
Abstract
Study Design
Retrospective comparative study.
Objectives
Optimal surgical treatment for low-grade L5-S1 isthmic spondylolisthesis (IS) is still subject of debate. While various surgical approaches exist, anchored stand-alone (SA) ALIF has emerged as a promising alternative technique. This study aimed to compare the efficacy, as well as the clinical and radiological outcomes of anchored SA-ALIF and posterior lumbar interbody fusion in the management of low-grade L5-S1 IS.
Methods
A total of 53 patients, 26 from the anterior group and 27 from the posterior group, met the inclusion criteria. Intraoperative blood loss, operative time, radiation exposure and postoperative length of hospitalization were retrospectively evaluated. Clinical outcomes were assessed using the ODI and VAS scales. Upright lumbosacral X-ray and lumbosacral CT scan were used to evaluate spinopelvic parameters and intersomatic fusion according to Brantigan-Steffee-Fraser (BSF) scale, respectively.
Results
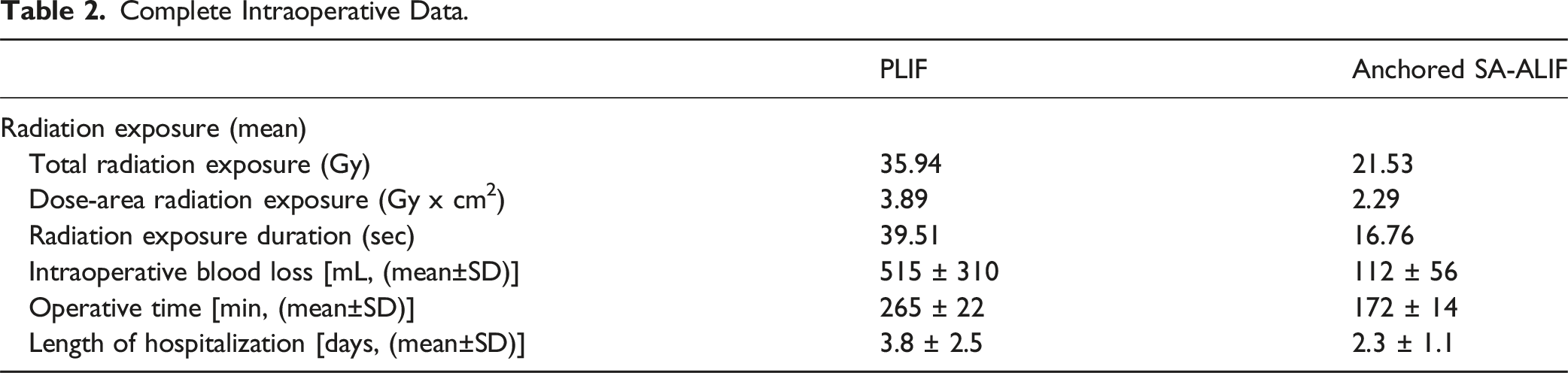
The mean postoperative follow-up was 39 months. Intraoperative blood loss, radiation exposure, operative time, and postoperative length of hospitalization were significantly lower in the anterior group. Effective ODI and VAS improvement was achieved in both anterior and posterior groups. No significant differences were observed between the two groups in postoperative spinopelvic parameters assessment. Effective spinal fusion was achieved in 23 patients (88.4%) in the anterior group, and in 21 patients (77.8%) in the posterior group.
Conclusion
While both techniques effectively achieve spinal fusion and symptom relief, anchored SA-ALIF offers significant advantages over posterior fusion techniques in terms of intraoperative blood loss, radiation exposure, operative time, and postoperative length of hospitalization.
Introduction
Isthmic lumbar spondylolisthesis (IS) is a spinal condition characterized by the forward displacement of one vertebra over another due to a defect or fracture in the vertebral isthmus, most commonly affecting the L5 vertebra and the adjacent segment of the sacrum. Low-grade (grade 1-2) spondylolisthesis refers to a relatively mild form of the condition, with the displacement of the cranial vertebra typically less than 50% of the length of the vertebral body, according to Meyerding classification. 1 Clinical presentation of low-grade lumbar IS heterogeneous, ranging from low back pain and stiffness to radicular pain with eventually neurological deficit. The degree of vertebral slippage and spinal instability often correlates with the severity of symptoms. The anterior displacement of the vertebral body alters the normal alignment of the spine, often resulting in compensatory changes aimed to maintain an upright posture. Over time, these adaptations may lead to muscle fatigue, chronic back pain, and, eventually, reduced functional capacity.
Optimal treatment of low-grade L5-S1 IS still controversial. Surgical treatment is considered when conservative measures like physical therapy, medications, and activity modification fail, or when neurological deficit occur. Common surgical treatment includes several approaches for spinal fusion.2,3 Minimally invasive techniques are increasingly utilized, primarily due to potential benefits deriving from minor tissue damage, quicker recovery time, and consequential reduced need for pain medications compared to traditional techniques. In this context, anchored stand-alone anterior lumbar interbody fusion (SA-ALIF) has emerged as a promising technique, offering distinct advantages in terms of tissue trauma and postoperative clinical and radiological outcome. 4
The existing literature on direct comparison of anchored SA-ALIF with other lumbar intersomatic fusion techniques in the surgical treatment of low grade L5-S1 IS remains limited.5,6 Therefore, the aim of this study is to compare anchored SA-ALIF and traditional open posterior lumbar interbody fusion (PLIF) technique for the management of low grade L5-S1 IS in terms of efficacy, safety, and clinical and radiological outcome.
Methods
This study was conducted following the Guidelines for Good Clinical Practice and the Declaration of Helsinki (2002) of the World Medical Association. Written informed consent was obtained from all the patients for each diagnostic and surgical procedure.
This single-center, retrospective, observational study analyzed prospectively collected data from patients who underwent stand-alone anterior lumbar interbody fusion (SA-ALIF) and posterior lumbar interbody fusion (PLIF) surgery for low grade L5-S1 IS from January 2018 to January 2023. The availability of all preoperative and postoperative radiological and clinical data was mandatory for patient inclusion. Exclusion criteria included previous lumbo-sacral surgery, degenerative spondylolisthesis, lumbar scoliosis, low bone quality (osteopenia or osteoporosis based on endocrinological diagnosis), and body mass index (BMI) > 30.
Study Design
All patients underwent a comprehensive preoperative clinical and radiological evaluation, followed by postoperative follow-ups at 1 month, 6 months and 12 months after surgery. Oswestry Disability Index (ODI) and Visual Analogue Scale (VAS) were used for patient function and pain evaluation, respectively. Preoperative radiological assessments included lumbosacral MRI and upright static and dynamic lumbosacral X-ray. Additionally, lumbosacral CT angiography was performed in all patients considered eligible for anchored SA-ALIF to facilitate detailed preoperative vascular anatomical planning. The degree of spondylolisthesis was evaluated using upright lumbosacral X-ray according to Meyerding classification. 1 Intraoperative assessment included surgical duration, intraoperative blood loss, and radiation exposure in terms of total dose, dose-area product, and exposure time. Postoperative length of hospitalization (LoH) was recorded for all cases.
The PLIF procedure was performed according to the standard surgical technique, using bilateral porous tantalum cages (TM Ardis®, Zimmer) filled with autogenous bone graft harvested locally from bone obtained during decompression maneuvers. All anchored SA-ALIF procedures were performed with the assistance of a vascular surgeon, via a standard median subumbilical-suprapubic incision followed by retroperitoneal approach to the lumbar spine. All anterior procedures were conducted using trabecular titanium cages (Modulus ALIF®, Nuvasive) filled with bone allograft (AttraX Putty®, Nuvasive). Cage implantation in each anchored SA-ALIF procedure was secured with self-locking trans-somatic screws without anterior plating. The decision to proceed with either an anterior or posterior approach for lumbar fusion was individualized and based on several preoperative factors. These included the favorability of the iliac vessel anatomy as inferred from lumbosacral MRI, the sacral slope angle, history of prior abdominal surgery, and patient preference after a thorough discussion of the risks and benefits of each approach.
Postoperative Assessment
Each postoperative follow-up consisted of neurological examination and clinical outcome evaluation in terms of ODI and VAS scores. Early and late complications were defined as occurring during the hospitalization period or after discharge, respectively. Pseudoarthrosis requiring revision surgery, adjacent segment syndrome, intraoperative vascular injury, retrograde ejaculation, wound disorders, and thrombosis were the main postoperative complications considered at each follow-up evaluation.
Postoperative radiological outcome protocol included immediate postoperative and 6-month postoperative upright static lumbosacral X-ray for sagittal balance parameters evaluation. All patients underwent postoperative lumbosacral CT scan for intersomatic fusion assessment at least 12 months after surgical intervention. In all cases, interbody fusion was assessed using the Brantigan-Steffee-Fraser (BSF) classification. 7 Radiographic pseudoarthrosis was defined as collapse of construct, loss of disc height, vertebral slip, broken screw, displacement of the cage, or a visible gap >2 mm in the fusion area. When deemed necessary, the assessment of interbody fusion based on CT imaging was complemented by the evaluation and comparison of postoperative lumbosacral X-rays. Additionally, preoperative and postoperative spinopelvic parameters were evaluated using lumbosacral X-ray. Radiographic sagittal balance parameters included pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), segmental L5-S1 lordosis, segmental L4-S1 lordosis, global L1-S1 lordosis. All radiographic measurements were performed by two independent observers.
Statistical Analysis
Descriptive statistics were reported as mean and standard deviation (SD) for continuous variables or frequency and percentage for qualitative variables. A P-value ≤0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics software (IBM SPSS Statistics for Windows, Version 28.0; IBM Corp., Armonk, New York, USA) and JAMOVI software (Version 2.3).
The association between qualitative variables was assessed using the Chi-Square (χ2) test. The difference of a quantitative variable related to a qualitative variable was assessed with the Mann-Whitney U test. The Spearman’s Rho correlation test was used to assess the correlation between two quantitative variables, with values interpreted as follows: 0.0 – 0.2 scarce correlation, 0.2 – 0.4 weak correlation, 0.4 – 0.6 good correlation, 0.6 – 0.8 strong correlation, 0.8 – 1.00 excellent correlation. Mixed ANOVA and partial η2 index were used to evaluate the interaction effect of a qualitative variable in relation to the difference of scores of an independent variable observed at different times. Values of partial η2 index were interpreted as follows: 0.0 – 0.2 weak relation, 0.2 – 0.4 moderate relation, 0.4 – 0.6 good relation, 0.6 – 0.9 strong relation, >0.9 excellent relation. A linear regression model was used to determine the dependence of an independent variable on a continuous dependent variable.
Results
Preoperative Data
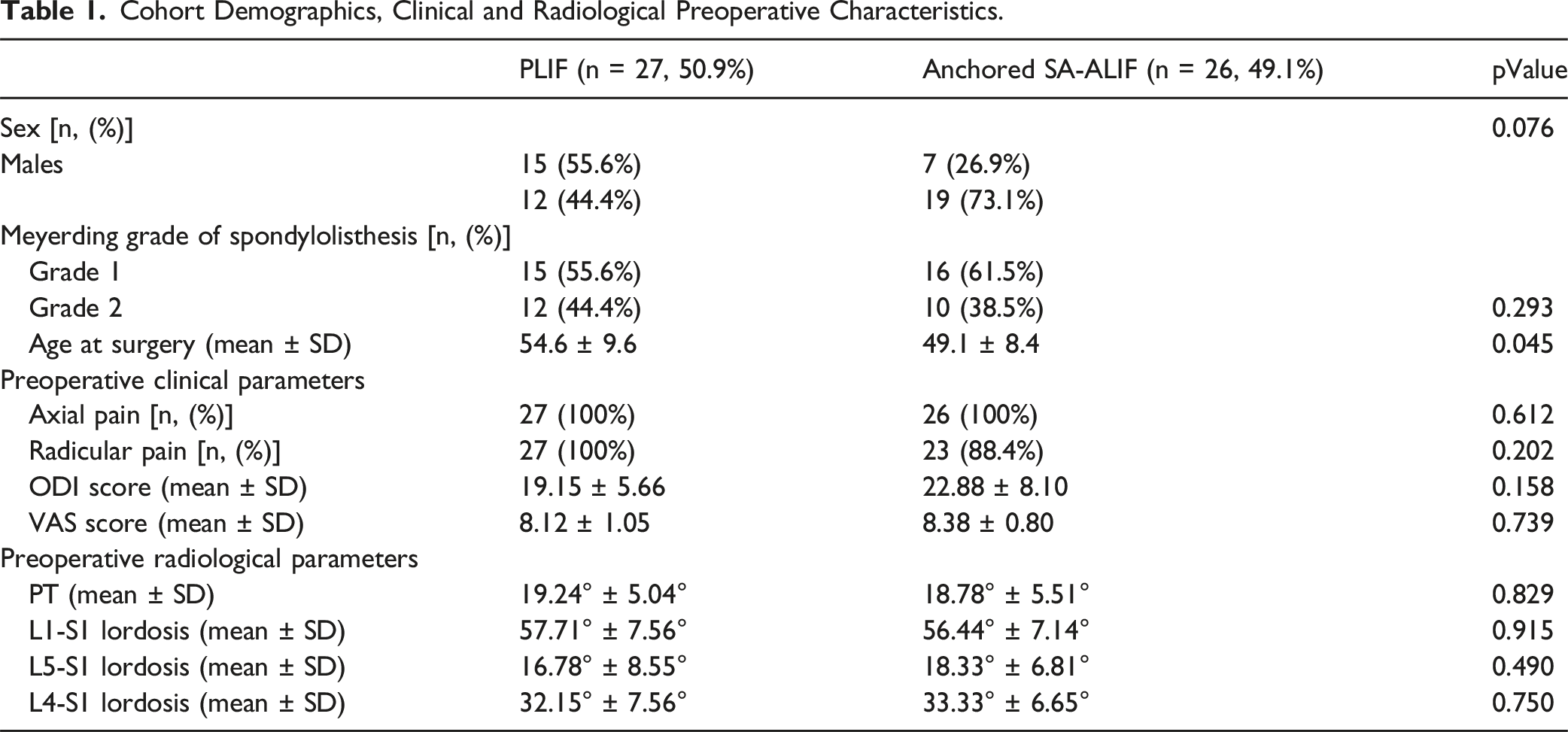
A total of 53 patients with symptomatic low grade L5-S1 IS were included in the study. Among them, 26 patients (49.1%) were considered eligible for anchored SA-ALIF surgery, while 27 patients (50.9%) were treated with PLIF surgery. The mean age at the time of surgical intervention was 54.6 ± 9.6 years in the posterior group and 49.1 ± 8.4 years in the anterior group. Overall, 31 (58.4%) patients presented with Meyerding grade 1 spondylolisthesis, and 22 (41.6%) patients presented with Meyerding grade 2 spondylolisthesis. All patients reported axial lumbar back pain; 23 (88.4%) patients in the anterior group experienced radicular pain, whereas all patients in the posterior group reported of radicular pain. Preoperative mean ODI and VAS scores in the posterior group were 19.15 ± 5.66 and 8.12 ± 1.05, respectively; preoperative mean ODI and VAS scores in the anterior group were 22.88 ± 8.10 and 8.38 ± 0.80, respectively.
Cohort Demographics, Clinical and Radiological Preoperative Characteristics.
Intraoperative Data
Complete Intraoperative Data.
Postoperative Outcome
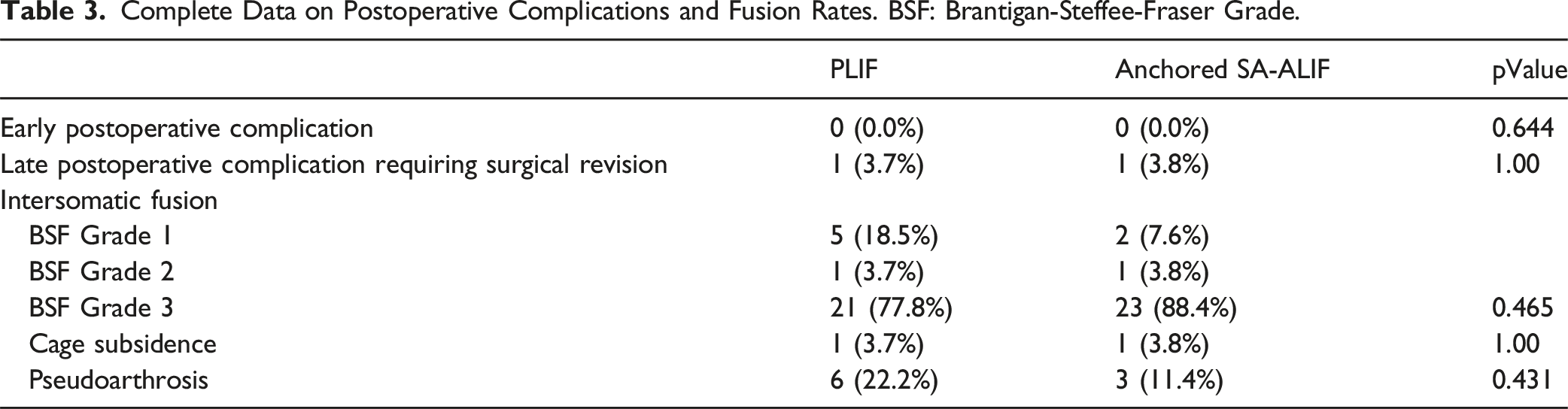
The mean overall postoperative follow-up was 39 ± 20 months, with a minimum of 12 months and a maximum of 71 months. No early postoperative complications were observed in either the posterior or anterior groups. Regarding late postoperative complications, one case of pseudoarthrosis requiring revision surgery was observed in the posterior group due to the atraumatic rupture of the S1 screws. Additionally, one patient from the anterior group underwent posterior revision surgery for symptomatic L5-S1 pseudoarthrosis. No cases of wound infections requiring surgical revision, retrograde ejaculation, vascular injury, or vascular thrombosis were observed in either group.
Complete Data on Postoperative Complications and Fusion Rates. BSF: Brantigan-Steffee-Fraser Grade.
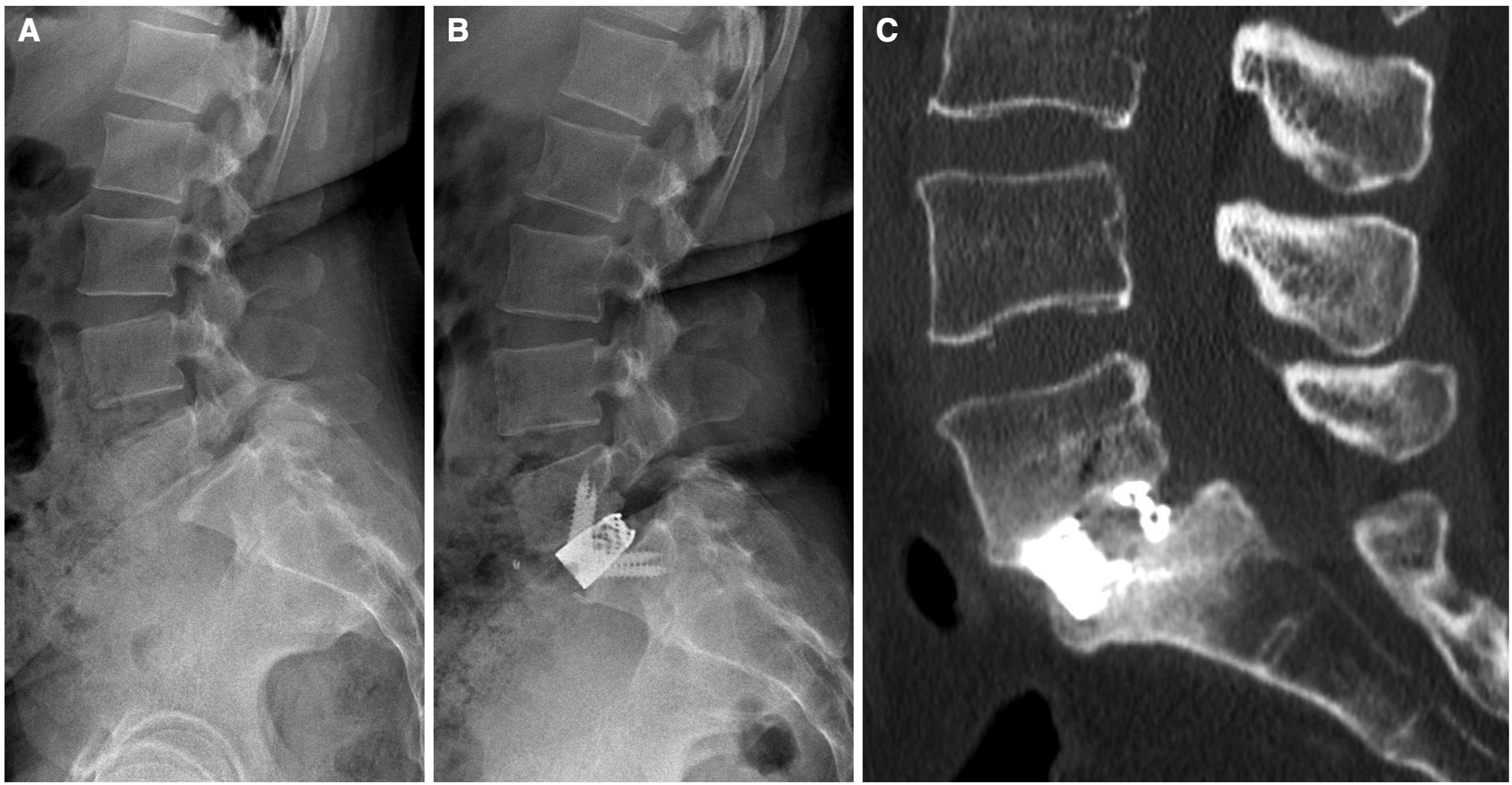
Preoperative (A) and postoperative (B) sagittal radiographs, and final follow-up CT scan (C) demonstrating effective intersomatic fusion (BSF grade 3) of a L5-S1 anchored SA-ALIF construct.
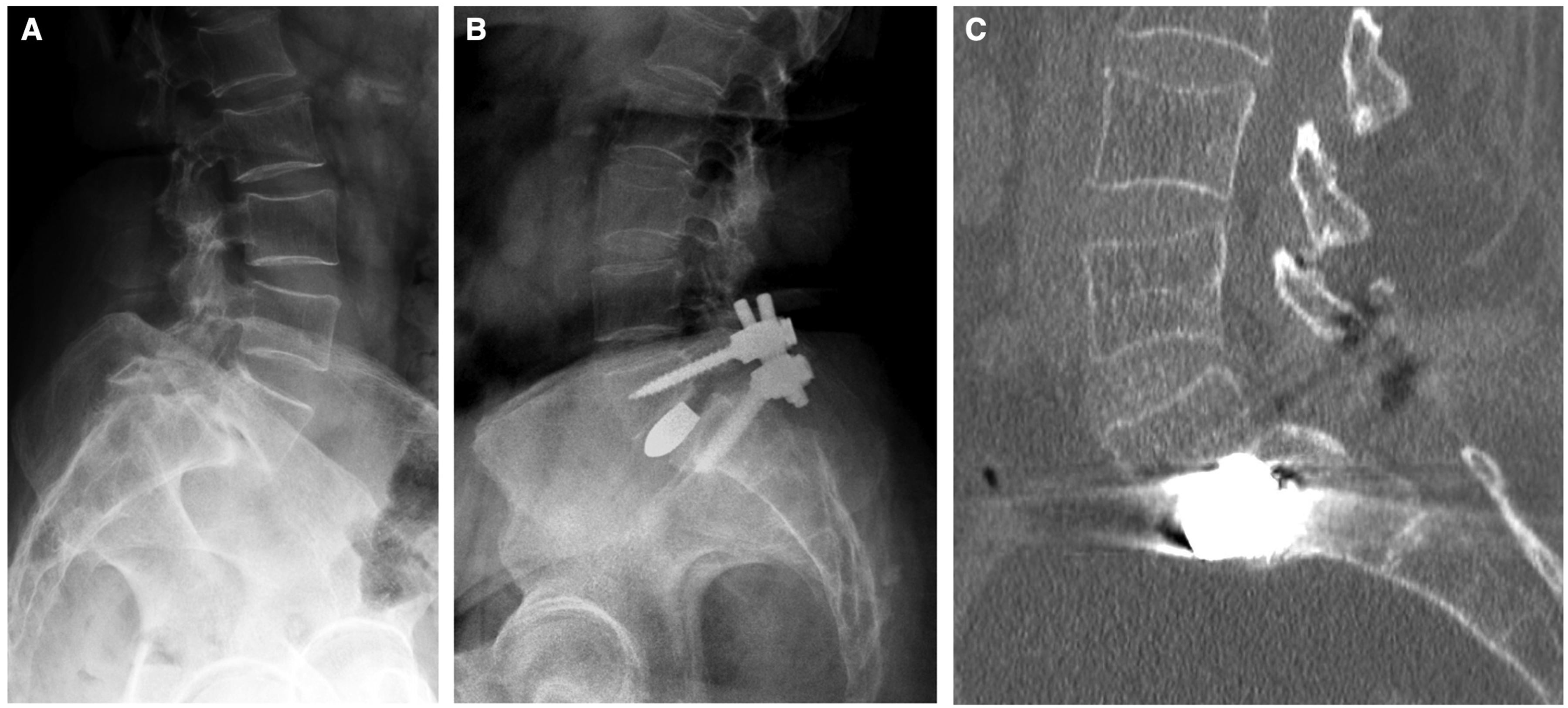
Preoperative (A) and postoperative (B) sagittal radiographs, and final follow-up CT scan (C) demonstrating effective intersomatic fusion (BSF grade 3) of a L5-S1 PLIF construct.
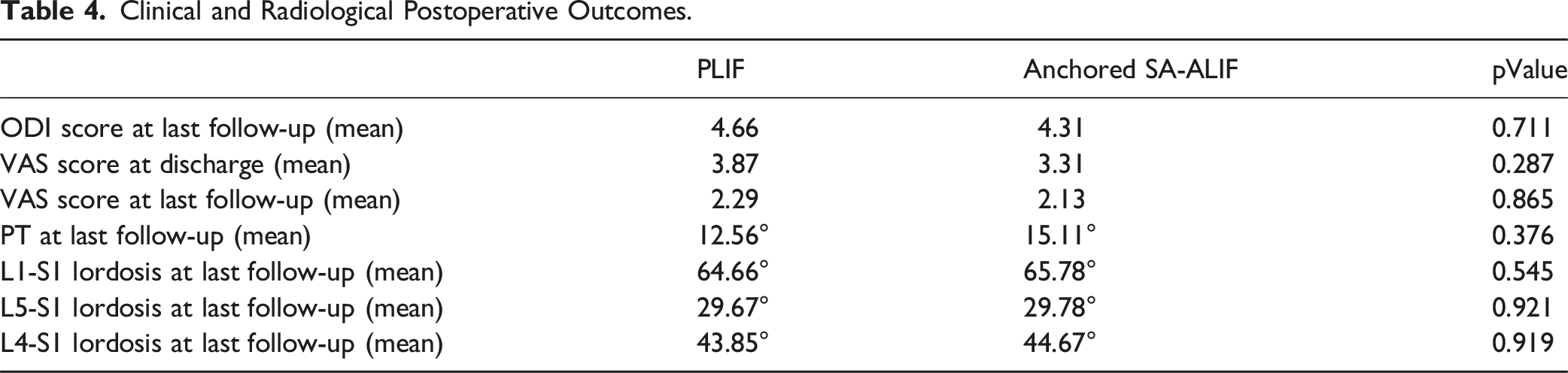
Clinical and Radiological Postoperative Outcomes.
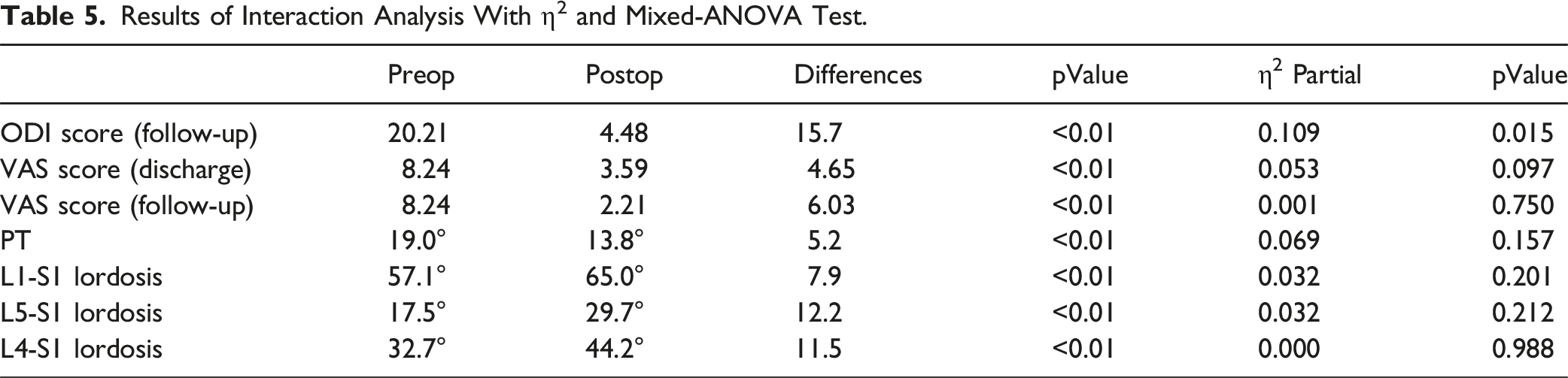
Results of Interaction Analysis With η2 and Mixed-ANOVA Test.
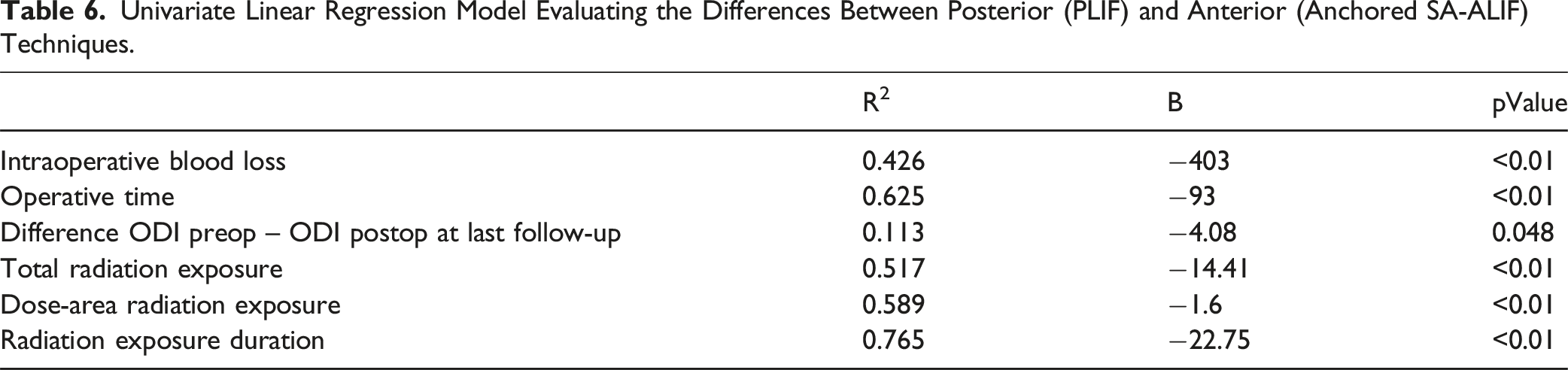
Univariate Linear Regression Model Evaluating the Differences Between Posterior (PLIF) and Anterior (Anchored SA-ALIF) Techniques.
Discussion
The results of our series demonstrate that anchored SA-ALIF can be considered a safe and effective surgical option for the treatment of L5-S1 low-grade isthmic spondylolisthesis. Compared to posterior techniques, patients treated with the anterior approach experienced lower intraoperative blood loss, reduced radiation exposure, and better clinical outcome in terms of postoperative ODI scores. Postoperative intersomatic fusion rates, subsidence risk, and complication rates were consistent with recent published series.
The surgical treatment of lumbosacral low-grade isthmic spondylolisthesis has evolved significantly over the last few decades. Since the first introduction of spinal fusion techniques in the 1950s, advances in imaging technology, understanding of spinal biomechanics, and improvement in surgical instruments and materials have led to more refined and minimally invasive procedures. 8 Currently, surgical techniques for the treatment of lumbosacral L5-S1 IS include decompression, instrumentation, and fusion using anterior, posterior, or combined approaches. Nonetheless, the optimal surgical treatment of low-grade IS still remains a subject of debate.9-11 In recent years, techniques for lumbosacral fusion have progressively shifted towards minimally invasive surgery (MIS) approaches to minimize tissue damage, intraoperative blood loss, and postoperative pain. Moreover, relatively new principles such as indirect decompression have demonstrated safety and efficacy in targeting foraminal stenosis.12,13 In this context, anterior techniques for spinal fusion provide excellent L5-S1 disc exposure through a minimally invasive approach, allowing the placement of large, wedge-shaped, lordotic intersomatic devices. 14 The evolution of technology with anterior trans-somatic self-retaining screws, and the diffusion of new osteoconductive materials such as trabecular titanium, has enabled surgeons to achieve optimal primary stability and effective long-term fusion while reducing the incidence of cage subsidence and pseudoarthrosis. Additionally, the resection of the anterior longitudinal ligament and the supine position of the patient during the surgery facilitate the restoration of lumbar lordosis and sagittal balance parameters.15,16 Exclusively anterior techniques, such anchored SA-ALIF, avoid the need for posterior fixation preserving the integrity of the back muscles and neural structures. 17 However, despite these advantages, there remains skepticism and controversy in the literature regarding the use of anterior stand-alone fusion for treating lumbosacral low-grade IS.
Jaeger et al (2019) analyzed the risk factors of instrumentation failure and pseudoarthrosis after stand-alone L5-S1 ALIF in a cohort of patients treated for degenerative disc disease and grade 1-3 isthmic spondylolisthesis. The presence of isthmic spondylolisthesis and type 4 Roussouly sagittal back classification were associated with an increased risk of instrumentation failure. However, multivariate analysis did not identify any risk factors for pseudoarthrosis. While effective in treating degenerative disc disease, the authors advised caution in using SA-ALIF for low-grade L5-S1 IS, recommending additional posterior instrumentation to reduce the risk of pseudoarthrosis. 18 In a systematic review by Viglione et al. (2017), anterior stand-alone and circumferential fusion approaches were considered superior to posterior techniques for treating L5-S1 IS regarding sagittal alignment restoration, reduced tissue damage, and the ability to limit spondylolisthesis progression. However, the limited number of cases and the low level of available evidence prevented firm conclusions regarding the safety and efficacy of SA-ALIF for L5-S1 IS. 5 A recent retrospective analysis by Jesse et al (2022) confirmed the efficacy and safety of SA-ALIF for the treatment of L5-S1 IS with an overall fusion rate of 84%. In their series, one patient developed L4-L5 adjacent segment disease, and three patients (8.8%) required reintervention for pseudoarthrosis, with no cases of postoperative retrograde ejaculation. 19 Riouallon et al. (2012) analyzed outcomes after SA-ALIF performed at L4-L5 and L5-S1 for IS with long-term postoperative follow-up, demonstrating a fusion rate of 92%-97.5% and acceptable postoperative complications and morbidity with only a case of transient retrograde ejaculation. 2 To the best of author’s knowledge, several comparative studies between anterior and posterior fusion approaches for treating lumbo-sacral IS exist in the literature. However, all the cited studies included only circumferential anterior approaches with posterior instrumentation, excluding anchored stand-alone anterior approaches from the analysis.20-27
Our data demonstrate that both anterior anchored stand-alone and posterior fusion techniques effectively treat low-grade L5-S1 IS. Clinical outcome based on ODI and VAS scales showed postoperative improvements for both techniques, confirming the comparable efficacy of direct and indirect neural foramina decompression for low-grade L5-S1 IS. However, anterior techniques proved to be significantly more effective in improving postoperative ODI scores compared to posterior techniques. Postoperative CT scans revealed an effective fusion rate of 88.4% for the anterior group and 77.8% for the posterior group. These findings align with other published series, which report an overall fusion rates for SA-ALIF of 88.6% (range: 57.5%-99.0%). 28 Intersomatic cage subsidence was observed in only one patient (3.8%) treated with anchored SA-ALIF with previous congenital L4-L5 fusion, which is comparable to the overall subsidence rate for anterior fusion techniques reported in the literature (2-16%).29,30 Radiological signs of pseudoarthrosis were identified in 3 (11.4%) patients in the anterior group and in 6 (22.2%) patients in the posterior group. All pseudoarthrosis cases, according to BSF scale, showed screw haloing or breakage (BSF 1-2) rather than significant cage mobilization or intersomatic non-union. Data from the literature on screw loosening after SA-ALIF are scarce, mainly due to the lack of studies relying exclusively on postoperative CT scans rather than plain X-ray for adequate radiological analysis. 5 Postoperative complication included 1 (3.7%) patient in the posterior group who experienced atraumatic rupture of S1 screws and required posterior revision surgery, and 1 (3.8%) patient from the anterior group who underwent posterior revision surgery for symptomatic L5-S1 pseudoarthrosis. The reported postoperative complication rates significantly differ from those in the literature, where adjacent segment syndrome and surgical revision rates are reported to be 19.1% and 9.6%-11%, respectively.28,31,32 Radiographic outcome regarding lumbar lordosis and sagittal balance parameters restoration were similar between the two techniques, consistent with previous published studies. 33
This study has several limitations. The lack of randomization and the retrospective nature of this study may have introduced selection bias. Additionally, the relatively small sample size limits the generalizability of our findings. However, the study’s strengths include the homogeneity between the two groups and the assessment of postoperative fusion rates using CT scans in all patients. Lastly, all surgical procedures were conducted by the same surgical team (two senior surgeons with comparable experience) at a single academic institution.
Conclusions
This is the first comparative study between anchored stand-alone anterior and posterior fusion techniques for the surgical treatment of L5-S1 low-grade isthmic spondylolisthesis. The results of our series demonstrate that anchored SA-ALIF is a safe and effective surgical option for this subset of patients, yielding favorable clinical and radiological outcomes with acceptable postoperative complication and morbidity.
Advancements in cage technology, particularly the development of anterior anchored cages with trans-somatic self-locking screws, along with improvements in implant materials - such as trabecular titanium, which ensures excellent primary and secondary stability - allow anchored SA-ALIF to be considered for treating conditions like low-grade L5-S1 isthmic spondylolisthesis, which historically required circumferential fusion techniques. However, accurate patient selection remains critical to minimizing the risk of pseudoarthrosis, especially in patients with predisposing factors such as prior lumbar fusion surgery, obesity, diabetes, and poor bone quality.
Thus, anchored SA-ALIF can be considered a viable alternative to posterior circumferential fusion techniques for the treatment of low-grade L5-S1 isthmic spondylolisthesis. Future multicenter prospective studies are warranted to provide additional data and further validate these findings.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to Publication
This study was conducted following the Guidelines for Good Clinical Practice and the Declaration of Helsinki (2002) of the World Medical Association. Written informed consent was obtained from all the patients for each diagnostic and surgical procedure.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.