
Abstract
Study Design:
Retrospective cohort study.
Objective:
This study aims to report the incidence, risk factors, and recovery rate of neurological complications (NC) in patients with adult cervical deformity (ACD) who underwent corrective surgery.
Methods:
ACD patients undergoing surgery from 2013 to 2015 were enrolled in a prospective, multicenter database. Patients were separated into 2 groups according to the presence of neurological complications (NC vs no-NC groups). The types, timing, recovery patterns, and interventions for NC were recorded. Patients’ demographics, surgical details, radiographic parameters, and health-related quality of life (HRQOL) scores were compared.
Results:
106 patients were prospectively included. Average age was 60.8 years with a mean of 18.2 months follow-up. The overall incidence of NC was 18.9%; of these, 68.1% were major complications. Nerve root motor deficit was the most common complication, followed by radiculopathy, sensory deficit, and spinal cord injury. The proportion of complications occurring within 30 days of surgery was 54.5%. The recovery rate from neurological complication was high (90.9%), with most of the recoveries occurring within 6 months and continuing even after 12 months. Only 2 patients (1.9%) had continuous neurological complication. No demographic or preoperative radiographic risk factors could be identified, and anterior corpectomy and posterior foraminotomy were found to be performed less in the NC group. The final HRQOL outcome was not significantly different between the 2 groups.
Conclusions:
Our data is valuable to surgeons and patients to better understand the neurological complications before performing or undergoing complex cervical deformity surgery.
Keywords
Introduction
Adult cervical deformity (ACD) is caused by numerous etiologies, including iatrogenic, inflammatory congenital, traumatic, infectious, and neuromuscular disorders, arthropathy, and spondylosis.1,2 In severe ACD patients, cervical instability and sagittal malalignment can lead to pain, neurologic symptoms, and cervical specific symptoms, including difficulty in maintaining a horizontal gaze, dysphagia, and dyspnea. Recent studies had addressed the association between sagittal malalignment of the cervical spine and its health impact on symptomatic ACD patients.3-6 Corrective surgery is effective for most symptomatic patients, as it restores the sagittal malalignment, relieves symptoms, and improves patient-reported outcomes.1,7-10
The wide variations in surgical correction techniques, including different surgical approaches, osteotomy methods, and selection of fusion levels and numbers, make the surgical decision-making in ACD settings challenging and controversial. While recent endeavors have evolved around the development of classifications of treatment strategies,11-14 a strong consensus on the characteristics and surgical corrective techniques are still lacking. 15 Prior studies showed that variations in surgical approaches and osteotomy methods can significantly affect patient outcomes and occurrence of complications.15-21
Neurological complications are among the most significant concerns of ACD patients after a complex surgery. The reported incidence of overall complication in ACD patients was 34%-64.2%,19,20,22-26 and that of neurologic complications was 13.5%-28.9%.7,20,23-27 However, only a few studies focused solely on neurological complications. The types, risk factors, timing of neurological complications, management strategies, and recovery are still underreported. Thus, the present study aimed to report the details of neurological complications in ACD patients who had undergone corrective surgeries.
Materials and Methods
This was a retrospective study of a prospectively collected multicenter database of patients with CD from 2013 to 2015. Institutional review board approval was obtained from each of the participating sites across the country. Informed consent was obtained from the patients. Inclusion criteria of the database were patients aged >18 years and at least 1 of the following radiographic criteria: cervical scoliosis with Cobb angle ≥10°, C2-C7 sagittal vertical axis (SVA) ≥4 cm, cervical kyphosis ≥25°, and/or chin-brow vertical angle (CBVA) ≥25°. An additional criterion for patients included in this study was a minimum of 6-week follow-up to capture all acute and perioperative neurologic complications. Patients with an active tumor or infection were excluded.
Patients’ demographics and surgical details were collected and included age, sex, body mass index (BMI), Charlson comorbidity index (CCI), smoking status, history of cervical surgery, estimated blood loss (EBL), surgical time, levels fused, type of osteotomy, surgical approach, decompression, osteotomy, perioperative steroid used, bone morphogenic protein (BMP) used, and length of hospital stay. Radiographic parameters, including C2-C7 lordosis, C2-C7 sagittal vertical axis (cSVA), T1 slope (TS), and TS minus cervical lordosis (TS-CL), were measured on the standing cervical radiographs obtained preoperatively (baseline) and at the 6-week, 3-month, 6-month, 1-year, and 2-year post-operative follow-up.
Neurological complications were separated into surgery-related and non-surgery-related complications. Surgery-related complications included motor deficits, sensory deficits, radiculopathy, and spinal cord injury with myelopathy. Non-surgery-related complications included meralgia paresthesica, mental status changes, and stroke. The primary outcome of this study was the surgery-related complications at each time-point. Patients were then separated into groups with neurological complications (NC group) or without neurological complications (no-NC group).
Major complications were defined as those requiring additional intervention or a return to the operating room, resulting in increased length of hospital stay, or that were not resolved during follow-up. Minor complications were those that did not compromise the length of hospital stay, or require additional interventions, or managed with minimal changes to the plan of care. Recovery from neurological complications was recorded as none, partial, and complete during follow-up. Interventions for the neurological complications were recorded as observation, physiotherapy, or reoperation. The health-related quality of life (HRQOL) scores, including the neck numerical rating scale (NRS), EQ-5D, Neck Disability Index (NDI), and modified Japanese Orthopaedic Association (mJOA) score, were obtained preoperatively and at each post-operative follow-up visit.
Statistical analysis was performed using IBM SPSS (version 22.0; IBM Corp., Armonk, NY USA). Categorical data was compared using the chi-squared or Fisher’s exact tests. Continuous data was compared using an independent t-test or Wilcoxon rank-sum tests, where appropriate. A 2-tailed significance level was set at p < 0.1.
Results
A total of 124 patients were reviewed in the database, and 106 patients met the study’s inclusion criteria. Patients’ average age was 60.8 ± 11.0 years, and the mean follow-up duration was 18.2 ± 9.2 months. The proportion of female patients was 58.5%. Twenty-two neurological complications were observed in 20 patients; of which 15 were major (68.1%), and 7 were minor complications (31.9%) (Table 1). The overall incidence of surgery-related neurological complications was 18.9%. More than half of the neurological complications were identified within 30 days of surgery (n = 12, 54.5%). The most common complication type was nerve root motor deficit (n = 9, 40.9%), followed by radiculopathy (n = 6, 27.4%), sensory deficit (n = 5, 22.7%), spinal cord deficit (n = 1, 4.5%), and others (n = 1, 4.5%) (Table 1). In the subgroup analysis of neurological complication type and timing, the nerve root motor deficits were identified more frequently within 30 days (88.9%, p = 0.01) than after 30 days of surgery, whereas the sensory deficits (80%, p = 0.14) and radiculopathy (66.6%, p = 0.35) were more frequently identified after 30 days of surgery.
Overview of all Neurological Complications.
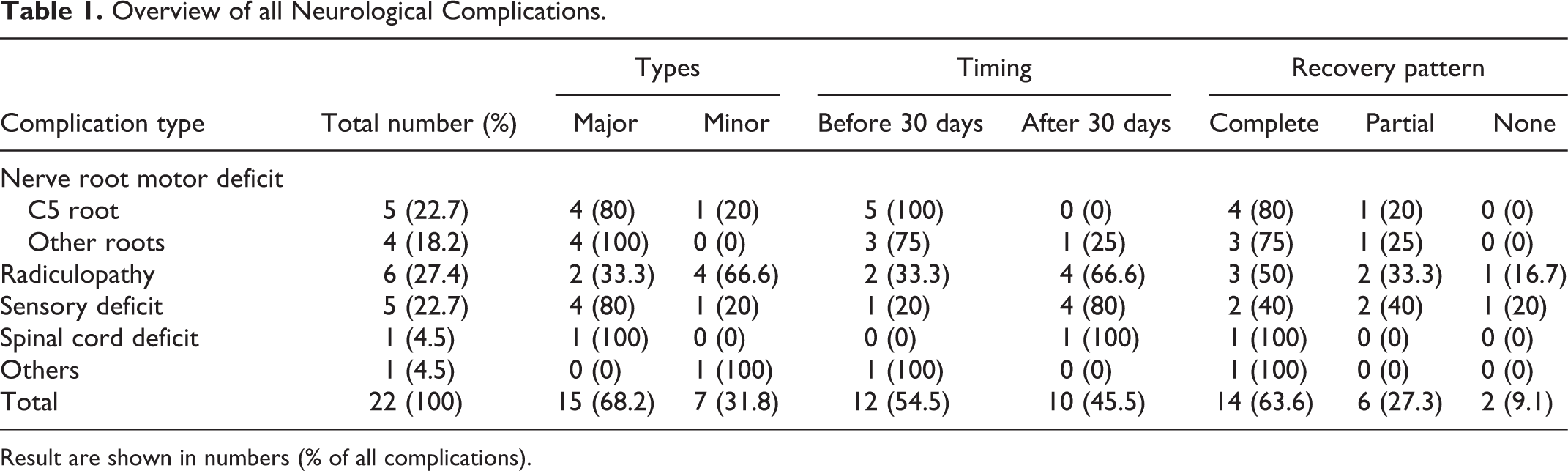
Result are shown in numbers (% of all complications).
Of the overall neurological complications, 90.9% (n = 20) had partial or complete recovery (63.6% complete recovery, 27.3% partial recovery). Most recoveries occurred in the first 6 months. Recovery was seen in 20% and 60% of patients at 6 weeks and 6 months, respectively. The proportion of patients with recovery continuing >12 months was 35%. The proportion of patients with complete recovery from nerve root motor deficits, sensory deficits and radiculopathy were 77.8%, 40% and 62.5%, respectively (Table 1). The neurological complication type was not correlated to the complete recovery rate (p = 0.2). Persistent neurological complication was observed in 2 patients (1.9% of patients), including one with radiculopathy and another with a sensory deficit. Ten patients received interventions for the neurological complications, including physical therapy (n = 6) and reoperations (n = 4). The reoperation rate of patients was 3.8% of the whole cohort and 20% of the NC group. The intervention type and timing were not significantly associated with the recovery from neurological complications.
Risk Analysis Between the NC and No NC Groups
Table 2 summarizes the demographic and baseline radiographic parameters of the NC and no-NC groups. The risk analysis of patients’ demographics showed that there were no significant differences between the NC and no-NC groups. The baseline values of the radiographic parameters of the entire cohort were as follows: C2-C7 lordosis, −6.9° ± 20.7°; T1 slope, 31.5° ± 17.1°; TS-CL, 38.3° ± 19.2°; and C2-C7 SVA, 39.4 ± 19.7 mm. The cSVA was higher in the NC group than in the no-NC group (44.2 ± 17.3 vs 38.3 ± 20.1 mm, p = 0.19), but the difference was not statistically significant. There was no significant difference in the baseline radiographic parameter values between the 2 groups.
Patient Demographic and Radiographic Parameters Between the 2 Groups.
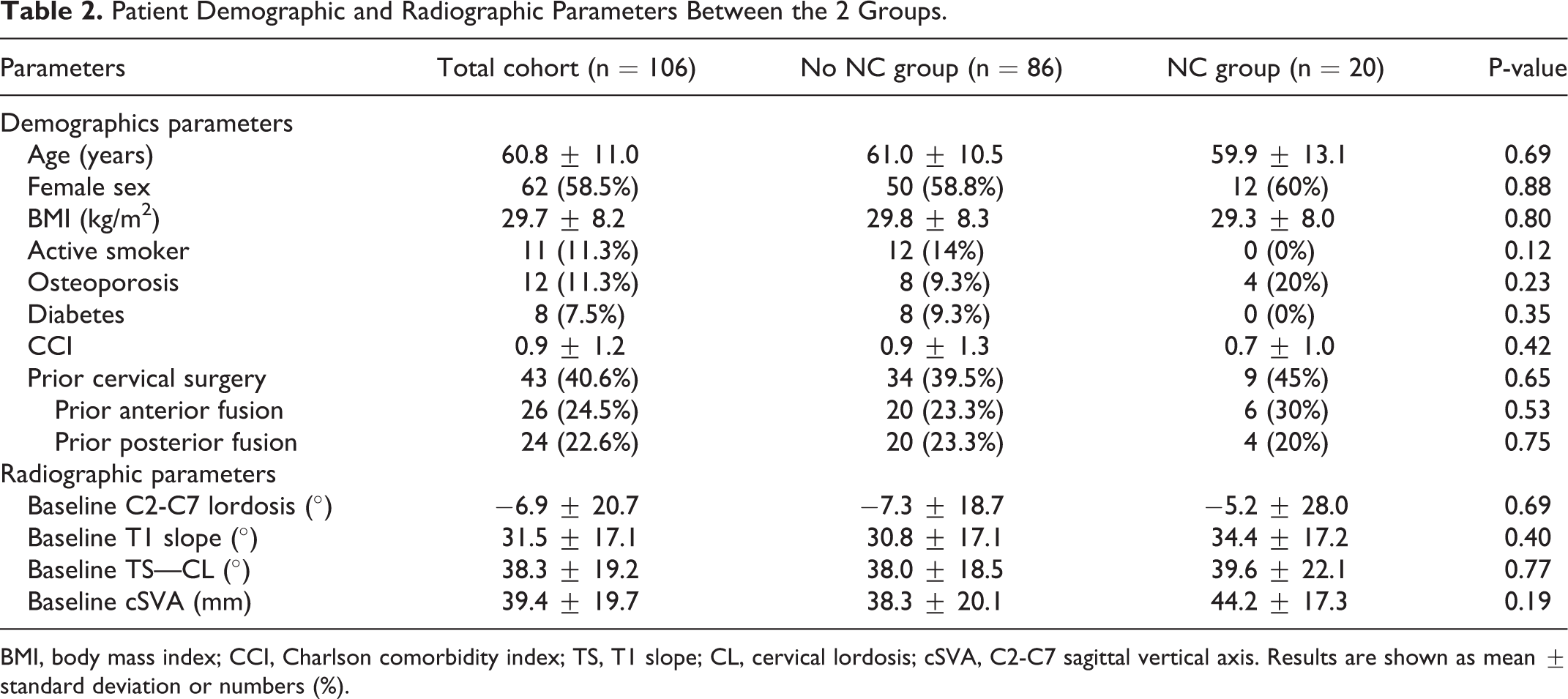
BMI, body mass index; CCI, Charlson comorbidity index; TS, T1 slope; CL, cervical lordosis; cSVA, C2-C7 sagittal vertical axis. Results are shown as mean ± standard deviation or numbers (%).
The results of the surgical parameter analysis showed that there were no differences in the type of approach, level fused, presence of anterior fusion, posterior three-column osteotomy (3CO), posterior laminectomy, and BMP used between the 2 groups (Table 3). The presence of anterior corpectomy and posterior foraminotomy was higher in the no-NC group (23.3% vs 17.4%) than in the NC group (5% vs 0% [p = 0.07], respectively). The NC group more frequently used perioperative steroids (70% vs 45.3%, p = 0.05). The length of hospital stay was higher in the NC group (9.4 ± 8.4 vs 6.2 ± 6.7 days, p = 0.07).
Surgical Details of Patients With and Without Neurologic Complications.
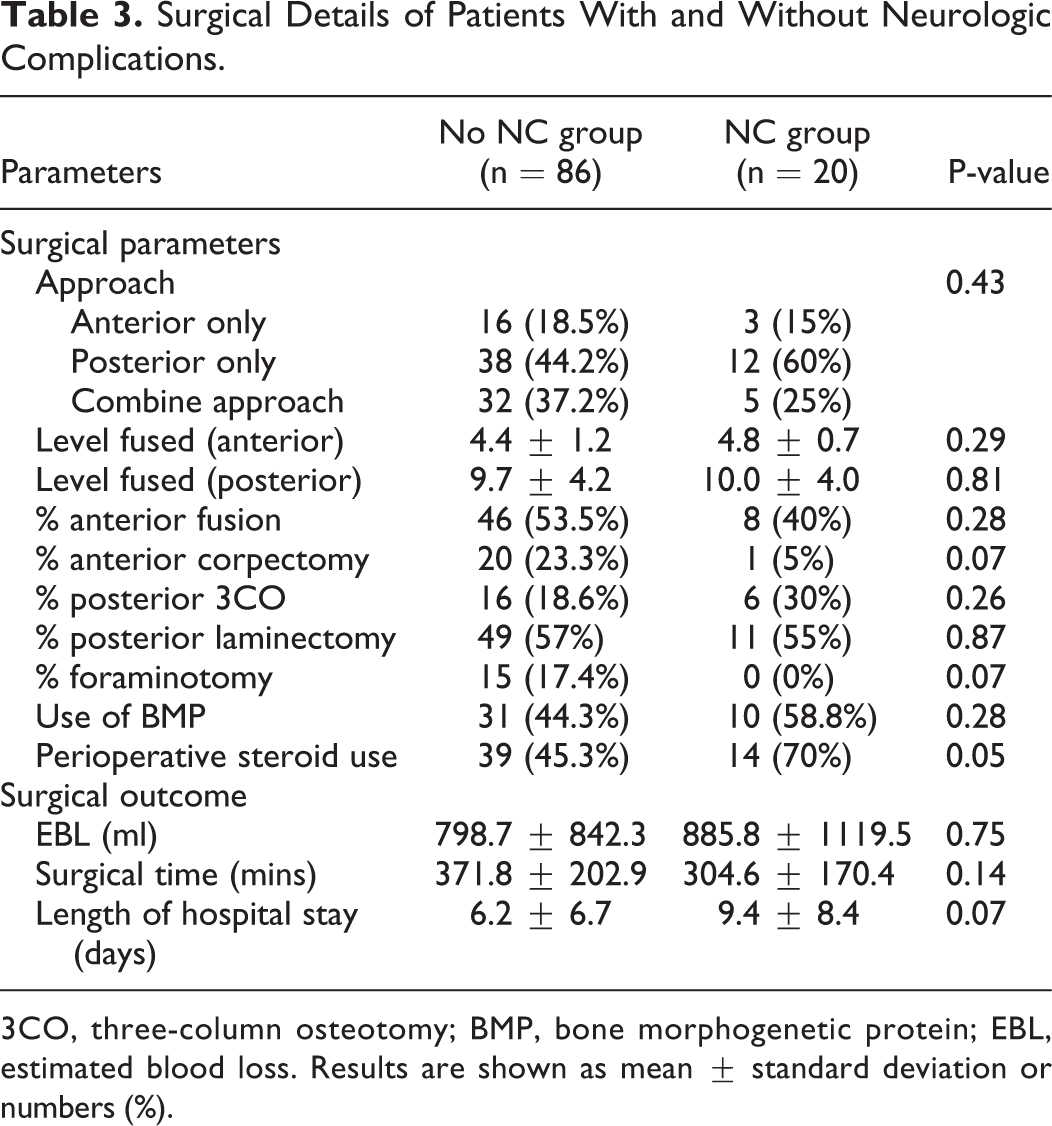
3CO, three-column osteotomy; BMP, bone morphogenetic protein; EBL, estimated blood loss. Results are shown as mean ± standard deviation or numbers (%).
HRQOL Outcomes
The mean preoperative baseline NRS and NDI scores were 6.9 ± 2.3 and 50.3 ± 17.6, respectively, indicating the presence of severe disability in the present cohort. The mJOA score was 13.3 ± 2.7, reflecting moderate cervical myelopathy. The NRS, NDI, and EQ5D scores improved significantly after surgery (p < 0.001) and were not significantly different between the 2 groups at baseline and final follow-up (Table 4). The NC group had a higher baseline mJOA score than the no NC group (14.4 ± 2.2 vs. 13.0 ± 2.7, p = 0.04). The NC group showed worsening in the mJOA score by −0.9 ± 2.3, whereas the no NC group showed an improvement by 1.4 ± 2.3. The change in mJOA score was significantly different between the 2 groups (p < 0.001); however, the final mJOA score between the 2 groups was not different.
Health-Related Quality of Life Scores of Patients Between Groups.
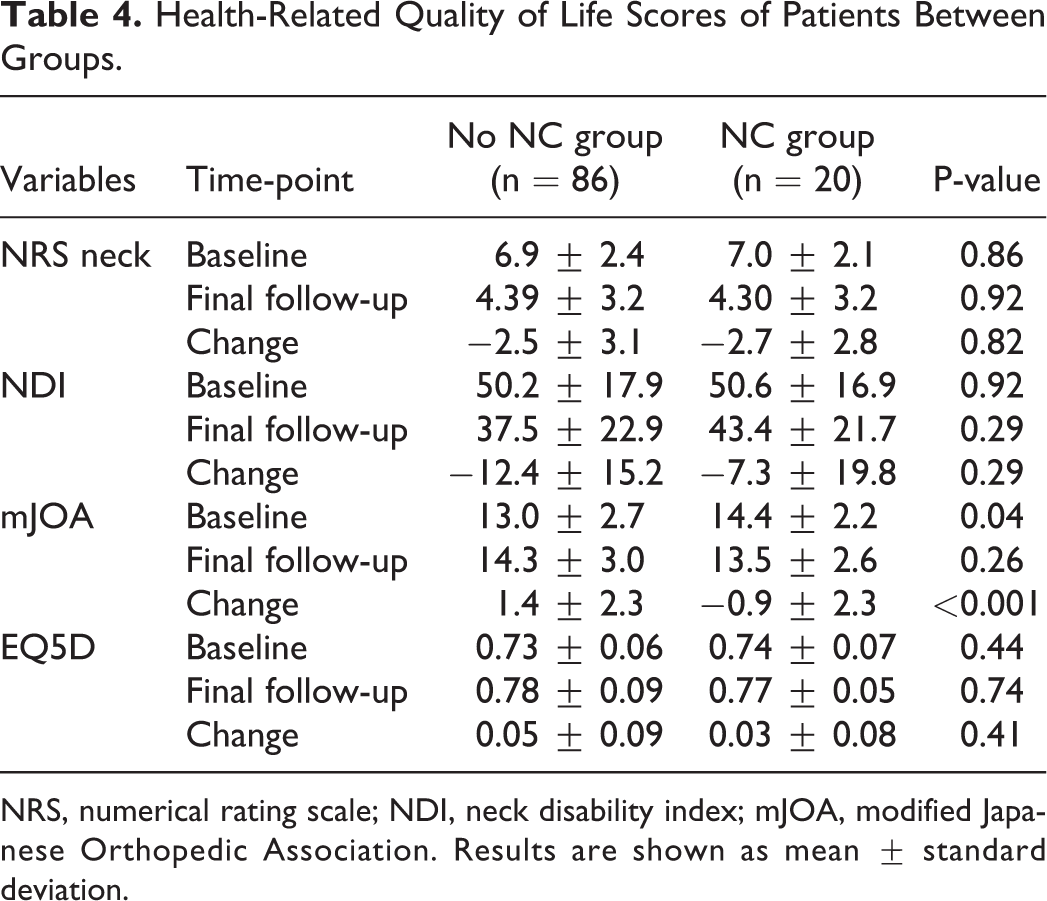
NRS, numerical rating scale; NDI, neck disability index; mJOA, modified Japanese Orthopedic Association. Results are shown as mean ± standard deviation.
Other Complications (Non-Neurologic) and Reoperations
There were 107 complications, other than neurological complications, identified in 57 patients. The types and rates of other complications between the NC and non-NC group were similar (Table 5). There was one death due to deep wound infection. The mortality rate was not significantly different between the 2 groups. Eighteen reoperations occurred in 16 patients. The reoperation rate of the patients due to other complications was 15.1% (Table 5). The reasons for reoperations were not different between the 2 groups. (Table 5)
Other Complications and Reoperations in Patients of the 2 Groups.
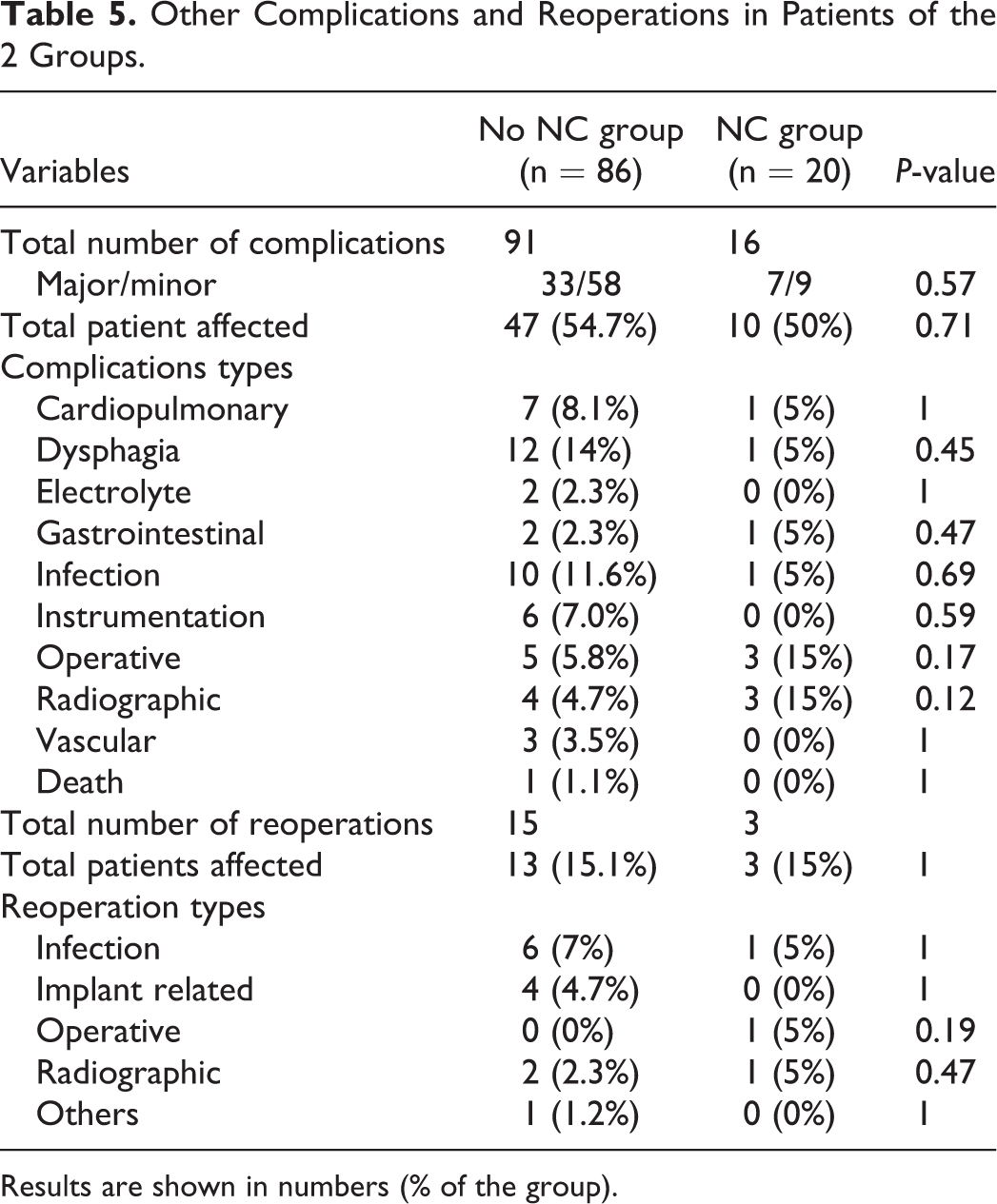
Results are shown in numbers (% of the group).
Discussion
To our knowledge, this is the first large prospective cohort study to report the incidence, timing of occurrence, and recovery patterns of the neurological complications in ACD patients undergoing operative intervention. The overall incidence of the neurological complications was high at 18.9%, and 68.2% of them were major complications. Not all the neurological complications required reoperation, and the reoperation rate of the whole cohort was 3.8%, with only 20% of the neurological complications requiring reoperation. We found that the timing of neurological complications differed according to types. The nerve root motor deficits were frequently identified within 30 days of surgery, whereas the sensory deficit and radiculopathy were frequently identified after 30 days of surgery. The recovery rate from neurological complications was 90.9%. Most of the recoveries occurred in the first 6 months, and the recovery continued even after 12 months from the index surgery. The neurological complication type, timing, and type of intervention were not significantly correlated with recovery. Recent studies also reported a high incidence of neurologic complication. Passias et al. 25 reported a 24.4% mixed surgery- and medical-related neurological complication rate among 123 ACD patients during 1-year follow-up. Koller et al. 23 reported 25% nerve root irritation and 20.9% segmental motor deficit rates among 88 patients at a mean follow-up duration of 26.4 months. However, the timing and recovery pattern were not addressed in both studies. Other studies reported the incidence of neurological complications that ranged from 13.5% to 28.9%,7,20,23-27 and most of them had a retrospective design with a small case number.
Among the risk analysis, we found that there were no demographic or radiographic risk factors of neurological complications. Two surgical procedures were found to be associated with lower rates of neurological complications. The NC group had significantly fewer cases of posterior foraminotomy and anterior corpectomy than the no NC group. One of the possible reasons for this is that most of the neurological complications in our cohort are nerve root related, and the posterior foraminotomy creates adequate nerve root decompression, thereby avoiding iatrogenic foraminal stenosis during correction. Many reports had addressed the importance of prophylactic foraminotomy over C4-C5 and C7-T1 levels in preventing post-operative C5 palsy and C8-T1 radiculopathy in ACD patients.28-31 Although prior studies reported a positive correlation between increasing corpectomy levels and the incidence of C5 palsy,32,33 our result showed contradicting results. One possible reason is the low 3CO rate in patients undergoing anterior corpectomy in our study. In the subgroup analysis of our study, 21 patients underwent anterior corpectomy, and none of them underwent posterior 3CO at the same time (p = 0.006). Another possible reason is that the anterior corpectomy was performed through a distraction force between vertebral bodies, which increased the axial height to increase foraminal height and wide anterior decompression of the anterior dural sac and nerve root. Therefore, the possibility of iatrogenic foraminal stenosis after anterior corpectomy is low, thereby causing less nerve root injury.
Prior studies had reported that patients who had undergone posterior 3CO of cervicothoracic junction had good radiographic and clinical outcomes but they have a high incidence of complications.19,20 Theologis et al. 19 reported an overall complication rate of 60% in ACD patients undergoing 3CO of lower cervical levels. They found that 3CO performed over the upper thoracic levels had a lower complication rate than that performed over the lower cervical levels (27.3% vs. 60%). Smith et al. 20 reported similar results, reporting an overall complication rate of 56.5% 3CO and neurological complication rate of 17.4% among 23 ACD patients who underwent 3CO. In our study, the patients who underwent 3CO had higher neurological complication rates than those who did not (27.3% vs. 16.7%, p = 0.26), but the difference was not significant. This may be because most 3CO procedures were performed over the upper thoracic level (90.9% over T1-T4). This could also be attributed to the level of experience among the participating surgeons in our study.
The surgical approach types had been reported to be correlated with overall complications.22,24,26,34 Grosso et al. 22 reported that the combined approach had the highest complication rate than the ventral-only approach in the cervical kyphosis population. The ventral-only approach also had better neurological outcomes in terms of mJOA scores than the combined approach. Smith et al. 26 also reported a higher early complication rate in combined and posterior approaches than in the anterior approach. The possible reasons may be due to the substantially longer surgical time, greater magnitude of cervical alignment (cSVA), a higher number of fusion levels, and greater magnitude of correction for combined approaches. However, there was no difference in the new onset of neurological complication between the approaches. 26 In the present study we found similar results, in which the risk of neurological complications was not increased in the different surgical approaches.
The other surgical factor that was significantly different between the NC and no NC groups is steroid use. Our study showed that perioperative steroid use was more common in the NC group. Although there had been no established evidence showing that perioperative steroids could protect the nerve injury from surgery,30,35 45.3% and 70% of patients still received steroids in the no-NC and NC groups, respectively. Another significantly different surgical outcome is the length of hospital stay; patients with neurological complications had a longer length of hospital stay than those without such complications. Additionally, we did not find any differences in the HRQOL outcome in NRS, NDI, mJOA and EQ5D scores at the final follow-up. However, the NC group had a worse neurological outcome in the mJOA scores at the final follow-up than at baseline. This is because these patients did not have complete recovery from neurological complications. Two and 6 patients had no recovery and partial recovery, respectively, from neurological complications.
The prospective multi-center design of our study increases the generalizability of the result and ensures the capturing of any new neurological complications to reflect their true incidence. With proper understanding of the types and incidence of neurological complications, we can more accurately identify modifiable preoperative risk factors. We reported 2 surgical protective risk factors, although the mechanism of the posterior foraminotomy and anterior corpectomy and its association with post-operative neurological complication was still unclear. One should consider performing these procedures in suitable patients to minimize the risk for neurological complications. Further studies comparing specific risk factors and clarifying their associations with complication types and recovery patterns may help better understand the correlation in individuals with different cervical deformities.
The present study does have some limitations. First, we did not report the grading of motor deficits. The recovery from motor deficits could not be evaluated, and the comparison with preoperative neurological status could not be performed. Second, the included cohorts were those who underwent surgeries performed by experienced deformity surgeons in specialized institutions. Therefore, our results should be interpreted with caution when applied to cervical deformity surgeries in general.
Conclusion
The incidence of neurological complication was 18.9%. The recovery rate from neurological complication was high, with most of the recovery occurring within 6 months and continuing even after 12 months. Only 1.9% of patients had continuous neurological complications. Among patients with neurological complications, the neurological outcome worsened, but the HRQOL outcome was not different compared to those of the patients without neurological complications. Our study data is valuable to surgeons and patients to help them become more aware of details about the neurological complications before performing or undergoing aggressive surgeries.
Footnotes
Authors’ Note
Institutional Review Board approval for all participating institutes:
Baylor All Saints Medical Center at Fort Worth, TX, US, BRI IRB No. 096259
Rocky Mountain Hospital for Children, Presbyterian St Luke’s Medical Center, Denver, CO, USA. HCA-HealthONE IRB No. 325368-10
Hospital for Special Surgery, NY, NY, US, IRB No. 2014-373-CR2
Johns Hopkins Medicine, Baltimore, Maryland, US, IRB00084730/CR00012716
The University of Kansas Medical Center, KS, US, KUMC IRB No. 13226
Scripps Green Hospital and Scripps Memorial Hospital La Jolla, CA, US, IRB-14-6468
University of California, Davis, CA, US, IRB No. 463372-6
University of California, San Francisco, CA, US, IRB No. 12-08855
NYU School of Medicine, NYU Langone medical center, NY, US, IRB No. i12-02939
University of Virginia Health Sciences Center, Charlottesville, VA, US, HSR IRB No. 16273
Washington University in St. Louis, St. Louis, MO, US, IRB No. 201204137
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the International Spine Study Group foundation; Yu-Cheng Yao was supported by Taipei Veterans General Hospital—National Yang-Ming University Excellent Physician Scientists Cultivation Program, No. 108-V-A-010.