
Abstract
Study Design
A systematic review and meta-analysis.
Objective
To update the systematic review comparing the outcomes between surgical and non-surgical treatment for thoracolumbar burst fractures without neurological deficit.
Methods
We registered a protocol in PROSPERO (ID: CRD42021291769) and searched Medline, Embase, Web of Science, and Google Scholar databases. Surgical and non-surgical treatments were compared in patients with thoracolumbar burst fractures without neurological deficits. Predefined outcomes at ≥6 months included pain (defined as a visual analog scale [VAS] of 0-100), functional outcomes (Oswestry Disability Index [ODI] of 0-50 and Roland-Morris Disability Questionnaire [RMDQ] of 0-24), and kyphotic angulation.
Results
Nineteen studies involving 1056 patients were included in the analyses. For outcomes at ≥6 months, little to no difference was found in pain VAS score (mean difference, .95 [95% confidence interval {CI}, -6.02 to 7.92]; 827 participants; 15 studies; I2 = 92%), ODI (mean difference, -1.40 [95% CI, -5.11 to 2.31]; 446 participants; 7 studies; I2 = 79%), and RMDQ (mean difference, -.73 [95% CI, -5.13 to 3.66]; 216 participants; 5 studies; I2 = 77%). The kyphotic angulation in the surgery group was 6.35° lower than that in the non-surgery group (mean difference, -6.56° [95% CI, -10.26° to -2.87°]; 527 participants; ten studies; I2 = 86%). The trial sequential analysis indicated all outcomes reached adequate statistical power. The certainty of the evidence for all 4 outcomes was very low. For the analysis of minimally invasive procedures compared to traditional open surgeries, a statistically significant subgroup difference was found for VAS and ODI (P < .01 and P < .04, respectively).
Conclusion
Surgical and non-surgical treatments showed little or no difference in outcomes at ≥6 months. This review provides a conclusion with adequate statistical power by including non-randomized studies. However, non-randomized studies also lowered the certainty of the evidence to a very low level.
Introduction
Thoracolumbar burst fractures are commonly caused by motor vehicle accidents or fall from heights. Axial compression and flexion disrupt the anterior and middle spinal columns. Surgery can theoretically achieve immediate spinal stability, neural decompression, deformity reduction, and earlier physical and social recovery at the expense of surgical complications. 1 Conversely, conservative treatments avoid the additional risks of surgery-related morbidities at the expense of a longer recovery.
Although surgery is unequivocally adopted for those with neurological deficits, the superiority of either of the 2 approaches remains unanswered for those without neurological deficits. The first systematic review to seek an answer was in 2006, 2 updated by Abudou et al in 2013. 3 In the study, a clear conclusion was not possible because only 2 trials with 79 participants were included. 3 The trials were also clinically heterogeneous. 3 Both reviews were confined to randomized studies. When evidence from randomized studies is insufficient to provide an answer, it is suggested that non-randomized studies should be included and analyzed. 4 To the best of our knowledge, no further randomized trials have been published since then. Therefore, no further systematic reviews have been published.
Given that the controversy surrounding this topic has persisted for over a decade without resolution, it is imperative to conduct an updated analysis that includes non-randomized studies. Therefore, the purpose of our systematic review was to compare the outcomes of surgical and non-surgical treatment for thoracolumbar burst fractures without neurological deficit. Our review adhered to the PRISMA-2020 guidelines to ensure rigorous methodology and reporting. 5
Methods
Definitions and Search Strategy
All data are available in the article and Supplementary Material. The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42021291769) 6 on December 19, 2021, to guide the study process.
Full details regarding definition, time of assessment, and outcome measurement are available online as protocol. 6 The study population included adult patients with a radiologically confirmed acute thoracolumbar burst fracture without neurological deficits. Adults were defined by the age of 18 or above. Acute stage was defined by those within 4 weeks. Burst fractures were defined according to the AO thoracolumbar system as Type A3 or A4, as well as other equivalent systems. Cases without neurological deficits were defined using the AO thoracolumbar system as Type N0 or N1, along with other equivalent systems. Metastatic lesions and osteoporotic fracture were excluded. The intervention was defined as any surgical treatment, percutaneous, or other minimally invasive intervention. The comparator was defined as all supportive measures besides surgical treatment, such as medication and bracing. Finally, back pain was measured using a visual analog scale (VAS) of 0-100 mm. Functional outcomes were assessed using the Oswestry Disability Index (ODI) of 0-50 and the Roland-Morris Disability Questionnaire (RMDQ) of 0-24. The kyphotic angulation was measured in degrees. The timing of the aforementioned outcomes was at 1, 3, and ≥6 months after treatment. The minimal clinically important difference (MCID) of pain VAS, ODI, RMDQ, and kyphotic angulation were defined as 11, 7 7.8, 7 5, 8 and 3.8°, respectively. 9
Subsequently, the concepts of the above definitions were used to formulate a search strategy. We searched Medline, EMBASE, Web of Science, and Google Scholar, as illustrated in Figure 1. The search strategy for each database is described in detail in Appendix 1. No language restrictions were imposed. Data extraction forms (Appendix 2) were used for study inclusion and data extraction to enhance transparency and reproducibility. Automation tools were not used in this study. PRISMA 2020 flow-chart.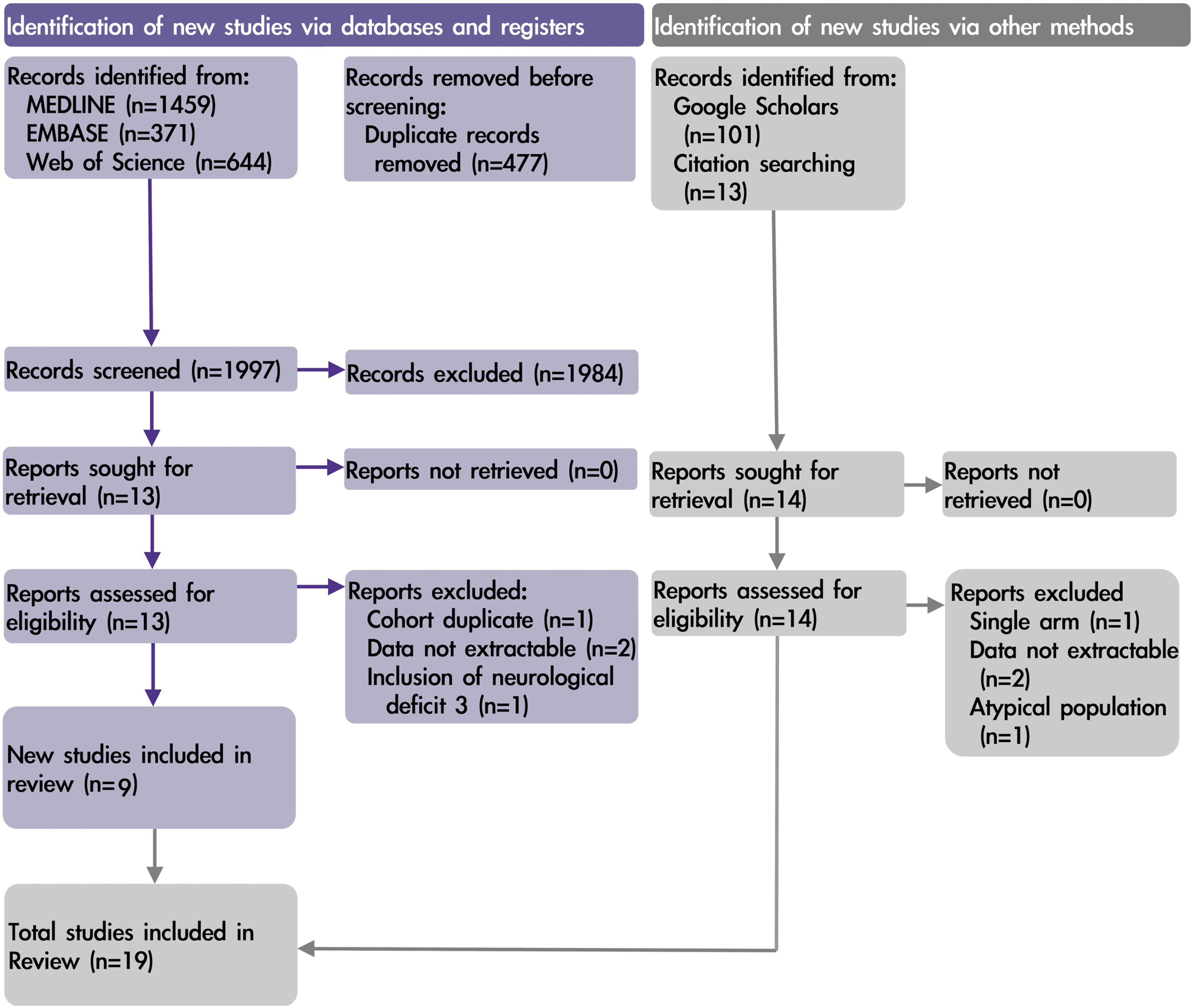
Finding and Assessing Individual Studies
The search was performed in November 2021. Study titles, abstracts, and full texts were independently screened for inclusion by TYC and CLC, and discrepancies were determined by consensus discussions with FYT. Citation searching was performed manually according to the references of eligible studies.
For qualitative assessment, the effect of bias in individual studies was assessed with the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I). 4 The overall judgment for a specific outcome was derived according to the table provided by ROBINS-I (Appendix 3). The certainty of the body of evidence was assessed with Grading of Recommendations, Assessment, Development and Evaluation (GRADE). 10 The bias judgment of ROBINS-I was integrated into the risk of bias domain of GRADE according to an established guideline. 11 Details of GRADE and the integration are described in Appendix 4. TYC and CLC independently assessed all qualitative assessments, and discrepancies were resolved based on consensus with FYT.
Synthesizing the Body of Evidence
A meta-analysis was performed if the data were appropriate for pooling. The summary of estimates of all outcomes was presented as the mean difference. The Hartung-Knapp-Sidik-Jonkman method 12 was used to estimate the heterogeneity variance within the random-effects model. A narrative synthesis was performed if pooling was inappropriate. The R package meta 13 was used for meta-analysis and meta-regression. A Web-based GRADEpro GDT was used for GRADE. Trial Sequential Analysis software 14 was used for power analysis, with an overall type I error of 5% (α = .05) and a power of 90% (β = .9). Conventional definitions were used for 95% confidence interval (CI), heterogeneity (I2 < 40%: unimportant; 30%-60%: moderate; 50%-90%: substantial, 75%-100%: considerable), and P-value (P < .05: significant, and P < .1 for subgroup difference: significant).
Results
Characteristics of Included Studies.
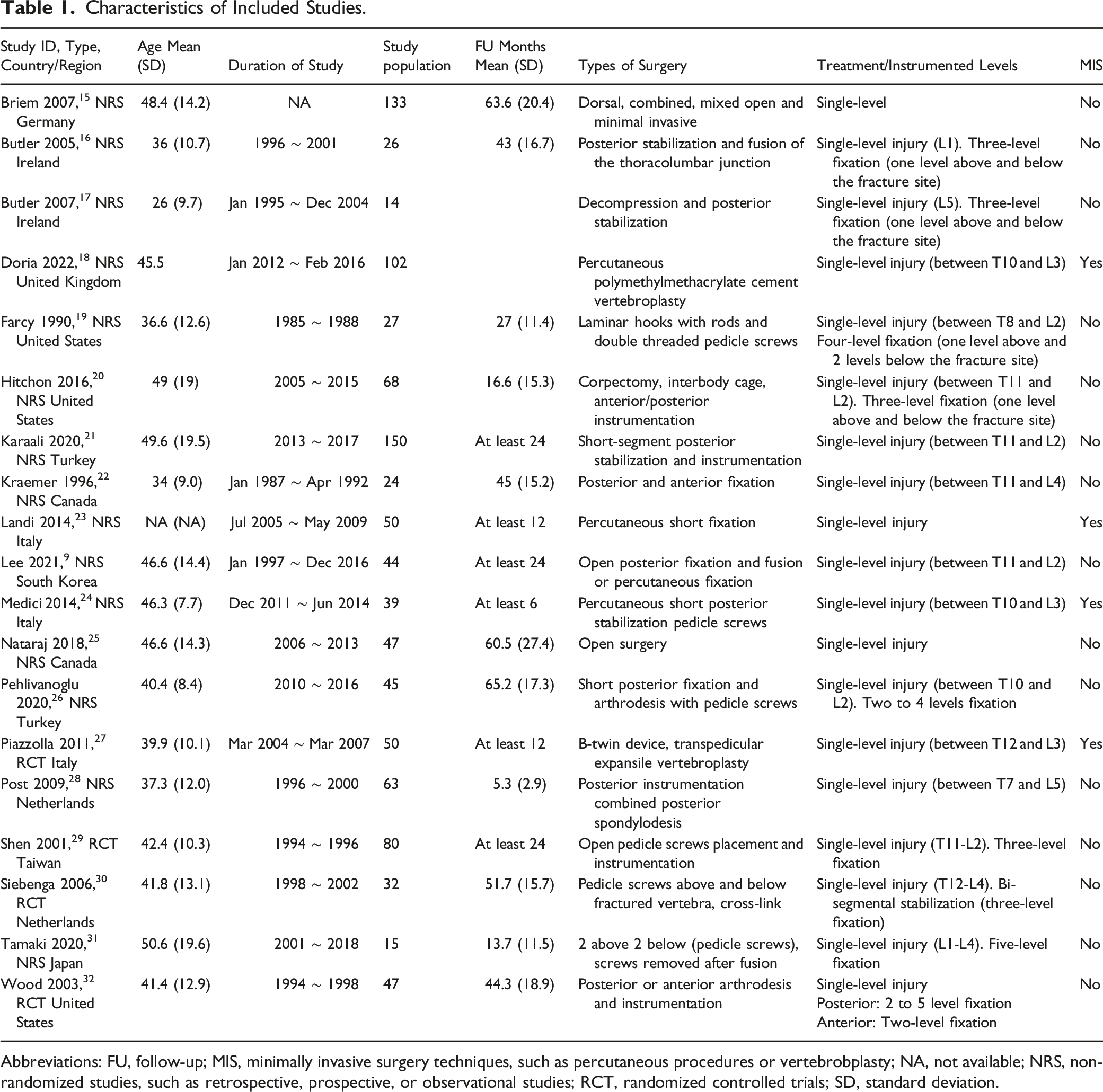
Abbreviations: FU, follow-up; MIS, minimally invasive surgery techniques, such as percutaneous procedures or vertebrobplasty; NA, not available; NRS, non-randomized studies, such as retrospective, prospective, or observational studies; RCT, randomized controlled trials; SD, standard deviation.
Pain in VAS at ≥6 Months
Summary of Findings.
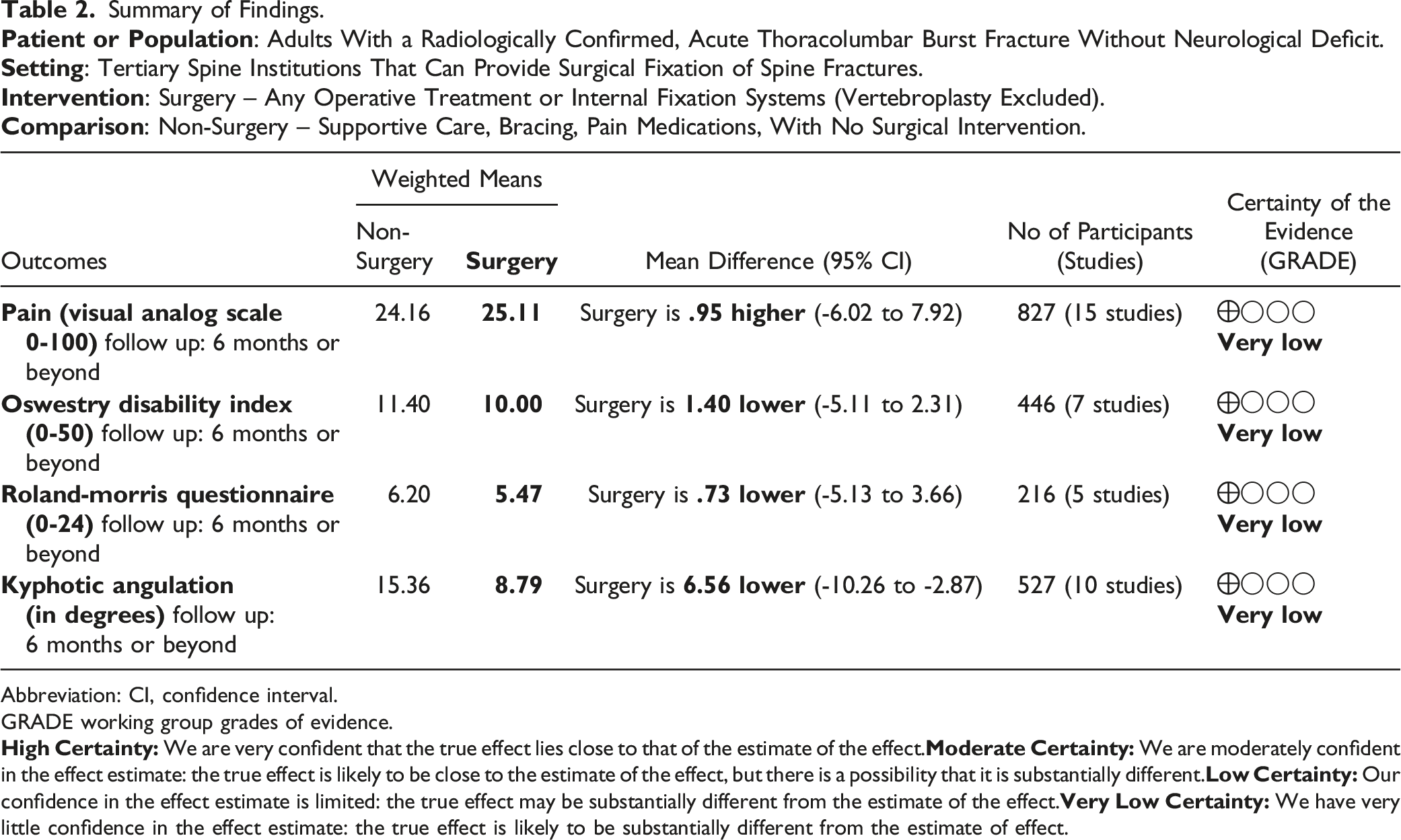
Abbreviation: CI, confidence interval.
GRADE working group grades of evidence.
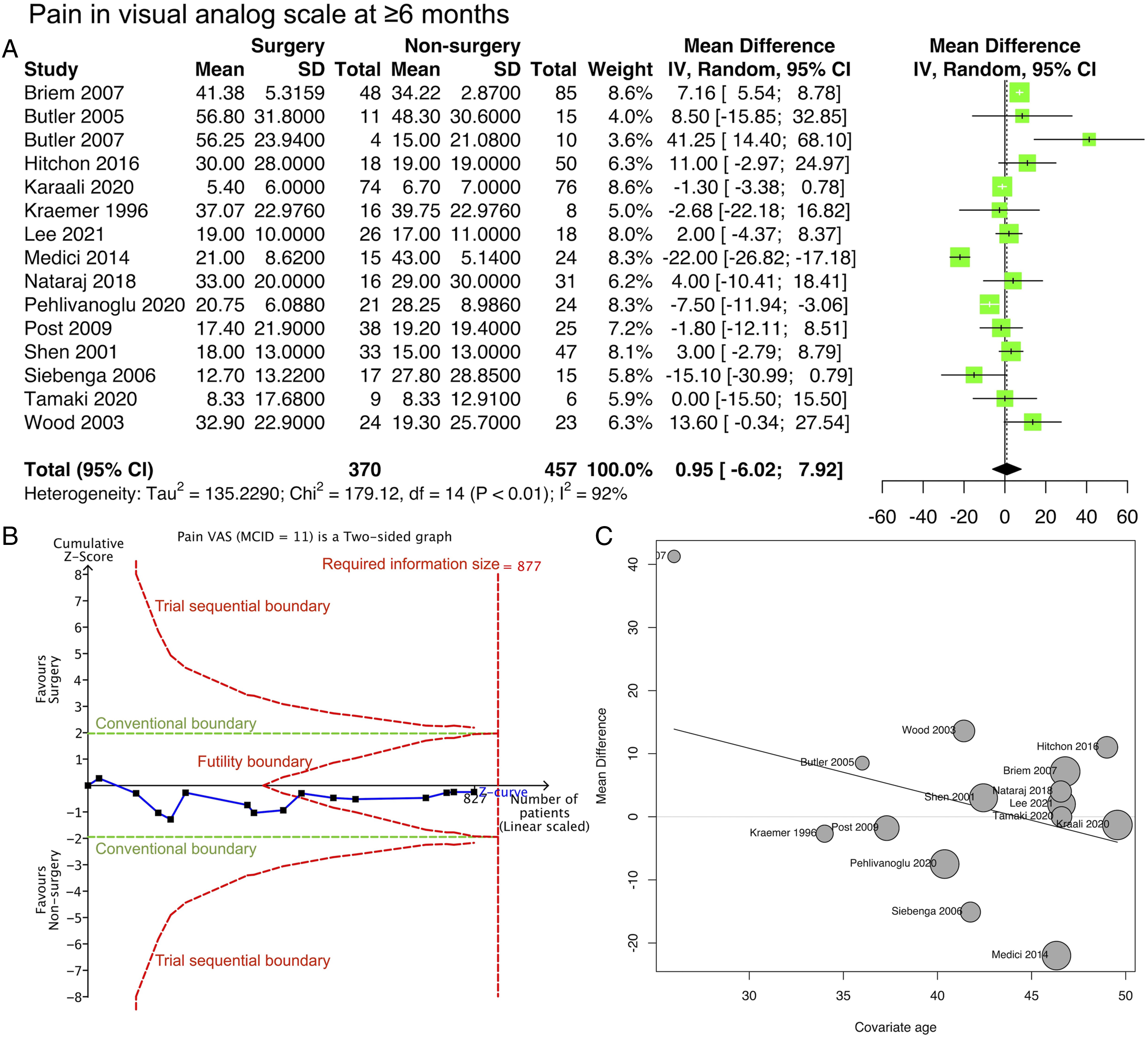
Pain VAS. (A) Forest plot. (B) Trial sequential analysis. (C) Meta-regression with study-level age as the covariate.
ODI at ≥6 Months
Meta-analysis of 7 studies (Table 2; Figure 3A) showed little to no difference in ODI between the surgery and non-surgery groups (mean difference, -1.4 [95% CI: -5.11 to 2.31]; 446 participants; 7 studies; I2 = 79%). The risk of bias was serious according to ROBINS-I (Appendix 3). The GRADE certainty of the evidence was very low (Appendix 4). Trial sequential analysis (Figure 3B) indicated that the number of patients (required information size) was sufficient to determine the similarity between the surgery and non-surgery groups, further supporting the meta-analysis in terms of 90% statistical power. Meta-regression (Figure 3C) suggested that the mean difference between the surgery and non-surgery groups decreased by 5.8 in ODI score for every 10-year increase in mean age at the study level. However, this regression was not statistically significant (P = .237; R2 = 13.9%). ODI. (A) Forest plot. (B) Trial sequential analysis. (C) Meta-regression with study-level age as the covariate.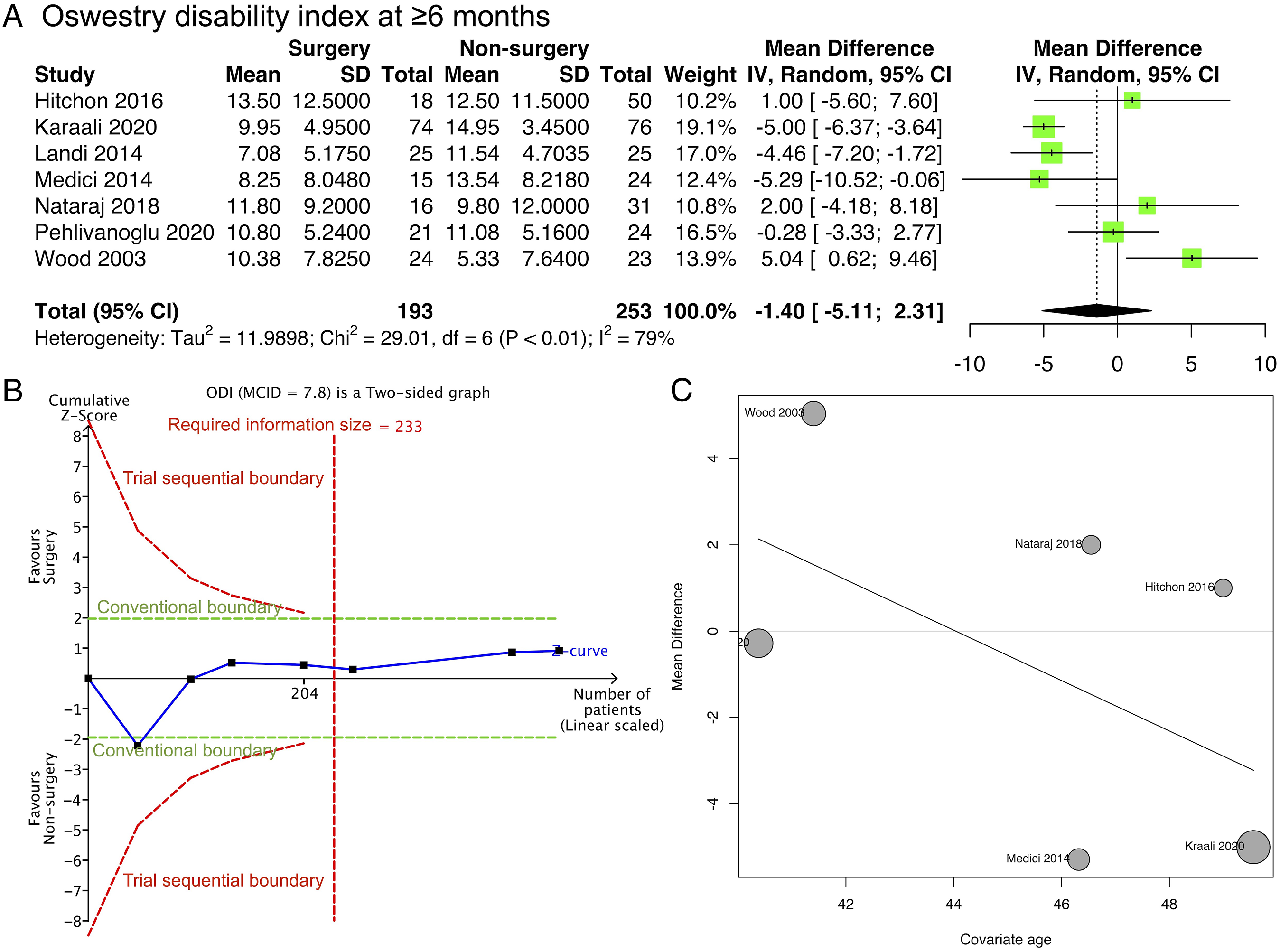
RMDQ at ≥6 Months
Meta-analysis of 5 studies (Table 2; Figure 4A) showed little to no difference in RMDQ between the surgery and non-surgery groups (mean difference, -.73 [95% CI: -5.13 to 3.66]; 216 participants; 5 studies; I2 = 77%). The risk of bias was serious according to ROBINS-I (Appendix 3). The GRADE certainty of the evidence was very low (Appendix 4). Trial sequential analysis (Figure 4B) indicated that the cumulative Z-score breached the futility boundary, indicating a similarity between the surgery and non-surgery groups. Meta-regression analysis (Figure 4C) against mean age was not significant (P = .92, R2 = .00%). RMDQ. (A) Forest plot. (B) Trial sequential analysis. (C) Meta-regression with study-level age as the covariate.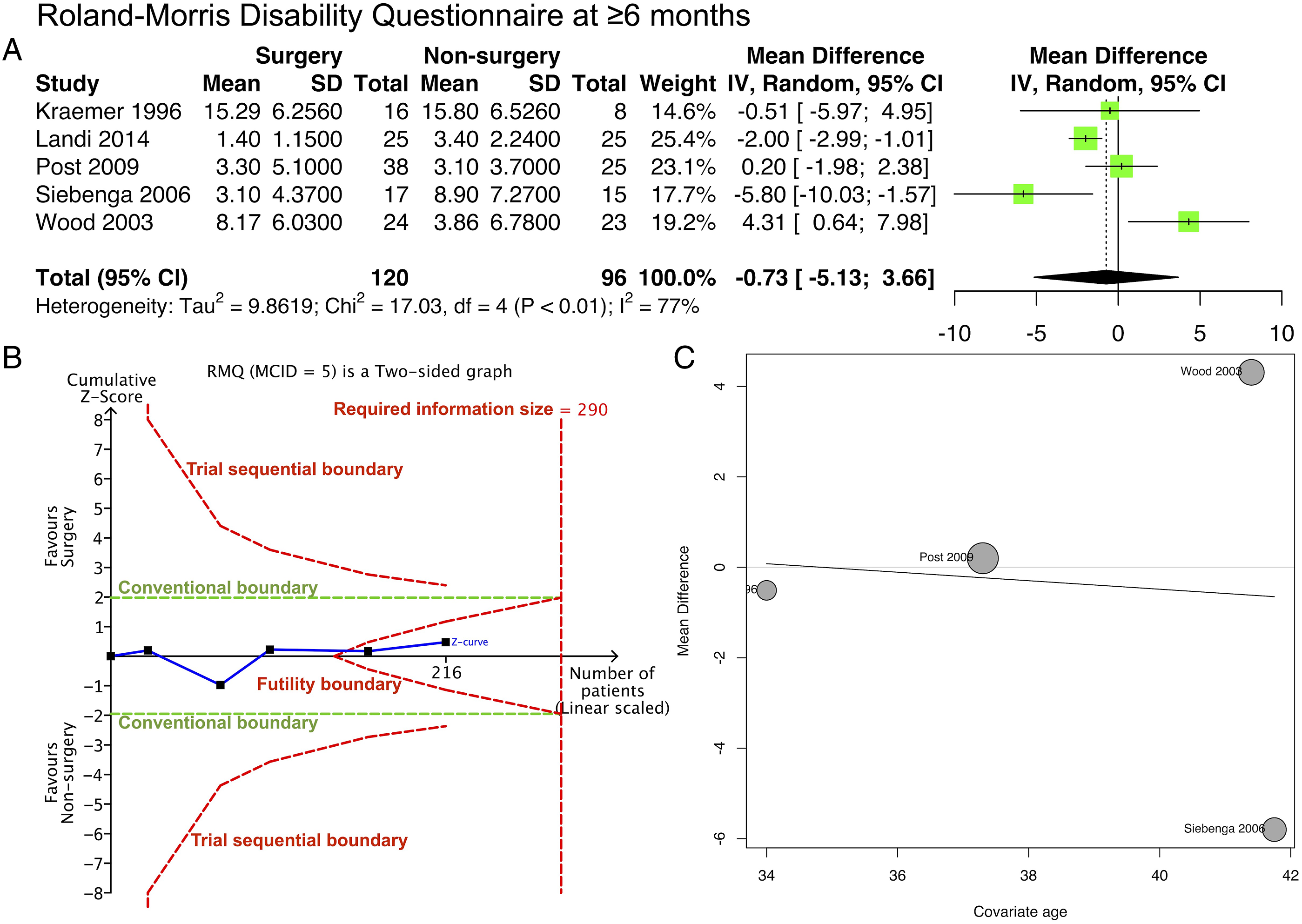
Kyphotic Angulation at ≥6 Months
Meta-analysis of 10 studies (Table 2; Figure 5A) showed that kyphotic angulation in the surgery group was 6.35° lower than that in the non-surgery group (mean difference, -6.56° [95% CI: -10.26° to -2.87°]; 527 participants; 10 studies; I2 = 86%). The risk of bias was serious according to ROBINS-I (Appendix 3). The GRADE certainty of the evidence was very low (Appendix 4). Trial sequential analysis (Figure 5B) indicated that the cumulative Z-score breached the trial sequential boundary in favor of the surgery, further supporting the meta-analysis’s 90% statistical power. Meta-regression (Figure 5C) suggested that the mean difference between the surgery and non-surgery groups decreased by 4.5° for every 10-year increase in mean age at the study level. However, this regression was not statistically significant (P = .227; R2 = 7.92%). Kyphotic angulation. (A) Forest plot. (B) Trial sequential analysis. (C) Meta-regression with study-level age as the covariate.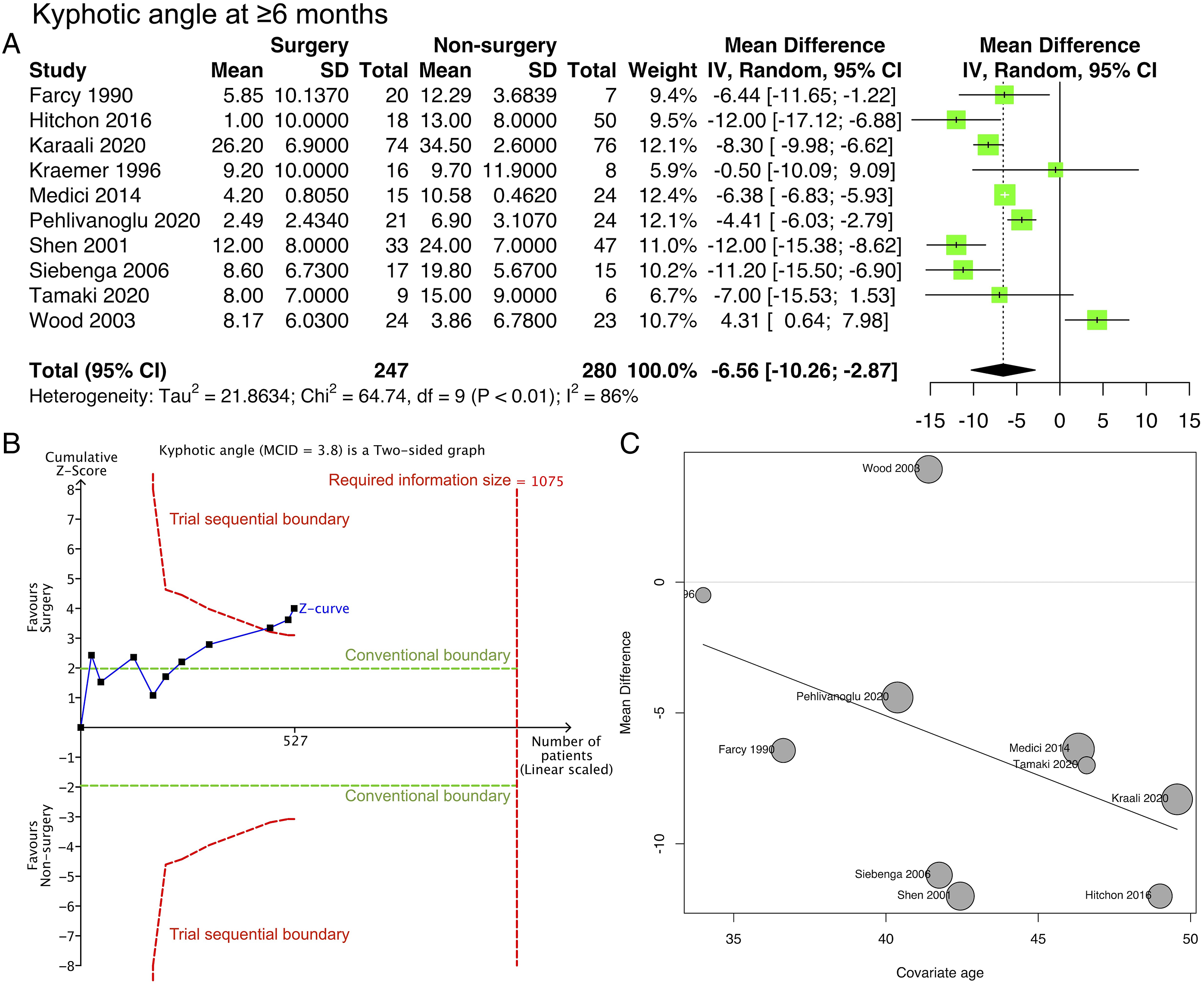
Subgroup Analyses
The presence of randomization and minimally invasive procedures were 2 study characteristics determined a priori to be investigated in the subgroup analysis. For the analysis of minimally invasive procedures compared to traditional open surgeries, a statistically significant subgroup difference was found for VAS and ODI (P < .01 and P < .04, respectively, for subgroup difference; Appendix 8 A1, A2), meaning that minimally invasive techniques may have different and better outcomes than traditional open surgeries. No significant subgroup difference was found for kyphotic angulation (P = .70, for subgroup difference) (Appendix 8, A3). No significant subgroup difference was found for randomized studies compared to non-randomized ones; the P-value for subgroup difference ranged from .29 to .92 for all analyses (Appendix 8, B).
Discussion
In our analysis, the focus was on long-term outcomes of 6 months or longer. Patient-reported outcomes, such as pain and functional outcomes, were found to have little or no superiority in surgery over non-surgical treatments (with very low certainty of the evidence). However, concerning kyphotic angulation, an advantage in surgery over non-surgical treatments was suggested by our analysis, resulting in a 6.35° difference. To determine whether this difference is clinically significant, a predetermined MCID of 3.8° was used. Since there is no widely accepted MCID for this variable, an anchor-based method was employed, as described in a 2021 article by Lee et al, 9 which reported that a difference of 3.8° or higher correlated with clinical outcomes. Upon applying this MCID to our analysis, the confidence intervals of the pooled effect estimate of kyphotic angulation were found to include 3.8°, raising doubts about its clinical significance. This finding is consistent with patient-reported outcomes, pain, and functional outcomes, all of which suggest that surgery has little or no advantage over non-surgical treatments.
Previous meta-analyses3,33 compared surgical to non-surgical approaches but could not draw conclusions. The major reason for this was the small number of studies included: Abudou et al included 2 studies, 3 while Gnanenthiran et al included 4. 33 However, the “absent of evidence” does not mean “evidence of absence.” No between-group differences in pain, kyphosis, and RMDQ, as concluded by Gnanenthiran et al, 33 were most likely the result of an inadequately powered meta-analysis. We included trial sequential analysis as a component of our meta-analysis to ensure that the outcomes were based on adequate statistical power. In contrast to previous studies, this review included 19 studies, and the meta-analysis reached a statistical power of 90%. A more confident suggestion can be made from a quantitative (statistical) perspective.
However, owing to the inclusion of non-randomized studies, the high risk of bias lowered the qualitative implications of this review. Based on the GRADE assessment, the certainty of evidence remained very low. The major bias was inherent in confounding and patient selection, which is inevitable in non-randomized studies. For example, Hitchon et al reported that patients who underwent surgery only after non-surgical measures had treatment failure, mostly due to pain. 20 The participants in the non-surgical arm in the cohort of D’Oria et al and Pehlivanoglu et al were significantly older.18,26 Other factors such as male sex, higher angulation, and a higher proportion of spinal canal compromise are more likely but understandably placed in the surgical group. The effect of age as a covariate on outcomes was evident in the meta-regression bubble plot (Figure 2C, 3C, 4C, and 5C).
This review suggests that surgical treatment is unlikely to be considered a priority because of its low superiority over non-surgical treatment in burst fractures without neurological deficits. Conversely, minimally invasive procedures such as percutaneous transpedicular fixation or vertebroplasty could be beneficial per pain VAS and ODI at ≥6 months. However, it should be noted that the interpretation from subgroup analysis can only be regarded as exploratory instead of causative. Nonetheless, future studies could use minimally invasive techniques, and further analysis is anticipated. It would be noteworthy for surgeons to follow the trend of minimally invasive techniques and utilize their advantages as much as possible. 34
Although statistical significance was not reached, the meta-regression revealed that a higher study-level mean age minimizes the differences between surgical and non-surgical interventions (Figure 2C, 3C, 4C, and 5C). This trend was consistent for all outcomes. Younger patients could have better outcomes after surgery. Whether younger patients benefit more from surgery should be the subject of future investigations.
Although the superiority of surgery is not apparent in the long term, it does not dismiss its role in burst fracture treatment. Together with the aforementioned findings, future studies and clinicians assess the benefits of surgery in younger patients, short-term outcomes, and earlier return to work.
Limitation
Since many of the included studies were non-randomized, the risk of bias was understandably high. Consequently, the certainty of the evidence is very low. Furthermore, the results of meta-regression and sensitivity analyses can only be exploratory.
Conclusion
Surgical and non-surgical treatments showed little or no difference in outcomes at ≥6 months. This review provides a conclusion with adequate statistical power by including non-randomized studies. However, non-randomized studies also lowered the certainty of the evidence to a very low level.
Supplemental Material
Supplemental Material - Surgical Versus Non-Surgical Treatment for Thoracolumbar Burst Fractures Without Neurological Deficit: A Systematic Review and Meta-Analysis
Supplemental Material for Surgical Versus Non-Surgical Treatment for Thoracolumbar Burst Fractures Without Neurological Deficit: A Systematic Review and Meta-Analysis by Tzu-Yi Chou, Fon-Yih Tsuang, Yu-Lun Hsu, and Chung L. Chai in Global Spine Journal.
Footnotes
Author Contributions
Conceptualization: [Tzu-Yi Chou]; Methodology: [Chung Liang Chai, Tzu-Yi Chou]; Formal analysis and investigation: [Chung Liang Chai, Tzu-Yi Chou]; Data acquisition: [Chung Liang Chai, Tzu-Yi Chou, Yu-Lun Hsu]; Writing - original draft preparation: [Chung Liang Chai, Tzu-Yi Chou, Fon-Yih Tsuang]; Writing - review and editing: [Chung Liang Chai]; Funding acquisition: [Fon-Yih Tsuang].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Good Liver Foundation and Taiwan Brain Disease Foundation of Taiwan (MS476).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.