
Abstract
Purpose:
To compare treatment efficacy between the Boston full-time brace and the Providence part-time brace in main thoracic adolescent idiopathic scoliosis (AIS).
Methods:
Patients were treated with either the Boston brace (n = 37) or the Providence brace (n = 40). Inclusion criteria were Risser grade ≤2, major curve between 25° and 40° with the apex of the curve between T7 and T11 vertebrae. Two-year follow-up was available in all patients unless brace treatment had reached endpoint. The primary outcome measure was main curve progression to ≥45°.
Results:
Median age was 12.6 years and median treatment length at follow-up was 25 months (interquartile range (IQR): 18–32)) with no difference between the groups (p ≥ 0.116). Initial median main Cobb angle was 29° (IQR: 27–33) and 36° (IQR: 33–38) in the Boston and Providence groups, respectively (p < 0.001). At follow-up, 13 patients (35%) had progressed to ≥45° in the Boston group versus 16 patients (40%) in the Providence group (p = 0.838). Twenty-three patients (62%) had progressed by more than 5° in the Boston group versus 22 patients (55%) in the Providence group (p = 0.685). The secondary thoracolumbar/lumbar curve progressed by more than 5° in 14 (38%) and 18 (45%) in the Boston and Providence groups, respectively (p = 0.548).
Conclusions:
Despite a larger initial curve size in the Providence group, progression of more than 5° or to surgical indication area was similar in the Boston group. Our results indicate that nighttime bracing is a viable alternative to full-time bracing also in main thoracic AIS.
Introduction
Nonoperative treatment for adolescent idiopathic scoliosis (AIS) is controversial with different available treatment options, however bracing remains at the center of conservative treatment. The traditional thoracolumbosacral orthosis (TLSO) worn for 18–22 h/day is superior to observation in terms of preventing curve progression and thereby avoiding surgery. 1 However, compliance with the prescribed regimen is an issue and reduced compliance has consistently been shown to affect treatment outcome. 1 –4 Because of these issues, a part-time brace design was developed. This brace was designed to provide a higher level of curve correction allowing for nighttime use only. The most frequently used nighttime braces are the Charleston 5 –7 and the Providence brace. 8 –11 The available literature regarding the nighttime brace is scarce and whether the efficacy, in terms of limiting progression to a surgical level, is similar to the full-time brace has not been sufficiently assessed. Table 1 summarizes some of the main clinical studies on the traditional TLSO full-time brace and the Charleston and Providence nighttime braces. 1,3,5,7,8,11 –16 The largest published case series on the Providence nighttime brace is the original paper by D’Amato et al. 11 In 102 female patients, the authors found 26% progression of more than 5° in the whole cohort; however, the success rate was markedly different between curve types showing more than 90% success rate for thoracolumbar or lumbar (TL/L) curves and 63% for thoracic curves. Ohrt-Nissen et al. 8 confirmed these findings showing 76% and 43% success rate in the TL/L and thoracic curves, respectively. Consequently, some authors advocate that the use of the Providence brace should be reserved for TL/L curves. 17,18 A few clinical studies have compared full-time and nighttime bracing, 15,18,19 but none have examined the clinical relevance of differentiating brace treatment in patients with main thoracic curves.
Overview of studies reporting on the efficacy of full-time and nighttime bracing in AIS patients.a

TLSO: thoracolumbosacral orthosis; CP: curve progression.
aResults are in both thoracic and lumbar curves unless otherwise specified.
Objective of the study
To compare treatment efficacy between the Boston full-time brace and the Providence part-time brace for main thoracic AIS.
Materials and methods
A retrospective longitudinal dual-center study was conducted on two parallel series of AIS patients who underwent brace treatment between January 1, 2009 through December 30, 2015. Both centers are tertiary facilities specialized in conservative and surgical treatment of AIS. At one center, the standard bracing regime in main thoracic AIS (apex between T7 and T11) is a full-time Boston brace worn for a minimum of 18 h/day. At the second center, the standard treatment is a part-time Providence brace worn for 8 h/day during sleep. A subset of this population has previously been described. 8 The Boston brace is a prefabricated brace that works by applying compression to the convex side of the curve through pads placed at the apex of the curve and below 20 (Figure 1). The Providence brace is custom-made, typically using CAD-CAM modeling, and works by applying compressive and rotational forces to the spine. The correctional forces are substantial and in this “hypercorrected” position brace wearing is only feasible while lying down. 20

Left: Boston brace, frontal and lateral view. Right: Providence brace, frontal and lateral view.
Inclusion criteria were based on the recommendations by the Scoliosis Research Society (SRS) and the International Society on Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT) 21,22 : Age more than 10 years at the time of AIS diagnosis, Risser grade 0–2 at the start of treatment and a main curve between 25° and 40° at the start of treatment. Furthermore, we included only patients with the apex of the main curve between T7 and T11 vertebrae. We excluded patients who had been treated previously with a brace. Patients were followed until termination of brace treatment. Brace treatment was terminated when the patient was deemed skeletally mature defined by either Risser grade 4 and/or cessation of growth and/or more than 2 years past menarche. Patients who were surgically treated prior to reaching skeletal maturity was followed up until surgery. The following standing anteroposterior (AP) radiographs were analyzed: The most recent radiograph prior to brace treatment, initial standing (Boston) or supine (Providence) in-brace radiograph after the start of treatment and finally, the out-of-brace radiograph at the time of brace termination (Figure 2). Radiographic evaluation was performed after a full night out-of-brace in both groups. The primary outcome measure was treatment failure defined as main curve progression to ≥45° at follow-up. Secondary outcome measures were progression of the main thoracic, TL/L, or proximal thoracic (PT) curve of more than 5°.
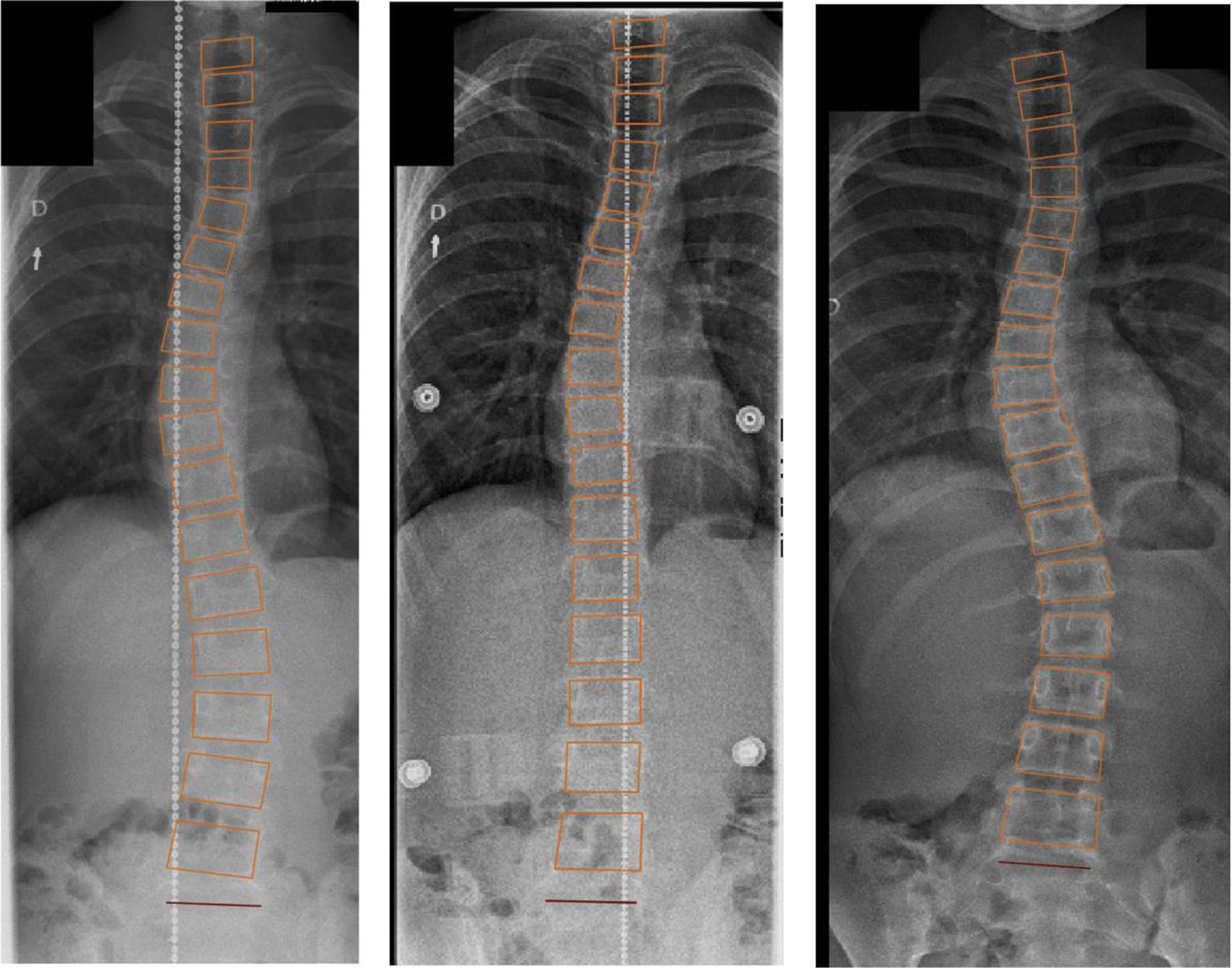
Left: Pretreatment standing frontal radiograph. Middle: Supine in-brace frontal radiograph. Right: Follow-up standing frontal radiograph.
Statistical analysis
All statistical analyses were performed using R version 3.4.0 (R core team, 2014, Vienna, Austria). Data distribution was assessed by histograms. For the majority of variables, the data were not normally distributed, and data are reported as proportions (%) or median with interquartile range (IQR). Curve progression exhibited normal distribution, which allowed for testing of equivalence with the two one-sided test (TOST) of equivalence procedure using −5° and 5° equivalence bounds. 23 Continuous data were compared using Wilcoxon rank sum test and categorical variables were compared using Pearson’s χ 2 test. Also, logistic regressions were performed to adjust for potentially confounding factors, including initial brace type, curve size, and age. The parameters included in the regression analysis were decided a priori based on prognostic factors for curve progression most consistently reported in the literature. Results are given as odds ratio (OR) with 95% confidence interval (CI). For all analyses, p < 0.05 was considered significant.
The study was approved by the Data Protection Agency and the Health and Medicines Authority.
Results
A total of 77 patients were included, 37 in the Boston group (36 females) and 40 in the Providence group (39 females). Median age was 12.6 years (IQR: 12.1–13.5) and median duration of treatment was 25 months (IQR: 18–32) with no significant difference between the groups (p ≥ 0.116) (Table 2). At the start of treatment, median main Cobb angle was 29° (IQR: 27–33) in the Boston group and 36° (IQR: 33–38) in the Providence group (p < 0.001). At follow-up, treatment failure was found in 13 (35%) patients in the Boston group and 16 (43%) patients in the Providence group, respectively (p = 0.838) (Figures 3 and 4). Median main curve progression was 8° (IQR: 1–15) versus 7° (IQR: 0–13) (p = 0.838) and progression by more than 5° was found in 23 (62%) and 22 (55%) patients, respectively (p = 0.685) (Figure 3). Multiple logistic regression showed that initial age was not significantly associated risk of progression (OR: 0.84, 95% CI: 0.55–1.25, p = 0.387). The use of a Boston brace did not significantly decrease the risk for progression even when adjusted for age and curve size (OR: 0.61, 95% CI: 0.18–1.88) (p = 0.400). The only significant predictor for treatment failure was main curve size at the start of treatment (OR = 1.16, 95% CI: 1.03–1.33) (p = 0.024) (Table 3).
Primary and secondary variables.a

IQR: interquartile range; TL/L: thoracolumbar/lumbar; PT: proximal thoracic.
aAll patients were Caucasians.
bMissing or nonapplicable (males) in seven patients.

Bar plot showing the rate of treatment failure (progression ≥ 45°) and the progression of more than 5° in the main thoracic, thoracolumbar/lumbar (TL/L), and proximal thoracic (PT) curves.

Density plot showing the distribution of main Cobb angle measurements at the start of treatment (left) and at follow-up (right). At the start of treatment, the two cohorts differed substantially in curve size distribution. At follow-up, the distribution was similar between the two groups.
Multiple logistic regression with progression ≥45° as outcome parameter.

The median initial TL/L Cobb angle was 19° (14–25) and 23° (19–29) (p = 0.014), respectively, and the median PT Cobb angle was 15° (IQR: 11–20) and 21° (IQR: 17–25) (p < 0.001). At follow-up, progression of the TL/L curve by more than 5° was found in 14 (38%) and 18 (45%) patients in the Boston and Providence groups, respectively (p = 0.548) (Figure 3). Progression of the PT curve was found in 10 (27%) patients and 11 (28%) patients, respectively (p = 0.754).
Test of equivalence using TOST showed that effect sizes larger than 5° could be rejected with the current sample size (Figure 5) (p = 0.022, 95% CI: −4.9 to 4.5).

TOST of equivalence showed that effect sizes larger than 5° between the two bracing groups could be rejected at the 0.05 significance level. A standard NHST using student’s t test showed no significant difference in progression between the groups (p = 0.932). TOST: two one-sided test; NHST: null hypothesis significance test.
Discussion
In the current study, we present the treatment results in high-risk AIS patients comparing full-time and nighttime bracing regimes. We did not find any statistically or clinically significant differences in primary or secondary outcomes between the two groups. The main predictor for treatment failure was the curve size at the start of treatment, not the brace type or age. Interestingly, the Providence group had significantly larger initial main thoracic, TL/L, and PT curves. This may be due to late referrals from general practitioners, pediatricians, and other entities. Both countries have a public healthcare system but in Denmark, school screening for AIS is not institutionalized, while in Finland, school screening for AIS is compulsory at fifth grade in girls and at seventh grade in boys. A previous paper showed that in the current Danish system, AIS patients are often referred late to specialized evaluation with large curves and after the onset of growth spurt. 24 Our results indicate that a key point of action to reduce treatment failure is to accelerate the referral process and maybe increase awareness of the disease and predictors of progression in the health community as well as the general society. Whether this involves the use of school screening programs is a controversial question that our study was not designed to answer.
The primary endpoint (progression ≥ 45°) was selected based on the recommendations of the SRS and SOSORT. Using a dual-center design, we did not find it appropriate to report surgical rate as this may be biased by local differences in the surgical indications or surgical waiting lists, and so on. Progression to 45° does not represent an absolute indication for surgery and several patients in the current cohort did not progress beyond 50° (Figure 4), which by some is considered a more appropriate outcome measure. We did see a few patients in the Providence group with a severe progression to more than 60° (Figure 4). There were no such patients in the Boston group. Whether this is due to the larger initial curve size in the Providence group or that an unrecognized high-risk group of patients should not be treated with the Providence brace remains unclear.
Katz et al. 19 compared the Boston brace to the Charleston nighttime brace and reported progression in 37% in the Boston group and 57% in the Charleston group. However, this study included TL/L curves, which are typically more flexible as well as more manageable with brace and may therefore explain the higher progression rate in our cohort. 9 The study also included patients with 40–45° curves and found that the Boston brace performed well in this group, whereas the Charleston group showed an 83% progression rate. Janicki et al. 15 compared the Boston brace to the Providence brace in 83 AIS patients with any curve using the SRS 2005 brace treatment criteria including also the main TL and L curves. In the Boston group, 85% of patients progressed more than 5° and 63% progressed beyond 45°. In the Providence group, progression rate was 69% and 43% progressed beyond 45°. In line with the current study, the authors found that the rate of progression was primarily influenced by the initial curve size.
In-brace correction with the full-time TLSO brace varies from 30% to 50% in the literature depending on curve type. 25,26 Chan et al. 27 found that thoracic curves correction is substantially less (19–25%) than for TL/L curves (45%) in the full-time TLSO, which is in line with previous results showing less flexibility and in-brace correction of thoracic curves. 9 In the current study, which only included thoracic curves, the median in-brace correction for the Boston group was 29%. In patients with less-than-expected correction, braces were adjusted with additional bolsters, but no subsequent radiograph was taken. Correction was 67% for the Providence group, but brace adjustment was routinely done after 1 month in the brace to achieve maximum correction after a period of brace assimilation. Again, no subsequent radiograph was done after this adjustment to avoid excessive radiation exposure.
Patients were included in the present study irrespective of estimated compliance. No objective measure for hours in-brace was available, which is a major limitation to our study. Patients were asked at outpatient follow-up visits about compliance and no patient reported noncompliance in either group. Objective compliance data have not been reported for the nighttime brace, whereas compliance is known to be low in full-time braces. The SRS and SOSORT recommend reporting intention-to-treat data including all patients irrespective of level of compliance and this issue is further complicated by the fact that brace monitoring has been shown to increase brace compliance 28,29 and therefore may act as a bias in interpreting the actual effect of the brace design. As the main indication of the nighttime brace is to increase compliance, we do not consider differences in compliance as a study bias but rather an expected difference as a consequence of decreasing the burden of treatment. However, our results should be interpreted carefully and as compliance monitoring becomes more common in nighttime braces, we will hopefully be able to differentiate whether the effect of the brace comes from the aggressive curve correction and/or increased compliance.
Both the Boston and Providence braces are custom-made and as such are designed to accommodate individual variation. Body mass index was identical between the two groups (Table 2) and no patients in the current cohorts were overweight, which can be an important factor to consider. Whether nighttime bracing is suitable in all patients remains to be determined and treatment may still need to be differentiated between patients based on risk of progression as well as physical and radiographic features.
Risser grading was limited in both cohorts as the AP radiograph in several cases did not visualize the most lateral part of the iliac crest. For this reason, we could not differentiate between Risser 0 and 1, which is a limitation to our study. However, the age distribution as well as menarchal stage were almost identical between the two groups, so we do not expect differences in skeletal maturity to be a significant confounder in our study. The Risser stage has been found to correlate with peak curve progression in AIS patients 30 ; however, several studies have questions about its use as a reliable indicator of growth. Studies have shown that the peak velocity of growth can occur before the first signs of iliac apophysis ossification and that curve progression and trunk growth can continue after Risser stage 4 is reached. 31,32 However, currently, internationally accepted guidelines for bracing do still use Risser staging as the primary risk indicator, but we would encourage future studies to assess the clinical utility of other radiographic or clinical growth markers. 33
The current study represents a large homogenous sample of AIS patients following two well-defined bracing protocols at parallel time points. Patients were selected using strict inclusion criteria and only main thoracic curves were included which add clarity to the results. Although a type 2 error due to inadequate sample size cannot be ruled out, we found no trends in the data supporting this notion. The current study brings important information that may have an impact on treatment compliance and patient satisfaction. We would encourage future studies to assess whether the use of a nighttime brace does actually increase the compliance rate and ultimately the patients’ quality of life during treatment.
Conclusion
Despite a larger initial curve size in the Providence group, progression of more than 5° or to surgical indication area was similar between the two groups. The main predictor for curve progression was initial curve size, not brace type. Our results indicate that nighttime bracing is a viable alternative to full-time bracing in main thoracic AIS.
Footnotes
Authors’ note
The study was approved by the regional data protection agency and the Danish Patient Safety Authority.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Søren Ohrt-Nissen received an institutional research grant from K2M outside the submitted work. Ilkka Helenius received an institutional research grant from Medtronic International and Innosurge outside the submitted work. Martin Gehrchen received an institutional research grant from Medtronic International and K2M outside the submitted work.