
Abstract
Study Design
A retrospective database analysis.
Objective
To determine the incidence of lower extremity deep vein thrombosis (DVT) and identify risk factors associated with DVT development in patients with spinal cord injury (SCI), stratified by level of injury.
Methods
The National Inpatient Sample from 2016 to 2021 was used to identify adult inpatients with SCI who developed DVT within the same admission and to categorize them by anatomical injury level. Multivariable logistic regression was used to assess independent risk factors by SCI level.
Results
Among 59,498 SCI patients, the overall DVT incidence was 2.8%. The DVT rate was lowest in cervical SCI (2.6%) and highest in thoracic SCI (3.2%). Pulmonary embolism was a strong independent risk factor for DVT across all SCI levels ([Cervical] OR: 12.82, CI: 10.46-15.63, [Thoracic] OR: 11.82, CI: 9.13-15.20, [Lumbar] OR: 11.38, CI: 6.74-18.74). For cervical SCI, risk factors included coagulopathies (OR: 1.90, CI: 1.54-2.32), older age (OR: 1.01, CI: 1.01-1.02), complete (OR: 1.84, CI: 1.43-2.35) or incomplete cervical lesion (OR: 1.38, CI: 1.17-1.63), cervical (OR: 1.34, CI: 1.16-1.54) or lumbar fracture (OR: 1.58, CI: 1.17-2.11), and upper extremity DVT (OR: 3.58, CI: 2.53-4.97). For thoracic SCI, risk factors included thoracic fracture (OR: 1.46, CI: 1.20-1.77), upper extremity DVT (OR: 3.82, CI: 2.18-6.36), and fluid/electrolyte disorder (OR: 1.35, CI: 1.13-1.62). For lumbar SCI, fluid/electrolyte disorder (OR: 1.92, CI: 1.38-2.66) was an independent predictor.
Conclusion
DVT incidence and risk factors vary by SCI level. Identifying these factors is critical for stratifying care and developing tailored prophylactic strategies that prevent adverse events and optimize patient outcomes.
Background
Traumatic spinal cord injury (SCI) results from an acute insult to the spinal cord, leading to transient or permanent neurologic deficits below the level of injury.1,2 In the United States, SCI has an annual incidence of roughly 54 per million, translating to approximately 18,000 new cases yearly. 3 Patients with SCI are susceptible to a range of complications that significantly decrease life expectancy,1,2,4 among which thromboembolic events represent a major concern. Among all hospitalized trauma patients, those with SCI have the highest risk for deep vein thrombosis (DVT) development, 5 with earlier studies reporting DVT rates as high as 100% in the absence of prophylaxis.6,7
Despite advancements in prophylactic management, DVT and its most serious complication, pulmonary embolism (PE), remain one of the leading causes of mortality in this population.8,9 Notably, long-term survival outcomes for patients with SCI have shown minimal improvement over the past several decades.4,10,11 DVT originating in the lower extremities poses a particularly high risk for progression to clinically significant PE,12,13 with the greatest mortality risk from thromboembolism occurring within the first three months post-injury.14-20
Previous studies have proposed various potential risk factors for DVT development in SCI, including older age, race, male sex, comorbidities, and paraplegia.5,16,18,21-24 However, these findings have been largely inconclusive due to small sample sizes and limited generalizability of single-institution studies.5,16,18,22,24 More crucially, prior studies have examined risk factors for DVT across all spinal levels in SCI, yet emerging evidence suggests that thromboembolic risk and complications vary substantially depending on the level of injury.17,25-27 Large-scale, multicenter studies utilizing nationally representative population data remain scarce, and no study to date has thoroughly investigated the DVT risk factors in relation to the different SCI levels. The present study aims to fill this critical gap by leveraging data from the National Inpatient Sample (NIS) database to stratify risk factors for lower extremity DVT by SCI level. To our knowledge, this is the first study to identify demographic and clinical risk factors associated with the development of symptomatic lower extremity DVT by level of SCI using a large population database.
Materials and Methods
Study Design and Setting
This is a retrospective study analyzing the de-identified patient data set from the National Inpatient Sample (NIS). The NIS is one of the largest publicly available databases of inpatient healthcare information in the United States (US). It captures approximately 98% of the US patient population across roughly 4500 hospitals in 49 states participating in the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality (AHRQ). 28 NIS is a 20% stratified sample of all discharges from US community hospitals, including specialty hospitals, public hospitals, academic medical centers, and long-term acute care facilities. 29 Annually, the NIS data reports on over 7 million hospital stays, providing detailed discharge information such as International Classification of Diseases (ICD) codes, demographics, comorbidity measures, and other variables. 28 Data collection and management is a collaboration between experienced community hospital staff, medical administrators of state and private organizations, hospital associations, and the federal government.28,30 The HCUP and AHRQ are not responsible for the conclusions drawn from this analysis. Due to the implementation of ICD-10-CM in October 2015, the analysis was restricted to data collected after 2015. 31
Eligibility Criteria
The 2016 to 2021 NIS database was used to identify adult (
Variables
The records were segregated into different spinal levels and compared between those who developed DVT vs those who did not. Data were collected on two main domains, namely: (a) Demographic characteristics: Age, sex, race, insurance status, patient location, etc. (b) Clinical data: Length of stay, costs, smoking status, Elixhauser comorbidity index (ECI),
32
and mortality.
Neurological injury was categorized into complete and incomplete spinal cord lesions. A complete SCI was defined as the total absence of sensory and motor function in the lowest sacral segments S4-5. 33 An incomplete SCI was defined as the preservation of any sensory or motor function below the neurological level that includes the lowest sacral segments S4-5. 34 The ECI paralysis variable was excluded to avoid redundancy with the SCI classification.
Data Management and Missing Data
Data was extracted using password-protected Microsoft ® Excel for Microsoft 365, version 2206 - Build 15330.20306 (Publisher: Microsoft Corporation, Redmond, Washington, USA, 2022). The de-identified patient data were analyzed using the Statistical Analysis System for Windows, Version 9.4 (Publisher: SAS Institute Inc., Cary, North Carolina, USA, 2013). The pairwise deletion method was utilized to deal with variables with missing data points.
Quantitative Variables and Statistical Methods
Demographic characteristics and clinical data, including history of infections, medical history, and laboratory data, were summarized using descriptive statistics. All monetary values were reported in United States Dollar (USD). The normal distribution of data was verified using Kolmogorov-Smirnov’s normality test. Continuous variables were represented as Mean (Standard Deviation - SD), and categorical variables as frequency (percentage). Categorical variables with normal distribution were compared using Pearson’s Chi-square statistical tests. Between-group comparisons (DVT versus no DVT) were made using z-test with P-values adjusted using the Bonferroni method. After the univariate analysis, multivariable logistic regression was done, adjusting for age, sex, race, and selected comorbidities to characterize statistical associations with the development of DVT. Statistical significance for all analyses was set at P < 0.05.
Results
Incidence
Incidence Rates of Deep Vein Thrombosis by Spinal Cord Injury Levels
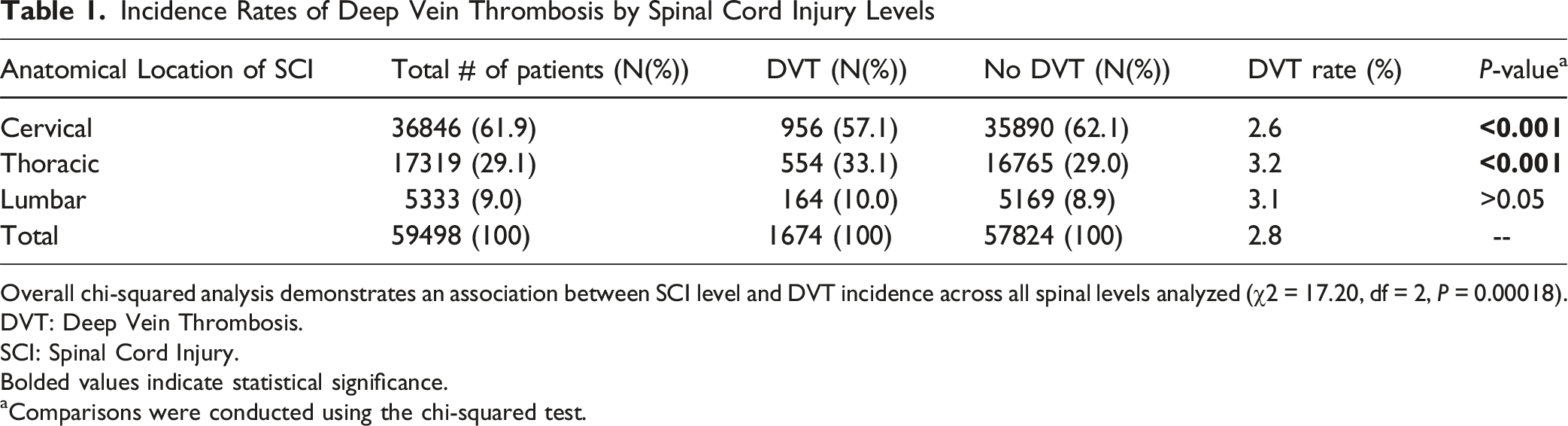
Overall chi-squared analysis demonstrates an association between SCI level and DVT incidence across all spinal levels analyzed (χ2 = 17.20, df = 2, P = 0.00018).
DVT: Deep Vein Thrombosis.
SCI: Spinal Cord Injury.
Bolded values indicate statistical significance.
aComparisons were conducted using the chi-squared test.
Patient Demographics and Characteristics
Demographic Characteristics of Patients With Cervical Spinal Cord Injury With or Without Lower Extremity Deep Vein Thrombosis Between 2016 and 2021 in the United States
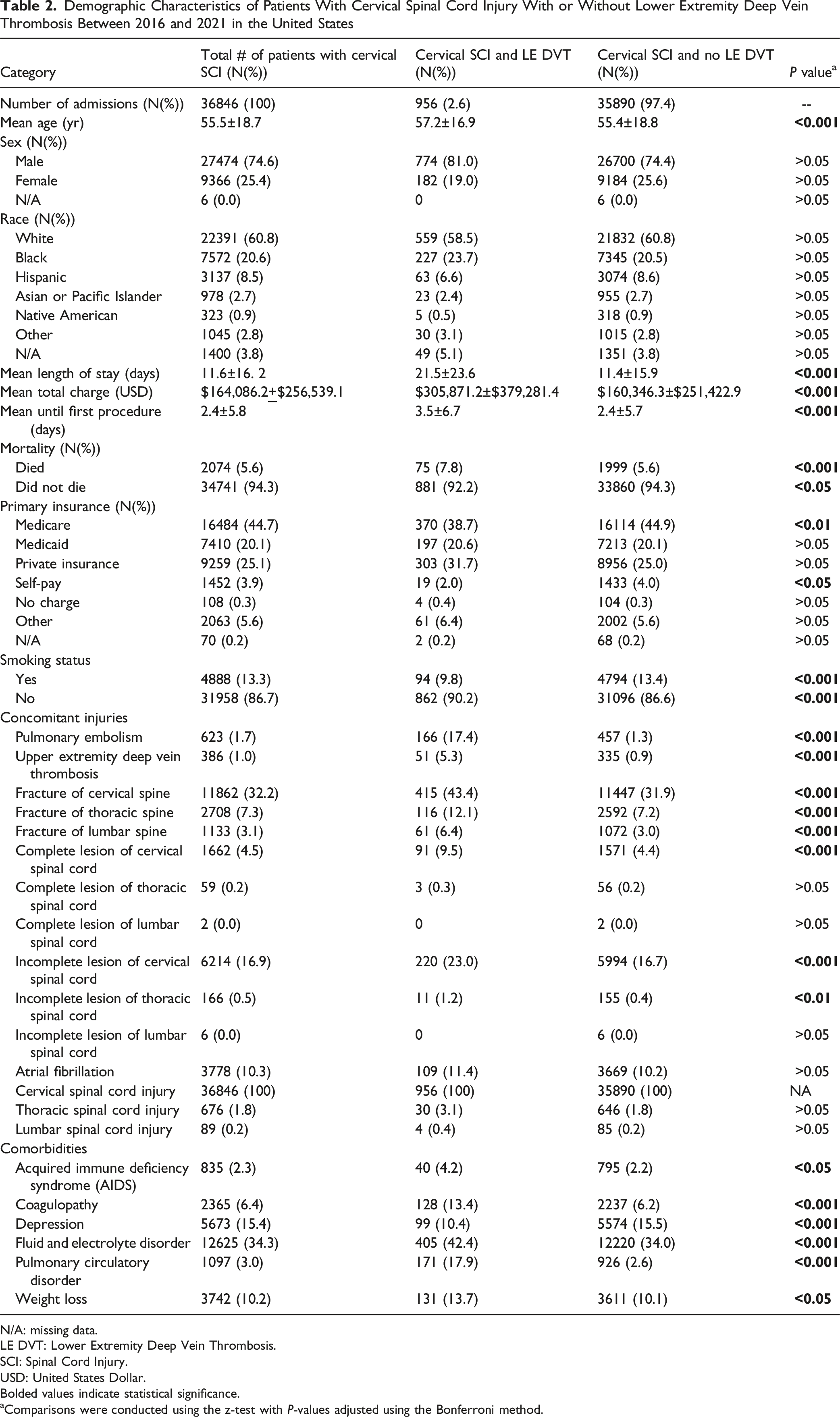
N/A: missing data.
LE DVT: Lower Extremity Deep Vein Thrombosis.
SCI: Spinal Cord Injury.
USD: United States Dollar.
Bolded values indicate statistical significance.
aComparisons were conducted using the z-test with P-values adjusted using the Bonferroni method.
Demographic Characteristics of Patients With Thoracic Spinal Cord Injury With or Without Lower Extremity Deep Vein Thrombosis Between 2016 and 2021 in the United States
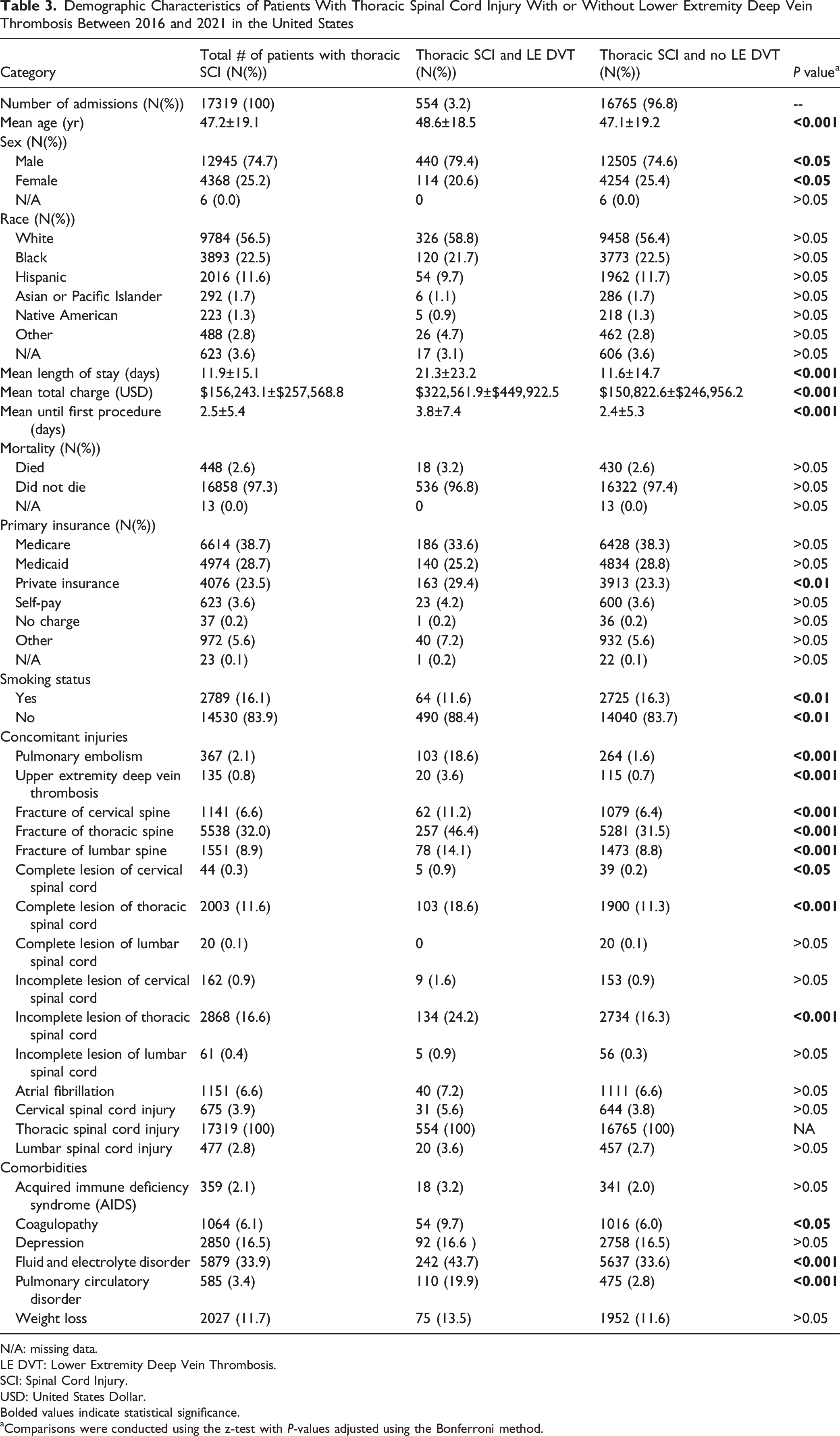
N/A: missing data.
LE DVT: Lower Extremity Deep Vein Thrombosis.
SCI: Spinal Cord Injury.
USD: United States Dollar.
Bolded values indicate statistical significance.
aComparisons were conducted using the z-test with P-values adjusted using the Bonferroni method.
Demographic Characteristics of Patients With Lumbar Spinal Cord Injury With or Without Lower Extremity Deep Vein Thrombosis Between 2016 and 2021 in the United States
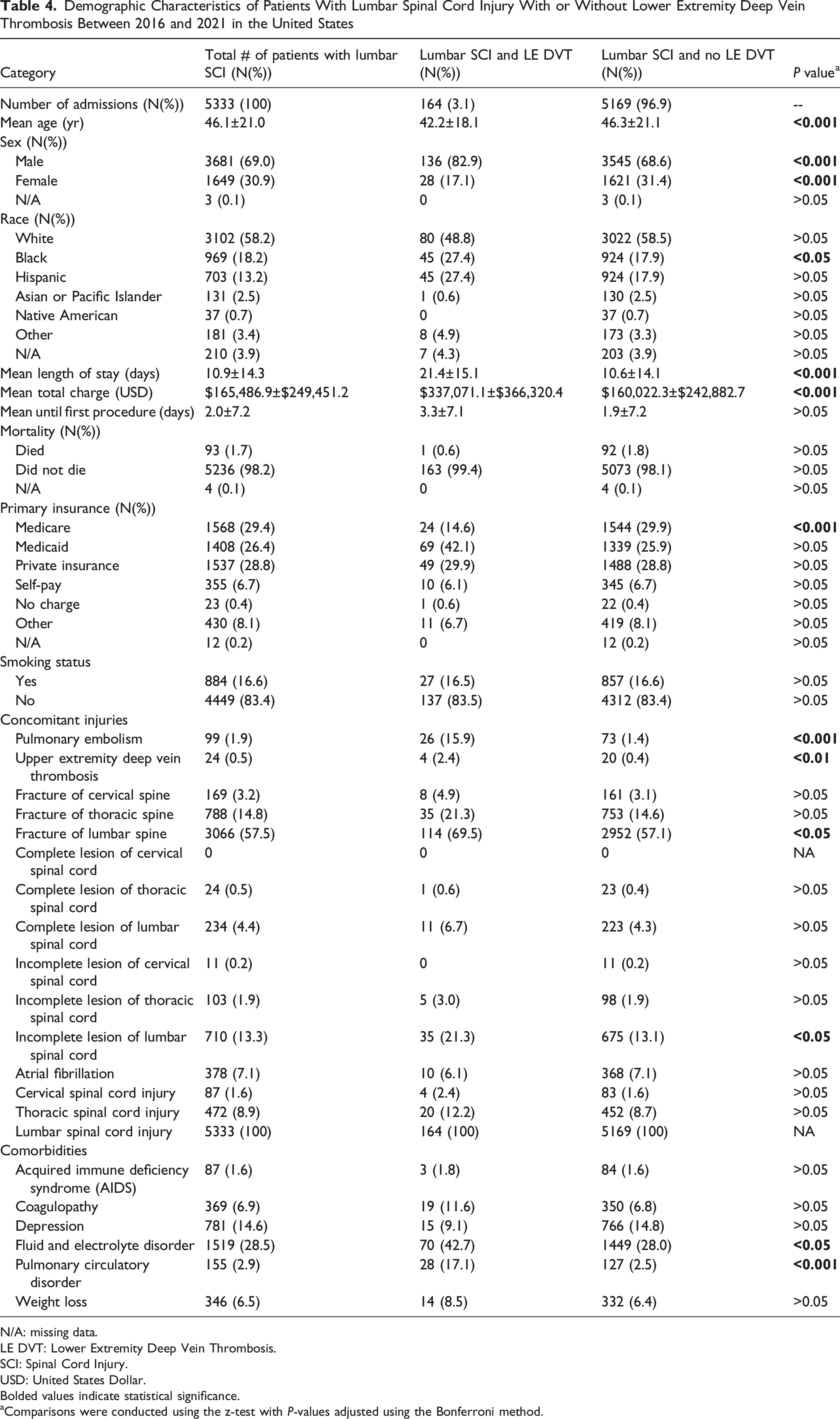
N/A: missing data.
LE DVT: Lower Extremity Deep Vein Thrombosis.
SCI: Spinal Cord Injury.
USD: United States Dollar.
Bolded values indicate statistical significance.
aComparisons were conducted using the z-test with P-values adjusted using the Bonferroni method.
Cervical SCI Risk Factors for DVT
Multivariate logistic regression analysis identified several significant risk factors associated with lower extremity DVT in patients with cervical SCI, including coagulopathies (Odds Ratio [OR]: 1.90, 95% Confidence Interval [CI]: 1.54-2.32, P < 0.001), complete cervical spinal cord lesions (OR: 1.84, CI: 1.43-2.35, P < 0.001), incomplete cervical spinal cord lesions (OR: 1.38, CI: 1.17-1.63, P < 0.01), concurrent cervical fractures (OR: 1.34, CI: 1.16-1.54, P < 0.01), concurrent lumbar fractures (OR: 1.58, CI: 1.17-2.11, P < 0.05), upper extremity DVT (OR: 3.58, CI: 2.53-4.97, P < 0.001), and pulmonary embolism (OR: 12.82, CI: 10.46-15.63, P < 0.001). Although older age was statistically significant (OR: 1.01, CI: 1.01-1.02, P < 0.001), its effect size was clinically negligible (Figure 1A). (A) Cervical: Multivariate Logistic Regression Adjusted for Age, Sex, Race, and Selected Factors. Note. Multivariate logistic regression adjusted for age, sex, year of admission, race, and selected comorbidities for cervical spine injury. Comparisons were conducted using the z-test with p-values adjusted using the Bonferroni method. Red dots denote statistically significant positive predictors based on odds ratio, while green dots denote statistically significant negative predictors. Bolded values indicate statistical significance. (B) Thoracic: Multivariate Logistic Regression Adjusted for Age, Sex, Race, and Selected Factors. Note. Multivariate logistic regression adjusted for age, sex, year of admission, race, and selected comorbidities for thoracic spine injury. Comparisons were conducted using the z-test with p-values adjusted using the Bonferroni method. Red dots denote statistically significant positive predictors based on odds ratio, while green dots denote statistically significant negative predictors. Bolded values indicate statistical significance. (C) Lumbar: Multivariate Logistic Regression Adjusted for Age, Sex, Race, and Selected Factors. Note.. Multivariate logistic regression adjusted for age, sex, year of admission, race, and selected comorbidities for lumbar spine injury. Comparisons were conducted using the z-test with p-values adjusted using the Bonferroni method. Red dots denote statistically significant positive predictors based on odds ratio, while green dots denote statistically significant negative predictors. Bolded values indicate statistical significance.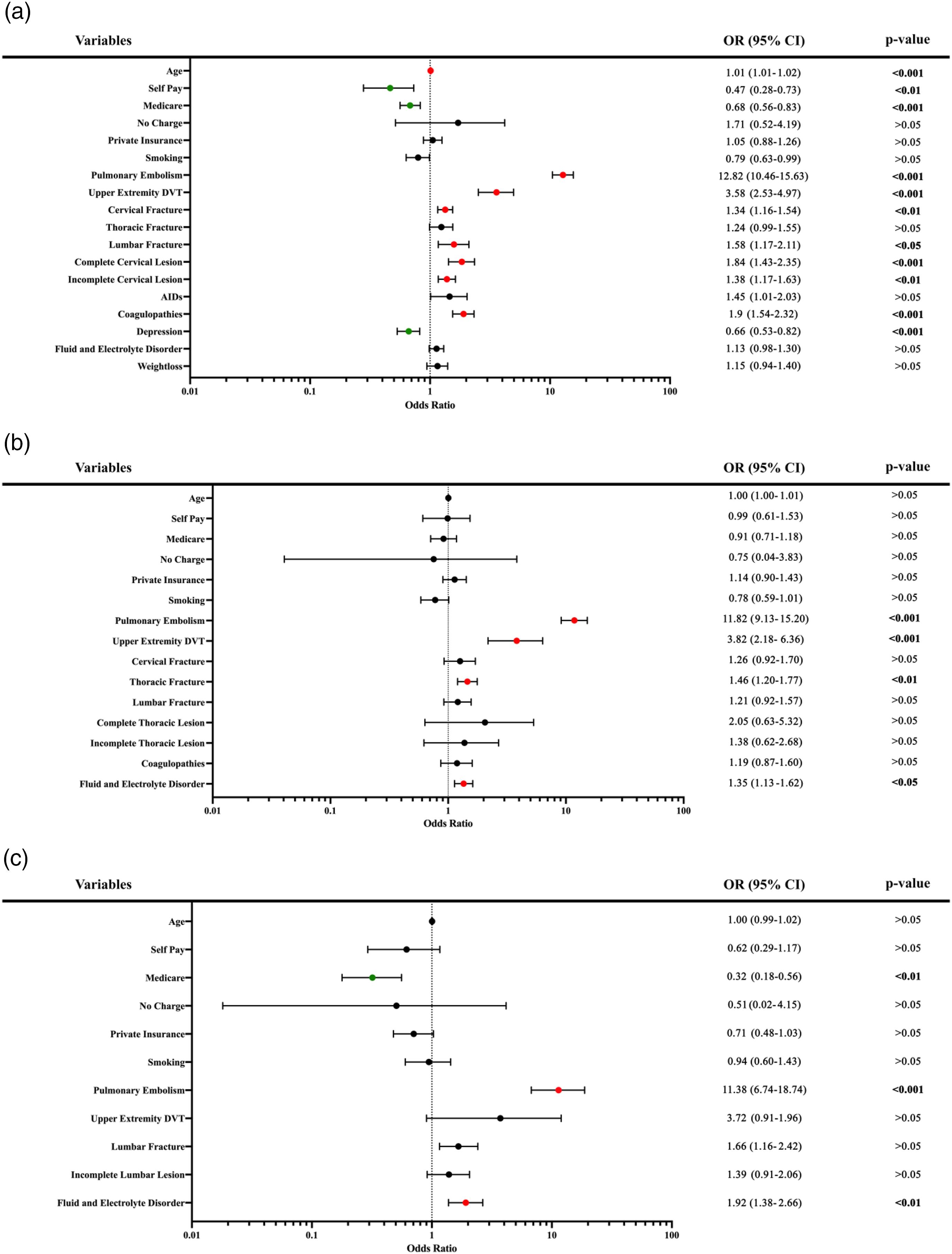
Thoracic SCI Risk Factors for DVT
Multivariate logistic regression analysis showed that upper extremity DVT (OR: 3.82, CI: 2.18 – 6.36, P < 0.001), pulmonary embolism (OR: 11.82, CI: 9.13 - 15.20, P < 0.001), thoracic fractures (OR: 1.46, CI: 1.20 – 1.77, P < 0.01), and fluid/electrolyte disorder (OR:1.35, CI:1.13-1.62, P < 0.05) were significantly associated with thoracic SCI and developing a lower extremity DVT (Figure 1B).
Lumbar SCI Risk Factors for DVT
Multivariate logistic regression analysis highlighted fluid and electrolyte disorders (OR: 1.92, CI: 1.38 – 2.66, P < 0.01), and pulmonary embolism (OR: 11.38, CI: 6.74-18.74, P < 0.001) as significantly associated with lumbar SCI and developing a lower extremity DVT (Figure 1C).
Outcomes
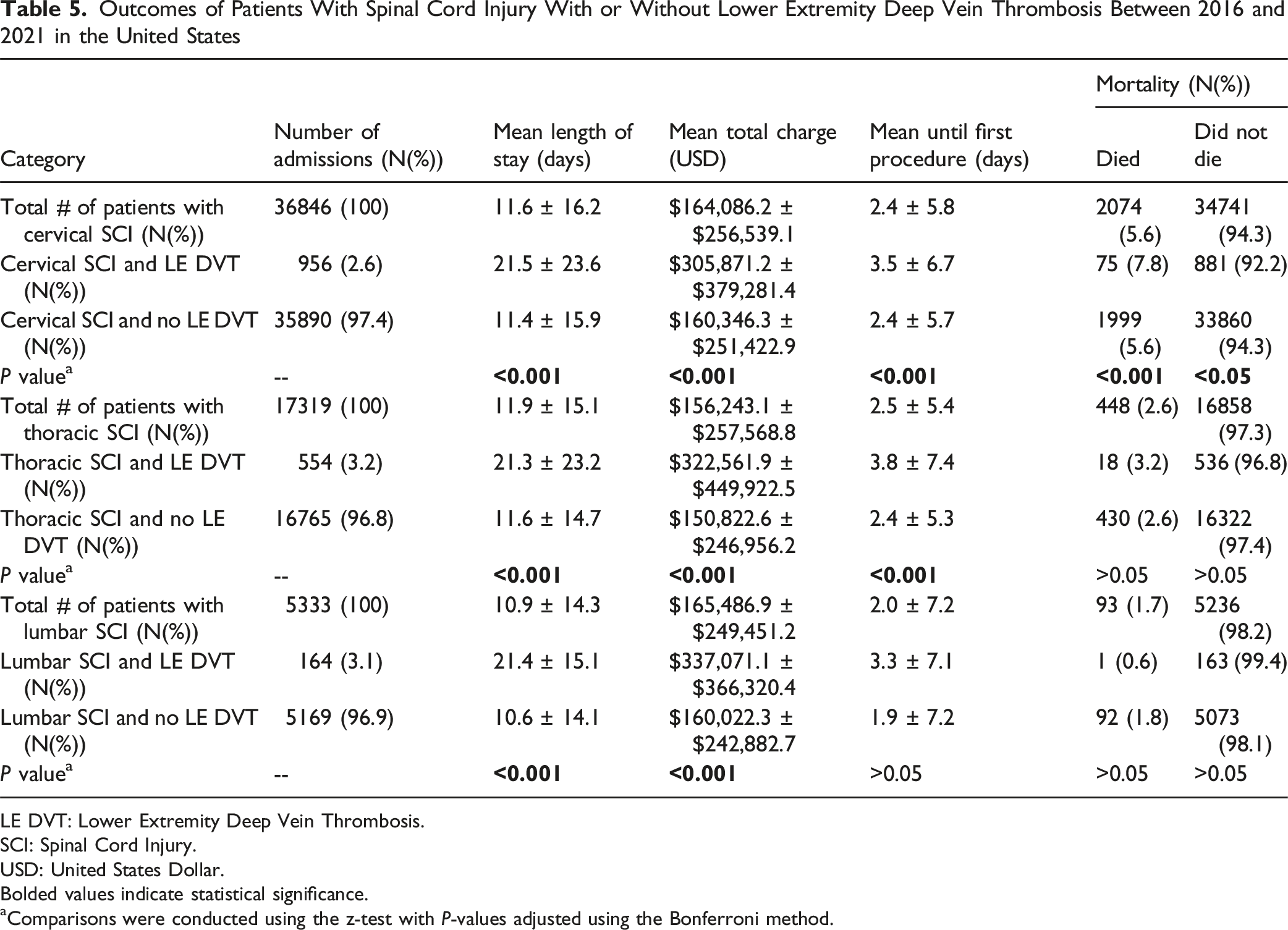
Outcomes of Patients With Spinal Cord Injury With or Without Lower Extremity Deep Vein Thrombosis Between 2016 and 2021 in the United States
LE DVT: Lower Extremity Deep Vein Thrombosis.
SCI: Spinal Cord Injury.
USD: United States Dollar.
Bolded values indicate statistical significance.
aComparisons were conducted using the z-test with P-values adjusted using the Bonferroni method.
Patients with thoracic SCI and lower extremity DVT also had increased length of stay (21.3 ± 23.2 days vs 11.6 ± 14.7 days, P < 0.001), and higher total costs ($322,561.9 ± $449,922.5 vs $150,822.6 ± $246,956.2, P < 0.001) compared to those without DVT (Table 5).
Patients with lumbar SCI and lower extremity DVT had increased length of stay (21.4 ± 15.1 days vs 10.6 ± 14.1 days, P < 0.001) and higher total costs ($337,071.1 ± $366,320.4 vs $160,023.3 ± $242,882.7, P < 0.001) compared to those without DVT (Table 5).
Mortality
Cervical SCI and the development of lower extremity DVT were associated with increased mortality (7.8% vs 5.6%, P < 0.001) compared to those who did not develop DVT (Table 5). No significant association between DVT and mortality was observed in the thoracic and lumbar SCI cohorts.
Discussion
Thromboembolic events, particularly DVT and PE, are major contributors to mortality among patients with SCI.4,9,35 Although complications following SCI have been extensively investigated, there is a lack of robust analyses identifying DVT risk factors stratified by cervical, thoracic, and lumbar spinal injuries. In this national database analysis, we identified thoracic SCIs as having the highest DVT risk, followed by lumbar and cervical SCIs. Risk factors for DVT in cervical SCI included coagulopathies, advanced age, complete injuries, and concurrent cervical and lumbar fractures. In both cervical and thoracic SCIs, lower extremity DVT was associated with concomitant upper extremity DVT. In thoracic and lumbar SCIs, DVT was associated with fluid and electrolyte disturbances. Multivariate logistic regression - adjusted for age, sex, race, and selected factors - revealed that PE was a strong, independent predictor of lower extremity DVT in patients with cervical, thoracic, and lumbar SCIs.
Incidence
The overall incidence of DVT across all spinal injury levels in our study was 2.8%, which aligns with the 3.4% rate reported by Maung et al. in a large population-based analysis. 25 However, the reported DVT incidences in the SCI populations across all spinal levels vary widely in the remaining literature, ranging from 2% to 100%.5,6,21,22,36-39 These discrepancies may be attributed to limitations in earlier studies, including small sample sizes, single-institution designs, variations in prophylactic protocols, and heterogeneity in DVT screening methods.5,6,21,22,36-39
Cervical SCIs constituted the largest cohort in our study yet had the lowest DVT incidence (2.6%) compared to lumbar (3.1%) and thoracic SCIs (3.2%). This lower incidence of cervical SCIs may be attributed to the higher mortality rates we observed associated with these injuries, reducing the number of survivors at risk for DVT. In contrast, thoracic or lumbar SCIs were not associated with increased mortality in our study. Consistent with our findings, DeVivo et al reported a relative risk of mortality of 11.1 for cervical SCIs at C1 to C3 compared to thoracic and lumbosacral injuries, suggesting survivor bias rather than indicating a true lower incidence of DVT in cervical SCI. 40 Thus, early mortality in patients with cervical SCIs may precede DVT onset and lead to underestimation of its incidence. Additionally, although current literature is limited in comparing prophylactic practices by injury level, it is possible that patients with cervical SCIs are more likely to receive early or aggressive prophylaxis, which could contribute to the lower observed DVT incidence.
Our findings underscore that the anatomical location of SCI influences DVT risk overall, with the strength of the association varying by injury level. While the present study’s level-specific differences in DVT incidence broadly align with prior investigations, there are differences in rank order.15,25 Specifically, Maung et al. reported the highest DVT incidence in thoracic SCIs (5.1% for T1-T6 and 3.71% for T7-T12), followed by cervical (2.7% - 3.8% for C1-C4 and C5-C7, respectively), and then lumbar (2.53%). 25 However, Maung et al conducted their analysis using the National Trauma Data Bank (NTDB), which relies on voluntarily submitted data, limiting its national representativeness and validity for inferences on injury incidence and prevalence.25,41,42 Conversely, Chung et al. found cervical SCI to carry the highest risk for DVT (HR = 2.96, 95% CI = 2.43, 3.61), followed by thoracic (HR = 2.68, 95% CI = 2.05, 3.50), and then lumbar SCI (HR = 1.60, 95% CI = 1.25, 2.05). 15 While partially consistent with our findings, Chung et al.’s study utilized data derived from the Taiwan National Health Insurance Research Database, which may reflect geographic variations in SCI distribution and risk.
Shared Risk Factors Across SCI Levels
Common risk factors for DVT across all SCI levels align with Virchow’s triad, encompassing hypercoagulability, venous stasis, and endothelial injury.43,44 Systemic complications such as pneumonia, sepsis, and multiple organ failure exacerbate hypercoagulability, while immobilization significantly contributes to venous stasis. These physiological effects are particularly prominent in higher-level spinal injuries, where the extent of neurological deficit and systemic dysregulation is greatest.45-51 Consequently, the number of independent risk factors for DVT decreases progressively from cervical to lumbar injuries, reflecting the reduced motor and autonomic impairment at lower-level spinal injuries.
Upper extremity DVT was identified as a shared risk factor for lower extremity DVT in both cervical and thoracic SCI. This reflects the profound immobility, thrombotic risks associated with catheter use, and systemic hypercoagulability in high-level injuries. Unlike lumbar SCIs, upper cervical and thoracic SCIs may disrupt sympathetic outflow and impair systemic vascular tone, necessitating the use of central venous catheters and peripherally inserted catheters for hemodynamic stabilization.52-54 These catheters can precipitate endothelial injury and worsen venous stasis, predisposing high-level SCI patients to thrombosis.43,44,54-59
Furthermore, the loss of upper extremity and trunk mobility following cervical SCI and the loss of trunk mobility following thoracic SCI may further promote venous stasis.60,61 This can increase the risk of upper extremity DVT, which is associated with concurrent lower extremity DVT in up to 16% of patients. 58
Our analysis found that both complete and incomplete lesions of the cervical and thoracic spine are independent risk factors for lower extremity DVT in cervical and thoracic SCI, respectively. This observation is consistent with prior studies, which report loss of motor function as a significant risk factor for VTE.6,14,22,23,25 Patients with American Spinal Injury Association Impairment Scale (AIS) A and B grades — indicating complete or incomplete loss of motor function—are particularly susceptible to DVT.62,63 Higher-level SCIs often result in severe immobility,2,61,64 leading to venous stasis in the lower extremities. 60 Additionally, autonomic dysregulation resulting from SCI at or above the T6 spinal level disrupts vascular tone, further promoting venous pooling.45,65,66 This creates a prothrombotic environment as blood viscosity increases, increasing muscle hypoxia and decreased contractility. 67 These shared mechanisms may collectively underlie the elevated DVT risk in cervical and thoracic SCIs and highlight the importance of vigilant monitoring and proactive thromboprophylaxis in high-level SCIs to mitigate cascading thromboembolic events.
Cervical SCI Risk Factors
As described by multivariate analysis, patients with cervical SCIs possessed several unique risk factors for lower extremity DVT, including coagulopathy, older age, and concurrent fractures. While coagulopathy as a risk factor is not surprising, the association of coagulopathy with cervical SCIs, as opposed to thoracolumbar injuries, may be due to unique cardio-pulmonary impairment and the systemic complications of these lesions. In contrast to lower injury levels, cervical SCI often results in more pronounced respiratory impairment due to disruption of the diaphragm and accessory muscle innervation,45,68,69 leading to respiratory muscle dysfunction45,70 and a hypoxic environment that promotes fibrin deposition.71-73 Furthermore, compared to thoracic and lumbar SCIs, cervical SCIs are more frequently associated with systemic complications such as sepsis, pneumonia, and multiple organ failure,25,27,74 which can activate coagulation pathways and increase thrombotic risk.75-78 For instance, Maung et al reported pneumonia in 51.1% of cervical SCI cases compared to only 18.9% in lumbar cases, 25 while Hoffman et al. observed higher rates of sepsis in cervical SCI but not in thoracic or lumbar SCIs. 27 Collectively, these findings suggest that a multifaceted pathophysiology associated with cervical SCIs heightens the DVT risk in these patients.
Older age was uniquely associated with DVT risk in cervical SCI, further emphasizing the vulnerability of this population. While age is a well-established risk factor for VTE, including DVT, in patients with SCI, this association has predominantly been established through studies that did not differentiate risk by injury level.14,15,20,21,25,79,80 Our findings suggest that specifically cervical-level injuries primarily drive the relationship between age and VTE in SCI. In elderly patients, the upper cervical levels are commonly injured, 81 and inherent age-related changes such as increased thrombosis risk and venous insufficiency,82,83 as well as cervical spine degeneration, may further predispose them to DVT.84,85 In contrast, prior studies suggest that thoracic and lumbar SCIs occur predominantly in younger adults, which may explain why older age was not associated with DVT risk in these injury levels.86,87
Thoracic SCI Risk Factors
Although thoracic SCI risk factors closely parallel those of cervical SCI, fluid and electrolyte disorders were an additional significant risk factor for patients with thoracic lesions. While prior studies have suggested that the level of injury does not influence electrolyte imbalances, these studies were limited by small sample sizes and did not distinguish between complete and incomplete lesions.88,89 For injuries at the level of T6 and above, autonomic dysreflexia can disrupt blood pressure dysregulation and lead to renal dysfunction. 90 Meanwhile, injuries involving T10 to L1 directly impair renal innervation, resulting in electrolyte disorders from altered kidney function and renal deterioration,91,92 which exacerbate inflammatory responses and promote VTE development.93,94 Fluid and electrolyte disorders may be associated with DVT risk in thoracic but not cervical SCI due to the preserved compensatory mechanisms, such as anti-diuretic hormone release and activation of the renin-angiotensin-aldosterone system (RAAS) for incomplete cervical lesions.95,96 In contrast, thoracic SCI disrupts the renal sympathetic nerves directly, impairing RAAS activation and further increasing the risk of DVT.
Lumbar SCI Risk Factors
Fluid and electrolyte imbalances were the primary contributors to DVT risk in patients with lumbar SCI. These findings are consistent with a study by Fineberg et al, which identified fluid electrolyte disorders as risk factors for developing both DVT and PE in patients undergoing lumbar spine surgery. 97 Although suboptimal renal perfusion and bladder innervation may contribute to fluid imbalances and DVT risk in both thoracic and lumbar SCIs, lumbar SCIs uniquely impair calf muscle pump activity, a key driver of venous return, leading to venous stasis. 98 Lumbar SCI had fewer predictive factors for lower extremity DVT than cervical and thoracic SCI. This difference may be attributed to the anatomical location of the conus medullaris, which terminates above L2, most commonly at the level of L1.99-101 As a result, lumbar injuries are less likely to involve the spinal cord itself and may only partially disrupt vascular regulation, reducing the extent of autonomic dysfunction and immobility commonly associated with higher-level SCIs.
Outcomes
Patients with lower extremity DVT across all SCI levels experienced significantly prolonged hospital stays and increased healthcare costs compared to those without DVT. In cases of cervical SCI, the presence of DVT led to a significant increase in the average length of stay, while total hospital charges were significantly increased across cervical, thoracic, and lumbar regions. This highlights the considerable economic and resource burden of DVT in patients with SCI. Longer hospitalizations are likely due to the need for additional interventions to address thromboembolic complications, which include further imaging, anticoagulation treatment, and ongoing monitoring, as well as secondary complications such as pain and decreased mobility. Higher healthcare costs also arise from the need for specialized prophylaxis, diagnostic imaging, potential surgical interventions, along with the prolonged use of inpatient care facilities. Implementing early DVT prophylaxis, either immediately following an injury or preoperatively, may reduce incidence, shorten hospital stays, and decrease costs, ultimately optimizing hospital resource utilization while providing clinical benefits.
Clinical Implications
These findings emphasize the need for a proactive, risk-stratified approach to DVT management in patients with SCI. For individuals with a prior history of DVT, coagulopathy, or prolonged immobility, early preoperative screening, including targeted blood tests for clotting markers, could facilitate the timely identification of high-risk patients. Additionally, early and aggressive mobilization strategies for patients capable of ambulation should be prioritized as soon as clinically feasible. The strong association between lower extremity DVT and PE, in cervical SCI (OR: 12.82, CI: 10.46-15.63, P < 0.001), thoracic (OR: 11.82, CI: 9.13 - 15.20, P < 0.001), and lumbar (OR:11.38, CI: 6.74-18.74, P < 0.001) underscores the need for targeted prevention strategies. Although routine venous duplex ultrasonography is not currently recommended for DVT screening in all SCI patients, its selective use in high-risk cervical SCI patients may facilitate early detection and intervention. 102 Additionally, extended-duration pharmacological prophylaxis may provide a benefit for those with persistent immobility or other risk factors for PE, such as cervical and thoracic SCIs, with some evidence supporting prophylaxis beyond 12 weeks.103-105 However, further research is needed to determine the optimal duration of prophylaxis based on SCI level and recovery trajectory. In addition, electrolyte imbalances – particularly within the first two weeks of SCI – represent a significant yet underexplored risk factor for VTE.88,89,106 Careful fluid management and renal monitoring may be an effective strategy to reduce DVT risk in thoracic and lumbar SCI patients. Such interventions must be weighed against the potential risks of bleeding and fluid overload, emphasizing the importance of individualized treatment plans informed by injury level, mobility status, and systemic comorbidities.
Limitations
The current study’s primary strength lies in its large sample size and nationally representative dataset across the United States. Nevertheless, this study has several limitations. As a retrospective analysis, the study is subject to biases, including potential underreporting, misclassification, and missing data, which may impact the findings. Additionally, use of the NIS database has inherent limitations, including the absence of detailed clinical information such as physical and neurological exam findings, imaging results, and biomarker data to inform diagnostic accuracy. Furthermore, DVT screening methods may differ across different institutions, introducing heterogeneity in DVT identification rates.5,6,21,22,36-39 Another limitation is the lack of detailed temporal information on diagnoses, chronic conditions, and comorbidities, making it challenging to establish clear causal relationships. Additionally, databases typically do not routinely gather granular information such as the precise treatment regimen used, complications encountered during treatment, the patient’s functional and neurological status, and the AIS grades, all of which can provide insight into additional risk factors. While stratifying SCI according to AIS grading would have provided additional insight into additional risk factors, this was not feasible due to the limitations of ICD coding, which does not directly correspond to AIS classifications. Although it can be reasonably inferred that a complete lesion aligns with AIS-A, further differentiation (eg, AIS-B, C, D, E) requires detailed neurological examinations or specific documentation that was not available in the NIS. This restricts our ability to correlate the level of functional impairment with thromboembolic risk in SCI patients. Additionally, neurologic injury was identified using SCI-related diagnostic codes, which may not fully capture non-SCI causes of motor impairment (eg, stroke) that influence thrombotic risk. Furthermore, the NIS database provides only a limited view of each patient’s index admission and de-identifies all personal identifiers, resulting in each readmission being documented as an independent, new admission, thus potentially leading to an overestimation of rates. Despite these limitations, we performed multivariate analyses to control for confounding variables, offering the largest nationwide dataset analysis on identifying risk factors for DVT in SCI.
Conclusion
In our analysis, we identified critical risk factors for DVT in patients across different SCI levels. Using the NIS, we stratified DVT risk factors for cervical, thoracic, and lumbar SCI, demonstrating significant variability in risk based on injury level. Prior studies have largely combined all SCI levels or focused predominantly on cervical injuries, overlooking the distinct nuances in DVT risk associated with injury level. Specifically, thoracic SCI was associated with the highest incidence of DVT, followed by lumbar and cervical SCIs, with each level presenting unique risk factors. Patients with higher-level SCIs may benefit from earlier initiation or extended DVT prophylaxis and screening, whereas those with lower-level SCIs may require additional monitoring and management of fluid and electrolyte imbalances to reduce thrombotic risk. By using the NIS, a large national database, our study offers robust statistical power and broad generalizability, addressing the limitations of previous studies that likely reflected regional patterns. Our findings underscore the importance of tailored DVT prophylactic strategies based on SCI level and offer evidence for refining DVT risk stratification in SCI patients. Future studies should confirm these associations and validate the efficacy of SCI level-based DVT prophylactic interventions.
Supplemental Material
Supplemental Material - Risk Factors for Lower Extremity Deep Vein Thrombosis by Spinal Cord Injury Level: A Population-Based Analysis
Supplemental Material for Risk Factors for Lower Extremity Deep Vein Thrombosis by Spinal Cord Injury Level: A Population-Based Analysis by Alejandro Pando, MD, PhD, Caryn J. Ha, MSc, Yaxel Levin-Carrion, BA, Ahmed Sabra, BA, Max Ward, MD, Daniel M. Schneider, MD, Drew Thibault, DO, Sheng-fu Larry Lo, MD, and Daniel M. Sciubba, MD, MBA in Global Spine Journal.
Footnotes
Ethical Considerations
The NIS is a deidentified administrative database exempt from the Institutional Review Board approval and informed consent requirements.
Author Contributions
Alejandro Pando: conceptualization, methodology, formal analysis, investigation, writing – original draft, writing – review & editing; Caryn J. Ha: conceptualization, formal analysis, investigation, writing – original draft, writing – review & editing; Yaxel Levin-Carrion: investigation, writing – original draft, writing – review & editing; Ahmed Sabra: investigation, writing – original draft, writing – review & editing; Max Ward: methodology, writing – review & editing; Daniel M. Schneider: methodology, writing – review & editing; Sheng-fu Larry Lo: conceptualization, writing – review & editing; Daniel M. Sciubba: conceptualization, writing – review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the finding of this study are available from the first author (AP) upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.