
Abstract
Study design
Retrospective cohort study.
Objective
To compare the incidence of adjacent segmental pathology (ASP) following minimally invasive (MI) vs open transforaminal lumbar interbody fusion (TLIF) and to identify factors linked to ASP requiring reoperation.
Methods
This retrospective study reviewed the outcomes of patients who underwent MI-TLIF or open TLIF. Radiographic ASP (RASP) was evaluated using X-ray imaging to distinguish between degenerative changes, spondylolisthesis, and instability in the adjacent spinal segment. Clinical ASP (CASP) was assessed with the visual analog scale score for leg and back pain and the Oswestry disability index. Patient data were collected 1, 2, 5, and 10 years postoperatively. The timing and frequency of ASP reoperation were analyzed.
Results
Five years postoperatively, the RASP rate was 35.23% and 45.95% in the MI-TLIF and open TLIF groups. The frequency of CASP differed significantly between the MI-TLIF and open TLIF groups at 1 year postoperatively. The rates of RASP, CASP, and ASP necessitating reoperation were not significantly different 10 years postoperatively. Cranial facet violation significantly affected ASP in both groups. In the open TLIF group, preoperative adjacent segment disc degeneration significantly influenced ASP.
Conclusion
The RASP rate at 5 years postoperatively and the CASP rate at 1 year postoperatively differed significantly between groups. There was no difference in the rate of ASP requiring reoperation. Cranial facet violation is a crucial driving factor for ASP after both surgical procedures.
Keywords
Introduction
Adjacent segment pathology (ASP) is a significant contributing factor to reoperation following lumbar spine procedures. 1 Significant research has been conducted to identify the risk factors associated with ASP. Various factors, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) status, smoking, treatment level, cranial facet violation, preoperative adjacent disc degeneration, and postoperative sagittal alignment, have been found to be associated with the occurrence of ASP after surgery.2-4 In order to reduce this risk, surgeons have continuously been refining their operative techniques.
Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) is designed to minimize nerve damage by avoiding extensive soft tissue dissection and neural tissue retraction.5,6 This technique involves the use of a tubular retractor and unilateral facetectomy to achieve posterior nerve decompression and intervertebral arthrodesis. 7 Although controversial, 8 MI-TLIF is generally considered to offer several advantages to open TLIF, including reduced blood loss during surgery, faster postoperative rehabilitation, shorter hospital stay, and decreased perioperative pain, with similar outcomes.6,9-12 Studies comparing the 7-year and 10-year outcomes of MI-TLIF and open TLIF have consistently reported favorable results following MI-TLIF.10,13
In terms of ASP, several studies have compared MI-TLIF and open TLIF, and have reported comparable outcomes between the two procedures.14-16 A 7-year follow-up study found a lower incidence of radiologic ASP (RASP) and clinical ASP (CASP) with MI-TLIF, while the incidence of operative ASP was similar between the two approaches. 15 Furthermore, Lau et al. reported no difference in facet violation rates during pedicle screw placement between the two methods. 17 Overall, MI-TLIF has been shown to reduce the occurrence of ASP by minimizing surgical invasiveness and reducing damage to muscles and soft tissues, thereby reducing instability and the load on adjacent segments.
Considering these factors, we conducted the present study to analyze the 10-year incidence of each category of ASP in MI-TLIF compared to open TLIF, and to investigate the factors that influence the occurrence of ASP requiring reoperation after both approaches.
Materials and Methods
This study was approved by the appropriate Institutional Review Board (IRB no. 2021-11-002) of the National Health Insurance Service Ilsan Hospital. The need to obtain informed consent was waived due to the retrospective nature of the study.
Study Design
This retrospective cohort study analyzed 150 patients who underwent TLIF between March 2003 and December 2009. All operations were performed by the corresponding author, a senior orthopedic surgeon with over 10 years of surgical experience following completion of their fellowship. The study design and patient enrollment are shown in Figure 1. The inclusion criteria comprised an initial diagnosis of degenerative lumbar disease and spondylolisthesis, as well as age over 18. Patients who suffered a traumatic injury to the spine structure, had been diagnosed with malignancy on the spine structure, or had an autoimmune disease were excluded from the study. Subsequently, patients were divided in two groups, the MI-TLIF operation and the Open-TLIF group. In total, 62 patients in the MI-TLIF group and 32 patients in the open TLIF group who underwent consistent follow-up over a period of 10 years and were finally selected as the study subjects. Flowchart of the study. MI-TLIF: minimally invasive TLIF; TLIF: transforaminal lumbar interbody fusion.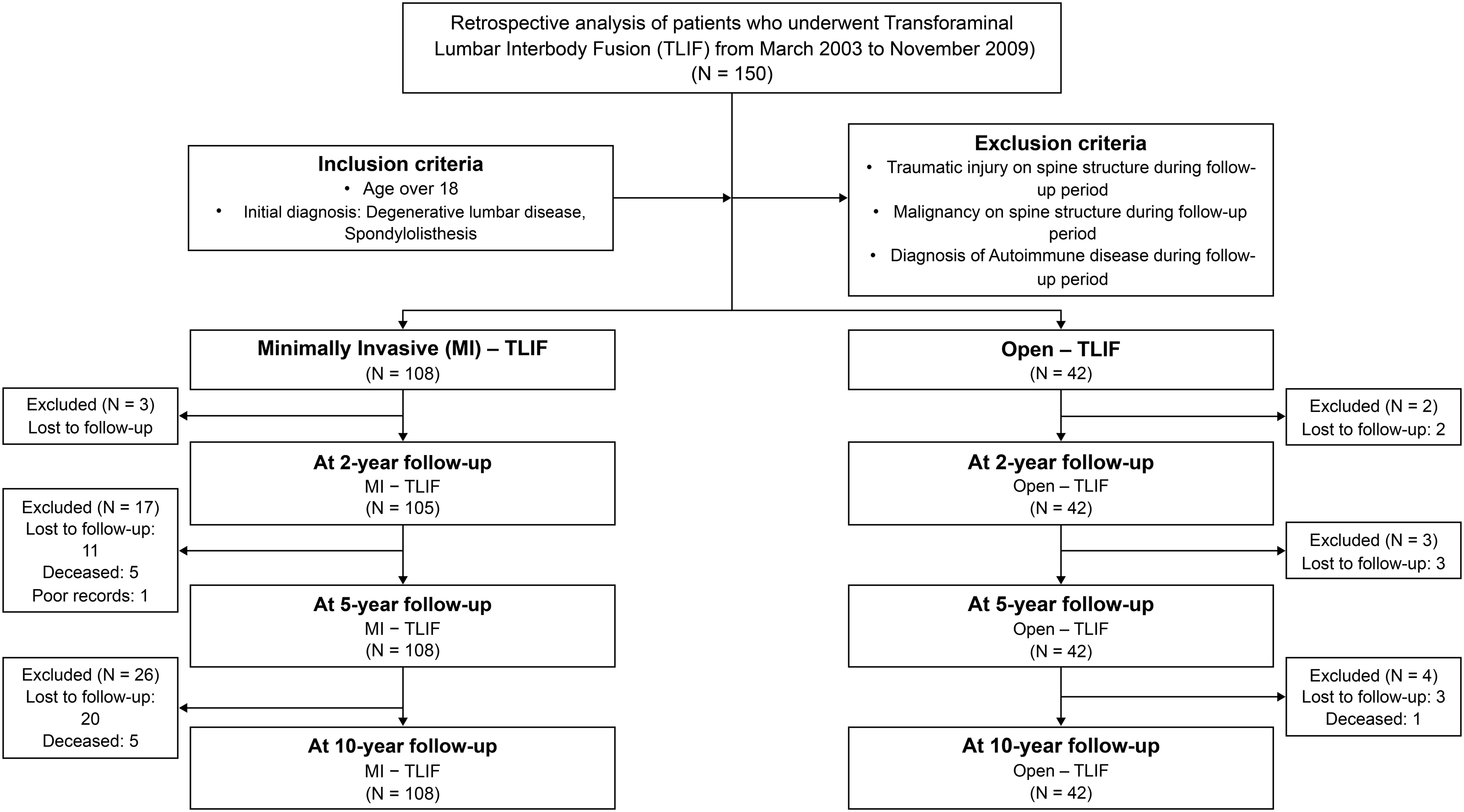
Surgical Indications and MI- TLIF Techniques
We typically prefer TLIF procedures for patients with degenerative lumbar pathologies, such as degenerative disc disease, spinal and foraminal stenosis, spondylolisthesis, and other forms of spondylotic disease. These patients show resistance to conservative management, and in our country, insurance assistance requires a minimum of 6 weeks conservative care. TLIF procedures can be performed using either an open or an MI technique, with no preference between the two methods. Open TLIF procedures have been extensively studied and documented in previous research, so in this section, we will focus on the MI-TLIF technique employed at our institution.
The spinal level of the planned surgical level was identified by intraoperative fluoroscopy, and a paramedian incision 1-2 inches in length was made. Subsequently, a tubular retractor with a diameter of 22 mm (METRxTM, Medtronic, Memphis, TN) was inserted. Ipsilateral laminectomy was initiated from the outer base of the spinous process and progressed upwards to the origin of the ligamentum flavum. Ipsilateral facetectomy was performed in an “L” shape, connecting vertically from the origin to the isthmus. This allowed for visualization of the ligamentum flavum lining beneath the lamina, which was subsequently removed. Percutaneously inserted screws and rods (Sextant, Medtronic, Memphis, TN) were utilized under fluoroscopic guidance on the contralateral side to achieve interbody space distraction. Following wide rectangular annulotomy, strict endplate preparation was conducted. Autologous bone obtained from the laminectomy was mixed with demineralized bone matrix (Osteofil1 RT DBM paste; Regeneration Technologies Inc., Alachua, FL) for grafting the intervertebral disc area. Subsequently, a polyetheretherketone (PEEK) cage (Capstone; Medtronic, Memphis, TN) was placed into the disc space under fluoroscopic guidance. Once successfully inserted, the tubular retractor utilized for decompression was removed, and the percutaneous pedicle screws and rods were applied to the ipsilateral side.
Primary Outcome Measurements
Adjacent segmental pathology (ASP) is commonly defined as a spinal degenerative pathology that commonly occurs following a previous spinal reconstructive procedure. However, the definitive criteria for diagnosing ASP remain unclear, as previous research studies have used inconsistent terms and criteria. 16 In the present study, we reviewed previous literature on the terminology and criteria used to define ASP. As a result, we divided ASP into three distinct categories: Radiologic ASP (RASP), clinical ASP (CASP), and ASP necessitating reoperation. 19
Radiologic ASP (RASP) was defined using standing lumbosacral anterior-posterior (AP) and lateral plain radiographs based on the following criteria, adopted from the study by Ghiseli et al. 1 : (1) presence of instability, defined as angulations of 10° or greater based on flexion/extension lateral radiographs; (2) listhesis greater than 4 mm, characterized by anterior, posterior, or lateral translation on anteroposterior and lateral radiographs; and (3) an increase in disc degeneration to grade 2, based on the University of California at Los Angeles grading scale. 20
Clinical ASP (CASP) is generally assessed based on the occurrence of newly developed back and leg pain. However, the definition of CASP is highly unclear, and there is a lack of consensus on the criteria used in the existing literature. In order to address this issue, we conducted a comprehensive review of multiple studies. Among them, Ramirez-Villaescusa et al. reported risk factors of CASP based on strict criteria, 21 including the reappearance of symptoms with a visual analog scale (VAS) score of at least 3 points in either lumbar or radicular pain, and/or changes in Oswestry disability index (ODI) indicating moderate or severe disability, with an increase of at least 15 points during follow-up. We decided to adopt these criteria as they provide a more precise and standardized approach to assessing CASP.
The indications for reoperation for ASP include confirmation of CASP with RASP, as well as resistance to conservative management over a period of 6 weeks. The main disease patterns observed in ASP were similar to those identified during the initial operation, as mentioned in the section on “Surgical Indications and MI-TLIF Technique.” These patterns include degenerative disc disease, spinal and foraminal stenosis, and spondylolisthesis. These criteria were also in line with previous studies.1,18
Assessment of Risk Factors
We conducted an evaluation of risk factors of ASP necessitating reoperation in 10 years. Demographic data, including the follow-up period, BMI, ASA status, smoking status, and the number of fusion segments, were reviewed. Additionally, sagittal parameters were assessed using standing lumbosacral AP and lateral plain radiographs. Furthermore, cranial facet violation, also known as superior facet violation, was also assessed using postoperative computed tomography (CT). Violation of the facet joint was defined according to the study of Moshirfar et al, 22 as a pedicle screw, head, connector, or rod located within 1 mm of the facet joint or abutting the facet joint. In addition, preoperative adjacent segment disc degeneration was assessed as a risk factor, with confirmation based on magnetic resonance imaging (MRI) findings of degenerative disc changes classified as Pfirmann grade III or IV.
All recorded data were obtained from the electronic medical record (EMR) of our institution, and radiologic data were collected from the Picture Archiving and Communication System (PACS) of our institution.
Statistical Analyses
To evaluate the statistical differences in continuous variables between subgroups, we initially conducted the Shapiro–Wilk and Kolmogorov–Smirnov tests to determine normality. Unpaired t-tests were performed for variables with a normal distribution, and Mann–Whitney U-tests were used for non-normally distributed variables. For categorical or non-continuous variables, a chi-squared test was conducted. Univariate logistic regression and multivariate logistic regression analyses were performed to investigate the risk factors associated with reoperation at the adjacent segment of the fusion level. Radiographic measurements and evaluations were initially performed by the first author as an independent observer, and subsequently reviewed and confirmed by another surgeon. Statistical significance was set at a two-tailed P-value < .05. All statistical analyses were performed using the SAS statistical software (version 9.4; SAS Inc., Cary, NC, USA).
Results
Demographic Factors
General Demographic and Surgical Data of the MI-TLIF and Open-TLIF Groups.
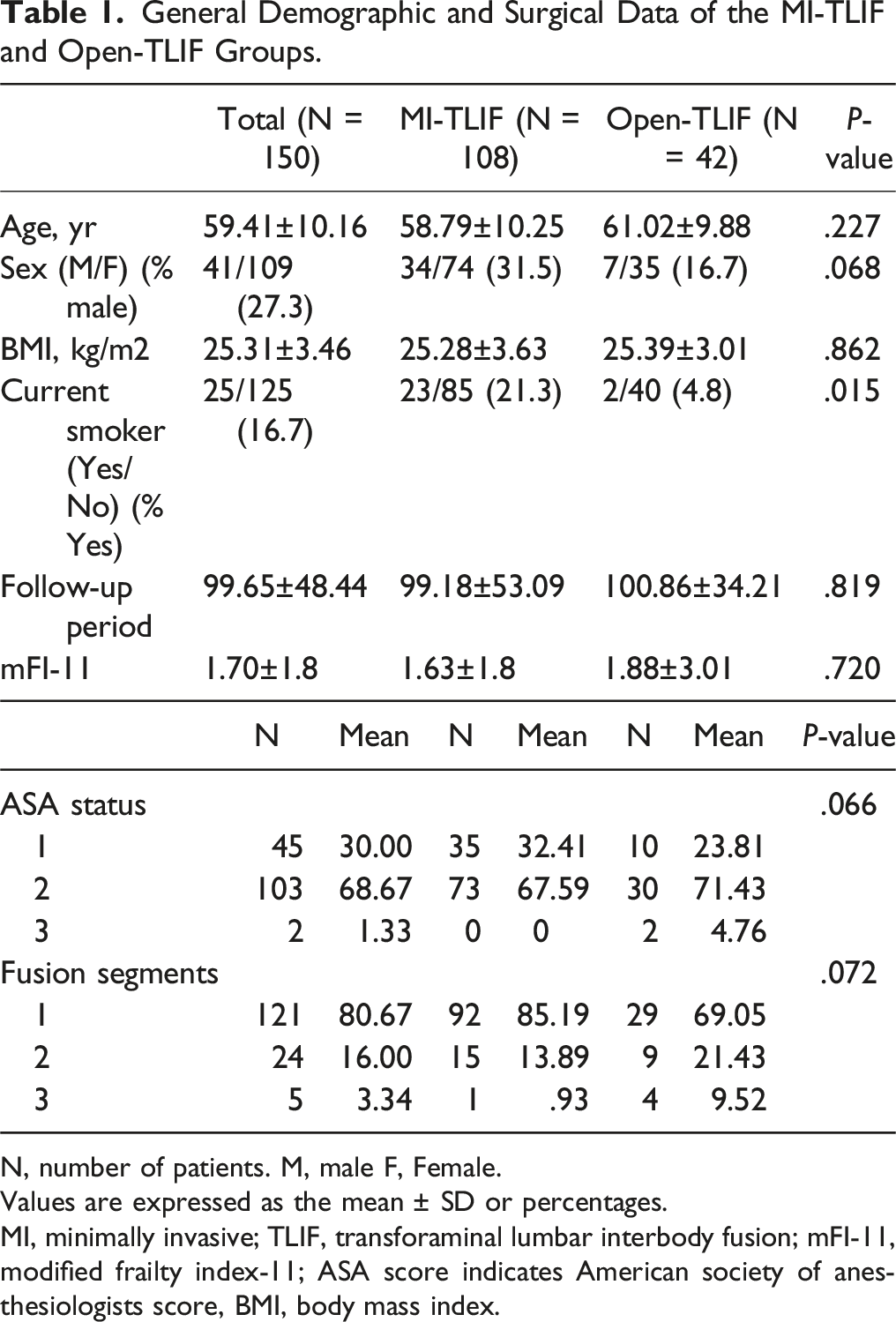
N, number of patients. M, male F, Female.
Values are expressed as the mean ± SD or percentages.
MI, minimally invasive; TLIF, transforaminal lumbar interbody fusion; mFI-11, modified frailty index-11; ASA score indicates American society of anesthesiologists score, BMI, body mass index.
Incidence of ASP following Operation
Until the 5-year follow-up, there was a difference in the frequency of RASP between the two surgery groups; however, this difference had disappeared by the 10-year follow-up. The RASP rate 1 year postoperatively was 6.6% in the MI-TLIF group and 16.7% in the open TLIF group (P = .061). Two years postoperatively, the RASP rate was 13.33% in the MI-TLIF group and 23.08% in the open TLIF group (P = .053). Five years postoperatively, the RASP rate was 35.23% in the MI-TLIF group and 45.95% in the open TLIF group (P = .024). Ten years postoperatively, the RASP rate was 58.06% in the MI-TLIF group and 60.61% in the open TLIF group (P = .132). Based on the 10-year follow-up data, the most common type of RASP in the MI-TLIF group was instability, accounting for 35.48% of the cases, followed by spondylolisthesis (12.9%) and degeneration (9.68%). Conversely, in the open TLIF group, degeneration was the most common (24.24%), followed by spondylolisthesis and instability (both 18.18%) (Figure 2). Radiographic adjacent segmental pathology distribution over 10 years. ASP: adjacent segmental pathology; MI-TLIF: minimally invasive TLIF; TLIF: transforaminal lumbar interbody fusion.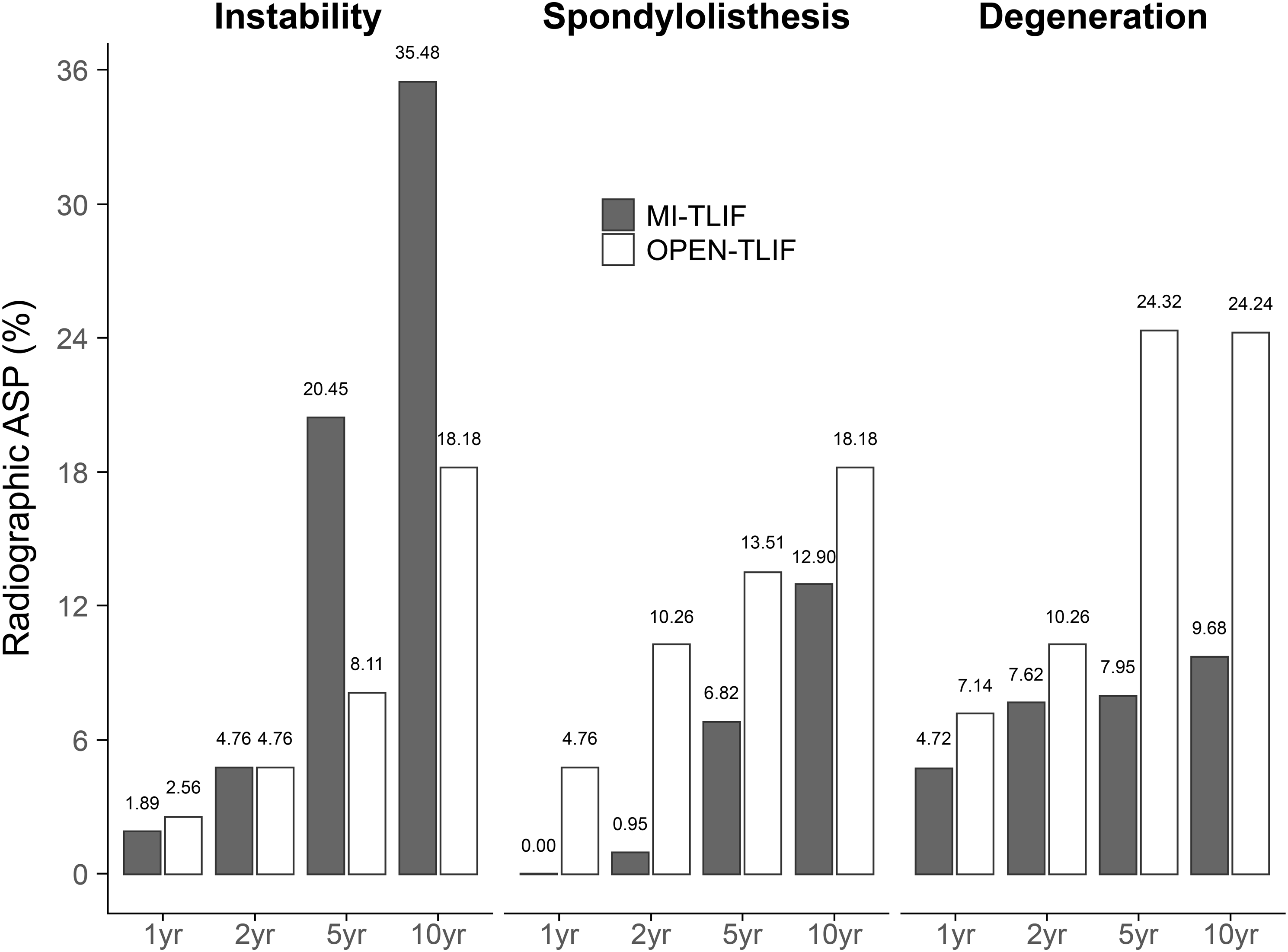
Our results revealed a significant difference in the frequency of CASP between the MI-TLIF and open TLIF groups 1-year post-surgery, with rates of 12.26% and 28.57%, respectively (P = .039). However, 2 years post-surgery, this difference was not significant, with rates of 23.81% for the MI-TLIF group and 35.9% for the open TLIF group (P = .149). At 5 years post-surgery, the rates were 42.22% for the MI-TLIF group and 54.05% for the open TLIF group (P = .227), and at 10 years post-surgery, the rates were 60.66% for the MI-TLIF group and 78.79% for the open TLIF group (P = .076). Back pain was the most common type of CASP in both groups, with rates of 42.62% for the MI-TLIF group and 60.61% for the open TLIF group 10 years post-surgery (Figure 3). Clinical adjacent segmental pathology distribution over 10 years. ASP: adjacent segmental pathology; MI-TLIF: minimally invasive TLIF; TLIF: transforaminal lumbar interbody fusion.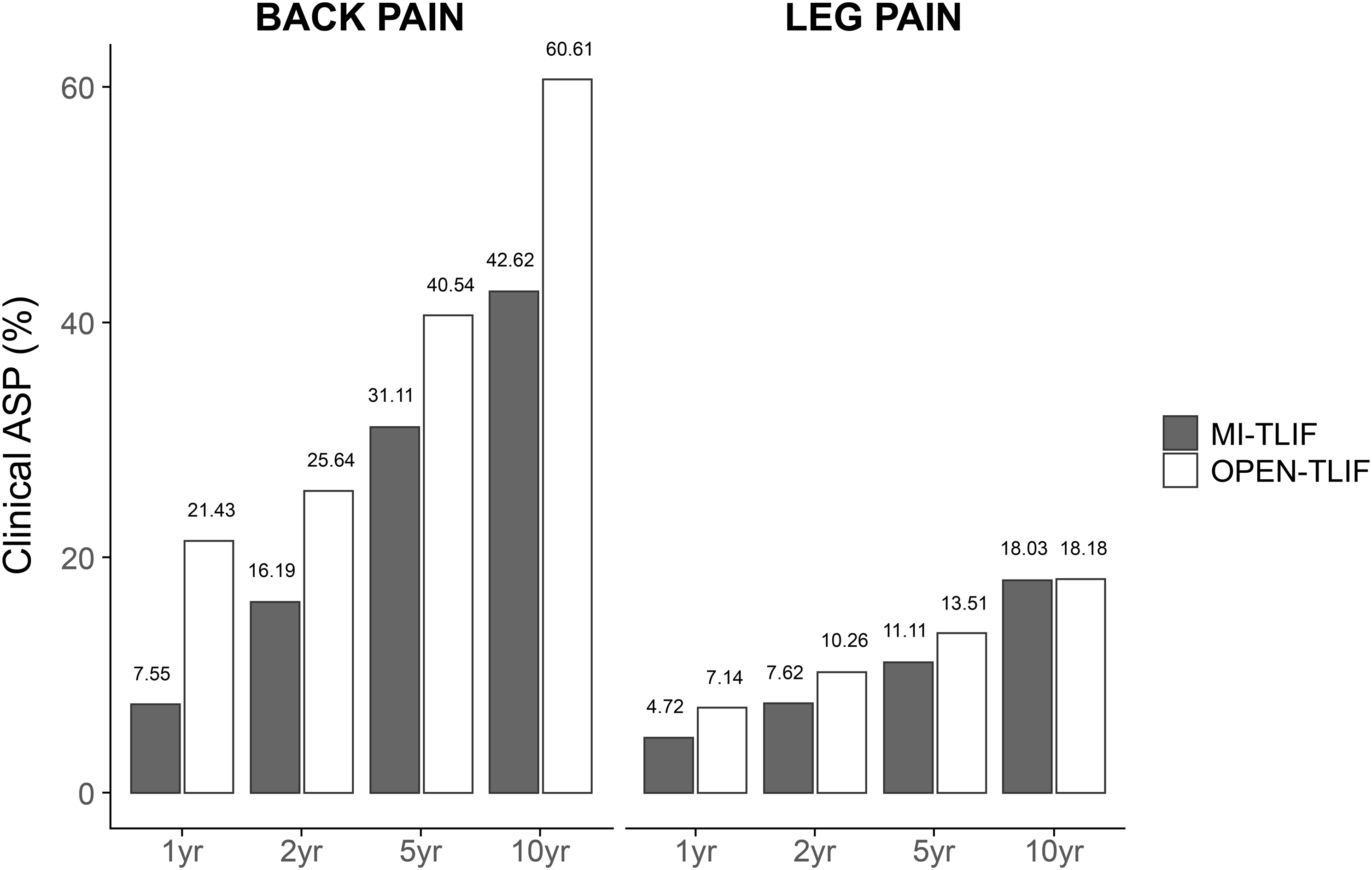
According to this study, 14 (12.96%) patients in the MI-TLIF group and 9 (21.42%) in the open TLIF group underwent reoperation because of ASP within 10 years after surgery. However, the difference between the two groups was not statistically significant (P = .072) (Figure 4). Reoperation rate over 10-year follow-up for each surgery type. ASP: adjacent segmental pathology; MI-TLIF: minimally invasive TLIF; TLIF: transforaminal lumbar interbody fusion.
Influencing Factors of ASP Requiring Reoperation
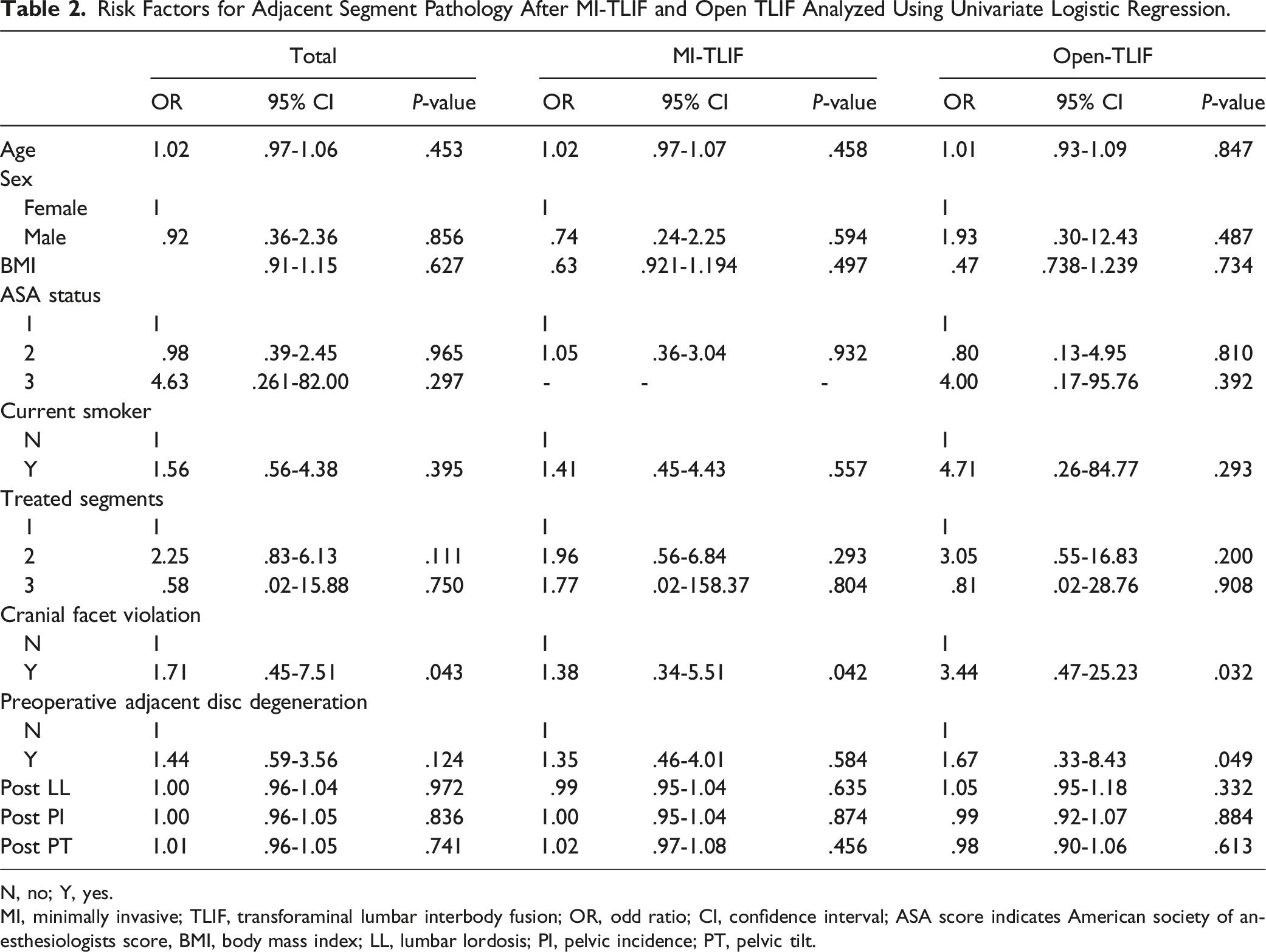
Risk Factors for Adjacent Segment Pathology After MI-TLIF and Open TLIF Analyzed Using Univariate Logistic Regression.
N, no; Y, yes.
MI, minimally invasive; TLIF, transforaminal lumbar interbody fusion; OR, odd ratio; CI, confidence interval; ASA score indicates American society of anesthesiologists score, BMI, body mass index; LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt.
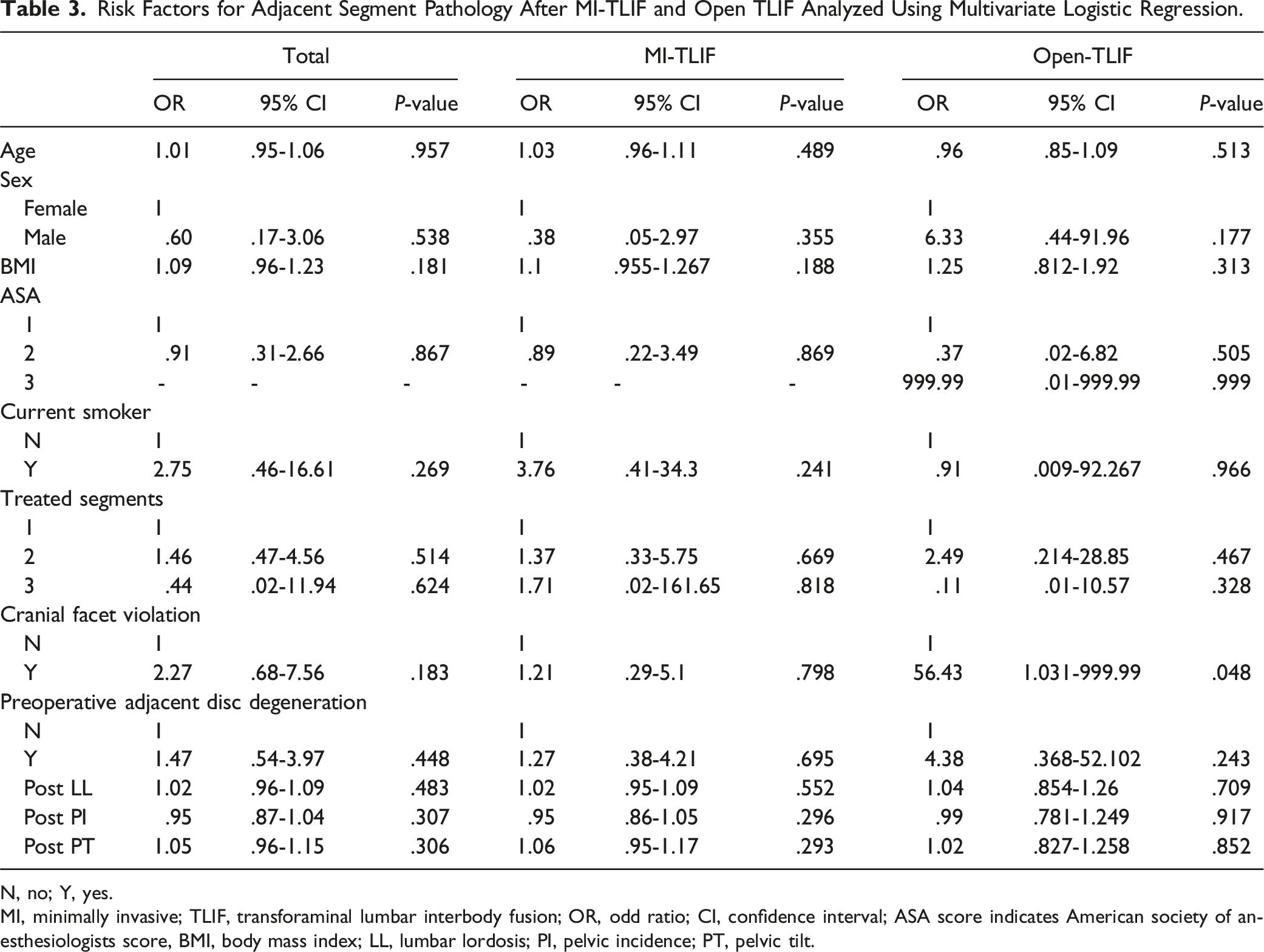
Risk Factors for Adjacent Segment Pathology After MI-TLIF and Open TLIF Analyzed Using Multivariate Logistic Regression.
N, no; Y, yes.
MI, minimally invasive; TLIF, transforaminal lumbar interbody fusion; OR, odd ratio; CI, confidence interval; ASA score indicates American society of anesthesiologists score, BMI, body mass index; LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt.
Discussion
With advancements in surgical techniques, minimally invasive techniques have become more popular, and MI-TLIF has emerged as one of the major fusion procedures. This is primarily due to its several advantages, including an associated reduction in tissue and paravertebral musculature damage, minimization of the risk of infection and blood loss, and ultimately shorter hospital stays and faster recovery time, enabling patients to resume their daily activities sooner.5-7 Moreover, studies have indicated that there is no significant difference in terms of fusion rate or clinical outcome between MI-TLIF and open TLIF procedures.9,10,13 Additionally, research on the rate of ASP following MI-TLIF has reported favorable outcomes.14-16
In the present study, we found a statistical difference between two groups in the rate of RASP at 5 years, but no difference was observed at the 10-year follow-up. However, the pattern of RASP differed between the two groups. The main pattern of RASP observed in patients who underwent MI-TLIF was instability, while the main pattern in patients who underwent open TLIF was degeneration. Regarding CASP, we observed a significant difference in the frequency of CASP between the MI-TLIF and open TLIF groups at 1-year post-surgery. However, no difference was found at 10-year follow-up. Both surgical groups showed a higher frequency of back pain than leg radiculopathy, believed to be related to various types of RASP. Additionally, the rate of adjacent segment pathology requiring reoperation showed no difference between the two procedures. The prime finding of this study was that although the RASP rates up to a 5-year follow-up were lower for the MI-TLIF group compared to the open TLIF group, there were no differences in the CASP rates between the two surgical groups after the first year postoperation. Similarly, the revision surgery rates did not differ between the groups. These results are consistent with previous studies. A 5-year study by Jia et al. also reported a difference in RASP at 5 years, but no difference in clinical outcomes. 16 Similarly, a 7-year study by Hong et al. reported a difference in RASP rate at 7 years, but no difference in reoperation rate. 15 The discrepancy observed in the occurrence of RASP, CASP, and reoperation rate has been previously discussed in the context of general fusion surgery 23 and posterolateral fusion procedures. 24 It can be inferred that the rate of RASP may be lower after MI-TLIF due to the maintenance of the posterior complex 25 and the lower degree of damage to the paravertebral muscles.5,7 However, further research is needed to fully understand this discrepancy.
We conducted a further analysis to determine whether certain factors had an impact on ASP requiring reoperation. Our findings revealed that cranial facet violation in the MI-TLIF group and both cranial facet violation and preoperative adjacent disc degeneration in the open TLIF group were significant factors in univariate logistic regression analysis. These results align with those of previous studies that have identified various risk factors associated with ASP.2,3 Regarding the effects of preoperative adjacent disc degeneration as a risk factor, this is likely due to the degenerated discs having to endure postoperative compensatory hypermobility adjacent to the fused construct, 26 without the support provided by the posterior complex or paravertebral musculature in open TLIF. Additionally, cranial facet violation directly reduces stability, leading to a higher rate of reoperation.
It is crucial to acknowledge the limitations of this study when interpreting the results. Firstly, the sample size was relatively small due to the high number of participants lost to follow-up, which may have limited the statistical significance of the findings. Secondly, the study design was retrospective, which inherently carries limitations and potential bias. Thirdly, there was a risk of selection bias as the sample was derived from a single surgeon at a single medical center, limiting the generalizability of the results to the wider population. However, despite these limitations, we believe that there is significance in analyzing the form of ASP over a prolonged follow-up period of 10 years.
Conclusion
Overall, we identified a statistically significant difference between the MI-TLIF group and the open TLIF group in terms of the RASP rate in the postoperative 5 years and CASP in the first postoperative year. However, no such difference was found at the 10-year follow-up. Additionally, there was no difference in the rate of ASP requiring reoperation between the two groups. Further, we identified cranial facet violation ASP requiring reoperation in both groups and preoperative adjacent disc degeneration in the open-TLIF group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.