
Abstract
Study Design
Retrospective Cohort Study.
Objectives
This study aimed to examine the characteristics of medical malpractice claims related to spinal fracture treatment in our country between 2018 and 2023.
Methods
The study utilized our database to analyze 65 closed spinal fracture medical malpractice cases. The inclusion criteria were vertebral fracture, traumatic origin, age >18 years, and available data. The study evaluated patient demographics, fracture characteristics, treatment details, complications, and the nature of the malpractice complaints.
Results
The results showed that 22 out of 65 cases were found to involve malpractice by the committee. The most common complaints were treatment errors, failure to diagnose the condition, and postoperative paralysis. In 22 cases of malpractice, there were twelve cases of failure of diagnosis, 3 cases of misdiagnosis, 6 cases of treatment error, and 1 case of inappropriate postoperative management. Three of the malpractice cases involved orthopedic surgeons, while 19 involved neurosurgeons. The study found no significant differences in any of the parameters between patients with and without malpractice. Five of the 15 defendant orthopaedic surgeons, 5 of the 41 defendant neurosurgeons, 6 of the 24 defendant emergency medicine specialists and 6 of the 8 defendant radiologists were found to be at fault in malpractice lawsuits.
Conclusions
Neurosurgeons receive the most complaints, but radiologists have the highest rate of malpractice, with 6 out of 8 of these cases being malpractice. The findings highlight the importance of accurate diagnosis and treatment in reducing the risk of malpractice claims in spinal fracture cases.
Introduction
Trauma and orthopedic surgery are often considered highly litigated specialties because of the volume of operations performed and the potential concerns arising from errors.1,2 Among medical subspecialties, spinal surgery is particularly affected by malpractice claims. 3 The number of medical malpractice claims against orthopedic surgeons is increasing due to the growing demand for functional recovery after surgery, heightened awareness of patient rights, and easy access to patients’ medical information. Orthopedic surgery has been subject to medical malpractice claims for more than 130 years. 4 Medical malpractice is a pervasive issue encountered by most physicians during their career. A 2017 study indicated that 99% of physicians in surgical subspecialties face at least one malpractice claim during their careers. 5 Despite the anticipated rise in orthopedic malpractice claims, significant gaps exist in the existing literature on this topic. Respect for patient autonomy has become an increasingly important focus in recent years.6,7 It is crucial to continually expand our understanding of the factors associated with medical malpractice and adopt preventive strategies.
Adults with spinal fractures experience a considerable degree of impairment, and in some cases, surgical intervention is necessary. 8 Spinal fractures are associated with increased morbidity, mortality, and disabilities. In many cases, the latter is the most evident cause. In some instances, surgical intervention is imperative to ensure proper spinal alignment and to expedite healing. Spinal fractures often result in numerous subsequent complications, including elevated mortality rates and substantial medical expenses. 9 The diagnosis, treatment, and follow-up of spinal trauma can be challenging and potentially prone to errors by orthopedic surgeons and neurosurgical specialists. However, a study analyzing malpractice lawsuits related to spinal trauma has not yet been conducted.
This study aimed to examine spinal surgery malpractice claims in terms of the characteristics of the case, type of hospital where the case occurred (public vs private hospitals), anatomical location affected, clinical outcome of the case (death vs permanent disability), and final medicolegal decision regarding the claim (confirmed malpractice vs denied malpractice).
Materials and Methods
In this investigative study, cases of patients diagnosed with spinal fracture who were referred to the 7th Specialized Board of Forensic Medicine between 2018 and 2023 for the evaluation of malpractice claims will be examined through retrospective analysis. To this end, the National Judicial Network Information System (UYAP), a program utilized by all justice system entities and court systems in our country, was employed to analyze all closed spinal fracture medical malpractice cases. Prior to the initiation of the scientific study, the necessary consent was obtained from each patient for the utilization of their data.
It has the largest collection of court records of cases submitted by judges and lawyers to arbitration or courts. For deeper knowledge, each case in UYAP contains comprehensive case summaries, court records including expert witness reports, and information regarding the plaintiffs and defendants, and radiological images are also available in most cases. In our county, medical malpractice cases are investigated by the malpractice specialization committee with the permission of the Council of Forensic Medicine Ethics Committee using the UYAP database. In order to guarantee that the established ethical principles are being adhered to, the our Ethics Committee formally approved the study protocol (2024/141). The inclusion criteria were as follows: vertebral fracture, traumatic origin, age >18 years, and complete UYAP data. Exclusion criteria were pathological fractures, osteoporotic fractures, sacral fractures, isolated posterior spinal element fractures, and data prior to 2014 due to missing information. The study included 65 patients. Utilization of the UYAP prompted the initiation of inquiries pertaining to vertebral injury, with the subsequent filtration of outcomes employing the spine fracture metric. A subsequent investigation was conducted using the following keywords: “thoracolumbar fracture,” “cervical fracture,” “thoracic fracture,” “lumbar fracture,” “spinal cord injury,” “vertebral compression fracture,” “vertebral fracture dislocation,” “burst fracture,” “posterior ligamentous complex injury,” and “flexion-distraction vertebral fracture.”
In the context of our nation’s legal system, the initiation of legal proceedings pertaining to medical malpractice entails a procedural sequence. The initial step in this sequence involved submitting a request for an expert opinion from a medical professional within the hospital setting. If such an assessment reveals a potential instance of malpractice, the case is referred to the relevant forensic medicine institution for further evaluation. Because of lawsuits, all cases were analyzed by experts from the relevant department of the Institute of Forensic Medicine. The institution has a team of highly skilled and qualified medical professionals who are leaders in their respective specialties (orthopedic surgeons, neurosurgeons, radiologists ie,). Decisions regarding malpractice are made after consulting with a physician who is an expert in the relevant sub-specialty. For each case identified from the database, patient demographics (age and sex), region (cervical, thoracic, and lumbar), cause of fracture, reason for litigation, complications, and case characteristics were recorded.
In our country, healthcare services are delivered by both public and private hospitals. Patients receiving care at private hospitals are responsible for paying fees, whereas those treated at public hospitals are exempt from financial obligations. An evaluation was conducted at the hospital where the surgery for spinal trauma was performed. The duration of hospital stays, need for surgical intervention, and temporal interval between trauma and surgery were determined through a subsequent review of the medical records. The etiologies of spinal fractures were divided into the following categories; falls from height, blunt trauma, and traffic accidents. As is widely recognized, spinal traumas are frequently observed in conjunction with abdominal, cranial, and thoracic injuries. In this study, we evaluated additional injuries sustained in the patient cohort. The team that operated on the operated patients comprised the following specialists: orthopedic surgeons and neurosurgeons. Malpractice claims were made in the following specialties: emergency medicine, neurosurgeons, musculoskeletal radiology, orthopedic surgeons, and physical therapy. Surgeries were performed using 4 different surgical techniques: posterior instrumentation, posterior instrumentation combined with anterior instrumentation, anterior instrumentation, and vertebroplasty. The degree and location of malposition of the pedicle screw remain subjects of considerable debate. In this study, malposition was defined as instances where the screw did not traverse the pedicle but instead deviated medially into the canal or laterally away from the pedicle. The following types of complications were examined: appropriate treatment, delayed or missed diagnosis, lack of informed consent, excessive or inappropriate surgery, surgical errors, and postoperative management errors. In our country, in cases of spinal fractures, additional injuries such as thoracic injuries may be present; therefore, patients may be referred to a higher-level center where departments such as thoracic surgery may be required for diagnosis and treatment. In instances where a patient is referred to a neurosurgeon or orthopaedic surgeon from the emergency department, and a definitive diagnosis cannot be made, the patient is then transferred to a high-level center for comprehensive treatment without a diagnosis; this is referred to as ‘failure to diagnose.’ The failure to undertake this consultation process also resulted in the patient being referred without a diagnosis, which was subsequently referred to as failure to diagnose. Preoperative examinations of the patients were performed, and their neurological status was noted. Treatment complications were characterized by postoperative neurologic injury, implant failure, dura mater injury, surgical site infection, permanent weakness, and chronic pain.
Statistically Analyses
The IBM Statistical Package for Social Science Statistics for Windows version 29.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Descriptive analysis was performed using dispersion parameters for quantitative data (mean or median, standard deviation, minimum, and maximum), and expressed as percentages for qualitative data. Student’s t-test was performed to compare quantitative, normally distributed variables using descriptive statistics. Fisher–Freeman–Halton test, Fisher’s exact test, and Pearson’s chi-square test were used to compare qualitative variables. Statistical significance was set at P < 0.05.
Results
Demographic Data of Patients
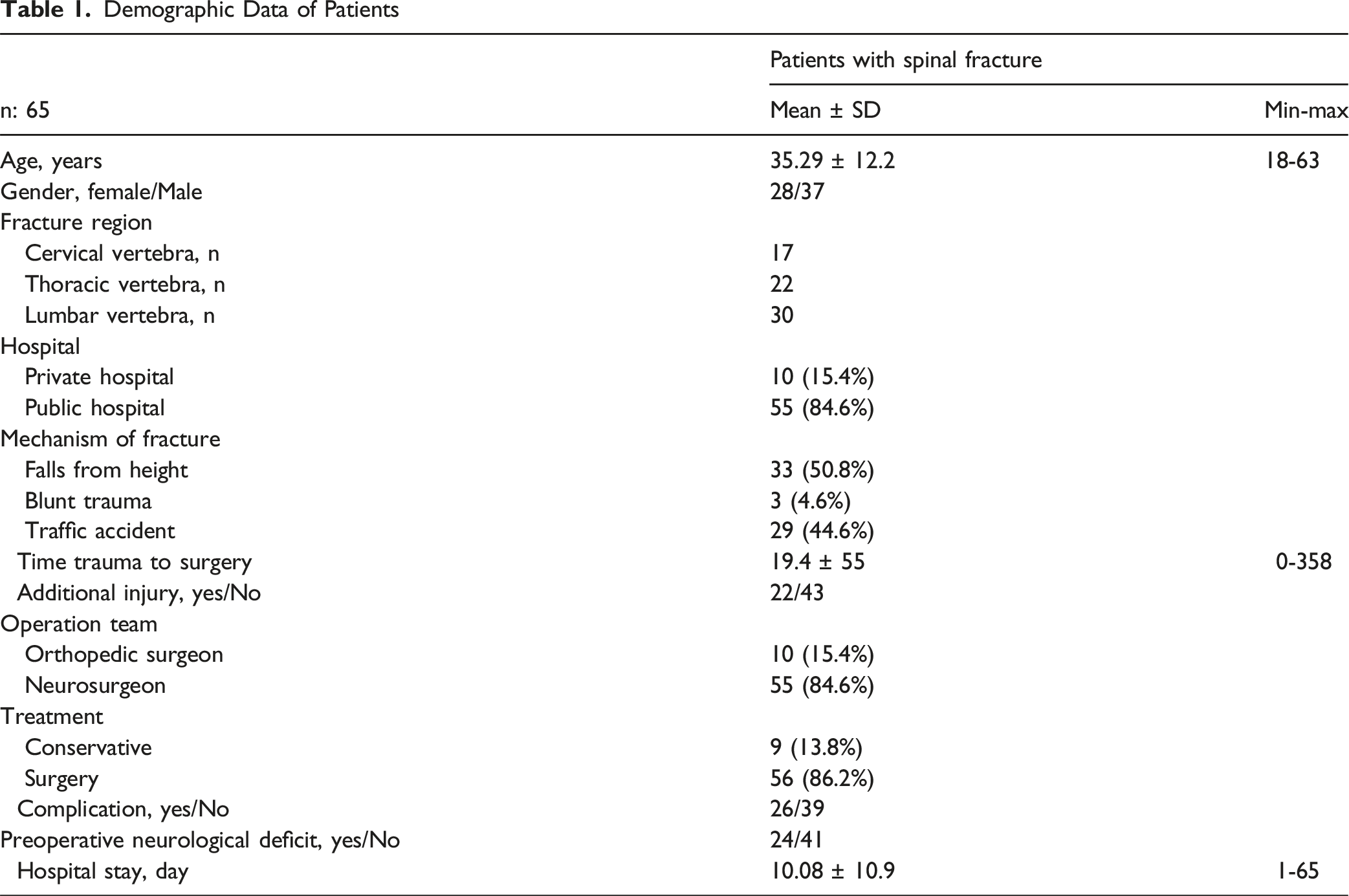
55 patients (84.6%) were treated in public hospitals and 10 (15.4%) were treated in private hospitals. The average time between trauma and surgery was 19.4 ± 55 (0-358) days. 22 patients had injuries other than a fractured spine. Seven patients had mediastinal injuries (rib fractures or haemotrax), 4 had abdominal injuries, 3 had tibia fractures, 2 had pelvic injuries, one had head trauma, one had elbow fracture, one had nose fracture, one had ankle fracture, one had distal radius fracture, and one had talar fracture. 56 patients were treated with surgery, and 9 patients were followed up with conservative treatment. The average length of hospital stay was 10 ± 10 days (range, 1-65 days).
Ten patients were treated by orthopaedic surgeons, while 55 were treated by neurosurgeons. Complications were observed in 26 patients (40%), with the majority involving screw malpositioning. 24 patients had neurological deficits due to trauma prior to treatment. However, neurological deficits were observed in 28 patients during the final follow-up. Twenty patients underwent a single revision operation, whereas 3 patients underwent more than 1 revision operation.
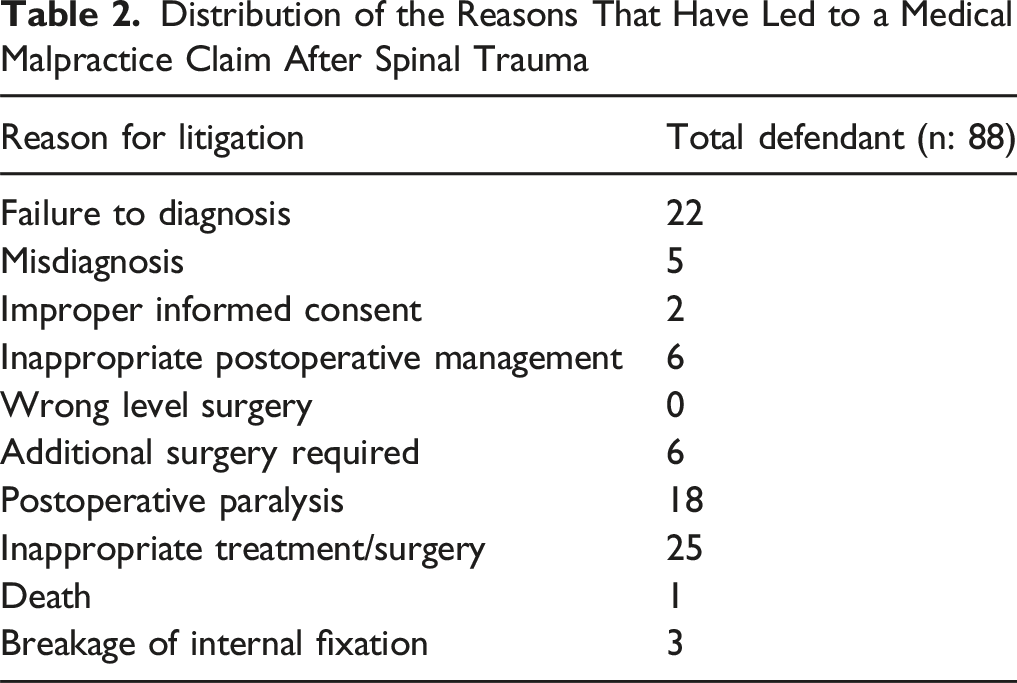
Distribution of the Reasons That Have Led to a Medical Malpractice Claim After Spinal Trauma
Comparison of Clinical Characteristics Between Cases With Malpractice and Without Malpractice
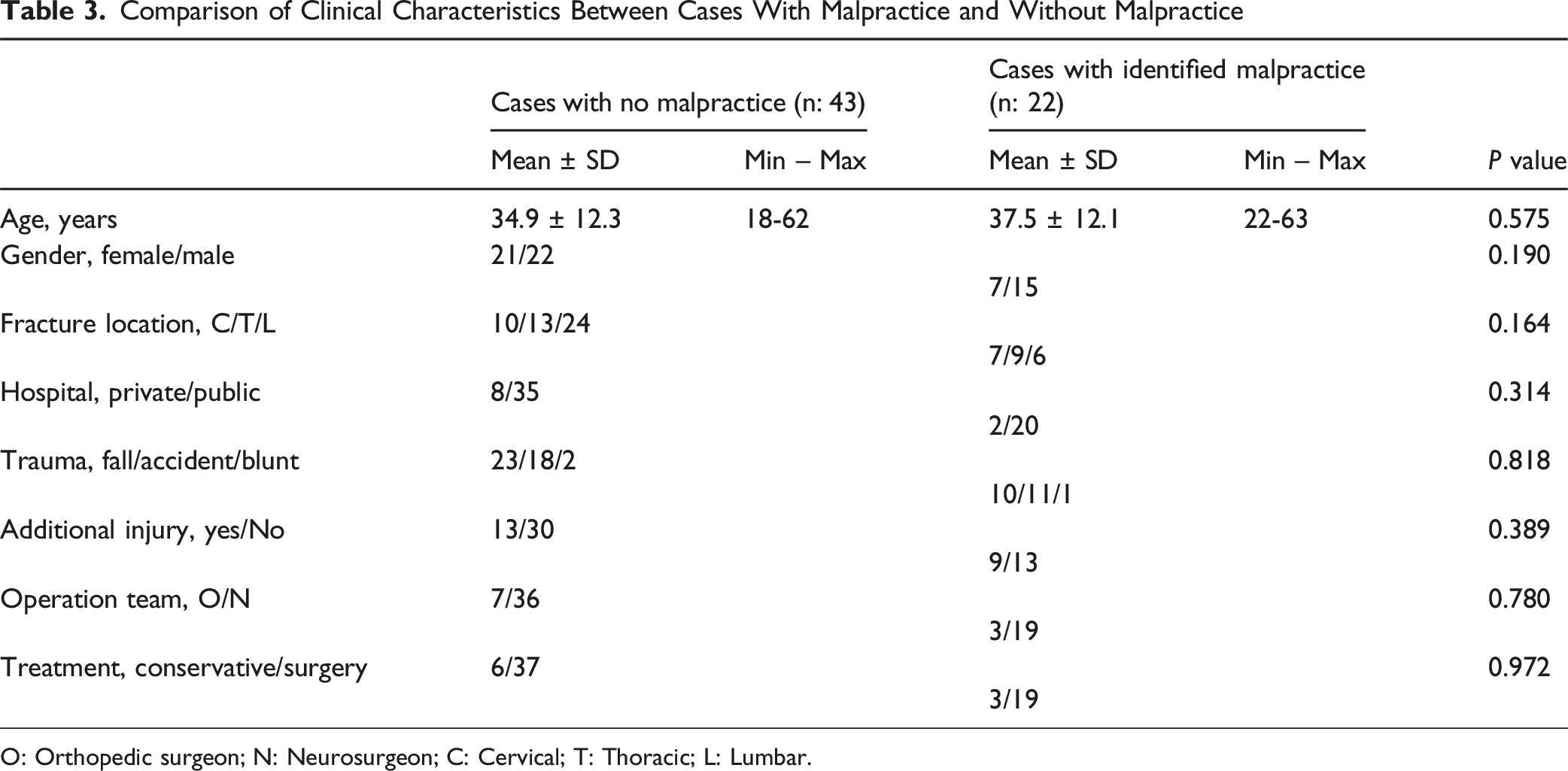
O: Orthopedic surgeon; N: Neurosurgeon; C: Cervical; T: Thoracic; L: Lumbar.
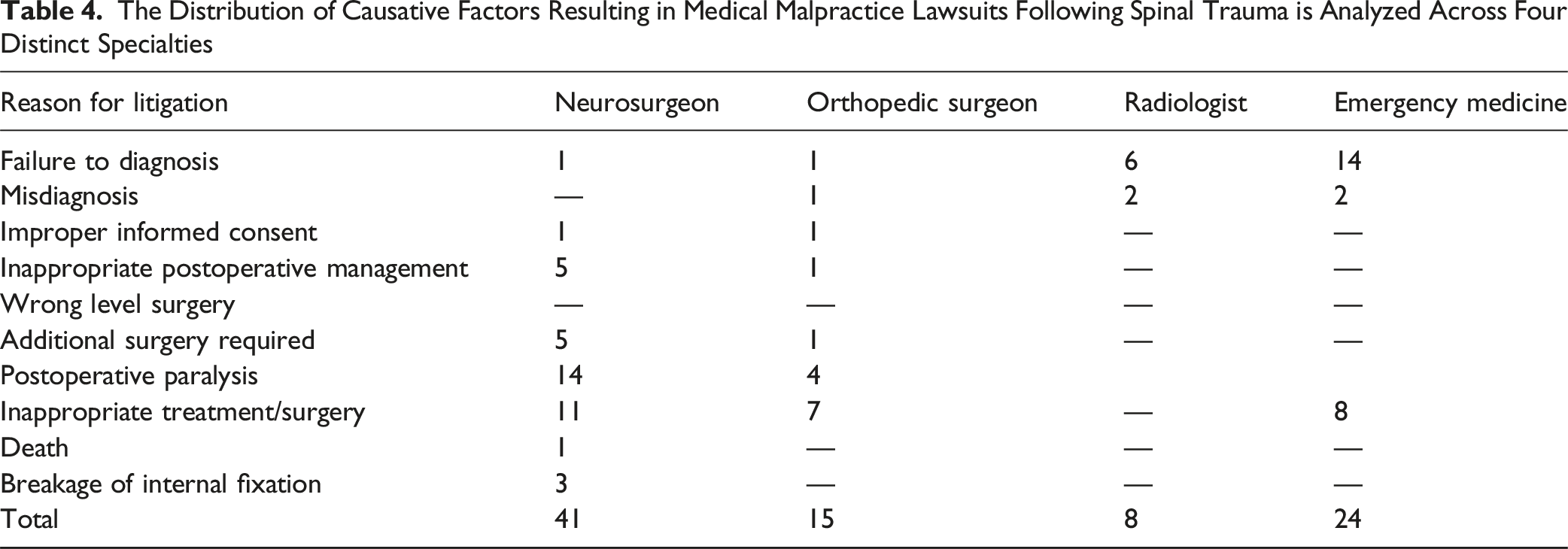
The Distribution of Causative Factors Resulting in Medical Malpractice Lawsuits Following Spinal Trauma is Analyzed Across Four Distinct Specialties
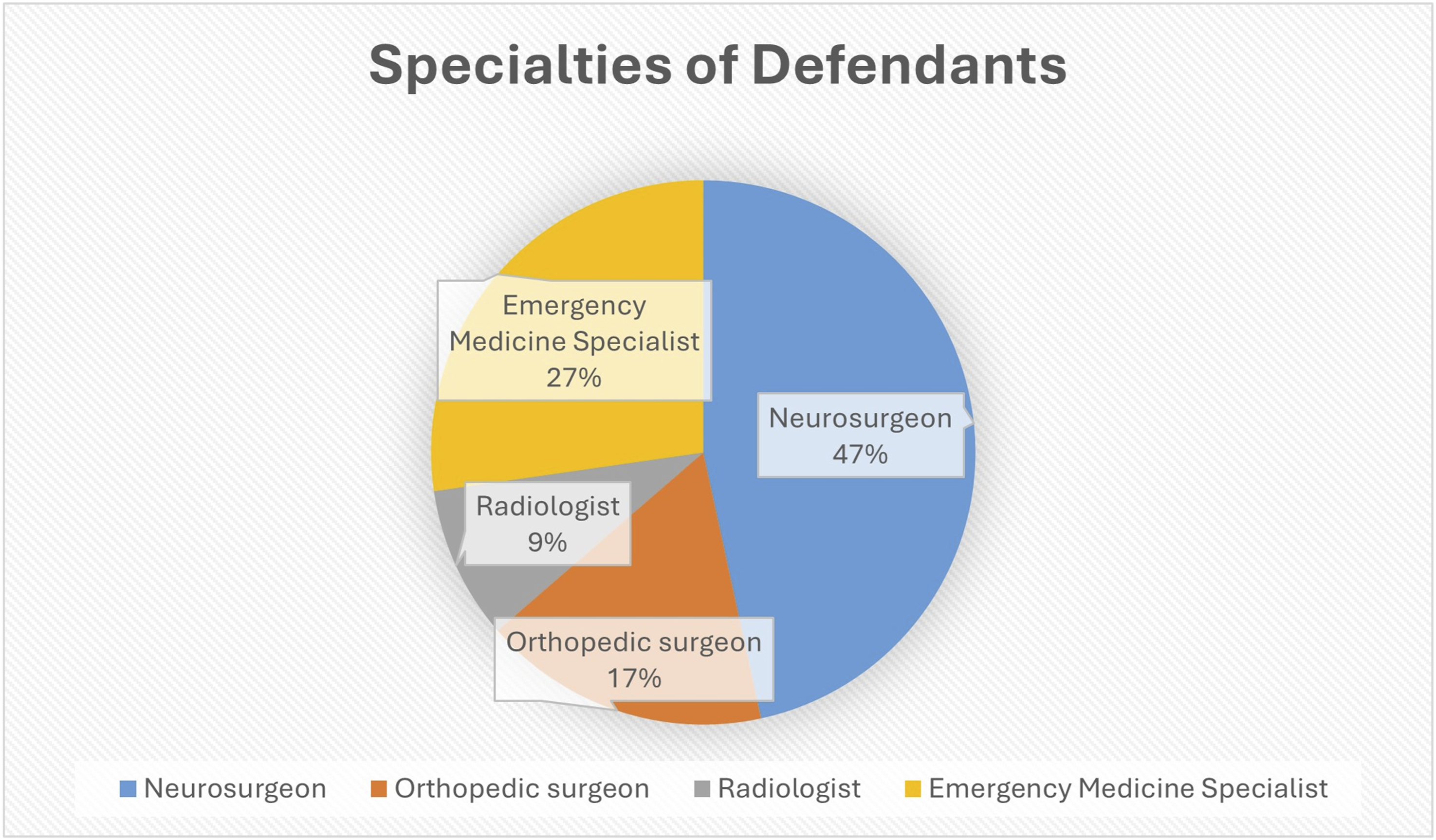
The Figure Shows the Specialties of Defendants Named in Spinal Fracture
After looking at these 22 malpractice cases, we saw that 5 of the doctors were orthopaedic surgeons, 5 were neurosurgeons, 6 were emergency medicine specialists and 6 were radiologists. Of the 5 cases in which the orthopaedic surgeon was found to have committed malpractice, 3 were treatment errors, one was a failure to diagnose, and one was a missed diagnosis. Of the 5 cases in which the neurosurgeon was found to have committed malpractice, 3 involved treatment errors, one involved a failure to diagnose, and one involved inappropriate management after surgery.
Discussion
Spinal surgery carries a significant inherent risk of litigation owing to the conditions being treated, the need for instrumentation often positioned near vital neurovascular systems, and the fragile nature of the spinal cord and nerve roots. Evidence shows that neurosurgery, particularly spinal neurosurgery, is among the specialties with the highest risk of malpractice lawsuits. Jena et al reported that, from 1991 to 2005, 7.4% of the 40 916 physicians had been subject to madical malpractice litigation, according to data from. 10 Lumbar spinal stenosis is the leading cause of malpractice in spinal surgery. Tumor surgery, cervical spondylosis, vertebral fracture, and scoliosis kyphosis follow in terms of frequency. 11 In our study, twenty-two of 65 spinal fracture cases involved more than 1 physician as a defendant, for a total of 84 defendants. Neurosurgeons were the first in 41 of 88 (46.5%), followed by emergency physicians (27.2%; 24 of 88 defendants), orthopedic surgeons (17%; 15 of 88 defendants), and radiologists (9%; 8 of 88 defendants). A total of 22 malpractice cases were reviewed, including those of 5 orthopaedic surgeons, 5 neurosurgeons, 6 emergency medicine specialists, and 6 radiologists. Of the 5 cases in which the orthopaedic surgeon was found to have committed malpractice, 3 were treatment errors, one was a failure to diagnose, and one was a missed diagnosis. Of the 5 cases in which the neurosurgeon was found to have committed malpractice, 3 involved treatment errors, one involved a failure to diagnose, and one involved inappropriate management after surgery.
Spinal surgeries are performed by 2 medical specialties: neurosurgery and orthopedics. This phenomenon has been thoroughly examined in a series of studies on spinal surgery malpractice. 11 Hu et al. evaluated malpractice cases in spinal surgeries between 2013 and 2018. 11 The most prevalent diagnoses in this study were lumbar spinal stenosis (28%), deformity (12.5%), cervical spondylosis (17%), spinal tumor (18%), and vertebral fractures (14%). A total of 13 of the 64 cases in this analysis were devoid of medical errors, resulting in no compensation. In the present study, 45 (70.3 %) patients were orthopedic, 11 (17.2%) were neurosurgical, and 8 (12.5%) could not be identified. In a study by Park et al., 257 cases were examined to ascertain the outcomes of medical malpractice following spine surgery. 12 A total of 257 cases were reviewed, resulting in 114 lawsuits against orthopedic surgeons and 122 lawsuits against neurosurgeons. The analysis revealed that 90 lawsuits against orthopedists and 79 lawsuits against neurosurgeons were decided in favor of the defendants. In a study conducted by Makhnini et al., spinal malpractice was evaluated; out of 103 spine cases, complaints were made to orthopedic surgeons in 49 cases, neurosurgeons in 42 cases, and surgeons of unknown primary in 12 cases. 13 They found that neurosurgery and orthopedic surgery were unrelated to the outcomes of the case. However, it has been reported that plaintiff compensation is significantly higher in cases of orthopedic surgery. n the present study, 65 cases of spinal fracture were examined, with more than 1 physician being named as a defendant in each instance, bringing the total number of defendants to 88. Neurosurgeons were the primary practitioners in 41 of the 88 cases (47%), followed by emergency physicians (27.2%; 24 of 88 defendants), orthopedic surgeons (17%; 15 of 88 defendants), and radiologists (9%; 8 of 88 defendants). However, 5 out of 15 orthopaedic surgeons, 5 out of 41 neurosurgeons, 6 out of 24 emergency medicine specialists, and 6 out of 8 radiologists were found to be at fault in malpractice lawsuits.
The most common reasons for malpractice claims in spine cases have been documented as inadequate informed consent, inappropriate surgical approach/level, incorrect level, delayed diagnosis and treatment, delays in receiving care, failure to use intraoperative neuromonitoring, inappropriate postoperative management, hardware malfunction, cervical plate malfunction, intraoperative error, and implant misuse.14-18 Iqbal et al. published a Systematic Review and Meta-Analysis of 15 retrospective studies covering the years 2002-2023 that examined more than 7890 malpractice claims related to spinal surgery. 14 In that systematic study, procedural errors accounted for 37.4% of the total number of complaints, followed by delayed diagnosis (32.1%) and treatment failure (28.8%). The prevalence of misdiagnosis or incorrect procedure choice (18.4%), death (17.3%), test interpretation (14.4%), improper patient referral for evaluation/treatment (14.3%), needless surgery (13.3%), and lack of informed consent (8.3%) were also significant. In a subsequent study, Epstein et al. conducted a comprehensive analysis of 17 articles on spinal surgery. 15 Their analysis aimed to identify the rationale underlying forensic cases related to spinal surgeries. As indicated by the findings of that study, the most prevalent etiologies of litigation subsequent to spinal surgery persist in the categories of failure to provide timely diagnosis or treatment, surgical negligence, and lack of informed consent. 16 Rae et al. conducted a comprehensive review of malpractice cases involving orthopedic spine surgeons over a 10-year period. 17 The most prevalent patient grievances reported in that study, which encompassed 214 orthopedists, pertained to availability and accessibility (35%), followed by care and treatment (32%). The malpractice occurrence rate ranges from 0.06% to 0.65%. 18 In our study, 65 cases of spinal trauma were reviewed, resulting in 88 complaints being identified. The most prevalent complaint was treatment error, accounting for 28.4% of cases. This was followed by a failure to diagnose and postoperative paralysis. In 22 malpractice cases, there were 12 cases of failure of diagnosis, 3 cases of misdiagnosis, 6 cases of treatment error, and 1 case of inappropriate postoperative management.
This study had some limitations that should be considered. The most important limitation is that the database used for our data did not contain the results of the cases and their judgments. Therefore, physician opinions (whether there was malpractice) were examined in this study. As radiographs were not evaluated in all cases, the decision regarding conservative or surgical treatment could not be evaluated. The study did not report the academic titles or years of experience of the physicians, which could have influenced treatment or even litigation. Due to the lack of sufficient data in the case files, social conditions such as smoking and additional patients were not included in the study.
Conclusion
This study examined medical malpractice lawsuits following spinal fracture treatment by reviewing 65 closed cases between 2018 and 2023. The study found that 22 out of 65 cases were malpractice by the committee. The most common complaints were treatment errors (28.4%), failure to diagnose the condition, and postoperative paralysis. Three of the 22 cases with malpractice were treated by orthopedic surgeons, while 19 were treated by neurosurgeons (P = 0.758). However, 5 out of 15 orthopaedic surgeons, 5 out of 41 neurosurgeons, 6 out of 24 emergency medicine specialists, and 6 out of 8 radiologists were found to be at fault in malpractice lawsuits. The utilization of artificial intelligence has the potential to contribute to a reduction in malpractice cases in the domain of accurate diagnosis, particularly in the context of radiology.
Footnotes
Ethical Consideration
This study was approved by Forensic Medicine Institution Scientific Board (IRB no: 2024/141 and 30.04.2024).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Code Availability
The code that support the findings of this study are available on request from the corresponding author.