
Abstract
Study Design
Retrospective cohort study.
Objectives
To investigate the risk factors and clinical impact of progression of thoracic kyphosis (PTK) in who underwent lower thoracic fusion for lumbar flatback deformity (LFBD).
Methods
The study included 170 patients (mean age 70.2 years; 90.6% female) who underwent fusion from the lower thoracic spine (T9 or T10) for LFBD with a minimum follow-up of 2 years. PTK was defined as a final thoracic kyphosis (TK) ≥ 40° and ΔTK ≥10°. Multivariate logistic regression was performed to identify independent risk factors for PTK. Receiver operating characteristic (ROC) curve analysis was used to determine predictive cutoff values.
Results
PTK developed in 55 patients (32.4%) during a mean follow-up of 35.8 months. Patients with PTK exhibited significantly higher final TK (48.2° vs 27.3°), worse sagittal alignment, and lower clinical outcome scores compared to those without PTK. Multivariate analysis identified preoperative TK (odds ratio [OR] = 1.120, P = 0.007) and age (OR = 1.094; P = 0.041) as independent risk factors for PTK. ROC analysis determined a preoperative TK cutoff value of 10.0° (area under the curve [AUC] = 0.834) and an age cutoff of 69.5 years (AUC = 0.661).
Conclusions
In this study, PTK developed in 32.4% of patients following fusion to the lower thoracic spine for LFBD. Advanced age (>70 years) and high baseline TK (>10°) were significant risk factors for PTK. Extending fusion to a more cephalad thoracic spine should be considered for patients at high risk of PTK development.
Keywords
Introduction
Lumbar flatback deformity (LFBD), a subset of adult spinal deformity (ASD), is a debilitating condition commonly seen in the aging population, leading to stooped posture, back pain, and functional disability.1,2 Most LFBD cases result from multilevel disc degeneration and pathological loss of lordosis throughout the whole lumbar spine, making surgical correction often necessary with fusion down to the sacrum or pelvis as the lowest instrumented vertebra.3,4
The selection of the uppermost instrumented vertebra (UIV) is based on the regional thoracic kyphosis (TK) status above the planned UIV. In cases with pre-existing thoracic hyperkyphosis (eg, TK ≥40°), fusion to the upper thoracic spine (T2–T5, typically) should be considered. 5 However, in the absence of such a significant deformity in the thoracic spine, fusion may be terminated at the lower thoracic spine (T9 to T12), as it is generally advisable to avoid the normal apex of TK (T6–T8).6,7 Stopping at the lower thoracic spine offers several advantages over upper thoracic fusion, including shorter operation time, reduced blood loss, greater preservation of motion segments, and a lower risk of pseudoarthrosis.8-11
Despite these benefits, terminating fusion at the lower thoracic spine carries the risk of progression of thoracic kyphosis (PTK) developing in the unfused thoracic spine over time. The incidence of PTK has been reported to range from 41% to 53%, depending on the definitions used.12,13 Despite the high incidence of PTK documented in the literature and observed in clinical practice, its risk factors and clinical impact have not been thoroughly explored particularly in patients with LFBD.
This study aims to investigate the risk factors for PTK in LFBD patients undergoing fusion from the lower thoracic spine to the sacrum or pelvis. Additionally, the clinical impact of PTK was evaluated.
Materials and Methods
A retrospective study was conducted using a prospectively-collected ASD database from a tertiary referral hospital. The institutional review board approved this study and waived the need for informed consent due to its retrospective nature.
Study Population
The study cohort consisted of consecutive patients who underwent instrumented spinal fusion for symptomatic LFBD between 2012 and 2022. Inclusion criteria included LFBD defined as pelvic incidence (PI) – lumbar lordosis (LL) mismatch ≥20°; UIV at T9 or T10; LIV at sacrum or pelvis; and a minimum follow-up period of 2 years. Considering that the thoracolumbar junction (ie, T11 and T12 vertebrae) has distinct biomechanical characteristics compared to T9 and T10 vertebrae, particular regarding junctional complications,14,15 only patients with UIVs at T9 and T10 were included to minimize UIV-related bias. Pelvic fixation was routinely performed for patients undergoing naïve lumbosacral fusion using conventional iliac screws. However, pelvic fixation was not performed for patients with relatively mild deformities who had lumbosacral solid fusion due to prior surgery or lumbosacral transitional vertebra (ie, assimilation of L5 to sacrum). Three attending spine surgeons performed the surgery. Patients were excluded if they had non-degenerative conditions such as trauma, infection, or neuromuscular disorders; primarily coronal deformities without significant sagittal malalignment (eg, adult idiopathic scoliosis); baseline TK exceeding 40°; underwent revision surgery for reasons other than junctional complications (eg, pseudoarthrosis or infection); or had nonflexible thoracic spine, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis. PTK was defined as a final TK of ≥40° with an increase in TK of at least 10° from the preoperative value. PTK was further classified into proximal junctional kyphosis (PJK) (defined as proximal junctional angle [PJA] ≥ 20°) and non-PJK types (PJA <20°). 16 Presumed related factors were compared according to the development of PTK.
Presumed Risk Factors
Demographic data were collected on age, sex, body mass index (BMI), and bone mineral density (BMD). Surgical factors included approach (anteroposterior [A-P] combined approach vs posterior-only approach), transverse process (TP) hook fixation, pelvic fixation, UIV levels (T9 vs T10), and follow-up duration. Radiographic parameters, including PI-LL, sacral slope (SS), pelvic tilt (PT), TK, and sagittal vertical axis (SVA), were measured preoperatively, at 6 weeks postoperatively, and at the final follow-up. In patients who underwent revision surgery for PTK, final sagittal parameters were measured at the time of revision. Preoperative TK statuses were evaluated from multiple perspectives. First, TK was measured from T4 to T12 in a standing position, with positive values indicating kyphosis. Second, supine TK and its difference from standing TK [ΔTK (standing-supine)] was measured. 17 ΔTK (standing-supine) represents the flexibility and compensatory status of TK; a greater change indicates more flexibility, while negative values (standing TK < supine TK) represent good thoracic compensation. Thoracic compensation was also evaluated using the PI-based expected TK, calculated as PI minus 20° according to Protopsaltis et al. 13 A lower current TK value relative to the expected TK value [smaller ΔTK (current-expected)] indicated better thoracic compensation. Postoperative radiographic factors included only those directly modifiable during surgery and known to affect PJK development, such as age-adjusted PI-LL and T10-pelvic angle (T10PA).18,19 Since this study aimed to evaluate PTK risk factors for preoperative planning, postoperative sagittal parameters that were not directly controllable during surgery, including SS, PT, TK, and SVA, were excluded from the risk factor analysis. To evaluate the extent of correction, the offset between ideal age-adjusted PI-LL and current PI-LL was calculated using the equation: age-adjusted PI-LL = (age-55)/2 + 3. 20 A positive PI-LL offset value indicates a relative overcorrection. T10PA was measured as the angle between the line connecting the center of the T10 vertebral body to the hip center and the line connecting the hip center to the midpoint of the S1 upper endplate. Given that the ideal T10PA varies by age and PI, we used the age- and PI-adjusted ideal T10PA values reported in a previous study (Supplementary table 1). 21 Offsets between ideal and current T10PA were calculated, with a positive value indicating relative overcorrection.
Clinical Outcomes
Clinical outcomes were assessed at the final visit using the Scoliosis Research Society-22r (SRS-22r) questionnaire. The SRS-22r total score and minimal clinically important difference (MCID) were evaluated. 22 In cases of revision surgery for junctional complications, clinical outcomes were assessed at the time of revision.
Statistical Analysis
Descriptive statistics were used to present baseline characteristics with mean ± standard deviation for continuous variables and number (%) for categorical variables. A paired t-test was performed to compare preoperative and postoperative sagittal parameters. A repeated measures analysis of variance (ANOVA) evaluated changes in TK over time (preoperatively, postoperatively, and at final follow-up) and compared patterns between patients with and without PTK. Sagittal parameters and clinical outcomes at final follow-up were compared using independent t-tests or chi-square tests. Risk factor analysis for PTK was conducted through bivariate comparison of baseline and radiographic data between non-PTK and PTK groups using independent t-tests and chi-square tests. Pearson’s correlation analysis evaluated the relationship among age, preoperative PI-LL, and TK profiles, including standing TK, supine TK, ΔTK (standing-supine), and ΔTK (current-expected). Subsequently, univariate and multivariate logistic regression analyses were performed to identify the independent risk factors for PTK. The cutoff values for identified risk factors were determined using receiver operating characteristic (ROC) curve analysis. A subanalysis compared the preoperative variables and final outcomes according to preoperative TK-based groups. The odds of PTK according to TK groups was calculated using logistic regression analysis. All statistical analyses were performed by professional statisticians using Python version 3.10 (Python Software Foundation, Wilmington, DE, USA). A P-value of <0.05 was considered statistically significant.
Results
Baseline Characteristics
Baseline Characteristics

Bold P values indicate statistical significance.BMI, body mass index; BMD, bone mineral density; A-P, anteroposterior; TP, transverse process; UIV, uppermost instrumented vertebra; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis
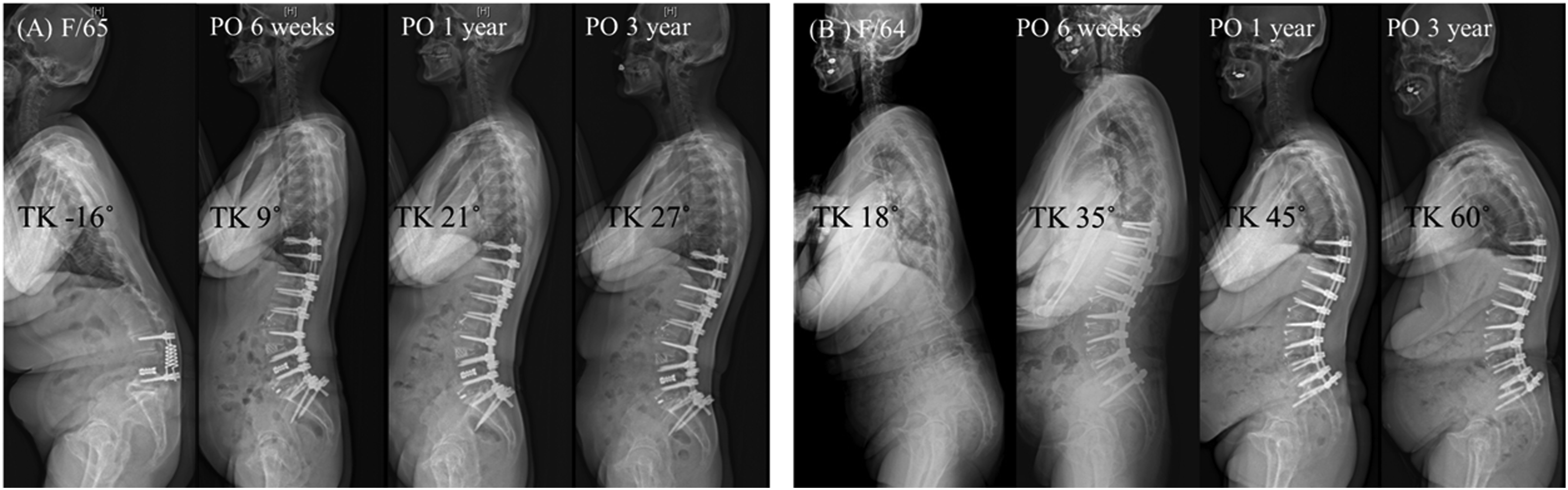
Case Examples Without Progression of Thoracic Kyphosis (PTK) (A) and With PTK (B). (A) Negative TK Value Indicates Thoracic Lordosis
Changes in TK according to PTK Occurrence
The final TK was 48.2° ± 7.2° in the PTK group and 27.3° ± 9.5° in the non-PTK group (P < 0.001) (Figure 2). Repeated measures ANOVA revealed significant TK changes across the 3 time points [F(2, df) = 486.0, P < 0.001]. The pattern of TK changes over time significantly differed between the groups [F(2, df) = 9.3, P < 0.001]; changes between the preoperative and postoperative periods were greater in the non-PTK group than in the PTK group (21.9° vs 16.7°, P = 0.008), while changes between postoperative period and final follow-up were lower in the non-PTK group than in the PTK group (6.4° vs 14.7°, P < 0.001). Changes in Thoracic Kyphosis (TK) Over Time in Patients With and Without Progression of Thoracic Kyphosis (PTK). Values are Expressed as Mean ± Standard Error. Significant Differences Between Groups at Each Time Point Were Observed. *** Indicates P < 0.001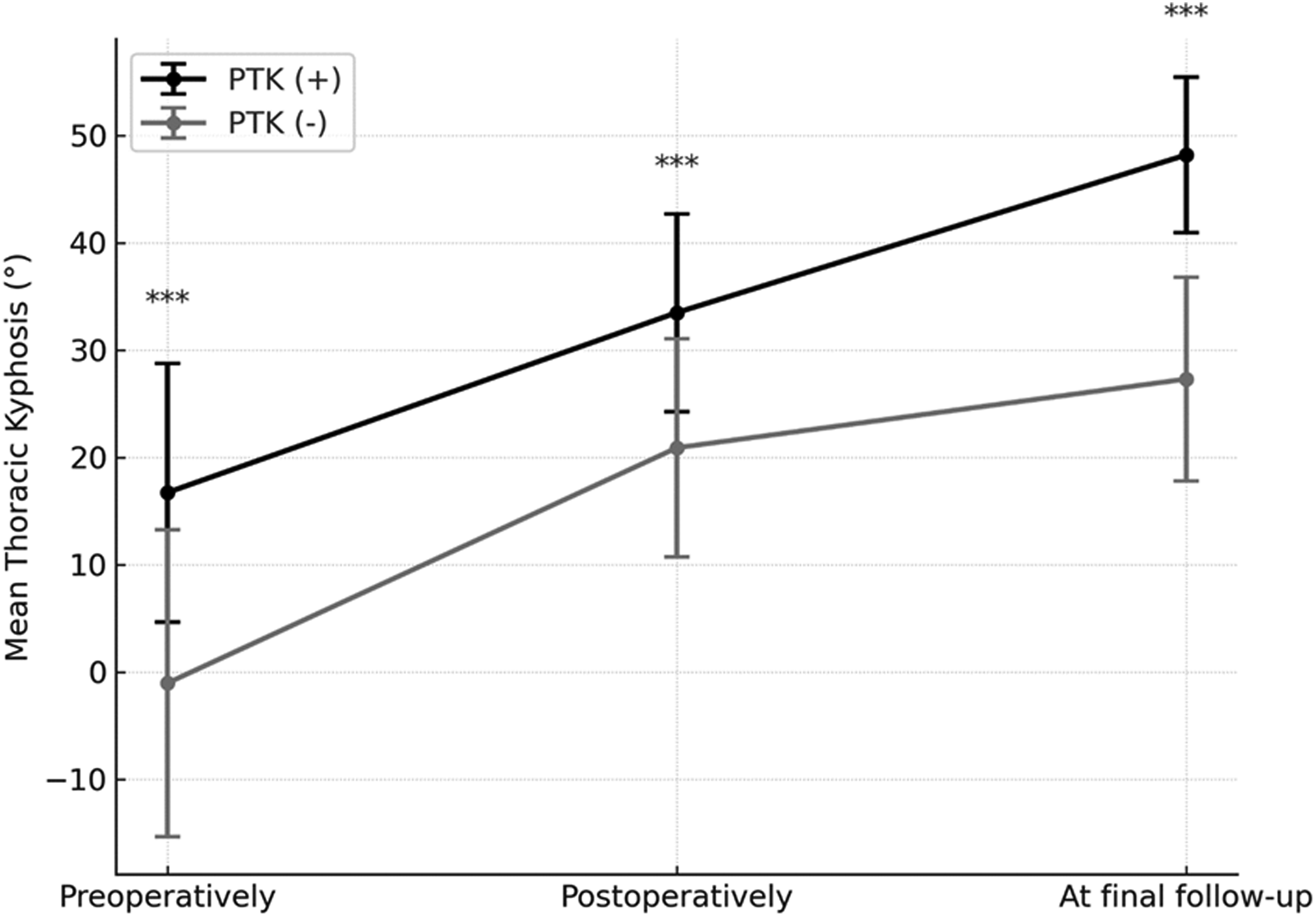
Clinical Consequences of PTK
Sagittal Parameters and Clinical Outcomes at the Final Follow-Up
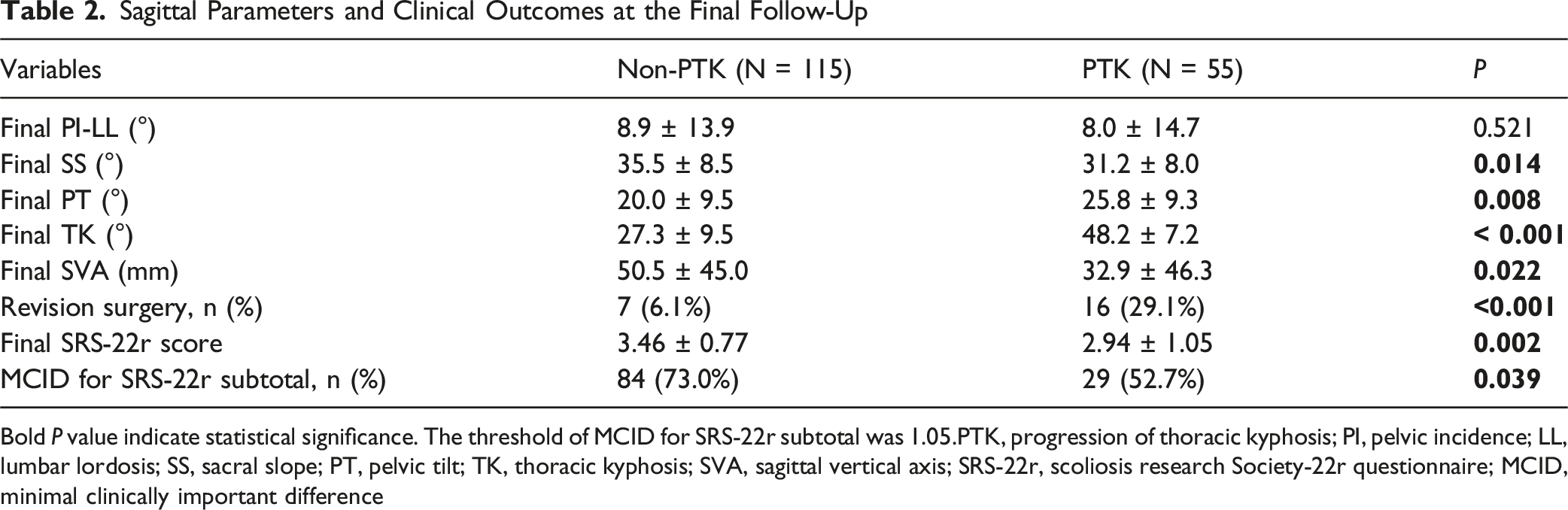
Bold P value indicate statistical significance. The threshold of MCID for SRS-22r subtotal was 1.05.PTK, progression of thoracic kyphosis; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; SRS-22r, scoliosis research Society-22r questionnaire; MCID, minimal clinically important difference
Risk Factor Analysis for PTK
Bivariate Comparison of Variables Between the Non-PTK and PTK Groups
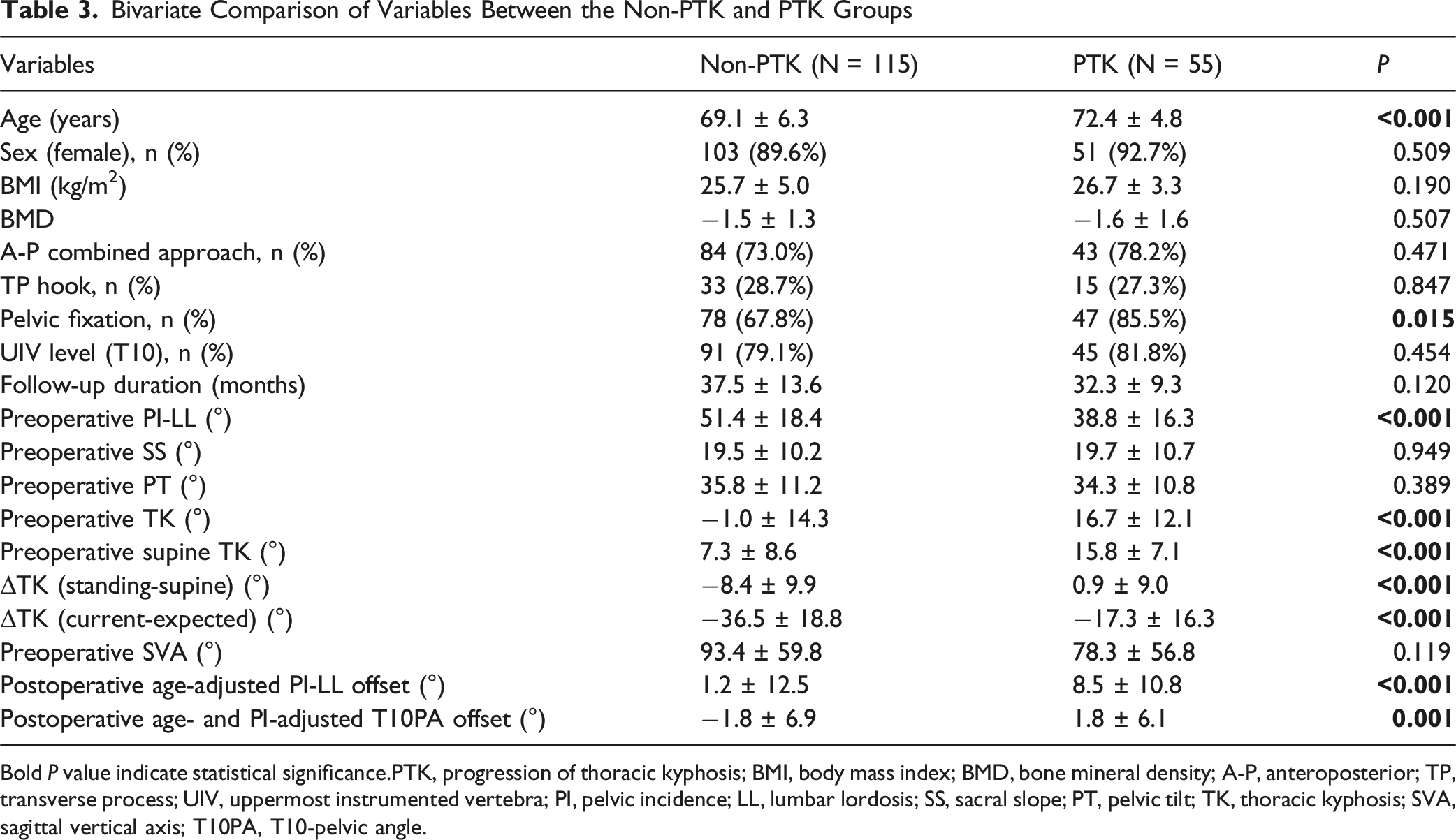
Bold P value indicate statistical significance.PTK, progression of thoracic kyphosis; BMI, body mass index; BMD, bone mineral density; A-P, anteroposterior; TP, transverse process; UIV, uppermost instrumented vertebra; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; T10PA, T10-pelvic angle.
Correlation Analysis Among Age, Preoperative PI-LL, and Preoperative TK-Related Parameters

*indicates P < 0.05 and ** indicates P < 0.01. PI, pelvic incidence; LL, lumbar lordosis; TK, thoracic kyphosis.
Univariate and Multivariate Logistic Regression Analyses to Identify the Risk Factors for PTK
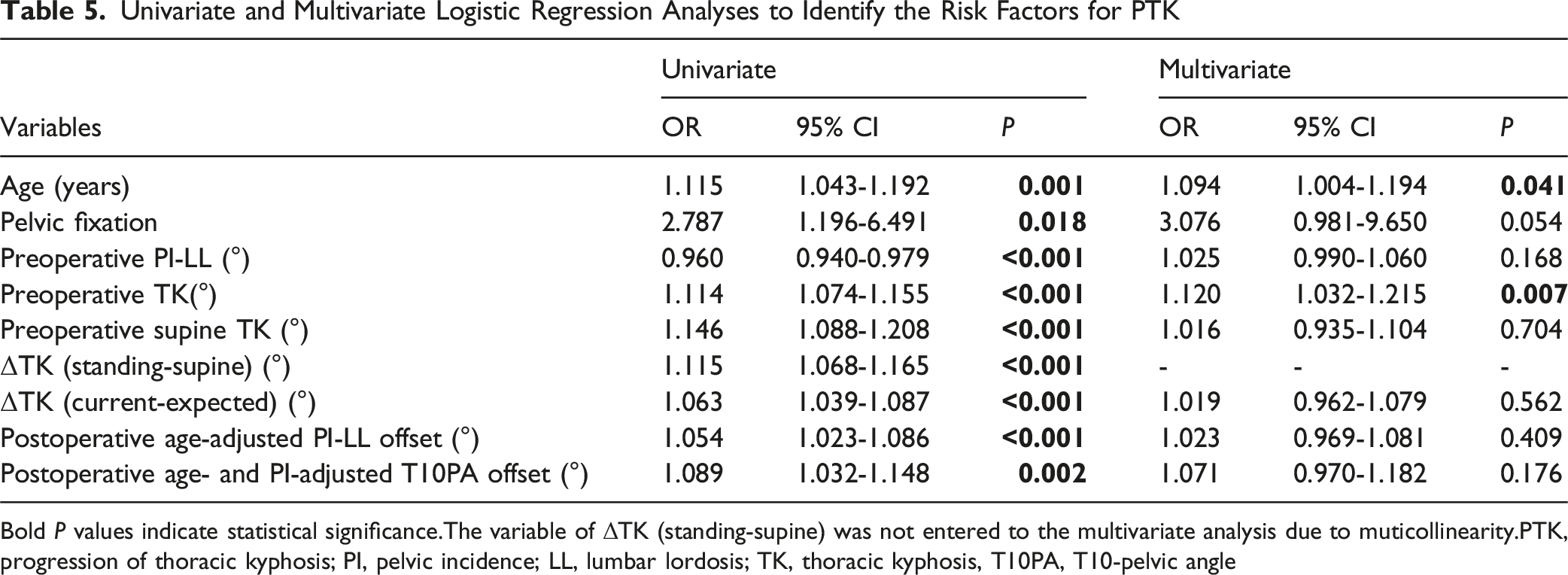
Bold P values indicate statistical significance.The variable of ΔTK (standing-supine) was not entered to the multivariate analysis due to muticollinearity.PTK, progression of thoracic kyphosis; PI, pelvic incidence; LL, lumbar lordosis; TK, thoracic kyphosis, T10PA, T10-pelvic angle
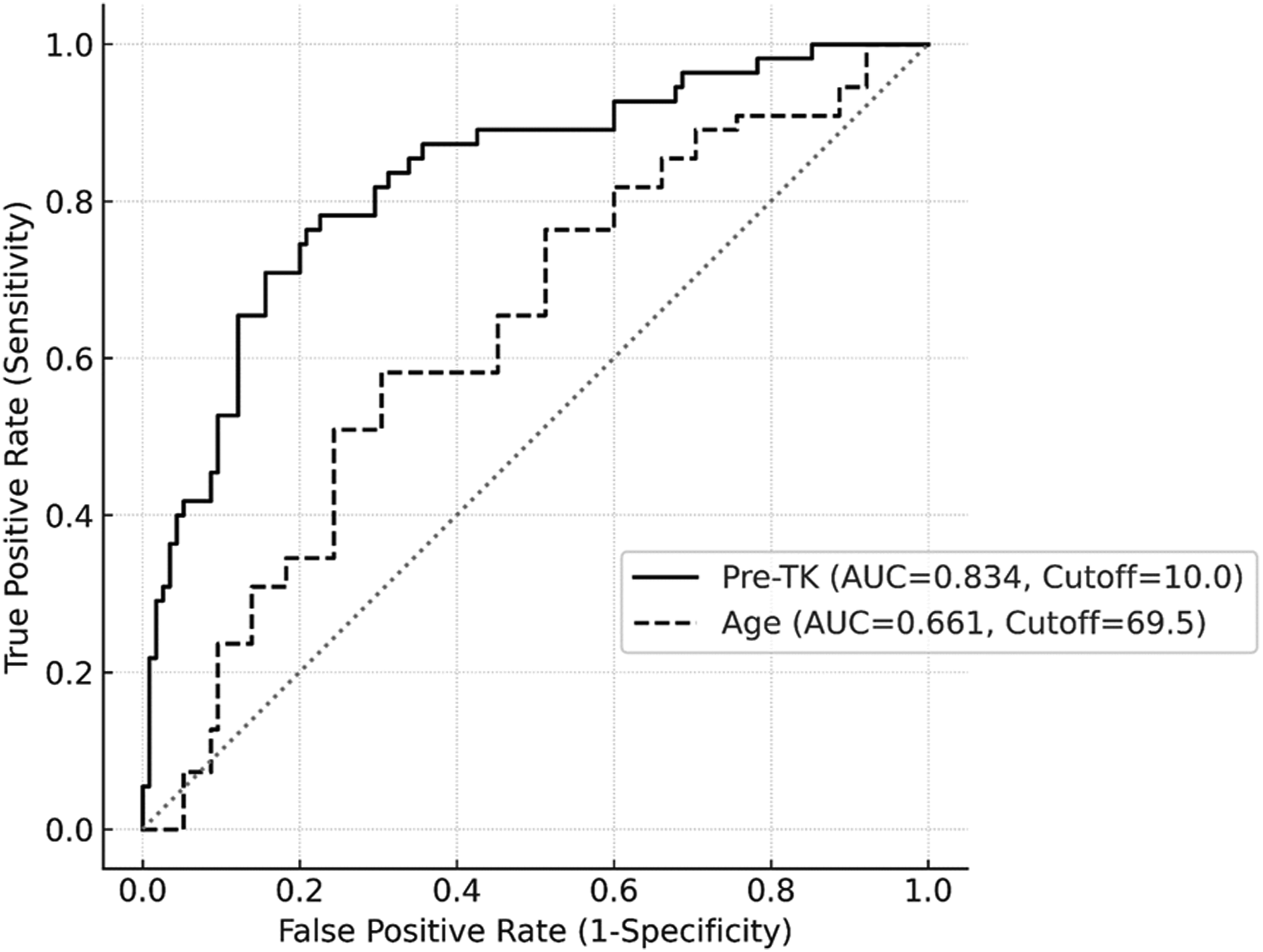
Receiver Operating Characteristic (ROC) Curve Analysis Showing the Cutoff Values for Preoperative TK (AUC = 0.834, 95% CI = 0.769 – 0.900, P < 0.001) and Age (AUC = 0.661, 95% CI = 0.574 – 0.747)
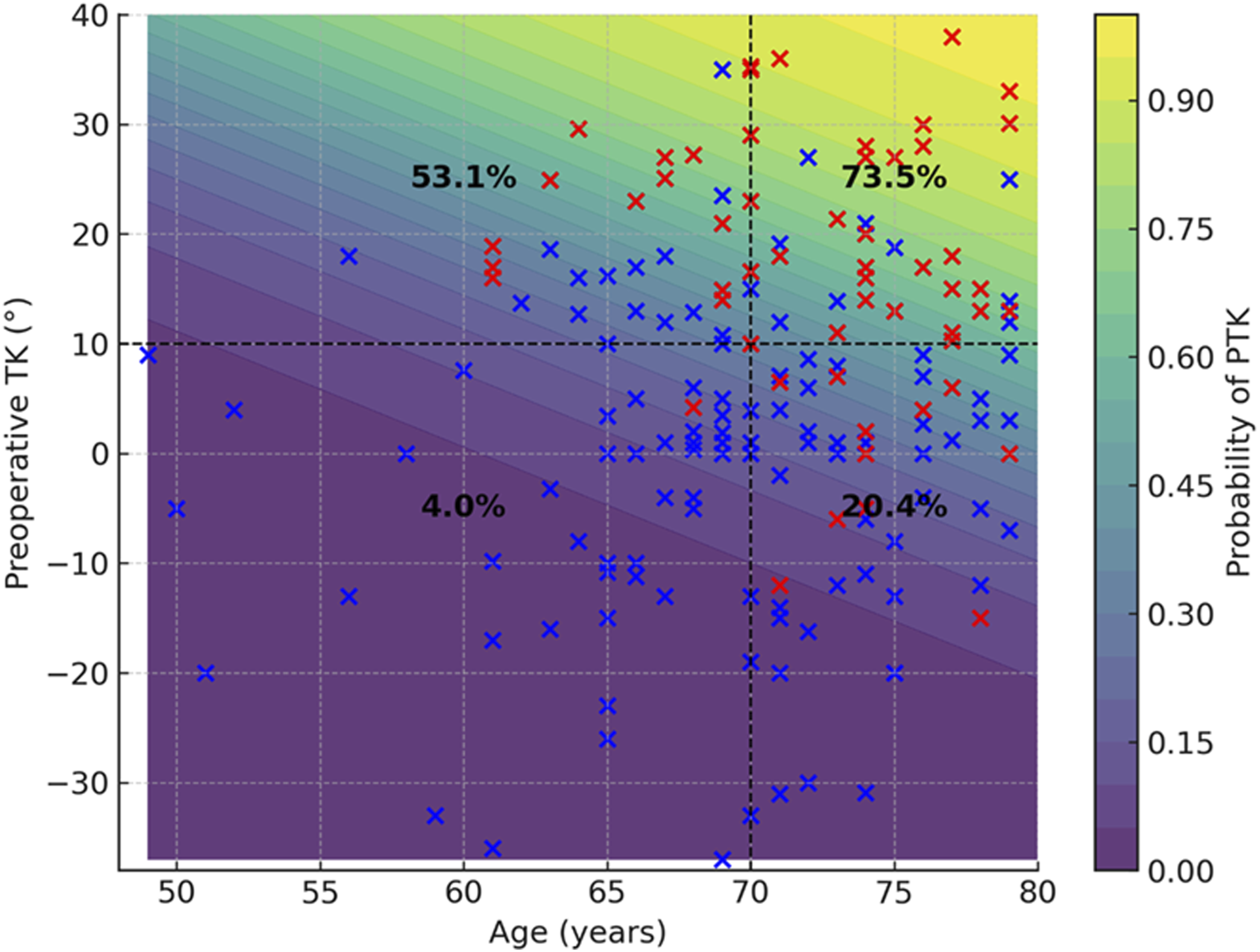
Contour Plot Depicting the Predicted Probability of Developing Progression of Thoracic Kyphosis (PTK) Based on Age and Preoperative Thoracic Kyphosis (TK). The Shaded Background Represents the Model-Predicted Probability of PTK, Ranging From 0% to 100%. Observed Data Points are Overlaid: Patients Without PTK are Shown as Blue Markers, while Those With PTK are Shown as Red Markers
Subanalysis According to Preoperative TK Groups
Subgroup Analysis According to Preoperative TK Groups
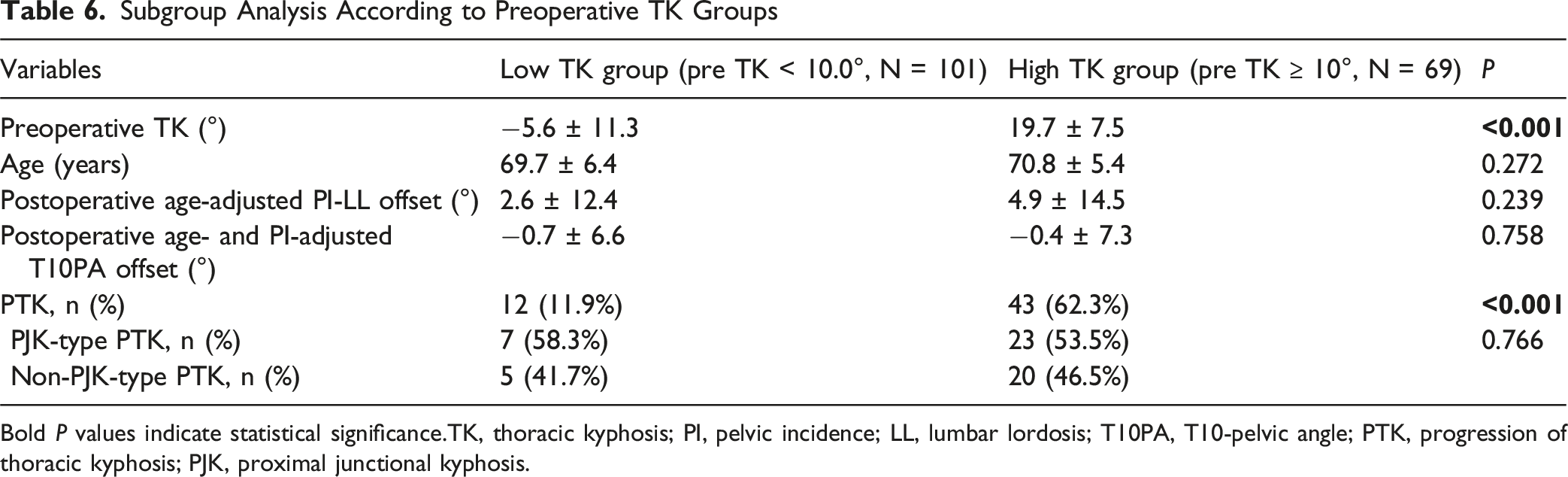
Bold P values indicate statistical significance.TK, thoracic kyphosis; PI, pelvic incidence; LL, lumbar lordosis; T10PA, T10-pelvic angle; PTK, progression of thoracic kyphosis; PJK, proximal junctional kyphosis.
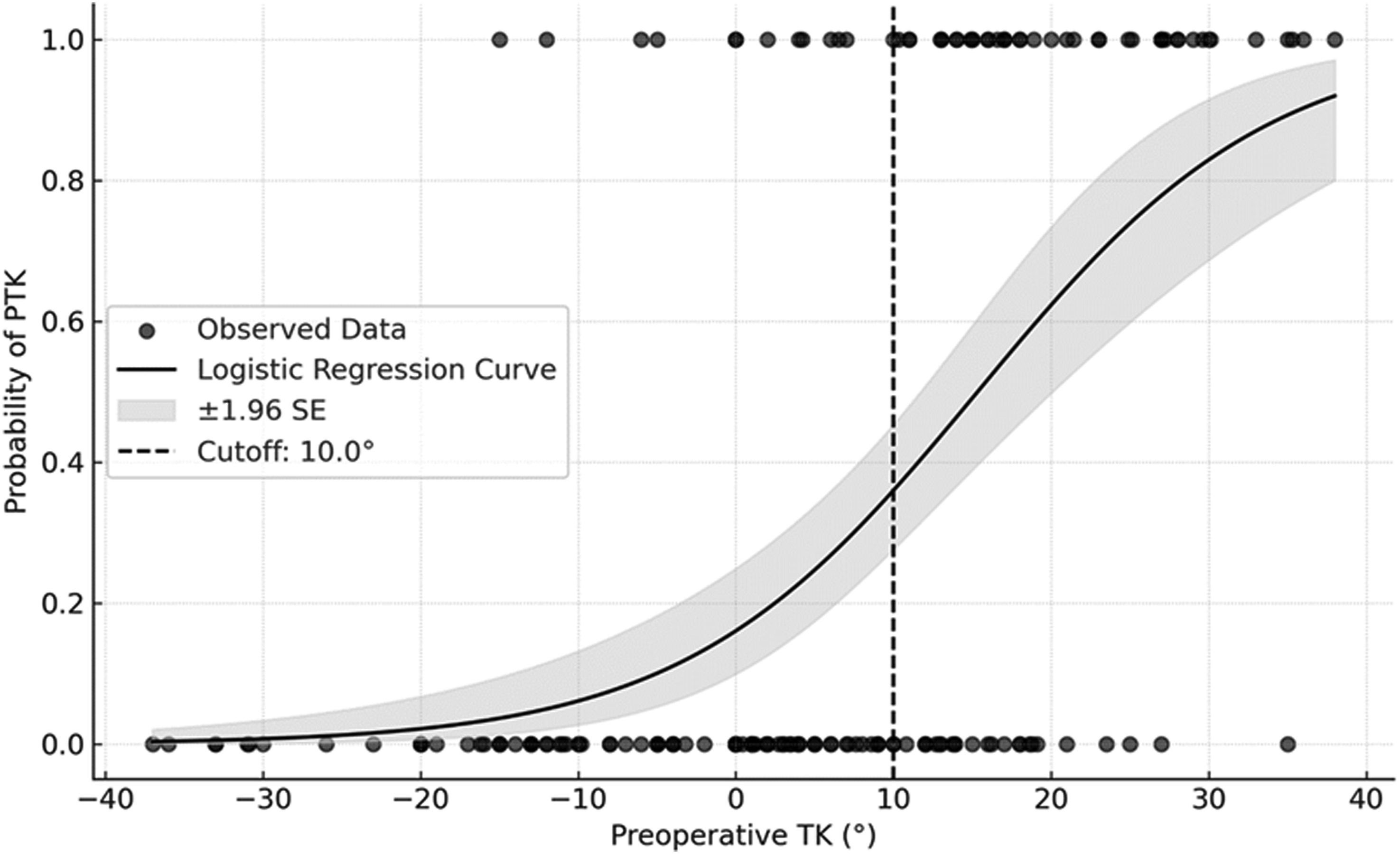
Logistic Regression Curve Illustrating the Relationship Between Preoperative Thoracic Kyphosis (TK) and the Probability of Developing Progression of Thoracic Kyphosis (PTK). The Solid Black Line Indicates the Predicted Probability, and the Shaded Area Represents the Standard Error (±1.96 SE). The Dashed Vertical Line Marks the Cutoff Value of 10.0°, Above which the Odds of PTK are Significantly Higher (Odds Ratio = 12.266, 95% CI = 5.652 – 26.620, P < 0.001)
Discussion
Selecting the appropriate UIV is 1 of the most critical decisions in ASD surgery. The primary factor to consider first when choosing the UIV is whether the thoracic spine has structural deformities such as hyperkyphosis. 5 In the absence of such deformities, fusion often terminates at the lower thoracic spine for long thoracolumbar constructs in ASD surgery. Among the lower thoracic vertebrae, T9 or T10 are commonly selected since they are anchored by true ribs, providing greater stability and potentially reducing the risk of junctional complications compared to T111 or T12. 15 Studies on UIV selection (eg, upper vs lower thoracic spine) have primarily focused on the development of PJK.5,9,16,23,24 While the occurrence of PJK is an important consideration in ASD surgery, there is still a lack of comprehensive investigations into the global progression of TK (referred to as PTK in this study), particularly in cases where fusion ends at lower thoracic levels. PTK can occur alongside PJK, but it can also present as a generalized increase in TK throughout unfused segments, significantly impacting global sagittal balance and clinical outcomes. In Yagi’s study of lumbar degenerative scoliosis patients, those who developed >10° TK progression had a larger forward offset (mean SVA, 4.7 cm) compared to those without progression (mean SVA, 1.5 cm). Lafage et al found that patients with normal TK preoperatively who deteriorated to hyper TK postoperatively had a significantly lower satisfaction rate (59.6% vs 77.3%). 25 Consistent with previous studies, we found that the development of PTK was associated with worsening sagittal parameters at the final follow-up, and an increased risk of revision surgery, and poorer clinical outcomes (Table 2). Given the adverse radiographic and clinical consequences of PTK, recognizing its risk factors is essential to ensure optimal clinical outcomes. Furthermore, these findings may guide UIV level selection; for patients at high risk for PTK, extending fusion to a more cephalad thoracic spine should be carefully considered.
Not all cases of postoperative increases in TK should be considered pathological. Patients with LFBD often decreases their TK as a compensatory effort, resulting in a physiological increase in TK following LL restoration. In this study, there was a significant increase in TK of 21.3° postoperatively (from 4.7° to 25.0°). This immediate TK increase is slightly greater than previous literature, which reported TK increases of 12°–18° depending on the study population.25-28 This may be due to the current study including only LFBD patients who exhibited decreased TK preoperatively; patients with thoracic hypokyphosis preoperatively (often resulting from long-standing compensatory flattening due to lumbar deformity) have more “room” to increase their kyphosis after surgery. Unlike this physiological TK increase, a progressive increase in TK over time beyond a certain threshold may indicate a pathological process and become clinically problematic, as shown in previous results. In this study, PTK developed in 32.4% of patients (55 of 170). Although TK values were significantly higher in the PTK group compared to the non-PTK group at all measured time points, the magnitude of the immediate postoperative TK increase (ie, reciprocal TK increase) was paradoxically greater in the non-PTK group than in the PTK group (Figure 2). This observation suggests that the smaller the preoperative TK, the larger the reciprocal change immediately after surgery, consistent with findings from previous studies. Yasuda et al. reported a negative correlation between postoperative changes in TK and preoperative TK magnitude. 28 Protopsaltis et al. also found that preoperative TK was significantly smaller in the reciprocal change group (defined as TK increase ≥15°) compared to the non-reciprocal change group. 13
Prior literature demonstrated that several factors influenced the development of PTK, including age, extent of lumbar correction, UIV stopping at thoracolumbar junction, and sacropelvic fixation.12,15,25,29 Consistent with previous studies, bivariate analysis in the current study confirmed that these factors affected the occurrence of PTK (Table 3). However, in the multivariate analysis, only advanced age (>70 years) and high preoperative TK (>10°) emerged as significant risk factors for PTK. The association between advanced age and PTK occurrence is expected, as it has been reported in several previous studies.12,13,28 This relationship may be due to lower musculature in the thoracic area or decreased compensatory ability (ie, thoracic hypokyphosis). 30 However, in the present study, we found that age was not strongly correlated with ΔTK (standing-supine) and ΔTK (current-expected), which represent the extent of thoracic compensation (Table 4). This indicates that advanced age itself does not compromise thoracic compensation. Unlike age, thoracic compensation was significantly correlated with preoperative PI-LL; the greater the preoperative PI-LL mismatch, the smaller the ΔTK (standing-supine) and ΔTK (current-expected) values.
Preoperative TK, particularly greater than 10°, was the strongest risk factor for PTK development; patients with TK ≥10° had a 12.27-fold increased odds of PTK compared to those with TK <10° (Figure 5). The mean preoperative TK was 4.7° for total study cohort, which is generally lower than previous reports.12,13,17,25-27 This may be due to the inclusion of only patients with LFBD, who are expected to exhibit varying degrees of thoracic compensation. We found that the non-PTK group had a lower preoperative TK than in the PTK group (−1.0 vs 16.7°, P < 0.001), indicating that the development of PTK is significantly affected by preoperative thoracic compensation status. Notably, patients with severe preoperative sagittal deformity were less likely to develop PTK; preoperative PI-LL was significantly greater in the non-PTK group than in the PTK group in the bivariate analysis (51.4° vs 38.8°, P < 0.001) (Table 3). This could be because increased lumbar deformity (ie, high PI-LL mismatch) is associated with a decrease in TK (ie, increased thoracic compensation), as confirmed by negative correlation between preoperative TK PI-LL mismatch (correlation coefficient of −0.635) (Table 4). We also observed that the values of ΔTK (standing-supine) and ΔTK (current-expected), both representing thoracic compensation extent, were significantly smaller in the non-PTK group than in the PTK group in bivariate comparison (Table 3). Although these parameters were not significant in multivariate analysis, they were strongly correlated with preoperative TK in Pearson’s correlation test (r = 0.842 and 0.847, respectively) (Table 4). Therefore, preoperative TK alone may serve as a sufficient indicator for assessing thoracic compensation in the context of PTK development. The ΔTK (standing-supine) value also represents thoracic flexibility. Ohba et al. reported that the cutoff for ΔTK (standing-supine) to increase the risk of PJK was 18.5°. 17 However, in our study, ΔTK (standing-supine) was 0.9° in the PTK group and −8.4° in the non-PTK group, with an expected cutoff of ΔTK (standing-supine) between −8.4° and 0.9°, which is lower than Ohba’s cutoff value. These results suggest that preventing PTK may require stricter thresholds for TK or TK flexibility than previously reported when treating patients with LFBD.
Limitation
This study has limitations. First, although prospectively collected data were used, the retrospective nature of this single-institution study may have introduced selection and recall bias. Additionally, surgical planning may vary based on the surgeon’s experience, particularly in selecting the UIV levels. However, by excluding cases with preoperative TK ≥40° and limiting the UIV to T9 and T10, we believe that this UIV-related bias can be minimized. Second, the strict inclusion criteria (eg, only LFBD, defined as PI-LL ≥20°) may limit the generalizability of our findings across the spectrum of ASD. Third, muscle function can influence thoracic compensation and subsequent PTK development.31,32 Although this study did not quantitatively evaluate musculature (eg, muscle volume or fatty degeneration) in the thoracic area, we think that the preoperative TK value adequately reflects the real capacity for thoracic compensation. Lastly, while we suggested extending the fusion to the upper thoracic spine for patients at high risk of PTK development, the decision to extend to the upper thoracic spine may depend on other various factors, including patient condition, bone quality, deformity types, adjacent segment disc degeneration, and surgeon preferences.
Conclusions
In this study, PTK developed in 32.4% of patients following fusion to the lower thoracic spine for LFBD. PTK occurrence was associated with worse radiographic and clinical outcomes at the final follow-up. Advanced age (>70 years) and high baseline TK (>10°) were significant risk factors for PTK. Extending fusion to a more cephalad thoracic spine should be considered for patients at high risk of PTK development.
Supplemental material
Supplemental material - Progression of Thoracic Kyphosis After Lower Thoracic Fusion in Lumbar Flatback Deformity: Analysis of Risk Factors and Clinical Consequences
Supplemental material for Progression of Thoracic Kyphosis After Lower ThoracicFusion in Lumbar Flatback Deformity: Analysis of RiskFactors and Clinical Consequences by Se-Jun Park, Jin-Sung Park, Dong-Ho Kang, Chong-Suh Lee in Global Spine Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Number
SMC 2024-07-144
Data Availability Statement
The data cannot be used publically, but can be presented in case of reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.