
Abstract
Study Design:
Systematic review.
Objectives:
The objective of this study was to answer 5 key questions: What is the comparative effectiveness and safety of (1a) anticoagulant thromboprophylaxis compared to no prophylaxis, placebo, or another anticoagulant strategy for preventing deep vein thrombosis (DVT) and pulmonary embolism (PE) after acute spinal cord injury (SCI)? (1b) Mechanical prophylaxis strategies alone or in combination with other strategies for preventing DVT and PE after acute SCI? (1c) Prophylactic inferior vena cava filter insertion alone or in combination with other strategies for preventing DVT and PE after acute SCI? (2) What is the optimal timing to initiate and/or discontinue anticoagulant, mechanical, and/or prophylactic inferior vena cava filter following acute SCI? (3) What is the cost-effectiveness of these treatment options?
Methods:
A systematic literature search was conducted to identify studies published through February 28, 2015. We sought randomized controlled trials evaluating efficacy and safety of antithrombotic strategies. Strength of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.
Results:
Nine studies satisfied inclusion criteria. We found a trend toward lower risk of DVT in patients treated with enoxaparin. There were no significant differences in rates of DVT, PE, bleeding, and mortality between patients treated with different types of low-molecular-weight heparin or between low-molecular-weight heparin and unfractionated heparin. Combined anticoagulant and mechanical prophylaxis initiated within 72 hours of SCI resulted in lower risk of DVT than treatment commenced after 72 hours of injury.
Conclusion:
Prophylactic treatments can be used to lower the risk of venous thromboembolic events in patients with acute SCI, without significant increase in risk of bleeding and mortality and should be initiated within 72 hours.
Introduction
Patients with spinal cord injury (SCI) are at an increased risk of venous thromboembolic (VTE) events due to hypercoagulability, stasis, and intimal injury. 1 Interruption of neurologic impulses and paralysis cause metabolic changes to the blood vessels and altered venous competence such as decreased distensibility and increased flow resistance. 2 Furthermore, immobilization of the lower extremities results in stagnant blood flow and ultimately the formation of venous thrombi. Patients with SCI often require complex spinal surgical procedures to decompress and stabilize their spine and, as a result, are often immobilized for several hours and subjected to further tissue and vessel damage.
VTE is a significant cause of morbidity and mortality in SCI patients and includes both deep vein thrombosis (DVT) and pulmonary embolism (PE). 1 Venous thrombi most commonly form in the lower extremities; here they remain as chronic venous abnormalities, undergo endogenous fibrinolysis and recanalization, or propagate and embolize to the pulmonary system. Obstruction of the pulmonary arteries may lead to a number of life-threatening physiologic changes, including impaired gas exchange, cardiovascular compromise, and right-sided heart failure.
The prevention of DVT and PE is critical in this high-risk population. Prophylactic treatment with anticoagulants and other mechanical strategies may significantly reduce the risk of VTE events in these patients. There may be significant risks to anticoagulant thromboprophylaxis in trauma patients, including symptomatic hematoma formation, enlargement of a spinal cord contusion, worsening of neurologic deficits, bleeding, and mortality. 3,4
The objective of this study was to conduct a systematic review to address the following key questions:
In adult patients with acute complete or incomplete traumatic SCI,
Materials and Methods
Electronic Literature Search
A systematic search of the literature was performed to identify potential studies published through February 28, 2015. Studies in all languages were considered for inclusion. The MEDLINE database was searched using the PubMed interface to identify primary studies and systematic reviews. The Cochrane Collaboration Library and bibliographies of relevant articles were also searched. We focused on studies designed to evaluate the efficacy/effectiveness and safety of pharmacological, mechanical, and/or prophylactic IVC filter in adults with complete or incomplete acute SCI. Specifically, we sought studies that reported the risks of PE, DVT, bleeding, mortality, and other adverse events following prophylactic treatment. In addition, we searched for studies that examined the optimal timing to initiate and discontinue prophylaxis.
The search strategies are described in the Supplemental Material (available in the online version of the article) and included use of controlled vocabulary (MeSH terms) as well as keywords. For all key questions, terms for anticoagulation were combined with terms specifying SCI. Additional terms for timing were added to the search strategy for Key Question 4 (Supplemental Material). For Key Questions 1, 2, and 3, we focused on randomized controlled trials (RCTs) that evaluated pharmacological and mechanical prophylaxis, and/or prophylactic IVC filters. Since timing of an intervention is a characteristic more likely observed than randomized, we expanded our criteria for Key Question 4 to include all comparative studies. We excluded nonclinical studies, case series, narrative reviews, abstracts/proceedings from meetings, white papers, editorials, and studies with fewer than 10 subjects per treatment arm. The PICO table provides a complete summary of our inclusion/exclusion criteria (Table 1).
Inclusion and Exclusion Criteria.
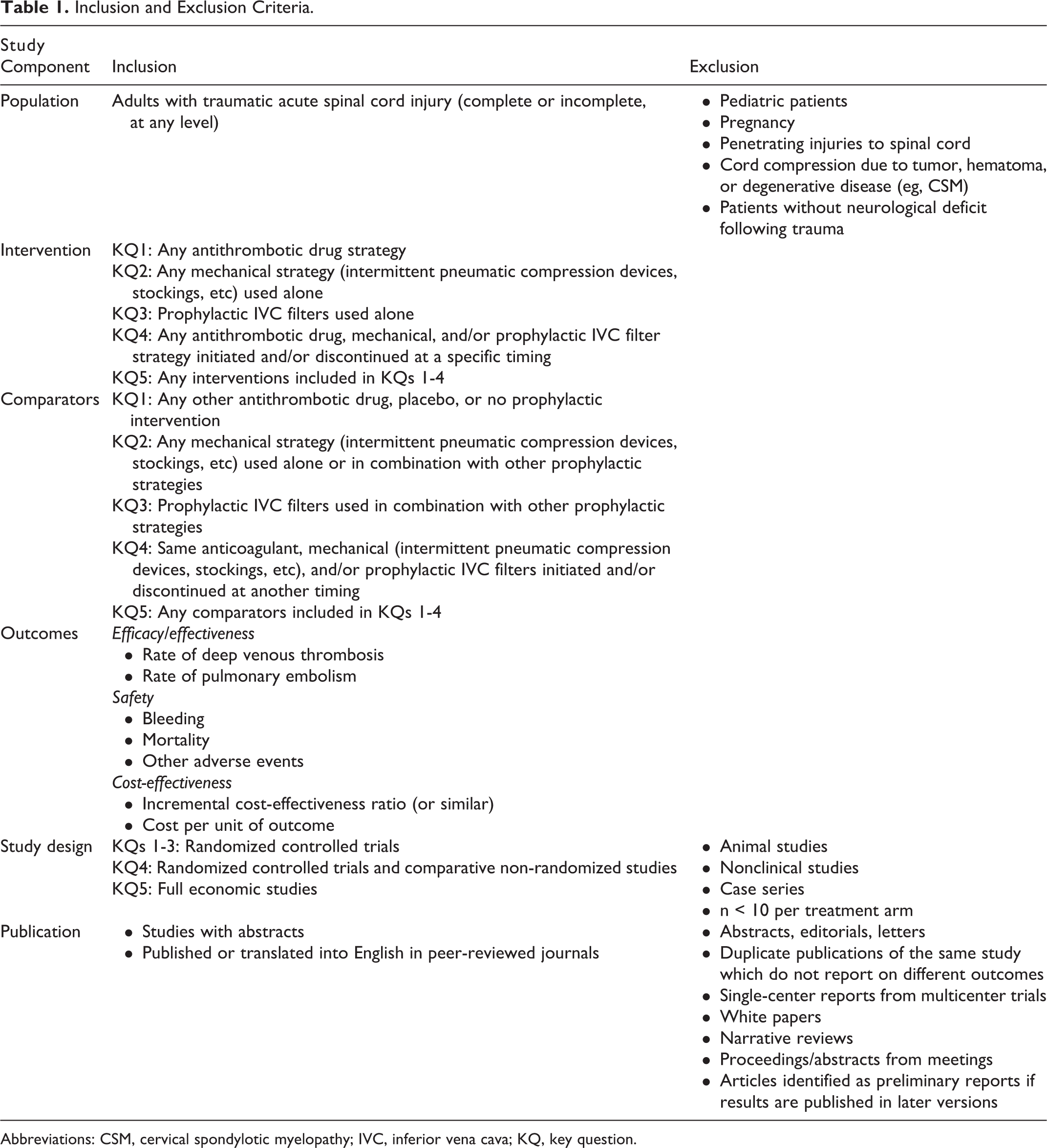
Abbreviations: CSM, cervical spondylotic myelopathy; IVC, inferior vena cava; KQ, key question.
Study Selection and Data Abstraction
Studies were included if they examined either (1) the efficacy and/or safety of anticoagulation prophylaxis or (2) the optimal timing to initiate and/or discontinue prophylaxis in patients with acute SCI. Two reviewers (JH and HH) independently identified potential studies from the literature search. In instances of disagreement regarding inclusion, a third reviewer (DN) was consulted and consensus achieved through discussion. If an article published in a foreign language appeared to meet inclusion criteria based on the English abstract, we used Google Translate 5 to translate the entire article into English. If any part of the translation was unclear, we sought human translation assistance.
One reviewer (JH) used standardized forms to extract the following data: age, sex, completeness and level of SCI, dose and frequency of antithrombotic drugs, intervention characteristics for mechanical and/or invasive prophylaxis, timing and duration of prophylaxis, methods used to diagnose DVT and PE, and results. A second reviewer checked the abstractions for accuracy and completeness (HH).
Individual Study Quality
Two independent reviewers (HH and DN) critically appraised each included study for risk of bias using criteria outlined by The Journal of Bone & Joint Surgery, American Volume 6 for therapeutic studies and modified to encompass criteria associated with methodological quality 7 (see the Supplemental Material for individual study ratings; available in the online version of the article). Disagreements in ratings were resolved through discussion.
Overall Strength of Body of Literature
After rating each individual article, the strength of the overall body of evidence with respect to each outcome was determined based on precepts outlined by the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group 8,9 and recommendations made by the Agency for Healthcare Research and Quality (AHRQ). 10,11 Additional qualitative analysis was performed according to AHRQ-required (risk of bias, consistency, directness, precision) and additional domains (dose-response, strength of association, publication bias). 12 In general, risk of bias was determined when evaluating each individual article as described above.
The initial strength of the overall body of evidence was considered “High” for RCTs and “Low” for observational studies. The body of evidence could be downgraded 1 or 2 levels based on the following criteria: (1) risk of bias (study limitations), (2) inconsistency of results, (3) indirectness of evidence, (4) imprecision of the effect estimates (eg, wide confidence intervals), or (4) failure to provide an a priori statement of subgroup analyses. The body of evidence could be upgraded 1 or 2 levels based on the following criteria: (1) large magnitude of effect or (2) dose-response gradient or (3) if all plausible biases would decrease the magnitude of an apparent effect.
The final overall strength of the body of literature expresses (1) our confidence that the effect size lies close to the true effect and (2) the extent to which the effect is believed to be stable based on the adequacy of or deficiencies in the body of evidence. 9 An overall strength of “High” means that we are very confident that the true effect lies close to that of the estimated effect. A “Moderate” rating means that we are moderately confident in the effect estimate; the true effect is likely to be close to the estimated effect, but there is a possibility that it is substantially different. An overall strength of “Low” means that our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate. Finally, a rating of “Insufficient” means that we have very little confidence in the effect estimate; the true effect is likely to be substantially different than the estimated effect. In addition, this rating may be used if there is no evidence or it is not possible to estimate an effect.
Analysis
When data was available, we calculated risk ratios (RRs) and risk differences (RDs) with 95% confidence intervals (95% CIs) to provide an estimate of effect size. Fisher exact test was used to calculate P values due to the low number of events. P values <.05 were considered statistically significant. Calculations were performed using Stata 9.0. 13 Pooling of data was performed if studies were reasonably homogeneous with respect to patient population, study quality, interventions, and outcome measures.
Results
The search yielded 282 citations. Four additional primary studies were identified from the bibliographies of other published articles. Two hundred and sixty-nine citations were excluded based on their title and/or abstract, while 17 were selected for full-text investigation (Figure 1). A total of 8 RCTs 14 –21 met inclusion criteria for Key Questions 1, 2, and 3 and are summarized in this review. Additionally, we identified one prospective, nonrandomized comparative study 22 that satisfied the inclusion criteria for Key Question 4. Study characteristics, patient demographics, and detailed results are provided in the abstraction tables located in the Supplemental Material (available in the online version of the article).
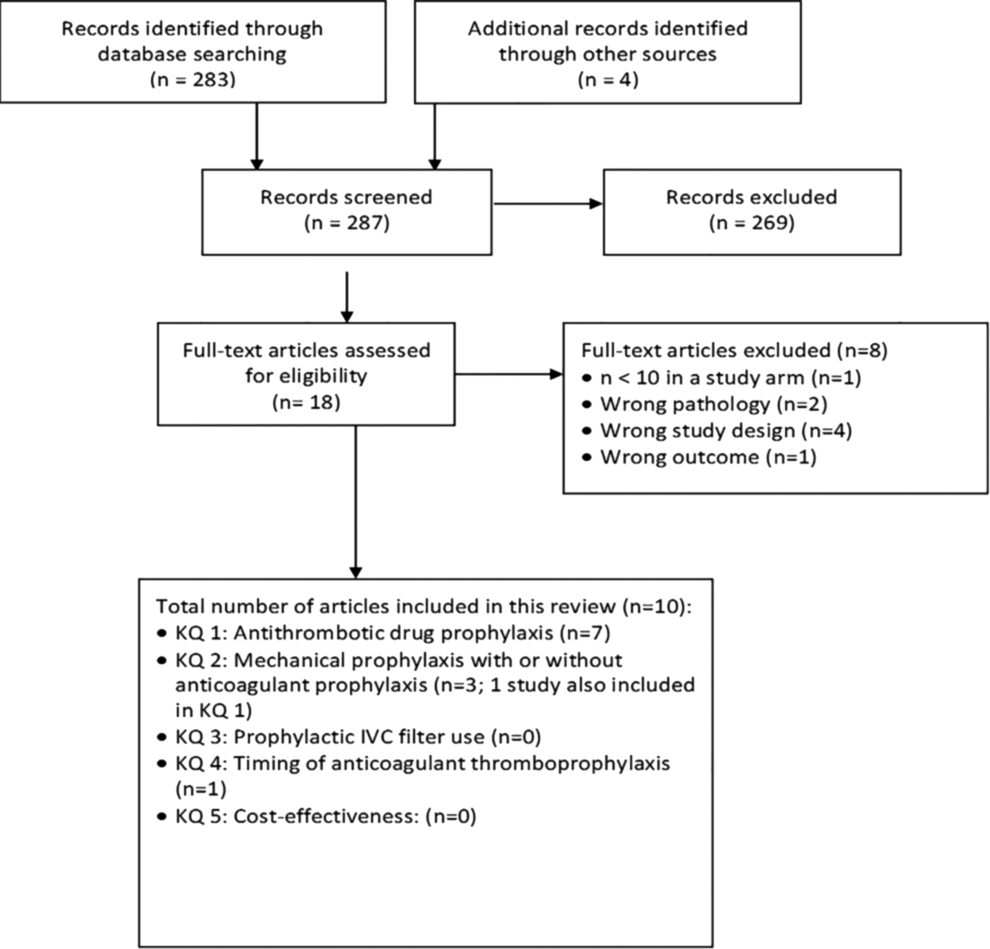
Study selection flow chart.
Our intent was to combine data into a meta-analysis where possible; however, all comparisons either did not have 2 or more studies, or the studies were too heterogeneous with regard to populations, interventions, and/or outcomes to enable pooling.
Key Question 1. What Is the Effectiveness and Safety of Anticoagulant Thromboprophylaxis Compared to No Prophylaxis, Placebo, or Another Anticoagulant Strategy for Preventing DVT and PE After Acute SCI?
Seven RCTs 14 –17,19,21,23 reported on the efficacy and/or safety of anticoagulant drug interventions. Two additional studies claimed randomization but were excluded for the following reasons: (1) one study 24 did not re-randomize patients following the acute phase of the trial but rather selected their subjects based on whether or not they successfully completed the acute treatment phase; and (2) a second study 25 included patients that were assigned alternately (ie, not randomly) to treatment groups. The 7 included studies were stratified as follows: (1) low-molecular-weight heparin (LMWH; enoxaparin) versus no prophylaxis 23 ; (2) LMWH (enoxaparin) versus LMWH (dalteparin) 15 ; (3) fixed-dose versus adjusted-dose unfractionated heparin (UFH) 16 ; (4) LMWH (tinzaparin and dalteparin) versus UFH 17,21 ; and (5) UFH versus no treatment or placebo. 14,19
LMWH Versus No Prophylaxis
A single RCT compared the efficacy of LMWH versus no anticoagulant prophylaxis. This trial 23 reported the risks of DVT and PE in groups that received either enoxaparin (40 mg subcutaneously one time per day for 8 weeks) or no prophylaxis (both groups had compression stockings). Patients treated with enoxaparin had a lower rate of DVT (5.4%) than those who received no LMWH prophylaxis (21.6%; RD = 16.2, 95% CI = 1.1 to 31.4; RR = 4.0, 95% CI = 0.91 to 17.6; P = .09). The authors reported a statistically significant difference (P = .04); however, we reanalyzed this data due to the low number of events using the more conservative Fisher exact test and found no significant difference. Risk of PE, bleeding, and mortality were not reported (Table 2).
Risks of DVT and PE in Patients With Traumatic Spinal Cord Injury Who Received Enoxaparin Versus No Prophylaxis.

Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; n, number of events; N, total number; PE, pulmonary embolism; RD, risk difference; RR, risk ratio.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
UFH Versus Placebo or No Treatment
Two RCTs assessed the risk of DVT in patients receiving UFH (5000 U subcutaneously every 12 hours 14 or every 8 hours 19 ) versus no treatment or placebo. 14,19 The rates of DVT did not significantly differ between the UFH and the placebo/no prophylaxis groups (1.8% and 3%, respectively, in one trial 14 and 50% and 47%, respectively, in the other trial 19 ; Table 3).
Risks of DVT in Patients With Traumatic Spinal Cord Injury Who Received UFH Versus Placebo/No Prophylaxis.
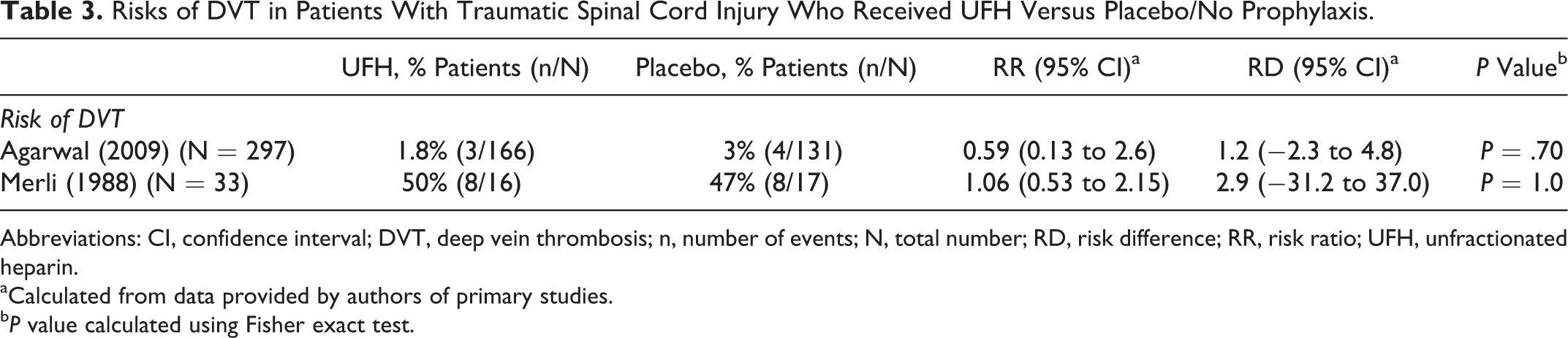
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; n, number of events; N, total number; RD, risk difference; RR, risk ratio; UFH, unfractionated heparin.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
LMWH Versus LMWH
A single RCT compared the efficacy and safety of 2 different LMWH drugs. This trial 15 reported on the risks of DVT, PE, bleeding, and mortality in groups that received either enoxaparin (30 mg subcutaneously every 12 hours) or dalteparin (5000 IU subcutaneously once daily). There was no statistically significant difference in the rate of DVT between the enoxaparin and dalteparin groups (6% and 4%, respectively; RD = 1.6, 95% CI = −7.3 to 10.5; RR = 1.35, 95% CI = 0.24 to 7.72; P = 1.0). Furthermore, no patients in either group suffered a PE. Both treatments were also equally safe: (1) only 1 patient in the enoxaparin group and 2 patients in the dalteparin group experienced a bleeding event (RD = 2.4, 95% CI = −9.6 to 4.7; RR = 0.45, 95% CI = 0.04 to 4.8; P = .6); and (2) no patients died in either group (Table 4).
Risks of DVT, PE, Bleeding, and Mortality in Patients With Traumatic Spinal Cord Injury Who Received Enoxaparin Versus Dalteparin.
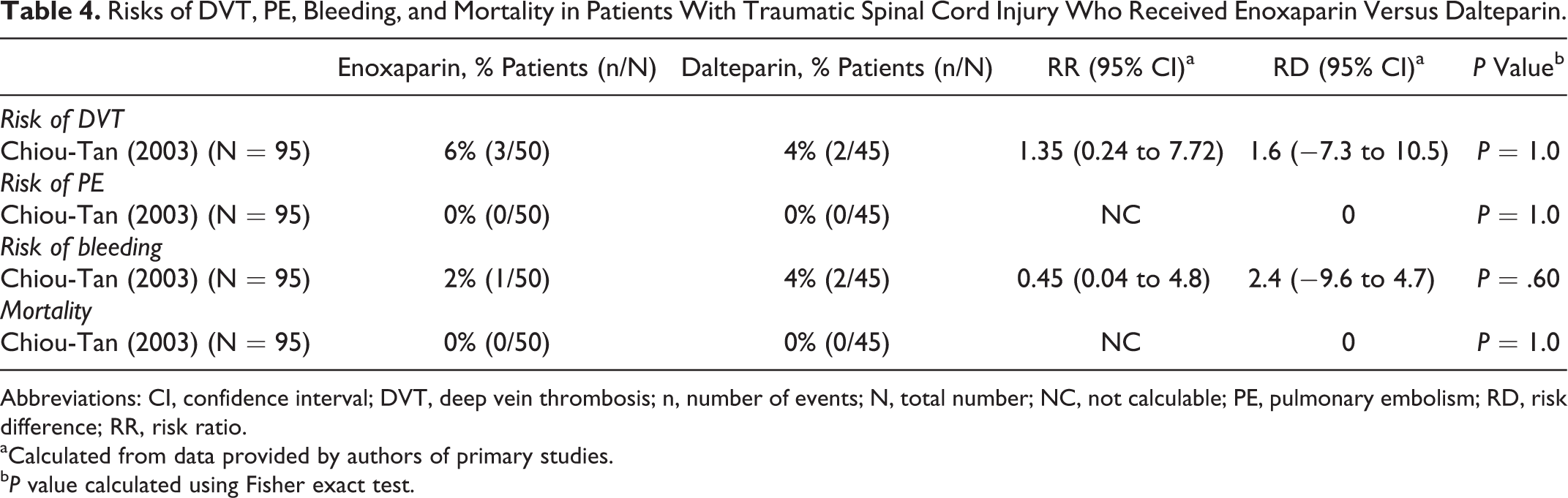
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; n, number of events; N, total number; NC, not calculable; PE, pulmonary embolism; RD, risk difference; RR, risk ratio.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
Fixed, Low-Dose UFH Versus Adjusted-Dose UFH
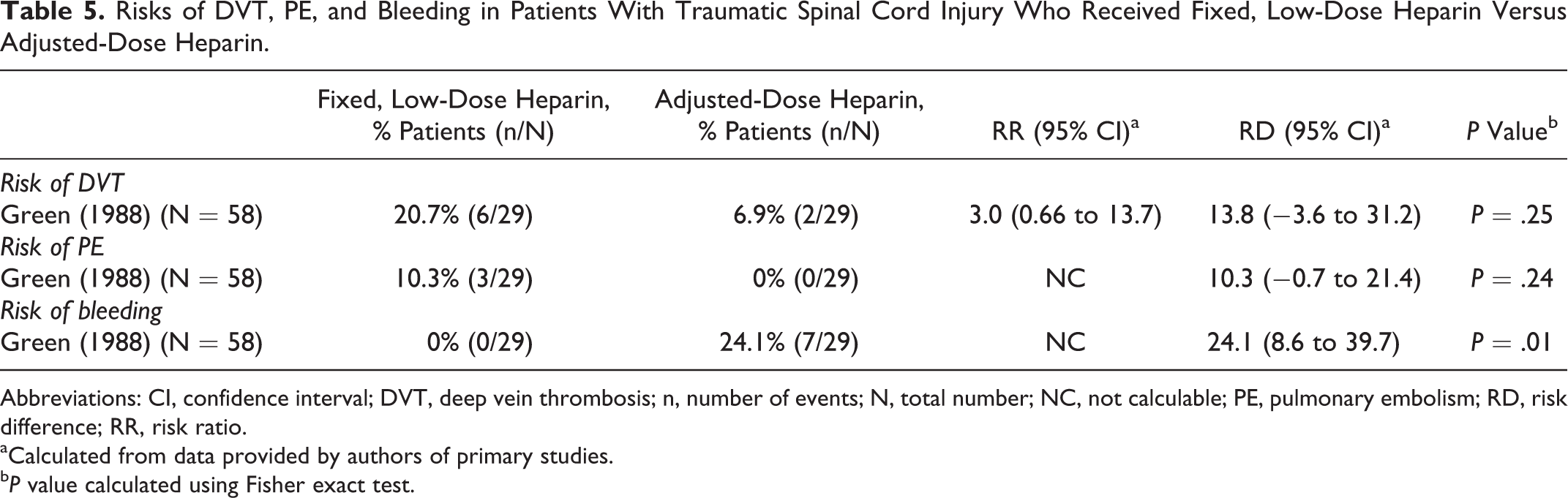
One RCT evaluated the efficacy and safety of fixed, low-dose versus adjusted-dose UFH. This trial 16 discussed the risks of DVT, PE, and bleeding in groups that received either a fixed, low-dose (initial dose of 5000 U and then 5000 U given subcutaneously every 12 hours) or adjusted-dose (initial dose of 5000 U and then adjusted as necessary to keep the activated partial thromboplastin time value in the 40-50 seconds range) of UFH. VTE (DVT and/or PE) was seen in 9/29 (31.0%) and 2/29 (6.9%), respectively (P = .04). The risk of DVT in the fixed, low-dose group was 3 times greater than the adjusted-dose group (RD = 13.8, 95% CI = −3.6 to 31.2; RR = 3.0, 95% CI = 0.66 to 13.7; P = .25; Table 5). Three patients (10.3%) in the fixed, low-dose group experienced a PE, whereas no patients in the adjusted group suffered this complication; this difference did not reach statistical significance (RD = 10.3, 95% CI = −0.7 to 21.4; P = .24). The rate of bleeding was significantly higher in patients treated with adjusted-dose heparin (24.1%) than those receiving low-dose (0%; RD = 24.1, 95% CI = 8.6 to 39.7; P = .01; Table 5).
Risks of DVT, PE, and Bleeding in Patients With Traumatic Spinal Cord Injury Who Received Fixed, Low-Dose Heparin Versus Adjusted-Dose Heparin.
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; n, number of events; N, total number; NC, not calculable; PE, pulmonary embolism; RD, risk difference; RR, risk ratio.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
LMWH Versus UFH
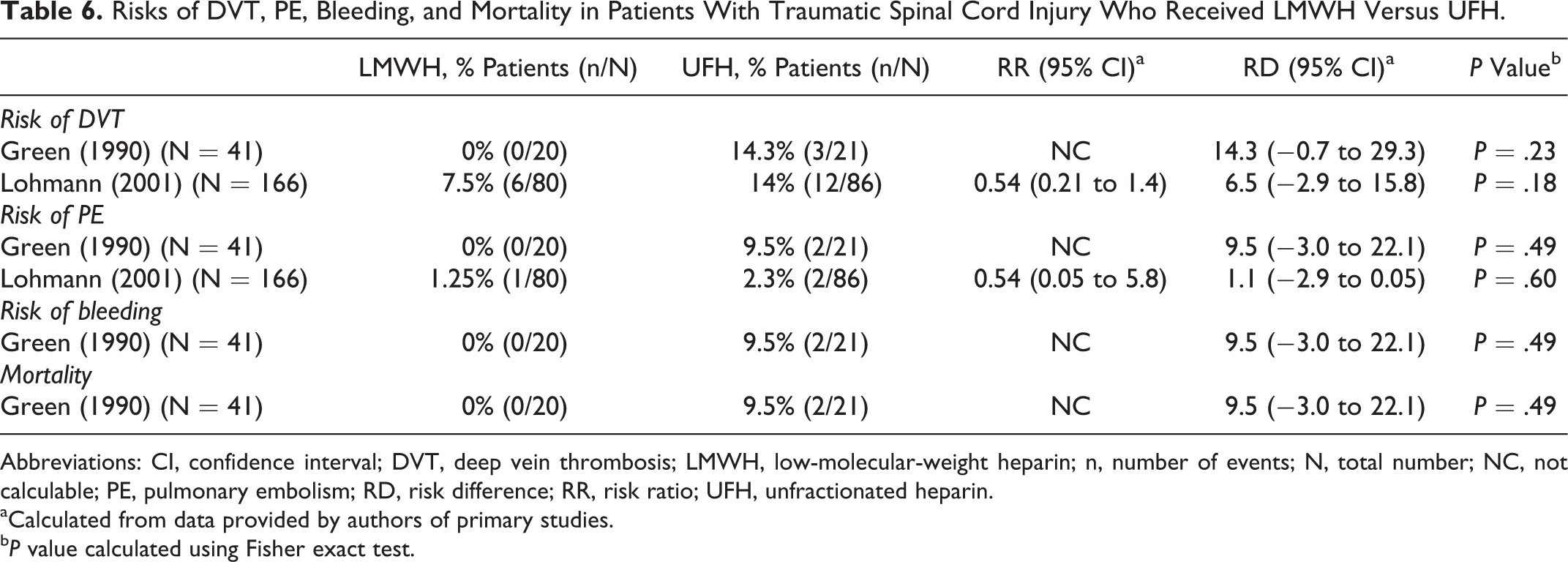
Two RCTs examined the relative efficacy and safety of LMWH versus UFH. One trial 17 reported on the risks of DVT, PE, bleeding, and mortality in patients that received either LMWH (tinzaparin 3500 anti-Xa units given subcutaneously once daily) or UFH (fixed doses of 5000 U given subcutaneously every 8 hours). No patients in the LMWH group experienced a DVT or PE, whereas in the UFH group, 3 (14%) patients suffered a DVT and 2 (9.5%) a PE; these differences were not statistically significant for either outcome due to the low number of events (Table 6). There was a higher rate of bleeding (9.5%) and mortality (9.5%) in the UFH group compared to the LMWH group (0% and 0%, respectively), although these relationships did not reach statistical significance.
Risks of DVT, PE, Bleeding, and Mortality in Patients With Traumatic Spinal Cord Injury Who Received LMWH Versus UFH.
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; n, number of events; N, total number; NC, not calculable; PE, pulmonary embolism; RD, risk difference; RR, risk ratio; UFH, unfractionated heparin.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
A second trial 21 also discussed the risks of DVT and PE events in patients who received either LMWH (dalteparin; 5000 anti-Xa units given subcutaneously once daily) or UFH (7500 U given subcutaneously twice daily). Similarly, the risks of DVT (7.5% and 14% for LMWH and UFH, respectively) and PE (1.25% and 2.3% for LMWH and UFH, respectively) were lower in the LMWH group than in the UFH group; however, these differences did not reach statistical significance (DVT: RD = 6.5, 95% CI = −2.9 to 15.8; RR = 0.54, 95% CI = 0.21 to 1.4; P = .18; PE: RD = 1.1, 95% CI = −2.9 to 0.05; RR = 0.54, 95% CI = 0.05 to 5.8; P = .60). In this analysis, we did not pool the data from these 2 studies due to differences between dalteparin and tinzaparin (Table 6).
Key Question 2. What Is the Comparative Effectiveness and Safety of Mechanical Strategies Alone or in Combination With Other Prophylactic Strategies for Preventing DVT and PE After Acute SCI?
Three RCTs 18 –20 reported on the efficacy and/or safety of mechanical strategies alone or in combination with antithrombotic drug interventions. The 3 included studies compared the following prophylactic treatments: (1) mechanical versus mechanical + antithrombotic drugs 18 and (2) anticoagulant versus anticoagulant + mechanical. 19,20
Mechanical Versus Mechanical + Antithrombotic Drugs
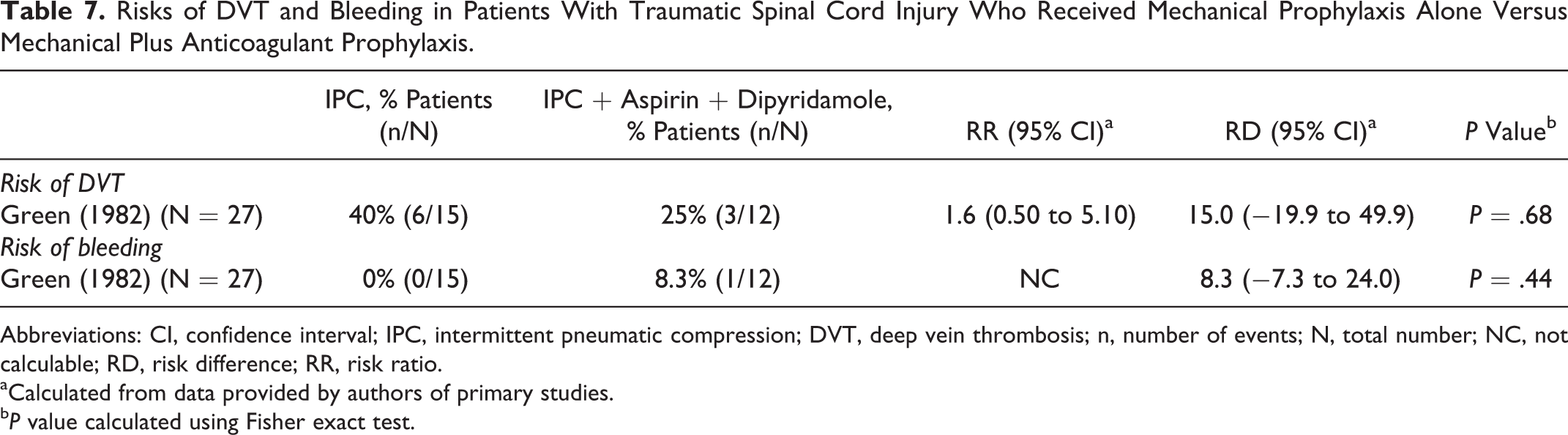
A single RCT compared the efficacy and safety of mechanical prophylaxis versus mechanical prophylaxis plus antithrombotic drugs. 18 This study reported on the risks of DVT and bleeding in 28 patients who received intermittent pneumatic compression (IPC) alone and those who were treated with IPC plus aspirin and dipyridamole (IPC plus aspirin 300 mg BID and dipyridamole 75 mg TID). A higher percentage of patients experienced a DVT in the IPC-only group (40%) than in the IPC plus aspirin and dipyridamole group (25%); however, this difference was not statistically significant (RD = 15.0, 95% CI = −19.9 to 49.9; RR = 1.6, 95% CI = 0.50 to 5.10; P = .68). There was also no difference in safety between treatment groups: no patients in the IPC group and only one patient in the IPC plus aspirin and dipyridamole group reported an adverse bleeding event (RD = 8.3, 95% CI = −7.3 to 24.0; P = .44; Table 7).
Risks of DVT and Bleeding in Patients With Traumatic Spinal Cord Injury Who Received Mechanical Prophylaxis Alone Versus Mechanical Plus Anticoagulant Prophylaxis.
Abbreviations: CI, confidence interval; IPC, intermittent pneumatic compression; DVT, deep vein thrombosis; n, number of events; N, total number; NC, not calculable; RD, risk difference; RR, risk ratio.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
Anticoagulant Versus Anticoagulant + Mechanical
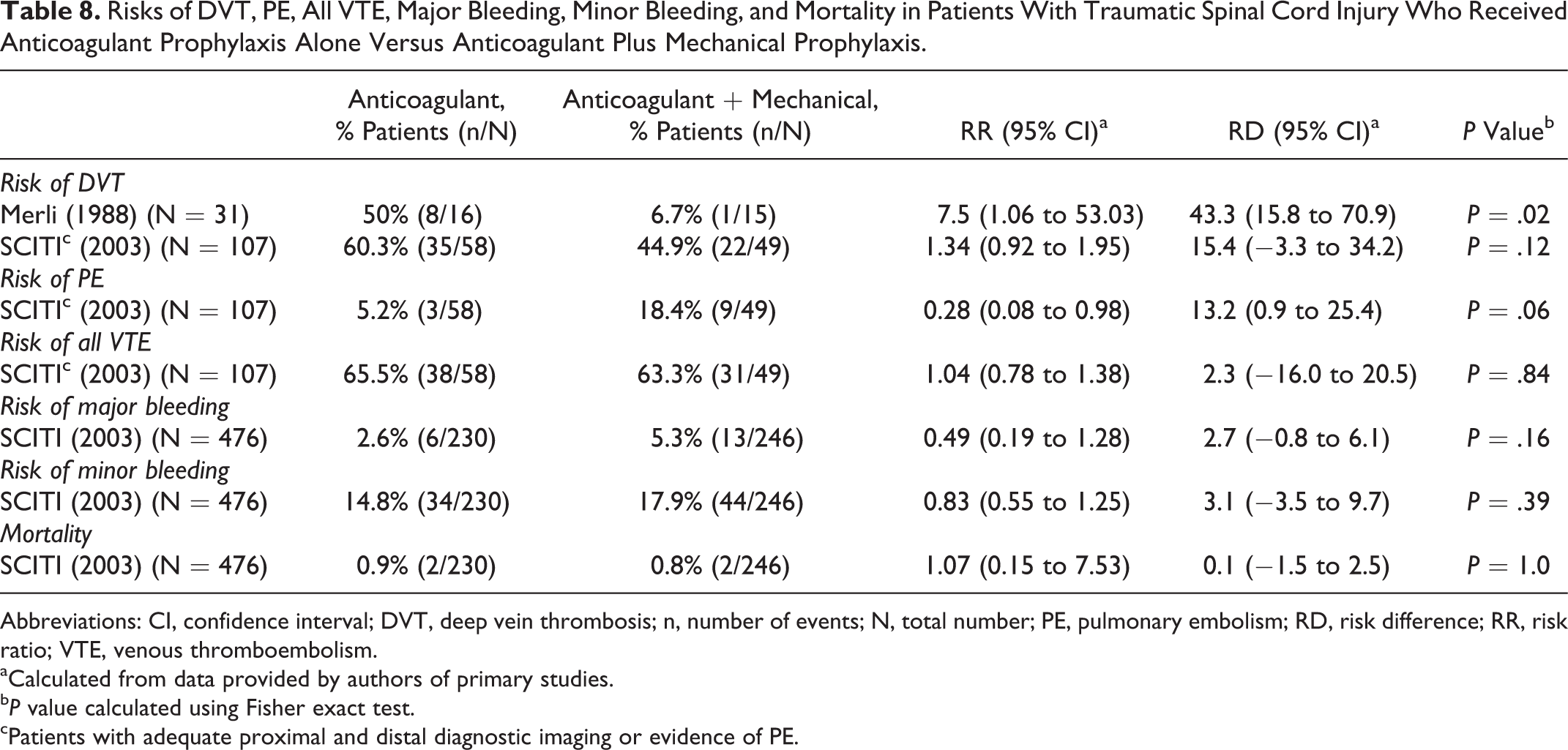
Two RCTs compared outcomes between anticoagulant thromboprophylaxis and anticoagulant plus mechanical prophylaxis. 19,20 The first trial 19 investigated the use of UFH alone (5000 U subcutaneously every 8 hours) versus UFH plus electric stimulation (UFH as described above, plus tibialis anterior and gastrocnemius-soleus stimulated bilaterally for 23 hours per day), and a second trial 20 compared the use of LMWH (enoxaparin; 30 mg subcutaneously every 12 hours) versus UFH (5000 U subcutaneously every 8 hours) plus IPC (used at least 22 hours each day). The first trial 19 only discussed the risk of DVT, whereas the other 20 reported on rates of DVT, PE, all VTE, major and minor bleeding, and mortality. Both studies reported higher risks of DVT in the group that received anticoagulant prophylaxis only (50% and 60.3%, respectively) than in the group that received combined anticoagulant and mechanical intervention (6.7% and 44.9%, respectively; Table 8). In the trial that compared UFH alone versus UFH plus electric stimulation, 19 the increased risk of DVT in the anticoagulant prophylaxis group (50%) was nearly 8 times that of the combined treatment group (6.7%; RD = 43.3, 95% CI = 15.8 to 70.9; RR = 7.5, 95% CI = 1.06 to 53.03; P = .02). In the second trial, 20 60.3% of patients treated with LMWH experienced a DVT, whereas only 44.9% of patients who received UFH plus IPC suffered this adverse event (RD = 15.4, 95% CI = −3.3 to 34.2; RR = 1.34, 95% CI = 0.92 to 1.95; P = .12; Table 8). The data was not pooled across studies due to differences in the anticoagulant and mechanical prophylaxis used in these trials.
Risks of DVT, PE, All VTE, Major Bleeding, Minor Bleeding, and Mortality in Patients With Traumatic Spinal Cord Injury Who Received Anticoagulant Prophylaxis Alone Versus Anticoagulant Plus Mechanical Prophylaxis.
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; n, number of events; N, total number; PE, pulmonary embolism; RD, risk difference; RR, risk ratio; VTE, venous thromboembolism.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
cPatients with adequate proximal and distal diagnostic imaging or evidence of PE.
In the Spinal Cord Injury Thromboprophylaxis Investigators (SCITI) trial, 20 patients in the LMWH-only group experienced fewer PE events compared to patients in the UFH plus IPC group (5.2% and 18.4%, respectively); this difference was nearly statistically significant (RD = 13.2, 95% CI = 0.9 to 25.4; RR = 0.28, 95% CI = 0.08 to 0.98; P = .06). The risk of all VTE, major and minor bleeding, and mortality were similar between groups (Table 8).
Key Question 3. What Is the Comparative Effectiveness and Safety of Prophylactic IVC Filter Insertion Alone or in Combination With Other Prophylactic Strategies for Preventing DVT and PE After Acute SCI?
We did not identify any RCTs that met our inclusion criteria for this key question.
Key Question 4. What Is the Optimal Timing to Initiate and/or Discontinue Anticoagulant, Mechanical, and/or Prophylactic IVC Filter Following Acute SCI?
One prospective, non-RCT 22 examined the timing of initiation of anticoagulant thromboprophylaxis in patients with acute SCI. This study reported on the risks of DVT and PE in patients that received prophylaxis initiated within (early group) or after (late group) 72 hours of injury. The prophylactic protocol consisted of LMWH (nadroparin; 0.4 mL once per day) plus early mobilization, graduated compression stockings (GCS), and IPC devices (3 hours per day given in 2 applications) for the lower limbs. The number of patients who suffered a DVT was significantly lower in the early group (n = 2) compared to the late group (n = 46; RD = 24.1, 95% CI = 17.1 to 31.2; RR = 12.9, 95% CI = 3.2 to 51.2; P < .001; Table 9). No patients in either group experienced a PE event. Safety outcomes were not reported in this study.
Risks of DVT and PE in Patients With Traumatic Spinal Cord Injury Who Received Early (≤72 Hours) Versus Late (>72 Hours) Prophylaxis.
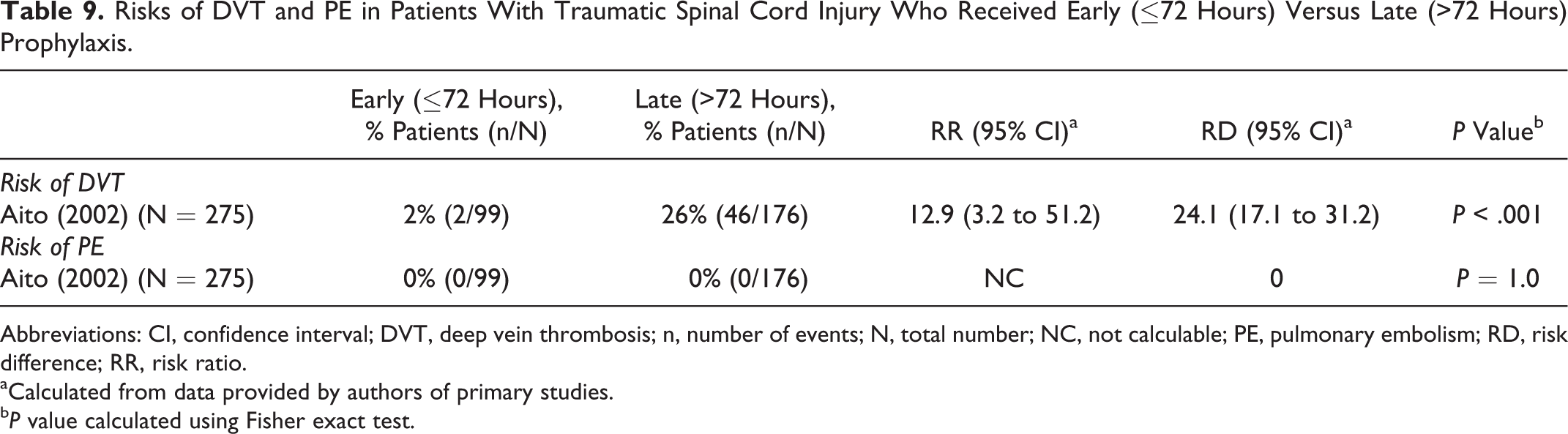
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; n, number of events; N, total number; NC, not calculable; PE, pulmonary embolism; RD, risk difference; RR, risk ratio.
aCalculated from data provided by authors of primary studies.
b P value calculated using Fisher exact test.
Key Question 5. What Is the Cost-Effectiveness of the Treatment Options Evaluated in Key Questions 1 to 4?
We did not identify any studies that met our inclusion criteria for this Key Question.
Strength of Evidence Summary
See the Supplemental Material for detailed tables (available in the online version of the article).
Key Question 1. What is the effectiveness and safety of anticoagulant thromboprophylaxis compared to no prophylaxis, placebo, or another anticoagulant strategy for preventing DVT and PE after acute SCI?
Overall, the strength of evidence was low for evaluating the comparative efficacy and safety of various anticoagulant prophylactic strategies (eg, enoxaparin, dalteparin, tinzaparin, UFH) in patients with acute SCI. The strength of evidence was moderate for comparing the efficacy and safety of fixed, low-dose versus adjusted-dose UFH.
LMWH versus no prophylaxis
There is low-quality evidence that the risk of DVT (but not PE) is higher in patients who received no prophylaxis compared to those who received LMWH (enoxaparin). The risk of DVT was 4 times greater in patients treated without prophylaxis; however, this did not quite reach statistical significance in our conservative analysis (Table 10).
Summary GRADE Table for Key Question 1: What Is the Effectiveness and Safety of Anticoagulant Thromboprophylaxis Compared to No Prophylaxis, Placebo, or Another Anticoagulant Strategy for Preventing DVT and PE After Acute Spinal Cord Injury?
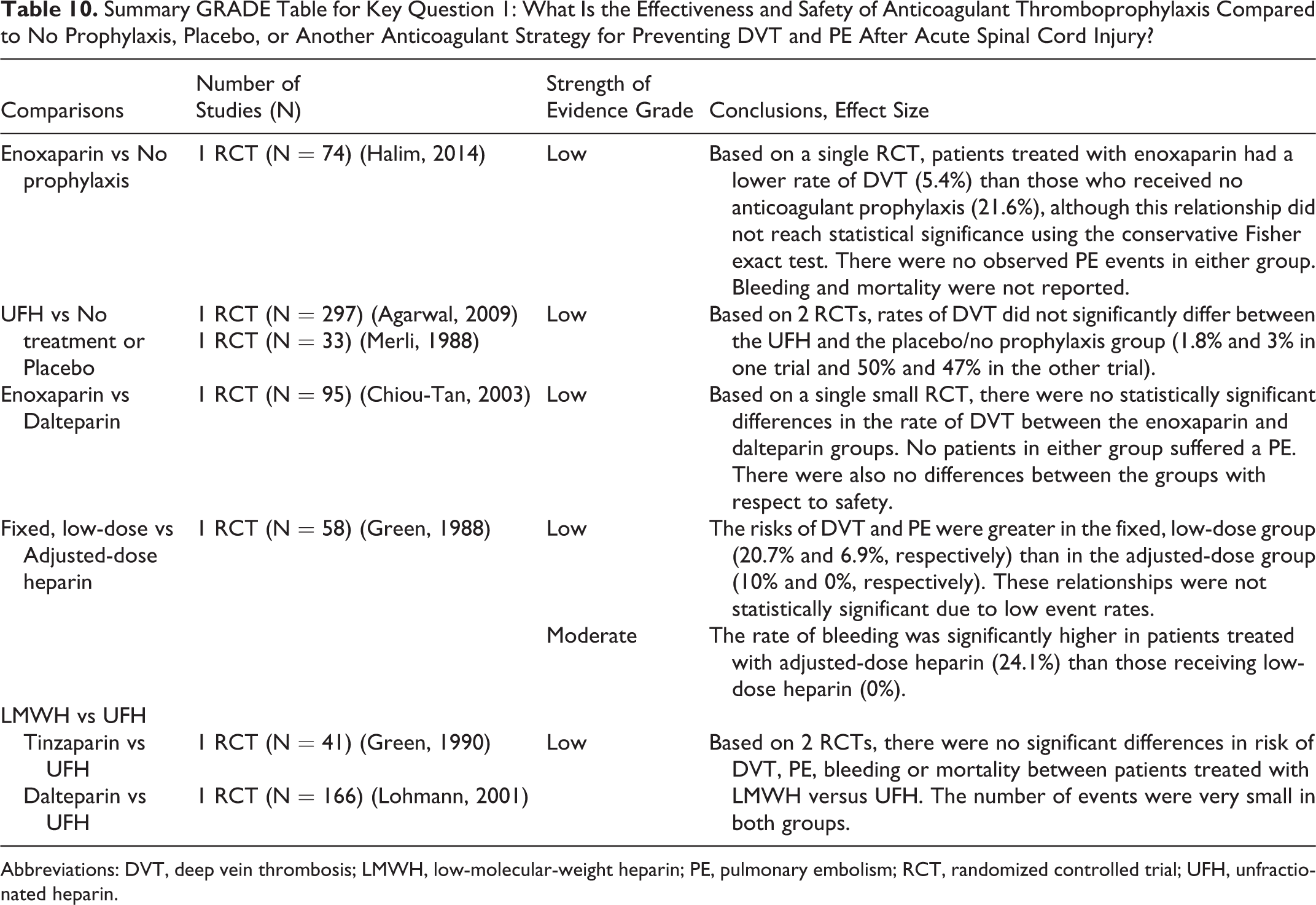
Abbreviations: DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; PE, pulmonary embolism; RCT, randomized controlled trial; UFH, unfractionated heparin.
UFH versus placebo or no treatment
There is low-quality evidence that there is no difference in the risk of DVT in patients treated with either UFH or placebo/no prophylaxis (Table 10).
LMWH versus LMWH
There is low-quality evidence that there is no difference in the risks of DVT, PE, bleeding, or mortality between patients administered with enoxaparin and those treated with dalteparin (Table 10).
LMWH versus UFH
There is low-quality evidence that there is no difference in the risks of DVT, PE, bleeding, or mortality in patients who received either LMWH (tinzaparin or dalteparin) or UFH (Table 10).
Fixed, low-dose UFH versus adjusted-dose UFH
There is low-quality evidence that the risk of DVT (but not PE) is higher in patients who received fixed, low-dose heparin compared to those treated with adjusted-dose heparin. There is moderate quality evidence that patients administered with fixed, low-dose heparin have a lower risk of bleeding than those who received an adjusted-dose (Table 10).
Key Question 2. What is the comparative effectiveness and safety of mechanical strategies alone or in combination with other prophylactic strategies for preventing DVT and PE after acute SCI?
Overall, the strength of evidence was low for evaluating the comparative efficacy and safety of mechanical prophylactic strategies (eg, IPC, electric calf stimulation) alone or in combination with other prophylactic strategies (eg, UFH, aspirin).
Mechanical versus mechanical + anticoagulant
There is low-quality evidence to suggest that there is no difference in the risk of DVT or bleeding between patients receiving IPC alone versus IPC plus aspirin and dipyridamole (Table 11).
Summary GRADE Table for Key Question 2: What Is the Comparative Effectiveness and Safety of Mechanical Strategies Alone or in Combination With Other Prophylactic Strategies for Preventing DVT and PE After Acute Spinal Cord Injury?
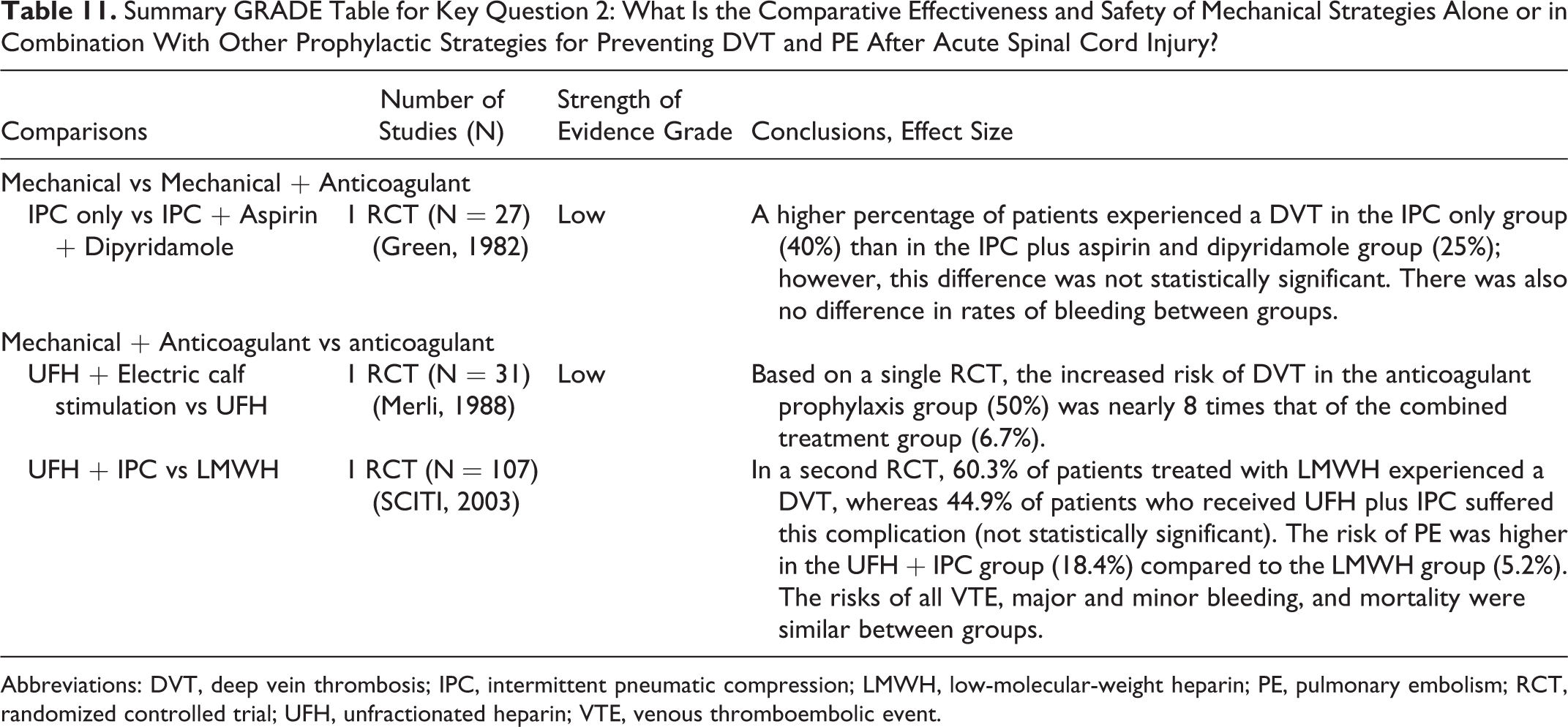
Abbreviations: DVT, deep vein thrombosis; IPC, intermittent pneumatic compression; LMWH, low-molecular-weight heparin; PE, pulmonary embolism; RCT, randomized controlled trial; UFH, unfractionated heparin; VTE, venous thromboembolic event.
Anticoagulant versus anticoagulant + mechanical
There is low-quality evidence that patients who received a combination of UFH and electric calf stimulation have a lower risk of DVT than patients treated with UFH alone. There is low-quality evidence that there is no difference in the risk of DVT in patients who received LMWH alone compared to those treated with UFH plus IPC. There is low-quality evidence that patients administered with LMWH alone have a lower risk of PE compared with patients who received UFH plus IPC. Based on low-quality evidence, there is also no difference in the risks of VTE, major and minor bleeding, and mortality between patients who received LMWH and those treated with UFH plus IPC (Table 11).
Key Question 3: What is the comparative effectiveness and safety of prophylactic IVC filter alone or in combination with other prophylactic strategies for preventing DVT and PE after acute SCI?
We did not identify any studies that met our inclusion criteria. There is therefore insufficient evidence to answer this key question.
Key Question 4. What is the optimal timing to initiate and/or discontinue anticoagulant, mechanical and/or prophylactic IVC filter following acute SCI?
There is low-quality evidence that the risk of DVT is significantly lower in patients receiving prophylaxis within 72 hours than those treated after 72 hours of injury. The prophylactic treatment protocol in this study was LMWH plus early mobilization, GCS, and IPC of the lower limbs. The level of evidence was upgraded from insufficient due to the strong magnitude of effect. There is no difference between these groups regarding the risk of PE; however, the evidence for this conclusion is insufficient (Table 12).
Summary GRADE Table for Key Question 4: What Is the Optimal Timing to Initiate and/or Discontinue Anticoagulant, Mechanical, and/or Prophylactic IVC Filter Following Acute Spinal Cord Injury?
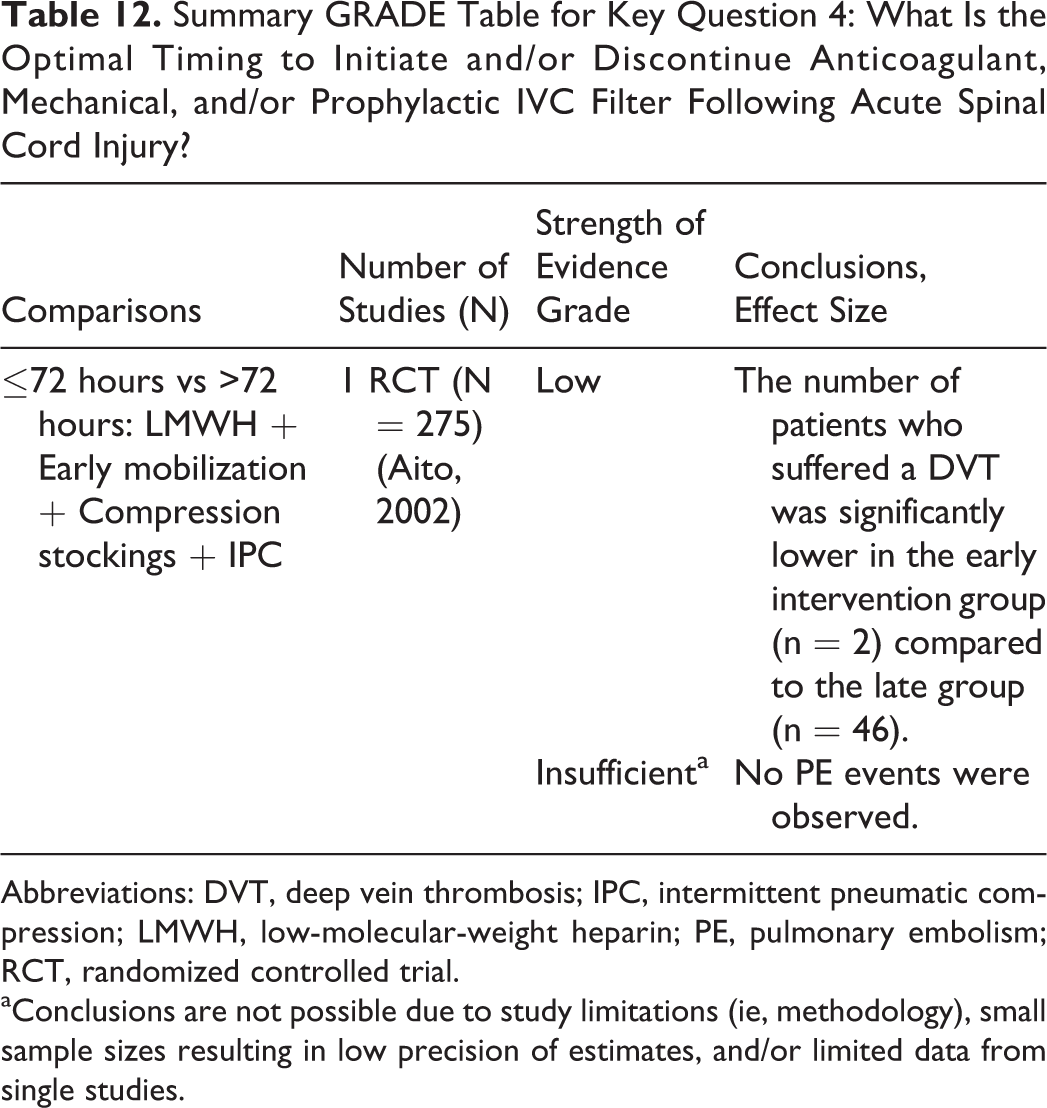
Abbreviations: DVT, deep vein thrombosis; IPC, intermittent pneumatic compression; LMWH, low-molecular-weight heparin; PE, pulmonary embolism; RCT, randomized controlled trial.
aConclusions are not possible due to study limitations (ie, methodology), small sample sizes resulting in low precision of estimates, and/or limited data from single studies.
Key Question 5. What is the cost-effectiveness of the treatment options evaluated in Key Questions 1 to 4?
We did not identify any studies that met our inclusion criteria. There is therefore insufficient evidence to answer this key question.
Discussion
SCI is associated with an increased risk of VTE due to neurologic dysfunction, immobilization, and hypercoagulability. 1 These patients experience extensive tissue damage and are commonly treated with invasive surgical procedures. As a result, there is a fear of hemorrhage or bleeding, particularly around neural tissues where a minor hematoma can have devastating consequences such as paralysis. Surgeons must implement appropriate anticoagulation strategies to reduce the risk of DVT and PE without increasing the risk of hemorrhagic complications. This review compared the efficacy and safety of various prophylactic treatment protocols, including antithrombotic drugs, mechanical strategies, and prophylactic IVC filter.
Antithrombotic Drug Strategies
Antithrombotic drugs for DVT and PE prophylaxis target the coagulation cascade. Halim et al reported that patients who did not receive any active thromboprophylaxis were at 4 times higher risk of DVT than those treated with LMWH (enoxaparin). 23 In their study, this relative risk was reported as statistically significant. In our systematic review, however, we reanalyzed their data using the conservative Fisher exact test due to the low number of events; the comparison between groups approached but did not reach statistical significance. Thus, although this conclusion agrees with clinical observations that anticoagulant thromboprophylaxis is superior to no treatment for preventing DVT, more definitive evidence is required.
In this review, several studies evaluated the relative efficacy and safety of various anticoagulant strategies, including enoxaparin versus dalteparin, 15 fixed- versus adjusted-dose UFH, 16 and UFH versus LMWH. 17,21 There was no statistically significant difference in the efficacy or safety between 2 types of LMWH, enoxaparin (30 mg subcutaneously every 12 hours) or dalteparin (5000 IU subcutaneously once daily); however, only 95 patients were evaluated.
In a study by Green et al, the risk of DVT in patients treated with fixed, low-dose UFH was nearly 3 times greater than in patients receiving an adjusted dose. 16 Although this conclusion might suggest that adjusted-dose UFH is a superior therapy, this relationship did not reach statistical significance and the rate of adverse bleeding events was significantly higher than in the fixed, low-dose group. Given that patients with SCI are often managed surgically, anticoagulant doses that cause excessive bleeding should be avoided.
There was a tendency for reduced risk of DVT and PE in patients receiving LMWH compared to those treated with UFH. 17 Low event rates in both groups, however, prevented definitive conclusions from being made. Furthermore, there were no statistically significant differences in rates of bleeding or mortality between prophylactic treatment groups. Other factors may also be considered when devising an appropriate treatment protocol, including cost and heparin-induced thrombocytopenia. LMWH is typically a more expensive therapy than UFH treatment. Patients treated with UFH, however, also have a much higher incidence of heparin-induced thrombocytopenia (2.6%) compared to users of LMWH (0.2%). 26
Combined Strategies
Green et al compared the risks of DVT and bleeding in patients who received mechanical prophylaxis alone or in combination with an antiplatelet strategy. 18 Based on their results, there was a higher rate of DVT in the IPC-only group (40%) than in the IPC plus aspirin and dipyridamole group (25%); however, this difference was not statistically significant. Mechanical prophylaxis, in combination with antithrombotic drug strategies, may work synergistically to reduce the risk of DVT. There was no significant difference in risk of bleeding between treatment groups.
Two other studies evaluated the relative efficacy and safety of anticoagulant thromboprophylaxis versus combined anticoagulant and mechanical strategies. 19,20 Merli et al reported a significantly reduced risk of DVT in patients who received UFH plus electric calf stimulation compared to those treated with only UFH. 19 This result indicates that DVT may be best prevented through combined strategies that reduce stasis as well as hypercoagulability. Furthermore, electric calf stimulation may decrease stasis better than IPC as it compresses the calf muscle at a greater frequency. 19
The SCITI trial compared the risk of DVT, PE, major and minor bleeding, and mortality between patients treated with LMWH and those who received a combination of UFH and IPC. 20 Rates of all VTE were similar between groups, 63% versus 66%, respectively. There was a trend toward a lower rate of DVT in the UFH plus IPC group (44.9%) compared with the LMWH group (60.3%), while the rate of PE was higher in the combined anticoagulant and mechanical prophylaxis group. The risk of major and minor bleeding and mortality did not differ between treatment groups.
Prophylactic IVC Filter Strategies
No studies evaluated the efficacy and safety of prophylactic IVC filters in patients with traumatic SCI. In a study by McClendon et al, the use of prophylactic IVC filters reduced the odds of developing a PE in patients undergoing major spinal reconstructive surgery compared to population controls. 27 Furthermore, Rodriguez et al reported a significantly decreased incidence of PE in patients at a high risk of this complication. 28 However, in a retrospective study of 54 SCI patients, the insertion of a prophylactic IVC filter increased the risk of DVT compared to a control group despite the routine use of anticoagulant thromboprophylaxis. 29 Further research is needed to confirm the efficacy and safety of prophylactic IVC filters in patients with SCI.
Timing of Prophylaxis
Spine surgeons must determine the ideal timing to initiate anticoagulant thromboprophylaxis in patients with either isolated SCI or with other additional traumatic injuries. These decisions must balance the need to prevent DVT and PE with the risk of increased bleeding. In a study by Aito et al, the risk of DVT was 13 times greater if prophylaxis (anticoagulant with mechanical) was employed >72 hours after injury compared to within 72 hours of injury. 22 There were no PE events reported in either group. Patients can generally be started on anticoagulant therapies within 72 hours to decrease the risk of DVT.
Cost-Effectiveness
No studies specifically analyzed the cost-effectiveness of DVT/PE prophylaxis in the traumatic SCI population. In patients with acute ischemic stroke, however, Pineo et al reported a lower average anticoagulant cost, including drug-administration costs, in patients treated with UFH ($259) compared to those who received LMWH ($360). 30 In contrast, total hospital costs, including both clinical events and drug costs, were lower in the LMWH group ($782) than in the UFH group ($922). In the traumatic SCI population, there is limited data to suggest superior outcomes of one treatment over another; as a result, direct drug and administration costs may have a larger impact on decision making. Future cost-effectiveness studies are required to confirm this hypothesis and must consider costs associated with length of stay, adverse events, and drug administration.
Strengths and Limitations
The strength of this systematic review is that it primarily summarizes results from RCTs. Furthermore, studies in all languages were considered for inclusion.
The limitations of this review include (1) poor methodologic quality of included studies, (2) small sample sizes and low event rates, and (3) significant clinical heterogeneity across studies prevented data pooling and meta-analysis (eg, differences in populations, antithrombotic drug and mechanical treatment protocols, diagnostic methods and outcomes).
Conclusions
Prophylactic treatments can be used to lower the risk of VTE events in patients with acute SCI, without significant increase in risk of bleeding and mortality. There were no significant differences in efficacy and safety of different types of LMWH or between LMWH and UFH. Patients should not be treated with adjusted-dose heparin due to significantly a higher risk of bleeding. Prophylaxis should generally be initiated as early as is safe after injury.
Footnotes
Acknowledgments
We would like to acknowledge Dr William Geerts for his thorough external review of this systematic review. We would also like thank Jeffrey Hermsmeyer, BS, for his assistance with literature searching, data abstraction, and critical appraisal of included studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AOSpine and the AANS/CNS Section on Neurotrauma and Critical Care. Dr Fehlings wishes to acknowledge support from the Gerald and Tootsie Halbert Chair in Neural Repair and Regeneration and the DeZwirek Family Foundation. Dr Tetreault acknowledges support from a Krembil Postdoctoral Fellowship Award. Analytic support for this work was provided by Spectrum Research, Inc, with funding from the AOSpine North America.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.