
Abstract
Study Design
Retrospective cohort study.
Objective
The study aimed to determine how obesity modifies operative time and the influence of operative time on wound complications or surgical infections for patients undergoing a single-level anterior cervical discectomy and fusion (ACDF) or a single-level posterior lumbar fusion (PLF).
Methods
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was queried to identify patients who had undergone either a single-level ACDF or a single-level PLF. Multivariable regression was used to determine the relationship between obesity and operative time as well as the relationship between operative time and wound complications or surgical infections.
Results
For every BMI unit of increase, ACDF operative times increased by 0.38 minutes while PLF operative times increased by 0.84 minutes. As operative time increased from the 25th to 75th quartile, the probability of a wound complication increased by 19.7% after a single-level PLF procedure, while there was an increase by 17.1% after a single-level ACDF procedure. The probability of a postoperative surgical infection increased by 30.0% and 12.5% for ACDF and PLF procedures, respectively.
Conclusion
Increases in BMI lead to a greater increase in operative time for patients undergoing single-level PLF compared to patients undergoing single-level ACDF. Patients undergoing either procedure with a prolonged operative time have a greater probability of developing a wound complication or surgical infection. This is the first study to establish a quantitative relationship between obesity and operative time in spine surgery.
Introduction
The prevalence of obesity among adults in the world is estimated to be approximately 890 million. 1 Estimates indicate that nearly 50% of the adult population in the United States will be obese by 2030. 2 Notably, obesity has been associated with the development of back pain and intervertebral disc degeneration.3-7 Given the rising prevalence of obesity in the adult population, spine surgeons will likely encounter an increasing proportion of patients with obesity in their practice.
Patients with obesity present challenges in all aspects of spine-related care and spine surgery. 8 Previous literature has demonstrated obesity as a risk factor in cervical and lumbar spine procedures for adverse complications, including wound infection, pulmonary embolism, urinary complications, deep vein thrombosis, and extended length of hospital stay.9-14 Patients with obesity and elevated body mass index (BMI) may also require increased operative time15,16 that may be secondary to changes in surgical techniques, patient positioning, anesthesia care, and intraoperative imaging strategy. 8 Operative time is clinically relevant as increased time has been identified as an independent predictor of both wound complications and surgical infections.17-19
Although obesity is associated with increased operative times, prior literature quantitatively comparing the differential impact of obesity on cervical and lumbar spine procedures is scarce.11,20-22 To improve surgical outcomes, surgical planning, and risk stratification, a greater understanding of how the impact of obesity may differ in cervical and lumbar spine surgery is necessary. Thus, the aim of this study was to determine how obesity modifies operative time in cervical and lumbar spine surgery by comparing single-level anterior cervical discectomy and fusion procedures and single-level posterior lumbar fusion procedures. Additionally, the study aimed to quantify the impact of operative time on the probability of developing a surgical infection or wound complication.
Materials and Methods
Study Design and Data Sources
A retrospective cohort study was performed using patients in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. The ACS-NSQIP is a prospectively collected multi-institutional program that provides procedure-specific outcomes collected from over 700 institutions across the United States. The program includes over one hundred variables related to patient demographics, patient comorbidities, risk factors, procedure details, and 30-day outcomes. Data is collected from the electronic medical record by certified clinical reviewers who are responsible for verifying the authenticity of the data. 23 The data is captured from a range of healthcare institutions, including academic, private, community, and tertiary medical centers. ACS-NSQIP has regular audits with inter-rater disagreements determined to occur at a rate of less than 2%. 24 The database is deidentified and institutional review board approval was obtained for this study.
Study Population and Outcomes of Interest
Data from 2011 to 2023 were collected on patients undergoing single-level anterior cervical discectomy and fusion (ACDF) procedures or single-level posterior lumbar fusion (PLF) procedures. Patients undergoing ACDF procedures were identified using the Current Procedural Terminology (CPT) code 22551. Patients undergoing PLF procedures were identified using the CPT code 22612 and the concurrent CPT code 63047. Patients undergoing an emergent, concurrent, multilevel, or revision procedure were excluded. Procedures with a combined approach, non-contiguous spinal involvement, or procedures secondary to infection, trauma, or malignancy were identified and excluded. We also excluded patients with missing data, including age, height, weight, and sex.
Patients were stratified into groups based on their World Health Organization (WHO) defined BMI obesity classes as follows: non-obese BMI (18.5-25.0 kg/m2), overweight (25.0-29.9 kg/m2), obese class I (30.0-34.9 kg/m2), obese class II (35.0-39.9 kg/m2), and obese class III (≥40.0 kg/m2). Preoperative variables were collected and stratified among the five obesity status groups. Patient demographic and clinical data collected included age, sex, race, BMI, smoking history, functional status, American Society of Anesthesiologists (ASA) class, diabetes, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), bleeding disorders, chronic steroid use, dialysis, ventilation, bleeding requiring a transfusion, sepsis, and hypertension (HTN). The primary outcome variables for this study were total operative time, wound complications, or surgical infections. The ACS-NSQIP database defines operative time as the time between “surgery start” and “surgery end”. Wound complications were defined to include wound disruption or superficial surgical site infection (SSI), while surgical infections were defined to include organ space SSI and deep space SSI.
Statistical Analysis
ACDF and PLF procedures were analyzed separately. Differences in pre- and peri-operative variables across the cohorts were assessed via Kruskal-Wallis for continuous variables and chi-square tests for categorical variables. Multivariable logistic regression analysis was used to explore the effect of obesity on operative time after adjusting for confounding variables. Additionally, multivariable logistic regression analyses were conducted to assess the relationship between operative time and surgical infections or wound complications. Significant characteristics controlled for in the multivariable analyses included the following: sex, race and ethnicity, admission status, ASA class, surgeon specialty, operative year, comorbidities, and body mass index. After multivariable regression, the change in the adjusted probability of developing a wound complication or surgical infection was determined. Statistical analyses were performed in Stata (Version 16.1, College Station, TX). Significance was defined as P < 0.05.
Disclaimer
American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Results
Cohort Characteristics
Demographics Variables and Comorbidities in Patients Undergoing Anterior Cervical Discectomy and Fusion
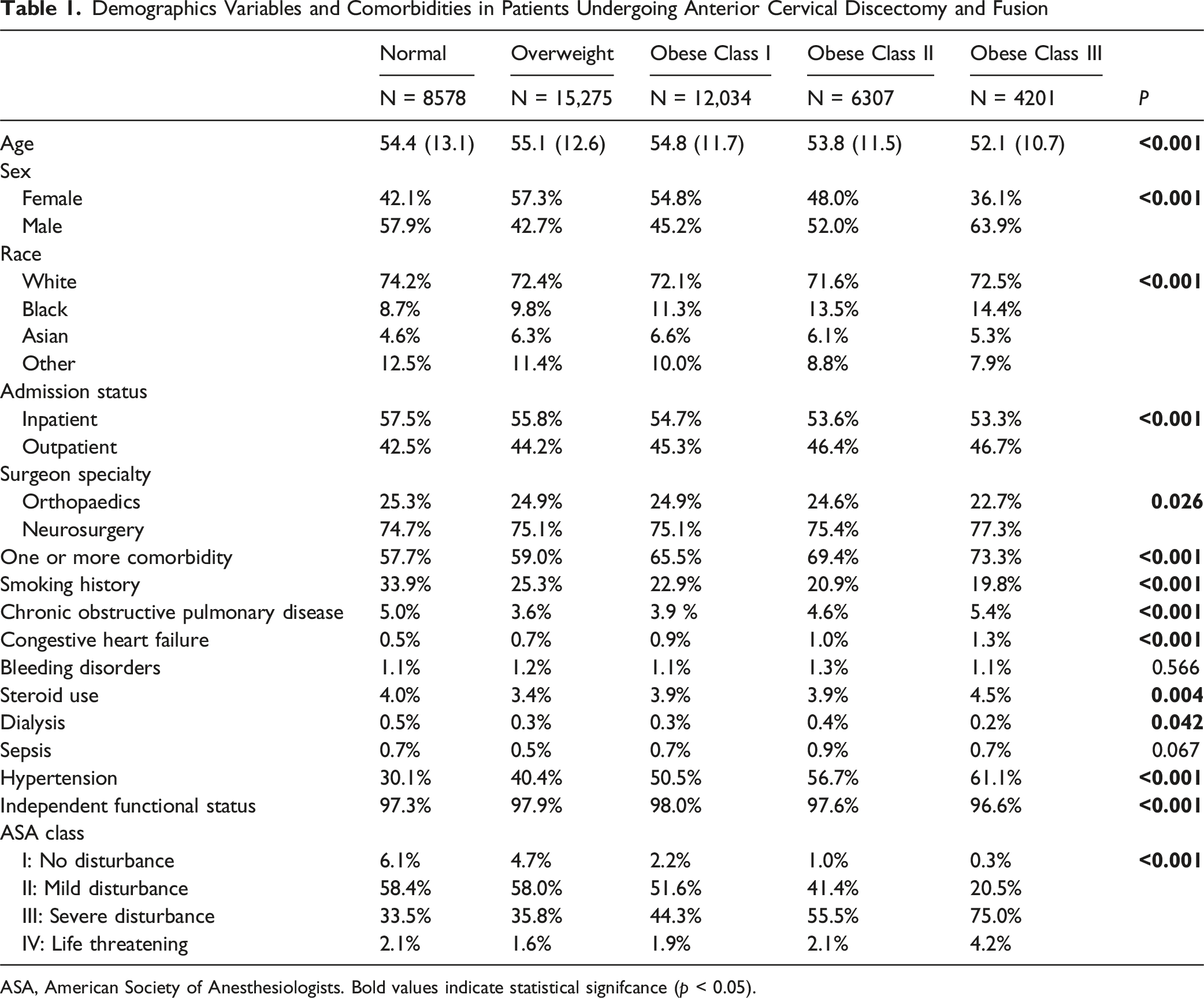
ASA, American Society of Anesthesiologists. Bold values indicate statistical signifcance (p < 0.05).
Demographics Variables and Comorbidities in Patients Undergoing Posterior Lumbar Fusion

ASA, American Society of Anesthesiologists. Bold values indicate statistical signifcance (p < 0.05).
Body Mass Index and Operative Time
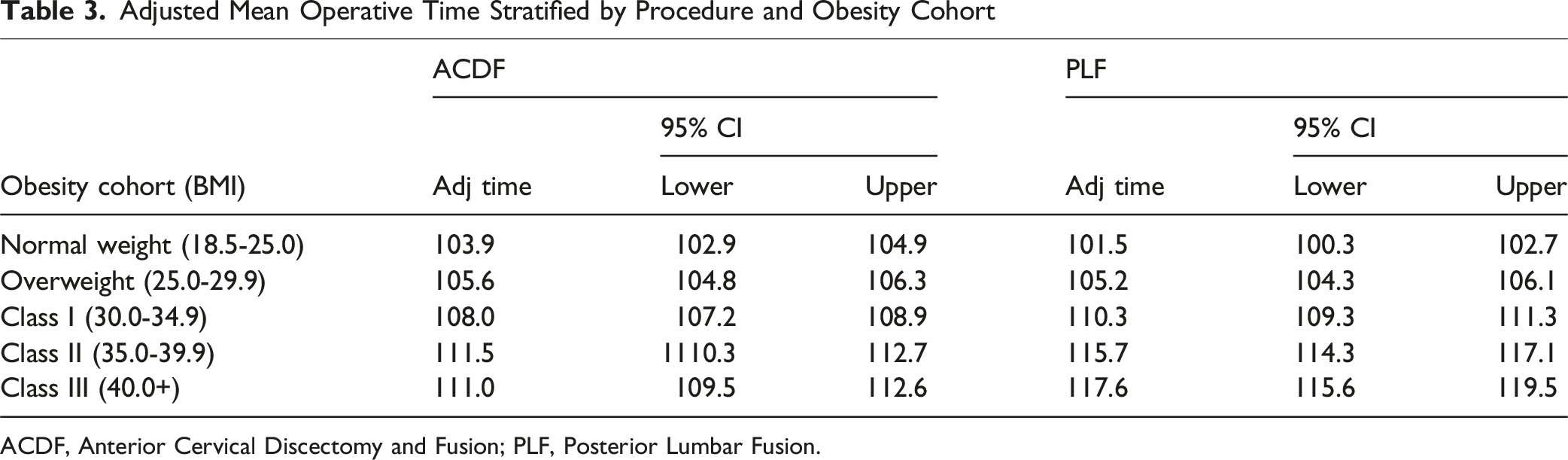
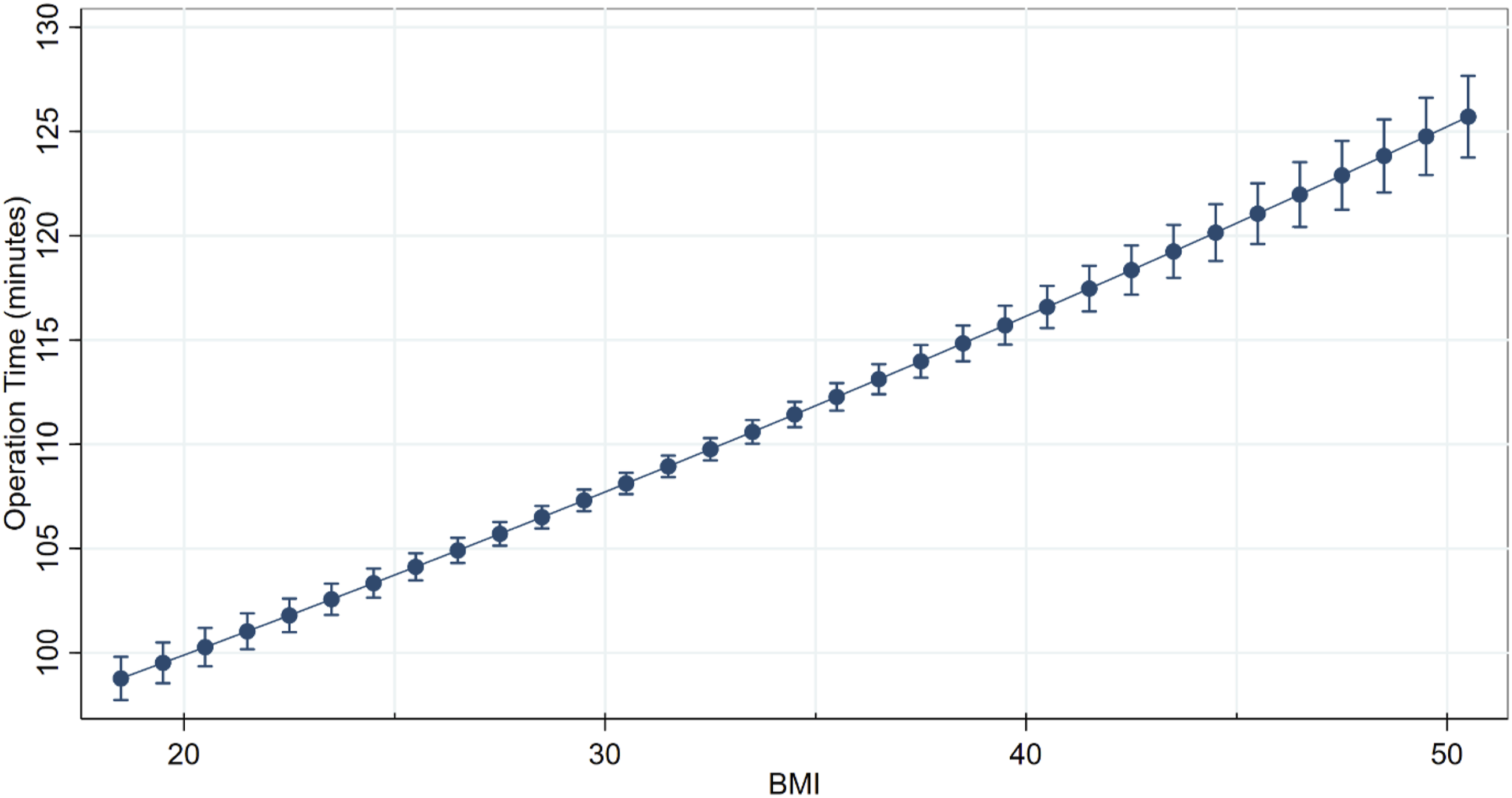
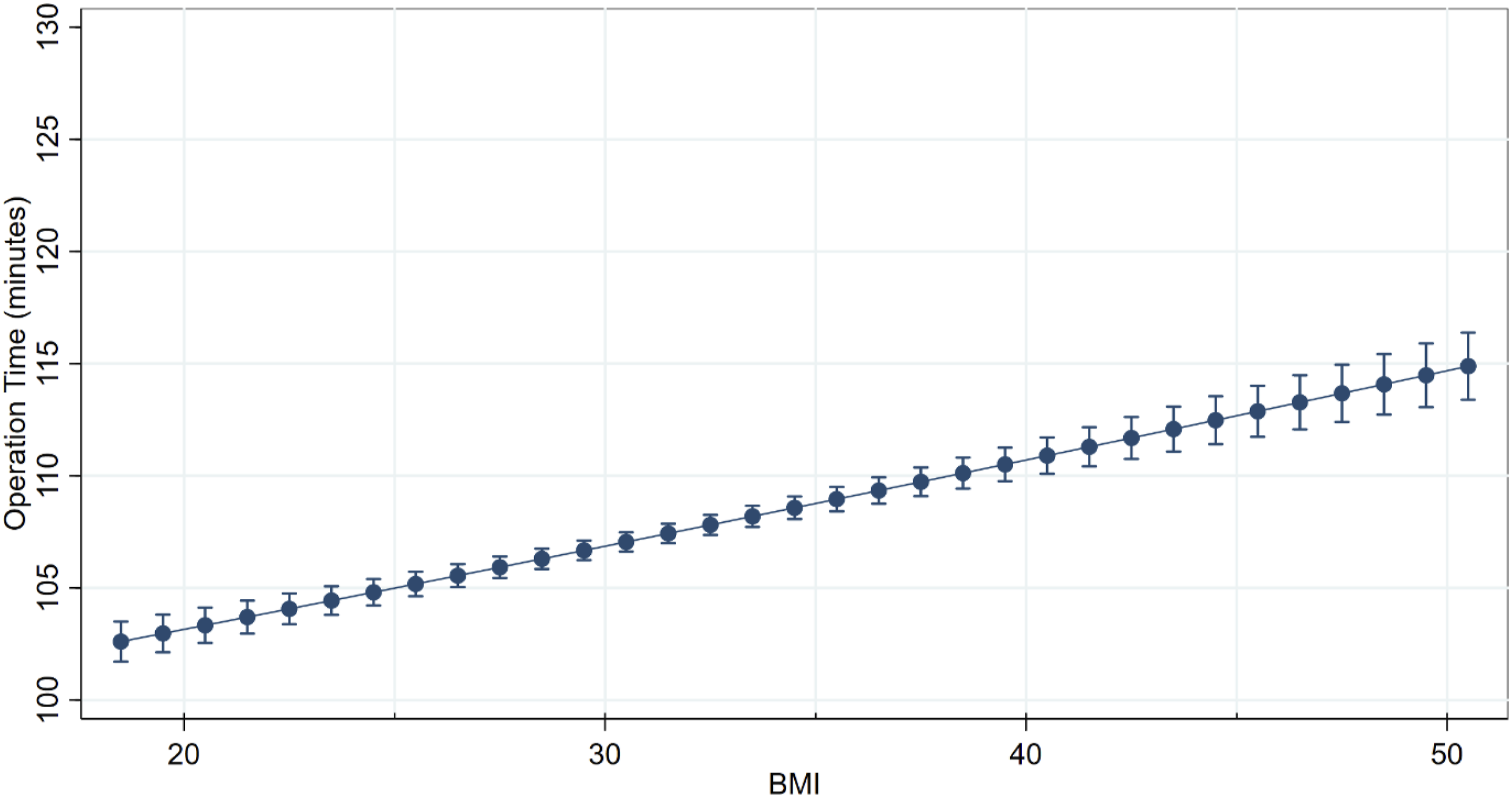
The mean unadjusted operative time for all single-level ACDF procedures was 107.2 ± 55.6 minutes while the mean for all single-level PLF procedures was 108.6 ± 71.3 minutes. After adjusting for confounding factors, obese class III increased operative time by 16% relative to normal-weight patients in single-level PLF vs 7% in single-level ACDF (Figure 1 and Table 3). The incremental increase in operative time for every unit of body mass index above 18.5 kg/m2 was assessed for both procedures. Every one-unit increase in BMI independently increased the mean operative time for a single-level PLF procedure by 0.84 minutes, with an average operative time of 82.7 minutes before the influence of BMI is considered (Figure 2). For a single-level ACDF procedures, a unit increase in BMI only increased operative time by 0.38 minutes with an average operative time of 95.4 minutes before BMI is considered (Figure 3). Adjusted Mean Operative Time for Single-Level Anterior Cervical Discectomy and Fusion and Single-Level Posterior Lumbar Fusion by Body Mass Index Cohort Adjusted Mean Operative Time Stratified by Procedure and Obesity Cohort ACDF, Anterior Cervical Discectomy and Fusion; PLF, Posterior Lumbar Fusion. Adjusted Mean Operative Time for Single-Level Posterior Lumbar Fusion by Body Mass Index Adjusted Mean Operative Time for Single-Level Anterior Cervical Discectomy and Fusion by Body Mass Index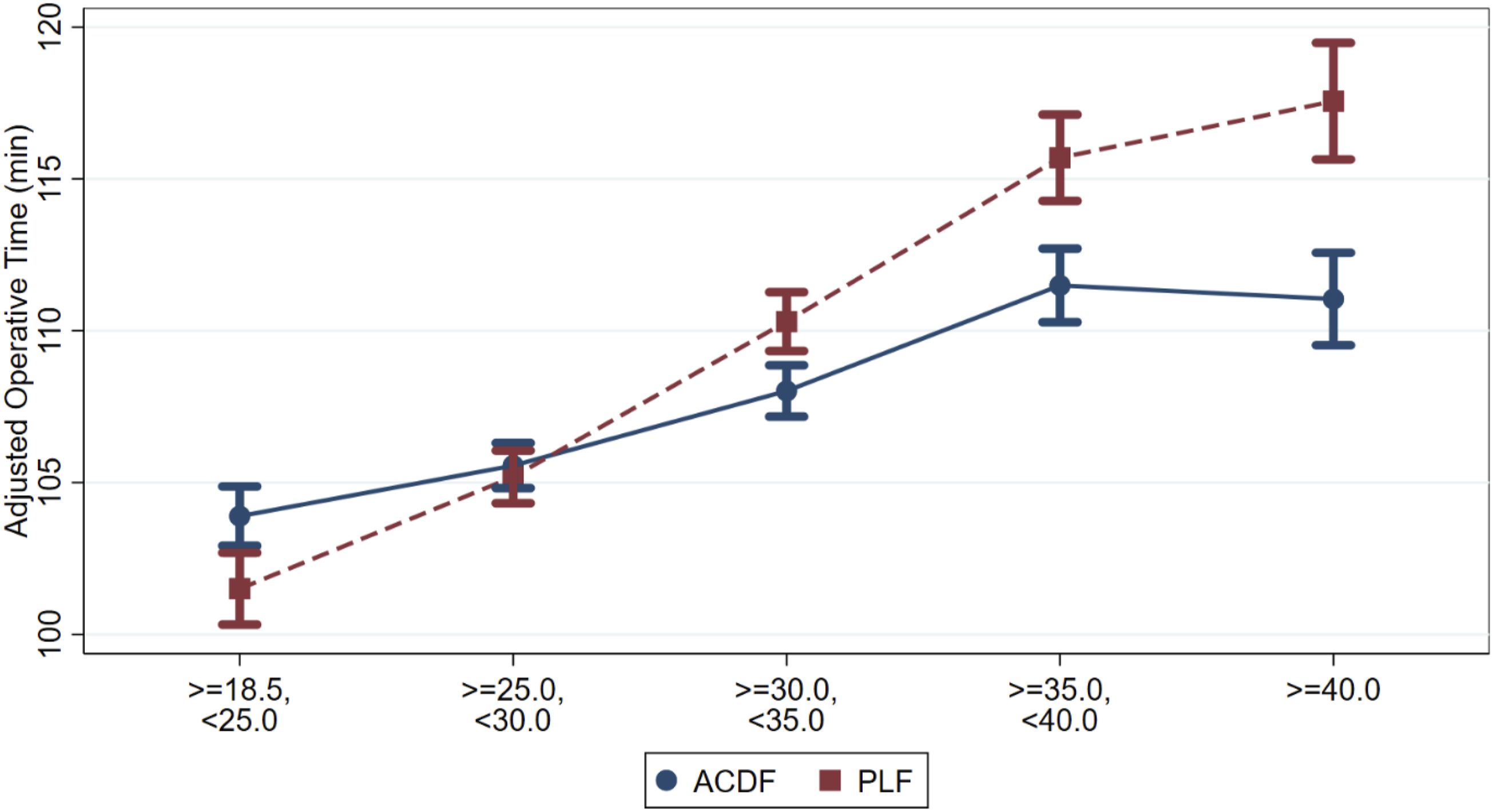
Surgical Infections and Wound Complications
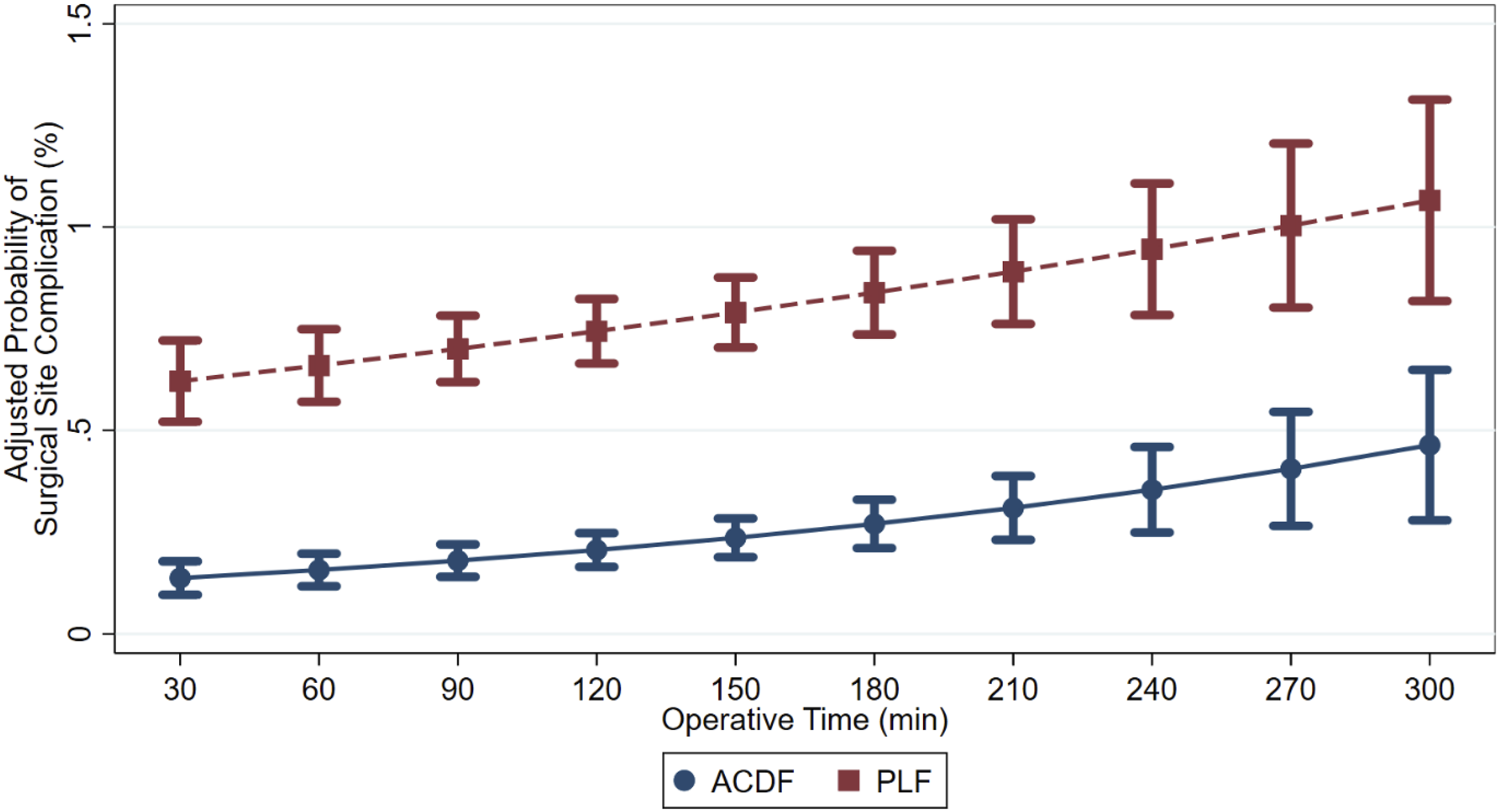
After controlling for confounders, the probability of a wound complication after a single-level PLF procedure increased by 19.7% as operative time increased from the 25th to 75th percentile quartiles (Figure 4). Similarly, the probability of a wound complication after single-level ACDF procedures increased by 17.1% for the same range. Notably, the probability of a postoperative surgical infection increased by 30.0% for ACDF procedures and 12.5% for PLF procedures as the operative time increased from the 25th to 75th percentile quartiles (Figure 5 and Table 4). Adjusted Probability for Wound Complications after Single-Level Anterior Cervical Discectomy and Fusion and Single-Level Posterior Lumbar Fusion by Body Mass Index Adjusted Probability for a Surgical Infection after a Single-Level Anterior Cervical Discectomy and Fusion and Single-Level Posterior Lumbar Fusion by Operative Time Mean Adjusted Operative Time and Complication Probability Stratified by Procedure and Body Mass Index Cohort ACDF, Anterior Cervical Discectomy and Fusion; PLF, Posterior Lumbar Fusion.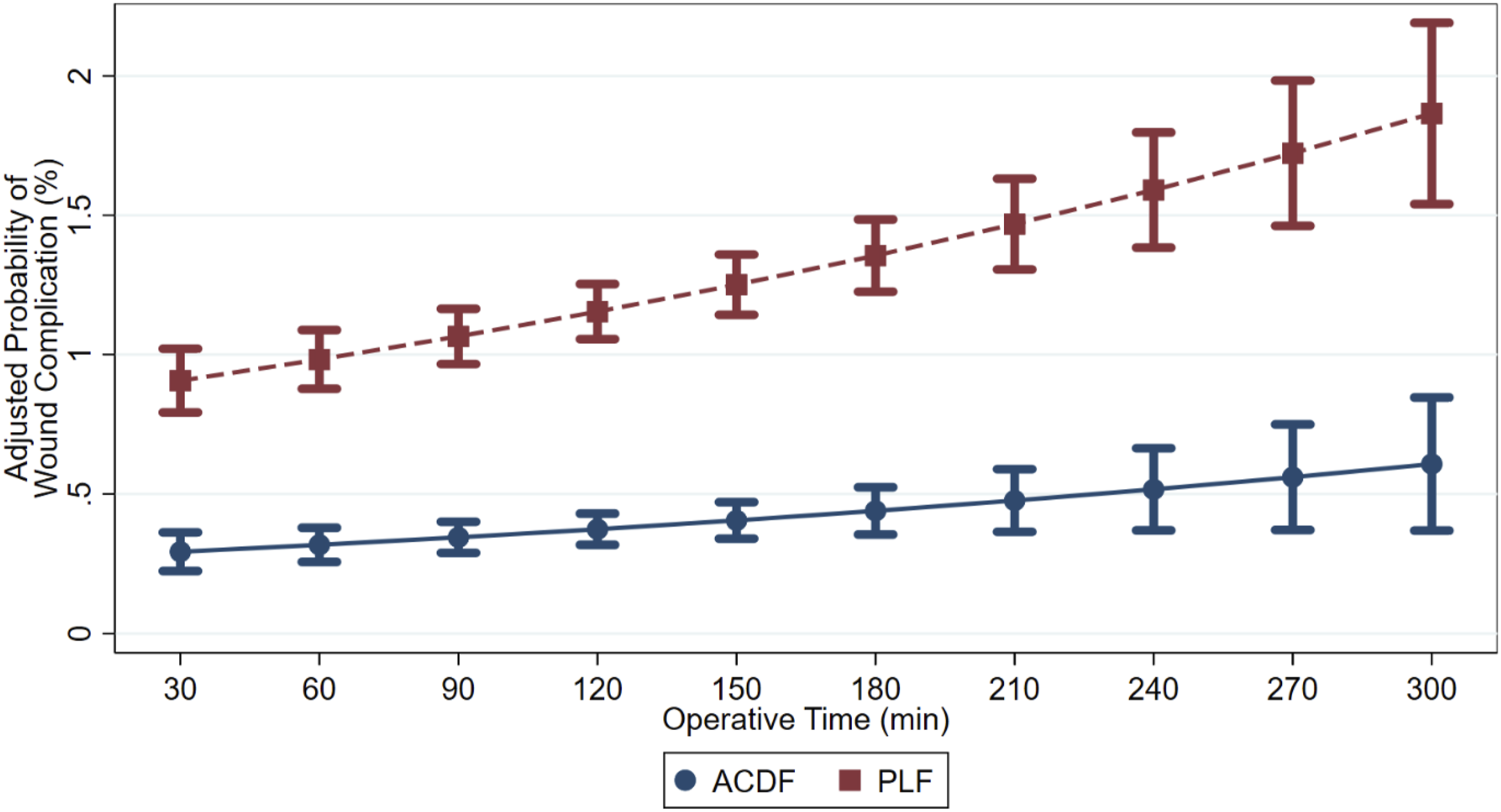

Discussion
The present study compared the incremental impact of BMI and obesity level in a national population of patients undergoing a single-level ACDF or single-level PLF over a 12-year period. Notably, obese class III increased ACDF operative times by 7% and PLF operative times by 16% after adjusting for confounders. For every increase in one unit of BMI, PLF operative times increased by 0.84 minutes, while ACDF operative times increased by 0.38 minutes. As operative time increased, the probability of wound complications increased at a higher rate in single-level PLF procedures compared to ACDF procedures. Overall, obesity was associated with a prolonged operative time, which independently increased the probability of wound complications and surgical infections in both ACDF and PLF procedures.
The relationship between obesity and an increased operative time has previously been shown in orthopaedic and spine literature.11,25-32 For patients undergoing total shoulder arthroplasty, patients with a mean BMI over 35 kg/m2 had a surgical time 12 minutes greater than the normal BMI cohort. 26 One additional study assessing the impact of obesity on operative time among patients undergoing arthroscopic rotator cuff repair observed that patients with a BMI >30 had a longer operative time compared to nonobese patients. 27 Similarly, Cooper et al. observed class II obesity increased operative time by 7.11 minutes while class III increased operative time by 8.70 minutes during anterior cruciate ligament reconstruction surgery. 31 However, few studies have examined the influence of obesity on operative time in spine surgery. Higgins et al determined that obesity increased operative time during instrumented spinal fusion surgery, 32 a finding supported by Buerba et al, who found that obese class III increased total time in the operating room (OR) by 13.2 minutes in patients undergoing various lumbar spine procedures. 11 Within the present study, we observed a significant increase in operative time for both ACDF and PLF procedures as BMI increased. However, obesity had a greater influence on operative time during PLF procedures as compared to ACDF procedures. This is particularly important as our study highlights obesity may influence cervical and lumbar spine procedures differently.
The presence of obesity increases the complexity of spine surgery, which can be attributed to challenges with exposure, difficulty with accurate instrumentation, and a larger depth of field during decompression. These surgical challenges are often anecdotally more prominent during a PLF compared to an ACDF, secondary to the patient’s anatomy in the lumbar vs cervical spine. For example, the amount of adipose tissue, muscle thickness, and spine depth tends to be greater in the posterior lumbar spine as compared to the anterior cervical spine. This anatomical difference may increase dissection time in PLFs more significantly compared to ACDFs in obese patients. Secondly, at the caudal lumbar levels, which are more frequently surgically addressed, pedicle screws have a significant lateral-to-medial trajectory, requiring precise anatomical localization and planning.33-35 In obese patients, the deep subcutaneous adipose tissue layer significantly limits visibility and increases the difficulty of accessing anatomical landmarks necessary for correct screw trajectory. Larger soft tissue envelopes necessitate more extensive retraction, which can hinder proper instrumentation despite fluoroscopic or navigation assistance. Compared to PLF, instrumentation in an ACDF does not require as wide of a lateral dissection and accurate placement does not place as much tension on the soft tissues due to the midline location of instrumentation. As such, time for ACDF instrumentation may exhibit less of an increase due to obesity as compared to PLF instrumentation.
Aside from technical considerations that may explain changes in operative time associated with obesity, it is important to consider the over-arching effect of increased operative time on patient outcomes. Operative time and obesity have been previously identified as risk factors for complications, including wound complications or surgical infections.17-19 After adjusting for comorbid conditions, including obesity, and other confounding factors in the present study, we found that an increase in operative time was associated with higher rates of both wound complications and infections following both ACDFs and PLFs, with particularly prominent increases in wound complications following PLFs. Although comorbid conditions often contribute to the increased risk for wound complications or surgical infections in the perioperative period, various time-related factors such as prolonged open surgical incision, diminished efficacy of antimicrobial prophylaxis over time, and violations in sterile technique due to increased procedure time, might be contributing factors.36-38 Though it is difficult to fully isolate the effect of technical aspects that may increase operative time vs inherent metabolic or nutritional issues that could influence post-operative healing, the present study highlights the need to further examine this issue to better understand potential avenues for improvement.
Limitations
Several limitations must be acknowledged. The ACS-NSQIP database collects information on an extensive set of predefined variables, which excludes detailed clinical information (eg, surgical technique and severity of complications) and specific spine surgery outcomes (eg, pseudoarthrosis). The database also fails to define pertinent surgical information, including the specific time from skin incision to closure. Furthermore, the database does not incorporate data on the surgeon’s surgical experience, technique, specific perioperative protocols, and hospital case-volume data. Previous spine surgery literature has demonstrated that both increased years of experience and case volumes have been significantly associated with shorter operative times.39,40 The CPT codes used to define single-level posterior decompression and fusion could be used to define different surgical techniques, including cortical trajectory pedicle screws, which would not require as extensive a lateral dissection. Additionally, while separate codes exist for placement of percutaneous pedicle screws and minimally invasive decompression techniques, there may be some cases in this database in which the surgeons used a mixed minimally invasive and open technique such as percutaneous pedicle screw placement with concomitant open decompression. The present study was unable to adjust for procedure details hidden with CPT codes including the use of only minimally invasive techniques vs open procedures, minimally invasive fusion with open decompression, or the use of navigation. Given procedural characteristics may affect operative time, future studies are needed to account for the effect of individual techniques used. Furthermore, preoperative imaging is not available in the database. Thus, the authors are unable to determine the severity of preoperative cervical or lumbar pathology. Given excess fat is distributed across many body compartments, local adipose deposition in the cervical and lumbar spine may vary greatly for each BMI. The database only incorporates data up to 30 days after a procedure. Therefore, the retrospective nature of the study design limits our ability to establish cause-effect relationships. To gain a more comprehensive understanding of a direct factor influencing operative time in patients with obesity, future multicenter prospective cohort trials are recommended.
The conclusions reached in this paper may not be applicable to multi-level lumbar decompression and fusions due to the larger incision required for these procedures. With multilevel lumbar decompression and fusion, there may be overall less soft tissue tension which could mitigate surgical challenges and as a result not increase total operative time as significantly as what was observed in single level fusions. As such, further studies would be needed to better quantify the effect of obesity on multi-level procedures.
Conclusion
Patients with obesity are at significantly increased risk of longer operative times following both anterior cervical discectomy with fusion and posterior lumbar fusion procedures. Patients undergoing lumbar fusion procedures had a greater increase in operative time per unit of BMI compared to patients undergoing cervical fusion procedures. Increased operative time is independently associated with increased risk of wound complications and surgical infections in the perioperative period. This study enhances risk stratification for patients with obesity and helps surgeons better counsel their patients in the preoperative setting.
Supplemental Material
Supplemental Material - The Impact of Obesity on Spine Surgery Operative Time: A Quantitative Analysis
Supplemental Material for The Impact of Obesity on Spine Surgery Operative Time: A Quantitative Analysis by Haseeb E. Goheer, BS, Mina Botros, MD, Andrew R. Leggett, MD, Gabriel Ramirez, MS, Ram Haddas, PhD, Robert W. Molinari, MD, and Varun Puvanesarajah, MD in Global Spine Journal.
Footnotes
Author Contributions
All authors intellectually contributed to and approved the final version to be published. HEG: Conceptualization, Writing- original draft, Writing-review & editing, Methodology, Formal Analysis. MB: Writing- original draft, Writing-review & editing, Conceptualization. ARL: Writing- original draft, Writing-review & editing G.R.: Writing-review & editing, Methodology, Formal Analysis. R.H.: Writing-review & editing. RWM: Writing-review & editing, Supervision, Project Administration. V.P. Conceptualization, Writing- original draft, Writing-review & editing, Methodology, Supervision, Project Administration.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. HEG, MB, ARL, GR, RWM, and VP have nothing to disclose. RH is a paid consultant for Medtronic and receives grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, Scoliosis Research Society, Medtronic, and Zimmer Biomed.
Data Availability Statement
Data sharing is not applicable as no new data was generated.
IRB Statement
The study received Institutional Review Board approval under Study Protocol #00009641. The Institutional Review Board waived the requirement for informed consent to participate.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.