
Abstract
Study Design
Retrospective study.
Objective
Quantify the effect of obesity on elective thoracolumbar spine surgery patients.
Methods
Five hundred consecutive adult patients undergoing thoracolumbar spine surgery to treat degenerative pathologies with minimum follow-up of at least 1 year were included. Primary outcome measures included Numerical Rating Scales for back and leg pain, the Short Form 36 Physical Component Summary and Mental Component Summary, the modified Oswestry Disability Index, and patient satisfaction scores collected preoperatively and at 3, 6, 12, and 24 months postoperatively. Secondary outcome measures included perioperative and postoperative adverse events, postoperative emergency department presentation, hospital readmission, and revision surgeries. Patients were grouped according to World Health Organization body mass index (BMI) guidelines to isolate the effect of obesity on primary and secondary outcome measures.
Results
Mean BMI was 30 kg/m2, reflecting a significantly overweight population. Each BMI group reported statistically significant improvement on all self-reported outcome measures. Contrary to our hypothesis, however, there was no association between BMI group and primary outcome measures. Patients with BMI of 35 to 39.99 visited the emergency department with complaints of pain significantly more often than the other groups. Otherwise, we did not detect any differences in the secondary outcome measures between BMI groups.
Conclusions
Patients of all levels of obesity experienced significant improvement following elective thoracolumbar spine surgery. These outcomes were achieved without increased risk of postoperative complications such as infection and reoperation. A risk–benefit algorithm to assist with surgical decision making for obese patients would be valuable to surgeons and patients alike.
Introduction
The obesity epidemic in North America continues to worsen. More than 60% of citizens of the United States and Canada are overweight; 35 and 25% are obese, respectively. 1 , 2 These numbers are rising, and projections suggest they will continue to rise.3,4 Geographical variability means even greater rates of obesity in certain regions, thus challenging the surgical techniques and technologies of surgeons in these areas. 5 Care providers need to understand the influence of body habitus on surgical outcomes to allow for optimal treatment decision making.
Body mass index (BMI) is presently the most widely used measure of body habitus. 6 , 7 It is calculated as weight in kilograms divided by the square of height in meters (kg/m2). 6 Elevated BMI has been identified as an independent risk factor for perioperative complications for a variety of surgeries. 8 , 9 , 10 Specific assessments of the effect of obesity on spine surgery suggest increased rates of perioperative complications and increased rates of reoperation. 11 , 12
The effects of obesity on spine surgery success have been controversial. At best, obesity was not seen to adversely affect outcomes. 13 , 14 Other studies, however, have identified deleterious effects of obesity. 15 For example, obese patients may report improvement, but perhaps not to the same level obtained by patients of normal weight. 16 These complications have been associated with higher costs for obese patients undergoing spine surgery. 17 Furthermore, there is no predictable weight reduction observed following spine surgery in the obese patient. 18 These mixed results highlight the complex relationship between obesity and spine surgery outcomes. It is clear that further investigation is required.
The purpose of this study was to evaluate the relationship between obesity and patient-reported outcomes following elective thoracolumbar spine surgery. We hypothesized that obese patients would demonstrate fewer postoperative benefits than nonobese patients.
Methods
Data was obtained retrospectively from the Canada East Spine Centre's database of consecutive patients who had spine surgery. Patients were treated by one of two fellowship-trained spine surgeons from a single tertiary-level institution. Inclusion criteria were patients 18 years of age or older undergoing elective thoracolumbar spine surgery for degenerative pathologies who completed at least 1 year of postoperative follow-up. Exclusion criteria were involvement in spine-related litigation, nondegenerative indication for surgery (malignancy, infection, trauma), or a previous spinal fusion. Institutional ethical review board approval was received prior to study commencement.
Data collection included the following variables.
Grouping Variable
The World Health Organization (WHO) has categorized BMI as normal (18.5 to 24.99), overweight (25 to 29.99), obese class I (30 to 34.99), obese class II (35 to 39.99), and obese class III (≥40). 6 BMI in our study was calculated according to WHO standards, by dividing patient weight by the square of patient height. 19 The cohort was then divided into four groups: normal weight (BMI ≤25, n = 107), overweight (BMI 25 to 29.99, n = 180), obese (BMI 30 to 34.99, n = 113), and morbidly obese (BMI ≥35, n = 100). Obese classes II and III were amalgamated into the morbidly obese category in this study for statistical reasons, due to the limited number of patients with BMI ≥40.
Demographics
Age, gender, number and type of comorbidities, diagnosis, symptom profile, and BMI were recorded prospectively at the patients’ presurgical evaluation.
Surgical Factors
Surgical details including traditional open versus minimally invasive technique, decompression versus decompression and fusion, primary versus revision surgery, number of levels treated, operative time, and blood loss were recorded immediately postoperatively. Length of hospital stay was recorded upon hospital discharge.
Outcome Measures
Primary study measures were patient-reported outcomes: Numerical Rating Scale for back pain (NRS-B) and leg pain (NRS-L), modified Oswestry Disability Index (mODI), Short Form 36 Physical Component Summary (SF-36 PCS) and Mental Component Summary (SF-36 MCS). These were evaluated preoperatively and at 3, 6, 12, and 24 months postoperatively. Patient satisfaction ratings were collected according to the same follow-up schedule.
Satisfaction scores were calculated using four questions: (1) “I was helped as much as I thought I would be by my spine treatment”; (2) “My pain was reduced as much as I expected it to be after my surgery”; (3) “Overall I am satisfied with the care I am receiving for my neck and/or back”; and (4) “All things considered, I would have my spine treatment again for the same condition.” Patients selected one of five responses: “definitely true,” “mostly true,” “don't know,” “mostly false,” and “definitely false.” Responses were then coded according to their answer to each question from 1 (definitely true) to 5 (definitely false) and assigned a total score. Scores from 4 to 9 represented satisfied patients, 10 to 14 represented neutral patients, and 15 to 20 represented dissatisfied patients.
Perioperative Adverse Events
Secondary outcome measures consisted of any unplanned surgery-related event. Each adverse event (AE) was recorded using the validated Spine Adverse Event Severity (v1.1) collection and scoring instrument. 20 Number, type, and timing of each AE were documented. Perioperative AEs included any event occurring between incision time and closure (e.g., dural tear); postoperative AEs included any surgery-related complication occurring between surgery and most recent follow-up (e.g., urinary retention). Revision surgery (performed or scheduled) reason and date was recorded if applicable.
Unscheduled emergency department presentation and hospital readmission were identified via retrospective review of the provincial electronic health record system. Otherwise, all data points were collected prospectively.
Statistics
An a priori power analysis was conducted using the minimum clinically important difference method described by Samsa et al. 21 , 22 , 23 Baseline standard deviations of the main outcome measures were each multiplied by 0.2 (a small effect size) to determine the minimum clinically relevant effect size for each variable. The smallest of these effect size values was then used, and power was set at 90%, which yielded a minimum group size of 80 patients per arm. Each of the group sizes in the present study significantly exceeded this minimum value.
Data was analyzed utilizing BMI SPSS software (v20; IBM Corp., Armonk, NY, United States). Non-normally distributed variables were log-transformed. Categorical baseline variables were assessed using chi-square analyses. Differences in the pre- versus postoperative SF-36 PCS, SF-36 MCS, mODI, NRS-L, and NRS-B scores were assessed between BMI groups while controlling for age, number of levels, surgery type, open or minimally invasive approach, gender, number of comorbidities, primary symptom, primary diagnosis, and physician using multivariate analysis of covariance analyses. Significant group main effects were followed up with pairwise comparisons and least significant difference post hoc analyses. Multivariate analysis of covariance was also used to investigate pathology (disk pathology, stenosis, and spondylolisthesis) differences in the pre- versus postoperative SF-36 PCS, SF-36 MCS, mODI, NRS-L, and NRS-B scores between BMI groups. Significance was considered as p < 0.05.
Results
Between 2008 and 2013, 500 consecutive patients (50.4% female) met the study inclusion criteria. The mean age was 55.16 years with a mean number of comorbidities of 0.44 per patient (range: 0 to 5). The mean BMI measured 30 kg/m2, reflecting a significantly overweight population. The average postoperative follow-up was 21 months, with a 1-year follow-up rate of 95%. The surgeon-reported primary indication for surgery included leg pain (40.4%), claudication (30.3%), equal back and leg pain (23.2%), or other symptoms (6.1%; back pain, deformity, neurologic deficit). The primary pathologies included stenosis (43.3%), disk pathology (39.5%), spondylolisthesis (11.7%), and other (5.5%; deformity, instability other than spondylolisthesis, failed fusion). Aside from BMI, there were some other statistically significant differences in demographic variables (Table 1), thereby justifying our controlled model.
Baseline patient demographics
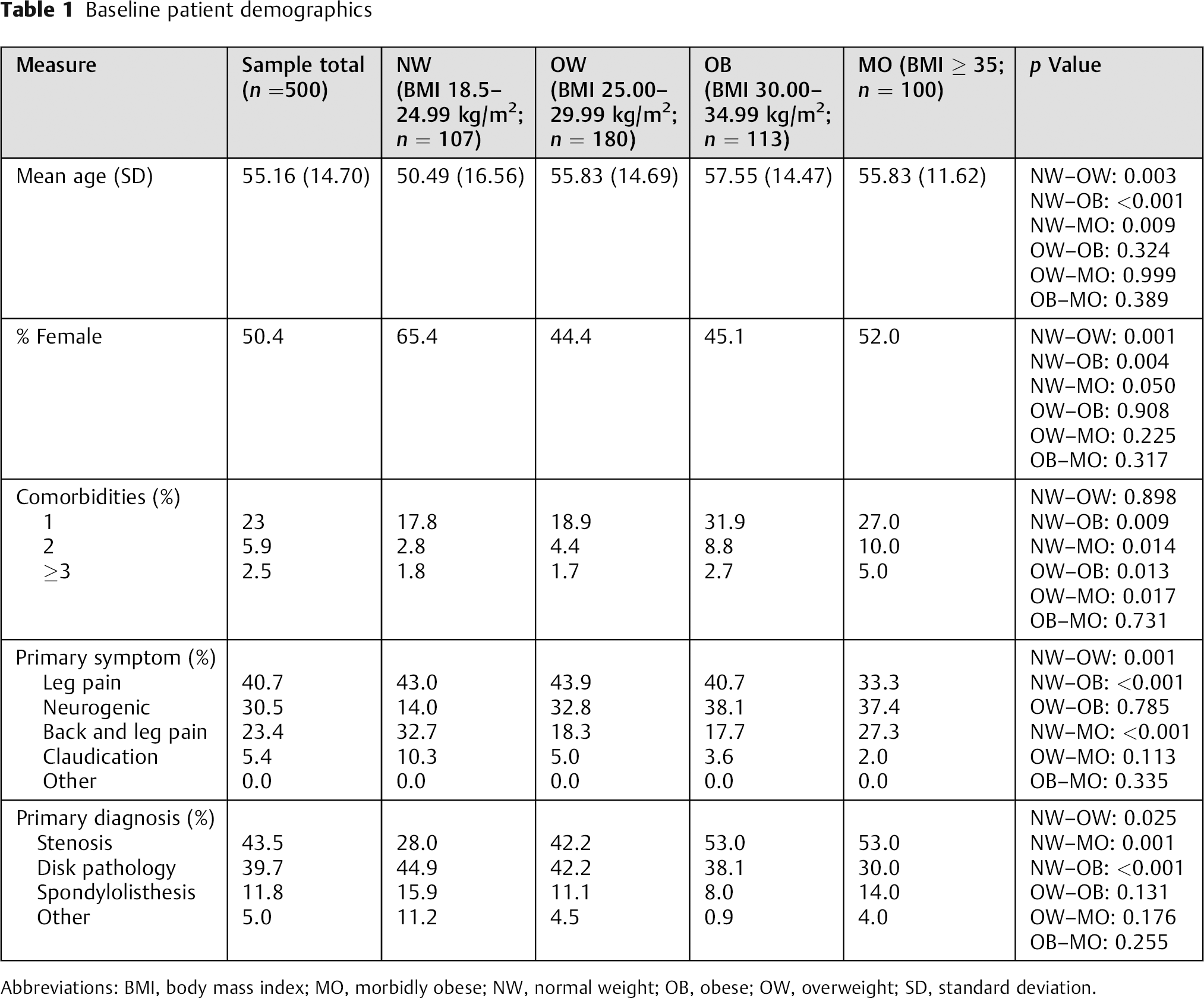
Abbreviations: BMI, body mass index; MO, morbidly obese; NW, normal weight; OB, obese; OW, overweight; SD, standard deviation.
There were also some statistically significant differences in the surgical factors between groups, including primary surgeon (chi-square [3, n = 500] = 10.681, p = 0.014) and number of levels of intervention (F[3,452] = 3.972, p = 0.008), which were accounted for in our model. There were no significant differences in the frequency of minimally invasive surgery versus open approach, percent of patients who had previous lumbar surgery, type of surgery (fusion versus nonfusion), surgical time, estimated blood loss, or length of stay between groups (Table 2).
Surgical factors
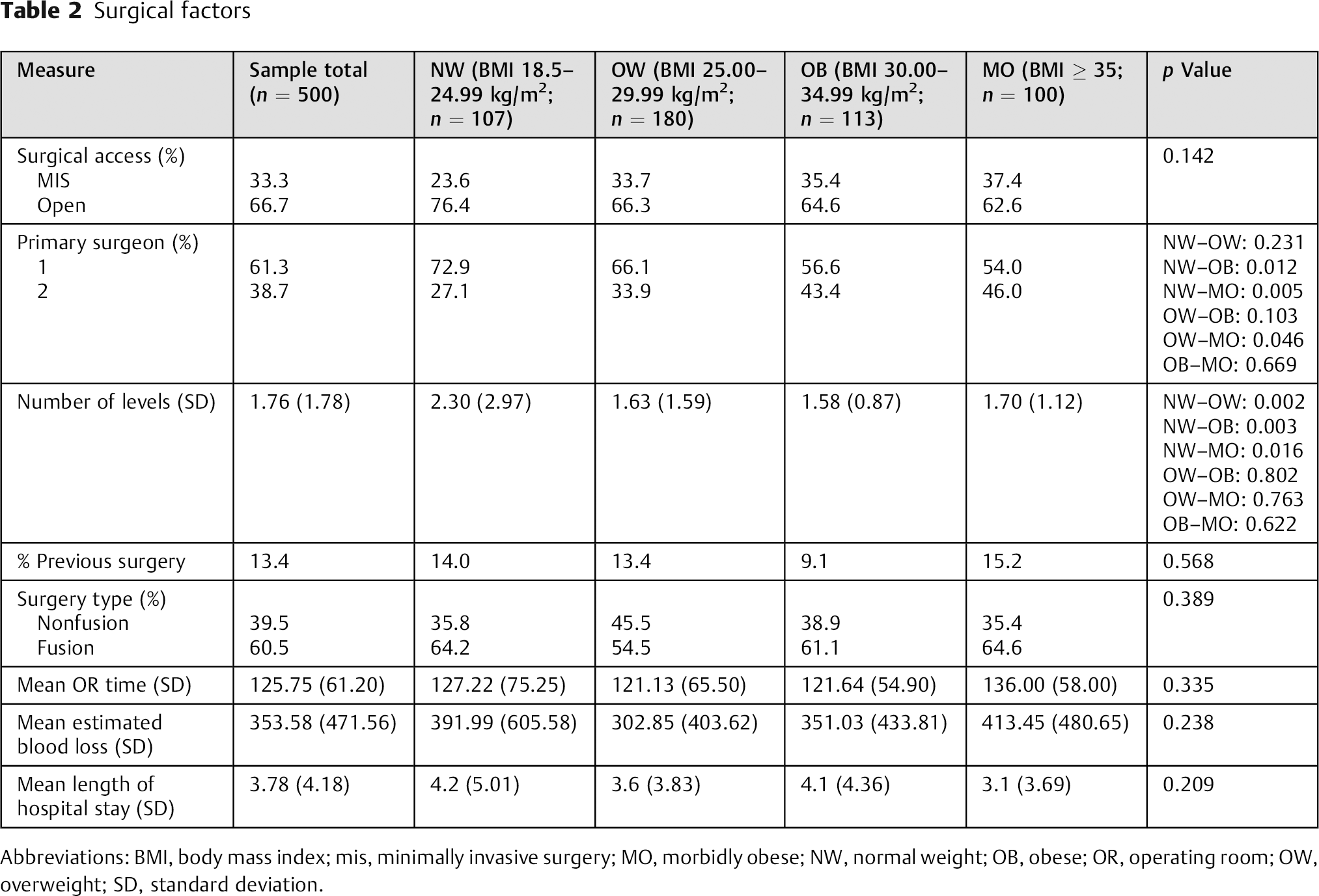
Abbreviations: BMI, body mass index; mis, minimally invasive surgery; MO, morbidly obese; NW, normal weight; OB, obese; OR, operating room; OW, overweight; SD, standard deviation.
The primary end points were patient satisfaction and change in SF-36 PCS, SF-36 MCS, mODI, NRS-B, and NRS-L scores. All the groups demonstrated statistically significant improvement for all primary outcome measures (mean Δ [standard deviation]: SF-36 PCS: 10.48 [10.37]; SF-36 MCS: 6.47 [12.86]; mODI: −22.35 [20.28]; NRS-B: −3.68 [2.88]; NRS-L: −4.15 [3.27]; satisfaction: 74.9% satisfied, 16.5% neutral, 8.6% dissatisfied). Contrary to our hypothesis, BMI was not associated with the degree of change for any primary outcome measures (Table 3 and Figs. 1A to E).
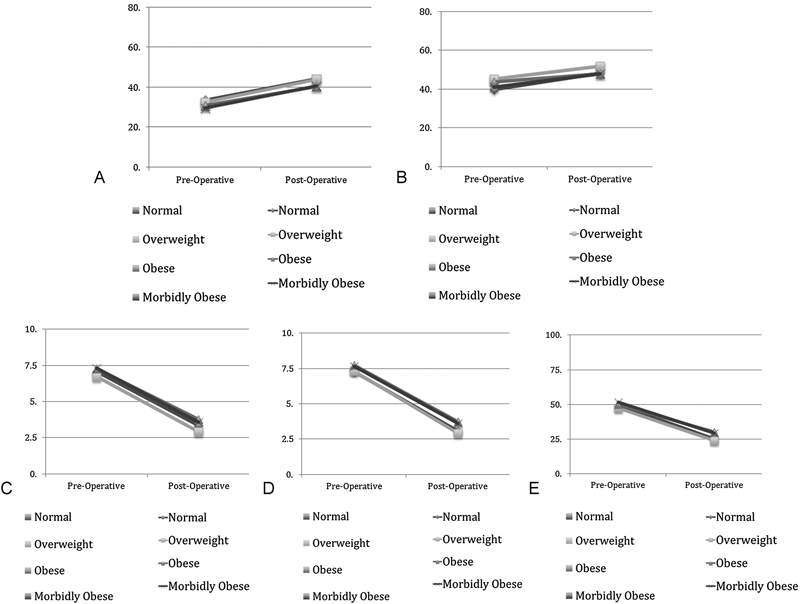
(A) Short Form 36 Physical Component Summary scores. (B) Short Form 36 Mental Component Summary scores. (C) Numerical Rating Scale back pain scores. (D) Numerical Rating Scale leg pain scores. (E) Modified Oswestry Disability Index scores.
Primary outcome measure results
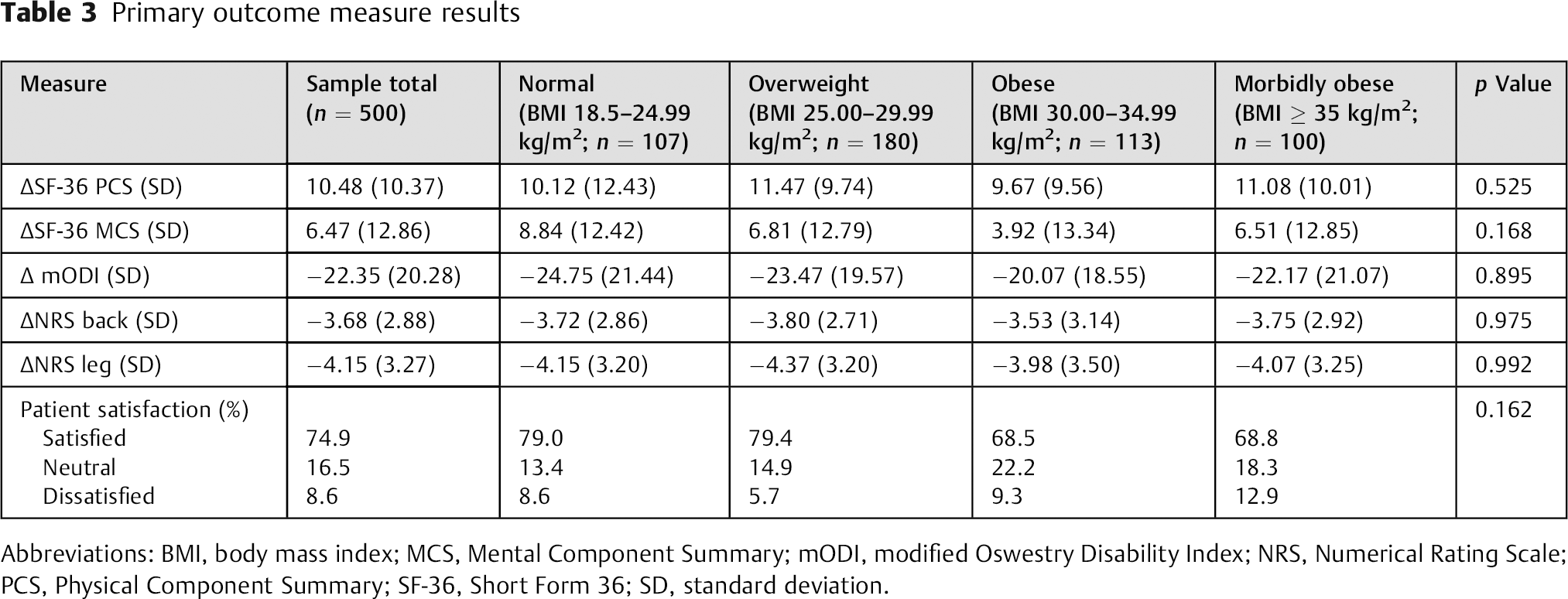
Abbreviations: BMI, body mass index; MCS, Mental Component Summary; mODI, modified Oswestry Disability Index; NRS, Numerical Rating Scale; PCS, Physical Component Summary; SF-36, Short Form 36; SD, standard deviation.
The secondary end points included any unplanned surgery-related events. For the entire study population, the average number of events per 100 patients was observed as follows: perioperative AE: 4 events/100 patients; postoperative AE: 19 events/100 patients; postoperative emergency department assessment: 35 visits/100 patients; reoperation: 13 revisions/100 patients; and readmission: 79 readmission days/100 patients. None of these were significantly different between groups. However, when we broke emergency department visits down by primary complaint (pain-related, physiology-related, psychology-related, and other), we observed that morbidly obese patients presented to the ER for pain-related complaints significantly more frequently than normal-weight patients (p = 0.043) and overweight patients (p = 0.005; Table 4 and Figs. 2A to E). To explore this aspect further, we conducted a regression analysis between preoperative MCS values and postoperative emergency department utilization. The results suggest that preoperative MCS values may be a risk factor for postoperative emergency department utilization, even though there were no differences in baseline MCS values between groups (R2 = 0.013, F[1,500] = 6.80, p = 0.009).
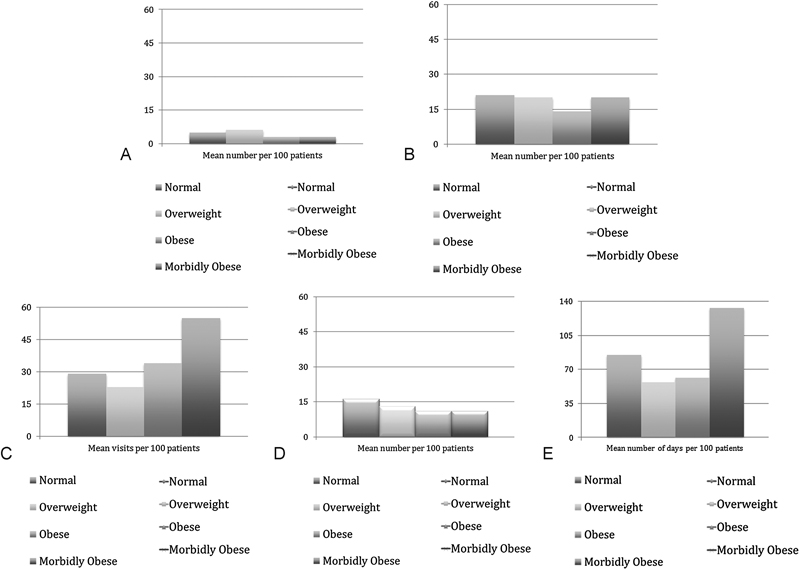
(A) Perioperative adverse events. (B) Postdischarge emergency department utilization. (C) In-hospital adverse events. (D) Reoperation rate. (E) Hospital readmissions.
Surgical complications
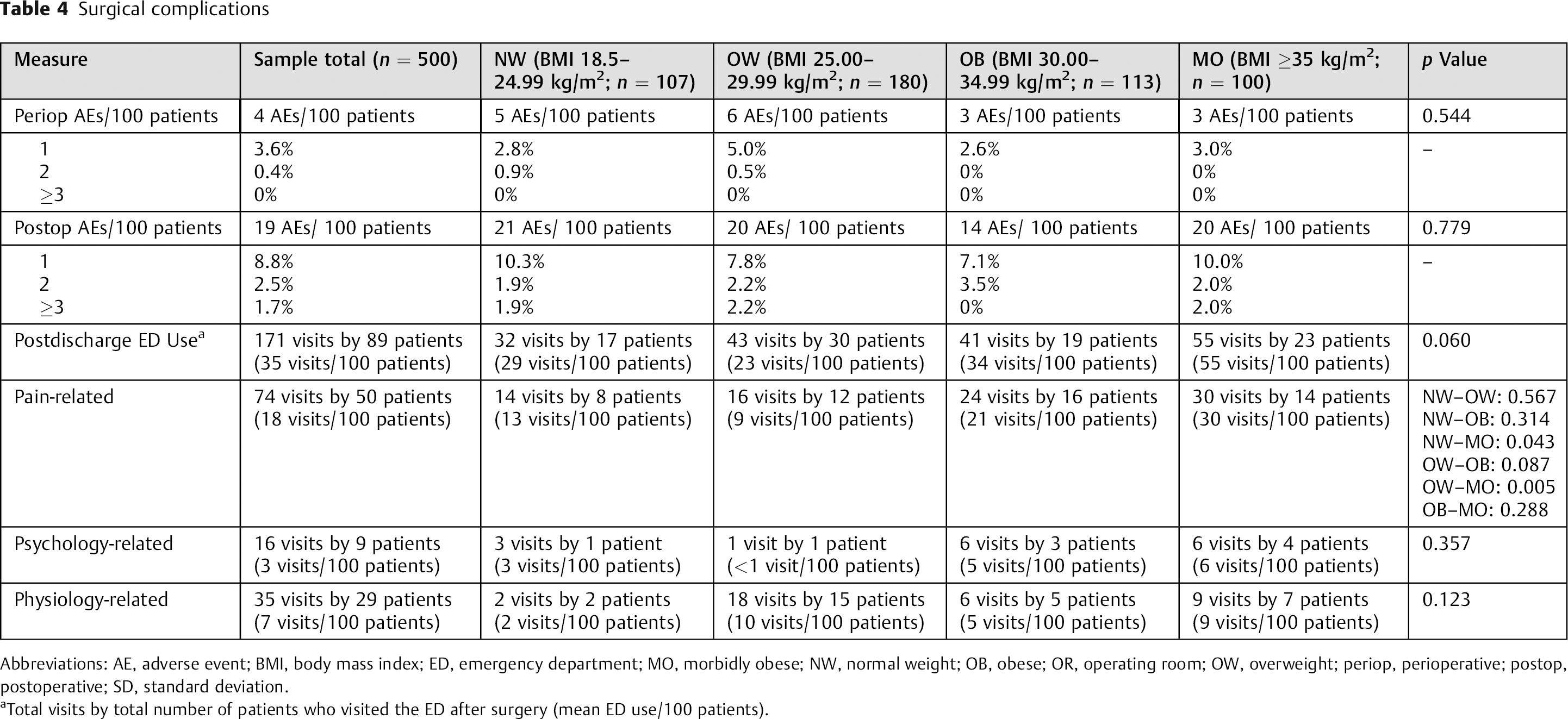
Abbreviations: AE, adverse event; BMI, body mass index; ED, emergency department; MO, morbidly obese; NW, normal weight; OB, obese; OR, operating room; OW, overweight; periop, perioperative; postop, postoperative; SD, standard deviation.
Total visits by total number of patients who visited the ED after surgery (mean ED use/100 patients).
Results by primary pathology showed no statistically significant differences within disk pathology (p = 0.204), stenosis (p = 0.088), or spondylolisthesis (p = 0.642).
Discussion
The Center for Disease Control reported the U.S. national obesity rate as 35%. 24 Similarly, the Canadian Institute for Health Information reported their national obesity rate as 25%.25 The United States ranked first and Canada fourth in obesity prevalence of the Organization for Economic Co-operation and Development countries. As there is no projected improvement in population health regarding BMI, understanding its effect on surgery is essential.
There are two main patterns in the body of research assessing BMI and spine surgery outcomes: studies assessing complications and those assessing subjective patient outcomes. This study enhances our understanding of patient-reported outcomes while also allowing us to observe postoperative complications.
Three systematic reviews and one large population-based study have identified obesity as a strong risk factor for the occurrence of postoperative spine surgical site infection. 8 , 10 , 26 Two additional large population-based studies identified obesity as a strong risk factor for the occurrence of any perioperative complication for spine surgery. 17 , 27 , 28 , 29 A third such study by Gaudelli and Thomas reported greater reoperation rates in obese patients. 12
A meta-analysis by Abdallah et al evaluated 10 studies and demonstrated a log-linear relationship between obesity and surgical site infection; for each 5-point increase in BMI, there was a 21% increase in risk for surgical site infection. 11 However, some authors reported no difference in complications between obese and nonobese patients, attributing this discrepancy to the use of minimally invasive techniques. 30 , 31 , 32
Although the correlation of elevated BMI and surgical complications appears strong, the effect of obesity on postoperative outcomes remains controversial. Swedish Spine Registry stenosis data and Spine Patient Outcomes Research Trial (SPORT) disk herniation data both demonstrated greater improvement in the nonobese patients undergoing surgery for lumbar disk herniation. 15
Conversely, the SPORT spondylolisthesis data demonstrated no difference in outcomes based on obesity. Several other authors have identified no deleterious effect of elevated BMI on patient-reported outcomes following spine surgery, suggesting the success may be related to the use of minimally invasive techniques. 13 , 33 , 34
The present study assessed a real-world sample of patients having spine surgery for a variety of pathologies, which is valuable for the generalizability of the results. However, if the relationship between BMI and outcomes is mediated by pathology, that might explain why we did not detect significant differences in the present study. The current study found that BMI did not have a statistically significant effect on surgical outcomes within specific pathologies. The current study was powered with pathologies collapsed; further investigation where analysis by pathology is the primary goal of the study is warranted.
It is also important to note that we did detect significant differences in the number of levels of surgical intervention between groups, which was controlled for in our statistical model but may indicate a surgical selection bias. The study is unable to quantify the conscious and unconscious decision making involved in selecting an obese patient for surgery. Surgeon perceptions are prone to change based on the physical appearance and fitness of the patient being considered for surgery. 35 , 36 ,37,38 Surgeon-perceived risk versus benefit may bias surgeons toward nonoperative care in obese patients. Thus, this study may simply include a subset of obese patients who present the lowest risk for surgical complications. Future research should aim to compare patients with elevated BMI who are managed both operatively and nonoperatively.
Surgical complications have been linked to increased care costs. 39 It is reasonable to conclude that there may be a link between elevated BMI and elevated cost of care in light of the findings reviewed here. Kalanithi et al identified a 28% increase in perioperative costs for the morbidly obese patient. 17 These costs were attributable to greater resource utilization for care of complications and length of hospital stay.
Our findings suggest that all other factors being equal (age, gender, number of levels, comorbidities, etc.), obese patients may obtain spine surgery outcomes that are as good as those reported by normal-weight patients. In light of this observation, BMI alone may not be an appropriate discriminator in surgical decision making. Although the magnification of risk and readmission and reoperation rates found in previous research need to be disclosed during the consent process, the potential for equivalent improvement is supported by this study. Surgeons prove sound decision makers in selecting those patients who will benefit from surgery, despite their body habitus.
There are several possible reasons for the discrepancy between our results and previous research. 15 , 16 Patients of normal weight comprised only 21.4% of our total study population. It is possible this high volume of obesity makes the team more proficient at mitigating problems and maximizing surgical success in these patients. Case volume has been reported as an advantage in improved outcomes and decreased complications in several clinical scenarios. 40 , 41
Similar findings have been reported previously in the orthopedic joint arthroplasty literature. Multiple authors have confirmed equal or greater success in the obese patient following total knee or total hip arthroplasty despite a less favorable complication profile. 42 So far, no one has defined a BMI above which surgical risk is too great or surgery is precluded.
The progression toward greater body habitus requires medical providers to reevaluate the provision of care in all areas of medicine and in spine care specifically. Clinical symptoms may present earlier, physical examination will be more challenging, diagnostic accuracy may be altered, and treatment efficacy may change. Surgical success will need reevaluation to understand the outcomes and complications specific to this new physiology. Technique modification may improve success—for example, the use of minimally invasive techniques. Payers should expect the evaluation and treatment of these patients to cost more. Ultimately, the care landscape must change to accommodate this new medical environment.
Advantages
The study outline follows the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting observational studies. 43 The sample size is large and well beyond the participant and group numbers needed to prevent type II error for primary outcomes. Perioperative measures, complications, revision surgery rates, and patient-reported outcomes are provided at minimum 1-year follow-up. The literature to date is limited on this outcome data and on medium-term follow-up. Finally, all surgical types were included, improving the generalizability of the data for surgical decision making.
Limitations
The study was designed to evaluate outcomes. It was not powered specifically to address the secondary measures of unplanned surgery-related events, and thus a type II error may be possible for detecting differences in variables such as readmission rates and revision surgery. The current study was also not powered by pathology; the ability to make conclusions by pathology could lead to enhanced understanding of the role of BMI in the surgical outcomes.
This study is also limited by the length of follow-up. Obese patients could be at greater risk of declined function, adjacent segment breakdown, and instrumentation/implant failure occurring beyond the period measured. Future research following patients for longer would be valuable.
At present, BMI represents the most widely used and easily obtained measure of obesity. However, measures such as subcutaneous fat thickness over the lumbar spine or percent body fat may be more accurate in correlating obesity and surgical complications. 44 , 45 No correlation has been found between these measures and BMI in the literature.
The study was unable to quantify the surgical challenges associated with treating obese patients. Obesity may increase the difficulty of certain technical aspects of the surgery. Obesity also often increases the nursing care burden postoperatively. Increased efforts required to achieve success are often absorbed by the individual providers and the system in general and thus are more difficult to identify.
Conclusions
Patients of all levels of obesity experienced significant improvement following elective thoracolumbar spine surgery. These outcomes were achieved without increased risk of postoperative complications such as infection and reoperation. Therefore, obesity alone may not be enough to preclude patients from elective thoracolumbar spine surgery.
Future research should address (1) the effect of BMI on surgical decision making, (2) surgical team volumes/surgical techniques best suited to patients with elevated BMI, and (3) the relationship between elevated BMI and postoperative emergency department presentation.
Multicenter studies with longer follow-up would help elucidate long-term outcomes. A risk–benefit algorithm based on large population-based data sets to assist with surgical decision making would be valuable.
Disclosures
Neil A. Manson, Research grant: Medtronic Canada
Alana J. Green, Personal fees: Canada East Spine Centre
Edward P. Abraham, Research grant: Medtronic Canada; Personal fees: Medtronic Canada
Footnotes
Acknowledgments
Research administration and personnel were supported via an unconditional research grant provided by Medtronic Canada. The database and database administration were supported via an unconditional research grant provided by Nuvasive.