
Abstract
Study Design
Retrospective cohort study.
Objectives
The purpose of this study was to report reference ranges for global sagittal alignment parameters stratified by age and sex in patients without spinal deformity.
Methods
This retrospective cohort study included consecutive patients undergoing biplanar full-body spine x-rays at a single institution, excluding those with spinal deformity or prior spine surgery. Global sagittal alignment parameters included cranial sagittal vertical axis to the sacrum (CrSVA-S), hip (CrSVA-H), knee (CrSVA-K), and ankle (CrSVA-A) as well as the cranium-hip-sacrum (CrHS), cranium-knee-sacrum (CrKS), and cranium-ankle-sacrum (CrAS) angles. Patients were stratified by age and sex, and ANOVA and multivariable logistic regression were used to compare groups, with age and sex as predictors of each radiographic parameter. Multivariable logistic regression models were created using age and sex as predictors, and each radiographic parameter as the outcome. In these models, age was treated as a continuous variable.
Results
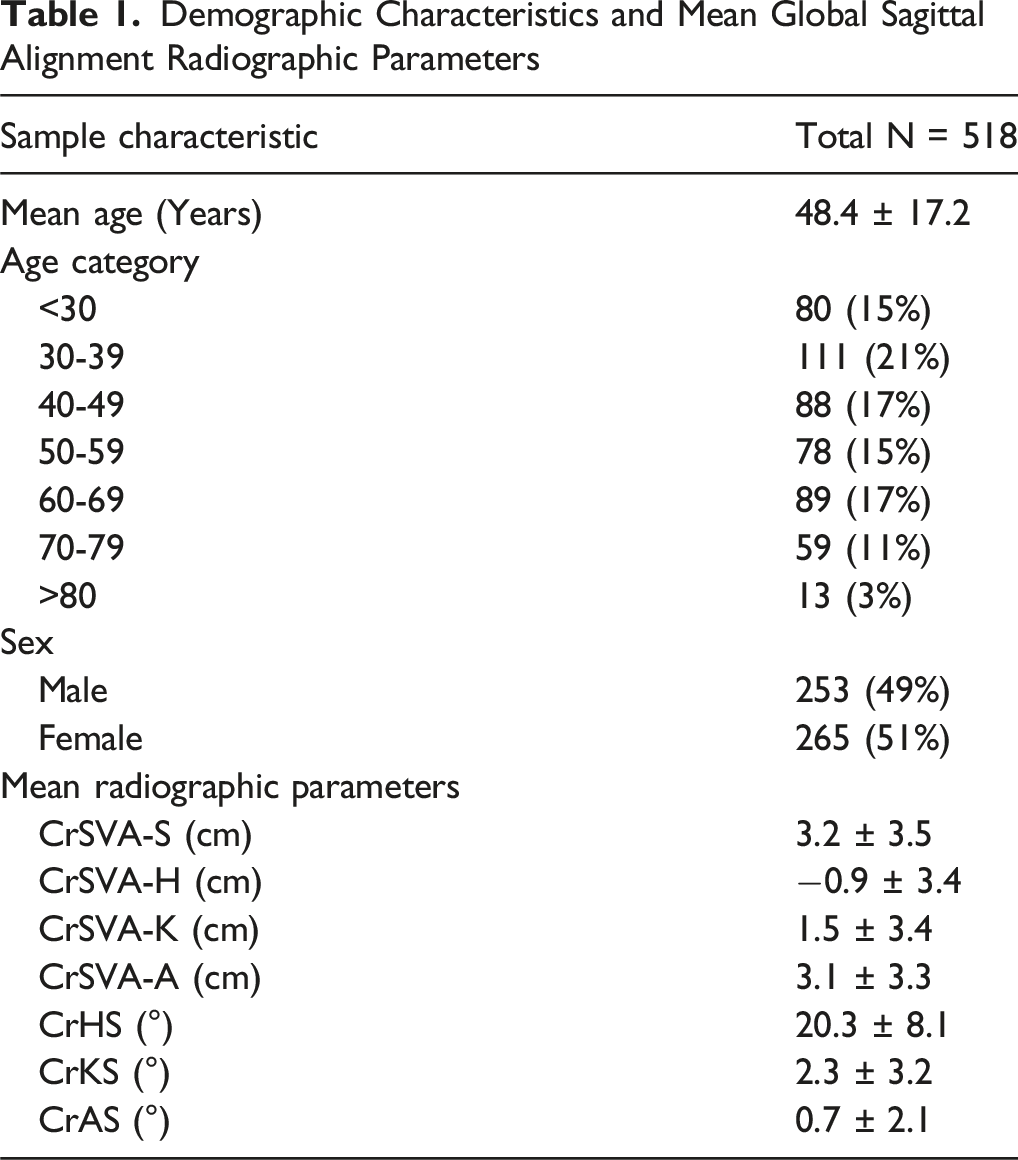
A total of 518 patients were included, 253 (48.8%) male and 265 (51.2%) female, with ages ranging from 12 to 91 years old. In multivariable linear regression models, each 10-year increase in age was associated with a 0.6 cm increase in CrSVA-S (P < .001) and a 0.3 cm increase in CrSVA-H (P < .001). Conversely, age was associated with a 0.3 cm decrease in CrSVA-K per decade (P = .002), with no significant association observed between age and CrSVA-A. Male sex was associated with greater CrSVA-S (1.3 cm; P < .001), CrSVA-H (1.2 cm; P < .001), and CrSVA-A (1.2 cm; P < .001) compared to females. CrSVA-K did not differ significantly by sex.
Conclusion
This study establishes reference values for normal global sagittal alignment to support operative planning and improve understanding of global sagittal alignment in spinal deformity.
Introduction
The spine is intricately connected to the pelvis and lower limbs, emphasizing the need for a comprehensive understanding of global sagittal alignment. 1 Sagittal alignment plays a crucial role in maintaining postural balance, spinal stability, and functional capacity,2,3 and misalignment in the sagittal plane has been associated with diminished functional status and adverse patient outcomes.4-6 However, current methods for assessing sagittal alignment often overlook key aspects such as the contributions of the head and lower extremities. 7
The first biplanar X-ray system was introduced in 2007, which allows for full-body imaging of the spine with less irradiation and distortion than conventional X-rays. 8 This full-body spine imaging has enabled the development of new global sagittal alignment parameters which can account for variations in pelvic and lower limb anatomy. In 2017, Kim et al 9 introduced the cranial sagittal vertical axis (CrSVA) global alignment parameters using full-body spine imaging to better characterize sagittal alignment in patients with spinal deformity. These measurements are based on distances from a vertical line centered at the midpoint of the nasion-inion cranial line on lateral full-spine radiographs. Kim et al demonstrated that CrSVA parameters were more strongly correlated with Oswestry Disability Index (ODI) as well as Scoliosis Research Society-22 Questionnaire (SRS-22) compared to C7 sagittal vertical axis (SVA), 9 a widely recognized radiographic measurement of sagittal balance.10,11
Despite these recent advancements in full-body spine imaging, global sagittal alignment in patients without spinal deformity has not been well studied. Characterization of global sagittal alignment values in the general population would provide a benchmark for spine deformity surgery. The objective of this study was to establish reference values for global sagittal alignment parameters stratified by age and sex.
Methods
Study Design & Demographics
This institutional review board-approved (STUDY-17-00660) retrospective study was conducted at a single institution between November 2022 and February 2024. Consecutive patients undergoing full-body spine imaging (EOS, France) were assessed for inclusion in the study. Patients with scoliosis >20°, severe cervical kyphosis, or prior spine surgeries were excluded. Demographic data including sex and age were collected from the electronic medical record. The IRB approved the present study and granted waiver for consent of patient data. The protocol number is IRB-17-02032.
Radiographic Measurements
Four distance parameters were collected: cranial sagittal vertical axis to the sacrum (CrSVA-S), hip (CrSVA-H), knee (CrSVA-K), and ankle (CrSVA-A). The cranial sagittal vertical axis was defined as a vertical line drawn from the midpoint of the nasion-inion line. These measurements were based on four anatomical landmarks: the posterior superior corner of the S1 endplate (CrSVA-S), and the midpoint of the lines connecting the femoral heads (CrSVA-H), tibial plateaus (CrSVA-K), and apices of the talar domes (CrSVA-A) on lateral view. 9 The direction of the measurement was defined as positive if the distance was posterior to the cranial sagittal vertical axis and negative if the distance was anterior to the cranial sagittal vertical axis.
Three additional angular parameters were collected: cranium-hip-sacrum (CrHS), cranium-knee-sacrum (CrKS), and cranium-hip-sacrum (CrAS).
7
Each angle was measured based on the anatomical landmarks described above. The angular direction was defined as positive if the line drawn from the cranial midpoint was anterior to the line drawn from the sacrum and negative if the line drawn from the cranial midpoint was posterior to the line drawn from the sacrum. LabelMe software was used to define the skeletal landmarks on lateral x-rays, and python scripts were used to calculate the parameter values based on the coordinates of the defined landmarks (Figure 1).
12
All measurements were performed by a single, trained reviewer to ensure consistency and reduce inter-rater reliability. Example Radiograph Demonstrating (A) Landmarks for Global Sagittal Alignment Parameters, (B) CrSVA Measurements, and (C) Cranium Angle Measurements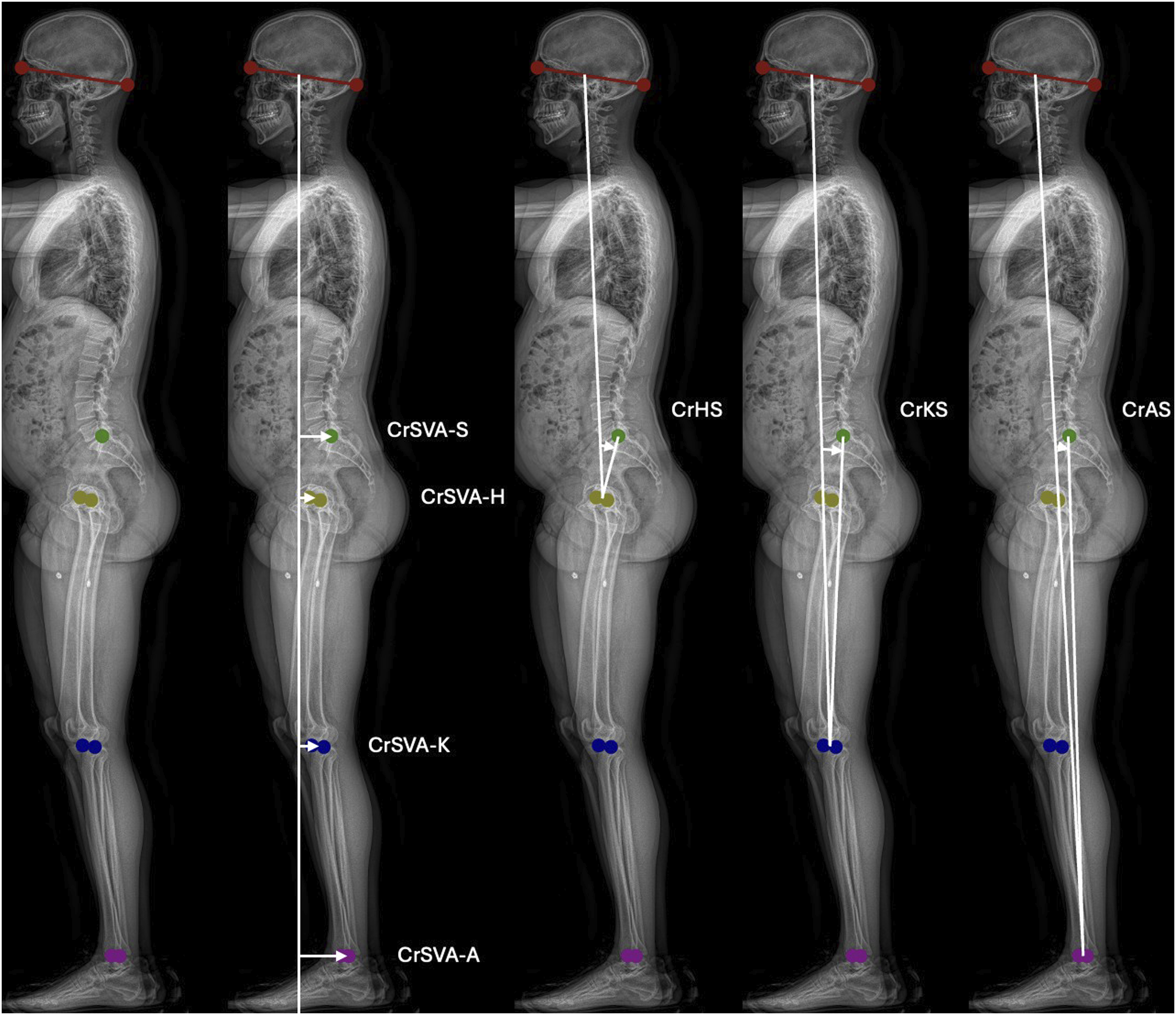
Statistical Analysis
Patients were stratified based on age (<29, 30-39, 40-49, 50-59, 60-69, 70-79, 80+ years) and sex, and ANOVA testing was used to compare groups. Continuous variables were reported as mean with standard deviation, and categorical variables were reported with frequencies and percentage. Multivariable regression models were created using age and sex as predictors of the radiographic measurements (CrSVA-S, Cr-SVAH, CrSVA-K, CrSVA-A, CrKS, CrAS, CrHS). In these models, age was treated as a continuous variable. Beta coefficients with 95% confidence intervals and P-values are reported for both age and sex variables. All statistical analyses were performed using IBM SPSS Version 29.0. P-values less than .05 were considered statistically significant.
Results
Demographic Characteristics and Mean Global Sagittal Alignment Radiographic Parameters
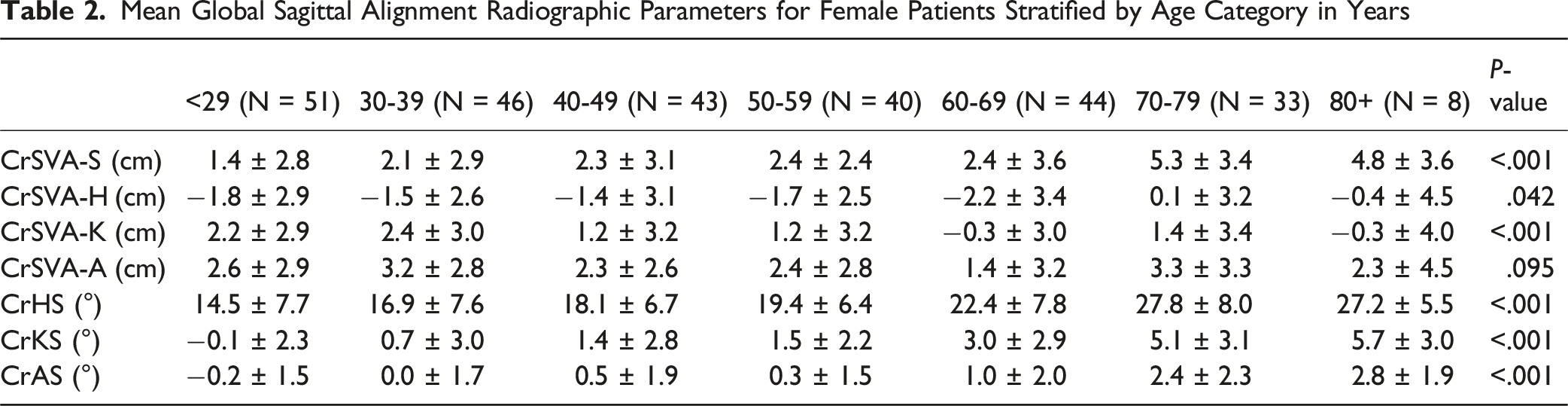
Mean Global Sagittal Alignment Radiographic Parameters for Female Patients Stratified by Age Category in Years
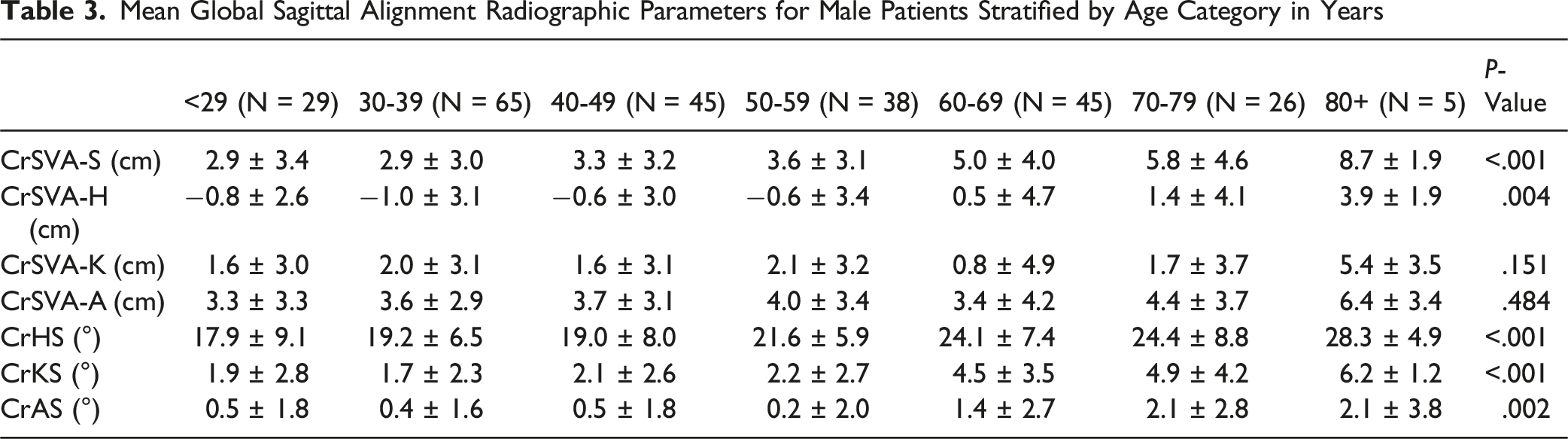
Mean Global Sagittal Alignment Radiographic Parameters for Male Patients Stratified by Age Category in Years
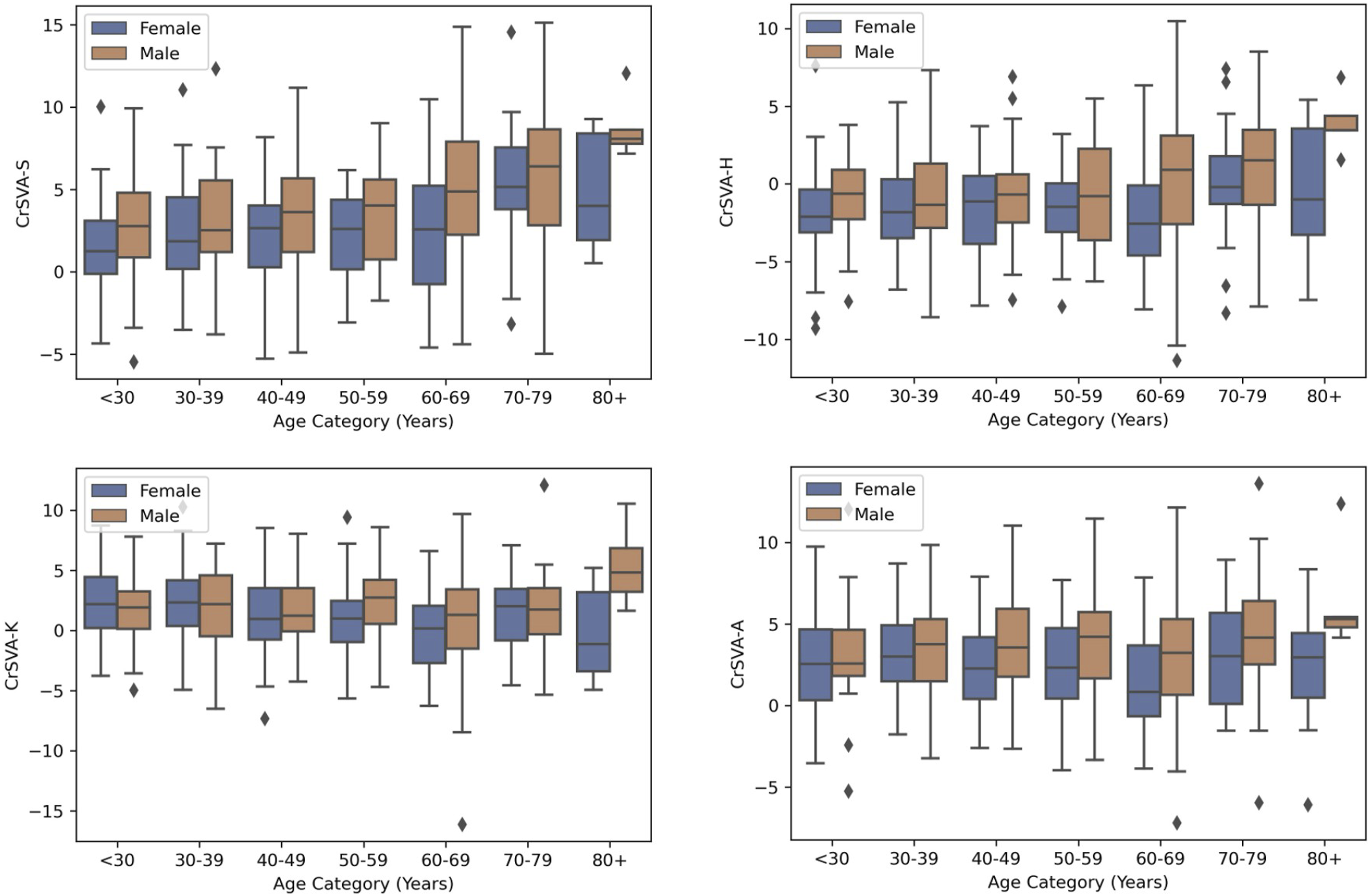
Boxplots Showing Variation in Global Alignment With Age and Stratified by Sex for CrSVA-S, CrSVA-H, CrSVA-K, and CrSVA-A
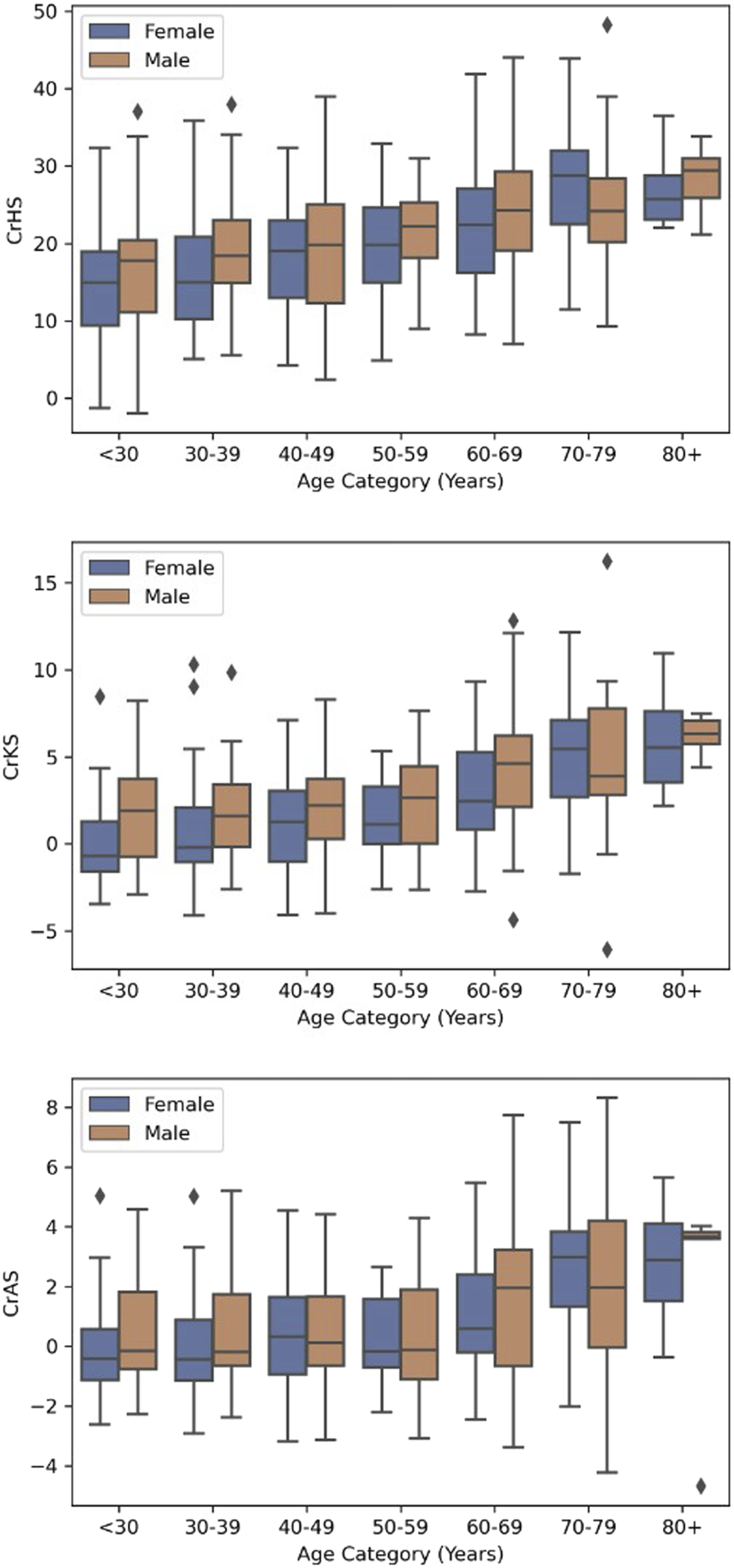
Boxplots Showing Variation in Global Alignment With Age and Stratified by Sex for CrHS, CrKS, and CrAS
Linear regression models demonstrated age as a significant positive predictor of CrSVA-S (β = 0.058, [0.041, 0.074], P < .001), CrSVA-H (β = 0.029, [0.013, 0.046], P < .001), CrHS (β = 0.194, [0.156, 0.231], P < .001), CrKS (β = 0.084, [0.070, 0.098], P < .001), and CrAS (β = 0.037, [0.027, 0.047], P < .001). Conversely, age was a negative predictor of CrSVA-K (β = −0.026, [−0.043, −0.009], P = .002) (Figure 4). Forest Plot for Multivariable Linear Regression Models With Age as a Predictor of Global Sagittal for Peer Review Alignment Radiographic Parameters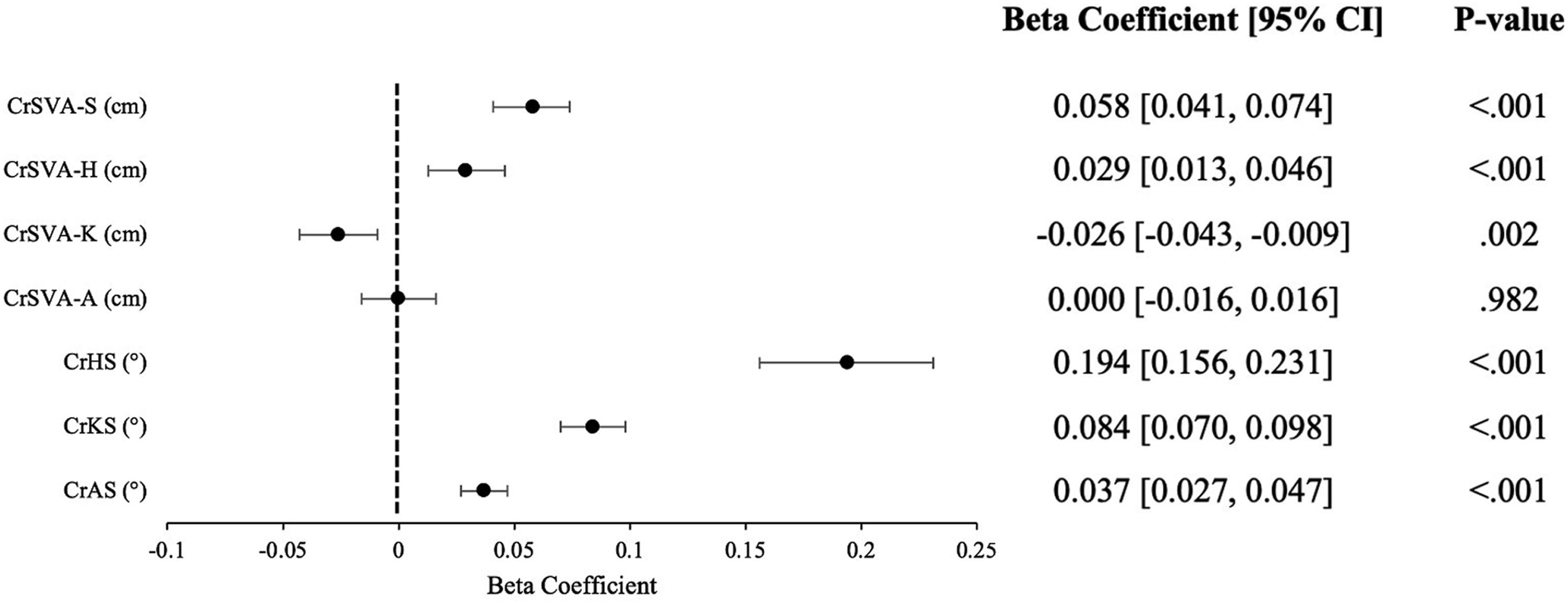
Male sex was a significant positive predictor of CrSVA-S (β = 1.313, [0.743, 1.882], P < .001), CrSVA-H (β = 1.211, [0.641, 1.781], P < .001), CrSVA-A (β = 1.226, [0.673, 1.779], P < .001), CrHS (β = 1.489, [0.211, 2.766], P = .022), and CrKS (β = 0.988, [0.495, 1.480], P < .001) (Figure 5). Forest Plot for Multivariable Linear Regression Models With Male Sex as a Predictor of Global Sagittal Alignment Radiographic Parameters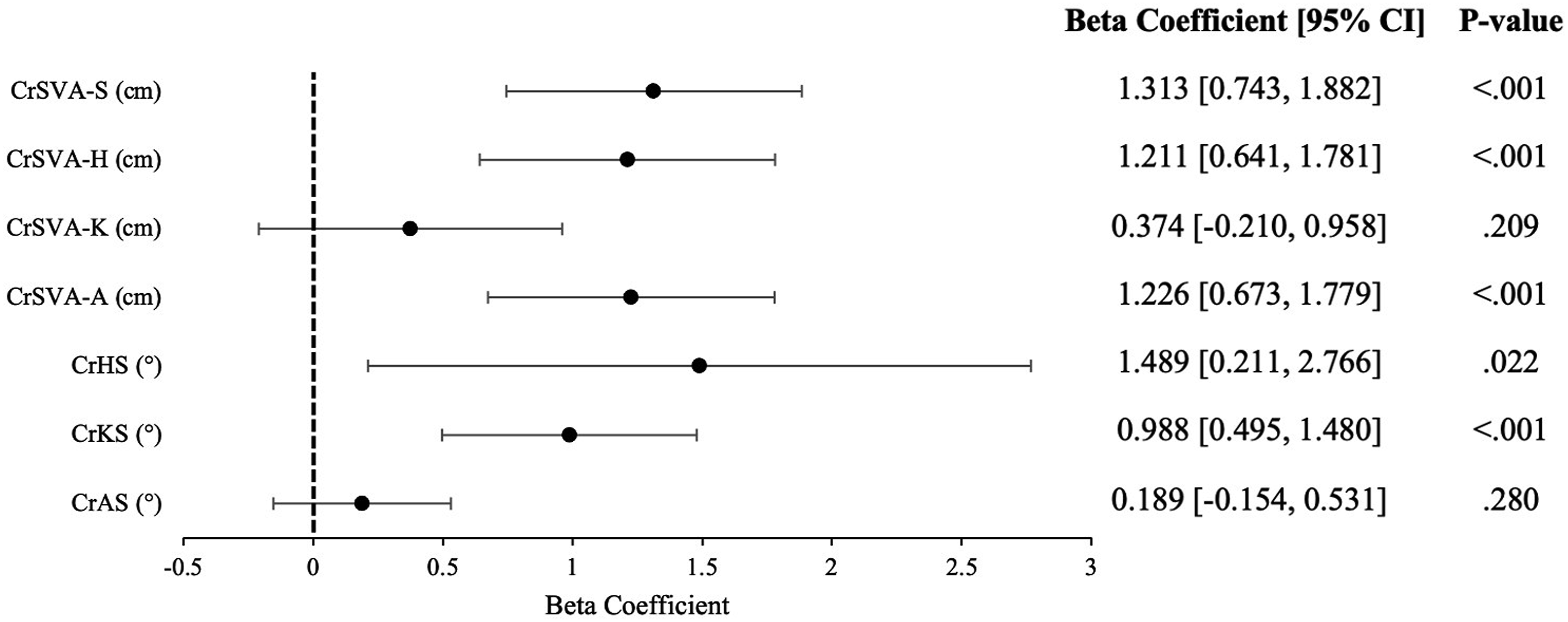
Discussion
Spinal deformity encompasses a broad range of radiographic patterns and clinical presentations, often leading to significant disability and reduced quality of life.10,13 The relationship between spinopelvic sagittal alignment and clinical outcomes in spinal deformity patients has been thoroughly investigated.6,14,15 While emphasis has previously been placed on spinopelvic parameters, recent full-body spine imaging techniques enable the analysis of global sagittal alignment. However, normal reference ranges of global sagittal alignment parameters in patients without spinal deformity have not been well-studied. Thus, the current study aimed to establish normal reference ranges for radiographic parameters of global sagittal alignment.
Spine surgeons have historically evaluated patients using non-global sagittal vertical alignment parameters on lateral spine x-rays.16-22 For example, C7 SVA measures the distance between the plumb line (extending from the center of the C7 vertebral body) to the posterior-superior corner of S1.16-19 Prior studies have demonstrated C7 SVA generally increases with age in both males and females, and there may be a pronounced increase from the 60 s to 80 s age groups.16-19 In the present study, an increase in age by 10 years was associated with a 0.6 cm increase in CrSVA-S and a 0.3 cm increase in CrSVA-H. Interestingly, an increase in age by 10 years was associated with a decrease in the value of CrSVA-K by 0.3 cm. A possible explanation for these findings is that increasing age is associated with progressive thoracic kyphosis and reduced lumbar lordosis which shifts the center of mass more anteriorly relative to the hip or ankle. This shift may explain the positive association between age and both CrSVA-S and CrSVA-H observed in our study. To compensate, patients may bend their knees bringing the knee joint closer to the vertical plumb line, accounting for the negative predictive value seen with CrSVA-K. This postural adjustment allows the lower limbs to absorb some of the anterior shift and reduces shear forces on the lumbar spine. Furthermore, with increasing age, osteoarthritis of the knees may lead to progressive varus alignment, potentially influencing anterior-posterior alignment at the knee joint. We did not find an association between age and CrSVA-A. Meanwhile, male sex was associated with a 1.3 cm greater CrSVA-S and a 1.2 cm greater CrSVA-H and CrSVA-A compared with female sex. CrSVA-K was not significantly associated with sex in our study.
C7 SVA and C2-7 SVA do not account for head position and compensatory changes in pelvic and lower extremity alignment which is a known limitation of non-global sagittal alignment parameters. 16 ,23-25 Thus, CrSVA measures may provide a more accurate understanding of the complex relationship between sagittal alignment, age, and sex. In terms of angular parameters collected in this study, we found that an increase in age by 10 years correlated with an increase in the CrHS angle by 2.0°, the CrKS angle by 0.8°, and the CrAS angle by 0.4°. Male sex was associated with a 1.5-degree higher CrHS and a 1.0-degree higher CrKS angle compared to female sex. CrAS did not have a significant association with male sex.
Prior studies of full-body lateral x-rays have focused on validating these global sagittal alignment parameters in the setting of spinal pathology, such as adult spinal deformity. For example, Kim et al 9 analyzed 108 consecutive adult spinal deformity patients and found CrSVA parameters had a strong correlation with the ODI and SRS-22r total score as well as the SRS-22r pain, self-image, and function subscores. Kim et al 7 in a subsequent study defined and validated an expanded set of measures of global sagittal alignment and demonstrated all radiographic parameters had strong linear correlation with the C7 SVA (the current standard for measuring sagittal balance). Their findings further supported the conclusion that CrSVA parameters were a stronger predictor of outcomes than C7 SVA.,26,27 While SVA measurements can be difficult to target intraoperatively, established normative reference values provide important clinical value. They can guide the decision to pursue surgery, inform the appropriate magnitude of correction, and assess postoperative alignment. Additionally, they can help identify patients who struggle to maintain alignment after surgery and who may benefit from more targeted rehabilitation.
The current literature on global sagittal alignment also highlights pre-to-postoperative changes in adult spinal deformity, adult spinal degeneration, and pediatric deformity pathologies.28-36 Sheikh Alshabab et al examined over 500 adult spinal deformity patients undergoing surgical management and determined postoperative global sagittal alignment is an independent predictor of both satisfaction and disability at 2 years post-operatively. 28 Yet, Smith et al 37 demonstrated when surgeons document their own sagittal alignment goals prior to surgical correction of adult spinal deformity (using C7 SVA, Cobb angle, and thoracic kyphosis), they only achieve goal alignment for all three parameters in about 37% of patients. Reliance on non-global parameters that do not account for pelvic and lower extremity alignment may contribute to this low rate of achieving goal alignment.38,39 Furthermore, current target spinal alignment parameters may not adequately account for age. Lafage et al studied nearly 800 adult spinal deformity patients and determined ideal values for spinopelvic parameters such as C7 SVA increased with age. Older patients had greater degenerative loss of lordosis, more compensation, and were more pitched forward. 40 Older patients may present with baseline alignment that differs from the sagittal parameters observed in younger individuals suggesting that less aggressive correction could be appropriate. However, our study did not evaluate clinical outcomes, so we cannot conclude whether reduced correction leads to improved function in this population. It is important to acknowledge that each patient has an individual baseline alignment, and alignment goals should be personalized. While patients may vary in their individualized needs, establishing reference ranges for global sagittal parameters based on age and sex has the potential to enhance preoperative planning and postoperative outcome assessment.
Limitations
There are several limitations to consider in the present study. First, although patients with prior spine surgery or evidence of deformity on X-ray were excluded from the present analysis, the patients included in this study were symptomatic, ie, presented with either cervical or lumbar related pain, at the time of imaging given their presentation to a spine clinic. Back pain is often unrelated to sagittal alignment and thus these patients still serve as a valuable reference for understanding normal global sagittal alignment. Second, unaccounted differences in patient positioning, shoe wear, and nasion-inion anatomy may contribute to variability in our measurements. For example, heeled shoes tilt the pelvis posteriorly, which may elicit compensatory changes in spine alignment. Patients were instructed to stand in their natural posture with their hands gently resting on a bar in front of them during imaging. While this approach promotes consistency, it may alter spinal alignment compared to a truly relaxed posture with the arms at the side of the body. Furthermore, head-tilt and nasion-inion anatomy (relative locations of nasal root and external occipital protuberance) can affect the location of the plumb line, thus influencing sagittal alignment measurements. Additionally, obesity and joint arthroplasty may influence pelvic tilt and thus influence global sagittal alignment measurements. 41 Obesity is known to increase anterior pelvic tilt, which can increase lumbar extension and thus influence measurements. 42 Lastly, we included patients with hip, knee, and limb pathologies to ensure our cohort remained representative of the broader spine population, many of whom have these comorbidities. These pathologies may have influenced alignment trends to some degree and warrant further investigation in future studies. Nevertheless, our large sample size helps to mitigate these confounding variables in determining mean values across the general population.
Conclusion
While several studies have focused on correlations between radiographic global sagittal alignment parameters and clinical outcomes in patient populations with abnormal spine pathology, normal reference ranges for whole-body sagittal spine alignment parameters have not been well-characterized. Our study provides reference values for radiographic global sagittal alignment parameters in patients without spinal deformity and stratified by age and sex. These reference values can aid in operative planning prior to spine deformity surgery and promote a better understanding of global sagittal alignment in the general population.
Footnotes
ORCID iDs
Consent to Participate
All procedures performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
IRB Approval
This study was approved by the Institutional Review Board (IRB) study number IRB-17-02032.
Disclosure
Samuel K. Cho, MD, FAAOS. American Orthopaedic Association: Board or Committee Member, AO Spine North America: Board or committee member and Fellowship support, ATEC: Paid consultant, Cerapedics: Fellowship support, Cervical Spine Research Society: Board or committee member, Globus Medical: IP royalties and Fellowship support, Scoliosis Research Society: Board or committee member, SIBone: IP royalties. Jun S. Kim, MD. ATEC: Paid consultant, Medcura: Paid consultant.