
Abstract
Study Design
Retrospective study.
Objectives
To investigate the prevalence of cervical kyphosis, identify factors influencing cervical sagittal alignment and analyze its relationship with spino-pelvic parameters in asymptomatic children and adolescents.
Methods
410 asymptomatic children and adolescents aged 4-18 years were included. Cervical sagittal alignment types and radiographic parameters were measured in the full-length spine X-ray. Three groups were assigned according to Toyama method: lordotic group, straight and sigmoid group, kyphotic group. Participants were stratified by gender and age, and differences in spinal parameters were analyzed. To determine factors influencing cervical sagittal alignment, a multinomial logistic regression was conducted.
Results
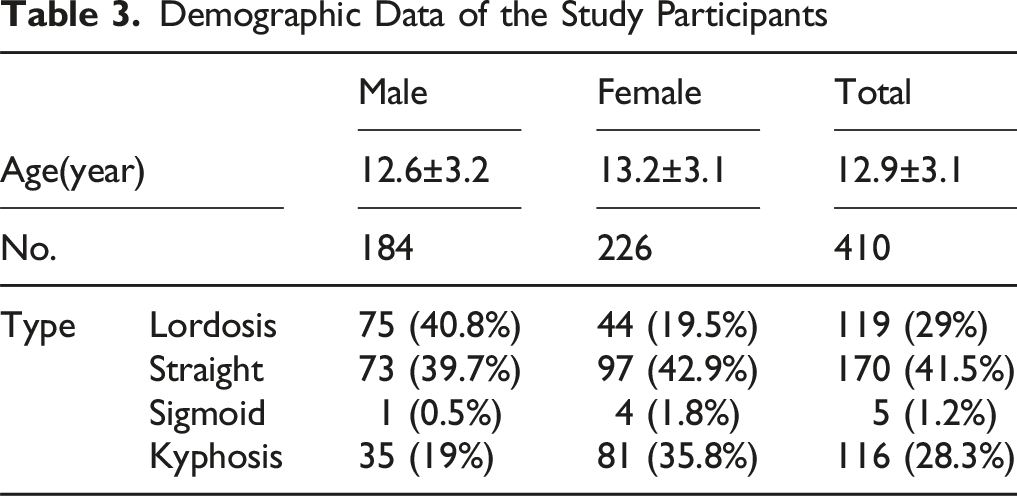
Among the 410 participants, 119 (29.0%) were classified as lordotic, 170 (41.5%) as straight, 5 (1.2%) as sigmoid, and 116 (28.3%) as kyphotic of the cervical sagittal alignment. Females exhibited a higher prevalence of kyphosis compared to males (35.8% vs 19.0%). Furthermore, kyphosis prevalence increased with age, from 0% in the 4-6-year-old group to 39.2% in the 16-18-year-old group. Strong positive correlations were observed between T1 slope and C2-C7 Cobb angle (r = 0.667, P < 0.01), as well as between lumbar lordosis and sacral slope (r = 0.758, P < 0.01). Age and C2-C7 Cobb angle were identified as predictors of cervical sagittal alignment via multinomial logistic regression analysis.
Conclusions
This study revealed that cervical kyphosis prevalence was comparable to lordosis in asymptomatic pediatric population, which challenged the traditional view of kyphosis as pathological. Additionally, cervical sagittal alignment showed significant gender- and age-related differences. These findings contribute to understanding pediatric cervical morphology and refining surgical strategies.
Keywords
Introduction
Maintaining a natural head position and horizontal gaze with minimal energy expenditure in daily life depends critically on cervical sagittal balance. 1 It has been well established since the 1960s that people have a lordotic curvature of the cervical spine. 2 However, recent studies showed that 14.8%–38.3% of asymptomatic adults exhibited physiological cervical kyphosis.3-5
The Multi-Ethnic Alignment Normative Study (MEANS) by Sardar et al reported that thoracic kyphosis (TK) increased with age, which led to an increase in T1-slope (T1S) and a compensatory increase in cervical lordosis. 6 These findings may not apply to pediatric population undergoing dynamic skeletal maturation. Previous studies on asymptomatic children and adolescents have predominantly focused on changes of spinal sagittal parameters during growth, while the distribution characteristics of cervical sagittal alignment have rarely been investigated.7-9
Therefore, this study aimed to explore the distribution characteristics of cervical sagittal alignment and its association with spino-pelvic parameters in asymptomatic children and adolescents. The findings are expected to address the knowledge gap in evaluating physiological cervical development in children and provide evidence-based guidance for pediatric cervical health management.
Methods
Study Population
This single-center retrospective study was approved by the Ethics Committee of Peking University People’s Hospital (2016PHB186-01) and initially included 1025 children and adolescents who underwent scoliosis evaluation at the Spine Surgery Outpatient Clinic of Peking University People’s Hospital between January 2020 and December 2024. All personally identifiable information of patients—including but not limited to names, residential addresses and telephone numbers— were anonymized to ensure patient confidentiality. The inclusion criteria comprised: (1) age ≤18 years; (2) absence of radiographic evidence of scoliosis (Cobb angle <10°) on full-length spine x-ray; (3) neutral head position during lateral full-length spine x-ray, defined by a chin-brow vertical angle (CBVA) range of −4.7° to 17.7°; and (4) a Neck Disability Index (NDI) score of 0 (indicating no neck pain or functional limitations). Exclusion criteria included: (1) history of spinal surgery, trauma, congenital malformations, tumors, or infections; (2) radiographic obscuration affecting parameter measurements; (3) presence of neuromuscular disorders or systemic skeletal developmental abnormalities.
Of the 1025 children and adolescents, 338 were excluded due to scoliosis, 149 were excluded for forward head position or hyperextension, and 128 were excluded due to radiographic obscuration, spinal deformities, or discomfort complaints. The final cohort included 410 children and adolescents stratified into five age groups: 4-6 years (n = 5), 7-9 years (n = 64), 10-12 years (n = 103), 13-15 years (n = 141), and 16-18 years (n = 97) for analysis of age-related variations in cervical sagittal parameters.
Radiographic Measurements and Data Collection
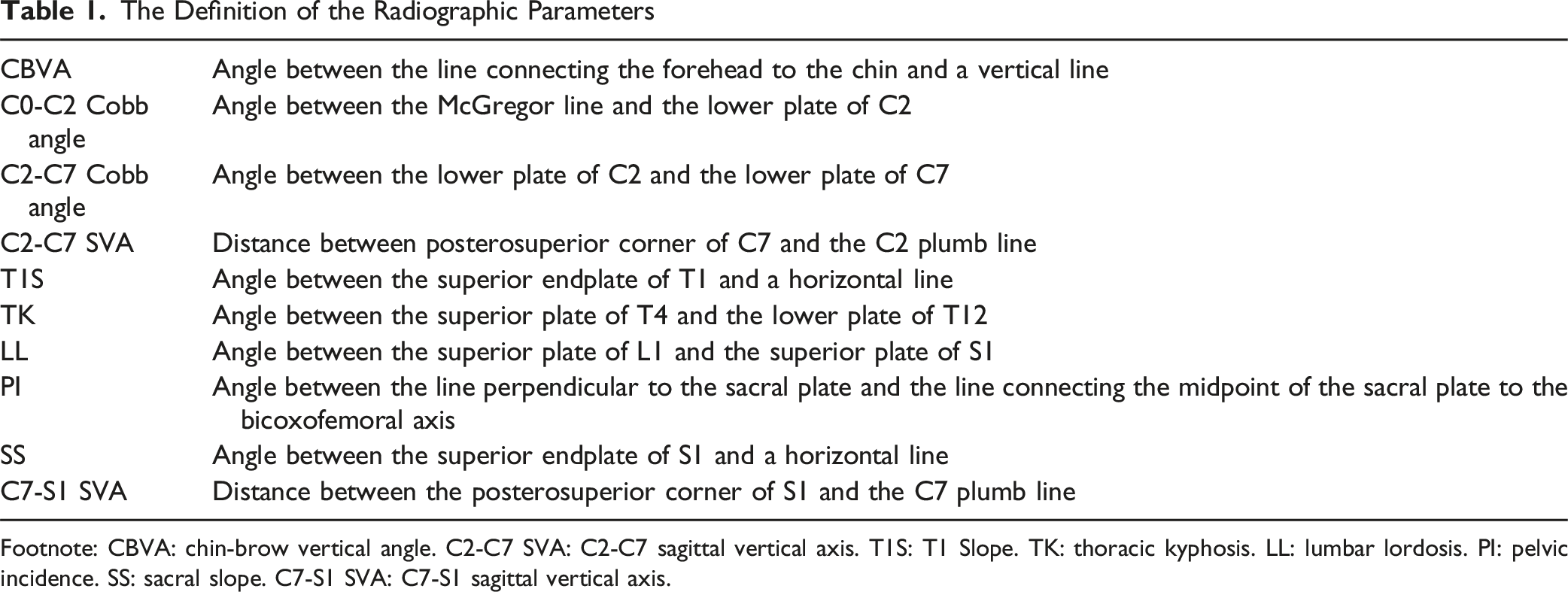
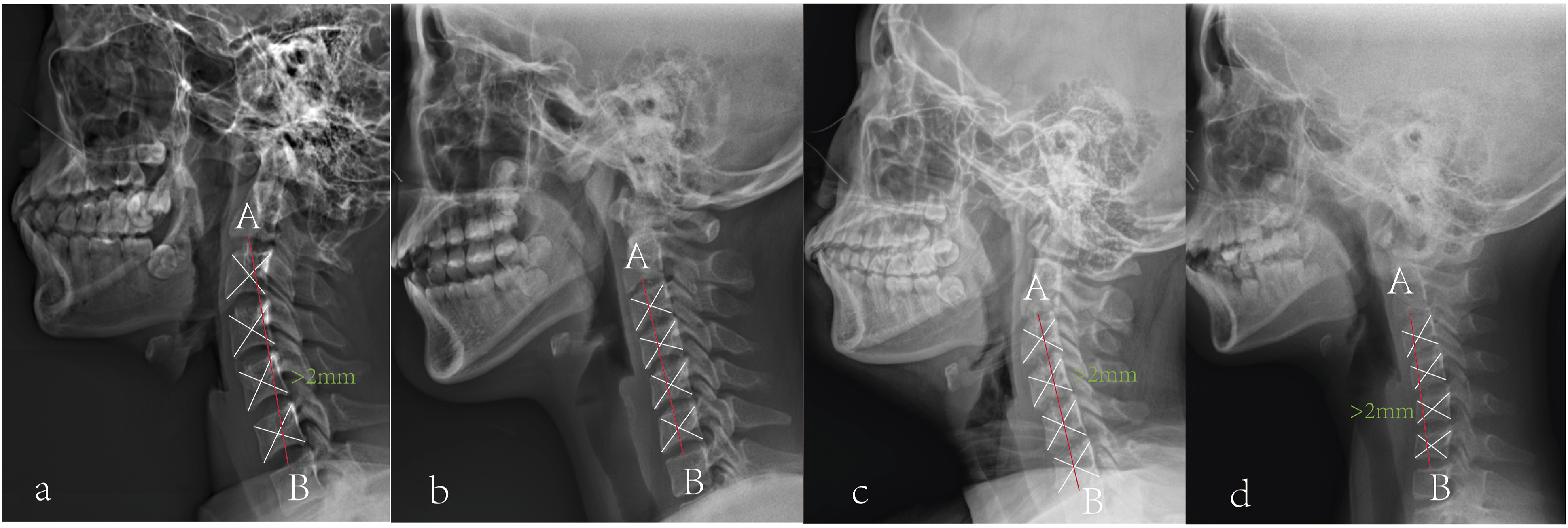
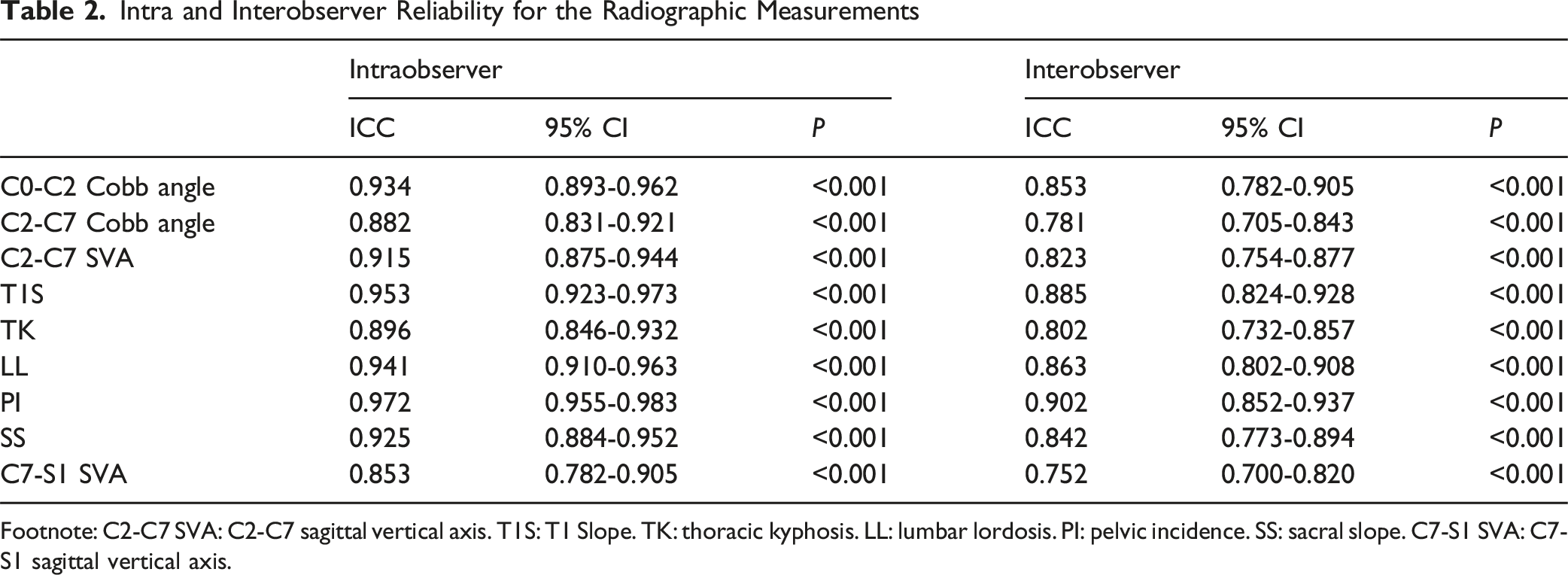
This study employed standardized radiographic protocols at our institution. During acquisition of full-length spine x-ray, participants were instructed to maintain an upright stance with feet shoulder-width apart, wrist flexed and hands relaxed with fingers in supraclavicular fossa, and head in neutral position (eyes gazing horizontally forward). Lateral radiographs were analyzed to measure the following parameters: cervical alignment type, CBVA, C0-C2 Cobb angle, C2-C7 Cobb angle, C2-C7 sagittal vertical axis (C2-C7 SVA), T1S, TK, lumbar lordosis (LL), pelvic incidence (PI), sacral slope (SS), C7-S1 sagittal vertical axis (C7-S1 SVA). Measurement methodologies are detailed in Figure 1 and Table 1. Cervical sagittal alignment was classified using the Toyama method. The geometric center of each vertebral body (C3–C6) was defined as the intersection point of the diagonals of a quadrilateral formed by the four edges of the vertebral body. Line AB was constructed by connecting point A (midpoint of the C2 inferior endplate) and point B (midpoint of the C7 superior endplate). Based on the positional relationship between the geometric centers of C3–C6 and line AB, 410 asymptomatic children were classified into four cervical sagittal alignment groups: lordotic, straight, sigmoid, and kyphotic (Figure 2). Using the institutional Picture Archiving and Communication System (PACS), two orthopedic surgeons with 7 and 5 years of clinical experience measured radiographic parameters independently. All parameters were reassessed with an interval of >1 month from the initial measurement. Inter-observer reliability (between surgeons) and intra-observer reliability (repeated measurements by the same surgeon) were quantified using intraclass correlation coefficient (ICC) (Table2). Measurements of Sagittal Parameters on a Representative Sagittal Radiograph. CBVA: Chin-Brow Vertical Angle. C2-C7 SVA: C2-C7 Sagittal Vertical Axis. TK: Thoracic Kyphosis. LL: Lumbar Lordosis. PI: Pelvic Incidence. SS: Sacral Slope. C7-S1 SVA: C7-S1 Sagittal Vertical Axis The Definition of the Radiographic Parameters Footnote: CBVA: chin-brow vertical angle. C2-C7 SVA: C2-C7 sagittal vertical axis. T1S: T1 Slope. TK: thoracic kyphosis. LL: lumbar lordosis. PI: pelvic incidence. SS: sacral slope. C7-S1 SVA: C7-S1 sagittal vertical axis. Cervical Sagittal Alignment by Toyama Method: (a) Lordosis: All Geometric Centers of C3–C6 Lay Anterior To Line AB, With at Least One Center Having a Horizontal Distance ≥2 mm From Line AB; (b) Straight: All Geometric Centers of C3–C6 Remained Within 2 mm of Line AB; (c) Sigmoid: Some Geometric Centers of C3–C6 Were Anterior to Line AB, While Others Were Posterior, With at Least One Center Having a Horizontal Distance ≥2 mm From Line AB; (d) Kyphosis: All Geometric Centers of C3–C6 Lay Posterior to Line AB, with at Least One Center Having a Horizontal Distance ≥2 mm From Line AB Intra and Interobserver Reliability for the Radiographic Measurements Footnote: C2-C7 SVA: C2-C7 sagittal vertical axis. T1S: T1 Slope. TK: thoracic kyphosis. LL: lumbar lordosis. PI: pelvic incidence. SS: sacral slope. C7-S1 SVA: C7-S1 sagittal vertical axis.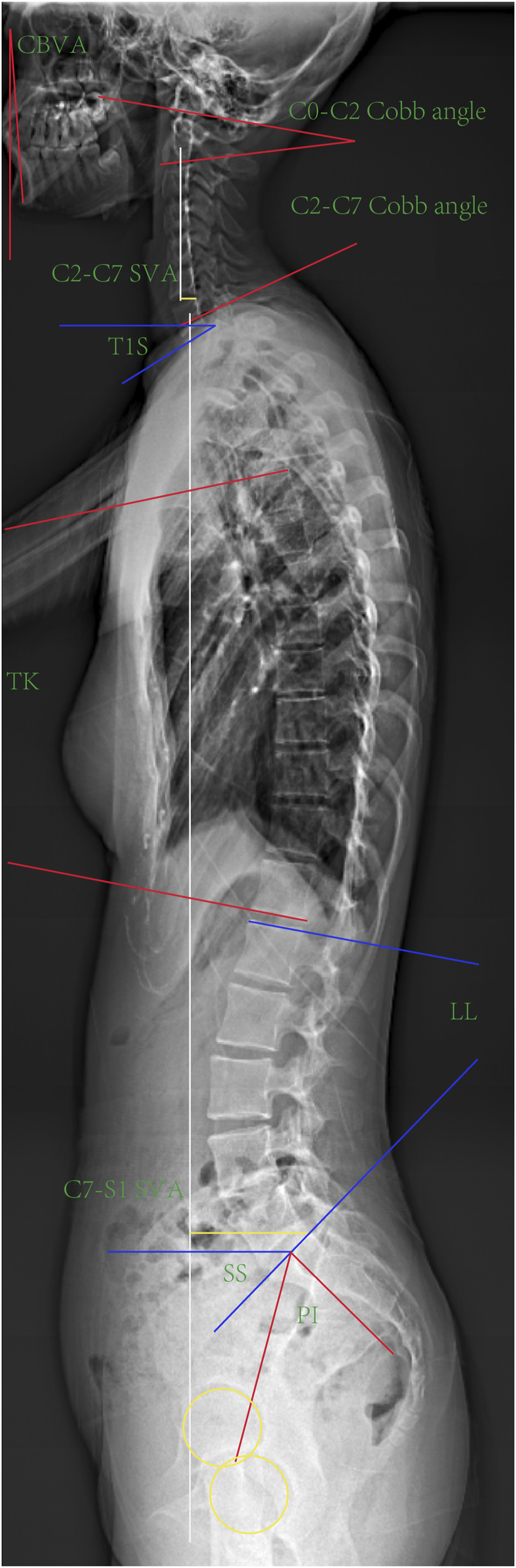
Statistical Analysis
All statistical analyses were performed using SPSS version 24.0 (IBM Corp, Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation, while categorical variables were described as frequency (percentage). Intergroup comparisons were conducted as follows: gender-related differences in spinal sagittal parameters were evaluated using Student’s t-test; Alignment type comparisons among lordotic, straight and sigmoid, and kyphotic groups were analyzed via one-way ANOVA; Correlation analyses between spinal sagittal parameters were assessed using Pearson’s correlation coefficients. Multinomial logistic regression models were constructed to identify predictors of cervical sagittal alignment, with age, gender, and spinal sagittal parameters as independent variables. Odds ratios (OR) with 95% confidence intervals (CI) were calculated to quantify associations. A two-tailed P < 0.05 was set as the significance threshold.
Results
Demographic Data of the Study Participants
Distribution of Radiographic Parameters Within the Three Groups in Terms of Cervical Alignment
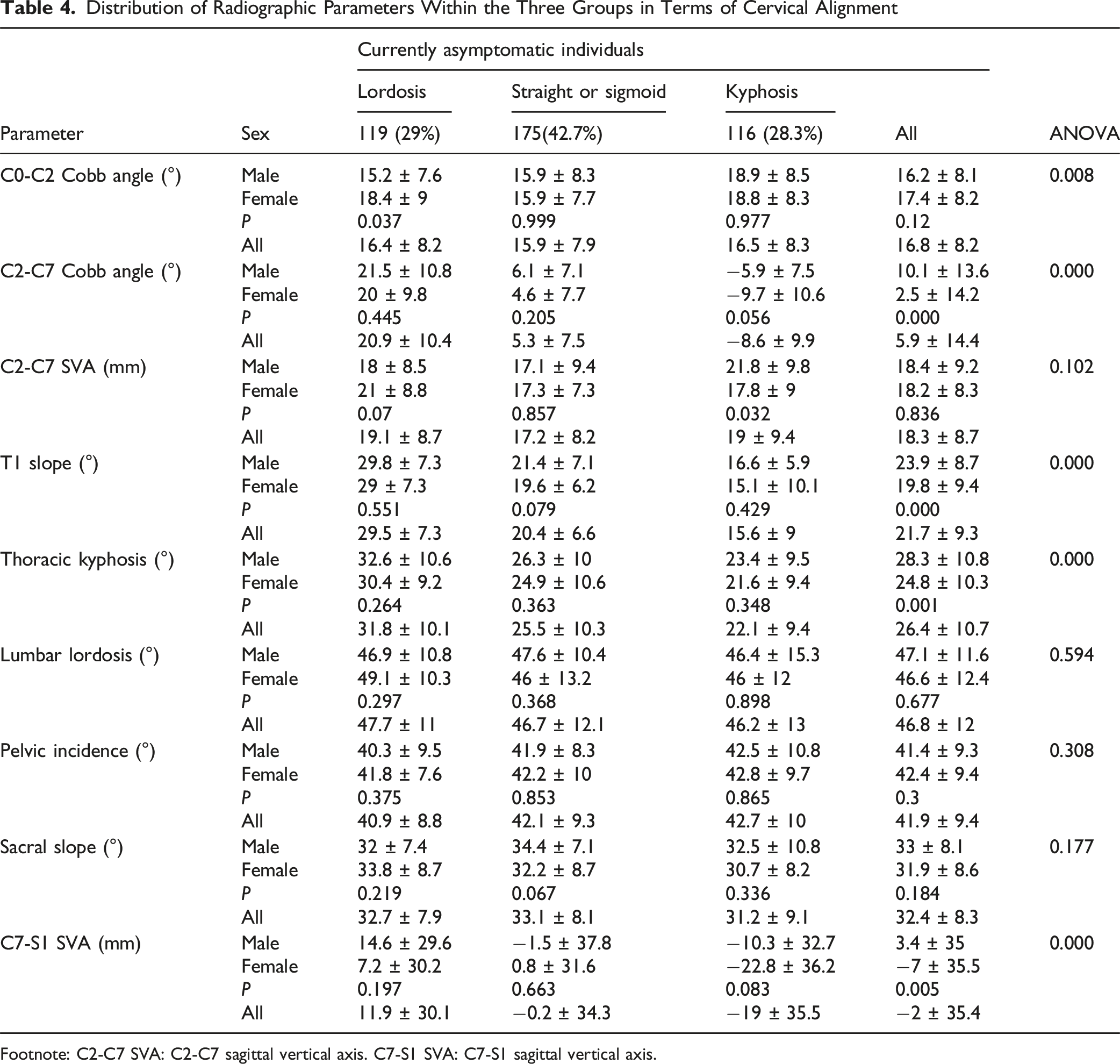
Footnote: C2-C7 SVA: C2-C7 sagittal vertical axis. C7-S1 SVA: C7-S1 sagittal vertical axis.
Significant age-related trends were observed: kyphotic prevalence increased with age (0%, 15.6%, 19.4%, 34.0%, 39.2%); C2-C7 Cobb Angle demonstrated a decreasing trajectory (14.9 ± 14.8°, 10.2 ± 14.7°, 7.0 ± 15.9°, 5.0 ± 12.8°, 2.8 ± 14.2°); PI showed gradual elevation (30.8 ± 7.7°, 38.0 ± 6.3°, 40.8 ± 10.1°, 44.3 ± 9.2°, 45.8 ± 8.9°). While, the C0-C2 Cobb angle remained stable across age groups (16.4 ± 5.0°, 16.9 ± 9.5°, 16.7 ± 8.2°, 17.3 ± 8.5°, 16.4 ± 7.1°), demonstrating minimal developmental variation (Figure 3). The Parameters in Five Age Groups: (a) (Kyphosis Prevalence), (b) (C0-C2 Cobb Angle), (c) (C2-C7 Cobb Angle), (d) (C2-C7 SVA), (e) (T1S), f (TK), (g) (LL), (h) (PI), (i) (SS)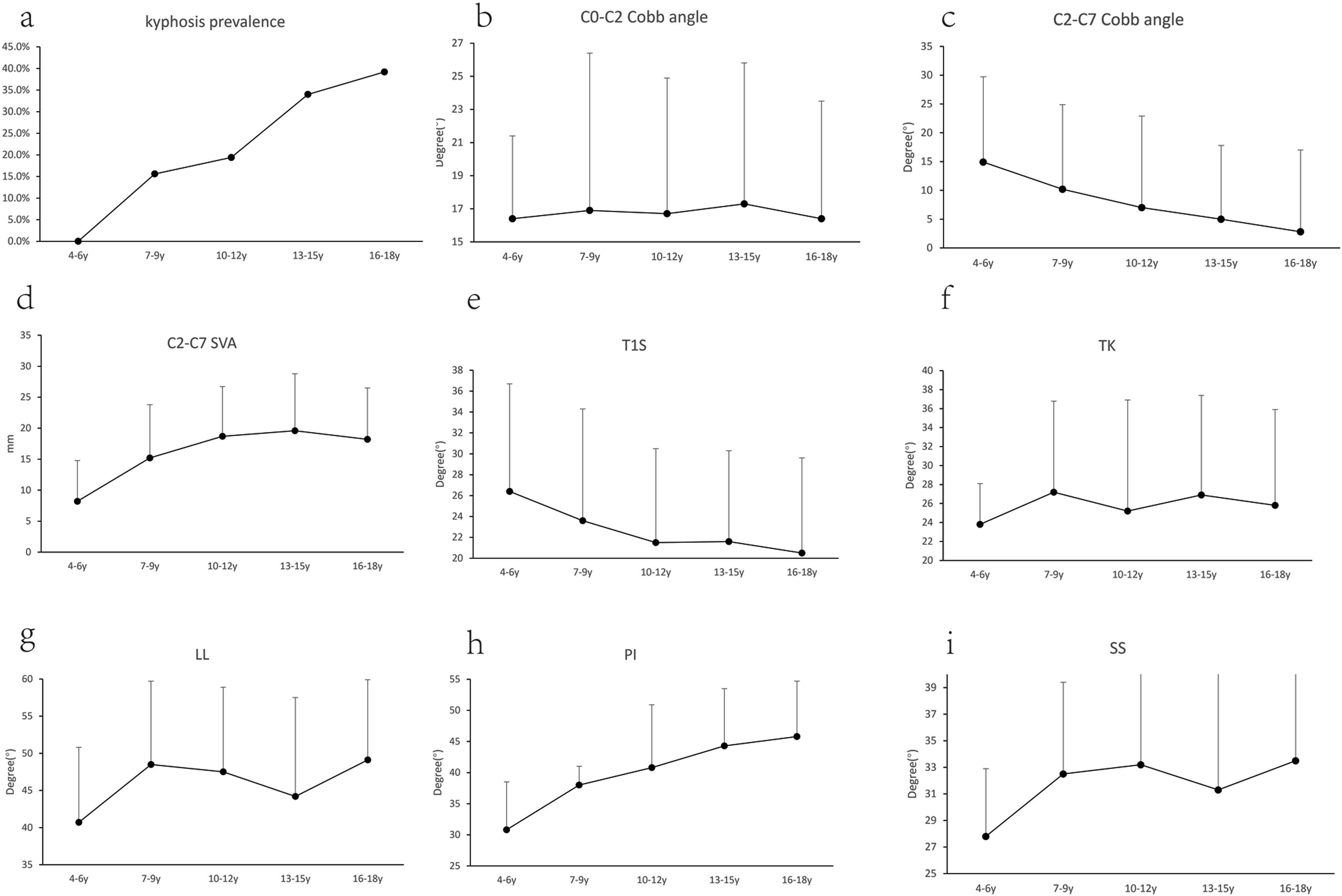
Pearson Correlation Coefficient and P Value of the Parameters
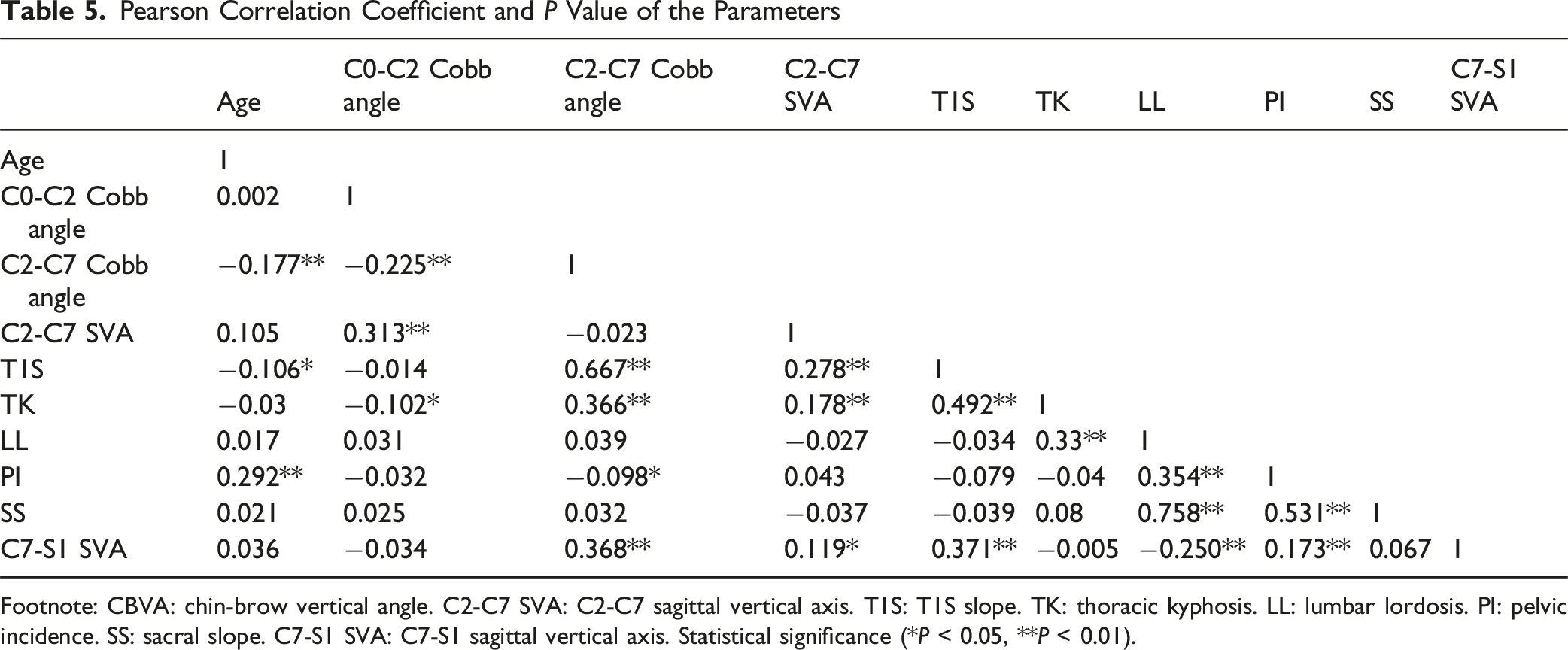
Footnote: CBVA: chin-brow vertical angle. C2-C7 SVA: C2-C7 sagittal vertical axis. T1S: T1S slope. TK: thoracic kyphosis. LL: lumbar lordosis. PI: pelvic incidence. SS: sacral slope. C7-S1 SVA: C7-S1 sagittal vertical axis. Statistical significance (*P < 0.05, **P < 0.01).
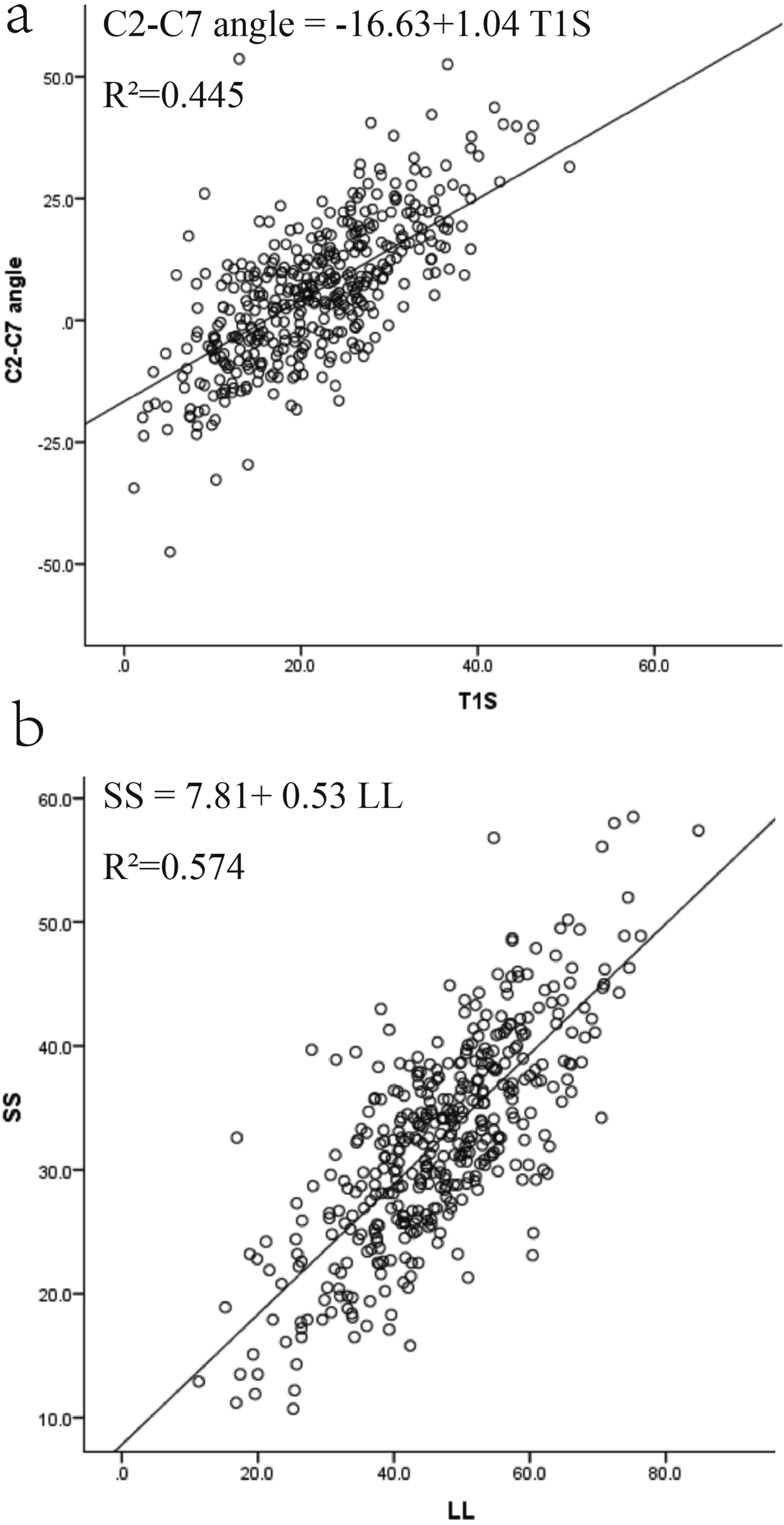
The Scatter Diagram on the Relationship Between T1S and C2-C7 angle (4a), as Well as Between LL and SS (4b)
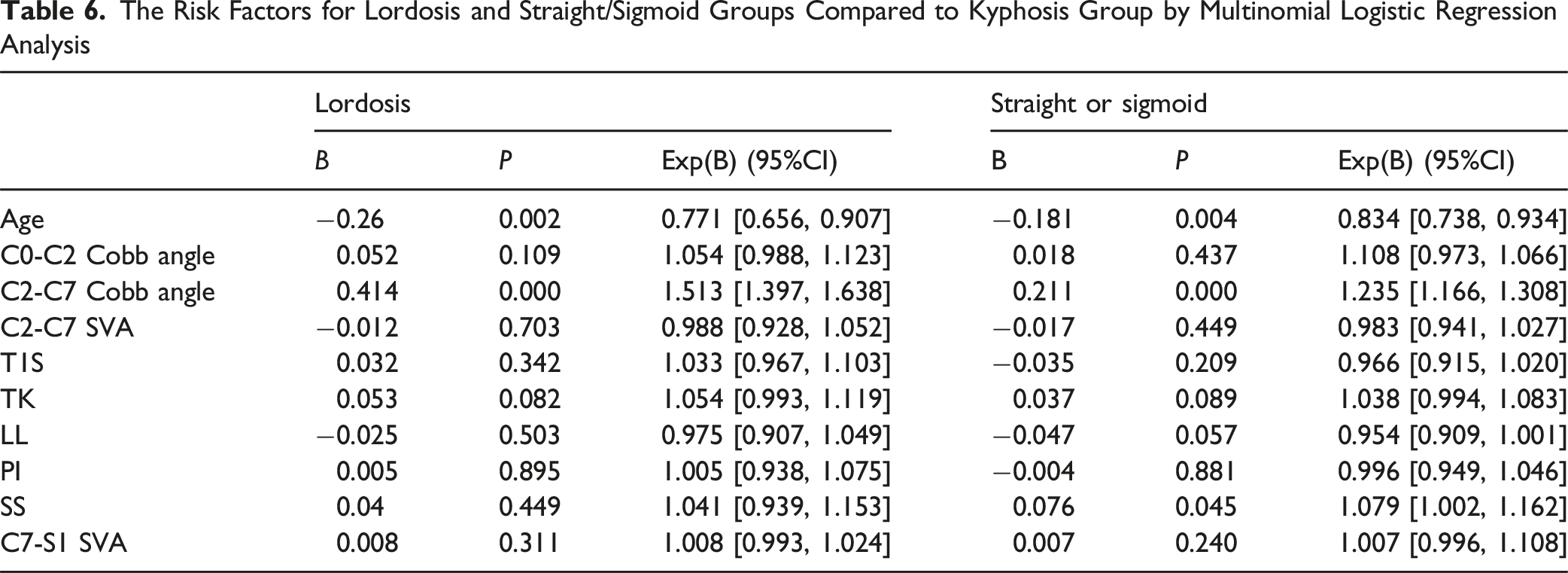
The Risk Factors for Lordosis and Straight/Sigmoid Groups Compared to Kyphosis Group by Multinomial Logistic Regression Analysis
Discussion
This study aimed to analyze the distribution of cervical sagittal alignment and its correlation with spino-pelvic parameters in 410 asymptomatic children and adolescents. The prevalence of cervical kyphosis (28.3%) was comparable to that of lordosis (29%) in this asymptomatic cohort. Males had a larger C2-C7 Cobb angle and lower kyphosis prevalence. Kyphotic prevalence increased with age, from 0% (4-6 years) to 39.2% (16-18 years). C2-C7 Cobb angle varied significantly among different groups: lordosis (20.9 ± 10.4°), straight and sigmoid (5.3 ± 7.5°), and kyphosis (−8.6 ± 9.9°) (P < 0.001). Strong correlations (r > 0.6) were observed between T1S and C2-C7 Cobb angle (r = 0.667), and between LL and SS (r = 0.758). Multinomial regression analysis identified both age and C2-C7 Cobb angle as predictors of cervical sagittal alignment.
With kyphosis defined as a C2-C7 Cobb angle less than 0°, previous studies reported a prevalence of 14.8-38.3% in asymptomatic adults.3,10,11 However, data remained scarce for asymptomatic children and adolescents. In this study, we considered children who visited the spinal surgery outpatient clinic solely for scoliosis screening and had no spine-related complaints as “asymptomatic,” a definition supported by other studies.9,12 Moreover, a more detailed Toyama method was employed which categorized cervical sagittal alignment into four types: lordotic, straight, sigmoid, and kyphotic. 13 Given the low proportion of sigmoid types (1.2%) in our cohort, sigmoid and straight types were combined into a single group to mitigate statistical errors.
A standard full-length spine X-ray requires participants to maintain a neutral head position with eyes gazing straight ahead. However, in practice, due to variations in postural habits, some participants may exhibit slight head extension or flexion while still maintaining a horizontal gaze through compensatory eye movements. Miyake et al demonstrated that such head position changes altered cervical sagittal alignment, particularly in the upper and mid-cervical spine.14,15 The CBVA, primarily used to assess spinal deformity and visual field limitations in ankylosing spondylitis patients, also reflects head extension or flexion status. Based on previous studies, we defined CBVA between −4.7° and 17.7° as a neutral head position.1,11
This study unexpectedly found that the prevalence of cervical kyphosis was nearly equal to that of cervical lordosis in asymptomatic children and adolescents. The mean C2-C7 Cobb angle was 5.9 ± 14.4°, which was similar to the range of 0.7-13.4° reported in previous studies of asymptomatic children and adolescents.9,12,16 Across the lordotic, straight and sigmoid, and kyphotic groups, the C0-C2 Cobb angle increased while the C2-C7 Cobb angle showed an inverse change. Pearson analysis further demonstrated a significant negative correlation between these two parameters. A reasonable explanation was that compensatory increase in lordosis at the C0–C2 level became necessary to maintain horizontal gaze, counterbalancing the reduced lordosis at the C2–C7 level. 17 Compared to females, males had a significantly lower prevalence of kyphosis (19% vs 35.8%) but a greater C2-C7 Cobb angle (10.1 ± 13.6° vs 2.5 ± 14.2°, P < 0.001). However, Yeh et al found no significant gender-related differences in the C2-C7 Cobb angle. 18 Cervical muscle function was closely linked to the maintenance of lordosis, as Wang et al reported superior muscle performance in the lordotic group compared to the kyphotic group. 19 We hypothesized that males, potentially due to higher androgen levels, developed stronger neck muscles than females, which may better maintain lordotic alignment.
In this study, participants were stratified into five age groups according to growth milestones. 9 During growth, the kyphotic prevalence and PI increased, while the C2-C7 Cobb angle gradually decreased. Based on an analysis of 257 asymptomatic children, Zhou et al demonstrated a linear correlation between PI and age, and proposed the formula “PI = 26.243 + 1.153 × age”. 20 However, MEANS reported an increase in the C2-C7 Cobb angle with age, which was consistent with other adult cervical sagittal alignment studies.4,6,10,21 This phenomenon in adults may be attributed to age-related regional stress redistribution within the spine. Prolonged stress concentration at the apex of thoracic kyphosis leads to relative height reduction in the anterior vertebral body compared to its middle and posterior portions. 22 Consequently, TK increases with age, driving compensatory elevation of the T1S and subsequent enhancement of cervical lordosis. 23 However, this mechanism does not appear to apply to children and adolescents. A study by Hu et al involving 1916 healthy Chinese children found no significant differences in TK during growth. 8 Similarly, Pesenti et al reported a U-shaped trajectory of TK (initial decrease followed by increase) during growth in 1059 asymptomatic French children, though neither study evaluated cervical sagittal alignment. 7 Our study further demonstrated that TK showed no progressive elevation during growth in children and adolescents. In a study involving 150 asymptomatic children and adolescents, Genevois et al also found that TK exhibited no significant changes with age, whereas the C2-C7 Cobb angle decreased. 16 Intriguingly, Lee et al observed an increase in TK but a decrease in C2-C7 Cobb angle during growth among 181 asymptomatic children.24These findings implied that cervical sagittal alignment in pediatric population may be predominantly influenced by skeletal maturation and postural habits rather than TK. Actually, alterations in any spinal region trigger adaptations in others through interdependent alignment mechanisms. 22 Cervical alignment changes in children and adolescents may precede and induce compensatory modifications in other regions. We postulate that increased academic demands and prolonged neck flexion during desk-based activities contribute to the age-related increase in kyphotic prevalence.
Correlation analysis revealed that age showed no or weak correlations (r < 0.3) with spinal sagittal parameters, which was in line with previous literature. 12 Strong correlations (r > 0.6) were observed between T1S and C2-C7 Cobb angle, as well as between LL and SS, which was consistent with previous study.20,23 The cervical spine, positioned between the cranium and thoracic spine, served as a transitional segment resting on the T1 base. Consequently, an increase in T1S or TK necessitated compensatory increase of the C2-C7 Cobb angle to maintain horizontal gaze. Similarly, the strong correlation between LL and SS reflected spino-pelvic balance: increased SS drove greater LL to preserve trunk equilibrium.
To identify the factors influencing the cervical sagittal alignment, we performed a multinomial logistic regression analysis. The results identified C2-C7 Cobb angle and age as predictors of cervical sagittal alignment. With advancing age, the likelihood of kyphotic classification increased significantly. We hypothesized that this phenomenon was attributed to the increasing academic demands with age. Larger C2-C7 Cobb angles were associated with a higher probability of lordotic classification, which was readily comprehensible.
This study indicated that cervical kyphosis in children and adolescents may be a physiological status. Pathological cervical kyphosis can lead to symptoms such as neurological deficits, neck pain, inability to maintain a horizontal gaze, and dysphagia, with severe cases requiring surgical intervention. Due to the “asymptomatic” nature of physiological cervical kyphosis, surgical treatment is rarely recommended. However, for patients with kyphosis and other cervical disorders, distinguishing between “physiological” and “pathological” kyphosis is crucial, as this determines the necessity of combined kyphosis corrective surgery. Furthermore, the cervical sagittal alignment in children and adolescents exhibits significant age- and gender-related variations. Considering these factors, it becomes clear that the restoration of lordosis following corrective surgery should be tailored to the individual patient rather than targeting a uniform standard.
This research has several limitations. Firstly, “asymptomatic” in this study does not equate to the broader concept of “healthy.” Furthermore, the single-center nature of this study restricts generalizability, highlighting the need for future prospective multicenter studies to validate our findings. Secondly, exclusion of children with significant radiographic obscuration may influence the results, requiring CT or MRI for precise assessment. Additionally, although head position was standardized using a CBVA range of −4.7° to 17.7°, variations in CBVA among participants might still subtly influence cervical alignment. Lastly, due to the exclusive inclusion of an outpatient population, lack of data on weight, height, study habits and daily routines, and other variables prevented further analysis.
Conclusion
The prevalence of cervical kyphosis in asymptomatic pediatric population was 28.3%. Our study established normative baseline data for spinal sagittal parameters in asymptomatic children and adolescents, which serves as a reference for subsequent research. Spine surgeons should consider age- and gender-related variations in cervical sagittal alignment when performing cervical spine surgery for pediatric patients.
Footnotes
Ethical Considerations
This study has been approved by Ethics Committee of Peking University People’s Hospital. This study is a retrospective study utilizing medical records obtained from previous clinical diagnoses and treatments. It poses no risks to the participants, and the research data have been anonymized. Therefore, this study is exempt from obtaining informed consent.
Author Contributions
Hy. L and Cj. L designed this study. Sq. Z collected the raw data, conducted statistical analyses, and drafted the initial manuscript. C. Z and Yh. Wu further revised and refined the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our study was supported by Beijing Natural Science Foundation (No. L242165), National Key R&D Program of China (No. 2022YFB4703000), Major Health Special Project of the Ministry of Finance of China (grant number: 2127000432).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data could be obtained by contacting the corresponding author.