
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Therapeutic strategies for Aneurysmal Bone Cysts (ABCs) of the spine remain controversial and encompass several modalities, including open surgery (ie, intralesional curettage and/or en bloc resection), localized injections, and pharmacotherapy. This study was designed to retrospectively analyze the clinical data from patients treated at our institution, with the objective of evaluating the clinical outcomes, safety profile, and efficacy of different treatments including open surgery, percutaneous injections of a doxycycline-albumin suspension, and Denosumab therapy in the management of these lesions, thereby establishing a basis for a comprehensive treatment algorithm.
Methods
From January 2010 to December 2024, 27 patients who had no/minor neurological deficits (modified Frankel scale D or E) were included in the study, of whom 6 were treated with open surgery (surgery group), 14 were treated with percutaneous doxycycline/albumin injection (injection group) and 7 were treated with Denosumab (Denosumab group). The demographic and clinical information of these groups were recorded and compared.
Results
In the surgery cohort (n = 6), complete neurological recovery was achieved in 5 patients (83.3%), while 1 patient experienced residual minor paresthesia; their mean Visual Analogue Scale (VAS) score decreased from 4.9 to 0.8. Two patients developed local recurrence over a mean follow-up period of 46.6 months (range, 15-113 months). In the injection cohort (n = 14), all patients demonstrated a significant reduction in lesion size and resumed normal daily activities. Complete symptomatic resolution was reported in 10 patients; 4 achieved partial resolution, with only mild, exertion-related local pain. Their mean VAS score decreased from 4.9 to 0.7. During a mean follow-up of 68.1 months (range, 7-117 months), no complications or recurrences were observed. In the Denosumab cohort (n = 7), all patients exhibited a significant reduction in lesion size and resumed normal activities. Complete symptomatic resolution was achieved in 6 patients, while 1 experienced partial resolution, characterized by intermittent, mild upper extremity weakness. Their mean VAS score decreased from 4.8 to 0.24. No complications or recurrences were documented over a median follow-up of 9.5 months (range, 1-88 months). No significant differences were observed among the cohorts regarding the rates of recurrence (P = 0.227) or complications (P = 0.304).
Conclusions
For patients presenting with spinal ABCs characterized by an absence of severe neurological deficits, both intralesional injection and systemic drug therapy are effective minimally invasive treatment options and can be considered as first-line choices. However, while both approaches demonstrate favorable short-term efficacy, their long-term outcomes require further investigation. Although not the preferred initial treatment, open surgery remains a crucial option for rapidly correcting spinal instability and reversing neurological deficits.
Keywords
Introduction
An Aneurysmal Bone Cyst (ABC) is a benign, expansile, osteolytic bone lesion composed of multiple blood-filled cystic chambers. Histologically, it is characterized by a proliferation of fibroblasts, osteoclast-like giant cells, and reactive woven bone, resulting in the destruction of the host bone.1,2 While rare, ABCs constitute approximately 1% of all primary bone tumors. The spine is affected in 10%-30% of cases, where these lesions account for roughly 15% of all primary spinal neoplasms.3,4 The clinical presentation typically includes symptoms of local mass effect, such as pain, as well as neurological deficits and pathological fractures.3,4
Due to the rarity of spinal ABCs, a standardized treatment protocol remains controversial. Although various therapeutic strategies have been reported in the literature, these studies are predominantly small-sample, single-center experiences, thus lacking high-level evidence to establish a definitive consensus on the optimal management approach. Treatment modalities for spinal ABCs encompass a range of interventions, including open surgery (ie, intralesional curettage and/or en bloc resection), intralesional injections, pharmacotherapy, selective arterial embolization (SAE), and radiotherapy.5-8 Open surgery has traditionally been the mainstay of treatment for spinal ABCs; however, resection of these spinal tumors is associated with significant surgical morbidity and a risk of iatrogenic neurological injury. In addition to open surgery, our institution has explored minimally invasive therapeutic strategies, establishing percutaneous injection of a doxycycline-albumin suspension as a viable alternative therapy. 9 This approach is particularly suitable for patients presenting with adequate spinal stability and an absence of severe neurological deficits. Furthermore, published reports have documented the successful use of Denosumab for managing recurrent, postoperative ABCs, 10 prompting our own investigation and effective clinical application of this pharmacotherapeutic agent.
Given the rarity of spinal ABCs, the literature pertaining to their management is limited. As one of the largest spinal tumor centers in China, our institution has managed a substantial cohort of patients with primary spinal ABCs. This experience provides a unique opportunity to analyze treatment outcomes from a large, single-center series. Therefore, the present study was undertaken to retrospectively analyze our clinical data, evaluating the outcomes associated with various therapeutic strategies with the goal of refining the treatment algorithm for these challenging lesions.
Materials and Methods
Clinical Data
This study was approved by the Ethics Committee of the University’s hospital (IRB00006761-M2023022) and its implementation adhered to the Declaration of Helsinki. We conducted a retrospective review of patients who were treated for primary spinal ABCs at our institution between January 2010 and December 2024. A key inclusion criterion was a definitive diagnosis confirmed by histopathological examination. Patients with extra-spinal or secondary ABCs were excluded from the study. A search of the institutional database identified a total of 27 patients who met the eligibility criteria and were subsequently included for analysis. This study was limited to a retrospective review of patients who underwent inpatient treatment. Outpatient cases were excluded from the analysis due to the potential for incomplete or inconsistent medical records, which could have compromised the integrity of the data.
Treatment Protocol
Prior to 2014, open surgery represented the standard of care for all patients with spinal ABCs at our institution. 9 Subsequently, beginning in 2014, percutaneous injection of a doxycycline-albumin suspension was introduced as a therapeutic option. This modality was reserved for select patients presenting with an absence of severe neurological deficits (muscle strength grade >3/5), and lesions exhibiting a distinct cystic architecture. 9 More recently, in 2018, pharmacotherapy was incorporated into our treatment paradigm.
Our current treatment algorithm stratifies patients based on clinical and radiological findings. Open surgery is the indicated treatment for individuals presenting with spinal instability or significant neurological compromise. The surgical strategy was determined based on the anatomical location of the lesion and the anticipated surgical difficulty. Operative procedures included en bloc resection (either via an intralesional or extralesional approach) or intralesional curettage with spinal reconstruction and decompression using pedicle screw fixation. For patients with stable spines and an absence of neural compression, the therapeutic pathway is further determined by the lesion’s architecture. Those with lesions exhibiting a prominent cystic component are considered candidates for either CT-guided percutaneous injection or Denosumab therapy. Conversely, if a stable lesion is predominantly solid, pharmacotherapy with Denosumab is the preferred non-operative approach. Surgical intervention is recommended for any patient undergoing non-operative management who demonstrates treatment failure or disease progression. Finally, for all patients, written informed consent was obtained after a comprehensive discussion of the risks and benefits of the proposed treatment plan.
Injectable therapies utilized in this study included a doxycycline-albumin suspension and a combination of calcitonin and corticosteroids. The doxycycline-albumin suspension was prepared according to our institutional protocol 9 : a homogenous mixture was created by repeatedly passing 5.0 mL of human serum albumin (20%) and 5.0 mL of doxycycline solution (200 mg total; 40 mg/mL) between two interconnected 10-mL syringes for approximately 30 cycles. This mixture was then emulsified with 5.0 mL of air through an additional 30 mixing cycles, yielding a stable, viscous foam resistant to dilution by blood. Subsequent injections were administered at 3-month intervals, unless significant new bone formation was confirmed on follow-up CT imaging. The treatment endpoint was defined as either the complete ossification of the lytic defect or the presence of a small, stable residual lesion after a 6-month observation period.9,11
In the absence of established clinical guidelines for Denosumab therapy in ABCs, our treatment protocol was adapted from a multicenter case series published by the French Society of Pediatric Cancers (SFCE) and the French Sarcoma Group (GSF). 12 The regimen consisted of a loading phase with Denosumab administered at 70 mg/m2, once weekly for 4 weeks, followed by a maintenance phase of monthly injections at the same dosage. All patients received concurrent supplementation with calcium acetate and calcitriol (an active vitamin D analog). The total duration of therapy was individualized, guided by a composite assessment of clinical response and radiological findings at follow-up evaluations. In most cases, treatment was discontinued after approximately two years.
Imaging and Biopsy
The standard diagnostic workup for all patients included anteroposterior and lateral spinal radiography, computed tomography (CT), and magnetic resonance imaging (MRI). Lesion volume was calculated using the ellipsoid volume formula. 13 For patients in whom a diagnosis was not established via an open surgical biopsy, a CT-guided core needle biopsy was performed by an interventional radiologist to obtain tissue for histopathological confirmation. Following histopathological confirmation, patients were allocated to a treatment arm: open surgery, percutaneous doxycycline-albumin injection, or Denosumab pharmacotherapy.
Follow-up
Post-discharge, follow-up examinations were scheduled at 3 and 6 months, and semiannually thereafter. These assessments included documentation of current symptoms, evaluation of neurological status using the Frankel grading system, VAS pain scores, and the occurrence of any treatment-related complications. Annual radiological surveillance with CT and MRI was performed to monitor for changes in lesion volume, evidence of lesion expansion, or local recurrence. Immediate CT and MRI examinations were indicated in the event of symptom recurrence. Recurrence was defined as the radiological identification on CT of new osteolytic areas or the expansion of a pre-existing lytic component that warranted further intervention.
Statistical Analysis
All statistical analyses were performed using SPSS Statistics, version 27.0 (IBM Corp., Armonk, NY). The normality of distribution for continuous variables was assessed using the Shapiro-Wilk test. Normally distributed data are presented as mean ± standard deviation (SD), while non-normally distributed (skewed) data are expressed as median and range. Intergroup comparisons of continuous variables—including age, disease duration, pre- and post-operative VAS scores (at 12 months) were conducted as follows: for normally distributed data, Student's t-test (for two groups) or Analysis of Variance (ANOVA) (for ≥3 groups) was used. For non-normally distributed data, the Mann-Whitney U test (for two groups) or the Kruskal-Wallis test (for ≥3 groups) was employed. Differences in categorical variables, including sex, recurrence rates, and complication rates, were analyzed using the chi-square (χ2) test. Lesion location was categorized as cervical, thoracic, or lumbar, and the distribution of these locations among the different treatment groups was also compared using the χ2 test. A P-value of less than 0.05 was considered to indicate statistical significance.
Results
Comparison of Clinical Data Among Surgery, Injection and Denosumab Group
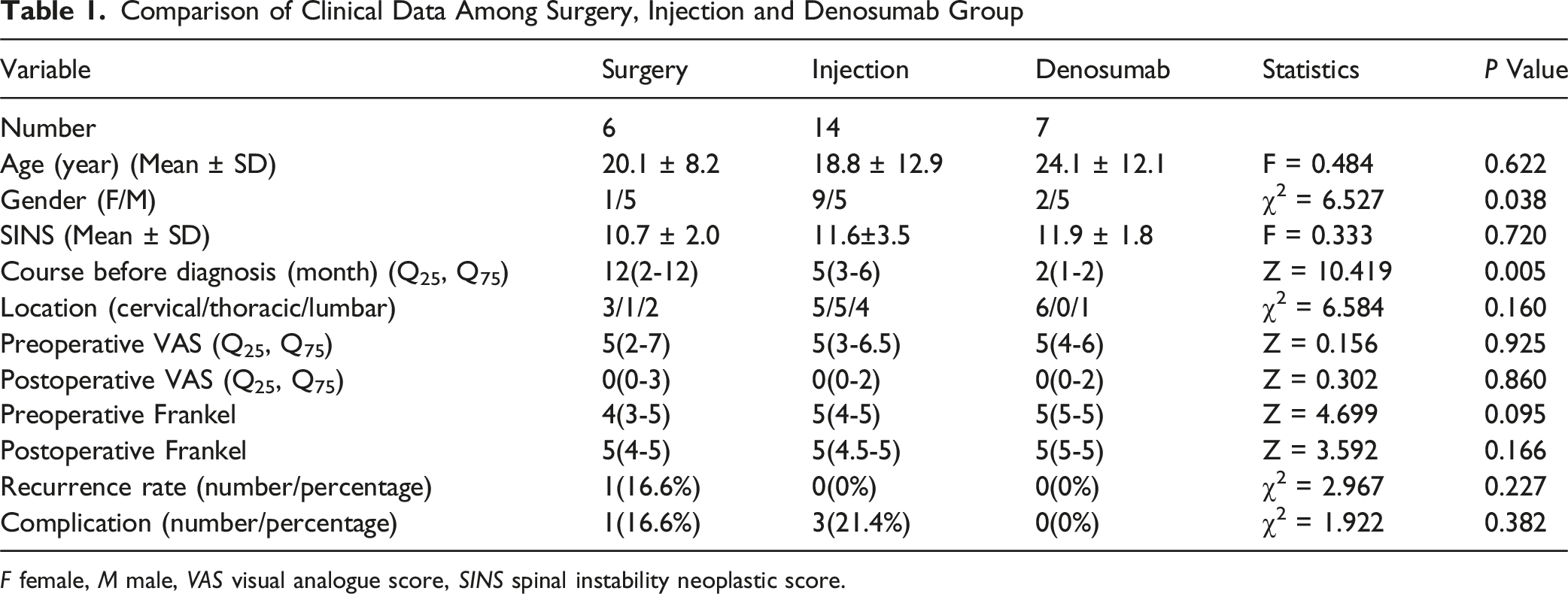
F female, M male, VAS visual analogue score, SINS spinal instability neoplastic score.
Baseline comparisons among the three treatment cohorts revealed no statistically significant differences in age (P = 0.622), Spinal Instability Neoplastic Score (SINS) (P = 0.720), lesion location (P = 0.160), or pre-treatment Visual Analogue Scale (VAS) scores (P = 0.925). However, a statistically significant difference was observed among the groups regarding sex distribution (P = 0.077) and the duration of symptoms prior to treatment (P = 0.005). Post-hoc analysis indicated that the Denosumab cohort had a significantly shorter pre-treatment symptom duration compared to both the open surgery cohort (P = 0.010) and the percutaneous injection cohort (P = 0.003).
In the open surgery cohort (n = 6), lesions were located in the cervical (n = 3), thoracic (n = 1), and lumbar spine (n = 2). The mean preoperative Spinal Instability Neoplastic Score (SINS) was 10.7 (range, 8-13). Of the 5 patients presenting with neurological compromise, 2 had bilateral lower extremity paresthesia, weakness, and gait instability, with one of these patients also reporting severe thoracolumbar pain and another experiencing bowel and bladder incontinence. The remaining 1 patients presented with quadriparesis and quadri-paresthesia, predominantly affecting the lower extremities. All patients were managed via a posterior surgical approach; 2 underwent en bloc resection (Figure 1), while 4 underwent intralesional curettage. The mean operative time was 221 minutes (range, 70-372 min), and the mean estimated blood loss (EBL) was 929 mL (range, 200-2200 mL). Case Illustration of a 15-Year-old Male Who Presented With Progressive Paraplegia (Frankel Grade C) and Bowel and Bladder Incontinence, Diagnosed With a Primary Aneurysmal Bone Cyst (ABC) Involving the T11-L1 Vertebrae. The Patient was Treated With en Bloc Resection and Showed no Evidence of Recurrence at 4-Year Follow-up. (A) Preoperative CT Scan Demonstrates an Extensive Osteolytic Lesion Destroying the T12 Vertebral Body and its Posterior Elements. (B) Preoperative MRI Reveals the Multi-Level Involvement From T11 to L1, With the Bulk of the Lesion Centered at T12. (C) Intraoperative Photograph Shows the Posterior en Bloc Resection of the T12 Vertebra and Portions of T11 and L1, and Subsequent Reconstruction Using a 3D-Printed Custom Vertebral Body. (D) Postoperative CT Scan at 4-Year Follow-up Confirms Stable Instrumentation and no Signs of Local Recurrence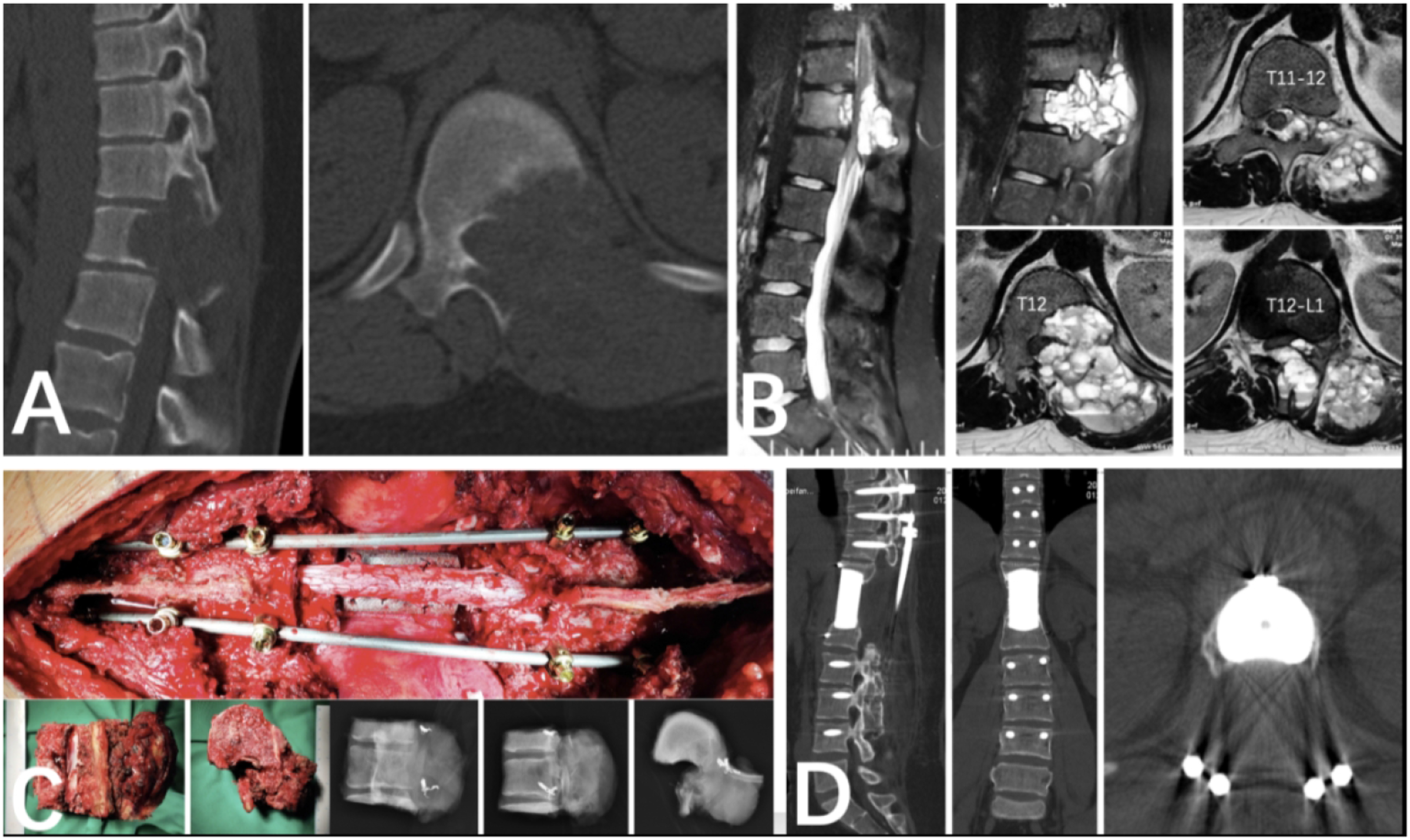
At a mean follow-up of 46.6 months (range, 15-113 months), significant clinical improvement was observed. The mean VAS score decreased from 4.9 to 0.9, and the median VAS score decreased from 5 (range, 2-9) to 0 (range, 0-3). Complete neurological recovery was achieved in 5 patients (83.3%), while 1 patient had residual minor paresthesia. Two patients (33.3%) experienced local recurrence. The first case, diagnosed 24 months postoperatively after follow-up imaging revealed an enlarging lytic lesion in L4, was confirmed by biopsy and subsequently managed conservatively with Denosumab, with no further recurrence. The second patient with recurrence underwent a repeat surgical procedure involving resection, fusion, and internal fixation. One major complication was recorded (16.6%): a fracture of an internal fixation rod occurred 36 months postoperatively, which was successfully treated with revision surgery.
In the percutaneous injection cohort (n = 14), lesions were located in the cervical (n = 5), thoracic (n = 5), and lumbar spine (n = 4). Patients presented with local pain for a mean duration of 4.8 months (range, 1-12 months), and the mean presenting Visual Analogue Scale (VAS) score was 4.9 (range, 2-8). Six patients reported functional impairment: 1 patient presented with L5 radiculopathy and 3 with myelopathy (1 with paraparesis/paresthesia and 2 with quadriparesis/paresthesia). Pre-treatment Frankel grades were E (n = 9), D (n = 3), and C (n = 2). The median pre-treatment lesion volume was 25.0 mL (range, 1-209 mL), and the mean preoperative Spinal Instability Neoplastic Score (SINS) was 11.6 (range, 7-17). Thirteen patients were treated with the doxycycline-albumin suspension, while one received injections of calcitonin and corticosteroids. Of these, 8 patients finished a single injection, 3 finished two injections, and 3 finished three.
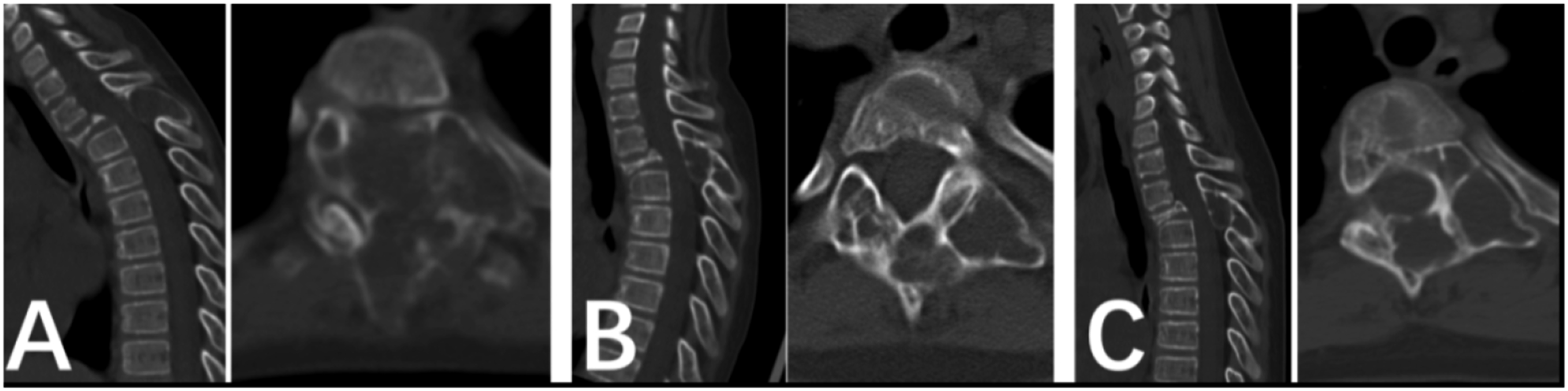
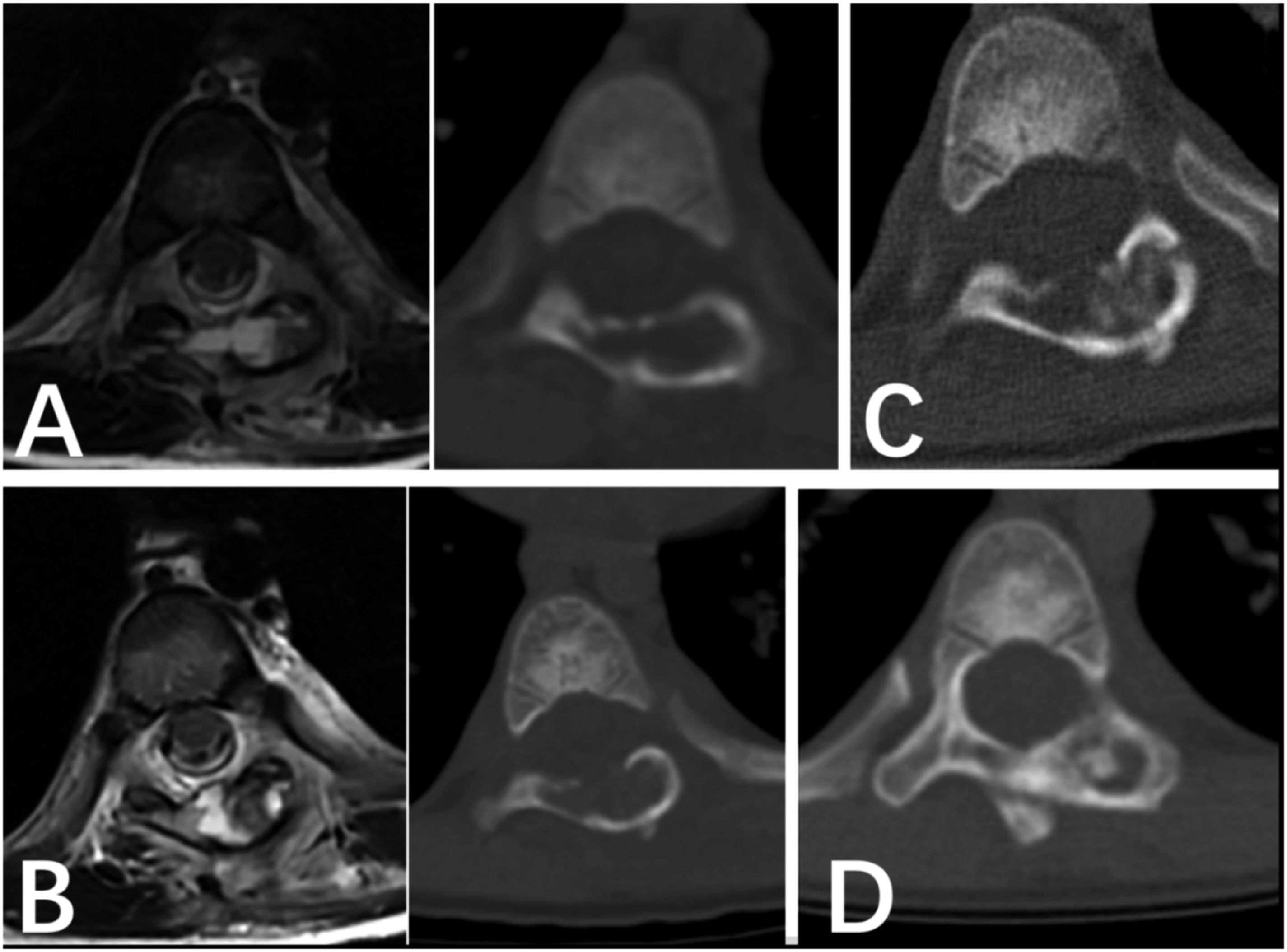
At a final mean follow-up of 68.1 months (range, 7-117 months), no recurrences were observed. Follow-up CT and MRI demonstrated a significant reduction in lesion volume (Figures 2 and 3). Functionally, all patients returned to normal activities. Complete symptomatic resolution was achieved in 10 patients (71.4%), while 4 (28.6%) reported partial resolution with only mild, exertion-related local pain. Notably, all 4 patients presenting with pre-treatment neurological deficits (Frankel grades C and D) achieved neurological recovery. The mean post-treatment VAS score decreased to 0.8, with a median of 0 (range, 0-2). Case Illustration of a 6-Year-old Female Who Presented With Neck Pain Following Minor Trauma and was Diagnosed With a Primary Aneurysmal Bone Cyst (ABC) of the C4 Vertebra. The Patient was Successfully Managed With Two Intralesional Injections of a Doxycycline-Albumin Suspension. (A) A Pre-treatment Imaging Montage (Radiograph, CT, MRI) Demonstrating an Osteolytic Lesion With a Multi-Cystic Architecture and Areas of Calcification Within C4. (B) Follow-up CT Scan Performed after Two Injections Administered One Month Apart, Showing Early Signs of Ossification. (C) A CT Scan at 1-Year Follow-up Reveals Significant Interval Ossification of the Lesion, which Correlated With Complete Pain Resolution and Allowed for Ambulation With a Cervical Brace. (D) At 2-Year Follow-up, the CT Scan Shows Near-Complete Consolidation and Remodeling of the Vertebra, Permitting the Discontinuation of the Brace. (E) An MRI at 8-Year Follow-up Confirms the Stable, Healed Appearance of the Lesion With no Evidence of Recurrence, Corresponding to a Full Return to normal Activities for the Patient Case Illustration of a 6-Year-old Female Diagnosed With a Primary Aneurysmal Bone Cyst (ABC) of the T3 Vertebra Who was Managed With Intralesional Sclerotherapy. (A) Pre-treatment CT Scan Demonstrates Extensive Osteolytic Destruction Involving the T3 Vertebral Body and Posterior Elements. (B) At 1-Year Follow-up, a CT Scan Reveals Partial Ossification, With new Bone Formation Occurring Predominantly Along the Internal Septa of the Lesion. (C) A CT Scan at 2-Year Follow-up Shows Further Consolidation. This Image Also Illustrates a Potential Limitation of Sclerotherapy, as the Ossification Along the Septa can Create Enclosed Compartments, which May Hinder the Efficacy and Distribution of Subsequent Injections Into Any Remaining Cystic Areas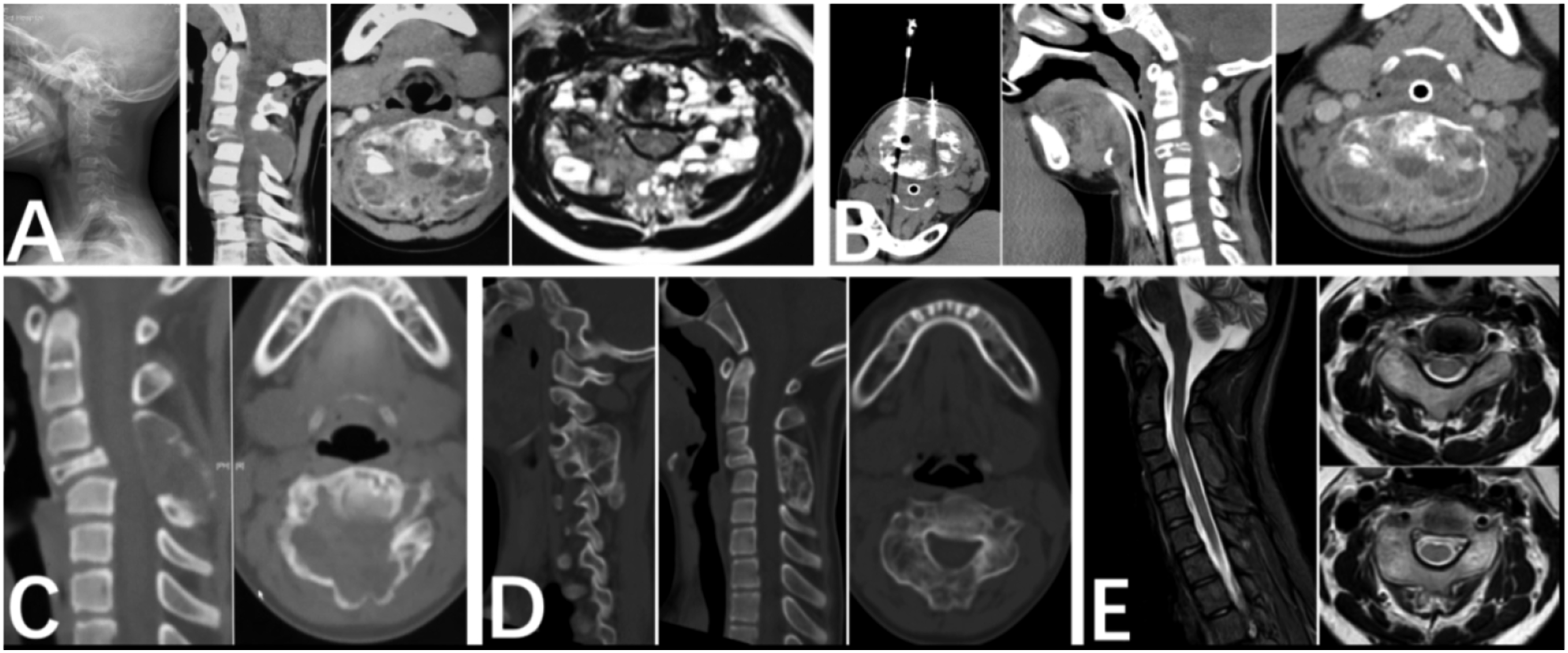
Three complications were recorded. One patient experienced transient dizziness on the day of injection, which resolved spontaneously and was attributed to a reaction to anesthesia. Another patient had a transient syncopal episode the day after injection, which resolved following intravenous fluids and administration of 5 mg of dexamethasone. One patient developed an acute neurological deficit on the day of injection, presenting with left-sided weakness and numbness below the nipple line. On examination, muscle strength was grade 4/5 in the left upper extremity and 3/5 in the left lower extremity, with lower limb hyperreflexia, ankle clonus, and positive pathological reflexes. An immediate presumptive diagnosis of acute epidural hematoma with neural compression was made. Conservative management was initiated with glucocorticoids, mannitol, and tranexamic acid. The patient responded well, and at discharge on day 5, left-sided muscle strength had recovered to grade 5-, and the patient was ambulatory with significantly reduced sensory deficits. No instances of infection, skin necrosis, or vascular embolism were recorded.
In the Denosumab pharmacotherapy cohort (n = 7), lesions were predominantly located in the mobile spine, with 6 in the cervical or cervicothoracic region and 1 in the lumbar spine. Patients presented with a mean symptom duration of 1.5 months (range, 0.5-3 months) and a mean initial Visual Analogue Scale (VAS) score of 4.7 (range, 3-6). Two patients reported functional impairment, and three presented with neurological deficits: one with C4-5 radiculopathy and two with myelopathy (one with quadriparesis and quadri-paresthesia with associated upper extremity pain, and one with isolated upper extremity paresthesia). Pre-treatment Frankel grades were E. The mean pre-treatment lesion volume was 32.7 mL (range, 3-68 mL), and the mean SINS score was 10.9 (range, 8-15). All patients received a standardized regimen of subcutaneous Denosumab injections, with a mean of 8 administrations (range, 2-16).
At a final mean follow-up of 10.6 months (range, 1-25 months), no recurrences were documented. All patients returned to normal activities. Notably, two patients in this cohort, who had previously failed intralesional sclerotherapy, were successfully salvaged with Denosumab therapy (Figures 4 and 5). Complete symptomatic resolution was achieved in 6 patients (85.7%), while 1 (14.3%) experienced partial resolution, with only intermittent, mild upper extremity weakness. The mean post-treatment VAS score decreased significantly to 0.3, with a median of 0 (range, 0-2). No major complications, including neurological injury, infection, skin necrosis, or vascular embolism, were recorded in this cohort. Case Illustration of a 34-Year-old Male With a Primary Aneurysmal Bone Cyst (ABC) of the L5 Vertebra, Demonstrating the Efficacy of Denosumab as a Second-Line Therapy Following an Incomplete Response to Intralesional Sclerotherapy. (A) Pre-treatment MRI and CT Scans Revealing Extensive Osteolytic Destruction of the L5 Vertebral Body. (B) A CT Scan 3 months after Sclerotherapy Shows Early Ossification, which Correlated With initial Symptomatic Relief. (C) However, at 8 months Post-injection, a Follow-up CT Demonstrates Incomplete Ossification With a Persistent Epidural Component of the Lesion (Arrow), Indicating Treatment Failure. (D) Following the Initiation of Denosumab, a CT Scan at 3 months Shows Marked Progression of Ossification. (E) At 12 months of Denosumab Therapy, Near-Complete, Robust Ossification of the Lesion is Observed Case Illustration of a Boy Aged 3 years and 11 Months, Demonstrating Rapid and Effective Rescue With Denosumab Therapy Following Lesion Progression after initial Intralesional Sclerotherapy for a T8 Primary Aneurysmal Bone Cyst (ABC). (A) Pre-treatment CT Scan Revealing an Osteolytic Lesion Involving the Posterior Elements of the T8 Vertebra. (B) One Month after an initial Sclerotherapy Injection, the Patient Experienced Increased Pain. The Corresponding CT Scan Confirmed Significant Disease Progression, With Expansion of the Osteolytic Defect. (C) Following the Initiation of Denosumab, a CT Scan at 1 month Demonstrates Early Consolidative Changes Within the Lesion, Correlating With a Marked Reduction in the Patient’s Pain. (D) At 3 months of Denosumab Therapy, There is Near-Complete Ossification of the Lesion, which Corresponded to the Complete Resolution of His Symptoms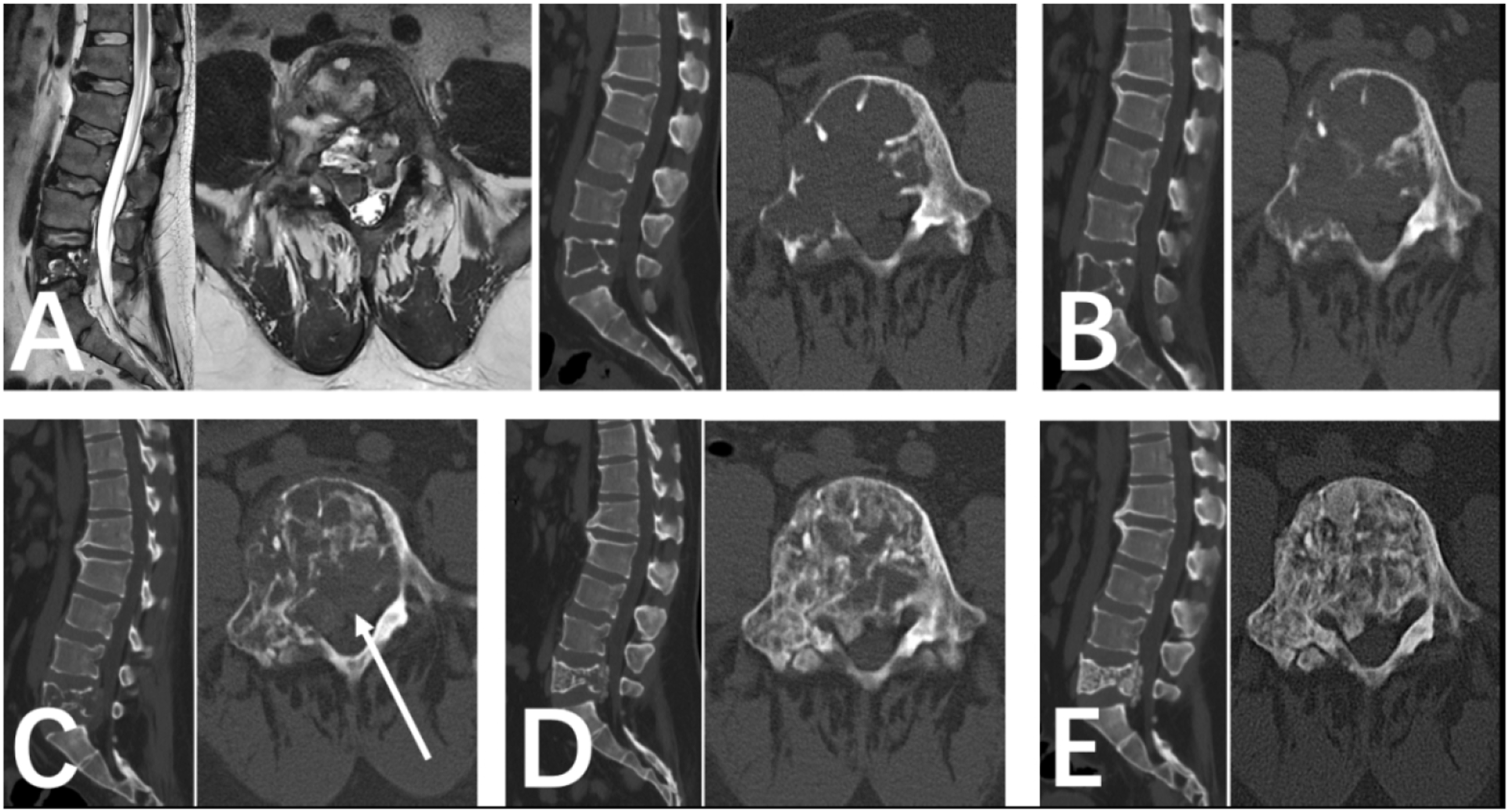
Comparisons of clinical outcomes among the three treatment cohorts revealed no statistically significant differences in recurrence rates (P = 0.227), complication rates (P = 0.382), or the magnitude of improvement in Visual Analogue Scale (VAS) scores (P = 0.907).
Discussion
ABCs were first described as a distinct clinical entity in 1942 by Jaffe et al. and Lichtenstein et al. 14 Although classified as benign, extradural bone tumors, their underlying pathogenesis has been a subject of considerable debate and evolving understanding. Initially, in 1950, Lichtenstein 15 postulated that ABCs were reactive lesions arising from a local vascular disturbance, which led to increased intraosseous pressure, subsequent bone destruction, and expansion. This was followed by a theory from Biesecker et al. 16 in 1970, who proposed that ABCs could represent an aberrant, post-traumatic reparative process. Regarding its pathogenesis, Boriani et al. 4 have postulated that the ABC is a vascular malformation rather than a true neoplasm. This theory is further supported by the consistent identification of a TRE17/USP6 oncogene fusion in these lesions. 17
ABCs predominantly affect individuals in the first two decades of life, with no significant sex predilection, and can involve any part of the skeleton. The natural history of an ABC is understood to progress through 4 distinct phases 18 : (1) The initial osteolytic phase, marked by a periosteal reaction; (2) The growth phase, characterized by progressive bone destruction; (3) The stabilization phase, where the lesion becomes well-circumscribed and expansile with a sclerotic rim and internal septations (the “typical” ABC appearance); and (4) The healing phase, defined by progressive ossification of the lesion.
The management of spinal ABCs is particularly challenging due to the intricate anatomy of the spine and the proximity of these lesions to critical neurovascular structures—a factor that significantly elevates the complexity and risk of iatrogenic injury associated with any intervention. Consequently, there is no consensus in the literature regarding the optimal treatment strategy for spinal ABCs. Therapeutic options range from open surgery (curettage or en bloc resection) and intralesional sclerotherapy (using agents such as doxycycline-albumin, calcitonin with corticosteroids, or concentrated bone marrow aspirate), to pharmacotherapy (Denosumab), selective arterial embolization (SAE), radiotherapy, or a combination of these modalities.7,19 To contribute to this ongoing discussion, the present study reviews our institutional experience with 27 patients treated with one of three primary modalities—open surgery, percutaneous injection, or Denosumab—with the aim of summarizing their respective outcomes.
Open surgery remains a conventional treatment for spinal ABCs and is frequently indicated for patients presenting with severe neurological deficits or pathological fractures causing intractable pain. Surgical approaches are broadly categorized as either intralesional curettage or en bloc resection. For lesions confined to the posterior elements, intralesional curettage via a posterior approach is common. While associated with recurrence rates of 10%-20% in the literature, this technique generally yields favorable clinical outcomes. 4 However, the hypervascular nature of ABCs means that intralesional curettage can be associated with significant intraoperative hemorrhage. In such cases, en bloc resection may be the preferred strategy, with the primary objective being hemorrhage control rather than achieving wide oncologic margins. 19 For more complex lesions involving both the posterior arch and the vertebral body, total spondylectomy may be considered. Although this can achieve a more thorough resection and potentially lower recurrence rates, the requisite extended removal of normal tissue often leads to increased blood loss and perioperative morbidity. 20
Consistent with previous reports, all patients in our surgical cohort experienced improved neurological function and a significant reduction in local pain. The local control rate for surgical resection is reported to be approximately 90% in large case series.21-23 In our study, 1 patient (16.6%) in the surgery cohort developed a recurrence, whereas no recurrences were observed in the non-operative cohorts. The lack of a statistically significant difference in recurrence rates among the groups is likely attributable to the small sample size of our study. Therefore, we recommend that the choice between intralesional and en bloc resection for spinal ABCs should be guided by a preoperative assessment of the anticipated bleeding risk, rather than by the goal of achieving wide surgical margins.
Minimally invasive approaches for spinal ABCs primarily comprise selective arterial embolization (SAE) and intralesional sclerotherapy. However, not all lesions are amenable to SAE, particularly those with small-caliber feeding arteries or arteriovenous fistulas. While Boriani et al. 19 reported excellent outcomes with SAE in 17 cases, the majority of these lesions were located in the lumbar spine, potentially limiting the generalizability to more complex cervical or thoracic locations.
Various sclerosing agents have been described, including local injections of calcitonin with corticosteroids (Tonomura et al. 8 ) and concentrated autologous bone marrow aspirate (Barbanti-Brodano et al. 7 ). In our practice, however, a doxycycline-albumin suspension is the most frequently utilized agent. The successful use of percutaneous doxycycline-albumin injections for spinal ABCs was first reported by Shiels and Mayerson et al. 11 in 2013. The proposed mechanism of action, as described by Shiels et al, 11 directly counteracts the underlying pathophysiology of ABCs. The characteristic USP6 gene rearrangement in these lesions upregulates matrix metalloproteinases (MMPs) and vascular endothelial growth factor (VEGF), which in turn inhibits osteogenesis and promotes osteoclast activity. Doxycycline is thought to work by inhibiting both MMPs and VEGF, thereby suppressing osteoclast function and inducing apoptosis. The albumin component serves as a biocompatible protein carrier, creating a viscous foam that ensures sustained local delivery of the doxycycline. 24
Supporting this approach, Shiels and Mayerson 11 reviewed 20 ABC patients treated with doxycycline-albumin, noting definitive healing responses in all cases, characterized by decreased osteolysis and cortical thickening. Similarly, a previous report from our institution on 14 patients treated with the same technique found that all lesions decreased in size and sclerosed, with no complications or recurrences at a mean follow-up of 30.7 months. The results of the present study are consistent with these favorable outcomes. Despite these positive results, intralesional sclerotherapy has recognized limitations. The multi-septated internal architecture of many ABCs can impede the uniform distribution of the sclerosing agent throughout the lesion. Furthermore, partial ossification following an initial injection may create enclosed compartments, potentially reducing the efficacy of subsequent injections.
The pathogenesis of ABCs is driven by the RANK/RANKL signaling pathway. Osteoclast-like multinucleated giant cells within the lesion highly express the RANK receptor, while stromal cells secrete its ligand, RANKL. The binding of RANKL to RANK activates osteoclast-mediated osteolysis. Denosumab, a human monoclonal antibody, directly targets this pathway by specifically binding to and neutralizing RANKL, thereby preventing its interaction with RANK and inhibiting bone resorption.
The therapeutic application of Denosumab for ABCs was first reported by Lange et al. 10 in 2013 in two cases of postoperative recurrence. Our institutional regimen is adapted from the multicenter case series by Raux et al, 12 consisting of Denosumab at 70 mg/m2 administered subcutaneously, once weekly for 4 weeks, followed by monthly maintenance injections. Concurrent calcium and vitamin D supplementation (calcium acetate and calcitriol in our series) is essential to prevent treatment-related hypocalcemia. In the present study, treatment with Denosumab resulted in significant volumetric reduction of the lesions. This radiological improvement correlated with complete pain relief, a return to normal activities, and no observed recurrences during the follow-up period. Based on our experience, we have found Denosumab to be a particularly effective salvage therapy for cases of postoperative recurrence or for lesions that demonstrate an incomplete response or progression following intralesional sclerotherapy.
Prior to its use in our pediatric patients, a literature review confirmed no significant reports of adverse effects on linear growth. 25 However, a key consideration is the risk of rebound hypercalcemia upon treatment cessation, particularly in children and adolescents who have higher baseline rates of bone turnover. Post-cessation hypercalcemia has been reported to occur at a mean of 5 months after stopping the drug in this population.12,26-28
Our institutional experience contributes to the evolving understanding of spinal ABC management and supports a treatment paradigm that prioritizes minimally invasive approaches. For patients presenting without severe neurological deficits or significant spinal instability, we recommend intralesional sclerotherapy with a doxycycline-albumin suspension as the first-line therapy, acknowledging that multiple injections may be required to achieve complete lesion consolidation. In cases where intralesional therapy yields an incomplete response or the lesion progresses, we advocate for systemic therapy with Denosumab as a highly effective second-line or salvage option, which has proven particularly valuable in our series for inducing significant volumetric reduction and symptomatic relief. Open surgery is not considered our primary treatment modality but remains an indispensable component of the management algorithm, reserved for patients with acute or progressive neurological compromise and significant spinal instability where rapid decompression and stabilization are paramount. Ultimately, the management of spinal ABCs necessitates a personalized approach, and while our proposed strategy has yielded favorable short-term outcomes, the long-term efficacy and potential late-onset complications of these treatments warrant continued, rigorous follow-up.
Limitations
The present study is subject to several inherent limitations. First and foremost, the retrospective design and small sample size—a consequence of the rarity of spinal ABCs—introduce the potential for selection bias and confounding variables. Consequently, large-scale, multicenter, prospective studies are warranted to definitively compare the efficacy of these different therapeutic modalities and to more comprehensively characterize the radiological healing patterns associated with each.
Secondly, the follow-up duration for the Denosumab cohort is considerably shorter than that for the open surgery and percutaneous injection cohorts, a reflection of its more recent incorporation into our treatment paradigm. As recommended by Hauschild et al, 29 extended clinical and radiological surveillance is crucial for several years post-treatment. Therefore, continued monitoring of our Denosumab cohort for a minimum of 5 years will be essential to ascertain long-term efficacy and to definitively rule out late recurrence.
Conclusion
Given the benign natural history of ABCs and the diversity of available treatments, a comprehensive, individualized, and judicious therapeutic strategy is paramount. For patients with spinal ABCs characterized by adequate stability and an absence of severe neurological deficits, intralesional sclerotherapy represents a viable first-line option, offering high efficacy, although multiple administrations may be required. In instances where sclerotherapy is contraindicated or yields a suboptimal response, Denosumab emerges as a valuable second-line therapy; however, its application necessitates a tailored regimen and diligent long-term monitoring to assess therapeutic effect. Finally, while not a primary intervention, open surgery remains indispensable for the rapid correction of spinal instability and the reversal of acute neurological compromise.
Footnotes
Acknowledgements
We thank Miss Chenmei Ren for her help with the data analysis.
Ethical Approval
The study protocol was approved by the institutional research ethics committee ((IRB00006761-M2023022), according to the principles of the Declaration of Helsinki. The institutional review board granted a waiver of informed consent because of the retrospective nature of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant from Peking University Third Hospital (301-2404-01-03) and Peking University Third Hospital (BYSYDL2023003).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Research data supporting this publication are available from the Peking University Third Hospital, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly.