
Abstract
Study Design:
This was an epidemiological study using national administrative data from the MarketScan database.
Objective:
To investigate the impact of early versus delayed adjuvant radiotherapy (RT) on wound healing following surgical resection for spinal metastatic disease.
Methods:
We queried the MarketScan database (2007-2016), identifying patients with a diagnosis of spinal metastasis who also underwent RT within 8 weeks of surgery. Patients were categorized into “Early RT” if they received RT within 4 weeks of surgery and as “Late RT” if they received RT between 4 and 8 weeks after surgery. Descriptive statistics and hypothesis testing were used to compare baseline characteristics and wound complication outcomes.
Results:
A total of 540 patients met the inclusion criteria: 307 (56.9%) received RT within 4 weeks (Early RT) and 233 (43.1%) received RT within 4 to 8 weeks (Late RT) of surgery. Mean days to RT for the Early RT cohort was 18.5 (SD, 6.9) and 39.7 (SD, 7.6) for the Late RT cohort. In a 90-day surveillance period, n = 9 (2.9%) of Early RT and n = 8 (3.4%) of Late RT patients developed wound complications (P = .574).
Conclusions:
When comparing patients who received RT early versus delayed following surgery, there were no significant differences in the rates of wound complications. Further prospective studies should aim to identify optimal patient criteria for early postoperative RT for spinal metastases.
Introduction
Broadening indications for surgical management such as neurological deterioration, spinal instability, and mechanical back pain have increased the role of surgical resection in the management of patients with spinal metastases. 1,2 The landmark study by Patchell et al 3 established a clear role for surgical decompression for spinal metastases, and several studies following have demonstrated the clinical benefit and cost effectiveness of surgery with adjuvant radiotherapy (RT) when compared with RT alone. 2 -5
However, wound healing complications may arise when administering adjuvant RT. 5 -7 Previous reports have indicated RT dose- and frequency-dependent wound breakdown in early postoperative patients. 8 -10 This may be further exacerbated by the cachexic nature of many patients undergoing concurrent chemotherapy. 10 Given the lack of guidelines on optimal postoperative RT timing, the decision is often left to the physician’s discretion, with a need to balance enough time post-operatively for wound healing with a need for RT to limit tumor progression. 11,12
The aim of the current study is to compare the rates of wound complications in patients undergoing early or delayed RT following surgical resection of spinal metastatic disease. We hypothesize that the rates of wound complications will vary between the cohorts, and that patients receiving RT with a longer healing period following surgery will have lower rates of wound complications.
Methods
Data
We obtained a sample of the MarketScan Commercial Claims and Encounters database (Truven Health Analytics, Ann Arbor, MI) from January 1, 2007 to December 31, 2016. This database is a collection of commercial inpatient, outpatient, and pharmaceutical claims of more than 75 million employees, retirees, and dependents representing a substantial portion of the US population covered by employer-sponsored insurance. The MarketScan database contains International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and 10th revision, Clinical Modification (ICD-10-CM), Current Procedural Terminology (CPT), Diagnosis Related Group (DRG) codes, as well as National Drug Codes (DEA).
Sample
A total of 1054 patients with a central nervous metastasis were identified via ICD-9 codes (198.3-198.5) and an associated CPT code for either laminectomy for tumor resection (63 275-63 278, 63 290) or corpectomy for tumor resection (63 300-63 303; 63 101-63 102). Patient records were then queried to identify patients who underwent RT within 8 weeks of surgery via stereotactic radiosurgery (CPT codes 77 435, 77 373, 63 620, 63 621) or external beam 3-dimensional (3D) conformal radiation therapy (CPT codes 77 301, 77 385, 77 386). Patients were categorized into 2 cohorts: early RT if RT was delivered within 4 weeks of surgery, or late RT if delivered between weeks 4 to 8 following surgery. A majority of patients initiated RT within 8 weeks of surgery, and the 4 week cutoff allowed for comparable cohorts to be analyzed. The RT window of 8 weeks was chosen because a vast majority of patients initiated RT in this interval after surgery. The distribution of patients receiving RT during this time was approximately split at the 4-week mark, which was the rationale behind making 4 weeks the cutoff for Early vs Late RT. Patients younger than 18 years or with ICD-9-CM codes consistent with trauma (N = 301) were excluded. A final cohort of N = 540 patients was analyzed (Figure 1).

Cohort diagram.
Outcomes and Variables
The primary outcome of this study was development of a wound complication following adjuvant radiation therapy and index surgery. Wound complication was defined by the following ICD-9-CM codes: wound infection (998.5, 998.51 998.59), wound dehiscence (9983, 99 830, 99 831, 99 832), wound hematoma (9981, 99 811, 999 812, 99 813) or unspecified wound complication (998.8, 99 881, 99 883, 9984, 9989). Patients were stratified not only by early or late RT, but also by surgical type and patient characteristics. Patient-level variables, including age at diagnosis, sex, geographic region, insurance plan type, and quality and cost metrics, were taken directly from the claims data. Complications and primary tumor type were assessed using ICD-9-CM codes.
Analyses
Two-sample t-tests and chi-square tests were utilized to assess significant differences in demographic data, primary tumor source of the spinal metastasis, postoperative complications, quality outcomes, and payments among the groups. P values were interpreted as significant only after applying the Bonferroni correction for multiple comparisons.
Ethical Considerations
All data from these databases was de-identified, and thus this study is exempt from institutional review board approval in accordance with the Health Insurance Portability and Accountability Act of 1996.
Results
Patient Cohort and Baseline Characteristics
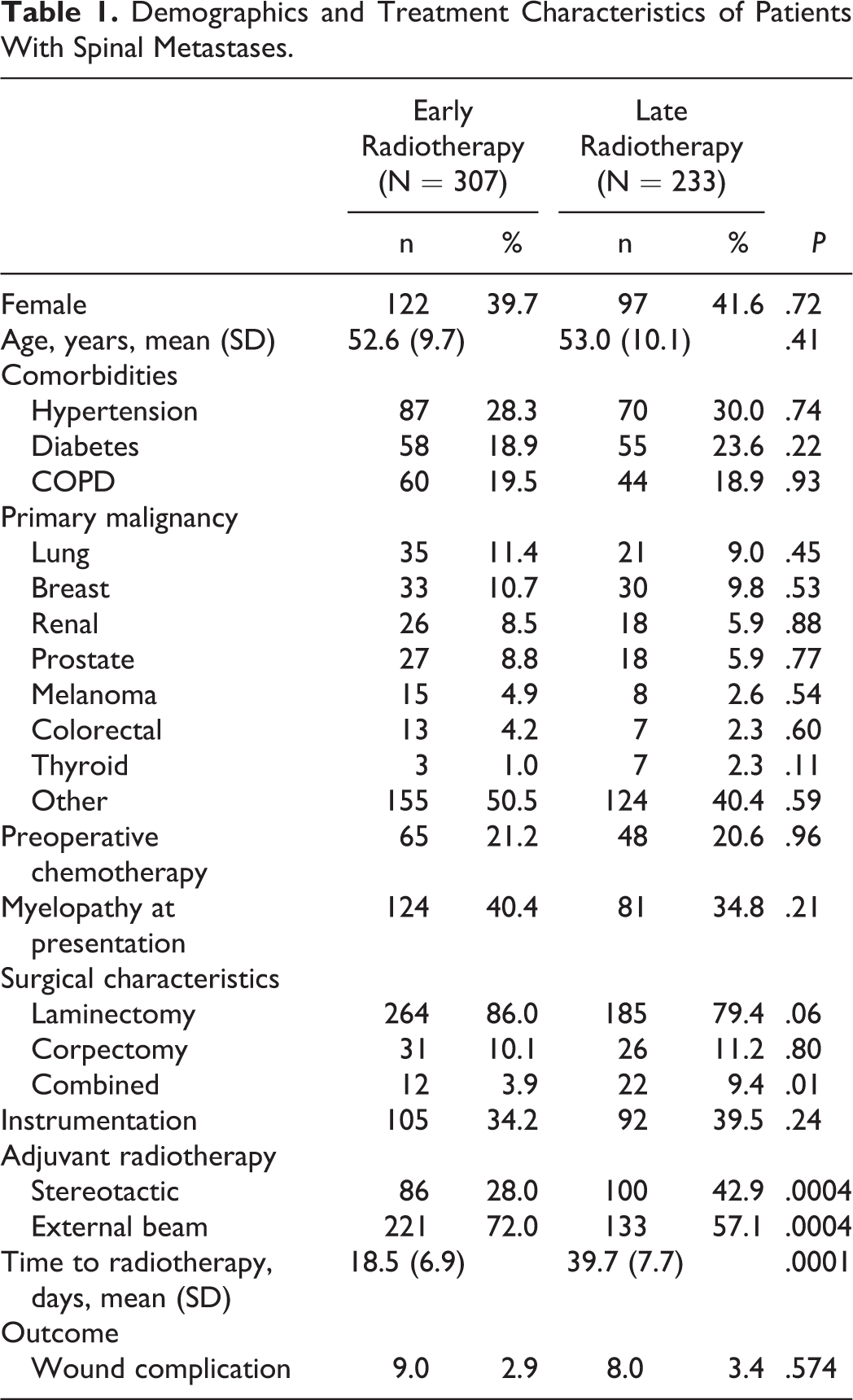
A total of 540 patients met the inclusion criteria of this study, of which 307 (56.9%) received RT within 4 weeks (“early”) and 233 (43.1%) received RT within 4 to 8 weeks (“late”) of surgery (Table 1, Figure 2). Mean days to radiation therapy were 18.5 (SD 6.9) in the Early RT cohort and 39.7 (SD, 7.6) in the Late RT cohort (P < .002). Mean age was 52.6 years (SD, 9.7) in the Early RT patients, and 53.0 years (SD, 10.1) in the Late RT patients. Rates of hypertension, diabetes, and chronic obstructive pulmonary disorder (COPD) between Early and Late RT groups were similar. Lung and breast cancer were the primary malignancies in this study accounting for 11.4% and 10.4% of patients in the Early RT cohort, respectively, and 9.0% and 9.8% in the Late RT cohort, respectively (P = .45, P = .53, respectively).
Demographics and Treatment Characteristics of Patients With Spinal Metastases.
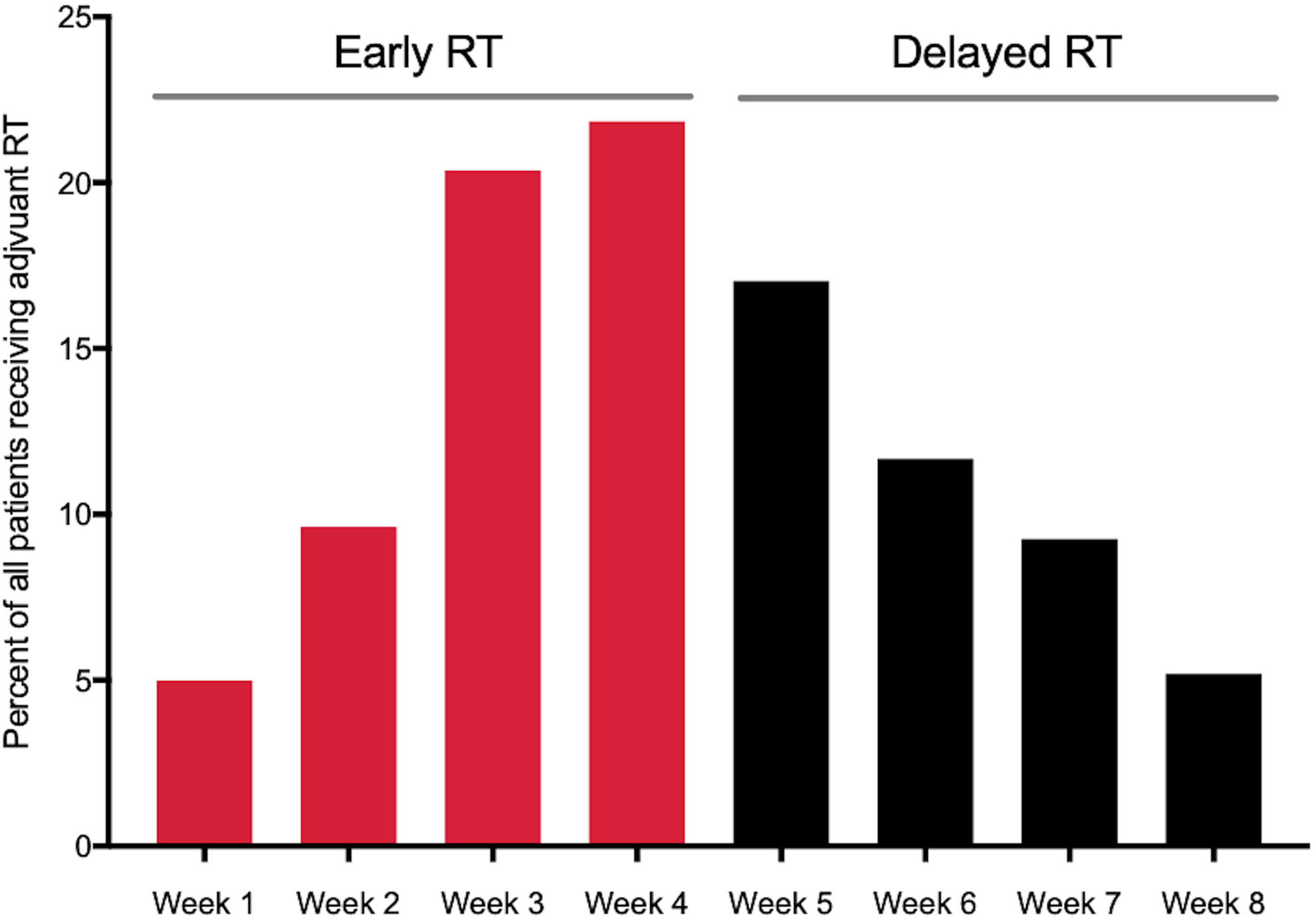
Timing of adjuvant radiotherapy following surgery for spinal metastasis.
Rates of preoperative chemotherapy were greater in the group receiving early RT (21.2% vs 20.6% in Late RT; P > .05). Patients undergoing Late RT had higher rates of combined anterior-posterior procedures (9.4% vs 3.9%; P = .01). The use of spinal instrumentation was similar in both groups (34.2% Early, 39.5% Late; P = .24). Modality of RT delivery was significantly different among groups, with patients undergoing early RT more likely to receive 3D conformal external beam radiation (3DCRT) and patients undergoing late RT more likely to receive stereotactic radiosurgery (SRS): 86 patients (28.0%) in the early RT group received SRS and 100 patients (42.9%) in the late RT group received SRS (P < .002). 3DCRT was used in 221 (72.0%) of Early RT patients, and 133 (57.1%) of late RT patients (P < .002).
Wound Complication Rates of Early Versus Late RT
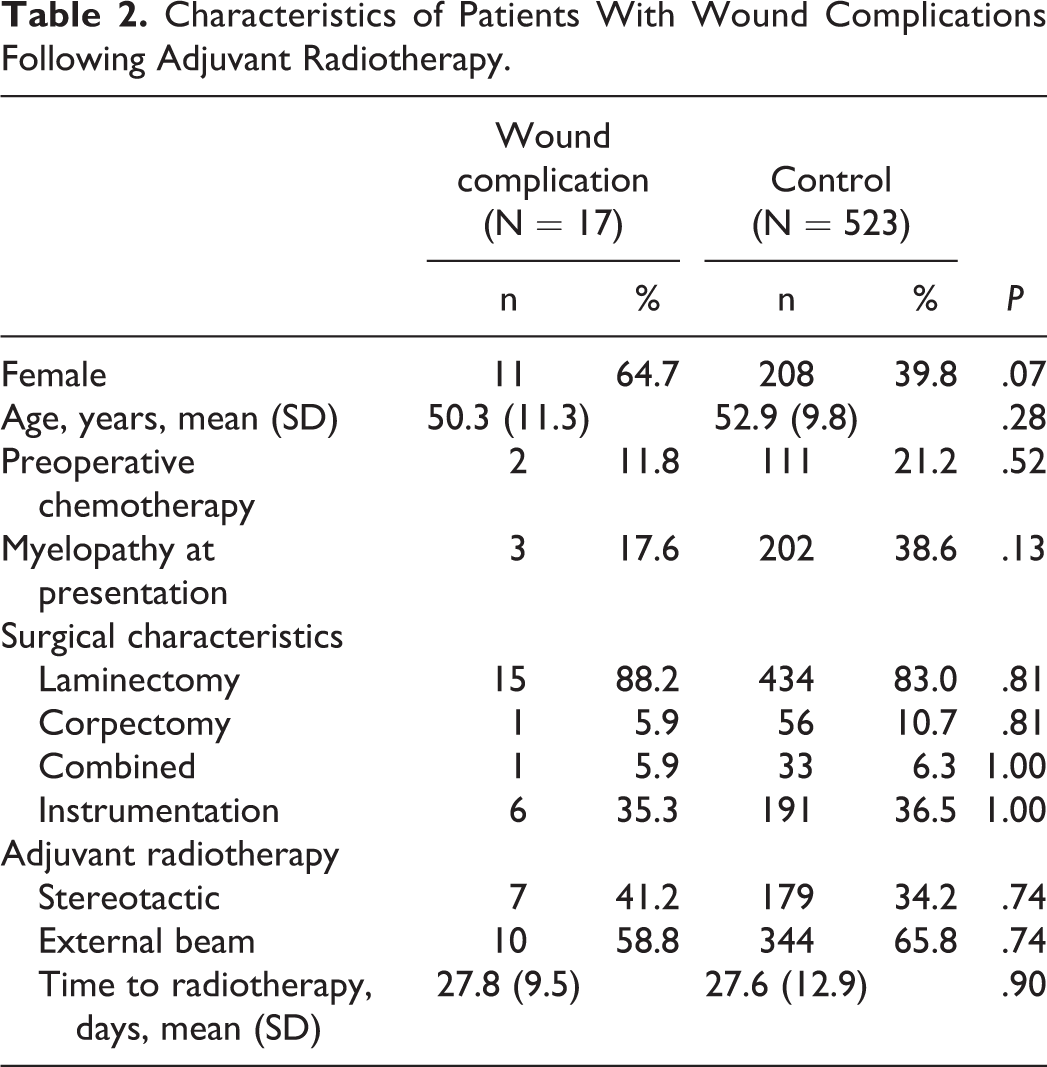
Wound-complication free duration is described for both cohorts in Figure 3. The rate of wound complication within 90 days was not significantly different between groups (Early RT 2.9%, late RT 3.4%; P = .574). Furthermore, there were no significant differences in age, gender, neurological status, type of surgery, type of radiation, and use of preoperative chemotherapy, in patients who developed wound complications versus patients that did not (Table 2).
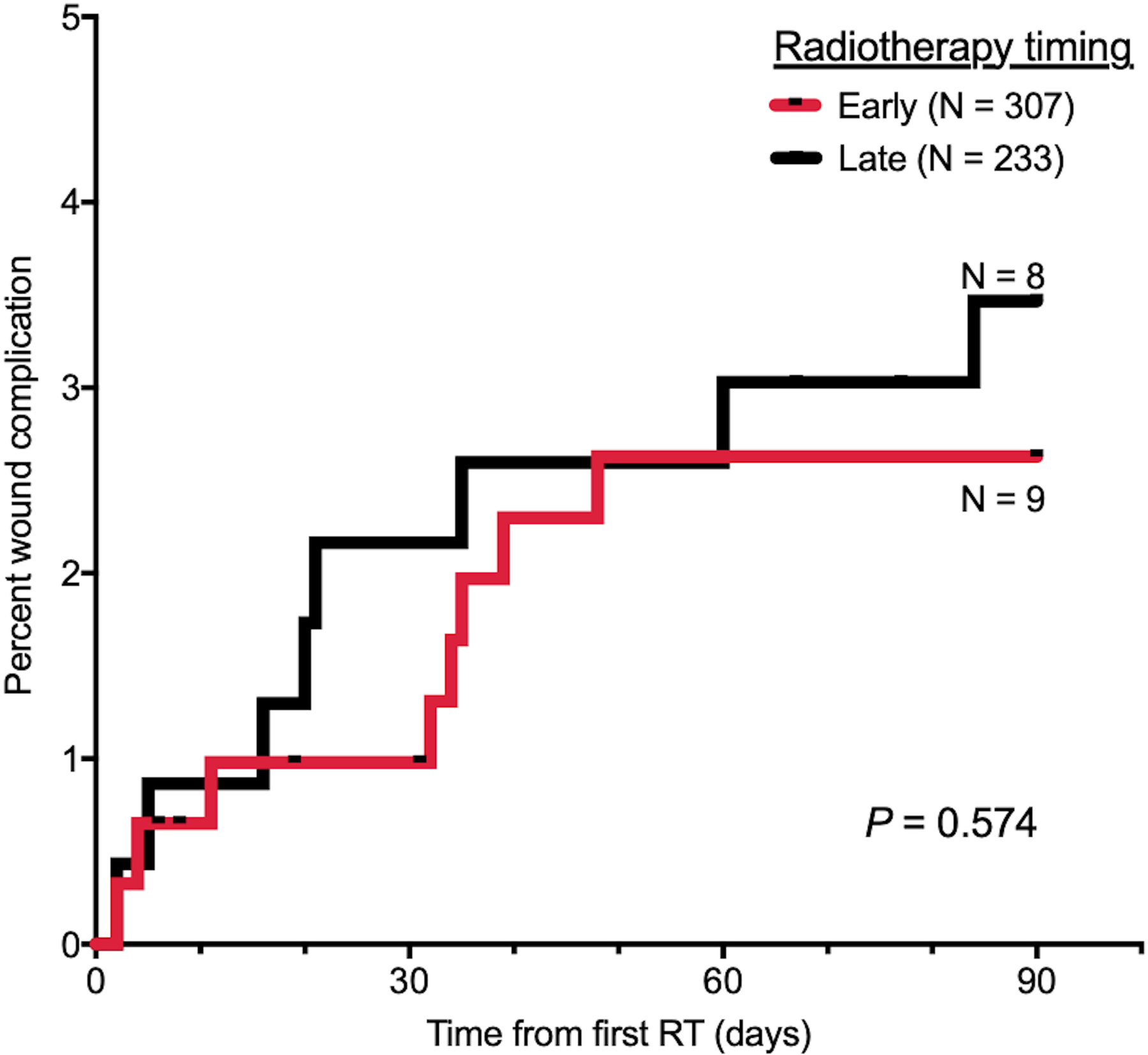
Kaplan-Meier curves for time to wound complication, stratified by radiotherapy timing.
Characteristics of Patients With Wound Complications Following Adjuvant Radiotherapy.
Discussion
Given the increasing role of combined surgery and RT for the management of spinal metastases, the optimal treatment timing is of significant interest. Guidelines have been created regarding optimal dosing and type of RT for spinal metastases based on numerous pathologic features; however, given concerns for wound deterioration, clear strategies for the timing of postoperative RT remain unknown. 11,13 This study utilized a novel dataset to conduct a comparative analysis of patients undergoing surgery and RT for metastatic disease of the spine from 2007 to 2016. Patients were categorized by the timing of RT following surgery: Early RT (delivered within 4 weeks after surgery) or Late RT (delivered between 4 and 8 weeks after surgery). Baseline characteristics, comorbidities, primary tumor type, surgical strategies were similar among cohorts. Although a majority of both cohorts received external beam RT, rates differed significantly between the early and late RT groups (Early RT 72.0%, Late RT 57.1%; P = .0004). This study found no significant difference in the rate of wound complications between the 2 cohorts within 90 days of RT (P = .574).
Early wound healing following surgery is characterized by 2 stages—inflammatory and proliferative. The inflammatory stage occurs 0 to 4 days following surgery, whereas the proliferative stage extends from days 2 to 21 after surgery. This early phase of healing constitutes migration and proliferation of inflammatory cells, and further proliferation of collagen-producing fibroblasts. Radiation during the inflammatory stage has been shown to diminish hyperplasia of inflammatory cells and inhibit deposition of collage during the proliferative stage. 14,15 Granulation, which occurs approximately a week after surgery, is less radiosensitive. 8 However, the preclinical and clinical data supporting this is inconsistent. Devereux et al 16 noted that wound complications rates were similar in rats irradiated after 1 week and those who were not irradiated at all. Another preclinical study found that RT could be more aggressively administered safely, and a 1- to 2-day window following surgery is adequate. 17 A study by Laocharoensombat et al 18 found that 7.1% (n = 1) patients undergoing RT 14 days after surgery for epidural metastases developed wound complications. Finally, a study by Onimus et al in a similar cohort showed that none of their patients (0/16) developed a wound complication when treated with RT 7 days following surgery. 19,20 Our findings echo much of these clinical data and indicate that early RT does not increase the risk of wound complications following resection of a spinal metastasis.
The mechanism of radiation delivery has also been implicated in wound complication development. Postoperative SRS may be a safer option than conventional, external beam radiation, with respect to development of a wound complication. 14,21 -26 However, our study did not find an association of radiation type with wound complications. This may be due to patient selection by the treating physician, where 3DCRT was not performed in patients clinically deemed to be at higher risk of a wound breakdown.
Several patient level and operative characteristics have been implicated as risk factors for wound complications following spine surgery. Patient age, 27,28 obesity, 29 -31 tobacco use, 32 poor nutritional status, 28,32 nonsteroidal anti-inflammatory drug (NSAID) use, 33 and high baseline comorbidity burden have been associated with postoperative wound complication. 34 Posterior surgical approach, tumor resection, revision surgery, 34 increased estimated blood loss (EBL), 35 longer operative time, multilevel fusion, and instrumentation 29 may also increase the risk of wound dehiscence, superficial surgical site infection (SSI), deep SSI, or organ space SSI. Although the initial studies that identified these risk factors were limited by their small sample sizes, more recent large studies using national databases and multivariate regression have corroborated much of these findings. 36,37 Many of these risk factors are not modifiable; however, they help in surgical planning and identifying patients that may benefit from prophylactic antibiotics. There is also a significant financial burden associated with postoperative wound complications—with neurosurgical SSIs contributing to a $23 755 per case increase compared with nonwound complication cases. 38 Wound complications have also been associated with increased mortality and readmission rates, and longer length of stays—making it exceedingly important for spine surgeons to prevent these. 39
Limitations
The main limitations of this study are due to the inherent flaws of the MarketScan administrative dataset. We assumed accuracy of all diagnosis and procedure codes in the database. In particular, we relied on the codes to identify the presence of wound complications, and this may have led to underestimation of true wound complication rates. Furthermore, this study was unable to assess overall tumor burden or extent of tumor progression, factors that could influence RT timing. Additionally, we are unable to determine the size of the wound in each group, and larger incisions could predispose patients to wound breakdown.
As previously mentioned, there are several other factors that may influence the rates of wound complications outside the timing of RT initiation that may confound these results. Because of the low incidence of wound complications, the study was underpowered and we could not conduct a propensity score match or logistic regression to control for the confounders, a limitation of our statistical findings. Further prospective studies are required to examine the impact of these factors. This study also does not answer the question as to whether there is an optimal timing of radiation therapy within the early 4-week postoperative window. The 4-week stratification of Early RT was arbitrary, and does not inform us of a more specific optimal time for adjuvant RT.
Conclusions
When comparing patients who received RT early vs delayed following surgery, there were no significant differences in the rates of wound complications, suggesting that adjuvant RT can be commenced within 4 weeks of surgery with an acceptable complication rate. Further prospective studies should aim to identify optimal patient criteria for early postoperative RT for spinal metastases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.