
Abstract
Study design
Systematic review and meta-analysis.
Objective
This systematic review with meta-analysis is aimed at evaluating the impact of smoking (tobacco) on spinal fusion rates and the resulting PROMs.
Methods
Following the PRISMA guidelines, a systematic literature search was conducted in 4 databases. Studies focused on adult smokers vs non-smokers undergoing spinal fusion. Odds ratios (ORs) were calculated for dichotomous variables and mean differences or standardized mean differences for continuous variables. The primary outcomes assessed were non-union/pseudoarthrosis incidence and PROMs.
Results
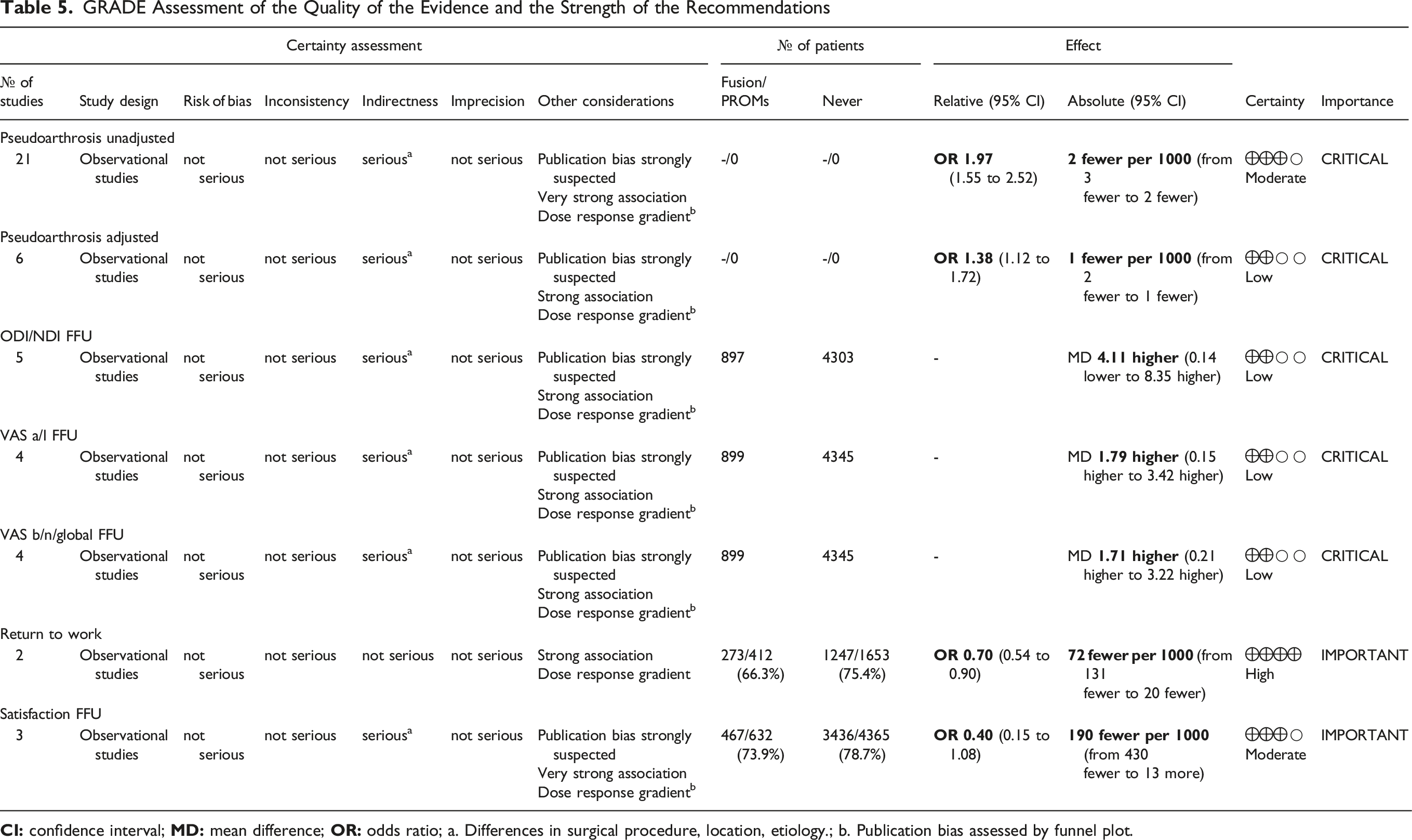
A total of 29 studies were included in this analysis. The unadjusted incidence of pseudoarthrosis was significantly higher in smokers than in non-smokers (OR 1.97, 95% CI 1.55-2.52, P < 0.001). Subgroup analysis revealed significant differences in the cervical (OR 2.09, 95% CI 1.27-3.44, P < 0.05) and lumbar (OR 1.97, 95% CI 1.45-2.68, P < 0.001) regions. Adjusted analysis also showed a significantly higher incidence of pseudoarthrosis in smokers (OR 1.38, 95% CI 1.12-1.72, P < 0.05). Changes in ODI, VAS, EQ-5D, and SF-12 and SF-36, consistently favored nonsmoking patients. Smoking was associated with a lower rate of returning to work (OR 0.70, 95% CI 0.54-0.90, P < 0.05), and in the lumbar subgroup, reduced satisfaction (OR 0.24, 95% CI 0.12-0.49, P < 0.001). Former smokers (smoking cessation for at least 1 year prior to surgery) did not show significant differences compared to nonsmokers in terms of pseudarthrosis rate or pain scores.
Conclusion
Smoking is associated with an increased risk of pseudarthrosis and poorer PROMs after spinal fusion surgery. Healthcare providers should emphasize smoking cessation interventions to improve surgical outcomes and patient satisfaction.
Introduction
Pseudoarthrosis is a common complication in spinal surgery, significantly impacting both patients and the healthcare system.1,2 Its incidence, especially at the cervical level, is approximately 2.6%. 3 A key contributor to this complication is smoking, which negatively affects graft success due to the vasoconstrictive effects of nicotine. 4 Studies in rabbits support this detrimental impact on spinal fusion. 5 Smoking also worsens patient-reported outcomes (PROMs),6,7 increasing the risk of complications and chronic pain after surgery.6,8 With 19.7% of American adults using tobacco in 2018, 9 understanding the full impact of smoking on surgical outcomes is vital. Evidence suggests that smoking interferes with spinal fusion and reduces patient satisfaction 10 and that smoking cessation improves surgical outcomes. 11 Current smokers tend to have worse outcomes than non-smokers, with a clinically significant difference in pain relief, 12 while former smokers fare better but still worse than non-smokers. 13 Despite associations with comorbidities, smoking independently raises surgical risks. 14 However, some studies, like that of Phan et al, report no differences in clinical outcomes. 15 Pseudoarthrosis and disability post-surgery also carry a considerable economic burden, 16 and the role of bone substitutes and osteobiologics is crucial. 17 Smoking is a modifiable risk factor, and previous systematic reviews indicate that cessation can improve surgical outcomes. 18 This meta-analysis aims to assess smoking’s impact on spinal fusion, specifically its effect on pseudoarthrosis and PROMs, to enhance patient care and outcomes.
Methods
Eligibility Criteria
This study had a written protocol with review questions, search strategy, inclusion/exclusion criteria, and risk of bias assessment (PROSPERO: CRD42023482226). The current study followed the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Figure 1).
19
Study Selection Flow Diagram (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)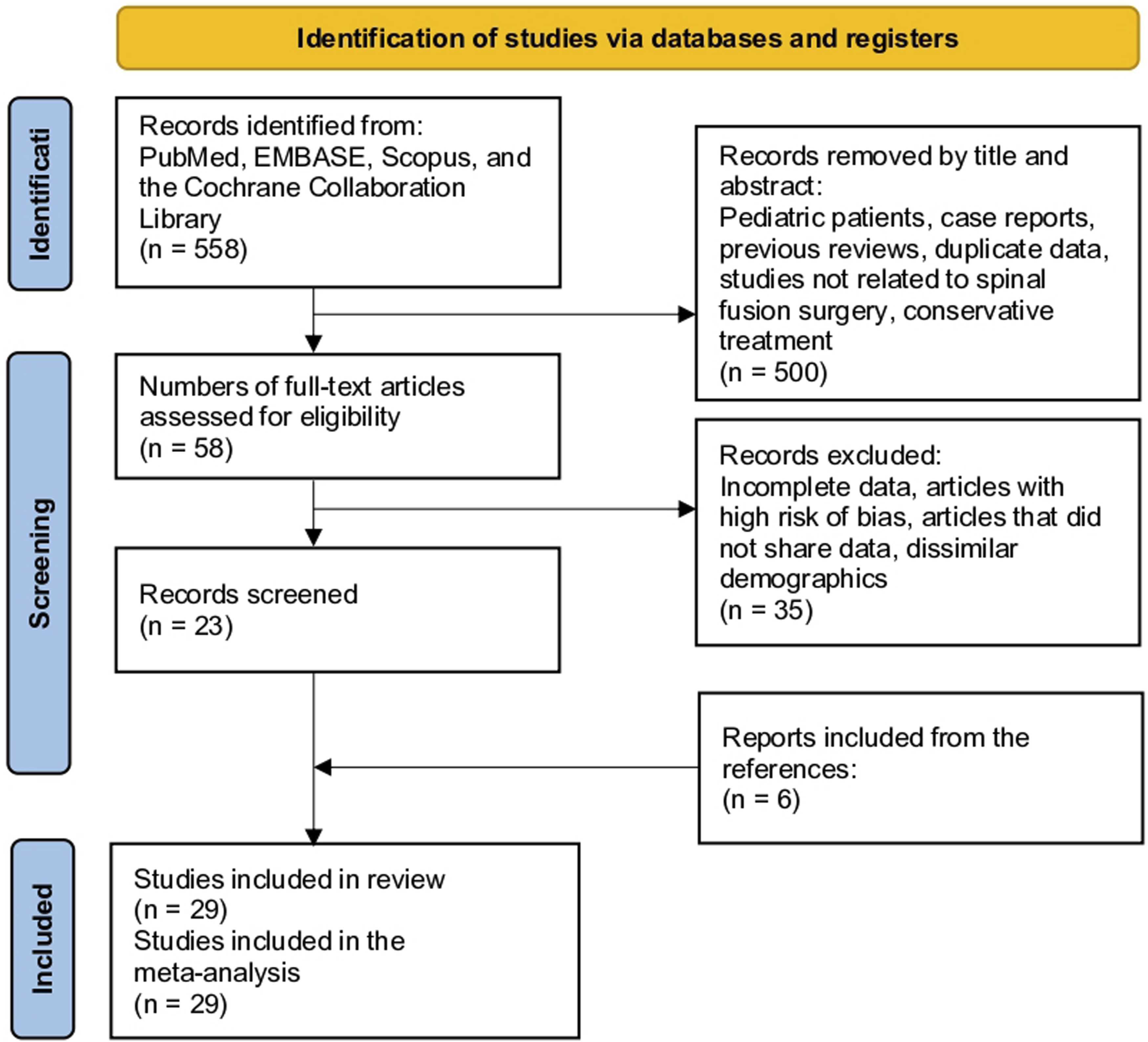
The systematic review question was structured following the Population, Intervention, Comparison, Outcomes, Study design (PICOS) strategy. The study population (P) included patients undergoing spinal fusion surgery. The intervention (I) evaluated the current smoker status. These patients were compared (C) with non-smoker controls who underwent the same surgical procedure. The primary outcomes (O) examined included radiographic evidence of pseudarthrosis or pseudarthrosis observed on follow-up imaging, as well as patient-reported outcome measures (PROMs) assessing pain, function, and quality of life. Only comparative study (S) designs were considered eligible for inclusion, as they are typically used to investigate the impact of exposures, such as smoking.
Articles were excluded if they involved pediatric populations, case reports, or previous literature reviews to ensure that only primary studies contributing to new comparative results were incorporated. Duplicate publications, presenting data from the same patient cohort, were also excluded to avoid overlapping analyses and skewing findings. Studies lacking sufficient reporting of methods, participant characteristics, or outcome data useful for appraising risk of bias, and informed meta-analyses, were excluded due to incomplete reporting. Papers that did not present quantitative outcome data in a format that could be compiled across studies, such as those that only provided qualitative results or narratives, were omitted. Investigations focused on non-surgical interventions, including conservative treatment modalities alone, rather than spinal fusion surgical procedures, were also excluded to maintain relevance to the examined population. Lastly, studies specifying that the included patient groups did not undergo spinal fusion techniques, were excluded to ensure comparability with the population of interest undergoing surgical treatment.
Information Sources
A comprehensive search of multiple databases was conducted to identify the relevant literature. This included PubMed, EMBASE, Scopus, and Cochrane Library. No date or language restrictions were applied to capture all eligible publications. The reference lists of the included articles were also screened to uncover any potentially missed studies that met the inclusion criteria.
Search Methods for Identification of Studies
We used the following search terms to search all trials registers and databases: (“Spinal Fusion” OR “fusion rate” OR “spine failure”) AND (smoking OR tobacco OR cigarette) NOT meta-analysis NOT “systematic review” NOT “case report” (Supplementary File 1). Two reviewers independently agreed on the selection of eligible studies and reached a consensus on which studies to include. Two authors independently reviewed the studies for data extraction. If consensus was not reached, a third author was asked to complete the data extraction form.
Data Extraction and Data Items
The baseline characteristics obtained from each study were as follows: study, period, follow-up, region, type of study, location, number of patients, number of female patients, age, surgical technique, etiologies, and method of assessing pseudarthrosis. The main outcomes that could be compared were the incidence of non-union or pseudoarthrosis, as well as patient-reported outcome measures: Visual Analog Scale (VAS), Oswestry Disability Index (ODI), EQ-5D, SF-12/36 physical component (PCS), SF-12/36 mental component (MCS), return to work rates, satisfaction, and the minimally clinically important difference (MCID). The data extraction process was independently conducted by two reviewers. Any discrepancies between the extracted data were identified and resolved through discussions between the two reviewers. If consensus could not be reached, a third reviewer was consulted to assess the discrepant data items and make a final determination to arrive at an agreement.
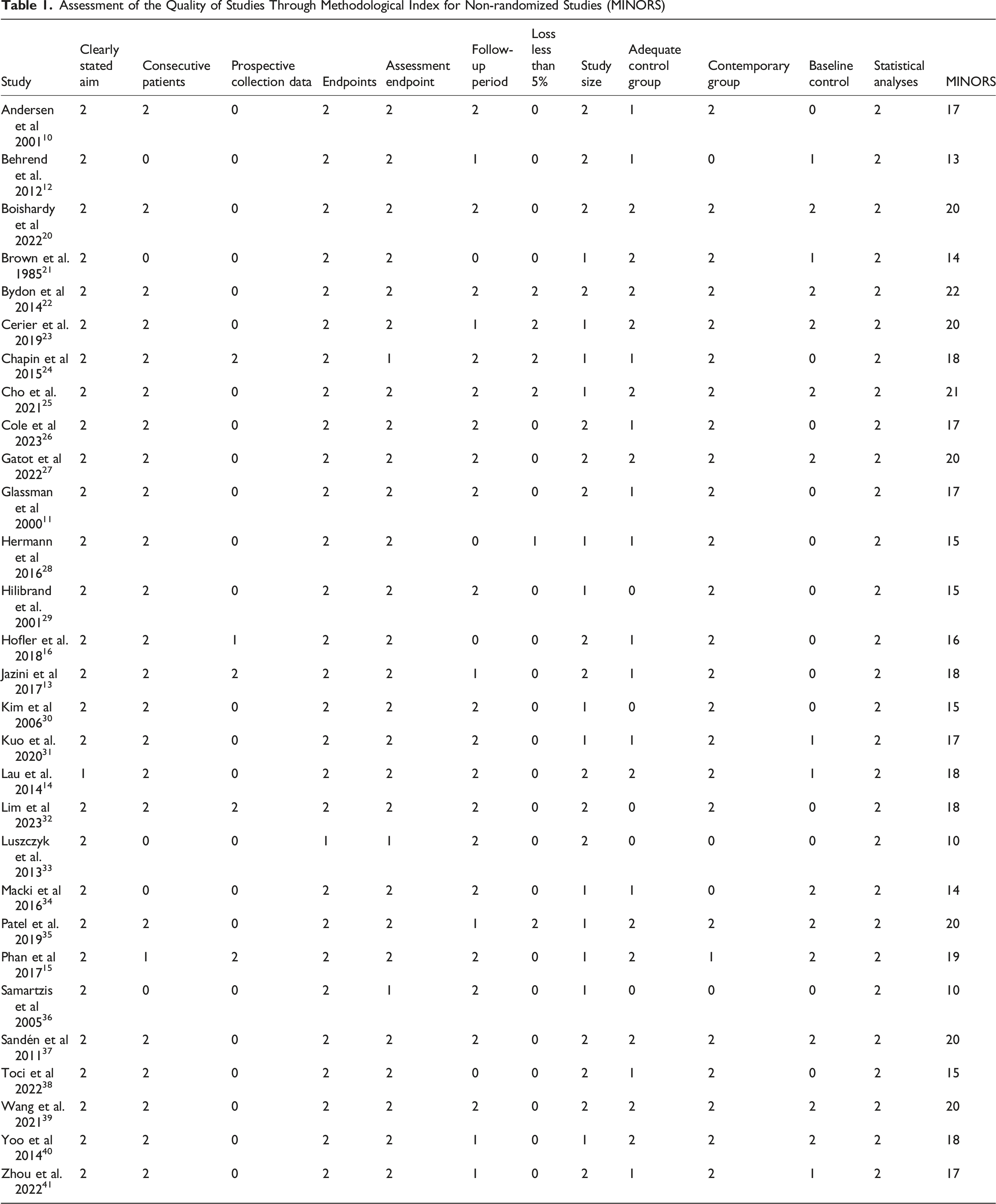
Assessment of Risk of Bias in Included Studies
Assessment of the Quality of Studies Through Methodological Index for Non-randomized Studies (MINORS)
Assessment of Results
The meta-analysis was conducted using the software Review Manager (RevMan, v5.4, Cochrane Collaboration). Odds ratios (OR) with 95% confidence intervals (CI) were calculated for dichotomous variables. Continuous variables were analyzed using mean differences (MD) with 95% confidence intervals (CI), except for variables that differed in scale or units, for which standard mean differences (SMD) with 95% CI were calculated. When individual studies presented risk factors as odds ratios, a generic inverse variance method was employed. To assess heterogeneity, both the chi-square test and I2 statistic were used. I2 values ranging from 0 to 100% were interpreted as indicative of low, moderate, and high heterogeneity at 25%, 50%, and 75% thresholds, respectively. In the absence of statistical evidence of heterogeneity, a fixed-effects model was used. A random-effects model was used when significant heterogeneity was detected. Whenever feasible, adjusted data derived from multivariate analyses were extracted to account for potential confounding variables. In cases where such information was not provided, unadjusted estimates from the univariate analyses were included in the meta-analysis. To extract precise information from figures within the articles, WebPlotDigitizer (version 4.5.0) was utilized. Missing data were managed according to the guidelines outlined in the Cochrane Handbook. 43
Risk of Bias Across the Studies
To evaluate the potential presence of publication bias, an assessment of small study effects was conducted through visual inspection of a funnel plot using RevMan, comparing each study’s effect size against its precision. A symmetrical distribution of points around the pooled estimate line would suggest a lack of bias, whereas asymmetry could indicate systematic non-publication of smaller trials with null or unfavorable results.
Additional Analyses
Subgroup analyses were conducted to explore sources of heterogeneity based on spinal region and smoking status classification. Information on smoking cessation, including its definition, timing relative to surgery, and potential impact on outcomes, was systematically collected from all included studies in which such data were available.
Sensitivity analyses, including a leave-one-out analysis using RevMan, were performed to assess the robustness of findings by iteratively removing the highest-weighted study from each meta-analysis.
In addition, Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology was employed to systematically assess the certainty of evidence for key outcomes. 44 This system rates evidence quality, with randomized trials considered high-quality but subject to downgrading for bias, inconsistency, or imprecision. Observational studies begin as low quality but may be upgraded based on large effects or minimal validity threats.
Results
Study Selection
A systematic search of PubMed, EMBASE, Scopus, and Cochrane Collaboration Library yielded 558 citations. After reviewing the titles and abstracts, 500 studies were excluded because they did not focus on smoking or were not comparative. The full texts of the remaining 58 citations were examined in detail; 35 studies did not meet the inclusion criteria, resulting in 23 studies. Six additional studies were identified by reviewing the references in the included articles. Ultimately, 29 studies were included in this meta-analysis (Figure 1).10–16,20–41
Study Characteristics
Baseline Characteristic of the 29 Included Studies
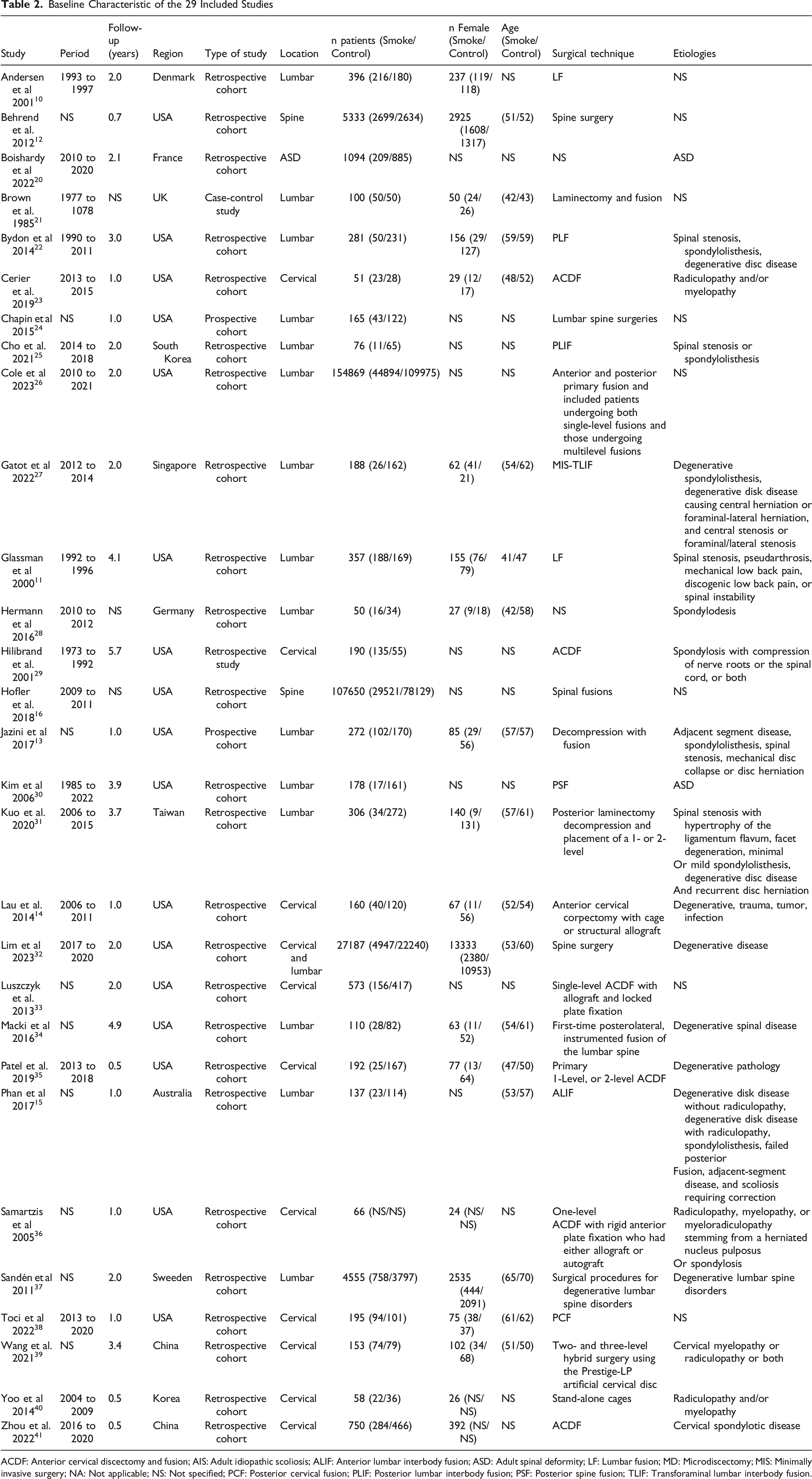
ACDF: Anterior cervical discectomy and fusion; AIS: Adult idiopathic scoliosis; ALIF: Anterior lumbar interbody fusion; ASD: Adult spinal deformity; LF: Lumbar fusion; MD: Microdiscectomy; MIS: Minimally invasive surgery; NA: Not applicable; NS: Not specified; PCF: Posterior cervical fusion; PLIF: Posterior lumbar interbody fusion; PSF: Posterior spine fusion; TLIF: Transforaminal lumbar interbody fusion.
Pseudoarthrosis
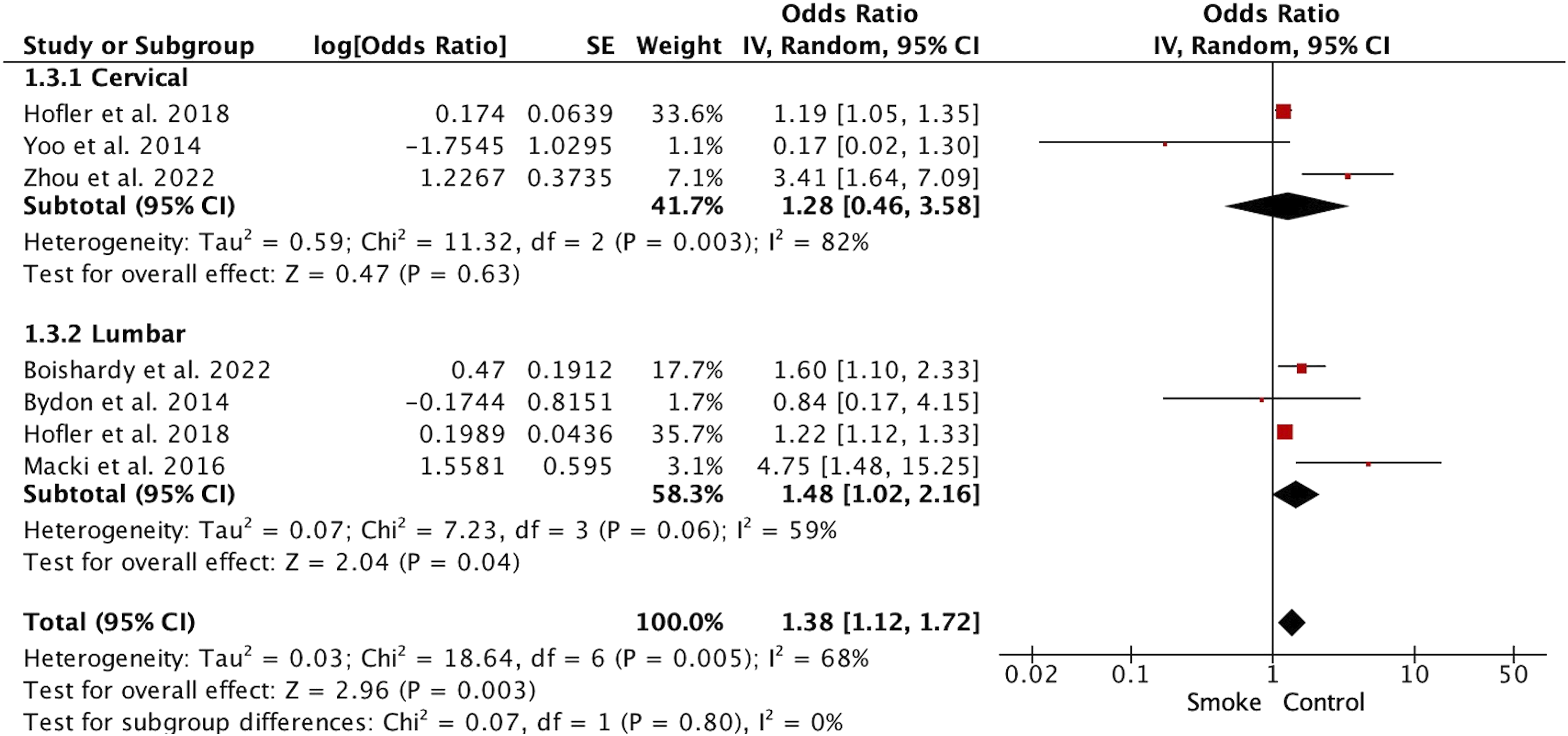
The unadjusted incidence of pseudarthrosis was significantly higher in the smoking group (OR1.97, 95%CI 1.55 to 2.52; studies = 22) (Figure 2). Significant differences were observed at the cervical (OR2.09, 95%CI 1.27 to 3.44; studies = 9) and lumbar (OR1.97, 95%CI 1.45 to 2.68; studies = 13) levels. When the adjusted incidence of pseudarthrosis was analyzed (considering comorbidities, demographics and type of surgery), smokers continued to show a significantly higher incidence (OR1.38, 95%CI 1.12 to 1.72; studies = 7) (Figure 3). When subgroup analyses were performed using the adjusted incidence at the cervical level, no significant differences were observed (OR1.28, 95%CI 0.46 to 3.58; studies = 3). In contrast, at the lumbar level, smokers had a higher frequency of adjusted incidence of pseudarthrosis (OR1.48, 95%CI 1.02 to 2.16; studies = 4). Forest Plot Showing Smoking Patients (Smoke) had Twice the Risk of Cervical and Lumbar Pseudarthrosis than Non-smoking Patients (Control) Forest Plot Showing Adjusted Risk of Pseudarthrosis. In Total, Smoking Patients (Smoke) Were Found to Have a Significantly Higher Risk than Non-smokers (Control) (OR 1.38, 95% CI 1.12 to 1.72, P < 0.01)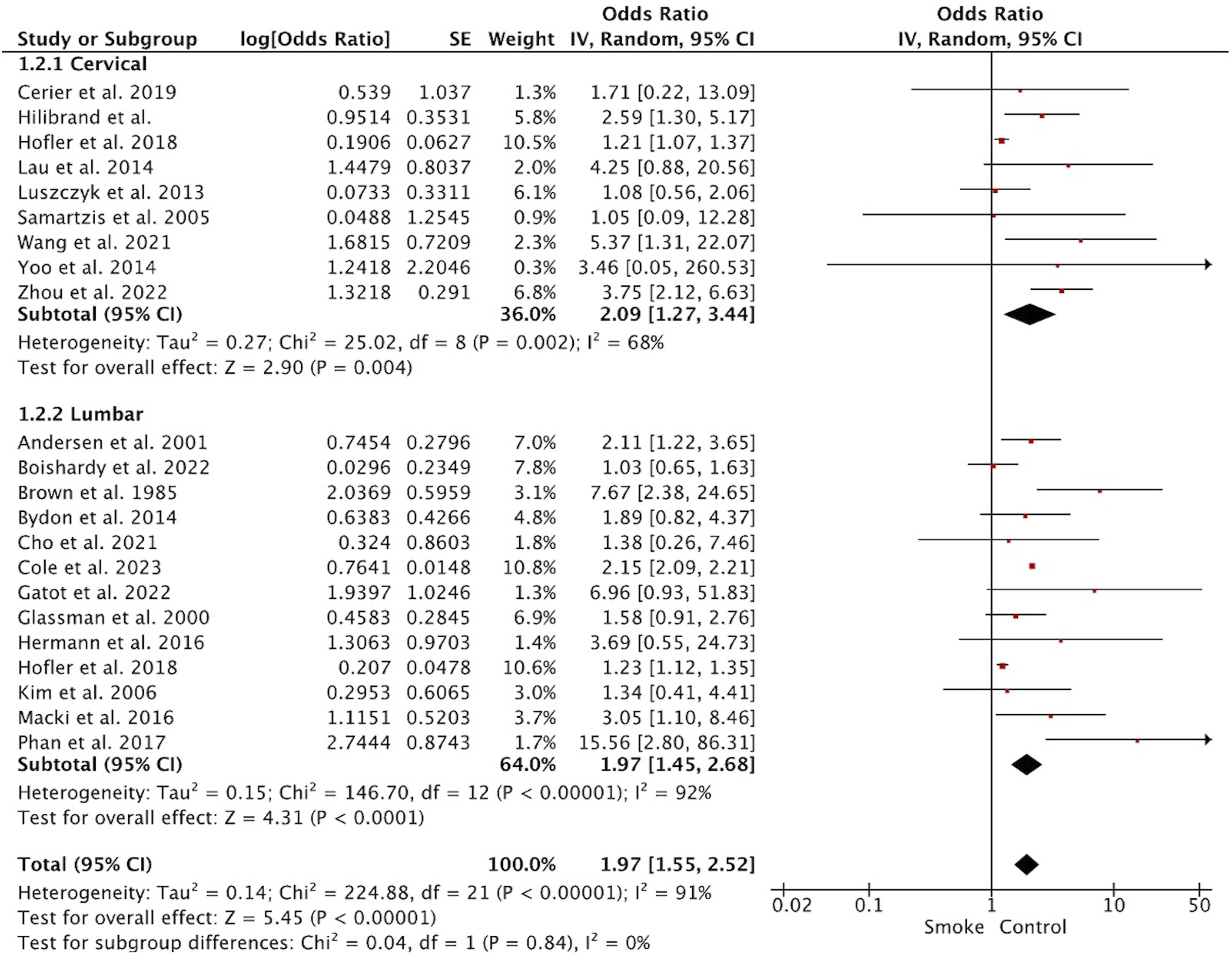
Patient Reported Outcome Measures
Patient-Reported Outcome Measures
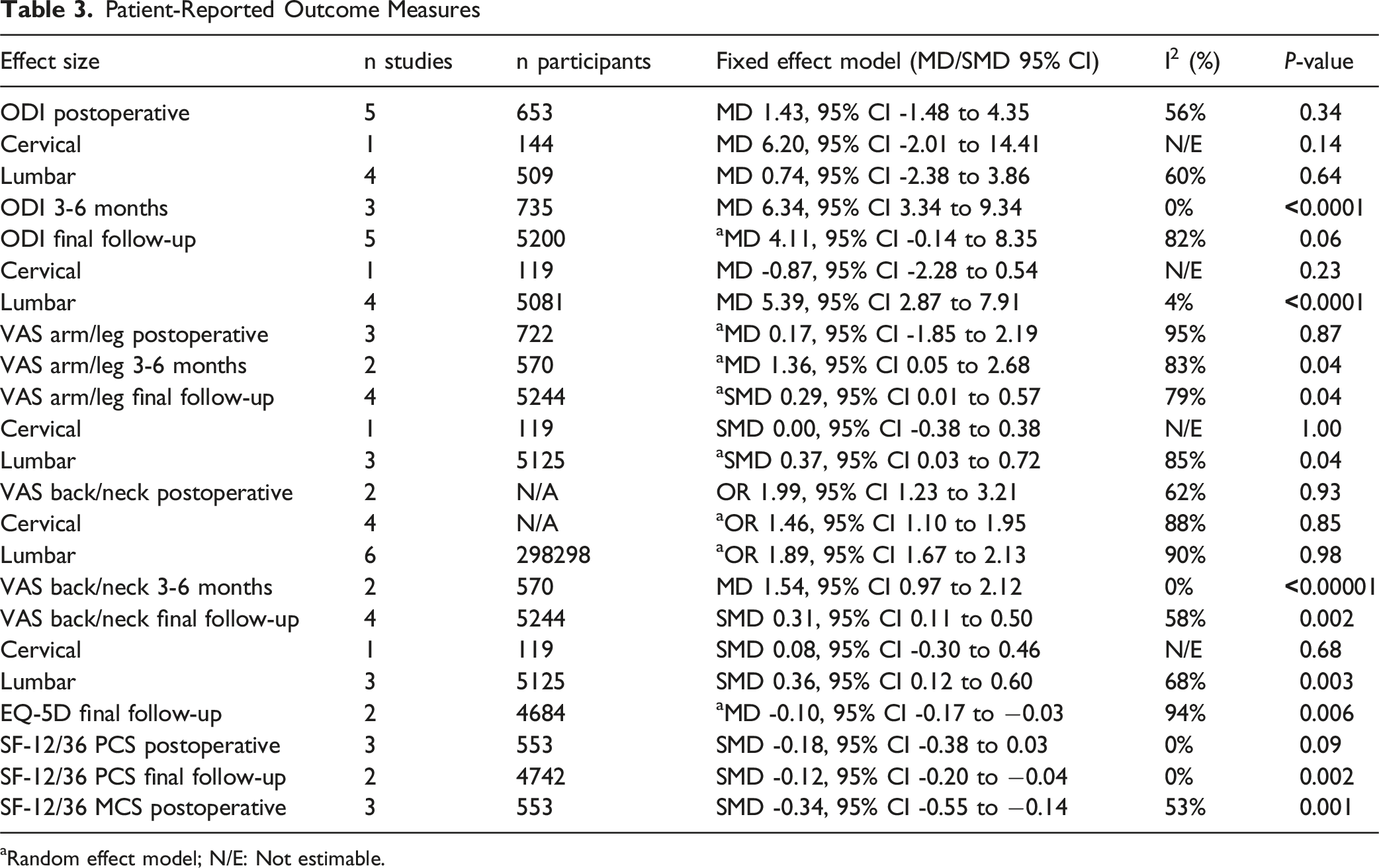
aRandom effect model; N/E: Not estimable.
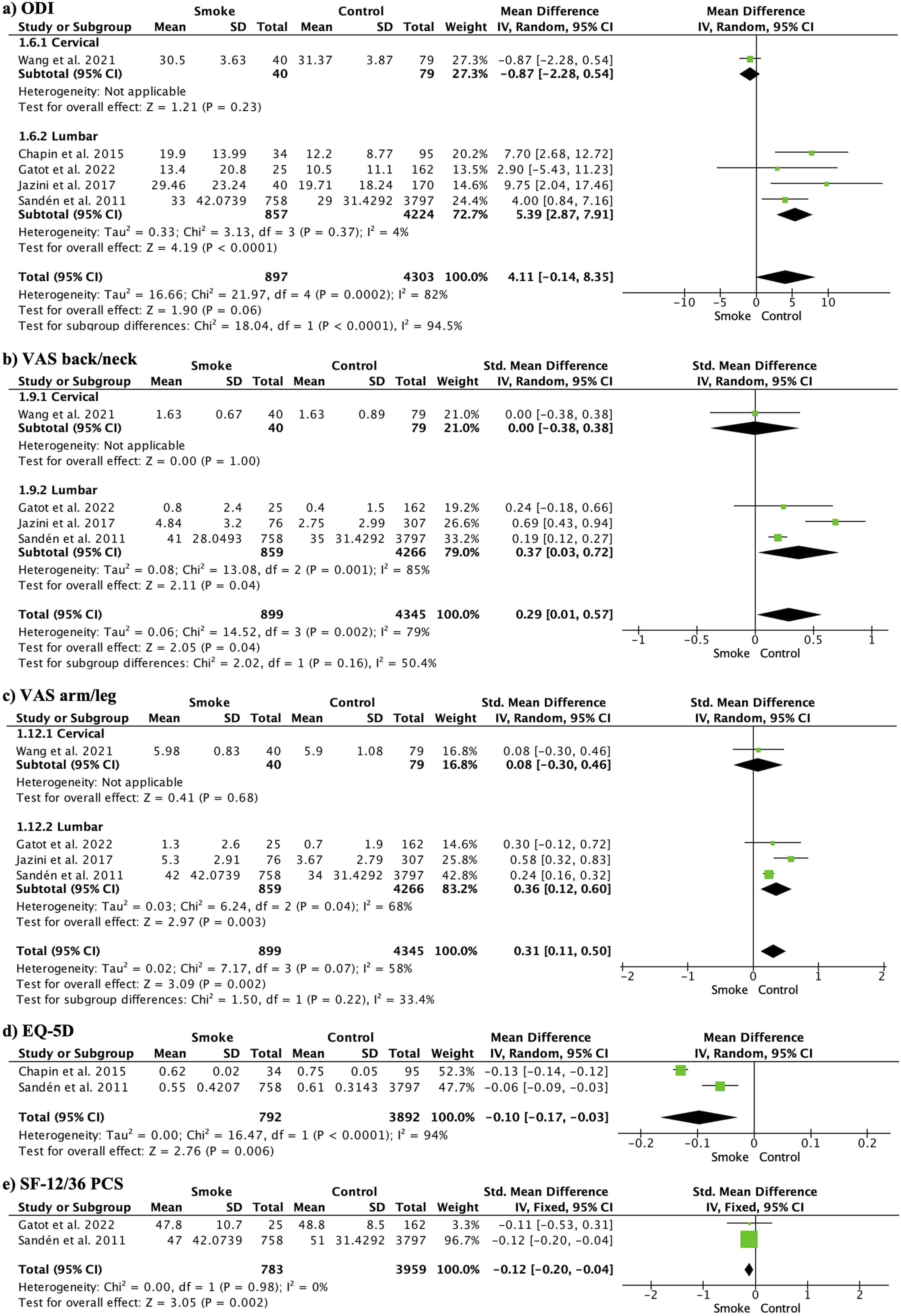
Forest Plots Comparing Smokers (Smoke) With Non-smokers (Control) for Each of the PROMs Studied at the Final Follow-up
The postoperative VAS arm/leg did not show significant differences between smokers and non-smokers (MD0.17, 95% CI -1.85 to 2.19; participants = 722; studies = 3; I2 = 95%). However, at 3-6 months (MD1.36, 95% CI 0.05 to 2.68; participants = 570; studies = 2; I2 = 83%) and at the final follow-up (SMD0.29, 95% CI 0.01 to 0.57; participants = 5244; studies = 4; I2 = 79%), smokers experienced significantly more pain (Figure 4B). Sensitivity analysis did not show any differences at the final follow-up (MD1.73, 95%CI -0.33 to 3.79; participants = 4861; studies = 4; I2 = 93%).
The postoperative VAS back/neck scores did not show significant differences between smokers and non-smokers (SMD-0.02, 95%CI -0.38 to 0.35; participants = 772; studies = 4; I2 = 72%). However, at 3-6 months (MD1.54, 95% CI 0.97 to 2.12; participants = 570; studies = 2; I2 = 0%) and at the final follow-up (SMD0.31, 95% CI 0.11 to 0.50; participants = 5244; studies = 4; I2 = 58%), the smoking group experienced significantly more pain (Figure 4C). Sensitivity analysis did not show any differences at the final follow-up (MD0.35, 95% CI -0.03 to 0.66; participants = 689; studies = 3; I2 = 59%).
The EQ-5D showed worse results in the smoking group (MD-0.12, 95% CI -0.13 to −0.11; participants = 4684; studies = 2; I2 = 94%) (Figure 4D).
Postoperative SF-12/36 PCS did not show significant differences (SMD-0.18, 95% CI -0.38 to 0.03; participants = 553; studies =; I2 = 0%), but the smoking group showed worse results at the final follow-up (SMD-0.12, 95% CI -0.20, −0.04; participants = 4742; studies = 2; I2 = 0%) (Figure 4E). SF-12/36 MCS could only be analyzed postoperatively and did not show significant differences (SMD-0.34, 95% CI -0.55 to −0.14; participants = 553; studies = 3; I2 = 53%). Sensitivity analyses of these variables showed consistency and did not change the direction of the results.
Assessment of the Minimally Clinical Important Difference (MCID)
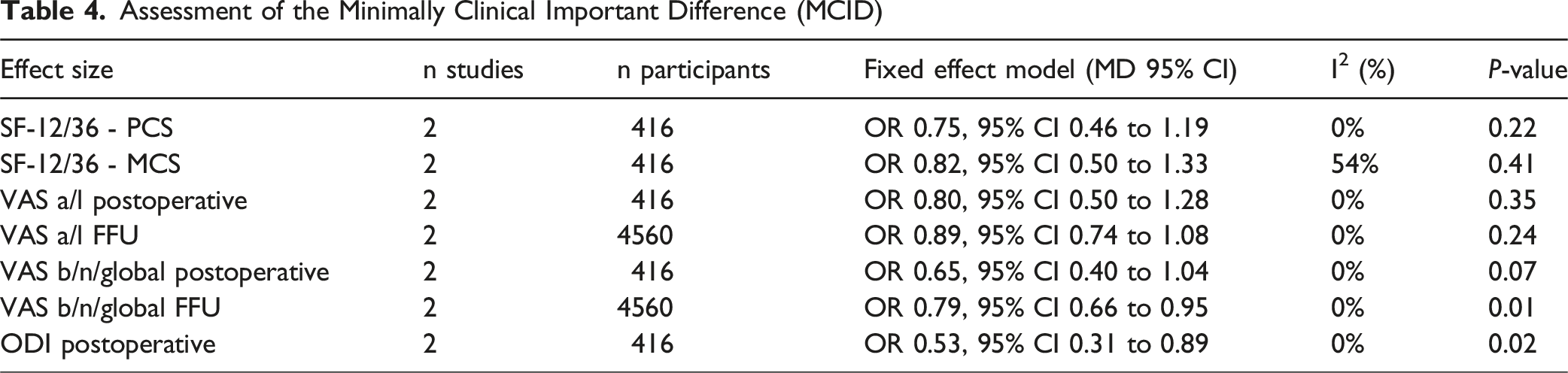
Smokers had a lower return to work frequency (OR0.70, 95% CI 0.54 to 0.90; participants = 2065; studies = 2; I2 = 0%) (Figure 5A). Satisfaction at the final follow-up was also lower in the smoking group (OR0.40, 95% CI 0.15 to 1.08; participants = 4997; studies = 3; I2 = 82%) (Figure 5B). Forest Plot Comparing Return to Work 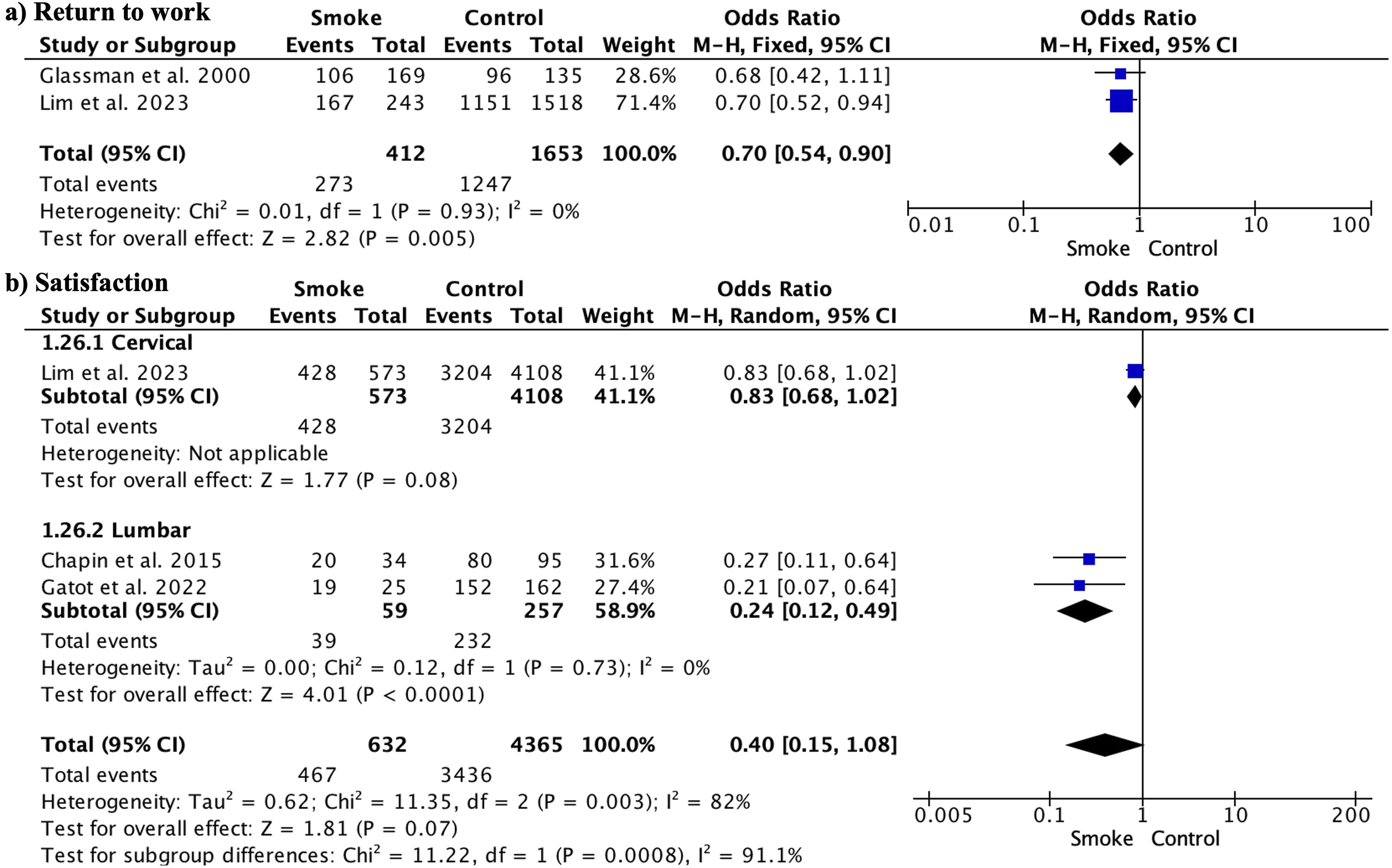
Effect of Smoking Cessation
Data on the effect of smoking cessation were extracted from eight studies (Supplemental Table 3). In lumbar surgery, quitting smoking was associated with higher fusion rates (e.g., Andersen et al, 86.6% vs 77.4%) and a trend toward reduced nonunion even when cessation occurred just 1 month before surgery (Glassman et al). In cervical fusion, lower pseudarthrosis rates were observed in quitters (8.1% vs 16.0%; Lau et al). Improvements in pain scores were inconsistently reported, although some studies noted greater pain reduction or correlation between longer cessation and lower pain (Behrend et al, Jazini et al). The definition of cessation timing varied substantially across studies, ranging from ≥2 weeks to ≥1 year before surgery.
Publication Bias
Publication bias was assessed using funnel plot analysis of the primary outcomes (Figure 6). Upon visual inspection of funnel plots, with effect estimates plotted on the x-axis against their standard errors on the y-axis, asymmetry was observed. This suggests the potential for publication bias, such that smaller or non-significant studies may not have been published. However, funnel plot analysis alone cannot provide conclusive evidence of bias, as asymmetry could arise due to heterogeneity across the included studies. Nonetheless, the possibility of publication bias should be considered when interpreting the findings, as biased literature can overestimate true effects. Funnel Plots Examining Publication Bias for the Main Outcomes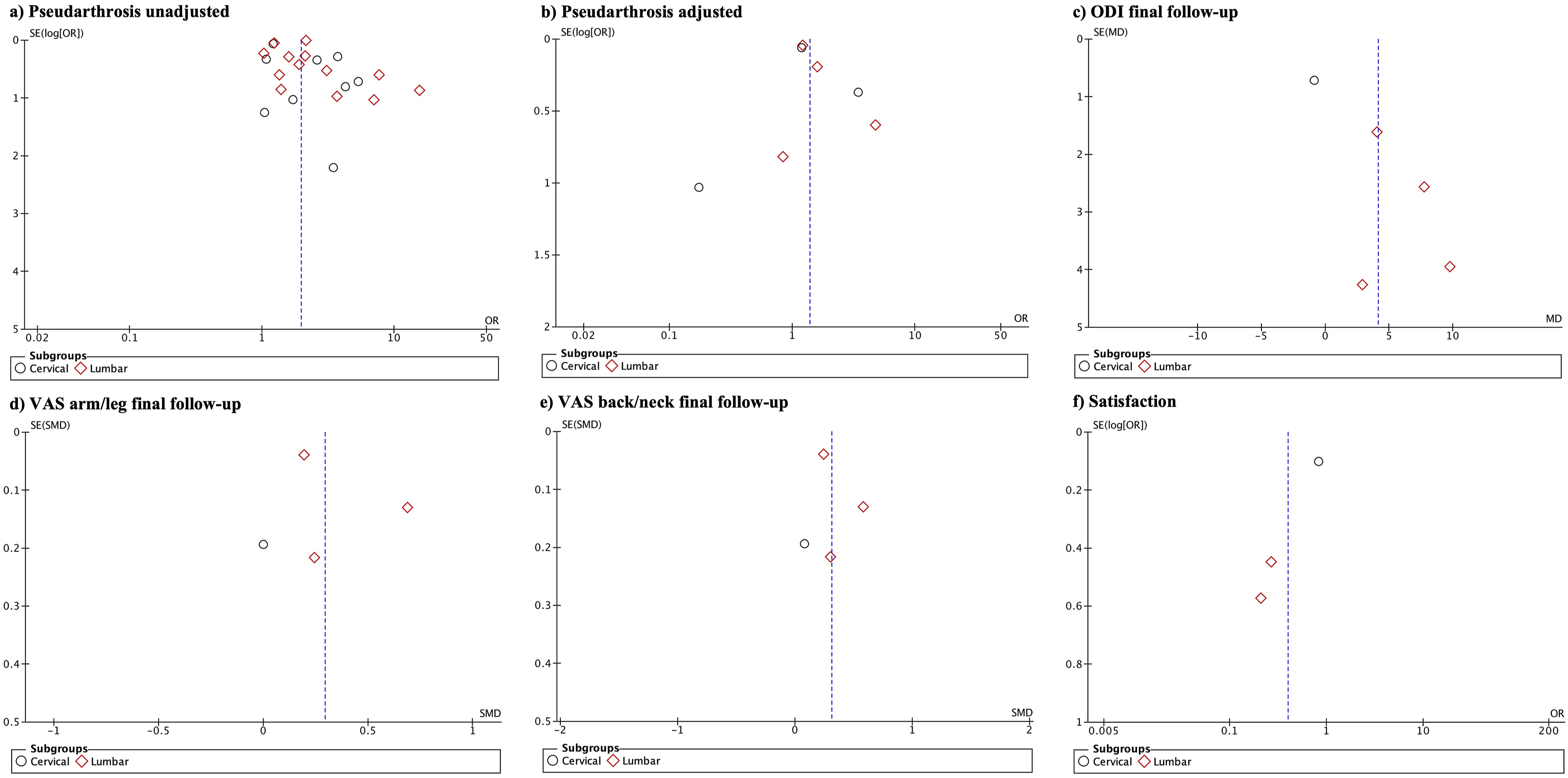
GRADE
GRADE Assessment of the Quality of the Evidence and the Strength of the Recommendations
Discussion
This meta-analysis found that smokers have a higher incidence of pseudarthrosis after spinal surgery compared to non-smokers. Smoking is also linked to greater pain, worse functionality, delayed return to work, and lower satisfaction post-spinal fusion. The quality of the included studies was generally high, but the evidence certainty was moderate to low for most outcomes. Variability in the definition and diagnosis of pseudarthrosis across studies must be considered, as some used clinical symptoms while others relied on imaging modalities like CT or X-rays. Standardizing diagnostic criteria would improve future analyses. The definition of smoking was not standardized or was unspecified in several of the included studies. Of the studies included, 13 did not provide a formal definition of smoking status. Among those that did, definitions varied considerably: some classified smokers based on the number of cigarettes consumed, while others used temporal criteria such as smoking within 2 weeks, 6 weeks, 6 months, or 1 year before surgery. A few distinguished between current, former, and never smokers using predefined cessation cut-offs. One study identified tobacco use exclusively through diagnostic codes, and another focused on chewing tobacco rather than smoking. This variability underscores the lack of standardization in assessing smoking status across the included literature.
Smoking’s negative impact on fusion outcomes may also depend on the type of implant material used; for instance, smokers had worse results with PEEK interbody cages. 45 Microvascular impairment, caused by nicotine-induced vasoconstriction, reduces blood flow and nutrient availability, leading to pseudarthrosis. 4 Smoking is also associated with lower vitamin D levels 46 and comorbidities like diabetes and hypertension, further increasing pseudarthrosis risk. 47
Smokers undergoing spinal fusion were, on average, younger than non-smokers in the studies, suggesting that smoking accelerates spinal degeneration. This aligns with the concept of “accelerated aging”, which is observed in cardiovascular, lung, and other organ systems. Consistent with prior studies, multilevel fusion procedures were linked to higher pseudarthrosis rates compared to single-level surgeries. 48 Increased instability over a larger bony surface area may make fusion more vulnerable to smoking-induced microvascular changes, possibly indicating a dose-response relationship. Regarding minimally invasive techniques (MIS), Emami et al. found that pseudarthrosis could also occur after MIS transforaminal lumbar interbody fusion (MIS TLIF). This suggests that pseudarthrosis is more influenced by physiological factors such as smoking, obesity, diabetes, and age, rather than the type of surgical procedure. 49
Kim et al suggested that the thoracolumbar area is at higher risk of pseudarthrosis, recommending additional grafts in this region. 30 However, this meta-analysis found no significant differences in pseudarthrosis rates between the thoracolumbar and cervical spine, despite the cervical spine being more vascularized. 50 For grafts to function properly, adequate vascularization is necessary, but smoking-induced vascular impairment can hinder this. 34 Regarding modern graft options, Advanced graft technologies may deliver options for improving fusion success, mitigating some of the negative effects reported with smoking. 46 Additionally, no differences were found in pseudarthrosis incidence based on study definitions or imaging tests (CT or X-ray).
Smokers undergoing spinal surgery reported worse pain and functional outcomes. This could be due to nicotine’s neurophysiological effects, mental health issues, 51 and reduced regenerative capacity. 52 Smoking may impede nerve recovery, increase psychological distress, and delay tissue healing, worsening clinical outcomes. Unresolved pseudarthrosis can also cause persistent pain. 53
Regarding return to work, the studies included in this meta-analysis only reported the incidence of patients resuming work and did not provide information on how other factors might influence this outcome. In spinal surgery, factors such as older age, higher body mass index (BMI), physically demanding jobs, pain, and worker’s compensation status have been shown to affect return to work. Additionally, none of the studies in this meta-analysis reported the average time to return to work, though some mentioned a timeframe around 9 months.54–56
Regarding smoking cessation, there is limited and heterogeneous evidence across the included studies, but the available data consistently point toward clinical benefits that warrant strong surgical recommendations (Supplemental Table 3). Smoking cessation was generally associated with higher fusion rates, with several studies reporting absolute improvements of 8-9% compared to continued smokers (e.g., Andersen et al, 86.6% vs 77.4% in lumbar cases; Lau et al, pseudarthrosis 8.1% vs 16.0% in cervical procedures). Glassman et al demonstrated a dose–response relationship particularly in lumbar fusion, where patients who quit even 1 month before surgery had lower nonunion rates than those who continued smoking, and quitting 6 months prior yielded the best return-to-work outcomes. Overall, the data on lumbar surgery are more extensive and consistent, while evidence for cervical fusion is less abundant but suggests a similar positive trend with smoking cessation. Effects on patient-reported measures (PROMs) were more variable: Andersen et al found no significant change in satisfaction primarily in lumbar cases, whereas Behrend et al (spine overall) observed greater reductions in worst pain among quitters, and Jazini et al reported that longer postoperative cessation correlated with lower pain scores at 12 months in lumbar patients. Definitions of cessation timing varied widely across locations (≥2 weeks, ≥6 weeks, ≥6 months, ≥1 year), yet the overall trend suggests that earlier and sustained quitting—ideally several weeks to months before surgery—maximizes the likelihood of solid fusion and may enhance pain outcomes regardless of spinal region. Based on this evidence, spine surgeons should actively integrate structured, early smoking cessation programs into preoperative management, clearly communicating that continued smoking increases the risk of pseudarthrosis, persistent pain, delayed functional recovery, and higher postoperative analgesic needs.52,53,57,58 Combining cessation counseling with optimized perioperative pain control may improve both structural and patient-reported outcomes across lumbar and cervical spine surgeries.
Can be high, but Andersen et al found that only 13% quit despite being warned of the risks.10,11 The studies included in our meta-analysis did not distinguish between the effects of cigarette smoking and smokeless tobacco use on spinal fusion rates; typically, “smoking” herein refers to combusted tobacco products. Only 1 study specifically assessed chewing tobacco, finding that its use was associated with a risk of pseudoarthrosis similar to that observed for cigarette smokers (OR 2.15, 95% CI 2.09-2.21), aligning closely with the global risk reported in our meta-analysis (Cole et al). 26
Emerging evidence suggests that other non-combustible nicotine products such as vapes and e-cigarettes may confer similar surgical risks to smoking, including impaired wound healing and bone health. For example, nicotine exposure from vaping in adolescents has been shown to be comparable to that of traditional smoking, particularly when nicotine salt products are used (Hammond et al). 59
Vaping is linked to postoperative complications such as delayed wound healing and increased infection risk, as highlighted in systematic reviews and clinical observations (Ashour et al). 60 E-liquids contain toxins such as cadmium and aromatic flavorings, which can impair osteoblast function, reduce bone mineral density, and increase susceptibility to osteoporosis and delayed fracture healing, all of which could theoretically contribute to spinal fusion failure (Fiani et al; Nicholson et al).61,62
Although the literature in spine and orthopedic surgery is still limited, recent data consistently show that use of non-tobacco nicotine products—including vaping and chewing tobacco—can substantially increase perioperative risks. A pioneering study demonstrated that vaping was associated with longer surgical times and increased readmissions in joint arthroplasty patients (Bieganowski et al). 63
On the other hand, substances such as cannabis have been shown to negatively impact spine surgery outcomes, both in lumbar and cervical fusions, by significantly increasing the rate of pseudarthrosis. Cannabis use is also associated with a three to fourfold increase in the risk of revision surgeries, along with higher opioid consumption and longer hospital stays. 64
Moreover, both nicotine and cannabis use have been shown to further complicate recovery following orthopedic and spinal surgery. Preoperative identification and management of these risk factors are essential for optimizing wound healing and improving functional outcomes (Shore et al 2021). 65
Limitations
This study has several limitations that should be considered when interpreting the results. Most included studies were retrospective, which can introduce bias and limit the validity of findings. Additionally, variations in the definition of pseudarthrosis hinder comparisons across studies. The lack of a standardized definition of smoking status across the included studies, with many not reporting it and others using highly variable criteria, prevented its inclusion in subgroup analyses. Another limitation of this meta-analysis was the inability to differentiate between the effects of cigarette smoking and other forms of nicotine use, such as smokeless tobacco or vaping, on fusion outcomes, as none of the included studies provided separate or specific data on these alternative nicotine products. Few studies focused on cervical-level assessments, limiting comparisons in this area, and most did not use Patient-Reported Outcome Measures (PROMs). Future studies should include additional PROMs, such as PROMIS, and provide more detailed information on return-to-work outcomes, emphasizing the type of occupation as well as the influence of factors such as spinal level. There was also variability in follow-up periods, with some studies having 1-year follow-ups while others had longer periods, affecting result comparability. Different functional scales using various instruments were combined, introducing potential bias. Some variables were based on only two studies, highlighting the need for larger sample sizes in future research. Furthermore, many studies compared smokers and non-smokers without distinguishing between current and former smokers, limiting the understanding of smoking’s impact. Few studies clearly defined smoking categories, complicating interpretation. Additionally, the heterogeneity of etiologies and procedures used in the studies limits the generalizability of results. Most studies lacked adjusted effect estimates or did not specify covariates, and the majority were conducted in the United States, limiting extrapolation to other countries and healthcare systems.
Conclusions
This study found that smokers had a significantly higher incidence of pseudarthrosis and worse patient-reported outcomes at both cervical and lumbar levels compared to non-smokers. These differences were more pronounced at 3-6 months and at final follow-up, with smokers also experiencing lower return-to-work rates and satisfaction. Prospective studies are needed to reduce bias, and a consensus on pseudarthrosis definitions should be established. Smoking cessation should be encouraged to improve clinical outcomes and health.
Supplemental Material
Supplemental Material - Adverse Impact of Smoking on Spine Fusion and Patient-Reported Outcomes: A Systematic Review and Meta-Analysis
Supplemental Material for Adverse Impact of Smoking on Spine Fusion and Patient-Reported Outcomes: A Systematic Review and Meta-Analysis by P.M. Arnold, J.S. Harrop, G. Mariscal, R.C. Sasso, M.P. Steinmetz, C.D. Chaput, W.B. Jacobs, C.D. Witiw, J.E. O'Toole in Global Spine Journal.
Footnotes
Ethical Considerations
As this research is a meta-analysis, it does not involve any direct human or animal subjects and therefore does not require ethical approval from an Institutional Review Board (IRB).
Author Contributions
Conceptualization; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Data curation; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Formal analysis; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Funding acquisition; C.D.C.; C.D.W.; Investigation; P.M.A.; J.S.H.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Methodology; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Project administration; P.M.A.; C.D.C.; C.D.W.; Resources; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Software; Supervision; P.M.A.; G.M.; Validation; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Visualization; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; Roles/Writing - original draft; P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.; and Writing - review & editing: P.M.A.; J.S.H.; G.M.; R.C.S.; M.P.S.; C.D.C.; W.B.J.; C.D.W.; J.E.O.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Cerapedics Inc.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Dr M.P. Steinmetz received royalties from Elsevier and Globus Medical, Inc an honorarium from Globus Medical, Inc and consulting fees from Cerapedics Inc.
Dr J.S. Harrop is a scientific advisor to Johnson & Johnson, Spiderwort Inc, and Kringle Pharma, Inc.
Dr C.D. Witiw received institutional research funding from the Canadian Institutes of Health Research and Cerapedics Inc, as well as speaking and consulting fees from Stryker Corp.
Dr J.E. O’Toole received consulting fees and royalties from Globus Medical, Inc, consulting fees from Cerapedics Inc, royalties from Medtronic plc and NuVasive, Inc and owns stock in Viseon Inc.
Dr C.D. Chaput received institutional research funding from Cerapedics Inc, Kuros Biosciences A.G., and Nuvasive, Inc and received royalties from Globus Medical, Inc.
Dr W.B. Jacobs received consulting and speaking fees from DePuy-Synthes, Inc, Stryker Corp, and Cerapedics Inc.
Dr R.C. Sasso received royalties from Medtronic plc and NuVasive, Inc.
Dr G. Mariscal received consulting fees from Cerapedics Inc.
Dr P.M. Arnold has no relevant financial or non-financial interests to disclose.
Data Availability Statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Data may be available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.