
Abstract
Study design
Literature review with clinical recommendation.
Objectives
To provide the readers with a concise curation of the relevant spine literature regarding the identification and management of osteoporosis in patients with adult spinal deformity (ASD) and set out recommendations for how the practicing clinician should interpret and make use of this evidence.
Methods
Key articles from the published literature surrounding osteoporosis in patients being treated for ASD were reviewed and clinical recommendations were formulated by consensus. The recommendations are dichotomously graded into strong and conditional after integrating an assessment of methodological quality and expert opinion. This opinion considers experience and practical issues such as risks, burdens, costs, patient values, and circumstances.
Results
6 articles were selected by practicing spinal deformity surgeons and each evaluated for the strength of methodology and scientific evidence.
Conclusions
The current evidence suggests that preoperative evaluation of osteoporosis before ASD surgery should be routine. Additionally, there is clinical benefit in using anabolic agents for at least 3 months to improve bone stock and prevent mechanical complications. While high quality, strong evidence is still yet to be reported, all healthcare providers managing patients with ASD should be aware of the importance of bone health for optimizing post-operative outcomes and minimising complications.
Keywords
Introduction
Osteoporosis is an increasingly global concern and its management has benefitted from significant advancements in its assessment and treatment over the last decade. With the broadening of indications for complex surgical reconstructions and the gradual aging of the patient cohort, the clinical implications of osteoporosis in adult spinal deformity (ASD) have increased in importance. Careful preoperative evaluation and treatment of a patient’s bone health must use reliable and accurate methodologies, as osteoporosis is a key predictor of peri-operative mechanical complications such as loss of fixation, proximal junctional failure, and pseudarthrosis. As the options for the preoperative management of osteoporosis expand, their application must be guided by accurate, precise and effective investigation to mitigate their risks and maximise their benefits.
A recent expert opinion paper proposed best practice guidelines for the assessment and treatment of poor bone health in elective spinal reconstruction. 1 Current guidelines recommend routine osteoporosis screening for all individuals aged 65 and older. For individuals aged 50 to 64, screening is advised if one or more risk factors are present. These risk factors include chronic glucocorticoid therapy, history of low-energy fractures, metabolic bone disorders, chronic kidney disease, prior failed spinal surgery, significant alcohol consumption, vitamin D deficiency, reduced mobility, history of cancer treatment, or diabetes. Whilst the evidence for its use in degenerative spine disorders is accumulating, evidence for its utility in patients with spinal deformity remains limited, though some previous knowledge could be extrapolated. In this review paper, the literature describing the identification, treatment and surgical implications of osteoporosis in patients with ASD is reviewed, with a focus on its evaluation, implications, and management. Lastly, clinical recommendations are formulated to guide practicing clinicians in interpreting and utilizing this evidence.
Article 1
Gupta A, Upadhyaya S, Patel A, Fogel HA, Cha T, Schwab J, Bono C, Hershman S. DEXA sensitivity analysis in patients with adult spinal deformity. Spine J. 2020 Feb;20(2):174-180. doi: 10.1016/j.spinee.2019.08.011. Epub 2019 Sep 1. PMID: 31479779. 2
Clinical Rationale
A Summary Table for the Clinical Recommendations
Study Summary
286 patients with a diagnosis of ASD and osteoporosis who underwent DEXA scanning were retrospectively reviewed. Patients were included in the study if the DEXA scan included the forearm and the hip (n = 66) or the forearm, hip and spine (n = 19) for a total of 85 patients. The mean age of the patients was 71.8 years, 90.6% were female, the average BMI was 25.7, and 46.4% of patients were either former or current smokers. In this cohort, the forearm had the lowest T score in 41.2% of case, the hip in 54.1% of cases and the hip and forearm were equal in 4.7% of cases. 17% of cases with osteoporosis were diagnosed with the forearm DEXA that would have otherwise been missed on scanning of the hip alone. As a result, an addition of a forearm DEXA is recommended to more accurately diagnose osteoporosis in ASD patients to better optimize the patient prior to surgery or to guide surgical strategy.
Methodological Review
The study makes use of a retrospective analysis of patients recruited from across a single hospital system between 2016 and 2018. Patients were required to have undergone a DEXA of either forearm or hip (or both) within 6 months of each other and be diagnosed with both scoliosis and osteoporosis at some point in their life. Basic demographics were collected. The diagnosis was based on ICD-10 codes and did not address the severity of the osteoporosis or the deformity. Only 30% of the potential cases could be enrolled as the majority of patients did not have DEXA scans of the forearm. Further, over 90% of the patients were female, and perhaps the results may not be accurately extrapolated to males. Those with bilateral hip osteoarthritis were excluded as this condition has been established to artificially improve the T score. The T score from the hip was compared to that of the forearm, and the lower of the 2 considered as the score informing the diagnosis, a variation from usual practice.
This is a simple yet informative study. The consequences of failing to diagnose osteoporosis can have major implications in patients undergoing multi-level spinal deformity corrective surgery.
While the quality of the evidence is low, based on the use of retrospective observational design, potential bias and the generalizability of the results, this study provides an important message to consider other sites like the forearm because of the potential overestimation of bone quality from the hip and spine.
Quality of Evidence: Low
Recommendations for Integrating into Your Clinical Practice
This study describes a simple modification to the normal assessment of bone health for ASD patients. Given that spinal DEXA is not as reliable in ASD patients as in normal population, and that hip DEXA is also not optimal in this cohort as hip arthritis in common, single location DEXA can show misleading results. Including the forearm in the investigation adds little cost, time or risk, and has the potential to improve the accuracy of diagnosing osteoporosis. The quality of the study is low and merits a conditional recommendation to include the forearm in DEXA scanning.
Article 2
St Jeor JD, Jackson TJ, Xiong AE, Freedman BA, Sebastian AS, Currier BL, Fogelson JL, Bydon M, Nassr A, Elder BD. Average Lumbar Hounsfield Units Predicts Osteoporosis-Related Complications Following Lumbar Spine Fusion. Global Spine J. 2022 Jun;12(5):851-857. doi: 10.1177/2192568220975365. Epub 2020 Nov 23. PMID: 33222537; PMCID: PMC9344520. 3
Clinical Rationale
Osteoporosis remains a difficult condition to manage in the perioperative setting, influencing both surgical technique and the postoperative complications after spinal fusion surgery. Osteoporosis related complications (ORCs), including proximal junctional kyphosis, pseudarthrosis, adjacent segment disease, fracture and instrumentation failure bring with them not only additional morbidity, but reoperation and cost. This study looked to identify those at risk of these complications through evaluating the ability of Hounsfield units, measured on preoperative CT scan within the 6 months prior to surgery, compared to DEXA scan within 1 year prior to surgery to predict the occurrence of an ORC.
Study Summary
One challenge in managing adult deformity osteoporosis patients is the absence of a ‘gold standard’ investigation to quantify the risk of ORC. Although DEXA is usually referenced, the degenerative lumbar spine is not amenable to this modality due to sclerosis and malalignment, however Hounsfield units (HU), measured on local CT is unaffected by these obstacles.
This study used data from 140 patients treated for 7 years up to 2014 at an academic medical center who had undergone a DEXA of either the hips or spine within 1 year, and a CT of the lumbar spine within 6 months prior to index spinal fusion. The HUs at the superior, middle and inferior portions of each of the 5 lumbar vertebral bodies were measured and an average taken. The lowest T-score from the DEXA was taken as the definitive value. ORCs comprised: revision surgery, compression fracture, proximal junctional kyphosis, pseudarthrosis, accelerated adjacent segment disease or instrumentation failure.
Using WHO criteria, 10% of all patients were defined as osteoporotic and 58.6% osteopenic. There were no differences in the rates of multilevel fusion, and ORCs were seen in 45/140 patients: in 15.9% of those with normal bone, 40.2% of osteopenic patients and 35.7% of those with osteoporosis. Pseudarthrosis (8.6%) and reoperation (7.1%) were the most common ORCs. No differences in demographics between those with ORCs and those without were found, except to say that those with ORCs were more likely to have been treated with teriparatide in the 6 months prior to surgery. Those with ORCs had a significantly lower T-score (−1.62 vs −1.10) and lower HUs (112.1 vs 148.1).
Multivariable binary regression shows that only treatment with teriparatide in the 6 months prior to surgery and lower HUs are independent predictors of ORCs. With every 25-point reduction in HUs, the risk of ORC climbed 1.7 fold. As a consequence, CT of the lumbar spine was recommended prior to lumbar fusion surgery to enable the management and counselling of those at risk of these difficult complications.
Methodological Review
This retrospective study is simple and informative. Although the sample is taken from just one center with 2 surgeons, the timeframe encompasses 7 years and the analysis of relevant cofactors is thorough. This is a straightforward, pragmatic study with immediately applicable clinical recommendations that can be brought to bear by any spine surgeon. The relatively small numbers of both patients and treating surgeons is a limitation of the work, however as the risks to patients of changing the analysis of the preoperative CT scan is essentially nil, a great deal of value can be placed upon the work.
The quality of evidence is low due to the retrospective methodology at a single center, a risk of residual confounding and the modest sample size available for subgroup analysis.
Quality of Evidence: Low
Recommendations for Integrating into Your Clinical Practice
This study shows the clinical value of a straightforward analysis of bone density that can be carried out on a routine preoperative CT scan. Bone can be assessed at any level of interest to identify poor bone density and potential for related complications after spinal fusion, allowing for appropriate preoperative osteoporosis management to be instituted. Despite DEXA being considered the gold standard for diagnosing osteoporosis, and being necessary in some cases to institute treatment, this result suggests that for spine surgery, the assessment of HUs on the CT contributes value. Even accounting for the low quality of the evidence, considering the low risk and substantial rewards offered by bone density analysis of routine preoperative CT, we recommend the inclusion of HU analysis into the preoperative assessment of patients.
Article 3
Mugge L, DeBacker Dang D, Caras A, Dang JV, Diekemper N, Green BA, Gjolaj JP, Fanous AA. Osteoporosis as a Risk Factor for Intraoperative Complications and Long-term Instrumentation Failure in Patients With Scoliotic Spinal Deformity. Spine (Phila Pa 1976). 2022 Oct 15;47(20):1435-1442. doi: 10.1097/BRS.0000000000004418. Epub 2022 Jun 29. PMID: 36174132. 4
Clinical Rationale
There is little literature describing the role of osteoporosis as it relates to both perioperative complications and outcomes after scoliotic spinal deformity surgery. In answer to this, Mugge et al. designed and completed a single-center, retrospective review to investigate these phenomena.
Study Summary
Between 2006 and 2017, a prospective single-institution clinical database was maintained, and a retrospective review for inclusion and analysis was performed. All patients underwent surgery at the same institution, performed by one of 3 spinal surgeons. Inclusion criteria included any thoracolumbar fusion for thoracolumbar scoliosis, including progression of adolescent idiopathic scoliosis or ASD. A diagnosis of osteoporosis was established based on WHO criteria, including a T-score ≤ −2.5 on a preoperative DEXA scan. Patients with a preoperative diagnosis of osteoporosis were separated into a different cohort from those without osteoporosis. Medical comorbidities, surgical information, postoperative outcomes, complications, and revision surgery were analyzed in 2 groups.
Of 532 patients, 144 (27%) had a diagnosis of osteoporosis. Osteoporosis was significantly associated with increased blood volume loss (P = 0.003). Postoperatively, osteoporosis was associated with increased rates of instrumentation failure (19% vs 10%; P = 0.008). A total of 111 patients required revision surgery. Rates of reoperation were greater in the osteoporosis cohort (33% vs 16%, P < 0.001). With confounders controlled, patients with osteoporosis were significantly more likely to have a higher mean number of spinal segments fused (P < 0.002) and a higher mean blood volume loss (P = 0.003), instrumentation failure (P = 0.022), and revision surgery (P < 0.001). In summary, the authors concluded that osteoporosis is associated with increased rate of instrumentation failure and revision procedure following ASD surgery.
Methodological Review
This study was a single-center retrospective review consisting of 532 cases from a prospectively maintained database for patients undergoing scoliosis corrective surgery. Collected data included various demographic, clinical, and operative variables. The procedures were clearly laid out in the methods with well-described and reported primary and secondary outcomes. The sample size is relatively large for a single-center study compared to previous studies. Statistical analyses were appropriate for the data. Patients with a preoperative diagnosis of osteoporosis were separated into a different cohort from those without an osteoporosis diagnosis. Overall, this was a well-conducted study that analyzed the effect of osteoporosis on various complications after scoliosis corrective surgery.
Quality of Evidence: Moderate
Recommendations for Integrating into Your Clinical Practice
This study identified a significant association between osteoporosis and increased intraoperative blood volume loss and the development of postoperative venous thromboembolism as well as higher rates of revision surgery and instrumentation failure. The treating team should factor in plans for early transfusion and consider all options for post-operative thromboprophylaxis. This report details a clear comparative analysis between osteoporosis and non-osteoporosis cohorts with a relatively high level of evidence. We suggest taking blood management interventions into account when treating osteoporotic patients, although clear guidelines on best practices regarding the topic are lacking.
Article 4
Mohanty S, Sardar ZM, Hassan FM, Lombardi JM, Lehman RA, Lenke LG. Impact of Teriparatide on Complications and Patient-Reported Outcomes of Patients Undergoing Long Spinal Fusion According to Bone Density. J Bone Joint Surg Am. 2024 Feb 7;106(3):206-217. doi: 10.2106/JBJS.23.00272. Epub 2023 Nov 16. PMID: 37973052. 5
Clinical Rationale
Low bone mineral density (BMD) is associated with the risk of pseudarthrosis in patients undergoing ASD surgery. However, the effect of treatment of osteoporosis with anabolic agents such as teriparatide prior to ASD surgery has not been comprehensively investigated. Mohanty et al have contributed by studying the effect of perioperative teriparatide use on revision surgery and pseudarthrosis in patients undergoing ASD surgery.
Study Summary
This was a retrospective review of 542 patients who underwent ASD surgery involving >7 instrumented levels at a single center. Bone health was determined through a DEXA scan. 52.6% had normal BMD, 32.9% showed osteopenia (OPE), and 14.4% were diagnosed with osteoporosis that was treated with Teriparatide (OP-T) for at least 6 months preoperatively and 1 year postoperatively. Included patients were followed for 2 years. The outcomes measured were 2-year reoperation rate, implant failure, proximal junctional kyphosis (PJK), and changes in patient-reported outcomes (PROs).
Two-year reoperation rates (11.5% vs 21.9%, OR: 0.45) and pseudarthrosis rates (6.4% vs 20.8%, OR: 0.25) were significantly lower in the OP-T group vs the OPE group. Matched analysis of 78 patients in OP-T group and 156 in the OPE group also showed lower reoperation (11.5% vs 23.1%, OR: 0.45) and pseudarthrosis rates (6.4% vs 21.8%, OR: 0.25) in the OP-T group compared to OPE. The rate of PJK was not different between groups. Matched analysis of 78 patients in OP-T group and 156 in the normal BMD group showed no difference in terms of 2-year reoperation, pseudarthrosis, or PJK rates.
Methodological Review
This is a retrospective case series comparing outcomes in patients with normal BMD, osteopenia (OPE), or osteoporosis treated with Teriparatide (OP-T). The team analyzed the unmatched cohort and went on to perform propensity score matching (PSM) in a 1:2 ratio (OP-T to OPE or normal BMD). This is a single surgeon and single center patient cohort. This may decrease the effects of variables such as different surgical approaches or surgical techniques. However, the generalizability of the findings to global populations remains unvalidated. Additionally, this predisposes the results to selection and treatment bias. Moreover, the assessment of bone health in this study is based purely on DEXA results. Such an assessment underestimates clinical osteoporosis and may overestimate the effect of osteopenia on outcomes. Importantly, the study does not discuss any adverse effects associated with the use of teriparatide in this patient population and does not address the high cost of treatment with teriparatide in relation to perceived benefits. Finally, the study does not have a control group with osteoporosis that was not treated with teriparatide to determine the true effects of Teriparatide in patients with osteoporosis undergoing ASD surgery.
Quality of Evidence: Low
Recommendation for Integrating into Your Clinical Practice
The authors addressed an important question of the effect of treating osteoporotic patients with teriparatide prior to ASD surgery. There are certain limitations of the study due to its single centered, retrospective nature. However, the benefits of this treatment probably outweigh the undesirable effects, therefore we suggest teriparatide treatment be incorporated into clinical practice, given absence of contraindications, availability and affordable cost.
Article 5
Sawakami K, Watanabe K, Hasegawa K, Yamamoto N, Shimakura T, Ohashi M, Shoji H, Mizouchi T, Tanaka Y, Segawa H, Ishikawa S, Hirano T, Kawashima H, Endo N, Takahashi HE. Neoadjuvant teriparatide therapy targeting the osteoporotic spine: influence of administration period from the perspective of bone histomorphometry. J Neurosurg Spine. 2021 Oct 15;36(3):429-439. doi: 10.3171/2021.5.SPINE202003. PMID: 34653987. 6
Clinical Rationale
Teriparatide (TPTD) is an osteogenic parathyroid hormone analog that has been shown to reduce complications related to osteoporosis in spine surgery. The optimal duration of preoperative TPTD treatment is unknown. To evaluate qualitative and quantitative TPTD effects on in vivo bone microarchitecture, Sawakami et al obtained iliac crest biopsy from patients with osteoporosis undergoing spine surgery, comparing bone histomorphometry, radiographic complications, and patient-reported outcomes in various TPTD pre-treatment lengths compared to a non-treatment control (NTC) group.
Study Summary
57 patients with hip T-score DEXA BMD<−1.5 scheduled to undergo spinal fusion surgery for deformity or lumbar degenerative disease were enrolled over 3 years in this multi-center non-randomized controlled trial, with patient-preference selecting the treatment group: TPTD treatment (42 patients) vs NTC (15 patients). There were no significant differences in baseline demographics between the groups, except 6 TPTD had received treatment with bisphosphonate prior to enrollment while no NTC had medication treatment before enrollment.
TPTD patients had daily injections of 20 µg TPTD from the time of enrollment through 24 months of total treatment. Preoperative administration time varied between 1 month (n = 9 patients), 2 months (n = 8), 3 months (n = 9), 4 months (n = 7), and 6 months (n = 9). Both TPTD and NTC had baseline pre-treatment blood testing for procollagen type I N-terminal propeptide (P1NP) to measure osteoblast bone formation activity and tartrate-resistant acid phosphatase 5b (TRACP5b) for osteoclast bone resorption activity, with no difference between the preoperative baselines. P1NP and TRACP5b were repeated immediately prior to surgery. All patients had in vivo double-labeling for tetracycline and underwent an iliac crest bone biopsy during spine surgery while autogenous cancellous bone graft was harvested. Blinded qualitative and quantitative histomorphometric analyses were performed on the bone biopsy samples. Outcomes were assessed at 1 year and 2 years postoperatively with Oswestry Disability Index (ODI) scores and CT scans to evaluate for instrumentation loosening, vertebral fracture, or rod fracture.
P1NP was significantly increased in TPTD vs NTC at the time of biopsy, indicating increased bone formation. The osteogenic response to TPTD peaked at 3-4 months after initial administration, leading the authors to conclude that preoperative duration of TPTD should be 3 months or more. Cancellous bone resorption was significantly higher in TPTD. There was no difference in the cancellous bone structure between TPTD and NTC. The overall radiographic complication rate at 2 years was significantly reduced in TPTD (35.7%) compared to NTC (80%; P = 0.0032). However, TPTD patients who had previously undergone bisphosphonate treatment had the same rate of screw loosening as NTC patients, suggesting that pre-treatment with bisphosphonate lessens the anabolic effect of TPTD; therefore, optimal preoperative treatment duration in such patients requires further study. All patients had statistically significant improvement in their ODI at 2 years postop.
Methodological Review
This study was a non-randomized, open label controlled multicenter trial where patients self-selected to receive either TPTD for varying duration prior to spine surgery vs no medication treatment. The abstract clearly states purpose and results. Effect size and statistical analysis was appropriately calculated. The inclusion of qualitative bone histomorphometric data as well as radiographic complication rates and HRQOL results increases the strength of the findings despite lack of randomization, which is the study’s main weakness. Data visualization would be improved by addition of graphs to view treatment effect rather than solely tabular data. The authors’ assertion that the TPTD group with >3 months treatment tended to have better ODI outcomes than other groups was not supported statistically. Otherwise, the discussion clearly summarized the pertinent findings. It remains unclear as to whether bone fusion is affected in addition to burn turnover.
Overall, this was a well-designed study with clear purpose and clear results whose main weakness is lack of randomization and low numbers for multiple groups. The level of evidence is moderate, due to the risk of bias, moderate sample size and imbalance between study groups.
Quality of Evidence: Moderate
Recommendations for Integrating into Your Clinical Practice
The authors conducted a well-designed, non-randomized open label multicenter trial to fill a significant knowledge gap in spine surgery about the optimal pre-treatment duration with TPTD in osteoporotic patients prior to spine surgery. Given the overall study design and rigor, we suggest TPTD treatment to be incorporated into clinical practice, dependent on the local costs and availability.
Article 6
Alpantaki K, Dohm M, Korovessis P, Hadjipavlou AG. Surgical options for osteoporotic vertebral compression fractures complicated with spinal deformity and neurologic deficit. Injury. 2018 Feb;49(2):261-271. doi: 10.1016/j.injury.2017.11.008. Epub 2017 Nov 12. PMID: 29150315. 7
Clinical Rationale
Osteoporosis not only negatively affects the surgical outcomes of ASD, but it can also be the source of deformity by itself, as in kyphosis associated with osteoporotic vertebral fracture. Surgical management of deformity complicated by osteoporosis is notoriously challenging because of compromised anchor purchase and the risk of adjacent segment pathology. In the report from Alpantaki et al., the authors presented the outcomes of various surgical techniques for either acute flexible or progressive pseudarthrotic kyphosis manifested with severe pain or neurological deficit.
Study Summary
From 2010 to 2014, this study prospectively registered cases from 2 facilities involving spinal deformities (kyphotic deformity due to pseudarthrosis) and neurological symptoms caused by osteoporotic vertebral fractures. Of the 51 registered patients, 31 were followed up for at least 2 years. Among these, 28 patients underwent positioning-based reduction, augmentation through balloon kyphoplasty or similar methods, and short segment posterior spinal fusion surgery. The remaining 3 patients received multi-level fixation due to significant instability.
In the short segment fusion results, 4 out of 28 patients (14.3%) experienced complications associated with cement extravasation. Screw pullout secondary to adjacent segment disorders was observed in 4 patients (14.3%) due to screw fixation endpoints being located in the kyphotic region. However, given the good outcomes, this treatment method is recommended for acute and chronic pseudarthrosis-related kyphotic deformities with mobility. For immobile deformation cases, reconstruction surgery combining an anterior approach is recommended based on literature review. In conclusion, this study reports favorable outcomes even with short segment fusion; however, the discussion suggests that the fixation should include posterior screws spanning 2 or 3 segments above and below. Modifications to Hu’s suggestion 8 include: A: Avoid using the kyphotic segment as a fixation endpoint to prevent adjacent segment disorders. B: Place screws in multiple segments to disperse stress. C: Avoid using hooks as a single fixation method. D: Combine anterior and posterior approaches to disperse excessive implant fixation force. E: Avoid excessive correction of deformity. F: For anterior fixation, screws should penetrate the contralateral vertebral body to achieve bicortical fixation.
Methodology Review
This is a descriptive study tracking complications for 28 patients over 2 years who received the aforementioned treatments. Therefore, no comparative results or statistical analyses were conducted. The purpose of this study is to provide treatment guidelines for spinal kyphotic deformities with pseudarthrosis caused by osteoporotic vertebral fractures. Additionally, recommendations for treating immobile kyphotic deformation cases are presented through literature review. Multiple recommendations and guidelines are provided, however, the number of cases in this series is too small, the types of procedures too varied and the outcome measures too limited to justify any of these recommendations as anything but observations. They describe a 77% success rate which is defined as an improvement in pain.
Quality of Evidence: Low
Recommendations for Integrating into Your Clinical Practice
The results of this study can serve as a reference, albeit to a limited extent, for future treatment guidelines for kyphotic deformities with pseudarthrosis in osteoporotic vertebral fracture cases. While this paper covers an important topic in of osteoporotic fractures complicated with spinal deformity and neurological deficits, the paper is set up as a case series and literature review without a significant take home message. While informative, clinicians should not use these treatment guidelines in their practice until more evidence is generated.
Discussion
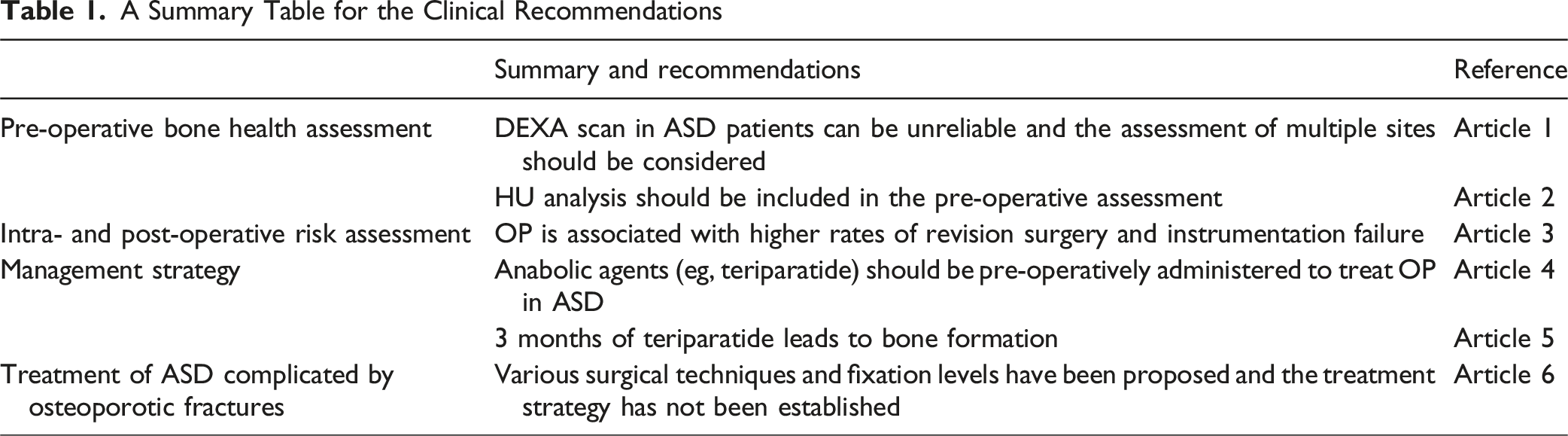
In the present review paper, we have focused on studies that cover the evaluation, implications, and management of osteoporosis in relation to spinal deformity surgery. A summary table of the recommendations for clinicians to apply in their practice is provided as Table 1. While osteoporosis and mechanical failures continue to be major challenges, the advent of Hounsfield units in directly measuring the density of the vertebra of interest and the effectiveness of newer osteoporosis medications like anabolic agents, have greatly impacted the current manner in managing bone health in ASD patients. However, DEXA scan results currently determine whether a patient is osteoporotic based on the WHO criteria. As such, low HUs alone may not be sufficient to confirm a diagnosis of osteoporosis and therefore in some jurisdictions, may not allow for the institution of medical treatments. Osteoporosis management with anabolic agents have become a major topic of current literature. Determining the appropriate dose and duration of treatment remains controversial, however, the benefits in terms of improved bone healing and reduced mechanical complications seem to be a recurring theme in multiple papers. The anabolic effect of these medications reinforces the bone density of osteoporotic vertebrae, enhances intra- and extra-articular bone formation, and improves trabecular structure leading to acceleration of the fusion process. Ebata et al. reported that weekly teriparatide administration improved the fusion rate at 6 months following posterior or transforaminal lumbar interbody fusion. 9 Pan et al concluded in their systematic review and meta-analyses that teriparatide showed significantly better outcomes in radiologic measures by increasing bone fusion rate and reducing the risk of screw loosening. 10 While the evidence specific to spinal deformity cohort is still lacking, it seems reasonable to extrapolate the excellent results of the degenerative cohorts to multi-level deformity constructs where obtaining a solid fusion is of paramount importance.
In everyday clinical practice, we recommend using forearm DEXA as an additional anatomical location and analysis of HUs from preoperative CT scan for more accurate assessment of osteoporosis. With osteoporosis shown to be associated with higher rates of adjacent level issues, pseudarthrosis, mechanical failures and blood loss, we recommend obtaining objective data regarding the status of patients’ bone prior to undergoing elective spine surgery to improve peri-operative planning and potentially improving their bone health prior to surgery. We suggest being aware of blood management interventions in patients with osteoporosis, although we recognize that clear guidelines are lacking. Lastly, when available, we suggest using anabolic agents in osteoporotic ASD patients who do not have contraindications for this treatment.
Rare adverse effects with the use of Teriparatide involve transient hypercalcemia, orthostatic hypotension, and a theoretical risk of osteosarcoma, which has been observed in animal studies but not confirmed in humans. 11 Contraindications to teriparatide use include pre-existing hypercalcemia, metabolic bone diseases other than osteoporosis (eg, Paget’s disease), bone metastases or skeletal malignancies, prior skeletal radiation therapy, and severe renal impairment. Monitoring recommendations include checking serum calcium levels after initiating therapy and periodically thereafter.
While we have provided recommendations based on the reviewed articles and current consensus, factors such as urgency of surgery, cost burdens, and health systems will have significant impact on the ability to implement osteoporosis protocols. Further, while strong associations between osteoporosis and adverse events have been established, we do not feel the evidence is sufficiently robust to mandate implementing these recommendations on a global level. Further clinical trials and prospective and retrospective reviews addressing these issues can help strengthen recommendations in the future.
In order to further strengthen clinical recommendations, we propose that more patient outcome-oriented studies be designed. These future investigations should aim to clarify which core sets for bone health assessment are most beneficial for specific patient populations, as well as which modalities and what duration of osteoporosis treatment can improve patient outcomes by mitigating perioperative risk. This knowledge will contribute to the establishment of standardized management strategies for ASD complicated by osteoporosis.
Conclusion
Bone health assessment should be routinely performed before ASD surgery. Despite DEXA scan being the gold standard for bone assessment, it has limited accuracy in deformed spines, and alternatives such as HUs have shown better correlation to mechanical complications in ASD patients. Osteoporosis has been shown to be a significant risk factor for post-operative mechanical complications in ASD surgery. Anabolic agents have demonstrated excellent results in restoring bone health prior to surgery and have been shown to reduce mechanical complications in spinal deformity surgery. While high-level evidence is still yet to be established, all healthcare providers dealing with ASD should be aware of the importance of bone health for optimizing post-operative outcomes.
Footnotes
Acknowledgement
This work was organized by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.