
Abstract
Study Design
Prospective single-center cohort study.
Objective
To evaluate cardiac morphology, cardiac function, and pulmonary hypertension impairment in patients with idiopathic scoliosis (IS) and their changes one year after scoliosis surgery.
Methods
70 patients with IS with predominantly thoracic curvature Cobb angle >40° were enrolled and categorized into moderate (<70°) and severe (≥70°) groups. Preoperative radiography and transthoracic echocardiography were performed. Postoperatively, 51 patients completed a one-year follow-up and were compared with preoperative data.
Results
(1) Left ventricular end-diastolic diameter (LVEDD), left ventricular global longitudinal strain (LVGLS), and e were lower and E/e was higher in the moderate vs severe group, and the aortic internal diameter and LVEF were lower in the severe group than in the control group (P < 0.05); (2) Right ventricular free wall strain (RVFWS), tricuspid annular plane systolic excursion (TAPSE), and TAPSE/systolic pulmonary artery pressure (SPAP) were lower, and SPAP was higher in the moderate vs severe group than in the control group (P < 0.05); (3) The thoracic curve Cobb angle was significantly negatively correlated with LVEDD, SV, LVGLS, RVFWS, TAPSE, TAPSE/SPAP and FVC and FEV1 measured/predicted (P < 0.05), and positively correlated with SPAP (P < 0.05); (4) After one-year postoperative follow-up, LVEDD, LVGLS, SV, e, RVFWS, TAPSE and TAPSE/SPAP were higher, and E/e and SPAP were lower (P < 0.05) compared to pre-operation.
Conclusion
Cardiac morphology, left and right heart function, and pulmonary function were impaired in patients with IS, and which showed significant improvement after posterior corrective surgery.
Keywords
Introduction
Idiopathic scoliosis (IS) is a complex three-dimensional spine deformity, characterized by abnormal curvature, which can lead to thoracic deformities. Severe spinal curvature, accompanied by thoracic distortion, may displace and compress intrathoracic structures—including the heart, lungs, bronchi, descending aorta, and pulmonary arteries— due to mechanical compression. This affects cardiopulmonary function to varying degrees and significantly impacts the patient’s quality of life. Previous reports on the effects of varying severities of IS on pulmonary function have yielded inconsistent findings, and the question of whether pulmonary function improves or deteriorates following different surgical procedures remains contentious. 1 Previous reports indicated that pulmonary function declined in patients who underwent thoracoplasty or anterior spinal corrective surgery, whereas posterior corrective surgery alone may not further significantly exacerbate the deterioration of pulmonary function.2–4 Previous preliminary study on cardiac function in IS has predominantly utilised a traditional single index of cardiac function, making it challenging to sensitively detect abnormalities or subclinical states of impaired cardiac function associated with IS. 5 Accurate preoperative assessment of cardiac function in patients with IS may significantly influence the timing of surgical intervention, management of operation duration, and maintenance of circulatory stability during anaesthesia. For instance, previous studies have demonstrated that intraoperative anaesthesia in the prone position for scoliosis is more likely to result in circulatory abnormalities, such as reduced cardiac output and hypotension, with the risk further heightened when scoliosis is accompanied by pulmonary hypertension.6,7 Unlike air-containing lung tissue, the heart is a solid organ with a continuous pumping function. It remains uncertain whether cardiac function improves following the relief of mechanical compression through posterior corrective surgery, and the long-term prognosis is also ambiguous. Two-dimensional speckle tracking echocardiography (2D-STE), a novel technique recommended by recent guidelines for assessing cardiac function, offers the advantage of being angle-independent, making it particularly suitable for patients with IS who exhibit significant variations in cardiac axial orientation and position due to spinal torsion. 8 What is the extent of cardiorespiratory impairment in young adults when spinal deformity progresses untreated during periods of rapid growth? What degree of improvement can be expected following posterior corrective surgery? These questions have garnered considerable attention. The objective of this study was to conduct a comprehensive investigation of preoperative right heart function, left heart function, pulmonary hypertension, and impaired pulmonary function in patients with moderate-to-severe IS. Additionally, the study aimed to assess the improvement in cardiac structure, function, and pulmonary function in IS patients after posterior corrective surgery. This was achieved through the application of conventional echocardiography, the innovative technique of 2D-STE, and the right ventricular-pulmonary artery coupling index, alongside pulmonary function evaluations.
Methods
Case Enrollment
This prospective study recruited 70 hospitalised patients with IS from October 2021 to August 2023, comprising 51 adults with IS and 19 patients with adolescent idiopathic scoliosis (AIS). According to the Lenke classification, the spinal types of IS included Lenke types I and II. 9 According to the 2016 SCOSORT guidelines, the severity of scoliosis was graded based on the coronal Cobb angle of the spinal curvature, serving as a critical determinant for distinguishing between conservative and surgical treatment options. The present study included patients with IS exhibiting a thoracic curvature coronal Cobb angle exceeding 40°, irrespective of whether the curvature pattern was left or right. 10 We considered the criteria outlined in the 2016 SCOSORT guidelines (40-50°) and previous studies that suggested a severity threshold of 80-90° and cautiously established 70° as the criterion for severity threshold.1,4,5,11–15 Patients with IS were categorised into a moderate group comprising 32 individuals (40° < Cobb angle <70°) and a severe group consisting of 38 individuals (Cobb angle ≥70°). The inclusion criteria for participants with IS were as follows: (1) isolation of scoliosis, (2) absence of congenital heart disease or significant valvular anomalies, (3) age between 10 and 35 years, (4) requirement for posterior corrective surgery, and (5) availability of satisfactory cardiac ultrasound images. The exclusion criteria were as follows: (1) congenital scoliosis; (2) neuromuscular scoliosis; (3) secondary causes of scoliosis, such as neurofibromatosis in conjunction with scoliosis and acquired scoliosis; (4) congenital heart disease, including atrial septal defect, ventricular septal defect, and patent ductus arteriosus; (5) primary lung disease; (6) significant valvular abnormalities; and (7) cases in which two-dimensional echocardiographic images of two or more segments could not be accurately tracked using the Qlab software, thereby precluding analysis via 2D-STE. A control group comprised 32 healthy individuals matched for age, sex.
Research Parameters
Height, arm length, weight, blood pressure, body surface area, and body mass index (BMI) were recorded for 70 patients with IS and 32 healthy controls. In four cases, arm length was used to calculate BMI due to extreme spinal distortion, which resulted in arm length significantly exceeding height.16,17 Preoperatively, all patients with IS underwent a comprehensive set of diagnostic evaluations, including full frontal and lateral spine radiography, transthoracic echocardiography, electrocardiography, and pulmonary function tests. The spine surgeon confirmed the Cobb angle measurements. Following preoperative evaluation, patients with IS were advised to undergo posterior corrective surgery and were regularly followed up for a minimum of one year postoperatively. A total of 51 patients completed the postoperative follow-up and were included in the postoperative group. Transthoracic echocardiography and pulmonary function tests were conducted one year postoperatively and compared with preoperative data. Informed consent was obtained from all adult participants and the parents of minors, and the study received approval from the Hospital Review Board.
Transthoracic Echocardiography
The Philips EPIQ 7C cardiovascular ultrasound diagnostic device (Philips, Netherlands) and the Qlab analysis software were used to obtain the following cardiovascular parameters:
Cardiovascular Structural Parameters
Left atrial internal diameter (LAD), left ventricular end-diastolic diameter (LVEDD), right atrial transverse diameter (RATD), right atrial longitudinal diameter (RALD), right ventricular internal diameter (RVD), aortic internal diameter (AOD), and main pulmonary artery diameter (MPAD).
Left Ventricular Function Parameters
Left ventricular ejection fraction (LVEF), stroke volume (SV), mitral orifice antegrade peak early diastolic velocity (E), peak late diastolic velocity (A), E/A ratio, tissue Doppler technique measurements of mitral annular peak early diastolic velocity (e) and late diastolic velocity (a), and calculations of e/a and E/e.
Right ventricular function parameters
M-mode ultrasound measurement of tricuspid annular plane systolic excursion (TAPSE), estimation of systolic pulmonary artery pressure (SPAP) via tricuspid regurgitant velocities, and the calculation of right ventricular-pulmonary artery coupling (TAPSE/SPAP).18,19
Ventricular myocardial mechanical parameters
The 2D-STE technique was used to calculate left ventricular global longitudinal strain (LVGLS) and right ventricular free wall strain (RVFWS).20,21
Pulmonary function tests
The following pulmonary function parameters were assessed: forced vital capacity (FVC) measured /predicted, forced expiratory volume in one second (FEV1) measured/predicted, FEV1/vital capacity (VC) measured/predicted, peak expiratory flow (PEF) measured/predicted, total lung capacity (TLC) measured/predicted, and maximal voluntary ventilation (MVV) measured/predicted.
Electrocardiogram (ECG)
An ECG was used to detect cardiac abnormalities in patients with IS and controls, including rhythm, heart rate, electrical axis, and ST-T wave changes.
Posterior corrective surgical procedure
The posterior spinal corrective surgery was performed in the prone position under general anaesthesia. The surgical procedure is as follows: (1) Incision and Exposure: A midline posterior longitudinal incision was made over the spine, with stepwise exposure of the spinous processes, laminae, facet joints, transverse processes, and proximal ends of the ribs. (2) Screw Insertion: Using a C-arm fluoroscopy system for guidance, appropriately sized pedicle screws were implanted at the corresponding vertebral segments, followed by temporary fixation. (3) Release and Osteotomy: A round-tipped dissector was employed to release the costovertebral and costotransverse joints, followed by osteotomy at the overlapping areas of the facet joints and laminae. (4) Correction of Spinal Deformity: After completing the osteotomy, correction of the scoliosis was achieved by distraction on the concave side and compression on the convex side. (5) Management of Rigid Kyphosis: Partial rib resection was performed on the concave side, with overlapping of the bilateral ends secured using tendon sutures. (6) Bone Fusion: Autologous bone grafting was performed to achieve fusion at the fixed segments. (7) Safety Monitoring: Intraoperative safety was ensured through the use of wake-up tests and monitoring of somatosensory evoked potentials.
Statistical Analysis
Statistical analysis was conducted using SPSS version 26. Continuous measurements are expressed as mean ± standard deviation, while categorical data are presented as frequencies. The t test was employed for comparing continuous variables, and the χ2 test was applied for categorical variables. Additionally, Pearson’s correlation coefficient was utilized to examine the relationship between the Cobb angle and cardiac and pulmonary function parameters. Multifactorial logistic regression analysis was performed to identify factors influencing the Cobb angle of thoracic curvature. A P-value of less than 0.05 was considered statistically significant.
Results
Comparison of Basic Characteristics of Patients with IS
Comparison of Basic Characteristics of Patients With IS.
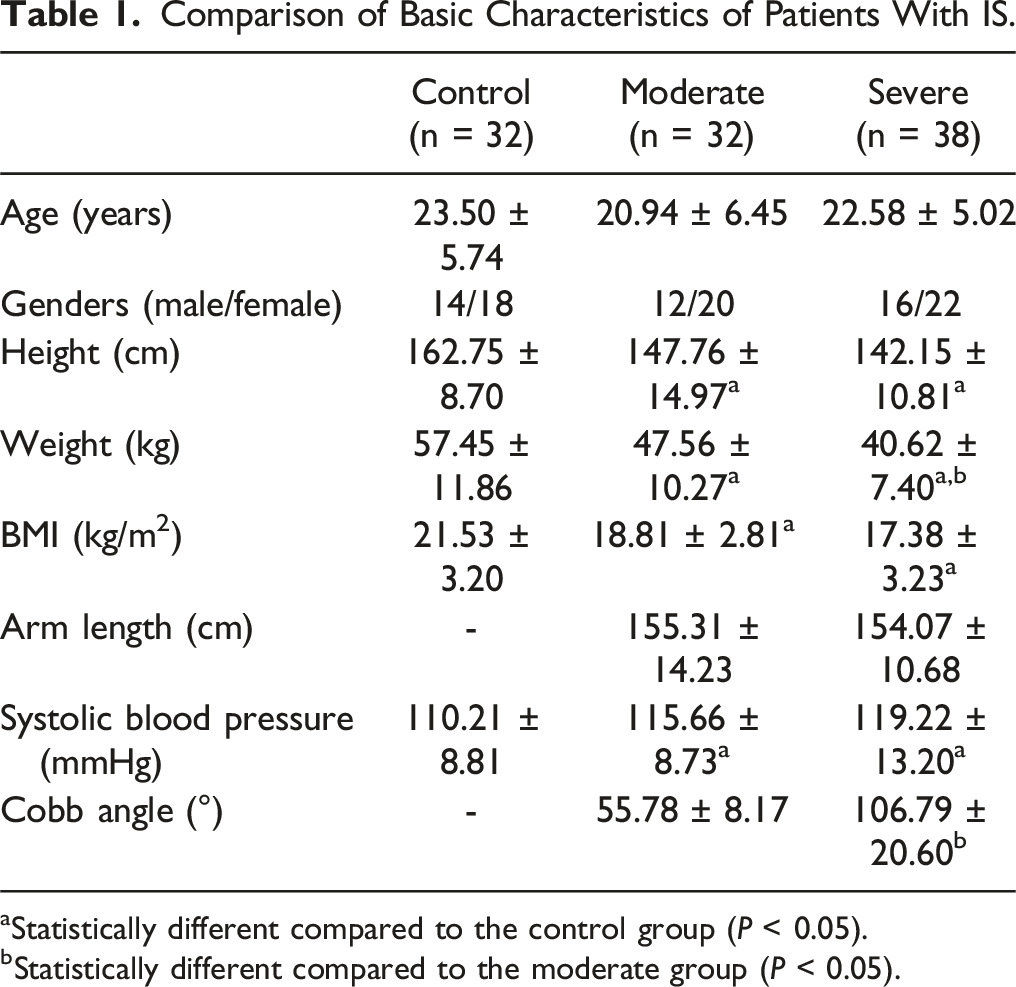
aStatistically different compared to the control group (P < 0.05).
bStatistically different compared to the moderate group (P < 0.05).
Comparison of Cardiac Structural Parameters of Patients with IS
Comparison of Structural and Functional Parameters of the Heart in Patients With IS.
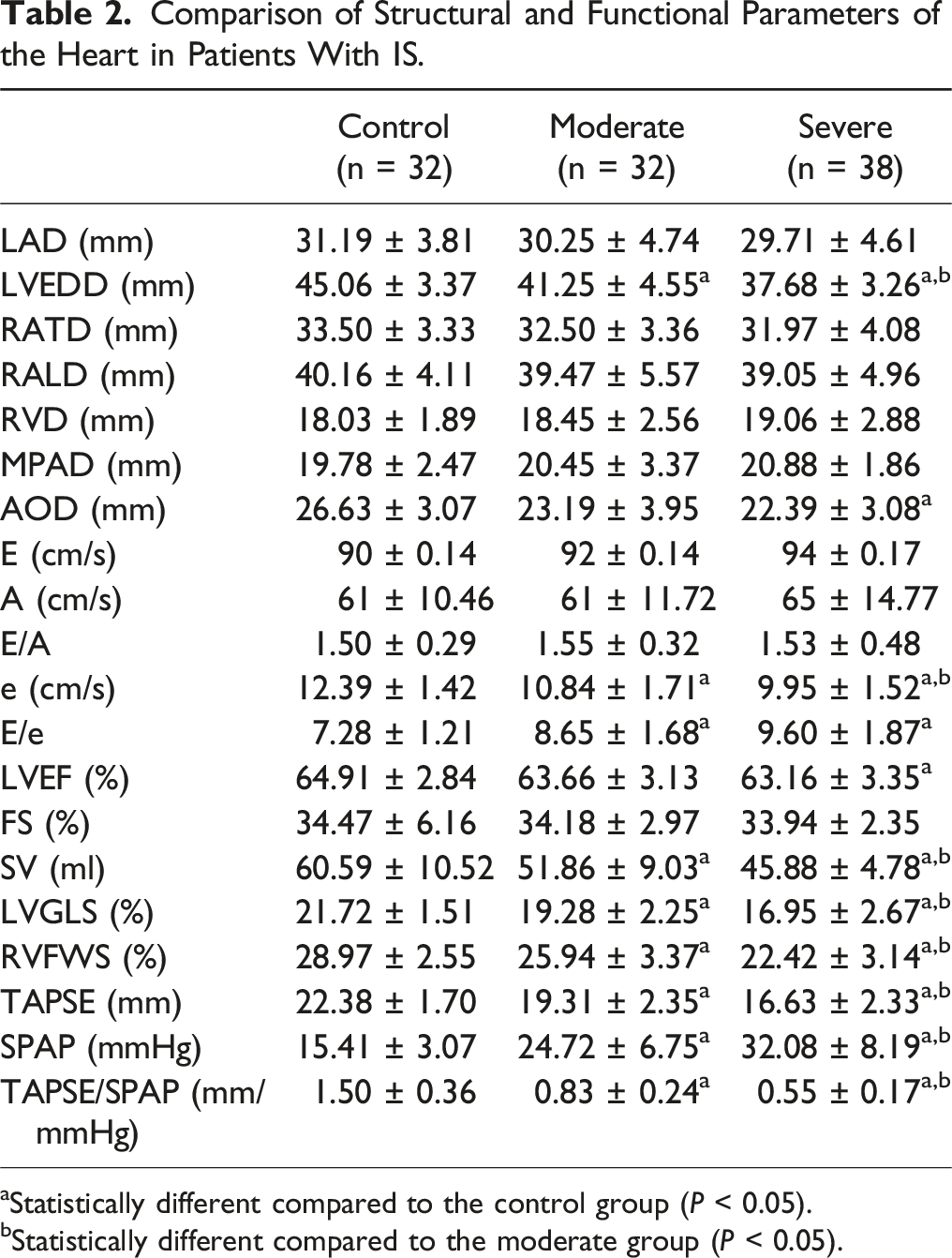
aStatistically different compared to the control group (P < 0.05).
bStatistically different compared to the moderate group (P < 0.05).
Comparison of Cardiac Function Parameters of Patients with IS
Left Ventricular systolic Function Parameters
Compared to the control group, SV and LVGLS were significantly lower in both the moderate and severe groups (P < 0.05), and LVEF was also lower in the severe group (P < 0.05), while the differences in LVEF and FS between the moderate and severe groups were not statistically significant. Furthermore, SV and LVGLS were significantly lower in the severe group compared to the moderate group (P < 0.05). Table 2.
Left ventricular diastolic function parameters
Compared to the control group, the e was significantly lower, and the E/e ratio was significantly higher in the moderate and severe groups (P < 0.05); the E, A, and E/A ratio were not statistically significantly different in the moderate and severe groups. Additionally, the e was significantly lower in the severe group (P < 0.05), whereas E, A, E/A, and E/e did not show statistically significant differences in comparison to the moderate group. Table 2.
Right ventricular function parameters
Compared with the control group, RVFWS, TAPSE, and the TAPSE/SPAP ratio were significantly lower, while SPAP was significantly higher in both the moderate and severe groups (P < 0.05). Additionally, RVFWS, TAPSE, and the TAPSE/SPAP ratio were lower, and SPAP was higher in the severe group compared to the moderate group (P < 0.05). Table 2.
Comparison of electrocardiograms in IS patients
In comparison to the control group (4/32 cases, 12.5%), the moderate (12/32 cases, 37.5%) and severe (18/38 cases, 47.4%) groups exhibited a significantly higher incidence of electrocardiographic abnormalities (P < 0.05).
Comparison of Pulmonary Function in IS Patients
Compared to the control group, both the moderate and severe groups exhibited significantly lower values for FVC measured/predicted, FEV1 measured/predicted, PEF measured/predicted, FEV1/VC measured/predicted, TLC measured/predicted, and MVV measured/predicted (P < 0.05). In the severe group, several pulmonary function test results were significantly lower when compared with the moderate group (P < 0.05), including FVC measured/predicted, FEV1 measured/predicted, PEF measured/predicted, FEV1/VC measured/predicted, TLC measured/predicted, and MVV measured/predicted. Figure 1. Pulmonary function in patients with IS Note: ***P < 0.001, **P < 0.01, *P < 0.05.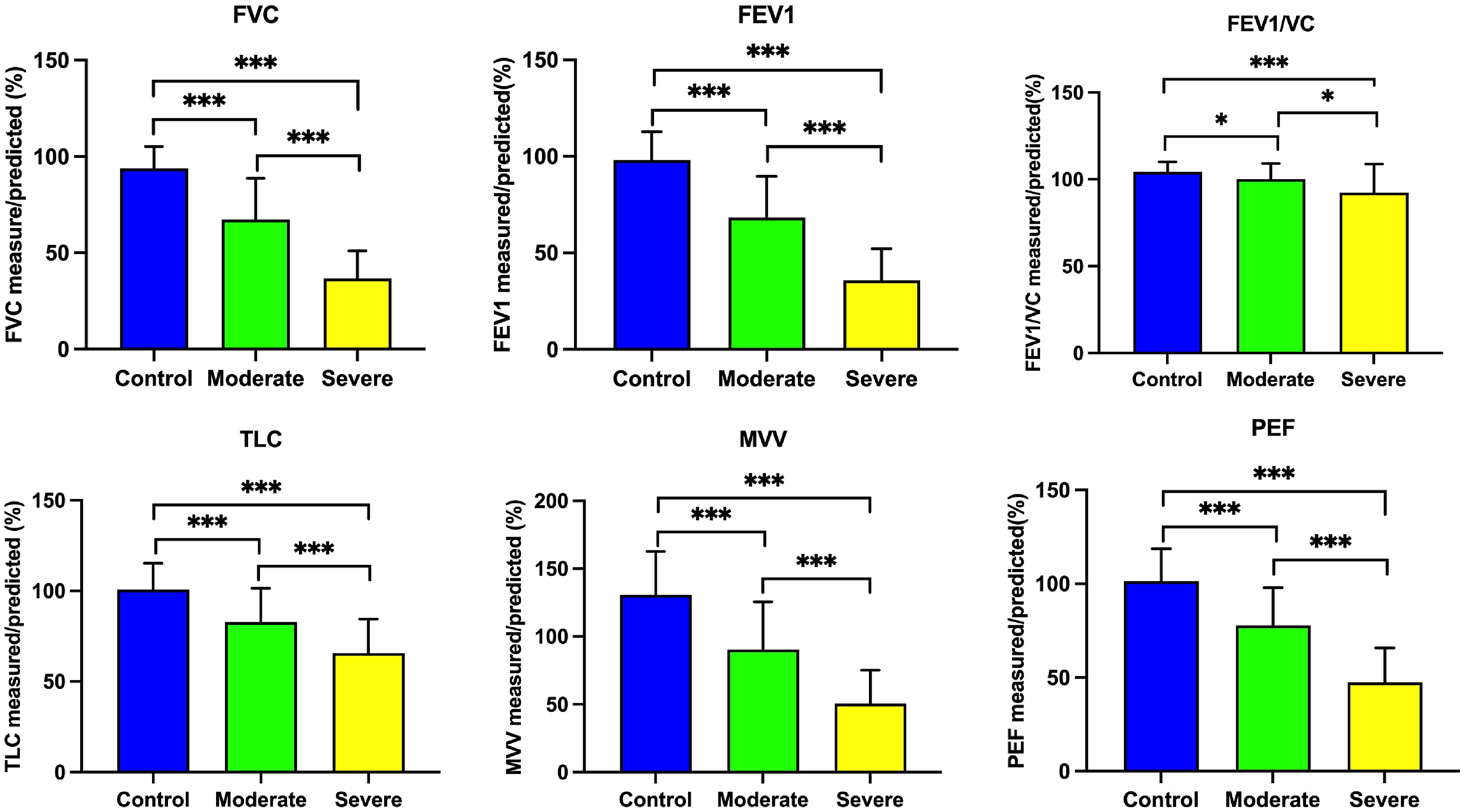
Correlation Analysis of Cobb Angle with Cardiac Function and Pulmonary Artery Pressure
Correlation Analysis of Cobb Angle With Cardiac Function and Pulmonary Artery Pressure.
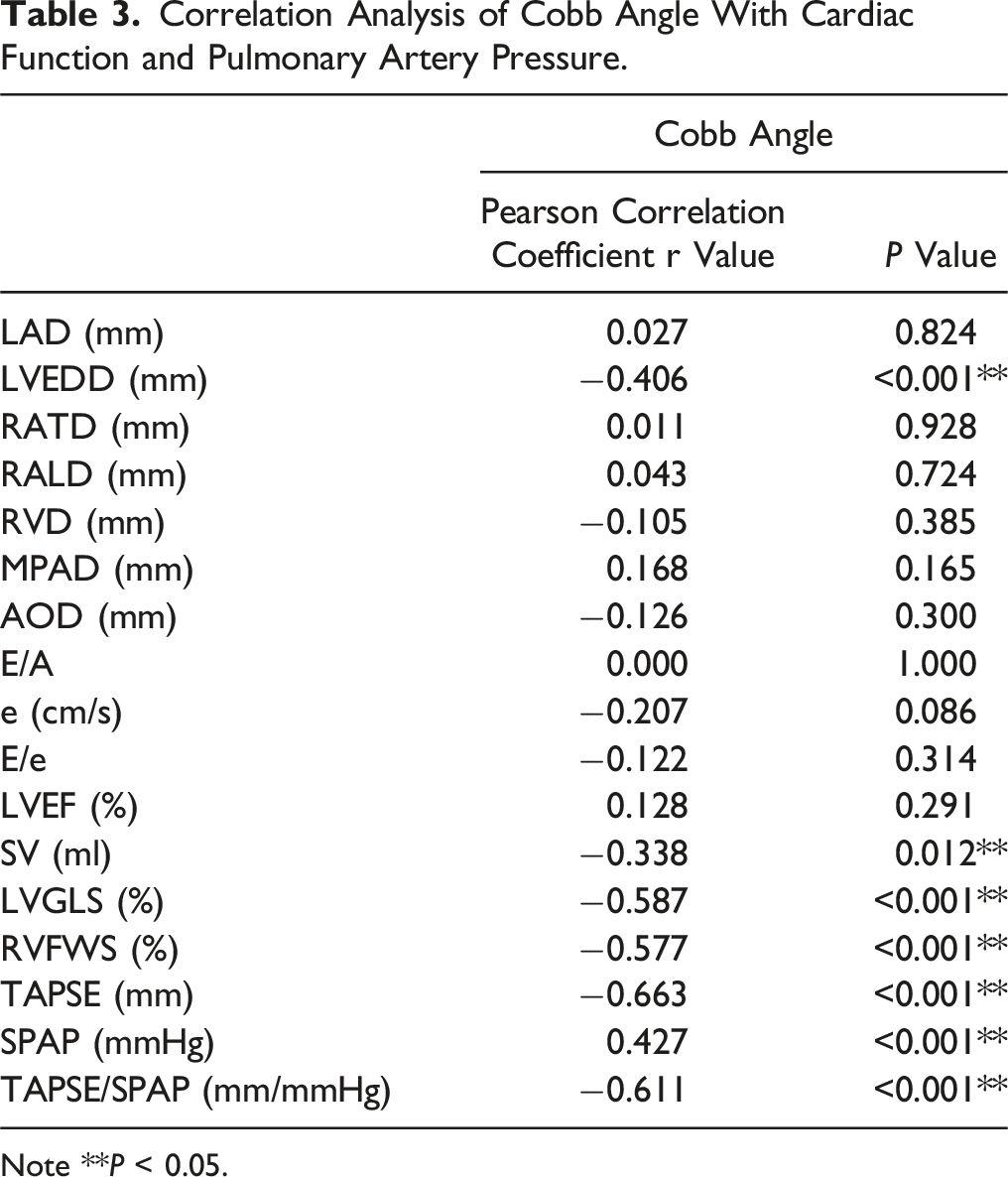
Note **P < 0.05.
Correlation Analysis of Cobb Angle with Pulmonary Function
Correlation Analysis of Cobb Angle With Pulmonary Function.
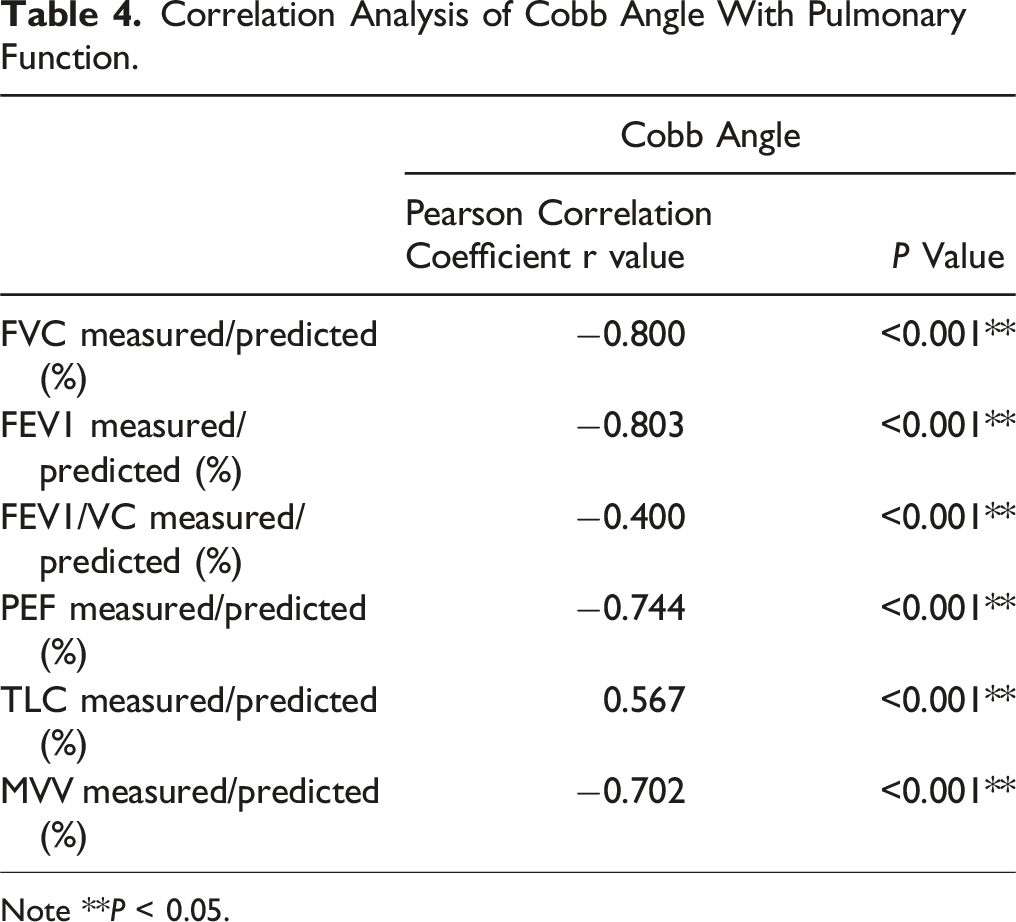
Note **P < 0.05.
Multifactorial Logistic Regression Analysis of Factors Influencing the Cobb Angle
The results of the multifactorial logistic regression analysis, with the thoracic curvature Cobb angle of scoliosis as the dependent variable, indicated that BMI [OR = 0.830 (B = −0.187, 95% CI:0.693-0.993, P = 0.042)] exhibited a slight negative correlation with the severity of scoliosis. In contrast, age [OR = 1.085 (B = 0.081, 95% CI:0.988-1.191, P = 0.086)] and gender [OR = 0.651 (B = −0.429, 95% CI:0.231-1.837, P = 0.418)] were not significantly correlated with Cobb angle.
Comparison of Postoperative and Preoperative Cardiac Structure and Function
Comparison of Postoperative and Preoperative Cardiac Morphology and Cardiac Function.
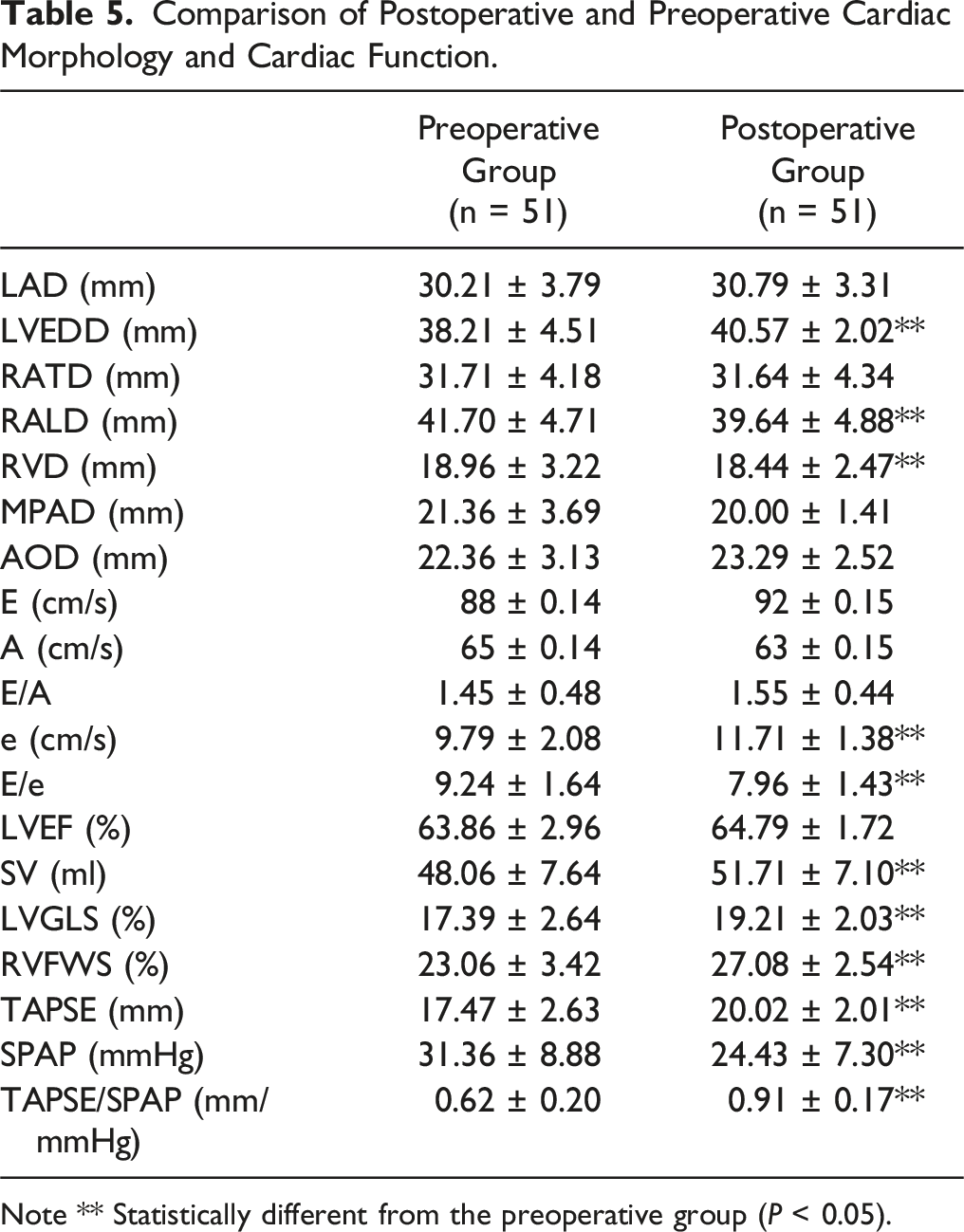
Note ** Statistically different from the preoperative group (P < 0.05).
In terms of cardiac function, the e was significantly higher and the E/e ratio was significantly lower in the postoperative group compared to the preoperative group (P < 0.05). The E, A, and E/A ratios did not demonstrate significant differences between the postoperative and preoperative groups. Additionally, the LVGLS, SV, RVFWS, TAPSE, and the TAPSE/SPAP ratio were significantly higher in the postoperative group (P < 0.05). The SPAP was significantly lower in the postoperative group compared to the preoperative group (P < 0.05). Conversely, the LVEF did not show a significant difference between the postoperative and preoperative groups. Table 5.
Comparison of Postoperative and Preoperative Pulmonary Function
Compared to the preoperative group, the postoperative group demonstrated significantly higher values for FVC measured/predicted, FEV1 measured/predicted, FEV1/VC measured/predicted, PEF measured/predicted, and MVV measured/predicted (P < 0.05). However, no statistically significant differences were observed in TLC measured/predicted between the groups. Figure 2. Comparison of postoperative and preoperative pulmonary function Note: ***P < 0.001, **P < 0.01, *P < 0.05.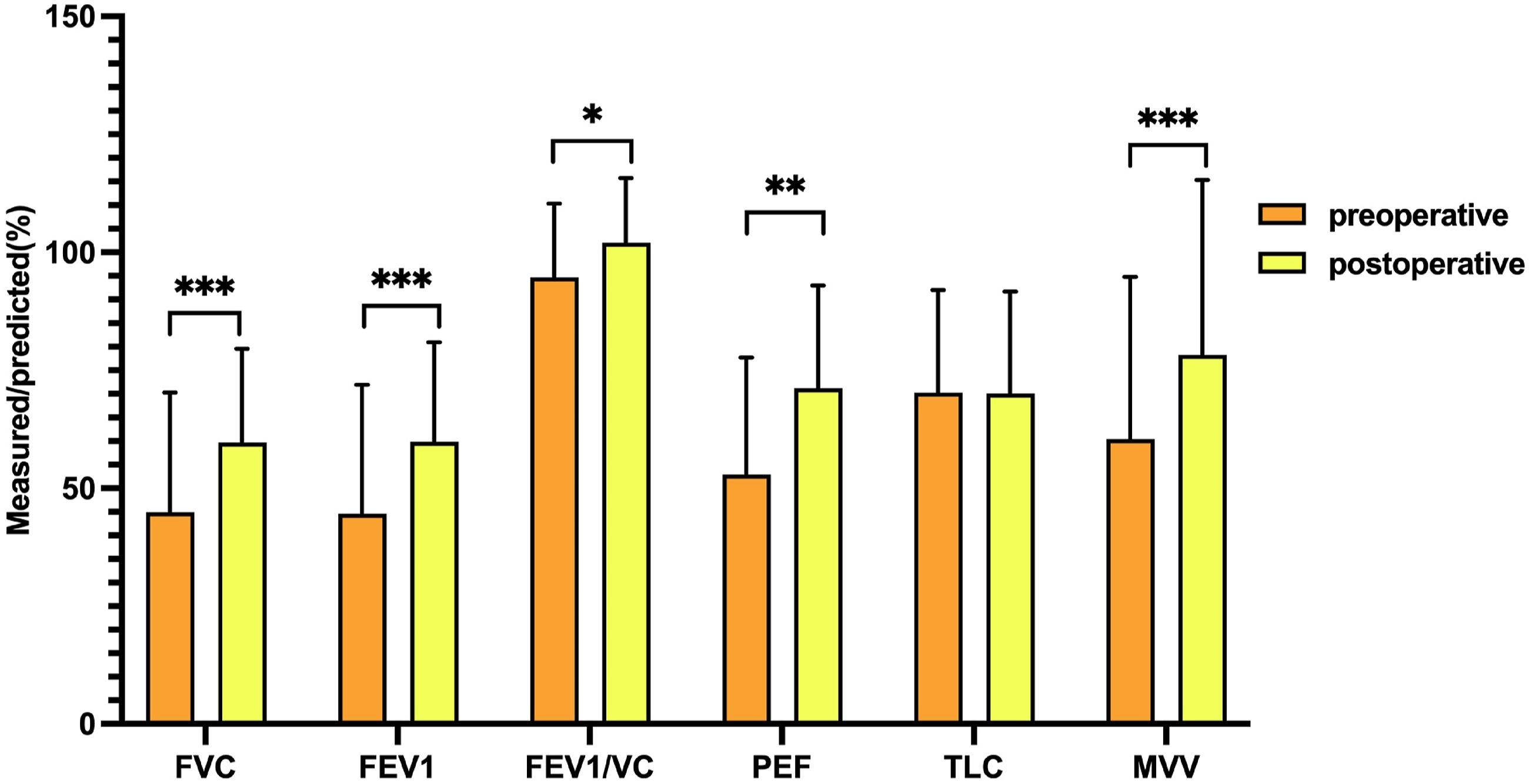
Discussion
Spinal deformities and thoracic wall anomalies can restrict the growth and/or limit the functional movement of intrathoracic organs. 22 This may result in mutual compression of these organs, leading to tortuosity or displacement of the bronchi, pulmonary arteries, and aorta. 23 Such alterations can induce anatomical and functional changes within the lungs, potentially affecting cardiac morphology and haemodynamics, ultimately resulting in abnormalities in both diastolic and systolic cardiac function. 11 Previous studies using cardiac MRI from the UK Biobank have demonstrated that adults with scoliosis exhibit a reduction in longitudinal peak diastolic strain rate alongside an increase in radial peak diastolic strain rate. Additionally, pulmonary hypertension may emerge as a secondary complication of scoliosis. 24 However, the study did not specify the type of scoliosis involved. Moreover, the application of cardiac MRI is limited due to high healthcare costs, and contraindications associated with metallic implants, which can often be mitigated through echocardiography. Establishing the cardiopulmonary function in patients with IS vital for determining surgical timing, assessing surgical risks, and formulating personalised surgical and anaesthetic strategies to minimise the incidence of perioperative complications. Furthermore, evaluating cardiopulmonary function is crucial for postoperative recovery. Spinal surgeons must closely monitor the cardiopulmonary status of their patients to devise an appropriate rehabilitation plan and enhance overall patient prognosis. 25 This study provides important evidence regarding the state of cardiopulmonary function rehabilitation following posterior corrective surgery.
In the present study, a significant decrease in height, weight, and BMI, along with an increase in blood pressure levels, was observed in patients with IS. Additionally, BMI in IS patients demonstrated a mild negative correlation with the Cobb angle. This decrease in BMI is consistent with the findings of Watanabe et al. 26
In terms of cardiac structure, patients with severe IS exhibited smaller left ventricular chambers and AOD. This finding indicates a reduction in left ventricular late diastolic filling and lower ejection fraction per heartbeat. Adequate diastolic filling is crucial for maintaining optimal cardiac output. In patients with severe IS, impaired late filling capacity of the LV may arise from thoracic deformity and compression of cardiac structures. During posterior corrective surgery, the prone position of the patient imposes an additional mechanical compressive load on the heart, exacerbated by the twisting of the thoracic cavity. Consequently, patients with IS exhibit an elevated risk of bleeding and blood loss, which may result in decreased cardiac output, mean arterial pressure, and hypotension during surgical procedures.6,27
Previous studies have indicated that mitral valve prolapse is the most prevalent cardiac abnormality associated with IS; however, severe mitral regurgitation leading to significant hemodynamic changes remains rare.28-31 According to the statistics by Lang et al., 28.81% of the 531 patients with IS exhibited cardiac abnormalities, with non-congenital cardiac anomalies constituting 23.9% of the cases. 29 Our study found cardiac morphological involvement in patients with severe IS, which may adversely affect LV diastolic filling and increase the risk of low cardiac output during anaesthesia.
When evaluating cardiac systolic function in patients with IS, it is crucial to assess cardiac compromise and potential tolerance. The data indicated that patients with severe IS exhibited lower LVEF and SV; however, the LVEF remained above 60%. LVGLS, measured using the novel 2D-STE technique, was found to be lower in both moderate and severe IS patients. These findings suggest that left ventricular myocardial mechanics are impaired in patients with IS. Furthermore, as the Cobb angle of the thoracic curvature increases in these patients, the subclinical systolic mechanics of cardiac function deteriorate. 2D-STE is a novel technique that reflects real-time myocardial tissue motion and deformation, providing diagnostic value that is independent of LVEF. 8
Regarding left ventricular diastolic function, our data exhibited lower values of e and higher values of E/e ratio in patients with moderate and severe IS. Notably, the e value was more impaired in severe IS patients with a mean Cobb angle of 107°. Correlation analysis indicated that spinal thoracic curvature, represented by the Cobb angle, may be an important factor influencing abnormal left ventricular diastolic function. Previously, Li et al. found that left ventricular mechanics were impaired relatively early in patients with congenital scoliosis; the e/a ratio was significantly lower and correlated with the severity of scoliosis. 32 Furthermore, Li et al. reported that the e and e/a ratio were significantly lower in AIS patients with a mean Cobb angle of 75 °compared to controls. 33 We recommend the routine application of tissue Doppler imaging and 2D-STE in patients with IS to evaluate potential abnormalities in left heart function.
According to guideline recommendations, the assessment of right ventricular systolic function should combine multiple indicators. 18 This study combined RVFWS, TAPSE and right ventricular-pulmonary artery coupling and found that right ventricular systolic function was lower in patients with moderate and severe IS compared to controls. RVFWS, TAPSE and right ventricular-pulmonary artery coupling were negatively correlated with the Cobb angle of the thoracic spine curvature. Li et al. previously assessed right ventricular function in patients with AIS using TAPSE, and found that 35% (13 out of 37 cases) had reduced right ventricular systolic function. 5 This study is the first to report the application of the right ventricular–pulmonary artery coupling index in patients with moderate to severe IS. It was found that the right ventricular–pulmonary artery coupling index is reduced in these patients, which is consistent with the changes in RVFWS obtained through 2D-STE. This indicates that right heart function is impaired in patients with moderate to severe IS. Furthermore, a significant negative correlation was observed between the right ventricular–pulmonary artery coupling index and the coronal Cobb angle of the thoracic spine. Patients with IS may require more cautious anaesthetic risk assessment and management.
Patients with moderate and severe IS had higher SPAP levels compared to the control group, which positively correlated with the Cobb angle of the thoracic curvature. We postulate that the deterioration of pulmonary function resulting from IS may lead to secondary pulmonary hypertension. This finding aligns with previous research by Li XY et al, who reported a positive correlation between SPAP and the coronal Cobb angle of the thoracic curvature in patients with IS. 10 During posterior corrective surgery, wake-up tests are conducted to assess spinal cord function. This presents a significant risk for patients with scoliosis complicated by pulmonary hypertension, necessitating closer anaesthetic monitoring and timely medication adjustments. 7
On ECG, the increased incidence of electrocardiographic abnormalities in patients with moderate and severe IS compared to controls may be attributed to alterations in ECG parameters resulting from the geometric and positional changes of the heart due to compression.
Mechanical compression arising from spinal abnormalities and thoracic distortion may affect cardiac morphology and haemodynamic changes, potentially leading to dysfunction of the right and/or left heart. Surgical intervention is the fundamental treatment strategy for treating IS. Early evaluation of the cardiac structure and functional status in IS patients is beneficial, as it aids in determining the timing of surgery, controlling intraoperative duration, predicting anaesthetic risks, and anticipating intraoperative circulatory status to facilitate timely pharmacological adjustments.
Our study found that pulmonary function in patients with IS was significantly impaired. Restrictive dysfunction indicators, including measured/predicted values of FEV1, FEV1/VC and TLC showed significant declines. Additionally, ventilatory function indicators including measured/predicted values of FVC, PEF and MVV were also significantly reduced. Severe scoliosis shows obstruction of the large airways, which may be related to the asymmetry of the thoracic cavity caused by the curvature of the spine, resulting in distortion of the main bronchus by anterior or posterior displacement. Correlation analysis revealed a significant negative correlation between pulmonary function impairment and the severity of the thoracic curvature as measured by the Cobb angle in IS patients. Previous research by Lin et al indicated that patients with congenital scoliosis also exhibited significant impairment in FEV1, FVC, and TLC, which correlated with the severity of thoracic curvature; distorted thoracic asymmetry and abnormal breathing patterns were associated with reduced locomotor ability.34,35 Wu et al. found that patients with congenital scoliosis and accompanying cardiac malformations had significantly lower values for FEV1, FVC, and PEF. 36 Additionally, Farrell et al reported lower FEV1 and FVC values in patients with AIS. 37 Our findings are consistent with Farrell et al. Untreated scoliosis may lead to progressive impairment of pulmonary function, thereby increasing the risk of pulmonary hypertension, pulmonary heart disease, and right heart failure, which could subsequently elevate surgery and anaesthesia risks.
Our study found that one year after posterior corrective surgery, patients with IS exhibited a significant increase in LVEDD, accompanied by a reduction in the dimensions of the right atrium and ventricle. In case of severe IS, the twisting of the thoracic cavity restricts the anterior-posterior diameter of the thorax, leading to mechanical compression of the heart, which may limit the ability to increase stroke volume. However, surgical intervention to correct spinal deformities significantly restores spinal morphology, facilitates thoracic reconstruction, and alleviates mechanical compression on the heart and lungs, resulting in improved left ventricular filling. Our findings indicate that left ventricular function parameters, including the LVGLS, e and E/e ratio values, demonstrated significant improvement. Additionally, parameters of right ventricular systolic function, comprising RVFWS, TAPSE, and right ventricular-pulmonary artery coupling, also showed improvement. A single-centre retrospective study revealed that among 201 patients with AIS (mean Cobb angle of 51.5°), 13.9% exhibited elevated tricuspid regurgitant velocities, indicating mild pulmonary hypertension, which normalised postoperatively. 38 Our study demonstrates that patients with IS experience significant enhancements in cardiac geometric morphology, as well as in left and right ventricular function, alongside a reduction in pulmonary hypertension following surgical intervention. This suggests that posterior corrective surgery has a beneficial significant impact on cardiac function in patients with IS.
In this study, we demonstrated that one year after posterior corrective surgery, patients with IS exhibited significant improvements in all pulmonary function indices, including the estimated/predicted values of FVC, FEV1, PEF, TLC, and MVV. The impact of s posterior corrective surgery on lungs growth and function remains a subject of debate. Lorente et al assessed cardiac and respiratory function, including heart rate, blood pressure, maximal oxygen consumption, and carbon dioxide excretion, in 20 patients who underwent posterior surgical correction for AIS. They found that maximal exercise cardiorespiratory endurance was markedly limited in patients with severe AIS, and no significant improvement was observed two years postoperatively. 39 Thoracic volume reaches 50% of adult capacity by age 10, with the remaining 50% developing during prepuberty and early adolescence. If one lung is hypoplastic or completely nonfunctional by puberty, the other lung may enlarge compensatorily. 40 The present study found that, although there was a statistical improvement in pulmonary function one year postoperatively compared to preoperatively, it did not return to relatively normal levels. This may be attributed to limited lungs development and atelectasis in the early stages. Although corrective surgery alleviates mechanical compression of the lungs, it may not result in full recovery of pulmonary function.
Conclusion
Our findings indicate that patients with IS exhibit impaired cardiac morphology, left heart function, right heart function, and pulmonary function, all of which correlate with the Cobb angle of the thoracic curvature. Impairment of left heart function is more prevalent in patients with scoliosis angles exceeding 70°. Posterior corrective surgery interventions lead to notable improvements in both left and right heart function, as well as pulmonary parameters, indicating a positive impact on overall cardiopulmonary function. The study also identifies a correlation between right ventricular-pulmonary artery coupling and the severity of scoliosis.
Limitations
There are several limitations to this study. Firstly, the small sample size may affect the accuracy of statistical analysis results. Secondly, this research was conducted in a single centre, which may have introduced patient selection bias, as the majority of patients with IS treated in our centre were early young adults, thereby may limit the generalisability of the findings. Additionally, the short follow-up period did not permit a comprehensive assessment of long-term outcomes. Future studies will aim to increase the sample size, conduct multicentre reseach, and extend the follow-up duration to more comprehensively assess preoperative cardiorespiratory function and postoperative recovery in patients with IS.
Footnotes
Author’s Note
Feng Xiong, PhD: Responsible for reviewing manuscripts and all stages of publication, as well as handling incoming and outgoing correspondence after publication.
Acknowledgments
The authors would like to acknowledge radiologist Zhengkai Zhao for his help in reading the x-rays.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Registration Number
Registration number: ChiCTR2400089292.