
Abstract
Study Design
Retrospective cohort study.
Objective
Condoliase is a chemonucleolysis for lumbar disc herniation (LDH) that enzymatically degrades herniated disc material with high specificity for chondroitin sulfate and hyaluronic acid. Few studies have compared condoliase treatment with surgical treatments. We compared the clinical outcomes of condoliase treatment and minimally invasive discectomy.
Methods
Patients who received condoliase treatment or minimally invasive discectomy at single institution were included. Propensity score matching was performed to adjust for age and sex. We included 146 patients with LDH (73 per group). The Japan Orthopaedic Association (JOA) score, visual analog scale (VAS) for leg pain, and disc height and degeneration were assessed at baseline and 2 weeks, 3 months, and 1 year after treatment.
Results
The JOA score and leg pain VAS improved significantly over time (P < .001, Friedman’s test). Two weeks after treatment, a marked improvement in JOA score and leg pain VAS was observed in the surgery group compared with the condoliase group (P < .001, mixed-effects model). However, 3 months and 1 year after treatment, the differences were not significant. In contrast, disc height reduction was significantly greater in the condoliase group than in the surgery group at 3 months and 1 year after treatment (P < .001, mixed-effects model). Condoliase treatment was identified as an independent risk factor for progression of disc degeneration (odds ratio, 23.60; P = .001, logistic regression analysis).
Conclusion
Condoliase treatment demonstrated mid-term efficacy comparable to surgical treatment; however, it required more time for pain relief and was potentially associated with progression of disc degeneration.
Keywords
Introduction
Lumbar disc herniation (LDH) is a common disease caused by displacement of the nucleus pulposus or annulus fibrosus beyond the intervertebral disc space, which affects approximately 1% to 3% of people annually. 1 The extruded disc material compresses the spinal nerve root, causing radicular leg pain that contributes to disability, increased healthcare utilization, and reduced quality of life (QOL). 2 While conservative treatment is standard, several studies have shown that surgery results in rapid pain relief and subjective recovery in patients with LDH.3-5 A prospective randomized cohort study showed that surgery led to greater improvement than nonoperative treatment. 6 However, surgical treatment requires hospitalization and is more costly than conservative treatment.7,8
Chemonucleolysis aims to enzymatically degrade herniated disc material and relieve associated symptoms and is considered an intermediate treatment between surgery and conservative therapy for LDH. 9 Chymopapain is a type of chemonucleolysis that has been previously used for LDH. 10 However, owing to its low substrate specificity, chymopapain also acts on the tissue surrounding the intervertebral disc and is currently unavailable owing to serious adverse events, including anaphylaxis, infection, hemorrhage, and neurological complications. 11 Condoliase (chondroitin sulfate ABC endolyase), which is available for chemonucleolysis, is a pure mucopolysaccharidase derived from the gram-negative rod Proteus vulgaris, with high substrate specificity for chondroitin sulfate and hyaluronic acid. 12 Unlike chymopapain, condoliase exhibits high substrate specificity for chondroitin sulfate and hyaluronic acid, allowing it to selectively break down proteoglycan-rich tissues while preserving surrounding non-proteoglycan structures. Additionally, condoliase lacks protease activity, making it a safe alternative. 13 A phase III, randomized, double-blind, placebo-controlled trial showed that condoliase significantly improved leg pain, physical function, and QOL for LDH. 14 Approved in Japan since 2018, a meta-analysis showed that condoliase treatment had a 78% success rate with no major adverse events. 10 Condoliase can be injected into the intervertebral disc under local anesthesia and generally does not require hospitalization. Considering rising healthcare costs, condoliase treatment may be a more effective option than surgical treatment, which requires general anesthesia and hospitalization.
In the current clinical practice, surgical and condoliase treatment are two options for patients with LDH that does not improve by conservative treatment. Although the effectiveness of condoliase treatment has been well validated compared with prolonged conservative treatment, few studies have compared condoliase treatment with surgery. We aimed to compare the early and midterm clinical outcomes, including intervertebral disc degeneration, of chemonucleolysis with condoliase and minimally invasive discectomy in patients with LDH.
Materials and Methods
Study Design
This retrospective cohort study included patients who received intradiscal condoliase injections for LDH between September 2018 and May 2024 and underwent minimally invasive discectomy for LDH between March 2010 and July 2023 at a single institution. The research protocol was approved by the Institutional Review Board, and all patients provided written informed consent. All the experiments were conducted in compliance with the principles of the Declaration of Helsinki.
Patients
LDH was diagnosed in patients who met the following criteria: presence of lower extremity pain, herniation verified on magnetic resonance imaging (MRI), and neurological symptoms consistent with the distribution of the compressed nerve root. Both condoliase treatment and minimally invasive discectomy were indicated for patients with LDH who were unresponsive to conservative treatment. Since the approval of the clinical use of condoliase, experienced spine surgeons selected one of the treatments for LDH based on patient preferences. The selection between surgery and condoliase treatment was based on patient preference, ability to be admitted to the hospital, and whether general anesthesia could be tolerated. Patients who had received condoliase treatment at a previously surgically treated intervertebral level were excluded. Among patients who underwent minimally invasive discectomy, those with a history of surgery or condoliase injection in the same intervertebral disc as well as those who underwent surgery at multiple intervertebral levels were excluded. Additionally, patients with a follow-up period of <2 weeks were excluded.
Condoliase Treatment
The condoliase injection was administered by a board-certified orthopaedic spine surgeon. Patients were placed in a semilateral decubitus position on a radiolucent bed. Using fluoroscopic guidance, the surgeon directed a needle into the intervertebral disc from the contralateral side of herniation and injected condoliase (1.25 U/1.0 mL saline) into the intervertebral disc as close to the center as possible. All patients received the same dose, following the approved clinical use of condoliase in Japan. After careful monitoring for 2 hours, patients with no observed abnormalities were permitted to return home.
Minimally Invasive Discectomy
Minimally invasive surgeries included microendoscopic discectomy (MED) and microscopic discectomy for LDH. MED was chosen as the first-line surgical treatment, whereas microscopic discectomy was selected after lumbar fusion surgery to avoid interference between the rod and tubular retractor. All patients were hospitalized, and surgeries were performed under general anesthesia in the prone position. The surgical procedure was as follows: for MED, a 2-cm skin incision was made lateral to the spinous process, a tubular retractor was inserted into the intervertebral space using a serial dilator system, and discectomy was performed. 15 For microscopic discectomy, a 2.5-cm skin incision was made, and discectomy was performed using a microscope. 16 All patients in this study received inpatient care within the national healthcare insurance system (Diagnosis Procedure Combination [DPC]), 17 which permits up to 30 days hospitalization for LDH postoperative care and rehabilitation.
Clinical Outcomes
The following data were collected from all the patients: age, sex, body height, body weight, comorbidities, herniation type, herniation level, symptomatic duration before treatment, duration of follow-up, and duration of hospitalization. At baseline and 2 weeks, 3 months, and 1 year after treatment, the Japan Orthopaedic Association (JOA) score for low back pain was assessed as an objective measure, and the visual analog scale (VAS) score for leg pain was used as a patient-reported outcome. 18 Patients with ≥50% improvement in leg pain VAS scores from the baseline were defined as having effective treatment. 19 Achievement of the minimum clinically important difference (MCID) in leg pain, defined as an improvement of ≥16 mm on the 0-100 mm VAS scale, 20 was also evaluated. One year after treatment, complications, including additional surgery, were evaluated. Additional surgery was assessed throughout the observation period.
Radiographic Data
MRI was performed at baseline and 3 months and 1 year after treatment. Disc height was defined as the line connecting the upper and lower endplates of the midsagittal slice on MRI (Figure 1).
21
Moreover, the Pfirrmann and Modic classification systems were evaluated using MRI.22,23 The proportion of patients whose Pfirrmann classification grade had progressed before and after treatment was also evaluated. Disc Height is Defined as the White Line Connecting the Upper and Lower Endplates in the Midsagittal Slice on Magnetic Resonance Imaging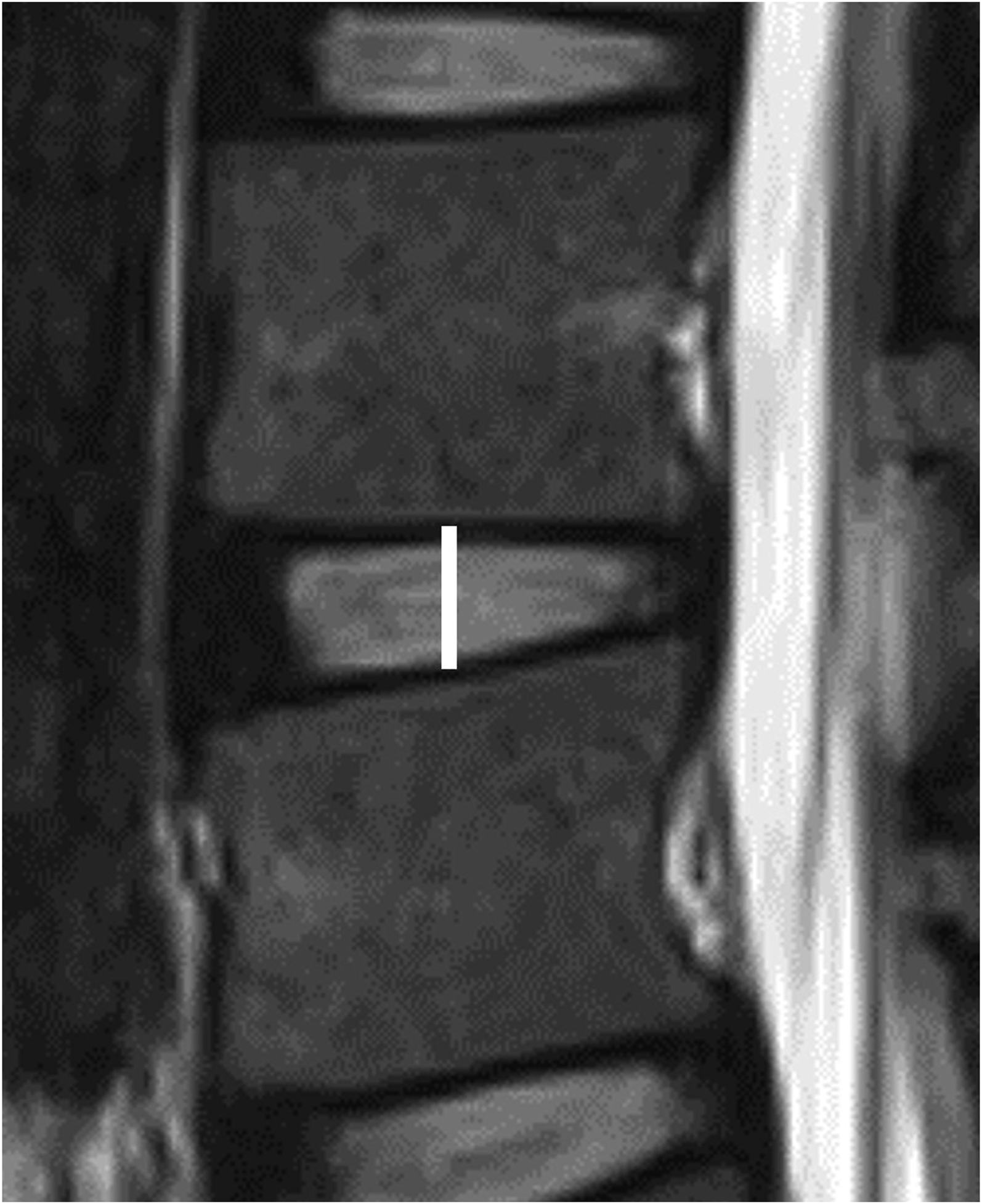
Statistical Analysis
Propensity score matching (PSM) was used to adjust for age and sex in patients who received condoliase treatment or underwent surgery for LDH. PSM was performed with a one-to-one nearest neighbor matching technique, a match tolerance of 0.2, and without replacement. After PSM, the group receiving condoliase treatment was defined as the condoliase group, and the group undergoing surgery was defined as the surgery group. Univariate analysis was performed using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables, followed by residual analysis. Changes in the JOA score, VAS score, and disc height were analyzed within each group using Friedman’s test. Mixed-effects models were used to assess the longitudinal changes and intergroup differences. The model included timepoint, treatment group, and their interaction as fixed effects, and a random intercept for each patient to account for repeated measures. Logistic regression analysis was used to identify the risk factors for Pfirrmann classification progression, with explanatory variables such as age, sex, herniation type, and treatment. Herniation types were categorized as contained (protrusion and subligamentous extrusion) or noncontained (transligamentous extrusion and sequestration). Kaplan–Meier survival analysis was used to estimate the cumulative incidence of additional surgery after treatment in each group, and differences between the two groups were compared using the log-rank test. Statistical analyses were performed using EZR, a graphical user interface for R (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria). All statistical tests were two-sided, and a P value of <.05 was considered statistically significant.
Results
Patients’ Demographics
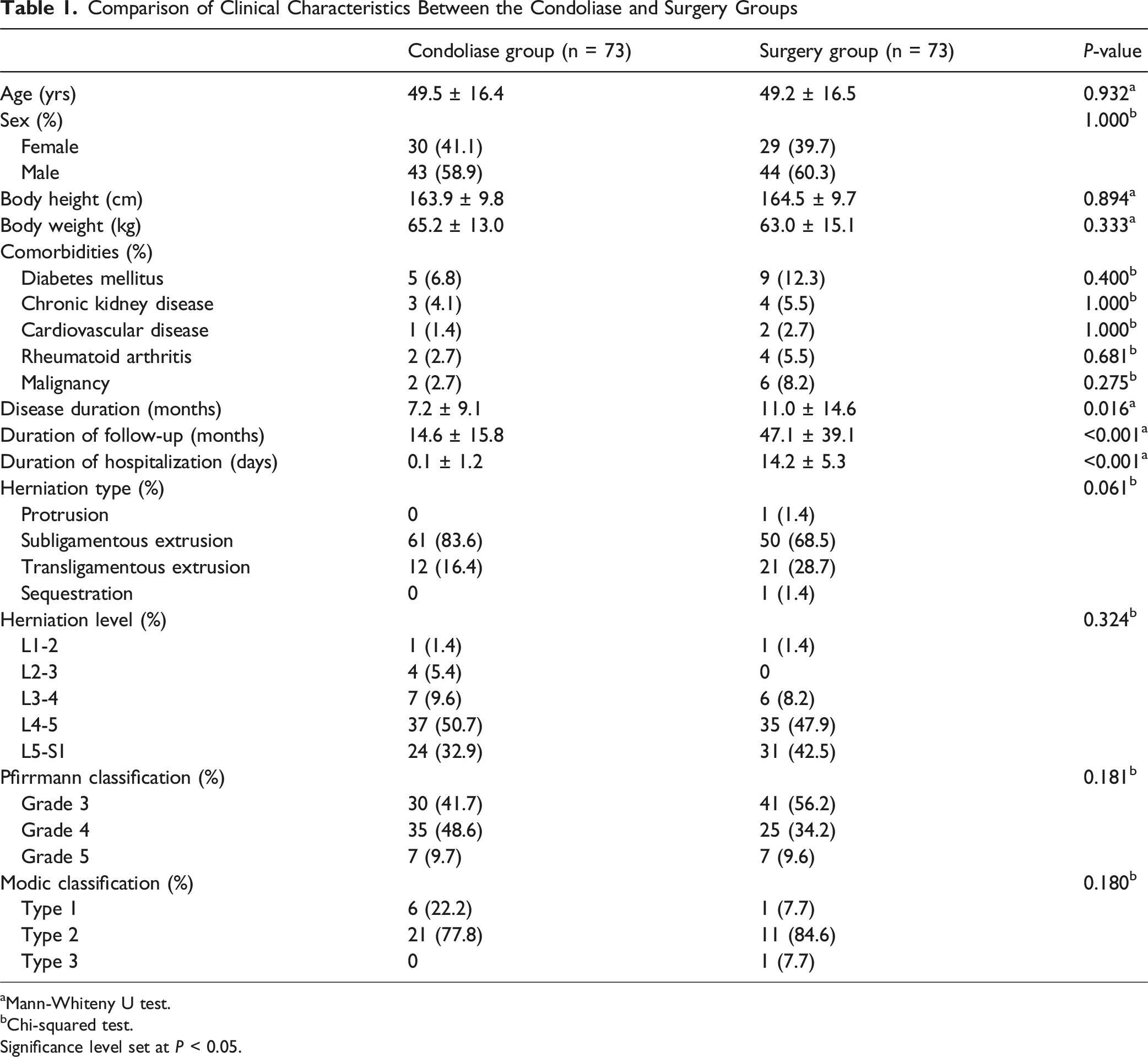
During the study period, 130 patients received an intradiscal injection of condoliase, and 121 underwent minimally invasive discectomy for LDH. Among them, 109 patients who received condoliase treatment and 92 who underwent surgery were included in the study. After PSM, 146 patients were included in the condoliase and surgery groups, with 73 patients in each group (Figure 2). Among the surgery group, 67 patients underwent MED, and 6 underwent microscopic discectomy. No significant differences in age, sex, body height, body weight, comorbidities (eg, diabetes mellitus, chronic kidney disease, cardiovascular disease, rheumatoid arthritis, and malignancy), herniation type, herniation level, Pfirrmann grade and Modic classification were observed between the two groups. Disease, follow-up, and hospitalization durations were significantly longer in the surgery group than in the condoliase group (P = .016, P < .001, and P < .001, respectively; Table 1). Flowchart of Patient Inclusion and Propensity Score Matching Comparison of Clinical Characteristics Between the Condoliase and Surgery Groups aMann-Whiteny U test. bChi-squared test. Significance level set at P < 0.05.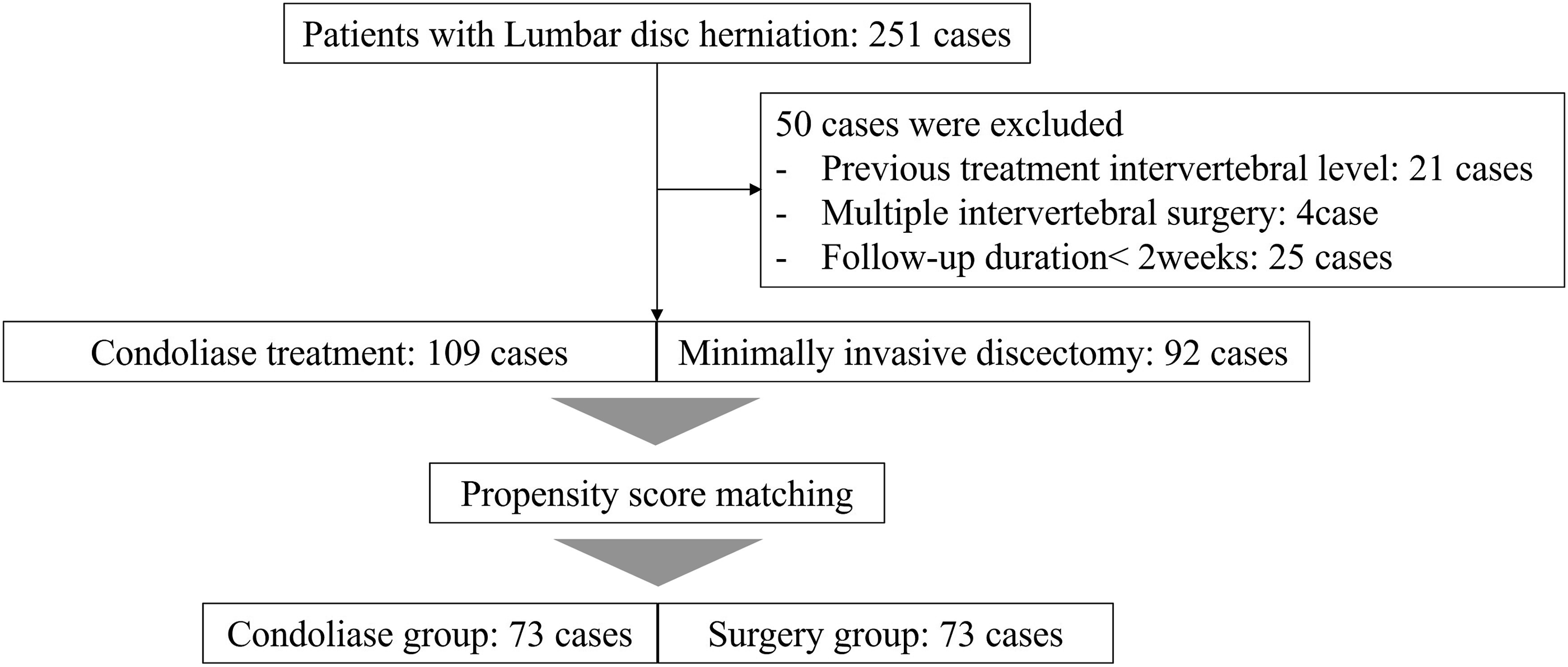
Efficacy
Changes Over Time in the Japanese Orthopaedic Association Score, Leg Pain Visual Analog Scale Score, and Disc Height
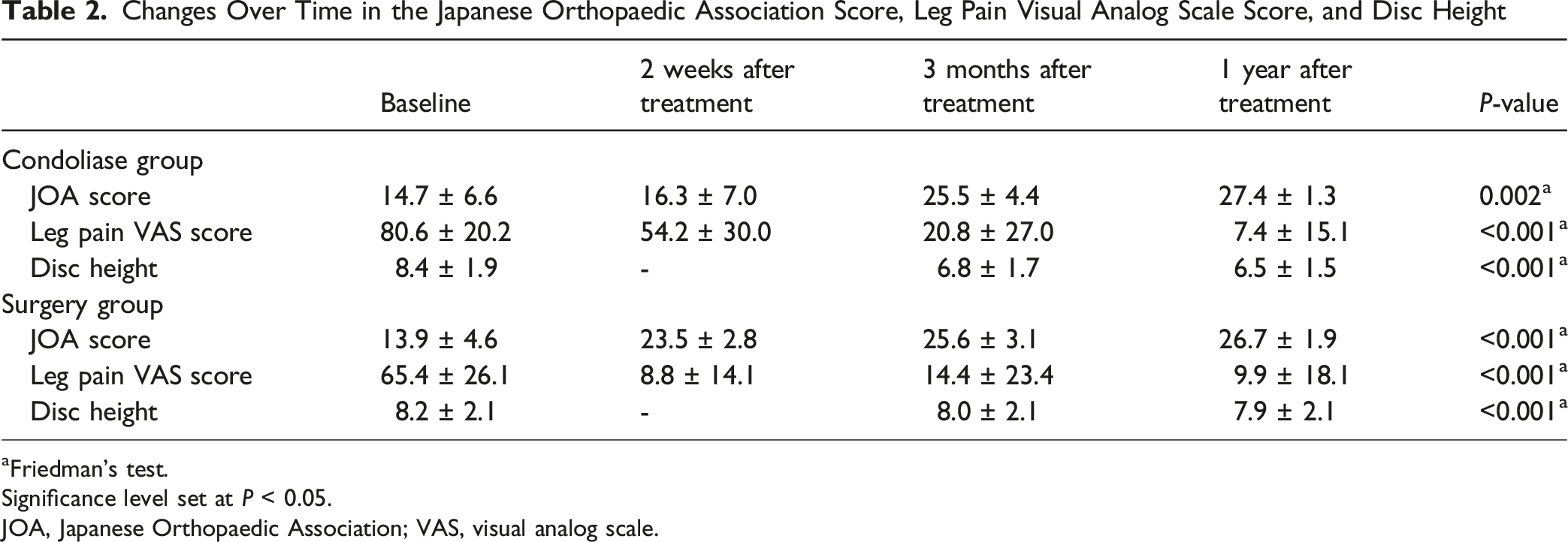
aFriedman’s test.
Significance level set at P < 0.05.
JOA, Japanese Orthopaedic Association; VAS, visual analog scale.
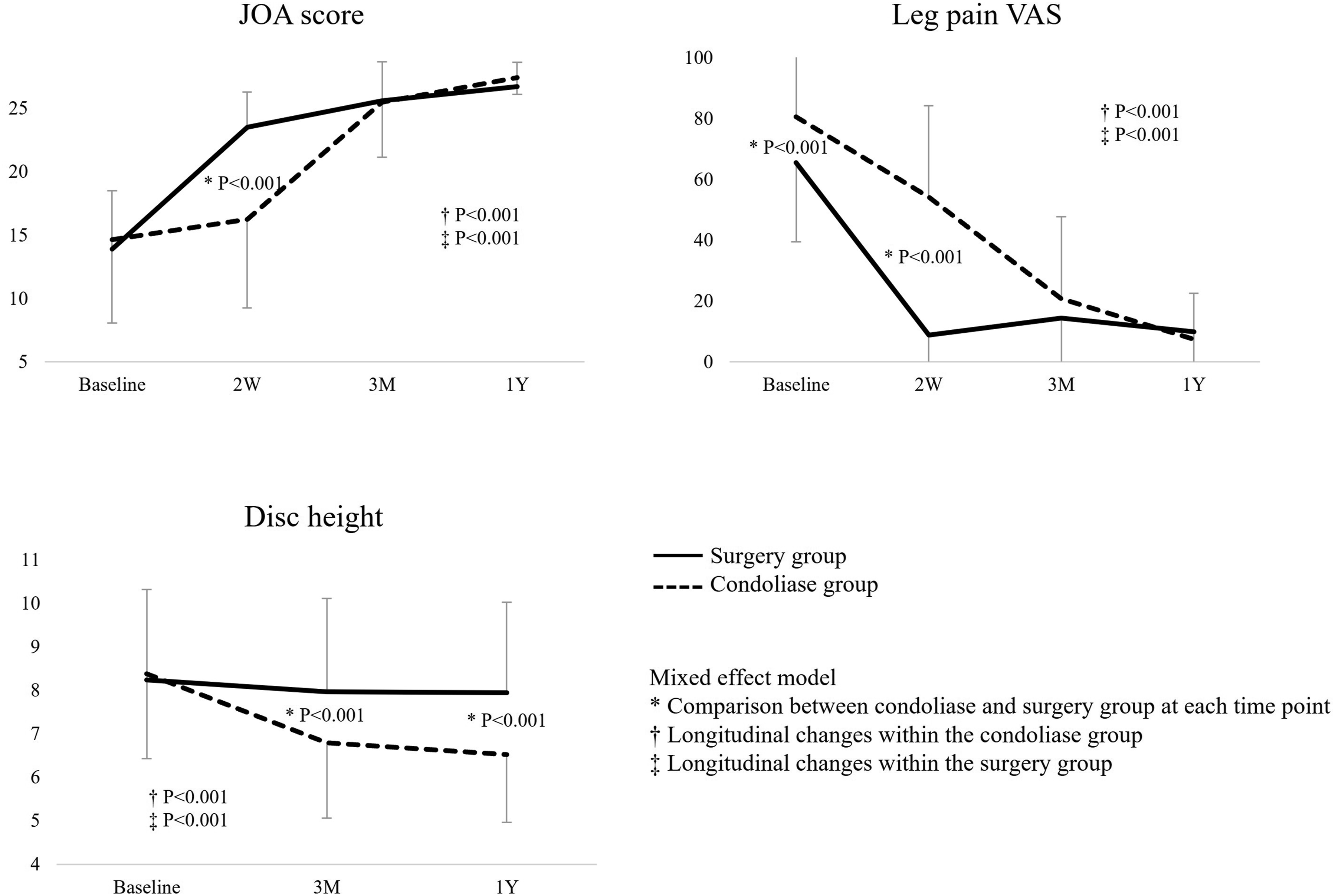
Longitudinal Changes in the Japanese Orthopaedic Association Score, Leg Pain Visual Analog Scale Score, and Disc Height Within Each Group and Comparison Between the Condoliase and Surgery Groups in the Mixed-Effects Model. JOA, Japanese Orthopaedic Association; VAS, Visual Analog Scale Solid Lines Represent the Surgery Group; Dotted Lines Represent the Condoliase Group
Comparison of Clinical Outcomes Between the Condoliase and Surgery Groups
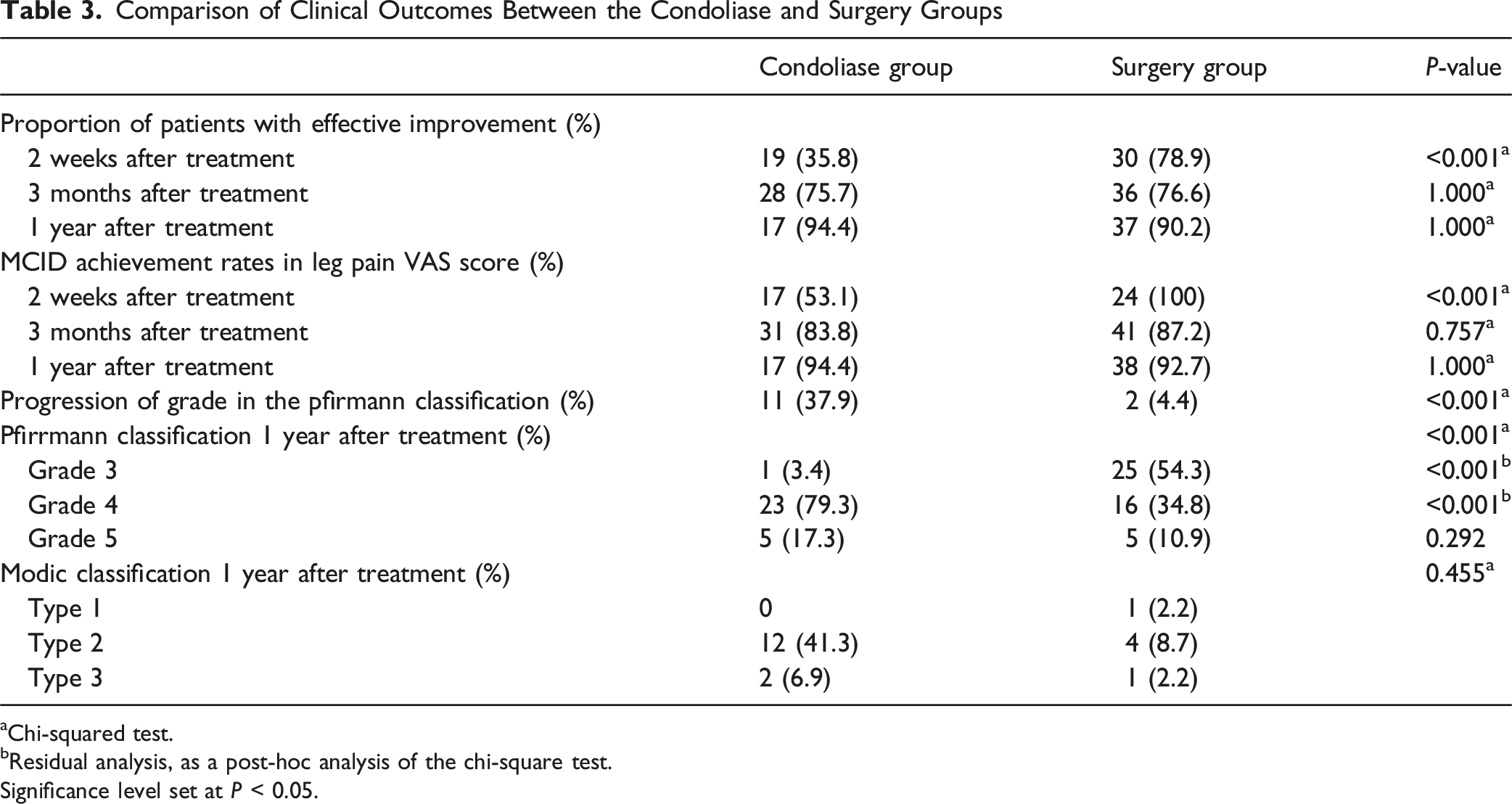
aChi-squared test.
bResidual analysis, as a post-hoc analysis of the chi-square test.
Significance level set at P < 0.05.
Disc Height and Degeneration
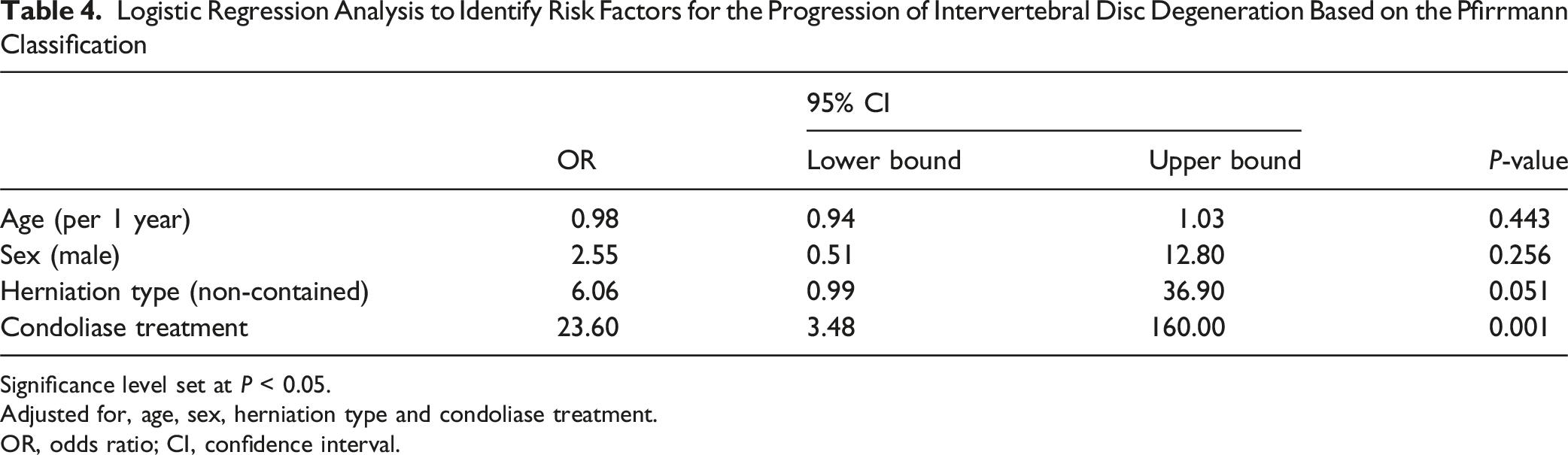
The disc height changed significantly in both groups before and after treatment (Friedman’s test, P < .001; Table 2). In the mixed-effects model, significant longitudinal changes in disc height were observed between the two groups; 3 months and 1 year after treatment, the reduction in disc height was significantly greater in the condoliase group than in the surgery group (Figure 3). The proportion of patients showing progression of grade in the Pfirrmann classification from pre-treatment to 1-year post-treatment was significantly higher in the condoliase group than in the surgery group (37.9% vs 4.4%, P < .001; Table 3, Figure 4). No significant differences in Modic classification changes were observed between the groups. Using logistic regression analysis, condoliase was identified as a significant risk factor for progression of intervertebral disc degeneration based on the Pfirrmann classification, independent of age, sex and herniation type (odds ratio, 23.60; 95% confidence interval, 3.48-160.00; P = .001; Table 4). Disc Degeneration Based on the Pfirrmann Classification Using Magnetic Resonance Imaging after Condoliase Injection Into the Intervertebral Disc. Left: Before Condoliase Treatment, Corresponding to Grade 3 according to the Pfirrmann Classification. Right: After Condoliase Treatment, Corresponding to Grade 4 according to the Pfirrmann Classification Logistic Regression Analysis to Identify Risk Factors for the Progression of Intervertebral Disc Degeneration Based on the Pfirrmann Classification Significance level set at P < 0.05. Adjusted for, age, sex, herniation type and condoliase treatment. OR, odds ratio; CI, confidence interval.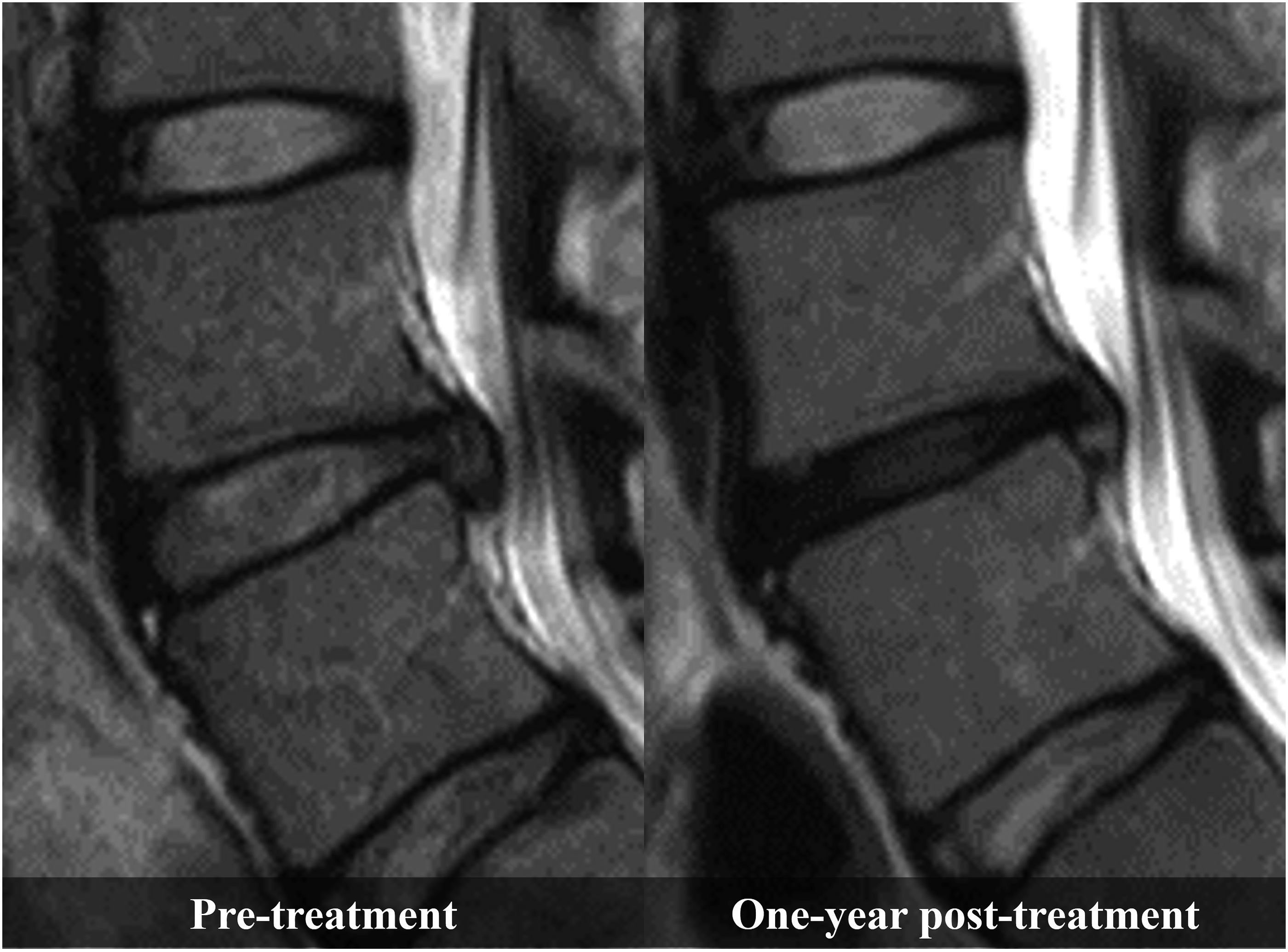
Additional Surgery and Safety
Comparison of Complications Between the Condoliase and Surgery Groups
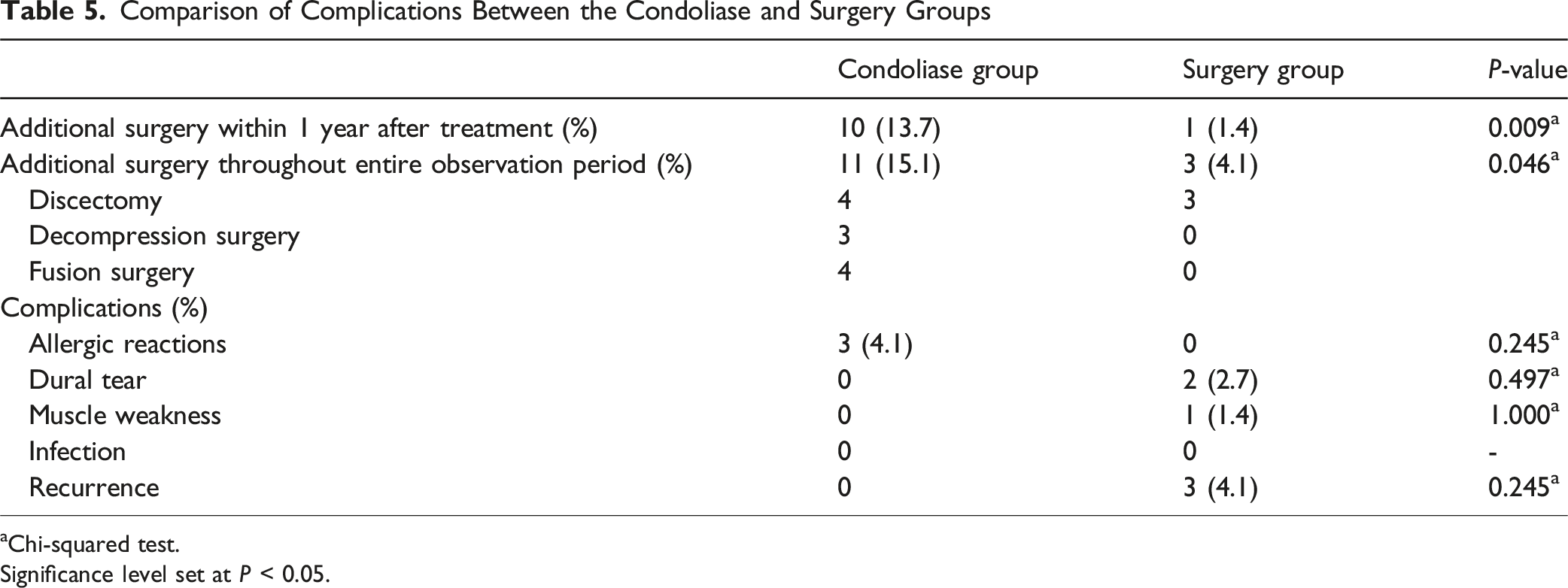
aChi-squared test.
Significance level set at P < 0.05.
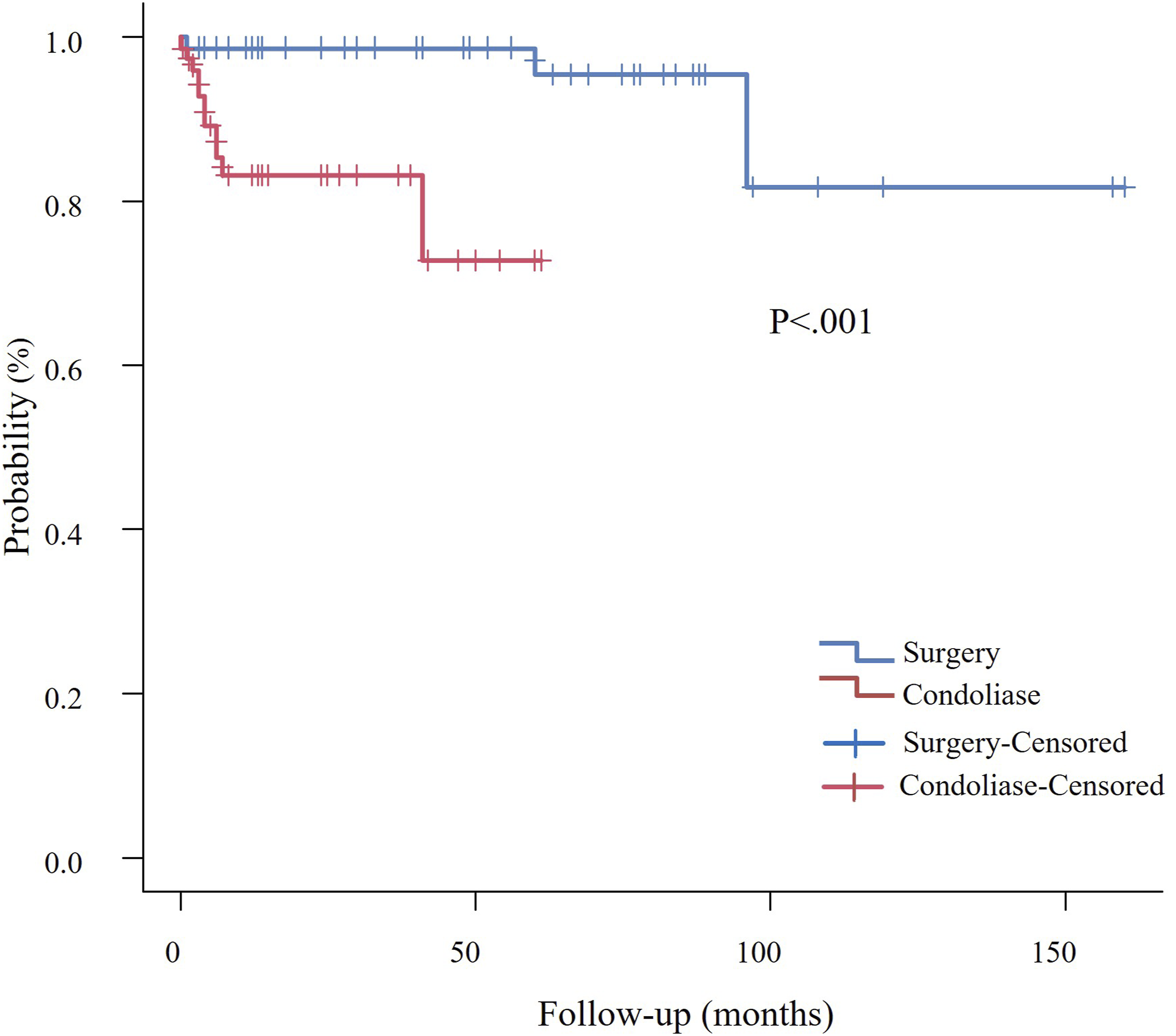
Kaplan–Meier Curves for Additional Surgery-free Survival. The Condoliase Group (Red Line) Exhibited a Higher Incidence of Additional Surgery, Particularly in the Early Period after Treatment, whereas Surgery Group (Blue Line) Demonstrated a Significantly Lower Incidence of Additional Surgery During the Follow-Up Period (Log-Rank Test, P < .001)
Discussion
In this retrospective cohort study, we used PSM to compare clinical outcomes of chemonucleolysis with condoliase and minimally invasive discectomy in patients with LDH. Surgery provided earlier pain relief and less disc degeneration 1 year after treatment than condoliase treatment. Additionally, condoliase treatment was identified as a risk factor for disc degeneration. Although no severe complications were observed with condoliase treatment, the need for additional surgery after treatment was significantly higher in the condoliase group than in the surgical group.
Previous studies have shown that >90% of patients with LDH who underwent surgical treatment experienced improvement in symptoms within a few months. 24 A systematic review and meta-analysis revealed that approximately 74% and 79% of patients reported pain improvement 3 and 12 months, respectively, after chemonucleolysis with condoliase. 25 Our results regarding improvements in leg pain after both treatments are consistent with those of previous reports. Few reports have compared timing of therapeutic effects between surgical and condoliase treatments. Although surgical treatment for LDH typically results in rapid improvement of pain symptoms,26,27 the onset of the therapeutic effects of condoliase treatment has been reported to occur within 3 to 6 months.28,29 In this study, a mixed-effects model showed that the improvement in leg pain VAS score after surgical treatment was significantly greater than that after condoliase treatment in the early phase. However, 3 months and 1 year after treatment, no significant differences were observed between the two treatments. A similar trend was observed for the JOA scores. Hence, although the therapeutic effect of condoliase appears to be more gradual than that of surgical treatment in the early post-treatment period, both treatments achieve comparable midterm outcomes. This difference is likely due to the following mechanism of action: Discectomy physically removes the herniation, providing immediate nerve decompression and rapid pain relief. In contrast, condoliase gradually degrades proteoglycans, reducing water content and shrinking herniation over time, leading to a delayed therapeutic effect.
The primary concern of condoliase treatment is its potential to accelerate disc degeneration. Although previous reports have suggested that condoliase treatment may lead to disc height reduction and accelerated disc degeneration, LDH can also contribute to disc degeneration. Therefore, evaluating the progression of disc degeneration solely within the condoliase group makes it difficult to precisely determine its impact. By comparing the condoliase and surgical groups, this study provides a relatively clear assessment of the effects of condoliase treatment. Previous studies have shown a 17.3% and 21.3% decrease in disc height at 52 weeks and 3 months, respectively, after condoliase injection.14,30 McGirt et al reported an 18% reduction in disc height at 3 months and 26% at 2 years after discectomy. 31 In this study, the reduction in disc height was 22.2% and 3.6% 1 year after condoliase treatment and minimally invasive discectomy, respectively. The rate of disc degeneration based on Pfirrmann grade progression after condoliase treatment has been reported to be 41.3% to 57.1%.14,19,32 In the present study, the rate of disc degeneration after condoliase treatment was 37.9%, which was significantly higher than that after surgical treatment. Furthermore, multivariable analysis demonstrated that condoliase treatment was significantly associated with grade progression according to the Pfirrmann classification, independent of other factors. In contrast to discectomy, which removes the herniated nucleus pulposus, condoliase treatment dissolves the entire nucleus pulposus of the intervertebral disc, which is thought to promote disc degeneration, leading to a reduction in disc height and progression of disc degeneration. In this study, significant disc degeneration progression was observed in the condoliase group. Meanwhile, there was no significant difference in JOA scores, which include the valuation of low back pain and disabilities due to the low back pain, at 1 year between the two groups, indicating no short-term functional decline. However, progressive disc degeneration may increase the risk of future low back pain and functional deterioration. Therefore, long-term follow-up is warranted to monitor potential late-onset symptoms associated with disc degeneration following condoliase treatment.
Schol et al reported an incidence of allergic reactions of 4.1% and surgical conversion rate of 13.4% after condoliase treatment. 10 In our study, these rates were 4.1% and 15.1%, respectively, which is consistent with previous findings. The observed rate of additional surgeries suggests that condoliase treatment may be insufficient in some cases, thus necessitating surgical intervention. Although the condoliase group had a shorter mean follow-up period, Kaplan–Meier analysis, accounting for differences in follow-up time, confirmed that the higher additional surgery rate in the condoliase group occurred mainly in the early postoperative period. Meanwhile, surgery itself has been reported to result in at least one unfavorable event, such as surgical complications, repeat surgery, or nonsurgical readmission, in 6.6% of patients, indicating that invasive treatment is not always the optimal choice for every patient. 8
Condoliase treatment offers significant advantages as a minimally invasive procedure that can be performed under local anesthesia in an outpatient setting. However, based on the current results, its early pain-relief effect is inferior to that of surgery, it may accelerate disc degeneration, and there remains a risk of requiring additional surgery. This information can be beneficial for both physicians and patients to understand the benefits and drawbacks of the new condoliase treatment for adequate treatment selection.
This study has some limitations. First, there was a selection bias in which patients with a longer disease duration, such as those with significant muscle weakness or bladder and bowel dysfunction, were likely to be selected for surgical treatment. Although PSM was performed to address background variability, residual bias cannot be fully eliminated. Particularly, PSM was performed using only age and sex, and the other important clinical variables such as baseline severity or symptom duration were not included. Therefore, residual confounding remains a potential limitation. Additionally, there was no standardized protocol for treatment decision-making. After condoliase became available, treatment decisions were made based on shared decision-making between the patient and the surgeon, potentially introducing additional selection bias. However, as both condoliase and surgery were fully covered by the national health insurance and equally accessible, insurance coverage or availability did not substantially influence the treatment choice. Second, this study had missing data, which may have introduced information bias. To mitigate this issue, we employed a mixed-effects model that allows for analysis despite missing values. However, complete correction of this bias could not be guaranteed. Third, the follow-up period was significantly shorter in the condoliase group than in the surgery group. In this study, adverse events, including additional surgery after treatment, were assessed only within 12 months after treatment; therefore, the risk of long-term complications or progressive degeneration may have been underestimated. Future prospective randomized controlled trials with extended follow-up periods are needed to evaluate long-term outcomes, including adjacent segment disease and delayed recurrence. Finally, the enrollment periods differed substantially between the two groups. This temporal imbalance may have introduced bias such as surgical techniques, perioperative management, and diagnostic practice.
Conclusion
Condoliase treatment tends to require more time for pain relief and may be associated with progression of disc degeneration. Nonetheless, it demonstrated midterm efficacy comparable to that of minimally invasive discectomy. Condoliase treatment, which can be administered under local anesthesia in an outpatient setting, may be a viable option for patients who do not wish to undergo surgery or have limited surgical tolerance. Spine physicians are expected to understand both the benefits and drawbacks of the new condoliase treatment.
Supplemental Material
Supplemental Material - Efficacy of Chemonucleolysis wWith Condoliase vVersus Minimally Invasive Discectomy for Lumbar Disc Herniation: A Propensity Score-mMatched Retrospective Cohort Study
Supplemental Material for Efficacy of Chemonucleolysis wWith Condoliase vVersus Minimally Invasive Discectomy for Lumbar Disc Herniation: A Propensity Score-mMatched Retrospective Cohort Study by Masato Uematsu, Koji Tamai, Minori Kato, Hiromitsu Toyoda, Akinobu Suzuki, Shinji Takahashi, Yuta Sawada, Masayoshi Iwamae, Yuki Okamura, Yuto Kobayashi, Hiroshi Taniwaki, Yuki Kinoshita, Hiroaki Nakamura, Hidetomi Terai in Global Spine Journal.
Footnotes
Informed Consent
All patients provided written informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Institutional Review Board Approval
This study was approved by the Institutional Review Board of Osaka Metropolitan University (approval number: 3170).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.