
Abstract
Study Design:
Retrospective chart review.
Objective:
The goal of this study is to examine the relationship between global alignment and proportion (GAP) score and postoperative orthoses with likelihood of developing proximal junctional kyphosis (PJK).
Methods:
Patients who underwent thoracic or lumbar fusions of ≥4 levels for adult spinal deformity (ASD) with 1-year post-operative alignment x-rays were included. Chart review was conducted to determine spinopelvic alignment parameters, PJK, and reoperation.
Results:
A total of 81 patients were included; baseline and 1-year postoperative alignment did not differ between patients with and without PJK. There was no PJK in 53.1%, 29.6% had PJK from 10-20°, and 17.3% had severe PJK over 20° (sPJK). At baseline, 80% of patients had severely disproportioned GAP, 13.75% moderate, 6.25% proportioned. GAP improved across the population, but improved GAP was not associated with sPJK. Greater correction of the upper instrumented vertebra to pelvic angle (UIV-PA) was associated with a larger PJK angle (PJKA) change (R = -0.28) as was the 1 year T1-upper instrumented vertebra (T1-UIV) angle (R = 0.30), both P < .05. GAP change was not correlated with PJKA change. Postoperative orthoses were used in 46% of patients and did not impact sPJK.
Conclusions:
There was no correlation between PJK and GAP or change in GAP. Greater correction of UIV-PA and larger postop T1-UIV was associated with greater PJKA change; suggesting that the greater alignment correction led to greater likelihood of failure. Postoperative orthoses had no impact on PJK.
Introduction
Adult spinal deformity (ASD) is an increasingly common diagnosis as the global population ages. 1 ASD manifests as coronal and sagittal spine deformities, which may also cause compression of nerve roots or the spinal cord. Patients suffer from postural disturbances, severe back pain, difficulty with ambulation, radiculopathy, and myelopathy. 2 ASD has been shown to dramatically negatively affect quality of life and surgery to correct these deformities can significantly improve both spinal alignment and health-related quality of life.3-7
Correcting spinal deformity is demanding for both the surgeon and the patient; it is fraught with post-operative complications, including mechanical complications necessitating additional surgery that is time consuming, painful, and expensive.8-10 Proximal junctional kyphosis (PJK), a change in proximal junctional sagittal Cobb angle of ≥ 10° and at least 10° greater than preoperative angle, is a devastating mechanical complication of ASD surgery that has been posited to be multi-factorial, influenced by biology, bone quality, neurological disorders, construct factors, and alignment.8,11 Previous studies have examined alignment parameters such as thoracic kyphosis, pelvic tilt, thoracic-pelvic angles (TPA’s), and age-adjusted alignment in order to predict mechanical failure.12-14 However optimal alignment targets to maximize quality of life while limiting PJK have yet to be fully defined.
In 2017, Yigor et al reported a new parameter, the Global Alignment and Proportion (GAP) score which integrates several existing parameters into a holistic score for the prediction of mechanical complications following ASD. 15 This score was developed by analysis asymptomatic patients of the European Spine Society Group (ESSG) database. Ideal angles for radiographic parameters: relative pelvic version (RPV), relative lumbar lordosis (RLL), lordosis distribution index (LDI), and relative spinopelvic alignment (RSA) were defined based on these asymptomatic patients [Figure 1]. The GAP score is calculated by characterizing the difference between this ideal and the patient in question, with an adjustment for age [Figure 2].
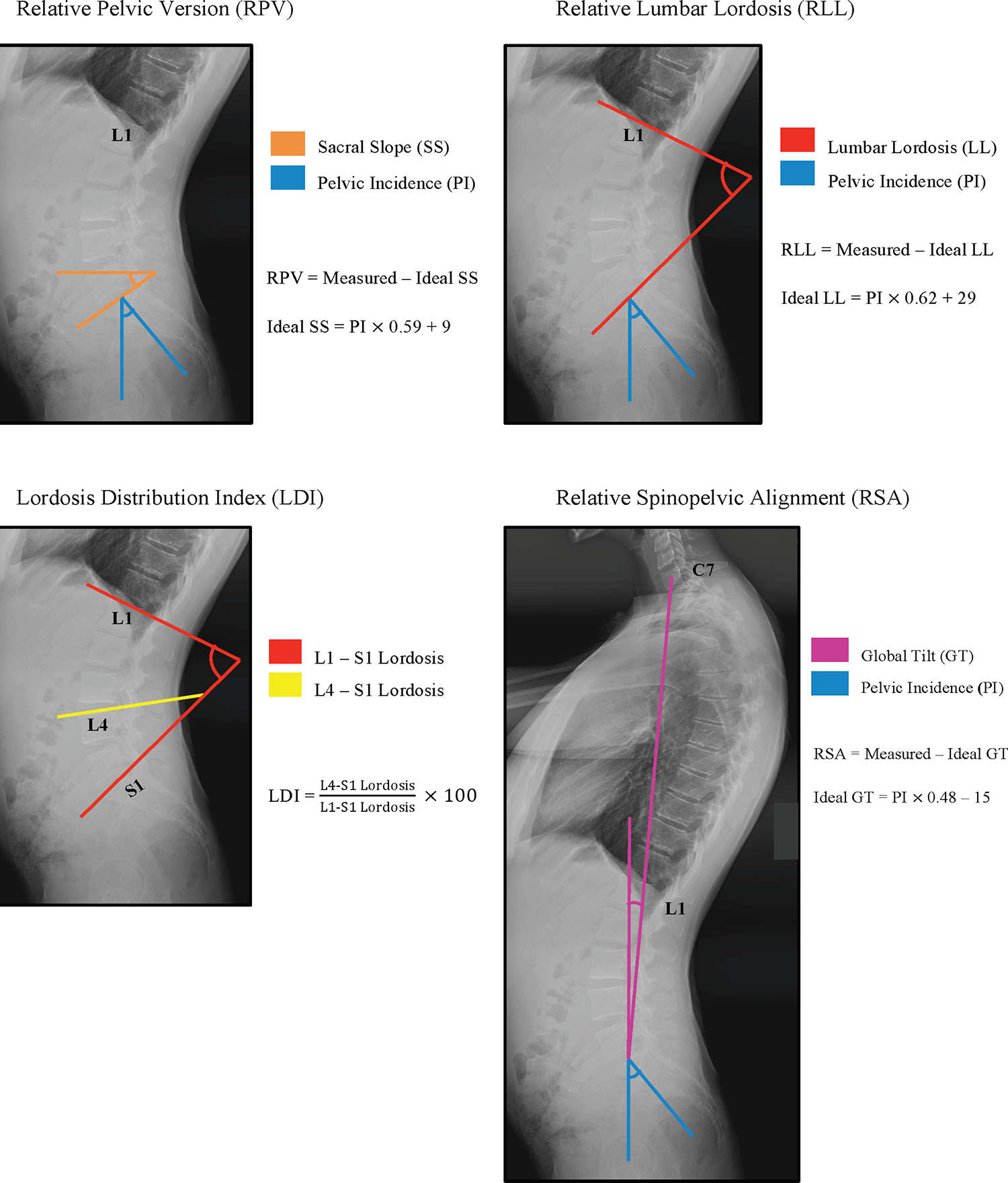
Methods for calculating the radiographic components of the Global Alignment and Proportion score. Relative pelvic version, relative lumbar lordosis, lordosis distribution index, and relative spinopelvic alignment are calculated based on the measured angle in relation to the ideal angle.
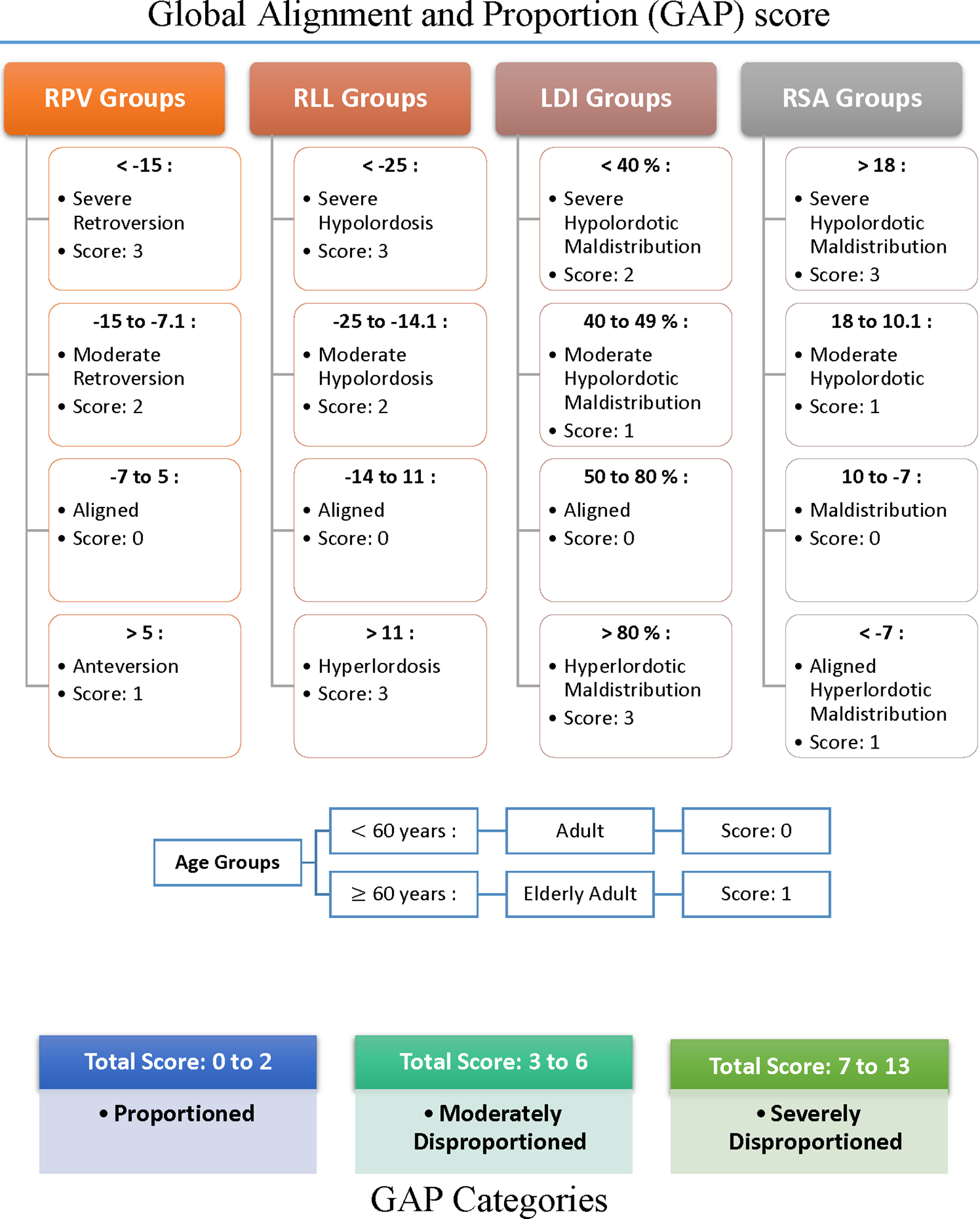
Each component of the Global Alignment and Proportion score includes a value based on the radiographic parameters as depicted in Figure 1 and an age component. Patients are given a score of each parameter, which are summarized as a total score (range 0-13) and further subcategorized. RPV, relative pelvic version; RLL, relative lumbar lordosis; LDI, lumbar distribution index; RSA, relative spinopelvic alignment.
Postoperative bracing is often used following ASD surgery, however its efficacy has yet to be defined. 16 There is a paucity of literature regarding their efficacy and cost utility in the thoracolumbar spine following corrective surgery. While some studies have demonstrated decreased segmental motion with orthoses, others have reported multiple complications such as pressure ulcers without improvement in pain control or fusion rate.17,18
The goal of this study is to examine the relationship between GAP score and TPA’s with likelihood of developing PJK in ASD patients who have undergone corrective surgery.
Methods
A retrospective chart review was conducted to identity ASD patients who underwent 4 or more levels of thoracolumbar fusion from 2013 to 2018 at a single, high-volume academic medical center. Inclusion criteria were: 1) age greater than or equal to 18 years old, 2) 4 or greater thoracic or lumbar levels fused, 3) primary or revision surgery, 4) at least 1-year postoperative alignment x-rays available for review. Exclusion criteria were: 1) age of 17 years or less, 2) active malignancy, 3) active infection, or 4) trauma as indication for surgery. This study was approved the Institutional Review Board.
Patient demographic data including age, sex, and body mass index (BMI) was collected by manual chart review.
Radiographic review was conducted to determine the following spinopelvic alignment parameters: pelvic incidence (PI), sacral slope (SS), lumbar lordosis (LL), L4-S1 lordosis, global tilt, C2-pelvic angle (C2PA), T1-upper instrumented vertebra (T1-UIV), T1-pelvic angle (T1PA), T9-pelvic angle (T9PA), T10-pelvic angle (T10PA), L1-pelvic angle (L1PA), and upper-instrumented vertebra-pelvic angle (UIV-PA) [Figure 3].
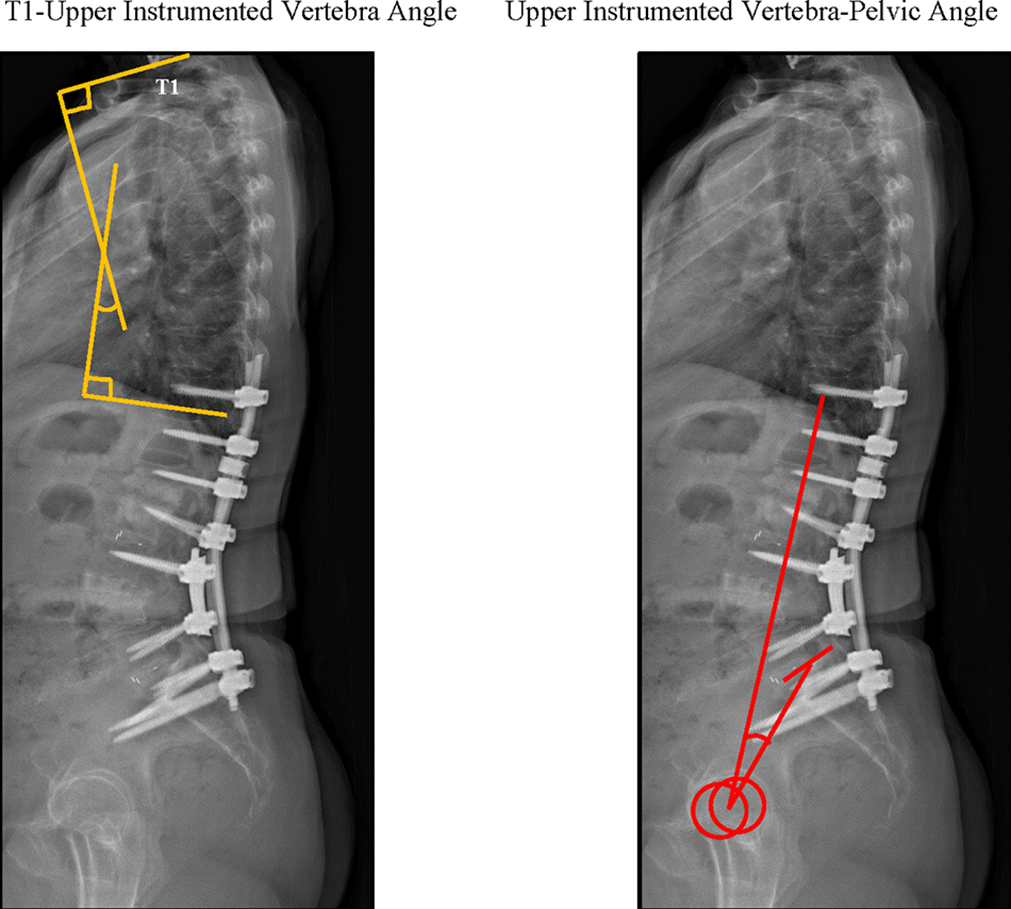
T1-Upper Instrumented vertebra level and upper instrumented vertebra-pelvic angle were explored as candidate angles that may predict PJK.
The pre and postoperative GAP scores were calculated from these data and patient age according to the original article [Figure 2]. 15 In certain cases, some parameters could not be measured by radiograph, hence some discordance is sum of patients.
Patients were categorized into 1 of 3 GAP categories preoperatively and immediately postoperatively: proportioned (P), moderately disproportioned (MD), and severely disproportioned (SD). The difference in ideal T1PA as previously defined and actual T1PA was also calculated. 12 Chart review was performed to assess reoperation. Radiographs were reviewed up to 1-year post operatively in order to determine alignment. The rate of radiographic PJK (change of 10-20°) and severe PJK (sPJK)(change >20°) was determined for each group.
Patient demographics, preoperative, and postoperative alignment were summarized for the entire study population using descriptive statistics. Means and standard deviations were reported for continuous variables, and percentages were reported for categorical variables.
Patients were stratified by whether they developed severe PJK (sPJK)(change of >20° in the Cobb angles between the upper instrumented vertebra (UIV) and the 2 levels above the UIV), radiographic PJK (rPJK)(change of 10-20°), and zero PJK (zPJK) (change of <10°) over the study period. For comparison, we sorted the groups into sPJK and those with <20° of PJK (no PJK). Patients who had sPJK were compared to the no PJK group in terms of baseline characteristics, osteoporosis, GAP scores, and other alignment parameters. Patients were stratified by preoperative GAP category (P, MD, or SD) then rates of sPJK were compared between the 3 groups. Patients were also stratified into those who had improvement, no change, or decline in GAP score postoperatively and rates of sPJK were compared between those 3 groups.
Independent-sample t-tests and Chi-square tests were used for continuous and categorical variables, respectively. Pearson Chi-square tests were used if at least 80% of the cells had expected values of at least 5. Fisher’s exact tests and maximum likelihood ratios were utilized if the sample size assumption for Pearson’s Chi-square test was not met. Linear associations between continuous variables were evaluated via Pearson product-moment correlations.
Statistical significance was set at P < 0.05. All statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS Inc., Version 23.0; Armonk, NY: IBM Corp).
Results
Baseline Characteristics
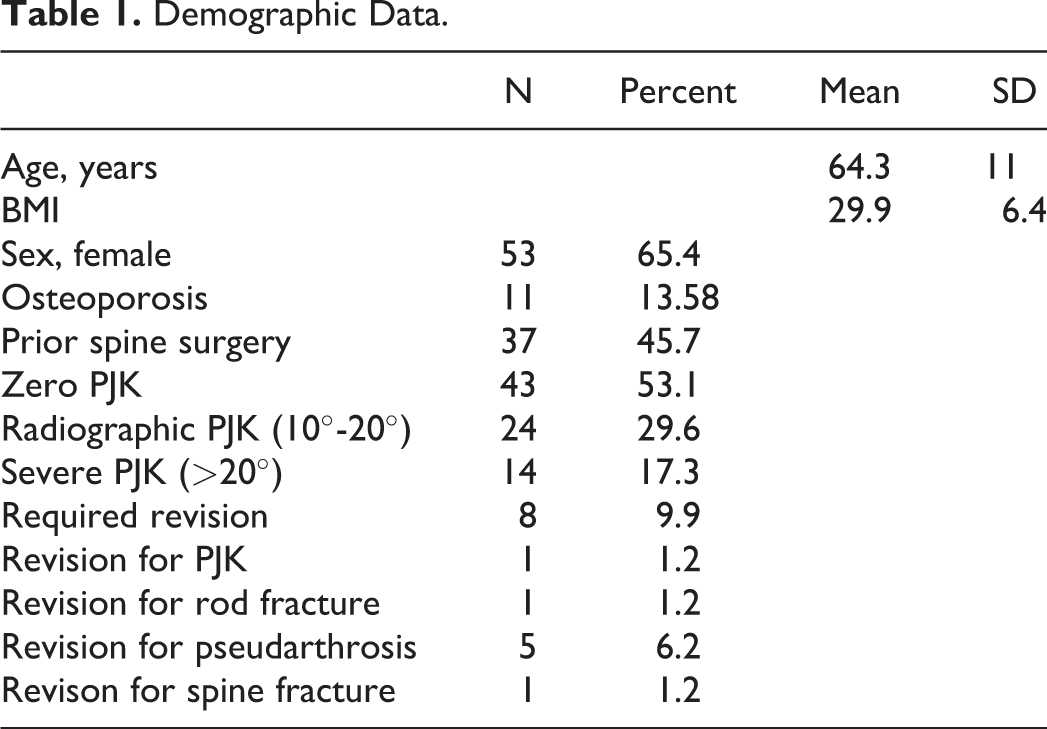
A total of 81 patients were included with a mean age 64 years, mean BMI 29.9, and 65.4% female (Table 1). Osteoporosis was present in 11 patients (13.6%).
Demographic Data.
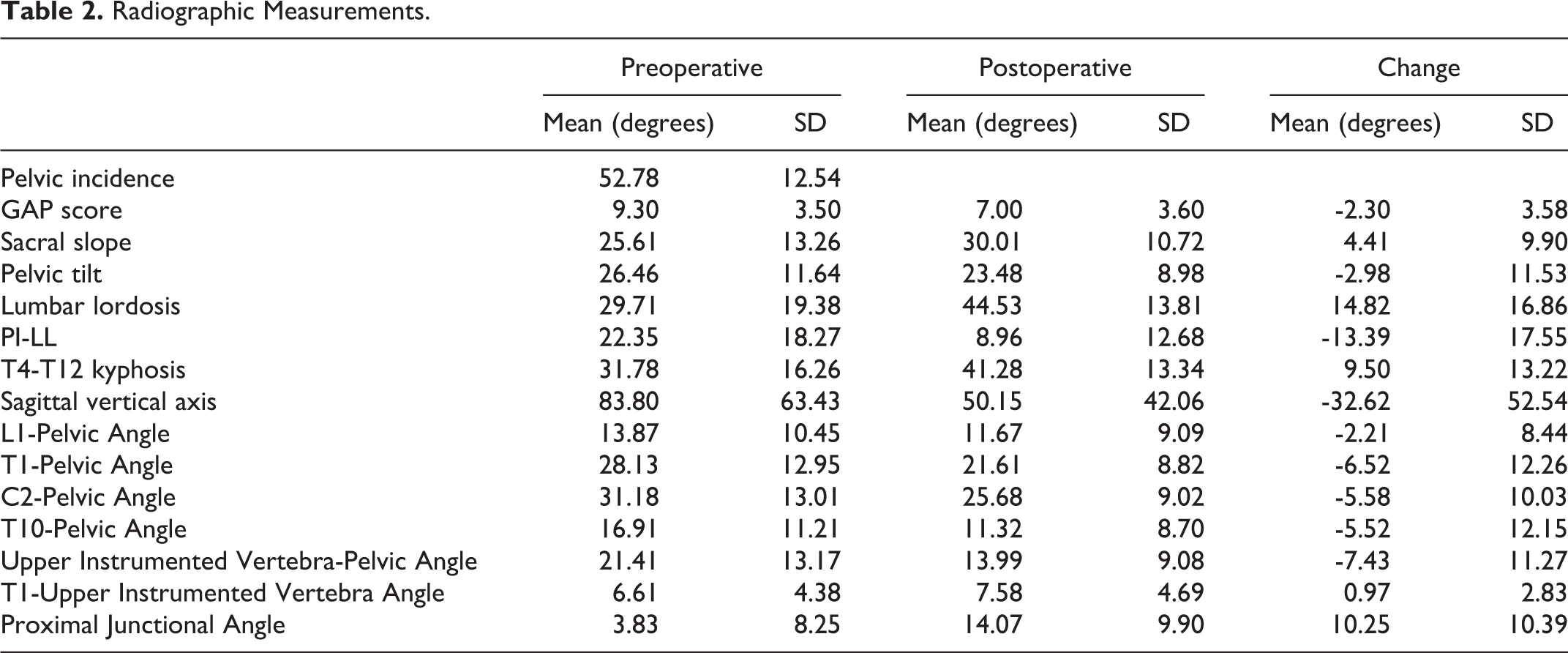
There was zPJK in 43 patients (53.1%); 24 had rPJK (29.6%) and 14 had sPJK (17.3%). Of those with sPJK, 8 underwent revision surgery: one each for PJK, rod fracture, and spine fracture, and five for pseudarthrosis. Patients had significant correction of their spinal deformity; preoperative GAP score improved from 9.3 to 7.0 at1-year postoperatively (Table 2). Other alignment parameters including sagittal vertical axis (SVA), L1-pelvic angle, T1-pelvic angle, C2-pelvic angle, T10-pelvic angle, and upper-instrumented vertebra—pelvic angle (UIV-PA) also improved (Table 2).
Radiographic Measurements.
Radiographic Change
Those patients with sPJK, were found to have significantly lower preoperative T1-UIV angle that those with nPJK (4.5
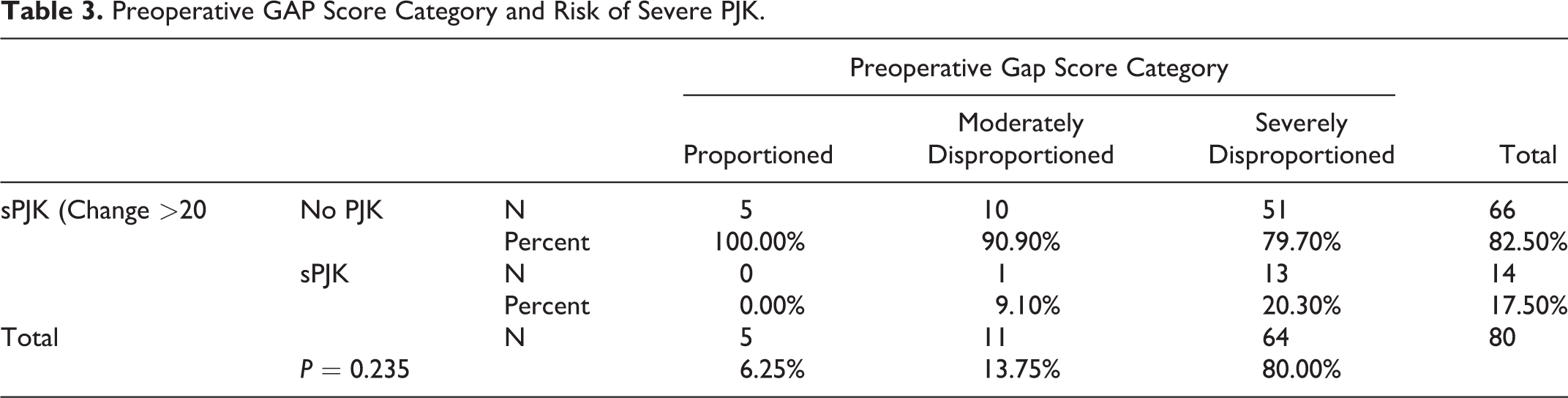
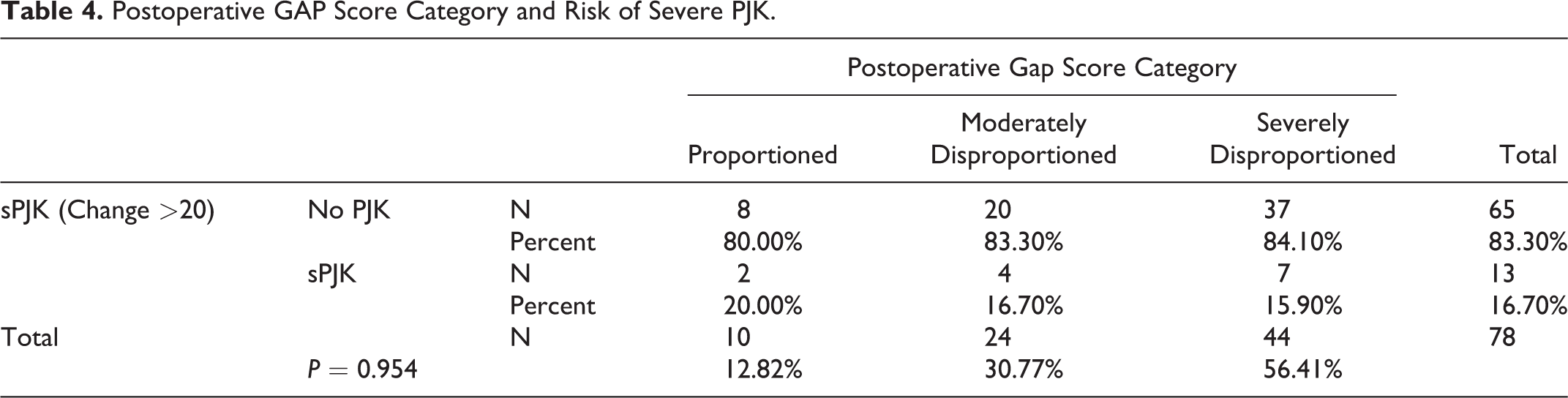
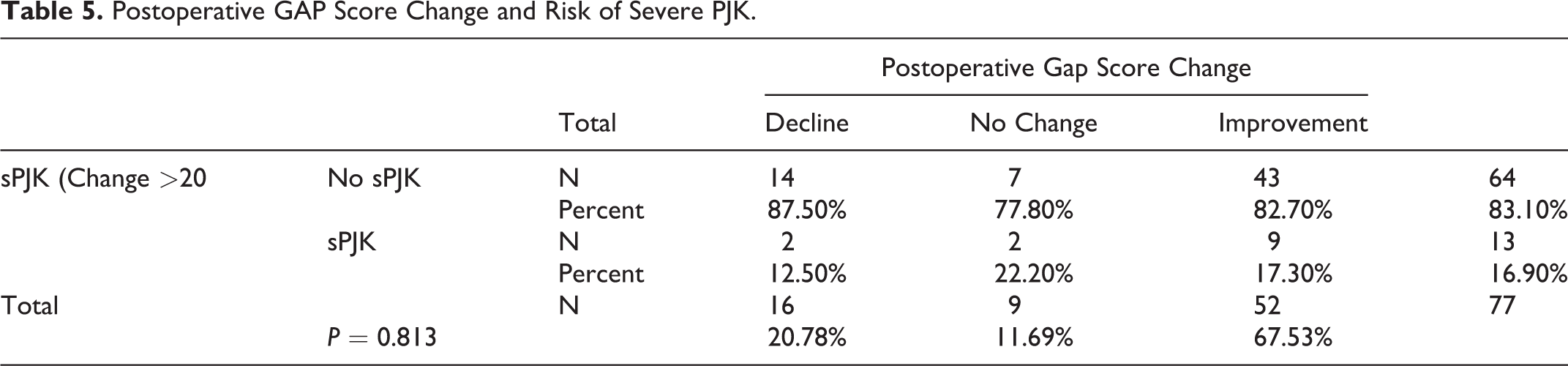
Preoperatively, 64 patients (80%) had severely disproportioned GAP score, 11 (13.75%) moderately, and 5 (6.25%) proportioned (Table 3). Concurrent with improvement in other alignment parameters, at 1 year postoperatively, GAP scores globally improved: 44 (56.4%) patients were severely disproportioned, 24 (30.7%) moderately, and 10 (12.8%) proportioned (Table 4). Interestingly, improvement, decline, or stability of GAP score was not associated with sPJK (Table 5). There was no association between pre or postoperative GAP score and PJK (Tables 4 and 6).
Preoperative GAP Score Category and Risk of Severe PJK.
Postoperative GAP Score Category and Risk of Severe PJK.
Postoperative GAP Score Change and Risk of Severe PJK.
Risk of Severe PJK by Pre and Postoperative GAP Score.

Greater correction of the UIV-PA was associated with a larger PJK angle change (R = -0.28, P = 0.012) as was the 1 year T1-UIV angle (R = 0.30, P = 0.005). GAP score change was not correlated with PJK angle change. The magnitude of T1PA correction was not associated with sPJK, P > 0.05.
Orthoses
Postoperative orthoses were used in 46 patients, representing 56.8% of the cohort. Of those braced, 9 (19.6%) developed sPJK. Of those who were not braced, 5 (14.3%) developed sPJK, P = 0.57 (Table 7). Osteoporosis was also not associated with sPJK in this cohort.
Postoperative Othrosis Use and sPJK.

Discussion
In ASD, the dual goals of correcting global alignment while minimizing postoperative complications remains a challenge. Multiple authors have attempted to define alignment goals to optimize outcomes and quality of life.19-21 However it is well established that complications of ASD surgery, including revision surgery and PJK significantly detract from postoperative quality of life. 22 This study aims to investigate whether the GAP score, which combines patient specific alignment parameters with age, predicts sPJK. In our cohort of patients, there was no correlation between postoperative GAP score or change in GAP score and sPJK. It is notable that the patients in our cohorts tended to be disproportioned both pre and postoperatively, perhaps suggesting a relative undercorrection of alignment surgery according to GAP criteria of “proportioned.” In fact only 10 patients (12.8%) were “proportioned” postoperatively although 52 patients (67.5%) did see some improvement in their numerical GAP score. As aggressive sagittal correction has been associated with sPJK, it is possible that the findings in this cohort of patients are not widely applicable to patients with more significant change GAP score.23,24 Further examination of patients who have correction from severely or moderately disproportioned preoperatively to proportioned postoperatively is warranted to define whether this alignment goal improves quality of life.
Several authors have examined the GAP score with mixed results; Bari et al examined a consecutive cohort of 149 ASD patients followed for a minimum of 2 years and failed to find an associate of GAP score or categories with mechanical failure or revision in ASD surgery. 25 Bari’s study has a notable amount of revision patients, 59% compared to 30% in Yilgor et al’s. The present study compares with almost 46% revision cases. Jacobs et al conducted a retrospective review of 39 ASD patients with a minimum of 2 years radiographic follow up and did find that the GAP score was correlated with mechanical complications, performing favorably to the SRS-Schwab classification. 26 Of note, mechanical complications in this study included proximal junctional failure (PJK ≥20°) in addition to proximal junctional kyphosis ≥10°, distal junctional kyphosis and failure, rod breakage, and implant related complications including screw loosening. These complications were reported in aggregate, not independently so it is difficult to compare rates to those found in this study. Ohba et al retrospectively reviewed 128 patients who underwent deformity surgery and found a positive correlation between increased proximal junctional angle 2 years post operatively, Oswetry Disability Index, and GAP score. 27 In this study, greater correction of UIV-PA and larger postoperative T1-UIV was associated with greater PJK angle change; suggesting that the greater alignment correction led to greater reciprocal kyphosis that may or may not meet the definition of sPJK.
There is very limited data examining postoperative orthoses for ASD patients. Crawford et al performed a retrospective review of 112 ASD patients and did not find a difference in PJK between those who were braced and those who were not. 28 Most other studies address bracing in the context of fusion and stabilization following thoracolumbar fractures, where there is a lack of clinical or biomechanical evidence to support their use, although some studies have demonstrated decrease in pseudoarthrosis with bracing at the expense of patient comfort. 29 There is biomechanical evidence to suggest that thoracolumbosacral orthosis (TLSO) dues reduce L3-L5 motion and motion at each individual lumbar motion segment. 30 However bracing is not without downsides; it raises costs, inhibits mobility, and is associated with skin breakdown. 31
This study has several limitations. It is a retrospective analysis with a limited number of patients. Most of the patients in this study were not corrected to the degree considered proportioned by the GAP score, thus the effect of larger corrections may not be accurately reflected. This study does not report on quality of life measures associated with either alignment or sPJK, however it has been established that improvement in sagittal alignment also improves quality of life measures and PJK decreases them. 32 Orthosis type was not specified in data extraction and certain types of orthoses are known to be more rigid than others.
This study adds to a growing body of work examining GAP score and other alignment targets in adult deformity surgery. We determined that GAP score does not predict sPJK.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.