
Abstract
Study Design
Retrospective cohort study.
Objective
To quantify and compare the carbon footprint (CF) of open and MIS microdiscectomy.
Methods
The study included 161 patients undergoing primary 1 level open or minimally invasive surgery (MIS) for lumbar disc herniation between 2018 and 2022. Life cycle assessment (LCA) modeling was used to calculate the CF produced during the distribution, use and waste phases of each item used during surgery. Independent samples t-tests and Chi square or Fischer’s exact tests were used to compare the CF of open and MIS procedures.
Results
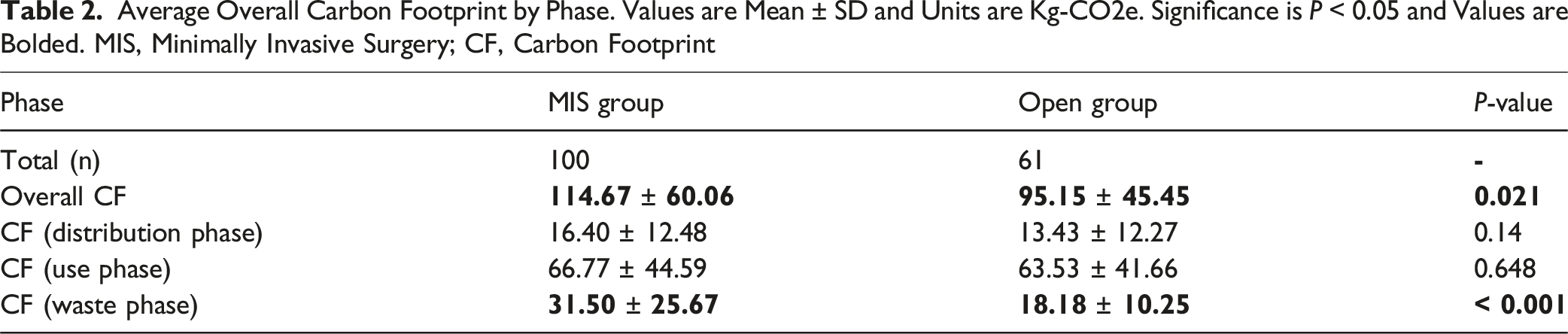
There were 161 cases (100 MIS, 61 Open). MIS had a significantly higher overall CF (114.67 ± 60.06 kg-CO2e) vs open surgery (95.15 ± 45.45 kg-CO2e, P = 0.021). Key contributors included disposable surgical supplies, energy-intensive OR equipment, and anesthetic gases. Only the waste phase had a significant difference in CF, with MIS producing more waste (MIS: 31.50 ± 25.67; Open: 18.18 ± 10.25; kg-CO2e; P < 0.001) and consuming more energy, especially for heating, ventilation, and air conditioning systems and fluoroscopy.
Conclusions
MIS microdiscectomy results in higher CF and environmental costs compared to open procedures, highlighting the need for sustainable practices, especially waste reduction, use of reusable materials and optimized energy use in ORs. A multifaceted approach is crucial to mitigate the environmental impact of spine surgeries and should be applied to both MIS and open techniques.
Keywords
Introduction
The significant amount of greenhouse gas (GHG) emissions produced by healthcare activities in the United States has become a growing concern, impacting both the environment and public health.1-3 A recent study found that a hospital in Brookyln, NY, produced an estimated 656 000 kg of carbon dioxide equivalents per year (kg-CO2e/year) for acute care and 349 000 kg-CO2e/year for intensive care. 4 Operating rooms (ORs) are recognized as the most resource-intensive areas within hospitals, consuming 3 to six times more energy than other departments and generating roughly 21%–30% of hospital waste. 3 Additionally, with expanding use of new surgical instruments, devices, and technologies, OR energy use continues to increase. High energy consumption is exacerbated by the indirect emissions arising from the supply chain that produces, transports, and disposes of healthcare materials and services including single-use instruments and anesthetic gases, which are potent GHGs.5,6 Therefore, surgical procedures, including spine surgery, contribute significantly to the overall carbon footprint (CF) and GHG emissions of the healthcare industry.
Previous studies have explored the environmental impact of surgery across surgical field and orthopedic subspecialties, however few focused on spine surgery.7-13 A CF analysis of urologic surgery found that transurethral resection of bladder tumors produced 131.8 kg-CO2e. 13 In orthopedics, knee arthroplasty produces between 87.2 kg-CO2e (primary) and 125.9 kg-CO2e (revision). 12 One study discussing the CF of spine surgery showed that adult spinal deformity (ASD) surgery produces roughly 147.7 kg-CO2e per procedure. 14 To address the lack of spine surgery CF data, this study aims to determine the CF of microdiscectomy surgery, comparing traditional open and minimally invasive surgery (MIS) techniques.
Methods
Patient Selection
Data for this study was obtained from an institutional review board-approved surgical patient database at a single urban academic hospital to identify patients over the age of 18 who underwent 1 level primary open or minimally invasive (MI) microdiscectomy for lumbar disc herniation between 2018 to 2022. MIS utilized tubular retractors and a microscope, whereas open surgery utilized larger incisions with muscle and soft tissue retractors to obtain direct visualization of the spine.
Defining and Calculating the Carbon Footprint
To perform our CF analysis, we followed the methodology described by Nakarai et al,
14
which utilized the International Organization for Standardization (ISO)-14040 standard, used for life cycle assessment (LCA). The functional unit was a single microdiscectomy surgery.
15
The LCA system boundary included the CF produced by 3 phases (Figure 1): distribution, utilization, and end-of-life (waste). This exclused the CF produced from the disposal (waste) of implants, bone graft products, and non-gas intravenous medications as they remain inside or are metabolized by the patient’s body, as well as the manufacturing phase due to a lack of available information. CF was evaluated using carbon dioxide equivalents (CO2e) which are relative to the amount of CO2 with an equivalent global warming potential. CF was calculated using the Ecoinvent 3.9.1 database (ecoinvent, Zurich, Switzerland) and Umberto ver. 11.9.2 (iPoint, Reutlingen, Germany) LCA modeling software. System boundary (Double red line) defining inclusion criteria for LCA.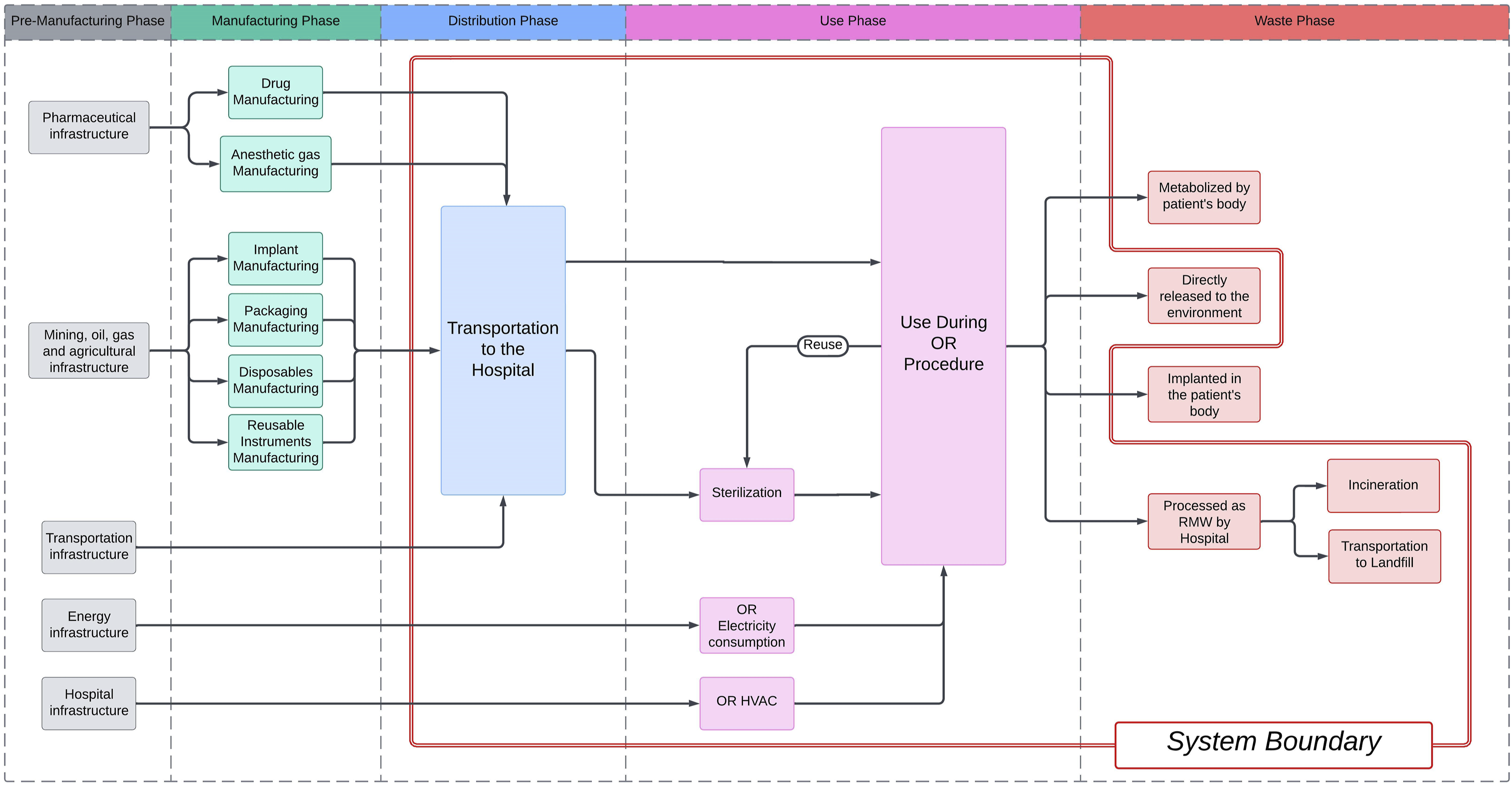
Single-Use Disposable Items, Reusable Instruments, and Medications
Medical records provided procedure length and a list of all disposable and reusable items, instruments, snd gaseous medications utilized per surgery. Each item and their packaging were weighed and recorded. We followed the methods described by Nakarai et al 14 for calculating the distance between the manufacturing site and our institution utilizing Google Maps (Alphabet Inc, Mountain View, CA, USA) to assess the CF generated during the distribution phase of each product and loaned instrument.14,16 Similarly, we simplified our transportation methods depending on whether products were manufactured within or outside of the US and Canada. Reusable equipment lifespan was assumed as 300 uses, and the CF produced by each phase was distributed across their life cycle to determine the CF per procedure.14,16
Gaseous medications are minimally metabolized by the body during inhalation and are then expelled during exhalation.6,14,15,17 For simplicity, we assume that the amount of gas inhaled is equal to the amount released into the environment.
17
CO2e was calculated by obtaining medical record data regarding anesthetic gas, liquid oxygen, and compressed medical air use and by using the following formula6,18:

The 100-year global warming potential (GWP100) value serves as a conversion unit for each agent compared to CO2, indicating the effectiveness of each gas in capturing heat in the Earth’s atmosphere over a century. Energy requirements for liquid oxygen (0.001 kWh/l) and compressed medical air (0.0003 kWh/l) were used to calculate the CF respectively for anesthesia.14,15,19 Amounts of non-gaseous medications used during the procedure were collected. Excess medication was weighed and added to waste phase calculations.
All waste from the operating room (OR) was categorized as regulated medical waste by New York state guidelines. 20 Disposing 1 kg of RMW is estimated to produce 1.1 kg of CO2e. 21
Energy Consumption
Energy consumption was calculated for heating, ventilation, and air conditioning (HVAC) (0.25 kWh/hour/m2), lighting (0.329 kWh/hour), patient air warmer (0.8 kWh/hour), anesthesia machine (0.08 kWh/hour), and fluoroscopy.14,15,19,22,23
Steam sterilization electricity use was calculated using the equation:

Statistical Analyses
Student t-tests (equal variances) or Welch’s t-test (unequal variances) (continuous variables) and Chi square or Fischer’s exact tests (categorical variables) were used. Statistical analysis was performed using IBM SPSS v29 Significance was determined at P < 0.05.
Results
Patient Characteristics and Surgical Factors
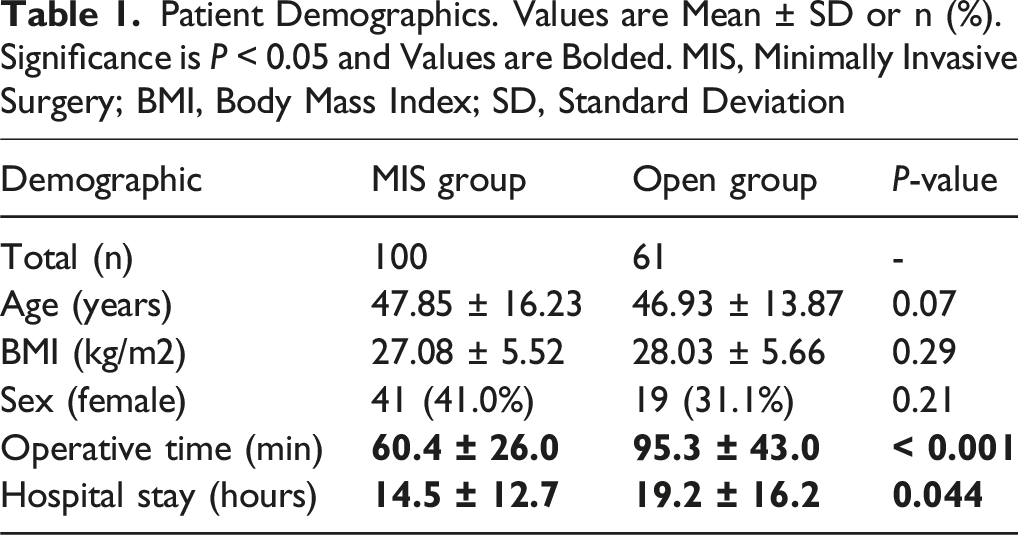
Patient Demographics. Values are Mean ± SD or n (%). Significance is P < 0.05 and Values are Bolded. MIS, Minimally Invasive Surgery; BMI, Body Mass Index; SD, Standard Deviation
Overall CF Produced
Average Overall Carbon Footprint by Phase. Values are Mean ± SD and Units are Kg-CO2e. Significance is P < 0.05 and Values are Bolded. MIS, Minimally Invasive Surgery; CF, Carbon Footprint
CF Produced in the Distribution Phase
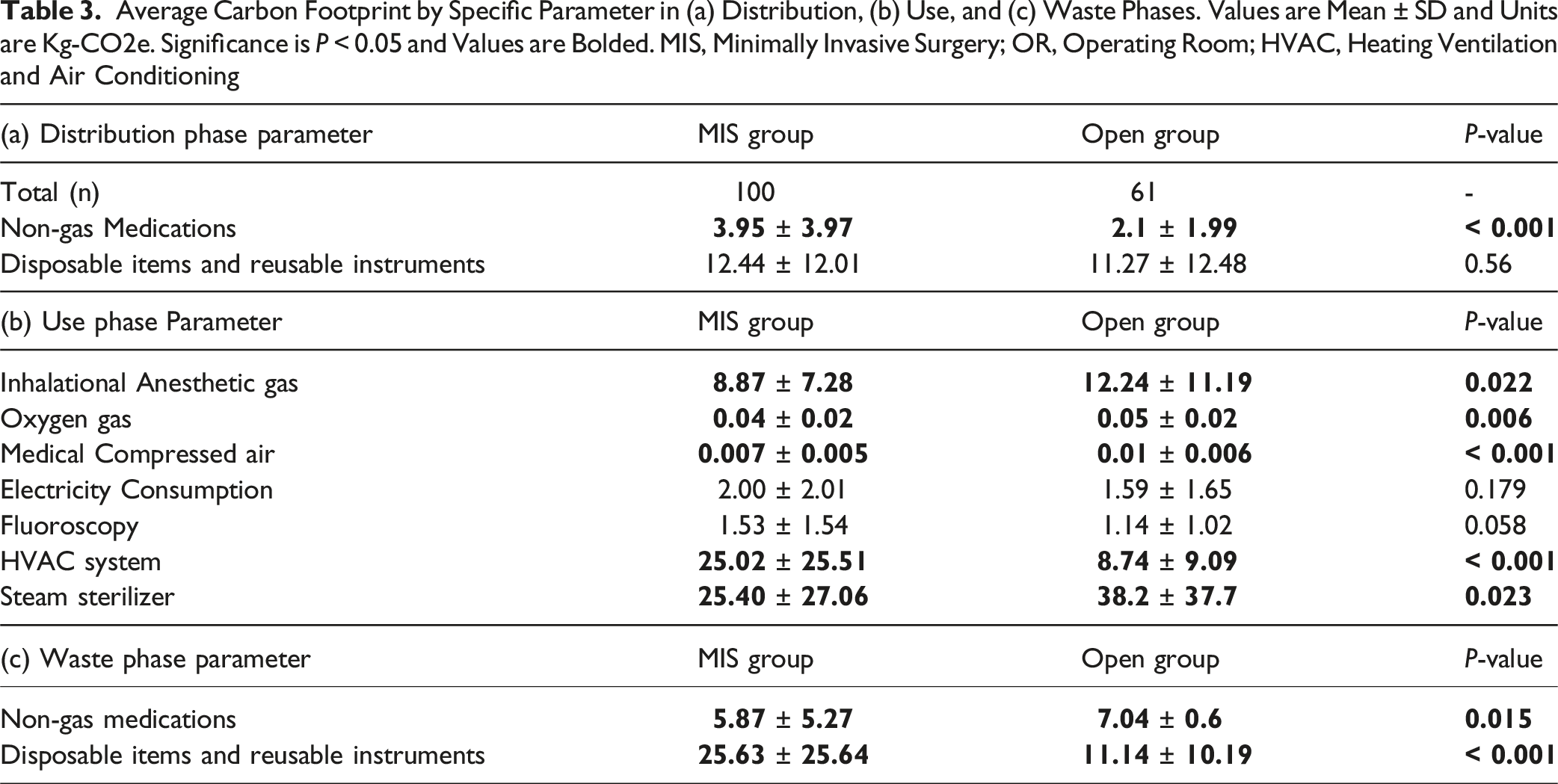
Average Carbon Footprint by Specific Parameter in (a) Distribution, (b) Use, and (c) Waste Phases. Values are Mean ± SD and Units are Kg-CO2e. Significance is P < 0.05 and Values are Bolded. MIS, Minimally Invasive Surgery; OR, Operating Room; HVAC, Heating Ventilation and Air Conditioning
CF Produced in the Use Phase
The use phase contributed to the largest portion of the overall CF for MIS (58.2%) and open surgery (66.8%). (Table 2). Among the key contributors, inhalational anesthetic gases generated significantly more to the CF in open surgery (12.24 ± 11.19 kg-CO2e) compared to MIS (8.87 ± 7.28 kg-CO2e, P = 0.02). Oxygen gas usage (0.05 ± 0.02, Open vs 0.04 ± 0.2, MIS kg-CO2e, P = 0.006) and medical compressed air (0.01 ± 0.006, Open vs 0.007 ± 0.005, MIS kg-CO2e, P < 0.001) also contributed more to the CF in open surgery (Table 3b).
Electricity consumption in the OR was slightly higher for MIS (2.00 ± 2.01 vs 1.59 ± 1.65 kg-CO2e, P = 0.179), as was the CF from fluoroscopy use (1.53 ± 1.54 vs 1.14 ± 1.02 kg-CO2e, P = 0.058) (Table 3b).
The HVAC system in the OR also produced a higher CF for MIS compared to open surgery (25.02 ± 25.51 vs 8.74 ± 9.09 kg-CO2e, P < 0.001). The CF from the steam sterilizer was significantly higher in the open surgery group (38.2 ± 37.7 vs 25.40 ± 27.06 kg-CO2e, P = 0.023) (Table 3b).
CF Produced in the Waste Phase
The CF during the waste phase was significantly higher for the MIS group compared to the open group (31.50 ± 25.67 vs 18.18 ± 10.25 kg-CO2e, P < 0.001) (Table 3c). This phase contributed to 27.5% and 19.1% of the CF for MIS and open surgery, respectively. Among specific contributors, the CF associated with non-gas medications was significantly higher in the open group (7.04 ± 0.60 vs 5.87 ± 5.27 kg-CO2e, P = 0.015). On the other hand, the CF related to disposable items and reusable instruments was significantly higher in MIS (25.63 ± 25.64 kg-CO2e) compared to open surgery (11.14 ± 10.19 kg-CO2e, P < 0.001) (Table 3c).
Discussion
From an environmental perspective, this study highlights the substantially greater CF of MIS over open microdiscectomies, primarily driven by the significantly larger CF produced by the waste phase in MIS. The 19.5 kg-CO2e difference between procedures represents a trade-off between environmental impact and clinical benefits including 35-minute shorter operative time and 4.7-hour reduced hospital stay. Targeted interventions could potentially mitigate this difference while preserving MIS advantages.
The distribution phase did not have a significant difference between the two groups. While there was a significantly greater CF produced by the distribution of non-gas medications in MIS surgery, the reason for this difference is unclear given the shorter operative duration in MIS procedures. This may reflect differences in medication selection or dosing protocols between the two groups. The similar amounts of CF produced by disposable items and reusable instruments during this phase in MIS and open procedures reflect how both require similar instruments and supplies to complete the case. The distribution of these instruments contributed 10.8% and 11.8% of the MIS and open CF’s respectively. This highlights the points both Nakarai et al and McGain et al make, highlighting single-use supplies such as instruments and drapes and complex reusable tools as key factors in higher lifecycle emissions.14,15 Hospitals should therefore make attempts to source their instruments from more local manufacturers, if possible, especially for disposable items.
Inhalational anesthetic gases, particularly agents with high global warming potential like desflurane and isoflurane, were large contributors to the CF of both open and MIS procedures during the use phase. Although the CF produced by these gases was greater in the open group, this is likely due to their longer operative time. While there was no difference in OR electricity consumption, there was a significant difference in HVAC use. MIS involves a small surgical field that is viewed through a tubular retractor, as compared to open microdiscectomies which involve direct visualization via a larger incision and soft tissue and muscle retractors. Therefore, it requires additional powered equipment to visualize the operative field and assess surgical progress including microscopes, surgical navigation cameras and screens, and/or fluoroscopy, which resulted in higher electricity consumption and greater heat production, ultimately requiring more energy-intensive HVAC system use. These findings align with studies by Rizan et al and Bravo et al, which highlight the environmental impact of HVAC, prolonged procedures, and advanced or newer surgical technologies that rely on single use instruments and their recommendation for optimization of energy use in the OR.3,5,8 The greater CF of the steam sterilizer in the open surgery group reflects the lower necessity for disposable items and instead, reliance on reusable and more commonly used surgical instruments.
The waste phase underscores MI surgery’s environmental challenges, with a significantly higher CF linked to the extensive use of disposable components, especially those associated with equipment such as sterile microscope and fluoroscopy machine drapes. Strategies to mitigate these impacts include reprocessing single-use items, optimizing reusable instrument workflows, and adopting sustainable surgical kits, as advocated by McGain et al and Nakarai et al.14,15 Although the waste phase for non-gas medications was greater in open surgery, this may be a result of its shorter duration and necessary disposal of partially used items.
To ensure the sustainability of MIS, targeted interventions are critical. These include improving OR energy efficiency and promoting lifecycle-based sustainability assessments.5,11,14,16,19,23 Such measures would align MIS practices with global sustainability goals while maintaining clinical benefits. Likewise, open procedures should adopt the same practices, as the CF difference was not significant in the distribution and use phases. Therefore, open surgery does create a large environmental impact and reflects the need for other interventions such as low-GWP anesthetic gases and the previously discussed recommendations by McGain et al, Nakarai et al, Rizan et al, Leiden et al, Christiansen et al and Phoon et al to be applied to any procedure in the OR, whether open or MIS.3,5,11,14,16,19,24
Finally, the real-world analogies in Figure 2A, and B provide a tangible understanding of MIS’s environmental trade-offs. The CF of a single MIS microdiscectomy equates to driving a gasoline vehicle 292 miles, burning 127 pounds of coal, or charging 9271 smartphones, compared to 242 miles, 106 pounds, and 7692 smartphones for a single open microdiscectomy surgery.
25
These analogies effectively illustrate the environmental trade-offs of MIS, which, while offering clinical benefits, demand greater energy and material utilization, underscoring the need for strategies to reduce its environmental impact. Equated Carbon Footprint of MIS (a) and Open Groups (b). Results from the United States EPA Greenhouse Gas Equivalencies Calculator. Note, the estimates are approximate.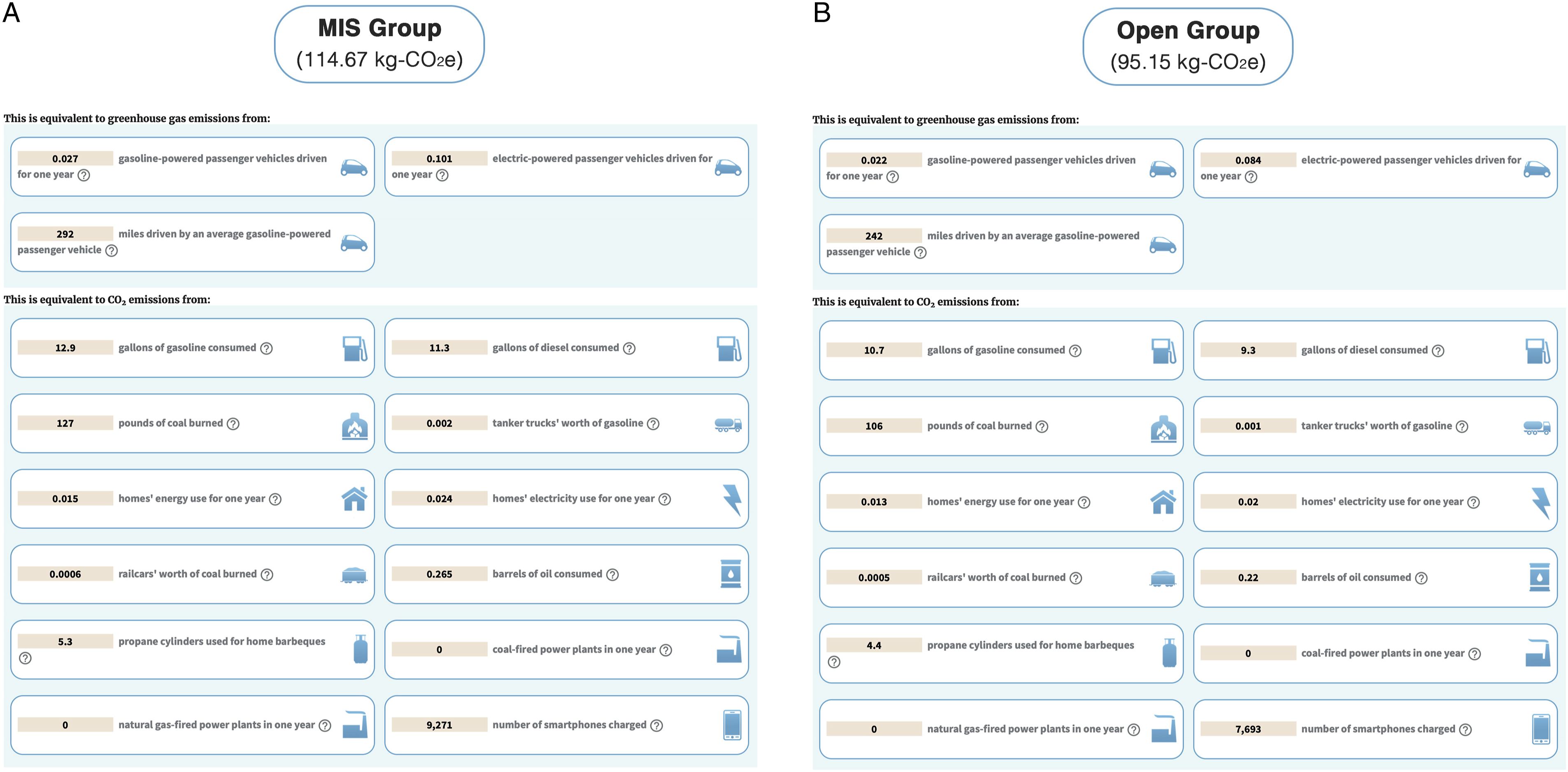
Despite the larger CF of MIS, adding the CF generated from a postoperative hospital stay may affect its overall CF when including inpatient hospital resources. There is limited data analyzing the CF of patient care postoperatively, but some insight may be drawn from Phull et al, 26 who describes a substantial reduction in the CF of urological surgery when performing a procedure as day-based rather than as inpatient. While this may help us suggest MIS will likely have a lower CF due to a shorter and less resource-intensive hospital stay, we did not perform an analysis for the differences in CF generated during the postoperative stay between MIS and open groups. Therefore, to fully quantify the true difference in the CF of MIS and open surgery, length of hospital stay must be considered. However, regardless of including hospital stay in the CF calculation, the findings of this study still represent a need for reducing the environmental impact of MI microdiscectomy surgery.
Importantly, as CF analysis of surgical procedures is a more recent topic of interest and there is limited information over the CF of spine surgery, understanding how the environmental impact of these procedures over time is not possible. Additionally, there are no guidelines defining a high CF for any process, including surgical procedures. We are therefore unable to discuss whether the values this study reported in both groups are elevated. However, when comparing procedures across orthopedic specialties, spine surgery does seem to produce a greater CF based on available information. For example, our results show an average of 95.15 kg-CO2e for an open microdiscectomy and Nakarai et al reported 147.7 kg-CO2e for ASD surgery, whereas Eidman et al reported 87.2 kg-CO2e for primary knee arthroplasty, 53.5 kg-CO2e for knee arthroscopy, and 81.0 kg-CO2e for ACL reconstruction.12,14 Despite the inability to qualify CF results, as the recommendations of this study and those cited are incorporated, future studies should further analyze their efficacy in reducing the CF of surgical procedures.
Finally, this study does have some limitations. First, the study did not account for the CF associated with the manufacturing of surgical products, which could lead to an underestimation of their total environmental impact. Second, variability in waste management, transportation, and electricity production across regions means that CF results may not be directly generalizable; Institutional and geographic differences must be considered when designing strategies to reduce the environmental impact of surgery. Lastly, future studies incorporating granular surgical technique variables, suture usage patterns, and complete post-operative resource utilization would provide a more comprehensive environmental impact assessment.
Conclusion
Although MI microdiscectomy surgery may offer clinical benefits for patients such as decreased operative time and hospital stay, its carbon footprint is notably higher than open surgery. Strategies such as adopting waste reduction, increased use of reusable materials and instruments, and optimizing energy use in operating rooms can mitigate the carbon footprint and should be applied to open surgery as well. Future research should aim to quantify these measures’ effectiveness in balancing patient outcomes and environmental sustainability.
Informed Consent
All participants provided informed consent for both study participation and publication, as approved by the Institution Review Board.
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from the Hospital for Special Surgery Institutional Review Board (IRB #2018-1599) with approval from the registry steering committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the No direct funding was received for this study. However, the data was collected and managed using REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384. REDCap is a secure, HIPAA-compliant web-based software platform designed to support data capture and data management for research studies.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.