-compliant (demonstrated partial adherence, either wearing the brace irregularly or for shorter-than-prescribed durations), and non-compliant (did not wear the brace as prescribed, with minimal or no documented compliance).
Radiographic Assessment
Spinal curvature changes and brace treatment effects were assessed by measuring Cobb angles, reflecting the functional alignment of the spine under physiological loading conditions. The first radiographic assessment, referred to as the initial Cobb angle (baseline), was performed at the time of brace prescription in a standing position. The in-brace Cobb angle was measured during the second assessment, approximately 6 to 9 months after brace initiation in a supine position. This interval aligns with institutional standards for monitoring mild AIS and is supported by prior studies suggesting that curves under 25° may be observed with radiographic evaluation every 6-12 months, 17 and night-time bracing protocols. 18 The in-brace correction angle, defined as the difference between the initial and in-brace Cobb angles, was used to evaluate the early corrective effect of the orthosis. 14 The final assessment, the post-brace Cobb angle, was performed at least 1 year after brace discontinuation during the final follow-up in a standing position. All radiographs were reviewed by a board-certified orthopedic surgeon to ensure measurement accuracy and consistency, minimizing observer variability. To assess treatment efficacy, patients were classified into 3 outcome groups based on the change in their post-brace Cobb angle relative to the initial Cobb angle: Curve regression (Cobb angle reduction of >5°), indicating significant improvement in spinal alignment; Curve stabilization (Cobb angle change within ±5° of baseline), suggesting maintenance of spinal alignment without significant deterioration; Curve progression (Cobb angle increase of >5°).4,19 In addition, the surgical intervention was also assessed for progression beyond 45°.
Completion Criteria
Bracing was considered complete upon reaching all of the following criteria: Risser stage ≥4, indicating near or complete skeletal maturity; and, in female patients, had surpassed 2 years post-menarche. Additionally, a final follow-up assessment was conducted at least 1-year post-brace discontinuation to monitor long-term spinal stability.
Statistical Analysis
Data were analyzed using SPSS Statistics 20 statistical software (SPSS, Inc, Chicago, IL, USA) and GraphPad Prism 8.0.1 (244) Software (Inc, San Diego, USA). Parametric or non-parametric tests were applied based on data distribution. Comparisons between two independent groups were conducted using independent-sample t-tests, while within-group comparisons (e.g., pre- and post-treatment) were analyzed using paired-sample t-tests. For comparisons across 3 or more groups, one-way analysis of variance (ANOVA) was employed, followed by Least Significant Difference post hoc analysis for data with homogeneous variance. For data with unequal variance, Welch’s ANOVA with Tamhane’s T2 post hoc test was applied. Pearson correlation coefficients were calculated to assess linear associations between continuous variables. The strength of Pearson correlation coefficients (r) was classified as follows: |r| < 0.40 = weak correlation; 0.40 ≤ |r| < 0.70 = moderate correlation; and |r| ≥ 0.70 = strong correlation. 20 Linear regression analyses were used to model the predictive relationships between clinical parameters. All results were expressed as mean ± standard deviation (SD) and range. A P-value of <0.05 was considered statistically significant.
Results
Patient Demographics and Follow-Up Characteristics
Patient Demographic Characteristics and Follow-up Information
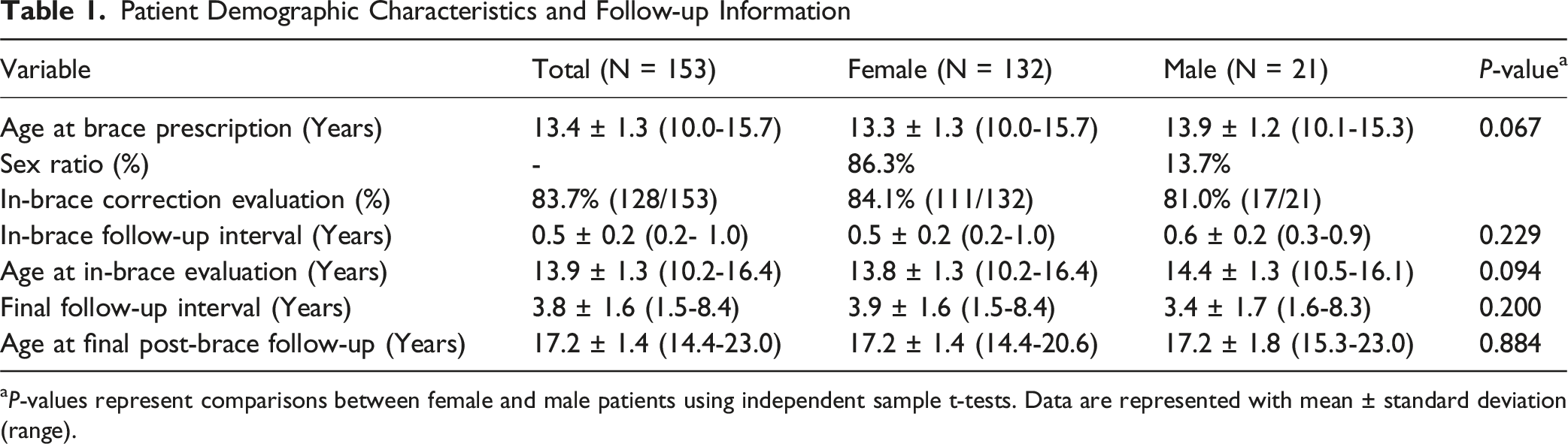
aP-values represent comparisons between female and male patients using independent sample t-tests. Data are represented with mean ± standard deviation (range).
In-Brace Correction Performance
Of the 153 AIS patients, 117 (76.5%) had complete radiographic data available for assessing the in-brace correction. The DNTB achieved a mean in-brace correction rate of 60.9%, indicating substantial early curve reduction. Correlation analyses demonstrated no significant association between the in-brace correction rate and age at brace prescription (r = −0.080, P = 0.393), age at the in-brace evaluation (r = −0.100, P = 0.282), or the in-brace follow-up interval (r = −0.157, P = 0.092), suggesting that these temporal variables did not influence early correction outcomes. Similarly, no statistically significant difference was found between the sexes (male: 65.6% vs female: 60.2%, P = 0.300), indicating that DNTB provided comparable in-brace corrective performance in both male and female patients (Figure 2A, Table S1). A moderate positive correlation was observed between the initial Cobb angle and the in-brace correction angle (r = 0.415, P < 0.001), suggesting that patients with more pronounced baseline curvatures tended to achieve greater in-brace correction. Linear regression analysis showed that the initial Cobb angle accounted for 17.2% of the variance in the in-brace correction angle (R2 = 0.172, P < 0.001), indicating a statistically significant but modest association between baseline curve magnitude and bracing response (Figure 2B). In summary, the DNTB demonstrated consistent and effective in-brace correction across age and sex groups, with moderate dependence on the initial severity of the spinal curve. The In-Brace Correction: Sex Comparison and Curve Severity Association. (A) Comparison of the In-Brace Correction Rates in Male and Female Patients. Data are Represented With Mean ± Standard Deviation. (B) Correlation Between Initial Cobb Angle and in-Brace Correction Angle. Shaded Areas Represent the 95% Confidence Interval (Inner Band) and 95% Prediction Interval (Outer Band) of the Regression Model.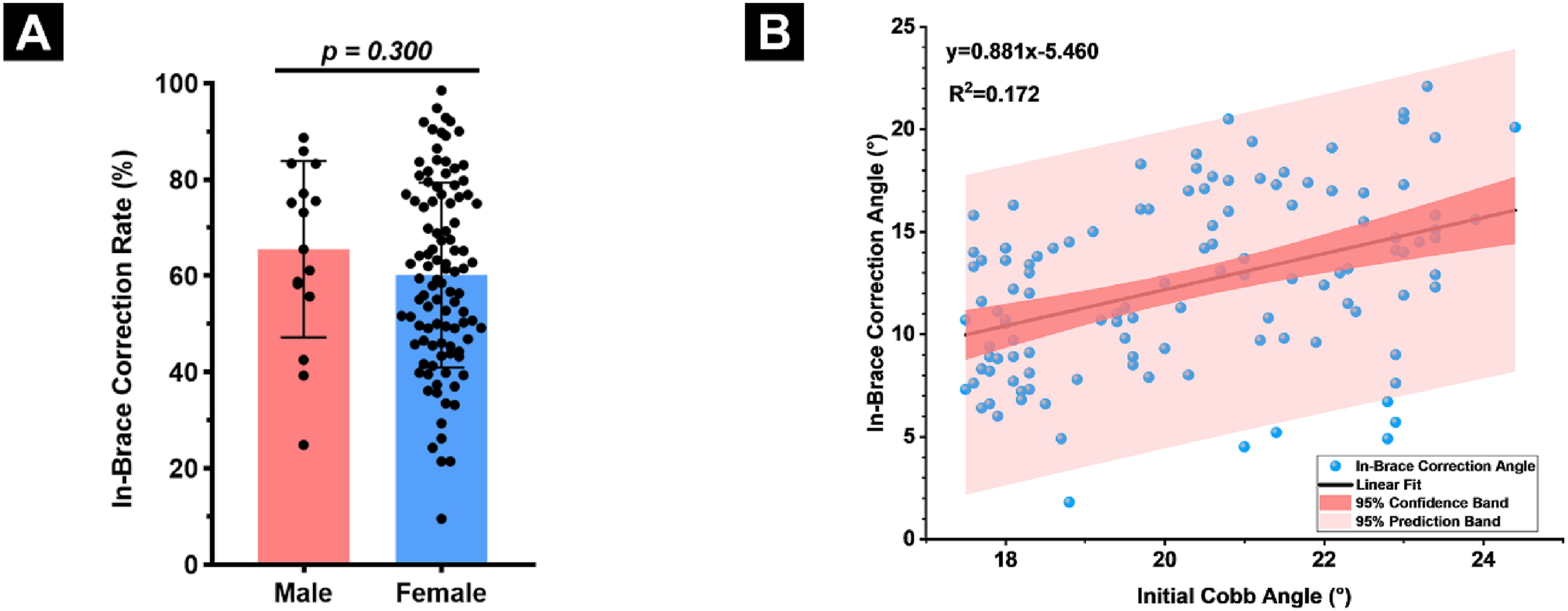
Brace Compliance Patterns and Baseline Associations
Compliance was stratified into 3 categories based on established night-time bracing criteria
16
: compliant (72.6%), partially compliant (15.0%), and non-compliant (12.4%) (Figure 3A). Sex distribution across these groups was similar (Figure 3B–C). Further analysis revealed no significant differences among the 3 compliance groups regarding initial Cobb angle, age at brace prescription, age at final follow-up, or final follow-up interval (Figure 3D, F-H; Table S2), indicating that baseline demographic, radiographic, and treatment duration parameters did not significantly influence brace compliance. However, a significant difference was identified in the in-brace correction across compliance groups (P = 0.024). Specifically, the non-compliant group exhibited a significantly lower in-brace correction (9.3 ± 5.2°) compared to the compliant (12.8 ± 3.8°) and partially-compliant (12.4 ± 4.8°) groups (Figure 3E; Table S2). This observation suggests a potential link between the early biomechanical response to bracing and long-term compliance. Whether reduced early correction negatively affects patient motivation, or whether suboptimal compliance limits early corrective outcomes, remains unclear and warrants further investigation. Compliance Stratification and Associations With Baseline Parameters. (A) Distribution of Compliance Categories Among AIS Patients Treated With DNTB. (B) Distribution of Sex Within Each Compliance Group. (C) Sex Proportion Across Compliance Categories, With no Significant Difference Observed. (D–H) Comparison of (D) Initial Cobb Angle, (E) the in-Brace Correction Angle, (F) Age at Brace Prescription, (G) Age at Final Follow-up, (H)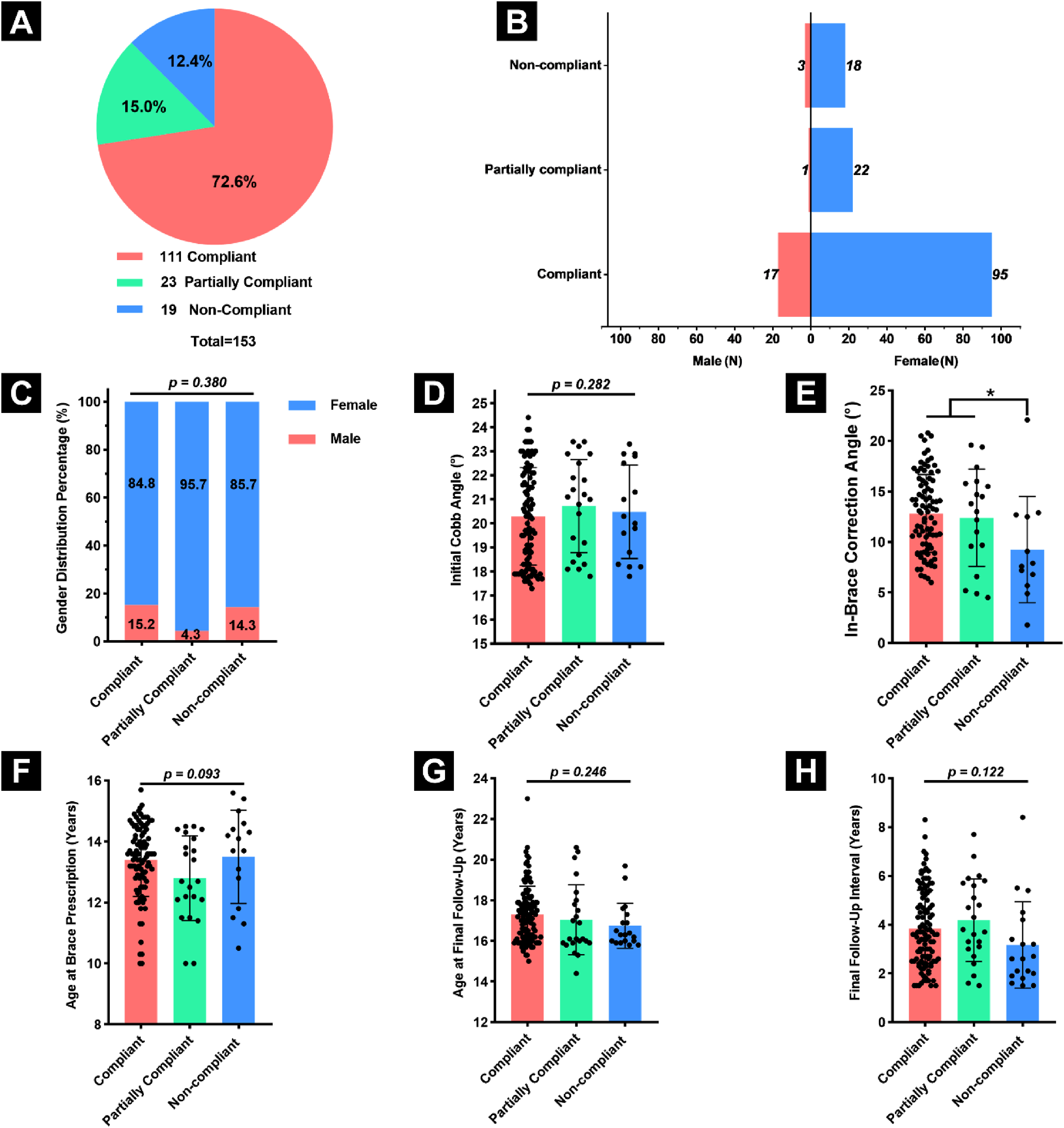
Final Post-Brace Outcomes
At the final follow-up, treatment with the DNTB predominantly resulted in curve stabilization, with the mean Cobb angle showing no significant difference from baseline (20.4° ± 2.0° at initiation vs 20.7° ± 5.1° at post-brace follow-up, P = 0.379), indicating effective maintenance of spinal alignment. This trend was consistent across the sexes, with no significant change observed in either male (P = 0.564) or female patients (P = 0.468) (Table S3). Based on established criteria for scoliosis brace treatment outcomes,4,19 6.5% of patients experienced curve regression (>5° improvement), 81.0% achieved curve stabilization (within ±5° change), and 12.4% exhibited curve progression (>5° increase), resulting in an overall treatment success rate of 87.5% (Figure 4A). Only 1.3% of patients progressed to the surgical threshold, indicating a low risk of severe deterioration. Outcome distributions were similar across sexes (Figure 4B–C). Post-Brace Outcomes: Distribution and Predictors of Treatment Response. (A) Distribution of Post-brace Treatment Outcomes Based on Standardized Criteria.4,19 (B) Treatment Outcome Distribution by Sex. (C) Sex Proportion Across Treatment Outcome Categories, With no Significant Difference Observed. (D–H) Comparison of (D) Initial Cobb Angle, (E) In-Brace Correction Angles, (F) Age at Brace Prescription, (G) Age at Final Follow-up, and (H) Final Follow-up Interval Among Outcome Groups. Data are Expressed as Mean ± Standard Deviation. *P < 0.05.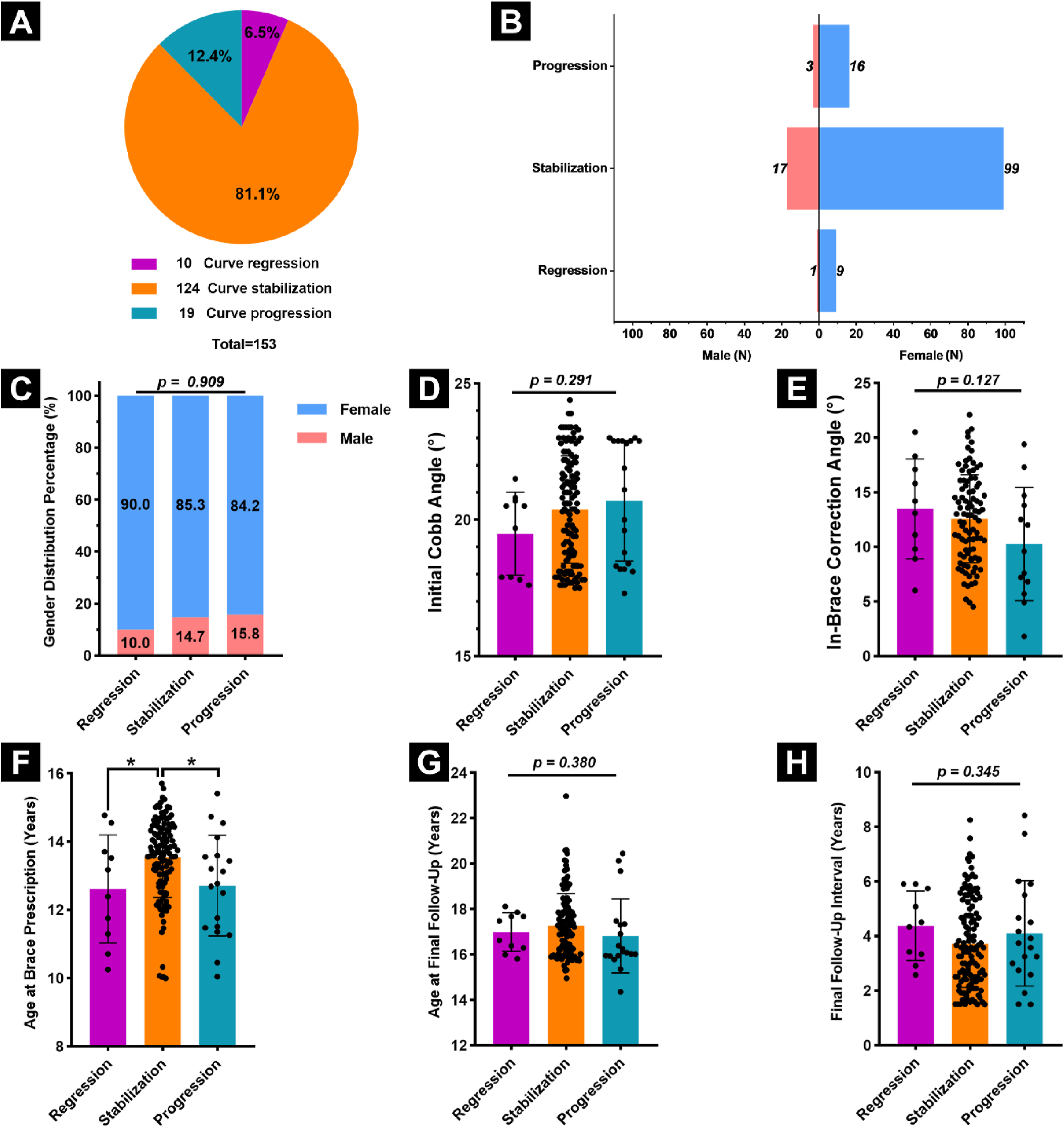
Subgroup analysis by outcome categories revealed no statistically significant differences in initial Cobb angle, in-brace correction, age at final follow-up, or final follow-up interval (Figure 4D–E, G-H). However, age at brace prescription differed significantly (P < 0.05), with patients in the stabilization group being older than those in the regression and progression groups (Figure 4F), suggesting that younger age at bracing initiation may be associated with greater growth potential and a higher risk of curve progression. However, initiating bracing before the peak growth period may enhance stabilization outcomes. In summary, these results highlight the efficacy of DNTB therapy in maintaining spinal alignment and preventing progression in mild AIS.
Compliance-Dependent Treatment Outcomes
Compliance is widely recognized as a critical determinant of treatment success in brace management for AIS patients.
21
In the present study, treatment outcomes varied significantly across compliance levels, highlighting the pivotal role of compliance in the clinical effectiveness of DNTB therapy. The compliant group demonstrated the most favorable results, with 9.0% achieving curve regression, 88.3% maintaining curve stability, and only 2.7% showing curve progression. In contrast, the partially compliant group had a progression rate of 30.4% and no cases of regression. The non-compliant group showed the poorest outcomes, with 47.4% showing curve progression and 10.5% requiring surgical intervention. These differences were statistically significant (χ2 test, P < 0.001), confirming a strong association between compliance and clinical outcome (Figure 5A, Table S4). Treatment Efficacy Across Compliance Levels and Predictive Curve Modeling. (A) Distribution of Final Treatment Outcomes Across Compliance Groups. (B) Linear Regression Analysis Within the Compliant Group Illustrates a Moderate Positive Correlation Between Initial and Final Cobb Angles (R2 = 0.238, P < 0.001), Suggesting a Limited yet Relevant Prognostic Value of Initial Curve Magnitude. Shaded Areas Represent the 95% Confidence Interval (Inner Band) and 95% Prediction Interval (Outer Band) of the Regression Model.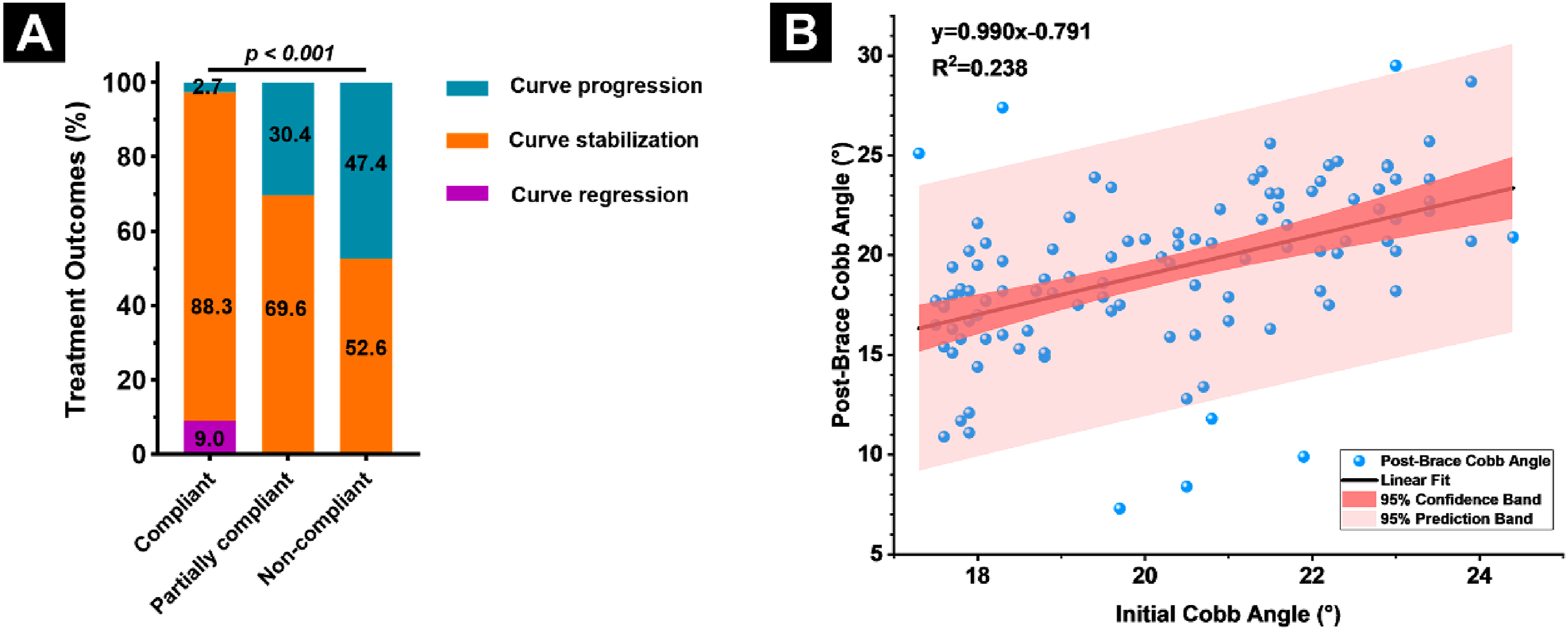
Within the compliant group, a moderate positive correlation existed between the initial Cobb angle and the final post-brace Cobb angle (r = 0.487, P < 0.001), and linear regression indicated that the initial Cobb angle accounted for 23.8% of the variance in the final post-brace Cobb angle (R2 = 0.238, P < 0.001) (Figure 5B). However, no statistically significant correlations were found between the final Cobb angle and either the in-brace Cobb angle (r = 0.152, P = 0.160) or the in-brace correction (r = 0.141, P = 0.193), suggesting that early correction response does not reliably predict long-term curve control. These findings reinforce that patient compliance is the critical factor in determining long-term bracing success in mild AIS treated with the DNTB.
Discussion
This study evaluated the clinical effectiveness and patient compliance of early intervention with the DNTB in mild AIS patients (Cobb angle 15°-25°). A total of 153 patients over 20 years were retrospectively analyzed. The DNTB achieved a mean in-brace correction of 60.9%, with high compliance rates (compliant: 72.6%, partially compliant: 15.0%, and non-compliant: 12.4%). A higher compliance level was strongly correlated with favorable long-term outcomes, including significantly greater rates of curve stabilization and regression, and a markedly reduced risk of progression. These findings support early intervention with the DNTB as an effective and well-tolerated conservative treatment for mild AIS.
Biomechanical Effectiveness of DNTB: In-Brace Correction as a Prognostic Indicator
In-brace correction is a widely recognized early predictor of long-term bracing success and serves as a benchmark for brace design and performance evaluation.22,23 In our study, the mean in-brace correction rate achieved with the DNTB was 60.96% (range: 1.65%-98.56%), indicating substantial early corrective capacity. This value exceeded the commonly accepted 40%-50% threshold, which is generally considered necessary for achieving favorable long-term outcomes. 24 However, it is somewhat lower than the correction rates reported for other night-time braces, such as the Providence brace (average 83%) in patients with curves between 20° and 45°, 25 and the Charleston brace (median 91%) in patients with curves ranging from 10.7° to 60.8°. 18 Several factors may explain this discrepancy. First, our cohort included only mild curves, and we found a moderate positive correlation between initial Cobb angle and in-brace correction; therefore, patients with smaller initial curves tended to achieve smaller absolute corrections. 23 Second, the timing of in-brace assessment (6-9 months after brace initiation) may have affected measured outcomes. Most prior studies assessed in-brace correction within days to several months of brace application. 26 Whether this delay leads to underestimation or overestimation of correction remains unclear and warrants further research. Overall, our findings support the DNTB as a biomechanically effective option in early-stage AIS, particularly when individualized correction goals are prioritized.
High Compliance with DNTB: Tolerance and Contributing Factors
Brace compliance is multifactorial, influenced by orthotic design, psychosocial factors, patient age, wear-time scheduling, and monitoring methods. 21 Different brace designs impact structure, appearance, and wearability, which in turn affect compliance. 21 Despite limited literature on night-time brace compliance, 27 previous studies have reported wide-ranging compliance rates, from as low as 45% 28 to as high as 84%. 29 In our cohort, 72.6% of patients were classified as compliant, a relatively high rate for night-time brace use. This suggests that the DNTB design offers acceptable comfort and wearability to support sustained use. Notably, compliance in this study was not significantly associated with sex, age at brace prescription, or initial Cobb angle. However, non-compliant patients had significantly lower in-brace correction, suggesting a possible link between early biomechanical response and long-term motivation. Whether reduced initial correction discourages compliance or whether poor compliance limits correction potential remains unclear and warrants further investigation.
Compliance-dependent Efficacy in Curve Progression Prevention
Compliance is widely recognized as a critical determinant of brace treatment efficacy in AIS management.12,27 However, current evidence specifically linking compliance to treatment outcomes in night-time bracing remains limited and inconclusive. 14 In the present study, patients with high compliance exhibited significantly more favorable outcomes, including markedly lower rates of curve progression and a substantially reduced need for surgical intervention. These findings support the role of compliance as a key factor in treatment success with the DNTB. Although the retrospective design of our study and absence of an untreated control group preclude direct comparison with the natural course of AIS, existing longitudinal data suggest that, in skeletally immature patients (Risser 0-1) with curves between 20° and 29°, the risk of progression without treatment may reach up to 68%. 30 In contrast, the overall progression rate in our DNTB-treated cohort was only 12.5%, indicating a substantial and clinically meaningful reduction in risk. To our knowledge, no prior studies have specifically evaluated the effectiveness of bracing, either full-time or night-time, in patients with mild scoliosis (Cobb angle 15°-25°). Therefore, our findings provide novel evidence that early night-time bracing, when supported by strong compliance, represents an effective conservative strategy for managing mild AIS.
Early Intervention of DNTB Enhances Long-Term Outcomes
Early bracing has been increasingly recognized as a key determinant of favorable outcomes in AIS. Although some studies suggest that the initial Cobb angle has only limited predictive value for treatment success in mild-to-moderate curves (20°-45°), 31 others have demonstrated that greater curve magnitudes correlate with higher progression risk. 32 Hawary et al reported a 100% risk of progression to >45° in patients with curves >30° during rapid skeletal growth, 22 and even curves <20° have been shown to worsen within 3 months in some cases. 18 However, current SRS guidelines recommend bracing for skeletally immature patients with Cobb angles between 25° and 40°-45°. 8 Accordingly, most existing studies on night-time bracing have focused on this moderate curve range. Reported success rates in patients with curves between 25° and 40° vary, including 57.1%, 33 and 76% 34 for general night-time braces, and 71%-89% for Providence bracing across curves ranging from 20° to 45.25,35 A meta-analysis reported an overall progression rate of 40.7% for night-time bracing, including 34.3% for the Charleston brace and 46.6% for the Providence brace. 10 Notably, the Providence brace has demonstrated success rates of 88% for curves between 20° and 29°, 93% for curves between 30° and 39°, and 77% for curves between 40° and 45°. 25 Similarly, meta-analytic data further demonstrate an increasing risk of progression with increasing Cobb angles: 37.9% for curves between 25°-29° and 41.9% for curves between 30°-42°. 10
In contrast, our study focused exclusively on mild curves (15°-25°) and achieved an 87.5% treatment success rate, with only 12.5% progression. These results suggest that early intervention with night-time bracing may be particularly effective in managing milder curves. The comparatively lower progression rate in our cohort underscores the potential benefit of initiating night-time bracing during earlier stages of curve development. Although not statistically significant, a trend was observed in our study: patients in the regression group had the lowest baseline Cobb angles, followed by the stabilization and progression groups, suggesting a potential association between initial curve severity and treatment outcome.
Beyond curve severity, age at brace initiation also appeared to influence outcomes. Patients in the stabilization group were significantly older than those in the regression or progression groups, indicating a complex relationship between skeletal maturity and bracing efficacy. While younger patients may have greater growth potential, they also face a longer window of progression risk. Conversely, initiating treatment too late may reduce corrective potential. These findings underscore the importance of timing and individualized patient assessment when prescribing early intervention.
Limitations
This study has several limitations. First, its retrospective dual-center design lacked a control group, limiting direct comparison with untreated or alternative conservative interventions for mild AIS patients of similar demographic profiles. Second, patient compliance was assessed using self-reports and clinical evaluations, without objective wear-time monitoring tools such as temperature or pressure sensors, rendering the data susceptible to recall and reporting bias. 21 Third, all included patients had mild curves, and to minimize radiation exposure, supplementary imaging (e.g., side-bending radiographs) for detailed curve classification was not routinely performed. As a result, the potential influence of curve pattern or structural features on treatment outcomes could not be evaluated. Fourth, important biomechanical parameters, such as curve flexibility, apical vertebral rotation, and sagittal alignment, were not included in the analysis due to their inconsistent availability in this retrospective dataset. These factors are known to affect brace effectiveness and should be incorporated into future prospective studies. 36
Conclusion
This dual-center study is the first to specifically evaluate bracing outcomes for mild AIS with Cobb angles between 15° and 25°, demonstrating that early intervention using the DNTB is a clinically effective and well-tolerated treatment strategy. The DNTB achieved a mean in-brace correction rate of 60.9%, indicating robust early biomechanical efficacy across age and sex groups. Compliance was high, with 72.6% of patients classified as compliant, 15.0% partially compliant, and 12.4% non-compliant. While compliance was not associated with age, sex, or initial Cobb angle, it showed a significant correlation with in-brace correction and was the strongest predictor of treatment success. The overall curve progression rate was 12.5%, substantially lower than expected from natural history data. Among compliant patients, only 2.7% experienced progression, with 97.3% achieving stabilization or regression. In contrast, progression rates increased to 30.4% and 47.4% in partially and non-compliant groups, respectively, with 10.5% of non-compliant patients requiring surgery. In summary, the DNTB offers an effective and well-tolerated early intervention strategy for skeletally immature patients with mild AIS. These findings support the timely initiation of bracing in this population and emphasize the critical role of patient compliance in achieving favorable long-term outcomes.
Supplemental Material
Supplemental Material - Early Night-Time Bracing for Mild Adolescent Idiopathic Scoliosis: A Retrospective Cohort Study
Supplemental Material for Early Night-Time Bracing for Mild Adolescent Idiopathic Scoliosis: A Retrospective Cohort Study by Stefan Zwingenberger, Lisa Mersiowsky, Matthew Newton Ede, Andreas Selle, Xinggui Tian, Xuan Pei, Peter Bernstein, Jens Seifert, Klaus-Dieter Schaser, Alexander C. Disch, Uwe Platz in Global Spine Journal.
Footnotes
Author Contributions
Conceptualization: SZ, AS, PB, JS, UP; Methodology: SZ, UP; Software: LM, XT; Validation: SZ, UP; Formal analysis: SZ, LM, XT; Investigation: SZ, LM, MNE; Resources: JS, KDS, AD; Data curation: SZ, XT; Writing-original draft preparation: SZ, LM, XT, XP; writing-review and editing: All authors; Visualization: SZ, XT; Supervision: SZ, UP; Project administration: SZ. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. A. Selle works for an orthopaedic technology company that manufactures scoliosis braces.
Data Availability Statement
The datasets and materials used in this study are available from the corresponding author upon reasonable request.
IRB Approval
The study was approved according to the local institutional review board (IRB) (#EK 27012018).
Supplemental Material
Supplemental material for this article is available online.