
Abstract
Study design
Prospective cohort study.
Objectives
Treatment for thoracolumbar (TL) burst fractures in neurologically intact patients remains controversial. The goal of this study was to utilize the international equipoise to determine whether surgery leads to a more rapid improvement of disability measured by minimal clinically important difference (MCID) in Oswestry Disability Index (ODI).
Methods
The primary endpoint was time to achieve an improvement in ODI of more than 12.8 points within 1 year after baseline (MCID). A post hoc analysis was conducted to assess time to minimal disability (ODI of <20). Time-to-event analyses were applied, including log rank test for equality of survivor functions, Kaplan Meier survival curves and Cox proportional hazard models.
Results
One hundred and ninety-eight patients were included (122 surgical and 76 non-surgical patients). Median time to achieve MCID in ODI (12.8 points) from baseline was similar between the two groups (25.0 days vs 25.5 days, P = 0.517). Post hoc analysis showed a potential trend towards a short time to achieve minimal disability for the surgical group (69.0 days vs 82.0 days, P = 0.057). Similar results were obtained when excluding all patients with suspected PLC injury.
Conclusion
Surgically and non-surgically treated patients with thoracolumbar burst fractures without neurological injury were similar in terms of time to reaching MCID in ODI at 1 year. Surgical patients may reach minimal disability faster than nonsurgical patients, but additional large scale studies are warranted.
Level of Evidence
Therapeutic Prospective Comparative Cohort Study Level II.
Introduction
Thoracolumbar trauma is a common pathology with significant burden to patients and society.1-3 Thoracolumbar (TL) ‘burst’ fractures are classified as compression injuries with failure of anterior structures corresponding to type A according to the AO Spine TL Classification System. 4 Many studies have attempted to determine what is the best treatment for TL burst fractures without neurological deficits: surgery vs nonoperative management.5-10 Studies have produced mixed and inconclusive results. Additionally, there is worldwide lack of consensus on best management with the opinions of expert being divided across the globe. Different schools of thoughts exist internationally with advocates for surgical management and others for nonoperative management. A critical knowledge gap persists within the spinal surgery community that warrants further investigative efforts. Proponents of non-surgical care, adopted widely in North America, have cited costs and adverse events associated with surgery.10-13 Surgical advocates, prominent in Europe, report improved radiographic alignment and a more rapid return to normal activity with surgery.9,14,15
Among the members of the AO Spine Trauma and Infection Knowledge Forum, an international network of spine trauma centers committed to collaborative prospective multicenter research, we recognized that a true state of equipoise exists wherein “there is genuine uncertainty within the expert medical community about the preferred treatment” of thoracolumbar burst fractures.16,17
As with many acute traumatic injuries, the objective of treatment should be to return patients to their pre-injury state of health and function as quickly as possible. These fractures occur in the working years of life and are associated with significant costs to both the individual and to society.3,18,19 Reaching international consensus on best treatment is primordial.
The main objective of this study was to utilize the existing international equipoise to determine whether surgery leads to a more rapid improvement of disability measured by minimal clinically important difference (MCID) in Oswestry Disability Index (ODI). We hypothesized that surgery would achieve a more rapid improvement within 1 year following baseline ODI than non-surgical care.
Methods
Study Design
Data was taken from a observational, prospective multicenter cohort study comparing surgical vs non-surgical treatment of TL burst fractures in neurological intact patients. All participating patients provided consent for the procedure and enrolment. Each enrolling center obtained local approval from their local institutional review board (UBC CREB NUMBER: H16-02527). The study included neurologically intact patients between 18 and 65 years of age with an acute (<10 days from injury) traumatic fracture between T10 - L2 inclusive where the fracture met the criteria of an AO Type A3 or A4 burst fracture. 4 Patients were included based on the primary injury fracture type (A3 or A4) and data regarding the suspicion of Posterior Ligamentous Complex (PLC) injury was also collected. Patients with other significant distracting injuries or unable to understand or report outcomes were excluded. Patients with pathologic processes such as osteoporosis or neoplasia, previous surgery or polytrauma were excluded.
Study sites were selected based upon their recruitment ability with a view of geographic and treatment diversity. The 14 study sites represented North America (6 sites), Europe (5 sites), and 1 site each in India, Middle East and Australia. Patients from India were classified as Asians while patients from the Middle East were classified as Caucasians.
Primary endpoint was defined as group differences in achieving minimal clinically important difference (MCID) in Oswestry disability index (ODI). MCID in ODI was defined as 12.8 points improvement within 1 year relative to the baseline ODI value. 20 In a post hoc analysis, we defined improvement in ODI as reaching minimal disability within 1 year (ODI of <20). 21 Baseline ODI was assessed at discharge or at 2 weeks post-treatment whichever was earliest. ODI was then assessed every 2 weeks until 6 months, then every 2 months till 2 years.
Secondary endpoint were defined as satisfaction, time to return to work and reoperations. These outcomes were collected at discharge, 6 weeks, 3 months, 6 months, 1-year and 2 years.
Treatment
The surgical/non-surgical procedure(s) were per standard of care at each institution and at the discretion of the treating surgeon. Non-surgical treatment was defined as pain management, early mobilization or bed rest if deemed necessary by treating surgeon with or without external immobilization. External immobilization included thermoplastaic removable brace, Jewett hyperextension brace, anterior hyperextension brace, Taylor-Knight brace, TLSO and other braces for comfort. Surgical treatment included and collected was (1) open long segment posterior fixation (2 levels above, 2 levels below); (2) open short posterior fixation (1 level above and/or 1 level below); (3) percutaneous navigated fixation with or without vertebroplasty; (4) anterior column reconstruction alone or combined anterior reconstruction and posterior fixation.
Statistical Analysis
A sample size calculation was performed on the basis of the log rank test for equality of survival during the first year of follow-up. Survival was defined as not having achieved an improvement in ODI of at least 12.8 points within 1 year after baseline ODI. 20 With an alpha level of 5%, power of 80%, two-sided, an expected dropout rate prior to achievement of the primary endpoint of 15%, an expectation that 25% of patients would not have reached the primary endpoint during 1 year of follow-up in the non-surgical group, and a hazard ratio of 1.6, a sample size of 208 patients with a ratio of 2:1 (ie, 137 surgical group; 71 non-surgical group) was calculated.
Summary statistics were produced for demographics, clinical presentation, injury type fracture classification and Charlson comorbidity score. Categorical variables were summarized with frequence and percentage. For categorical data, chi-square tests or Fisher’s exact tests were applied. Continuous variables were summarized using n, mean, standard deviations (SD), median, lower and upper values of the interquartile range, and minimum and maximum values. T-test or Wilcoxon rank sum test were used to evaluate differences in continuous variables between the treatment groups. Descriptive statistics on the Oswestry Disability Index by treatment were produced for baseline and 1 year after baseline whereas Wilcoxon rank sum test were used to evaluate differences between the treatment groups at these timepoints.
The primary time-to-event analysis included both the log rank test for equality of survivor functions and Kaplan-Meier survival curves. An event was defined as the time the ODI improved by 12.8 points relative to the baseline value or when the patient dropped out whichever occurred first. In the latter case, patients were censored at the date of dropout. Kaplan-Meier survival curves were plotted, and median event times and a 95% CI calculated for each treatment group. The Kaplan Meier curves were compared with the use of a log-rank test. Time at risk started at baseline. Further, univariate and multivariable Cox proportional hazard models were fitted using the Wald test to compare the treatment difference between the surgical and nonsurgical groups expressed as hazard ratios. The multivariable Cox proportional hazard model was adjusted for prespecified markers, namely gender, age, ODI at discharge and injury type. We tested the proportional hazards (PH) assumption in all multivariable Cox models using time-dependent covariates and Schoenfeld residual-based methods. Patients with missing ODI value at baseline or a baseline ODI value lower than 12.8 points were excluded. Analysis were performed for the entire cohort as well as with exclusion of patients with suspected PLC injury.
In an post hoc analysis, improvement in ODI was defined as achieving minimal disability (ODI of <20). 21 Similar to the analysis of the primary outcome, a time to event analysis included both the log rank test for equality of survivor functions and Kaplan-Meier survival curves. Adjustment within a multivariable Cox proportional hazard model was also done for gender, age and injury type. Patients with missing ODI values at discharge were also excluded.
Statistical significance was set at P = 0.05 and the hypothesis tests were two-sided. All analyses were performed using SAS Software version 9.4.
This study was conducted in accordance with the ethical principles set forth in the International Council for Harmonisation Good Clinical Practice (ICH GCP) guidelines, the European Standard EN ISO14155/2003-2011. Written informed consent was obtained from all patients and data was managed by the AO Innovation Translation Centre (ITC) [https://www.aofoundation.org/innovations/Innovation-Translation] in its capacity as the clinical research organization. The study was registered at ClinicalTrials.gov (NCT02827214).
Results
Population Baseline Characteristics
Fourteen centres recruited a total of 215 patients of whom 198 patients were enrolled, eligible and without protocol deviations (Figure 1). One hundred and twenty two (62%) patients were treated surgically and 76 (38%) treated non-surgically. Thirty five patients (18%) were lost to follow-up by the 1 year visit, 19 of them were surgically treated. Participant Recruitment, Follow-up, Inclusions and Exclusions Flowchart for the per Protocol Population With Follow-up at 1 Year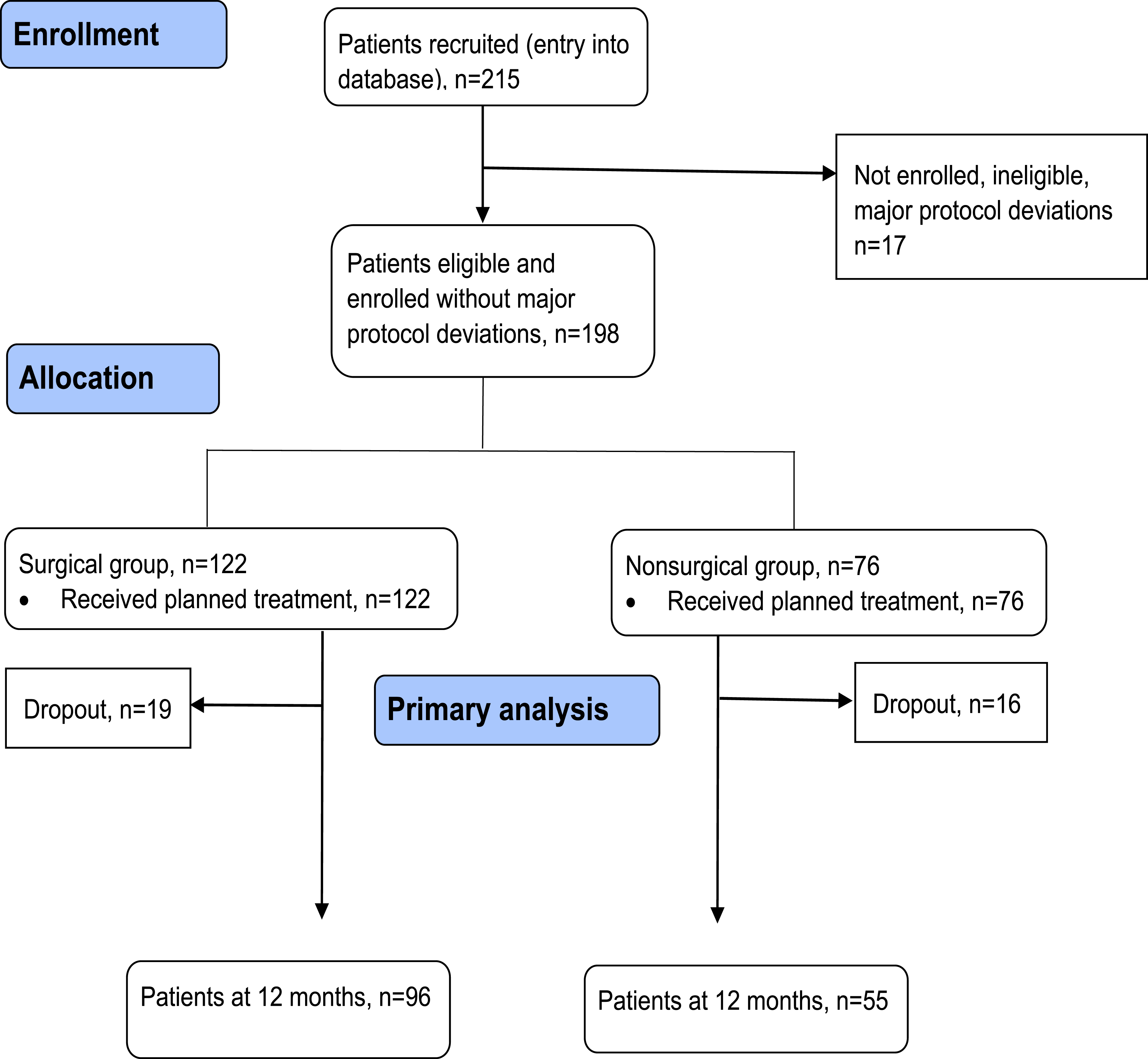
Summary of Patient Characteristics Categorized by Surgical and Non-surgical Treatment. This Table Excludes Patients Who did not Meet Eligibility Criteria or were not Treatment Compliant (per Protocol Population)
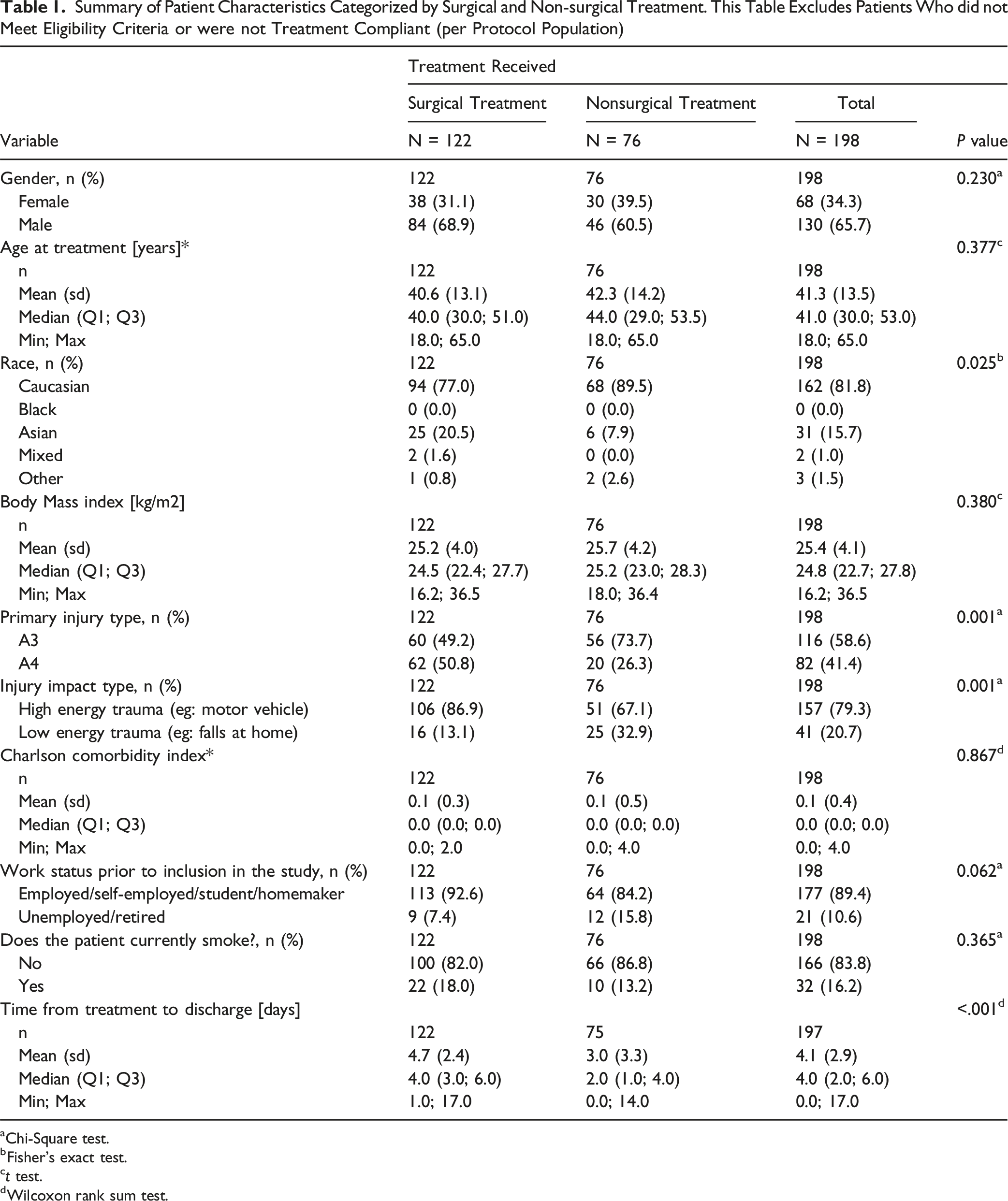
aChi-Square test.
bFisher’s exact test.
ct test.
dWilcoxon rank sum test.
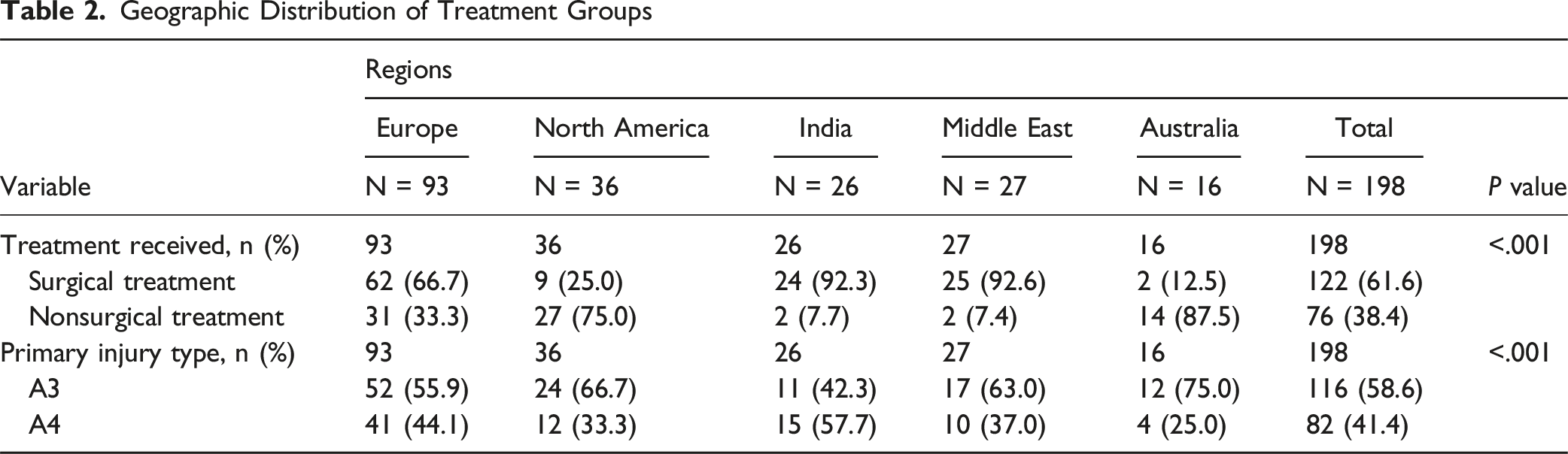
Geographic Distribution of Treatment Groups
The majority of the surgical patients in this cohort were treated via posterior fixation approach (88.6%). Specifically, 64.8% of patients received open short segment posterior fixation, 16.4% received posterior percutaneous fixation and lastly, 7.4% received open long segment posterior fixation. Only 11.5% received other types of techniques.
Primary Outcome
Oswestry Disability Index at Baseline and 1 Year, Achievement of Improvement in ODI of the MCID (12.8 Popints) Within 1 Year After Baseline by Treatment (per Protocol Population)
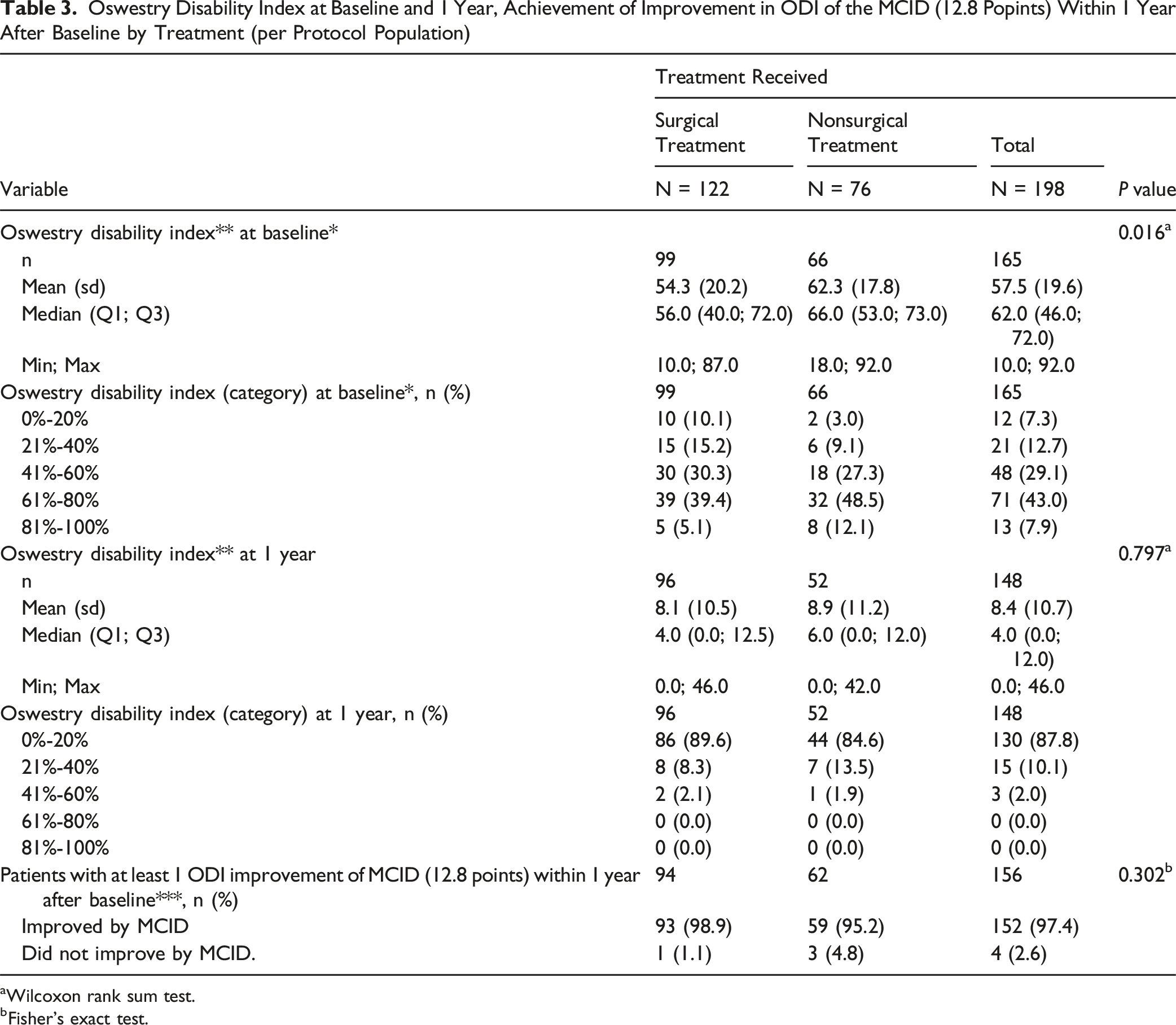
aWilcoxon rank sum test.
bFisher’s exact test.
Minimal Clinically Important Difference (MCID) in Disability (ODI) One Year After Treatment
Kaplan meier curve analyses showed no difference in the median time to achieve MCID in ODI between operative and nonoperative paitents (25.0 days (95% CI: 14.0; 28.0) vs 25.5 days (95% CI: 17.0; 31.0), P = 0.517). When applying multivariate Cox proportional hazard model, the chance in achieving improvement in ODI was similar between the groups (1.40 [95% CI, 0.97; 2.02]) (Figure 2). When excluding patients with suspected PLC injury, Kaplan meier curve analyses showed no difference in the median time to achieve MCID in ODI between operative and nonoperative patients (N = 124 patients, 22.0 days (95%CI: 14.0; 28.0) vs 24.5 days (95% CI: 17.0; 28.0), P = 0.438). When applying multivariate Cox proportional hazard model, the chance in achieving improvement in ODI was also similar between the groups (1.38 [95%CI, 0.93; 2.04]). Kaplan-Meier Plot for Achieving an ODI Improvement of at least 12.8 Points when Compared to the Baseline ODI Within 1 Year (per Protocol Population). Baseline ODI was the First ODI Measurement Taken and Varied From Time of Discharge to 2 weeks Post Injury. Baseline ODI was Day 0. One Surgical Patient had a Baseline ODI of less that 12.8 and Thus Could not Achieve the MCID Improvement and 3 Non-surgical Patients With Treatment Failure Could not Complete the Baseline ODI. These Four Patients Were Censored and not Included in This Analysis. Both the Unadjusted and Adjusted Hazard Ratios including 95% Confidence Intervals for Treatment Differences Were Calculated Using the Wald Test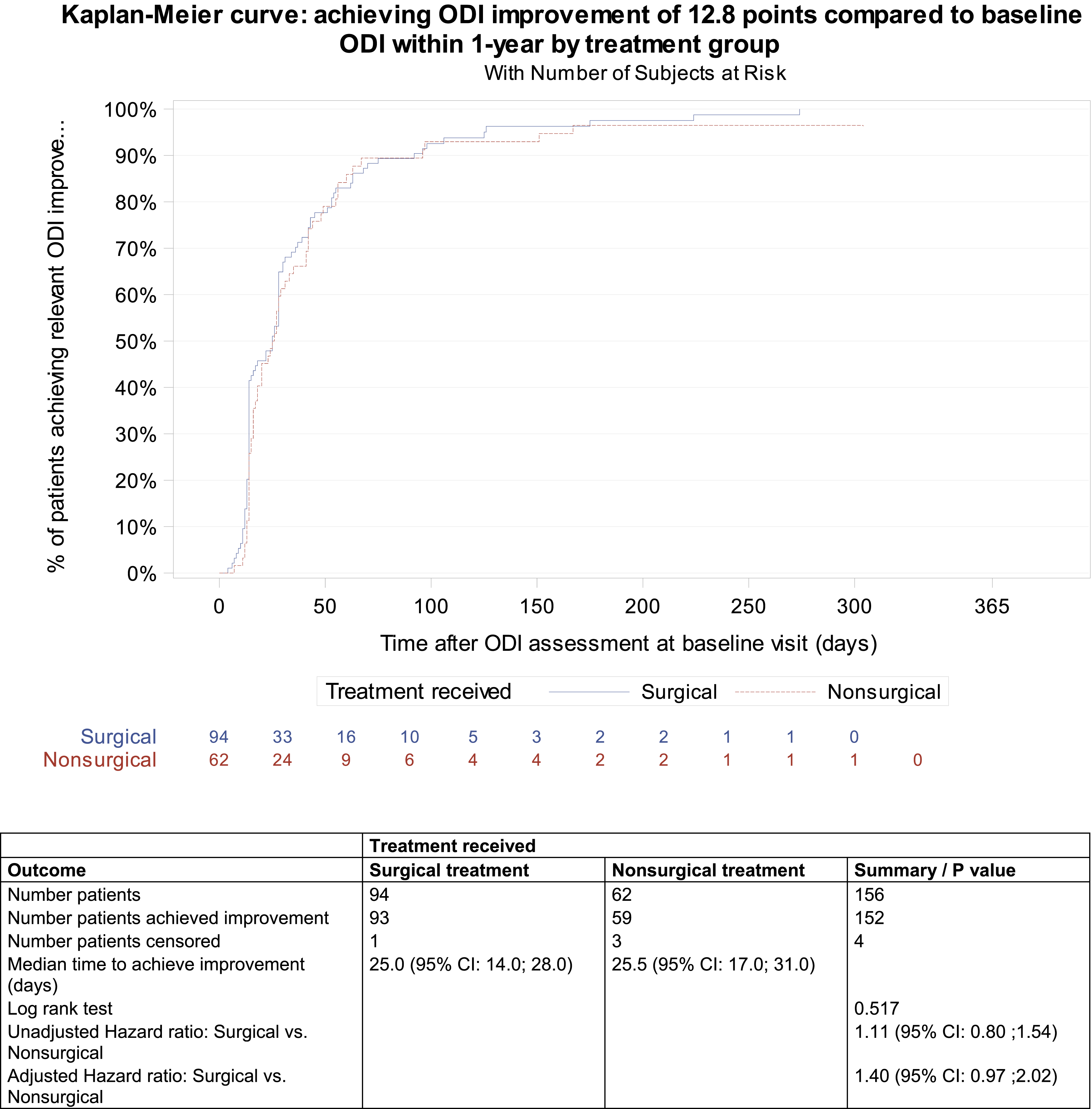
Secondary Outcomes: Satisfaction, Return to Work and Reoperations
Over 80% of all patients were either “extremely satisfied” or “very satisfied” with their treatment at 1 and 2 years after treatment.
The mean time to return to work was shorter for the surgical group, but did not reach statistical difference (90.8 (SD = 69.7) vs 118.7 (SD = 134.6), P = 0.776).
In the non-surgical group, three patients required delayed surgery for intractable mechanical back pain and progressive deformity. In the surgical group, three patients required revision surgery for instrumentation malposition (2) and non-union (1). Three additional patients had their instrumentation removed after healing due to prominence of the implants subcutaneously and local pain. There were no deaths or major complications within the cohort during the follow-up period.
Post Hoc Analysis: Minimal Disability (ODI of Less or Equal to 20) One Year After Treatment
Within 1 year after treatment, 88 out of 99 patients (88.9%) in the surgical group and 53 out of 66 patients (80.3%) in the nonsurgical group achieved an ODI of 20 points or less (defined as minimum disability). The proportions of patients reaching minimal disability was similar between the groups (P = 0.125).
Kaplan meier curves showed a shorter time to minimal disability for the surgical group, but this did not reach statistical significance (69 days (95% CI: 58.0, 77.0) vs 82 days (95% CI: 61.0, 126.0), P = 0.057). When applying multivariate Cox proportional hazard model, the chance in achieving improvement in ODI was similar between the groups (1.39 [95% CI, 0.97; 1.99]).
Discussion
This study provides valuable information in the attempt to solve the ongoing debate regarding best treatment for neurologically intact patients with TL burst fractures. This study is the largest prospective international analysis of TL burst fractures patients. With its unique international perspective, this study presents a global portrait. The results from the primary analysis applying time-to-event methods, revealed no significant differences between surgery and non-surgery in achieving the MCID improvement of 12.8 points in ODI and this finding supports both surgical and non-surgical treatment as equally efficacious in reducing disability as measured by the ODI. Although the nonsurgical patients in our study were more disabled as measured by the ODI at discharge, this difference was not observed 1 year after treatment.
In a geographically diverse and generalizable population, where surgeons where able to treat patients based on often strongly held preferences and local expertise, we have demonstrated that surgical and non-surgical patients achieve similar meaningful improvements in their disability through the first year after injury. Centres with strong preferences for either surgical or non-surgical care were selected based upon the self-declared predilection of the local site investigators. This created an ideal environment of equipoise whereby a surgeon who is committed to surgical treatment will do so for over 90% of patients at that site, whereas, similarly committed non-surgical sites treat the majority of their patients non-surgically.16,17 Differences in baseline characteristics are explained by the geographic diversity in treatment selection. Nonoperative patients had a greater proportion of Caucasian patients and were more concentrated in North America and Australia. The operative patients had a greater proportion of Asian patients and were more concentrated in India and Middle east.
We observed that patients with more comminuted A4 fractures (complete burst) were more often treated surgically. The patients with less comminuted A3 fractures (incomplete burst) were more often treated nonoperatively. This illustrates the perceived increased biomechanical instability with A4 fractures, which are more communited and have both endplates fractured compared to A3. Many surgeons perceive A4 fractures to be at more severe risk of heigh loss and progressive kyphosis. Future studies should aim at delineating the differences in outcomes between A3 and A4 as most studies have produced mixed and inconclusive results. 5
Given the different care pathways, we observed that the baseline ODI measurement was collected at an earlier time point from injury in the non-surgical group. The nonoperative group had a greater level of disability at baseline. This may have translated into non-surgical patients being more likely to achieve their MCID improvement of 12.8 points given that the baseline ODI for nonoperative patients was at alower value. However, ultimately, there was no difference between the groups.
This study highlights a persistent challenge in spinal trauma research where we lack validated outcomes. Paramount to the impact of studies is the outcome measure chosen to evaluate the superiority of one treatment strategy over another. This study highlights the necessary future work required by the spinal trauma research community. It is crucial to develop a validated outcome measure in spinal trauma as ODI has been developed for chronic low back pain and has not been validated in this trauma population. In trauma, there is lower incidence of back pain after the acute phase vs worsening in degenerative back pain. The emphasis of this tool may be misplaced in the long term. Furthermore, the MCID for this tool may not be transferrable from the back pain population to this trauma population. 22 Assessing the treatment effect in spinal trauma remains a challenge given the lack of validated instruments and the nature of the acute traumatic event. With no direct measure of preinjury health status other than relying on patient recall and no validated baseline measurement of disability in the acutely injured spine trauma patient, investigators must focus on improving the methodology for reliably assessing recovery from these injuries. 23 Thus, future studies should focus on solving this ongoing challenging of outcome selection in spinal trauma.
A post hoc analysis identified the potential for surgical patients potentially improving more rapidly from the disability related to their spinal column injury however this has ultimately not reached statistical significance. When performing an analysis of the time to achieve minimal disability (ODI < 20), the adjusted cox proportional hazard ratio of 1.39 (95% CI: 0.97; 1.99, P = 0.057) indicates that surgically treated patients may be more likely to achieve a faster improvement than non-surgically treated patients. This supports future efforts in creating a validated outcome measure tool for future studies in spinal trauma, which will allow researchers to quantify the acute loss of functioning and which treatment returns a patient more rapidly to its pre-injury functional status.
While this study provides valuable insight, its results have to be interpreted in light of its study design. Treatment allocation was at the surgeon’s preference and was non-randomized, which may introduce selection bias. These bias can be inherent in observational cohort studies. Treatment selection may also be influenced by cultural, geographic or sociodemographic factors. 24 However, randomization in spinal trauma with established schools of thought existing worldwide regarding operative vs nonoperative management faces challenges such as fear of receiving or providing suboptimal treatment, need for urgent decision-making, inability to blind and difficulty with patient’s accrual. With established local expertise, a high risk of crossover is possible. The international site selection distributed across North America, Europe, India, Middle East, and Australia enhances the generalizability of the results. This study produces a unique global portrait of international practices. It illustrates the ongoing lack of consensus worldwide and confirms the need for future studies. Furthermore, unknown remains in terms of diagnostic, interpretation and treatment decision in relation to the PLC in spinal trauma.25-27 With the current state of evidence, there is lack of consensus regarding standard imaging algorithms indicative of PLC damage, which limits imaging evaluation of PLC.25-27 We aimed to represent a real-world cohort where the regular use of MRI faces many financial constraints, availability, imaging time and safety in polytraumatized patients around the world. Those global challenges are illustrated by the small proportion of patients who received a pre-treatment MRI in our study (N = 39 patients, 19.7%). The major injury type (A3 and A4) guided inclusion and data was collected regarding the suspicion of PLC injury. Future investigative work is necessary to solve the diagnostic challenges for PLC injury in spinal trauma. ODI, similarly to other patient reported outcomes, are subjective by nature and can be affected by mood, expectations, time and sentiments. External factors may also come into play with treatment context, interactions with healthcare providers and patient’s socioeconomic status.
Conclusion
This prospective international analysis presents a unique global portrait and valuable information for the ongoing debate for best treatment of TL burst fractures. Surgically and non-surgically treated patients with thoracolumbar burst fractures without neurological injury were similar in terms of time to reaching MCID in ODI at 1 year. Surgical patients may reach minimal disability faster than nonsurgical patients, but additional large scale studies are warranted. Future investigative efforts should focus on creating a validated outcome tool in spinal trauma.
Footnotes
Acknowledgement
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international Trauma experts. AO Spine is a clinical division of the AO Foundation which is an independent medically guided not-for-profit organization. Study support was provided directly through the AO Clinical Research Network and the AO Innovation Translation Center, Clinical Evidence. We would like to acknowledge Olesja Hazenbiller, Brigitte Gallo and Alexander Joeris for their contributions to study development and execution.
ORCID iDs
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma. Study support was provided directly through AO Network Clinical Research.