
Abstract
Study Design:
Retrospective analysis of prospectively collected data.
Objective:
There is a paucity of data on the effect of operative duration on postoperative complications during adult spinal deformity surgery (ASDS). The study attempts to explore and quantify the association between increased operation times and postoperative complications.
Methods:
A retrospective cohort analysis was performed on the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2010 to 2014. Patients (≥18 years of age) from the NSQIP database undergoing ASDS were separated into cohorts based on quartiles of operation duration. Chi-square and multivariate logistic regression models were used to identify risk factors.
Results:
A total of 5338 patients met the inclusion criteria and were divided per quartiles based on operative duration in minutes (154, 235, 346, and 1156 minutes). Multivariate logistic regressions revealed that in comparison to the lowest quartile of operative duration, the highest quartile group was associated significantly with length of stay ≥5 days (odds ratio [OR] = 5.85), any complication (OR = 9.88), wound complication (OR = 5.95), pulmonary complication (OR = 2.85, P = .001), venous thromboembolism (OR = 12.37), intra-/postoperative transfusion (OR = 12.77), sepsis (OR = 5.27), reoperations (OR = 1.48), and unplanned readmissions (OR = 1.29). The odds ratio was higher when comparing a higher quartile group with the reference group across all associations. P < .001 unless otherwise noted.
Conclusion:
ASDS operation time is associated with multiple postoperative complications, including, but not limited to, wound and pulmonary complications, venous thromboembolism, postoperative transfusion, length of stay ≥5 days, sepsis, reoperation, and unplanned readmission.
Introduction
The prevalence of spinal deformity disorders and adult spinal deformity surgery (ASDS) is becoming increasingly prevalent, particularly in the elderly population. 1,2 ASDS involves a range of etiologies including degenerative scoliosis, idiopathic scoliosis, iatrogenic deformity, and coronal and sagittal imbalance. 3 Symptoms are often associated with progressive and asymmetric degeneration of the spinal structures, which may potentially lead to neural element compression. 4 There has been increasing focus on understanding the contributing factors to perioperative and late complications. 5 -8 A recent meta-analysis reported an overall complication rate of 41.2% and pseudarthrosis rate of 12.9%. 9 Improved understanding of the risk factors and predictors of surgical complications following ASDS may play a role in improved patient selection, which may help improve cost-effectiveness and optimize health care planning.
Prolonged operation duration (OD) has been identified as a potential risk factor for unfavorable outcomes such as surgical site infections and cardiorespiratory complications for a variety of procedures including general, vascular, and orthopedic surgery. 10 -17 Few studies have focused on the role of prolonged OD as a risk factor for postoperative surgical complications following spine surgery. In the context of spine surgery, Kim et al 18 investigated 4588 patients who underwent lumbar fusion, and they demonstrated that OD was significantly associated with overall complications, medical complications, surgical complications, superficial site infections, and postoperative transfusions. OD prolonged beyond 5 hours was associated with increased risk of reoperation, organ/space surgical site infection, sepsis/septic shock, wound dehiscence, and deep vein thrombosis. Although operative duration can plausibly be considered with limited applicability as a direct predictor for most postoperative outcomes, its significance as a proxy variable reflecting technical complexity of a procedure, level of training and expertise, and measure of blood loss cannot be undermined.
With regard to ASDS, limited literature exists on the impact of OD on patient outcomes. Therefore, we sought to investigate the ACS-NSQIP database to evaluate any associations between prolonged OD and postoperative complications in patients undergoing ASDS. We hypothesize that longer surgery duration would be associated with greater rates of postoperative complications.
Methods
Data Source
The ACS-NSQIP was originally created as a quality improvement initiative for the Veteran’s Administration health system in 1994. It has since expanded to the private sector after its initial success in the Veteran’s Administration system. 19,20 Details of the ACS-NSQIP (www.acsnsqip.org) have been described before and its use has been well established in the surgical literature. It is a validated outcomes registry that allows assessment of 30-day risk-adjusted surgical morbidity and mortality in order to provide feedback to participating hospitals.
The database consists of more than 150 preoperative, intraoperative, and 30-day postoperative variables that are collected prospectively from medical records and operative reports among other sources by on-site surgical clinical reviewers. Data is gathered through the entirety of the 30-day postoperative period, including patients discharged within this time period or treated on an outpatient basis.
Data Collection
The data in the NSQIP database from 2010 to 2014 was used in this study. Adult patients (≥18 years) undergoing adult deformity surgery were identified based on Current Procedural Terminology (CPT) codes 22800, 22802, 22804, 22808, 22810, 22812, 22818, 22819. CPT codes 22843, 22844, 22846, or 22847 were also included to capture long, multilevel fusion constructs. Patients with CPT codes 22842 and 22845 were included if they had an ICD-9 diagnosis for spinal deformity (including 737.1, 737.2, 737.3, 737.4, 737.8, 737.9). Cases with age <18 years of age; missing preoperative data; emergency cases; patients with a wound class of 2, 3, or 4; an open wound on their body; current sepsis; current pneumonia; prior surgeries within 30 days; cases requiring cardiopulmonary resuscitation prior to surgery; any patients undergoing a nonelective procedure; or cases with diagnoses of cervical spine, trauma or injury to spine, or neoplasm of spine were excluded in order to reduce the risk of confounding variables.
Variable Definitions
Patient demographic variables included age (≤50, 51-60, 61-70, 71-80, >80), sex, and race (white, black, Hispanic, and other). Other race included American Indian, Alaska Native, Asian, Native Hawaiian, Pacific Islander, or unknown/not reported. Preoperative variables included obesity (≥30 kg/m2), diabetes (non–insulin-dependent diabetes mellitus or insulin-dependent diabetes mellitus), current smoking (within 1 year of surgery), dyspnea (≤30 days prior to surgery), functional status prior to surgery (independent or partially/totally dependent ≤30 days prior to surgery), pulmonary comorbidity (ventilator dependent ≤48 hours prior to surgery or history of chronic obstructive pulmonary disease ≤30 days prior to surgery), cardiac comorbidity (use of hypertensive medication or history of chronic heart failure ≤30 days prior to surgery), renal comorbidity (acute renal failure ≤24 hours prior to surgery or dialysis treatment ≤2 weeks prior to surgery), steroid use for chronic condition (≤30 days prior to surgery), ≥10% loss of body weight (in the last 6 months), bleeding disorder (chronic, active condition), preoperative transfusion of ≥1 unit of whole/packed red blood cells (≤72 hours prior to surgery), and American Society of Anesthesiologists class (≥3).
Intraoperative variables included fusion length (long fusion is ≥4 levels during an anterior approach and ≥7 levels during a posterior approach), surgical approach (posterior, anterior, or combined), fusion to pelvis, and osteotomy. Thirty-day postoperative outcome variables include mortality, any postoperative complication, length of stay (LOS; ≥5 days), wound complication (superficial or deep surgical site infection, organ space infection, or wound dehiscence), pulmonary complication (pneumonia, unplanned reintubation, or duration of ventilator-assisted respiration ≥48 hours), venous thromboembolism (VTE; pulmonary embolism or deep vein thrombosis), renal complication (progressive renal insufficiency or acute renal failure), urinary tract infection (UTI), peripheral nerve injury, cardiac complication (cardiac arrest requiring cardiopulmonary resuscitation or myocardial infarction), intra-/postoperative red blood cell transfusion, sepsis, central nervous system complication (cerebrovascular accident or coma), reoperation (related to initial procedure), and unplanned readmission (related to initial procedure). Patients were separated and compared according to OD quartiles. The OD for each quartile was as follows: 154 minutes, 235 minutes, 346 minutes, and 1156 minutes.
Statistical Analysis
Descriptive and comparative statistics of demographics, comorbidities, operative details, and postoperative complications were analyzed for all patients. Univariate analyses were performed on patient demographic, preoperative, intraoperative, and postoperative characteristics using Pearson’s χ2 test. Fischer’s exact test was used where appropriate. Multivariable logistic regression analysis, adjusting for preoperative and intraoperative factors, with stepwise entry and removal criteria set to a significance level of .05, was performed to identify the association between operative duration and the occurrence of acute postoperative complications. The C-statistic, which is the area under the receiver operating characteristic curve, was also retrieved from the predictors of postoperative outcomes models and determined the accuracy of this model. The area under this curve measures the ability of the model to correctly classify those with the complication and those without. SAS Studio Version 3.4 (SAS Institute Inc, Cary NC) was used for all statistical analysis.
Results
The present study identified 5338 patients who underwent ASDS from the ACS-NSQIP database (Table 1). Patients were subdivided per operation time quartiles: first (n = 1346, 154 minutes), second (n = 1355, 235 minutes), third (n = 1320, 346 minutes), and fourth (n = 1317, 1156 minutes). The interquartile range of operative time was 192 minutes. In terms of baseline demographics, there was no significant difference in the proportion of females (P = .343) or obese patients (P = .718). There was a marginally higher proportion of white patients in the lowest quartile for operative time compared to the highest quartile (83.1% vs 80.4%, P < .001). There was a statistically significant differential distribution of patients by age into the 4 operation time quartiles, with older patients tending to require longer operations. The fourth quartile for operation time also had a significantly lower proportion of patients with diabetes (12.4% vs 15.5%, P = .008), smokers (17% vs 25.8%, P < .001), dyspnea (6.6% vs 7.5%, P = .001), and totally or partially functionally dependent (6.2% vs 3.8%, P < .001) compared to the first quartile.
Patient Demographics and Preoperative and Intraoperative Characteristics Between Operative Time Quartiles (N = 5338).a
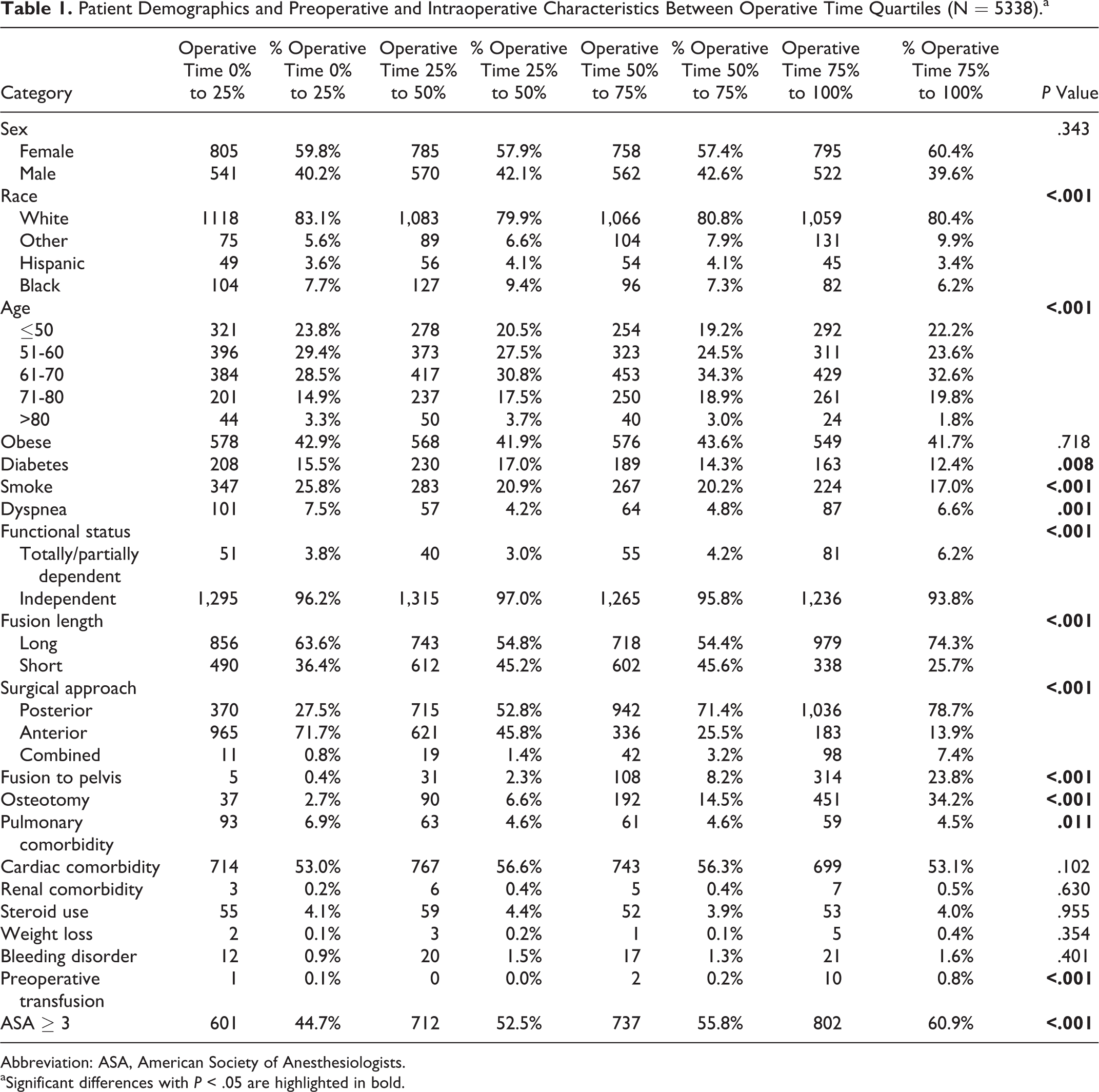
Abbreviation: ASA, American Society of Anesthesiologists.
aSignificant differences with P < .05 are highlighted in bold.
In terms of surgical variables, long fusions (long fusion is ≥4 levels during an anterior approach and ≥7 levels during a posterior approach) were more frequent in the fourth quartile compared to first quartile (74.3% vs 63.6%, P < .001). Patients with longer OD were more likely to undergoing surgery via a posterior approach (78.7% vs 27.5%, P < .001), more likely to have a fusion to pelvis (23.8% vs 0.4%, P < .001), and undergo osteotomy (34.2% vs 2.7%, P < .001) when comparing fourth quartile to first quartile, but also with increasing quartile (Table 1).
In terms of baseline comorbidities, patients in the fourth quartile were less likely to have pulmonary comorbidity (4.5% vs 6.9%, P = .011), more likely to require transfusions (0.8% vs 0.1%, P < .001), and more likely to have American Society of Anesthesiologists class ≥3 (60.9% vs 44.7%, P < .001), when comparing the fourth quartile versus first quartile for operative time. No significant differences were found between the cohorts in terms of cardiac comorbidity, renal comorbidity, steroid use, recent weight loss, or bleeding disorders.
Univariate Analysis of Complications
The proportion of patients with any complication was significantly higher in the fourth quartile compared to first quartile of operative time (66.4% vs 7.4%, P < .001). There was a higher mortality rate with prolonged OD, when comparing fourth and first quartiles (1.0% vs 0.1%, P = .012). For the quartile with the longest operative time, patients had significantly increased LOS ≥5 days (56.8% vs 8.6%, P < .001), wound complication (4.5% vs 0.7%, P < .001), pulmonary complications (5.8% vs 1.1%, P < .001), VTE (4.0% vs 0.1%, P < .001), UTI (3.4% vs 1.0%, P < .001), intra-/postoperative transfusions (62.3% vs 5.1%, P < .001), sepsis (3.5% vs 0.6%, P < .001), reoperations (6.2% vs 2.1%, P < .001), and unplanned readmissions (8.7% vs 4.0%, P < .001), when compared to the lowest quartile for operative duration. No significant difference between the groups was found in terms of renal complications, cardiac complications, peripheral nerve injury, graft failure, or central nervous system complications (see Table 2).
30-Day Postoperative Outcomes Between Operative Time Quartiles (N = 5338).a
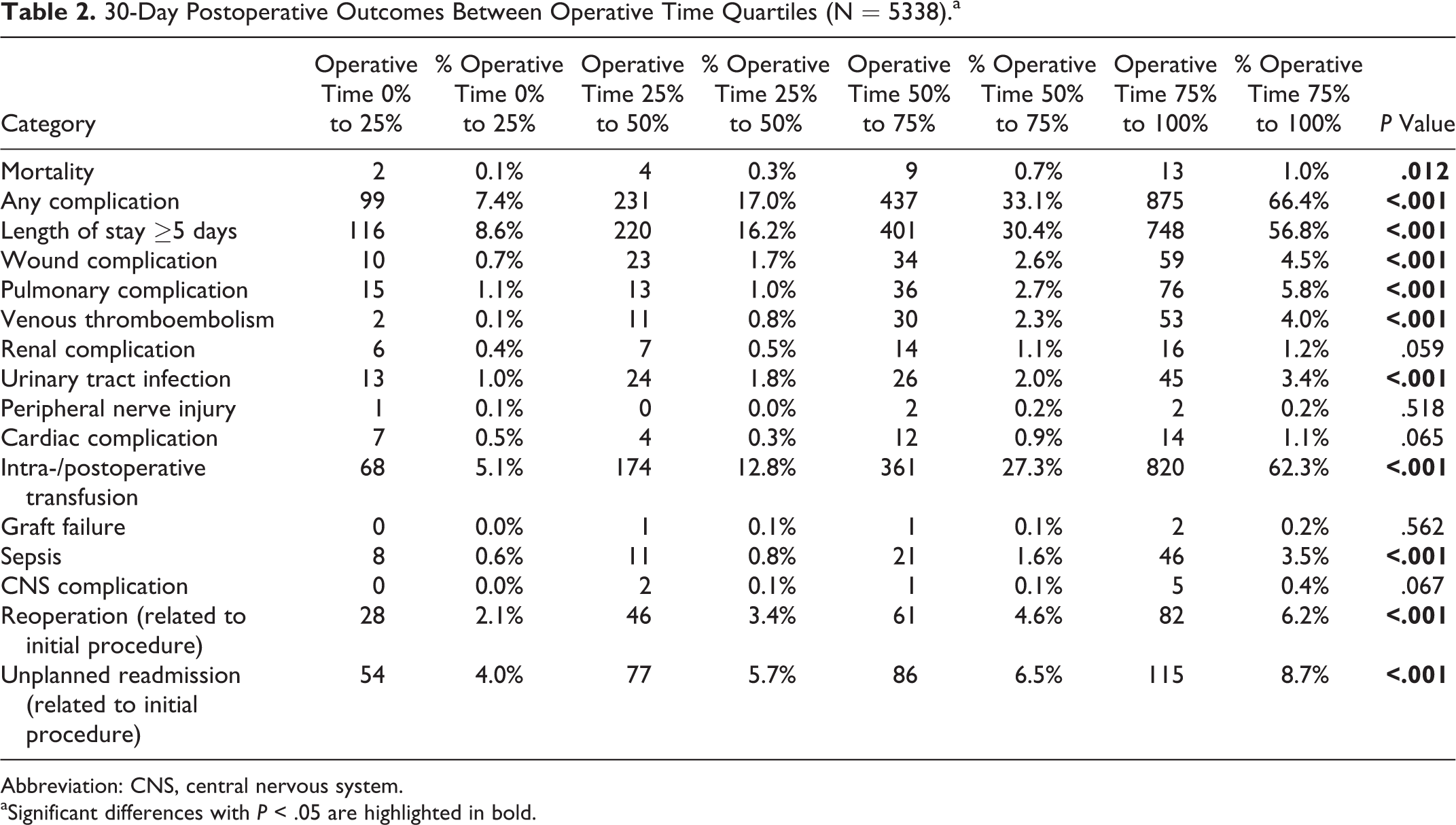
Abbreviation: CNS, central nervous system.
aSignificant differences with P < .05 are highlighted in bold.
Multivariate Analysis of Complications
Following multivariate adjustment for potential confounders, having a prolonged operative time was found to be significantly associated with LOS ≥5 days (fourth vs first quartile, odds ratio [OR] = 5.82, 95% confidence interval [CI] = 4.61-7.35, P < .001), any complication (OR = 9.88, 95% CI = 7.71-12.66, P < .001), wound complication (OR = 5.95, 95% CI = 3.31-11.34, P < .001), pulmonary complication (OR = 2.85, 95% CI = 1.53-5.32, P = .0001), VTE (OR = 17.09, 95% CI = 5.27-55.45, P < .001), intra-/postoperative transfusions (OR = 12.77, 95% CI = 9.64-16.92, P < .001), sepsis (OR = 5.27, 95% CI = 2.66-10.44, P < .001), reoperations (OR = 1.48, 95% CI = 1.48-3.74, P < .001), and unplanned readmissions (OR = 1.84, 95% CI = 1.29-2.64, P = .001) (see Figure 1). For all significant associations, a higher strength of association or odds ratio was found with higher quartile of OD (see Table 3).
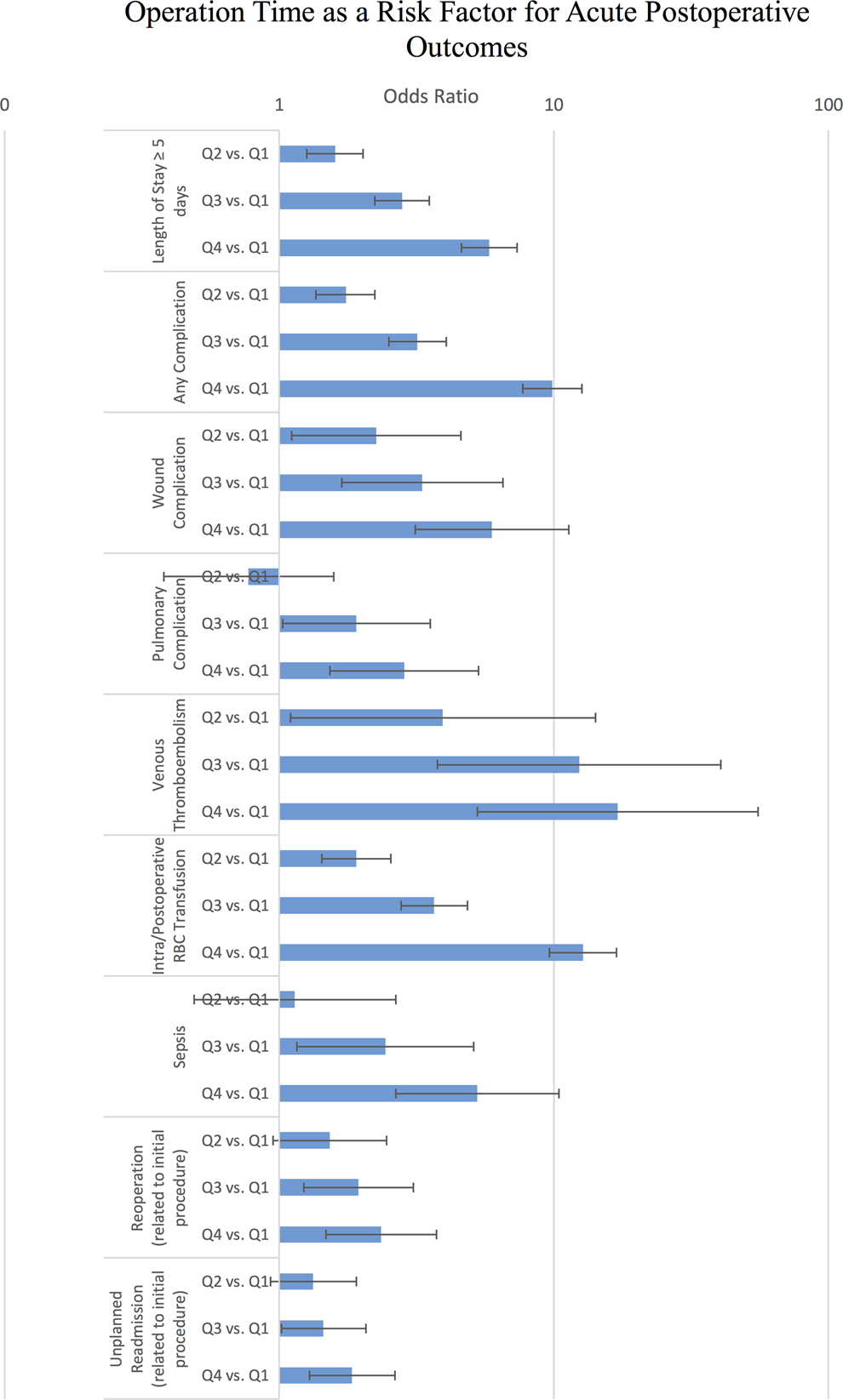
Bar graph illustrating odds ratios of increasing operation time on acute postoperative outcomes following elective ASDS.
Quartiles of Operative Time as a Risk Factor for 30-Day Postoperative Outcomes (N = 5809).a
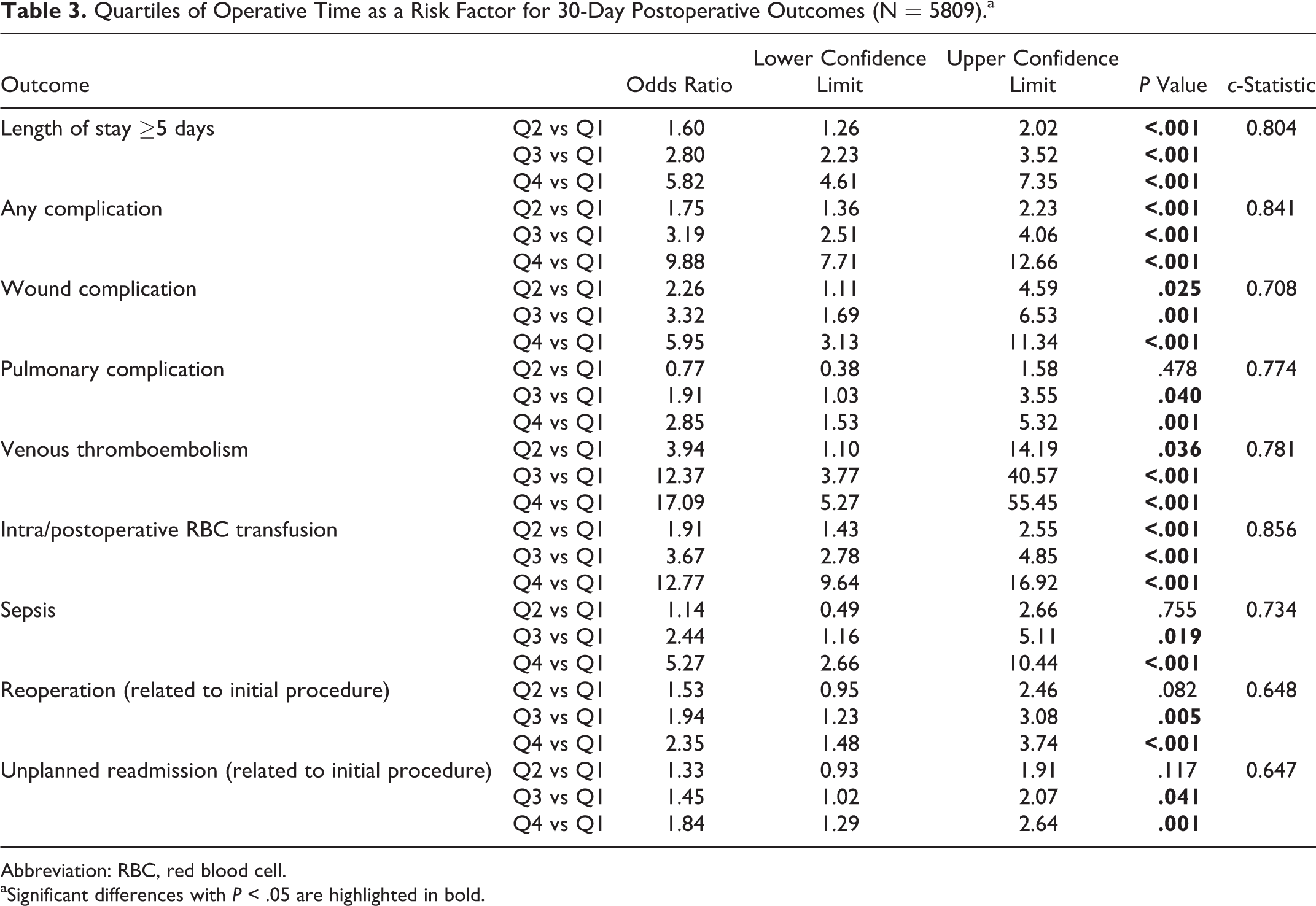
Abbreviation: RBC, red blood cell.
aSignificant differences with P < .05 are highlighted in bold.
Discussion
The impact of increased OD on postoperative outcomes has been described in the general surgical literature, 21,22 associated with various medical and surgical complications. 18,21,23,24 This relationship has not been extensively explored in the context of spinal deformity procedures. Being able to identify patients at risk for postoperative complications following ASDS and understanding the impact of OD on these risks may useful for optimizing discharge pathways and streamlining postoperative care for such patients. The present analysis demonstrated that prolonged OD for ASDS was significantly associated with increased wound and pulmonary complications, VTE, intra-/postoperative transfusion, LOS, sepsis, reoperation, and unplanned readmissions. Our findings imply that surgical duration may be an important quality metric when considering the performance and safety of ASDS.
Prior investigations have proposed potential associations between extended OD and a variety of postoperative complications, including increased infection and thromboembolic rates following knee arthroplasty, 10,25 infections following tibial plateau fractures, 26 surgical complications following laparoscopic cholecystectomy, 16 blood transfusion requirements following pancreatoduodenectomy, 17 infections following abdominal or vaginal hysterectomy, 27 as well as cardiorespiratory complications following general surgery. 28 It is not clear whether prolonged OD is an independent risk factor for postoperative morbidity, or rather is a reflection of the complexity of the type of procedure or patient health. 29,30 Furthermore, it is not clear whether this relationship holds for ASDS, which often involve complex, multilevel fusions that are prone to longer procedural durations and higher risk of complications.
In the present study, we examined OD as a potential risk factor for postoperative complications for ASDS. Prior to risk adjustment, analysis of primary outcomes suggested that prolonged OD was associated with LOS ≥5 days, any complication, higher wound complications, pulmonary complications, VTE, renal complications, UTI, transfusions, sepsis, reoperations, and unplanned readmissions. Further assessments of these trends were made using multivariate logistic regression to adjust for potential confounders. We found that prolonged OD remained significantly associated with these complications, and that the strength of association was stronger with higher quartile of OD. These results corroborate findings reported in the previous literature and suggest the utility of using OD as a quality metric for performance and outcomes of ASDS.
Our results, as well as prior literature, support a consistent association between prolonged OD and risk of postoperative infections. Peersman et al 10 investigated 113 infected patients after total knee arthroplasty who were matched with 236 controls. Infected patients were found to have significantly longer operation times compared to controls. Colman et al 26 also reported longer OD as significantly associated with surgical site infection in patients who sustained tibial plateau fractures. Increased OD results in increased surgical site exposure to the operating room surroundings, as well as increased duration of disrupted vascular supply to the wound site, which would likely translate into higher infection rates.
Traditionally, one method of assessing centers of excellence was based on the volume metric, with high-volume centers for lumbar spine surgery associated with superior outcomes. 31,32 An analysis of the National Inpatient Sample data from 1992 to 2005 demonstrated that for patients undergoing lumbar decompression with fusion, mortality and complication rates were lower when patients were treated by high-volume surgeons and hospitals. 31 This association has not been as well explored or documented in ASDS, with complication rates ranging from 37% to 78% in recent reports. 33 -36 This broad range may in part reflect the diverse range of case complexity and surgeon experience with ASDS from hospital to hospital. Several studies have suggested that the use of operative time may be an alternative measure of surgeon quality in various surgical specialties. 17,19,37,38 The results of the present study support the hypothesis that shorter operative times may also provide an alternative assessment of surgical skills and outcomes. It has been suggested that once the “learning curve” of a procedure has been traversed by newer, lesser experienced trainees for complex cases, the annual volume may not be significantly associated with outcome. 39 -41 As such, operative time may be an alternative objective measure of surgical proficiency and quality in this context.
Limitations
The present study is constrained by several limitations. First, the NSQIP database is susceptible to selection bias, representative only of hospitals participating in the program. The data collected is biased toward academic programs and thus not reflective of the whole population. Centers included in the NSQIP program are predominantly academic centers and as such resident involvement in cases could be a potential confounder in the present study, which was not accounted for. Second, there is the potential for coding errors, which would undermine the accuracy of the data collected. Next, the NSQIP database only captures 30-day postoperative outcomes, and hence the presented trends cannot be extrapolated to long-term follow-up. Variables captured by NSQIP uses highly standardized definitions that are applicable to various surgical disciplines. Therefore, clinical variables that are specific to spinal surgery and ASDS are not available for analysis, including open versus minimally invasive approaches, anterior versus lateral versus posterior approaches, technical and/or implant-related complications, as well as radiological or clinical functional scores. Despite these shortcomings, the present study was able to demonstrate significant associations between prolonged OD for ASDS with a variety of surgically and medically related postoperative complications.
Despite these limitations, this is the first national study to evaluate the association between operation time and acute outcomes following elective ASDS. ASDS operation time is a risk factor for many postoperative complications, including, but not limited to, wound and pulmonary complications, VTE, postoperative transfusion, LOS, sepsis, reoperation, and unplanned readmission. As such, operative time may be useful as a quality metric in the performance of ASDS. Strategies to reduce OD and the identification of factors associated with longer surgical duration may further assist in optimization of patient outcomes and improve patient risk stratification.
Footnotes
Authors’ Note
This study was qualified as exempt by the Mount Sinai Hospital Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.