
Abstract
Study design
Database study.
Objectives
Acute traumatic central cord syndrome (atCCS) is the most common incomplete spinal cord injury in the US, characterized by motor weakness of the upper extremities with relative sparing of the lower extremities and varying degrees of bladder dysfunction and sensory changes caudal to the lesion. Hypoalbuminemia (HA) has previously been associated with poorer outcomes following acute spinal cord injury. We hypothesized that patients with atCCS and HA treated non-surgically experienced worse outcomes than those without HA.
Methods
Data was collected using the PearldiverTM database and included adult patients who sustained atCCS from 2010-2022Q2. Pearson χ2 test and Welch’s t-test were used to evaluate differences in demographic and clinical data. Univariate analysis and multivariate logistic regression were performed.
Results
HA in conjunction with non-surgical care of atCCS was associated with an increased risk of development of renal failure and pressure ulcers as well as longer length of stay and two-year mortality. There was no significant increase in odds ratios for 90-day hospital readmission, pneumonia, UTI, respiratory failure, or sepsis.
Conclusions
Patients with hypoalbuminemia after atCCS treated non-surgically are at an increased risk of developing complications such as renal failure, pressure ulcers, longer lengths of stay and increased mortality. Surprisingly, respiratory failure, pneumonia, and sepsis were not found to be statistically different between patients with atCCS with and without HA. Inherent to a database study there are predictable limitations, however a large-scale analysis could help further delineate physiologic factors affecting outcomes of atCCS patients.
Introduction
Acute traumatic central cord syndrome (atCCS) is the most common incomplete spinal cord injury in the US which typically results from a hyperextension injury either affecting elderly patients with pre-existing cervical spondylotic stenosis or younger adults following motor vehicle crashes. 1 Together they represent about 9% of all adult spinal cord injuries and about 6.6% of pediatric spinal cord injuries. 2 The characterizing features of atCCS involve a disproportionate weakness of the upper extremities compared to the lower extremities combined with sacral sparing and, depending on the severity and extent of the lesion relative to its injury region, will be associated with some degree of spasticity, bladder dysfunction in addition to varying levels of sensory dysfunction. Within this injury constellation, motor function is typically more affected than sensory function. 3
While atCCS is a clinical diagnosis with strong imaging correlation that holds a relatively favorable recovery potential there remains a significant outcomes variability based on the underlying patient baseline health.4-6 Regardless of chosen management strategy, atCCS recovery likely depends in part on a number of underlying patient health factors such as the baseline nutritional status represented in the form of key blood-based proteins, such as albumin. Previous studies have confirmed hypoalbuminemia to be associated with complications following major reconstructive spine surgery, such as surgical site infections, poor wound healing, sepsis, pulmonary embolism, and even mortality.7,8 Hypoalbuminemia as a surrogate for malnutrition or active inflammatory disease state could also be applied as a potential predictor of poor outcomes in the setting of severe systemic challenges such as spinal cord injury.
The potential interrelationship of hypoalbuminemia and adverse clinical outcomes in patients with atCCS has not yet been explored. By applying the benefits of insights gained by analysis gained from a large database, we aimed to investigate outcomes in patients with and without hypoalbuminemia that were non-surgically treated, prompted by the intent to remove the many variables associated with different types of surgical care and explore as purely as possible the impact of the interaction of spinal cord injury and subsequent complications related to nutritional deficiency as expressed in the form of hypoalbuminemia. We hypothesized that there is a direct relationship of poor outcomes in the postinjury clinical course with hypoalbuminemia of patients treated non-surgically for atCCS.
Materials and Methods
Data Source
We performed a formal query of the PearlDiver database (https://www.pearldiverinc.com/, Colorado Springs, CO), a fee-based patient records database. This insurance-based database contains a combination of patient demographics, charge data, and procedural records for patients with disease coding using the International Classification of Diseases, 9th Revision (ICD-9-CM), 10th revision (ICD-10-CM) diagnoses and procedures or Current Procedural Terminology (CPT) codes from multiple different insurers, including both Medicare and Humana (representing a private insurer). The PearlDiver database houses records of over 165 million patients from either the Mariner claims or the Medicare Standard Analytical Files (SAF), which refers to any records that are billed to Medicare. Access to this database, which was stored on a password-protected server, was obtained from PearlDiver Technologies for the purpose of academic research. Patient data was de-identified and therefore exempt from institutional review board approval.
Study Population
The study population included adult patients who were managed nonoperatively for acute traumatic central cord syndrome from 2010 to 2022-Q2. Patients were categorized to having HA if they received the diagnosis at any point prior to admission for atCCS. Patients were then stratified into two groups based on the diagnosis of hypoalbuminemia (ICD-9-D-2738, ICD-10-D-E8809) and matched using a 1 to 10 ratio of HA vs control patients. Baseline status included a detailed assessment of comorbidities that collected sufficient data to enable calculation of the Charlson Comorbidity Index (CCI). We also specifically looked at typical comorbidities such as obesity, smoking, diabetes mellitus, chronic kidney disease, depression, and others. For our study we excluded patients who had any form of surgery as treatment for their spinal cord injury.
Outcome Measures
We assessed 90-day complications, including medical events such as arrhythmia, myocardial infarction, cardiac arrest, respiratory failure, pleural effusion, pulmonary embolism, deep vein thrombosis, cardiovascular accident, electrolyte abnormality, renal failure, urinary retention, pneumonia, sepsis, urinary tract infection, and pressure ulcer. Both 30-day and 90-day readmissions, length of stay, and mortality rates by the conclusion of 2 years were also documented. Patient discharge status was obtained from the Standard Analytic Files dataset.
Statistical Analysis
Pearson χ2 test and Welch’s t-test were used to assess for differences in demographic and clinical data. Univariate analysis was conducted first to determine significant postoperative outcomes. Multivariable logistic regression was performed using the significant variables derived from the univariate analysis and clinical expert opinion in order to determine the effects of hypoalbuminemia on various outcomes. All statistical analyses were performed using the research query interface provided by PearlDiver Bellwether. The common statistical metrics, including frequencies, mean values, and odds ratios (ORs), were collected by the Bellwether system using the R statistical package. Statistical significance was set at P < .05. Using the matplotlib library in Python, forest plots were created with the adjusted ORs plotted alongside their 95% confidence interval (CIs) for each outcome. For outcomes where the CIs crossed the null value of 1, the lines were bolded.
system using the R statistical package. Statistical significance was set at P < .05. Using the matplotlib library in Python, forest plots were created with the adjusted ORs plotted alongside their 95% confidence interval (CIs) for each outcome. For outcomes where the CIs crossed the null value of 1, the lines were bolded.
Results
Summary of Demographic Variables for 2695 Patients Managed Nonoperatively for Central Cord Syndrome.
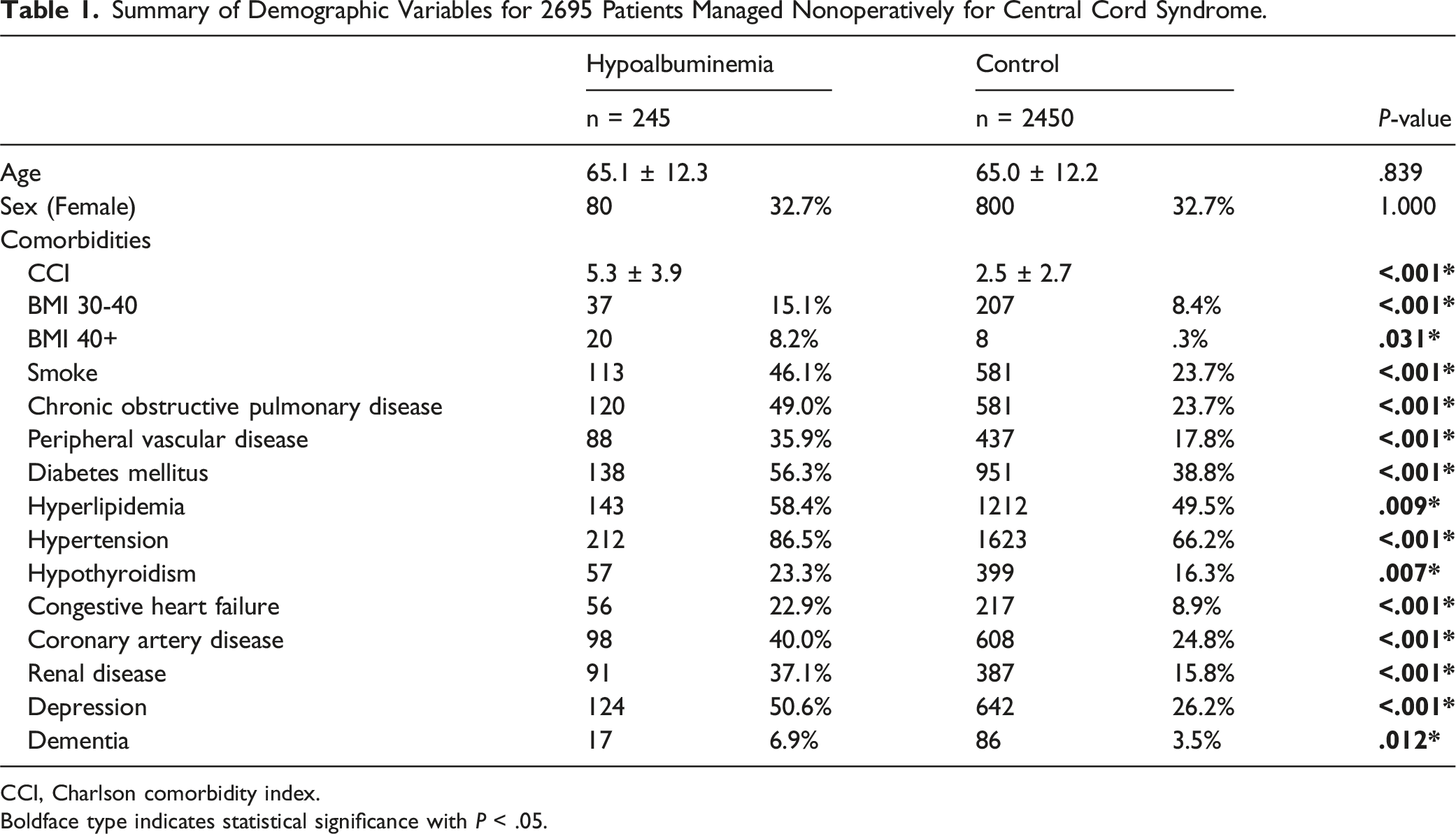
CCI, Charlson comorbidity index.
Boldface type indicates statistical significance with P < .05.
Univariate Analysis of 90-Day Complications.
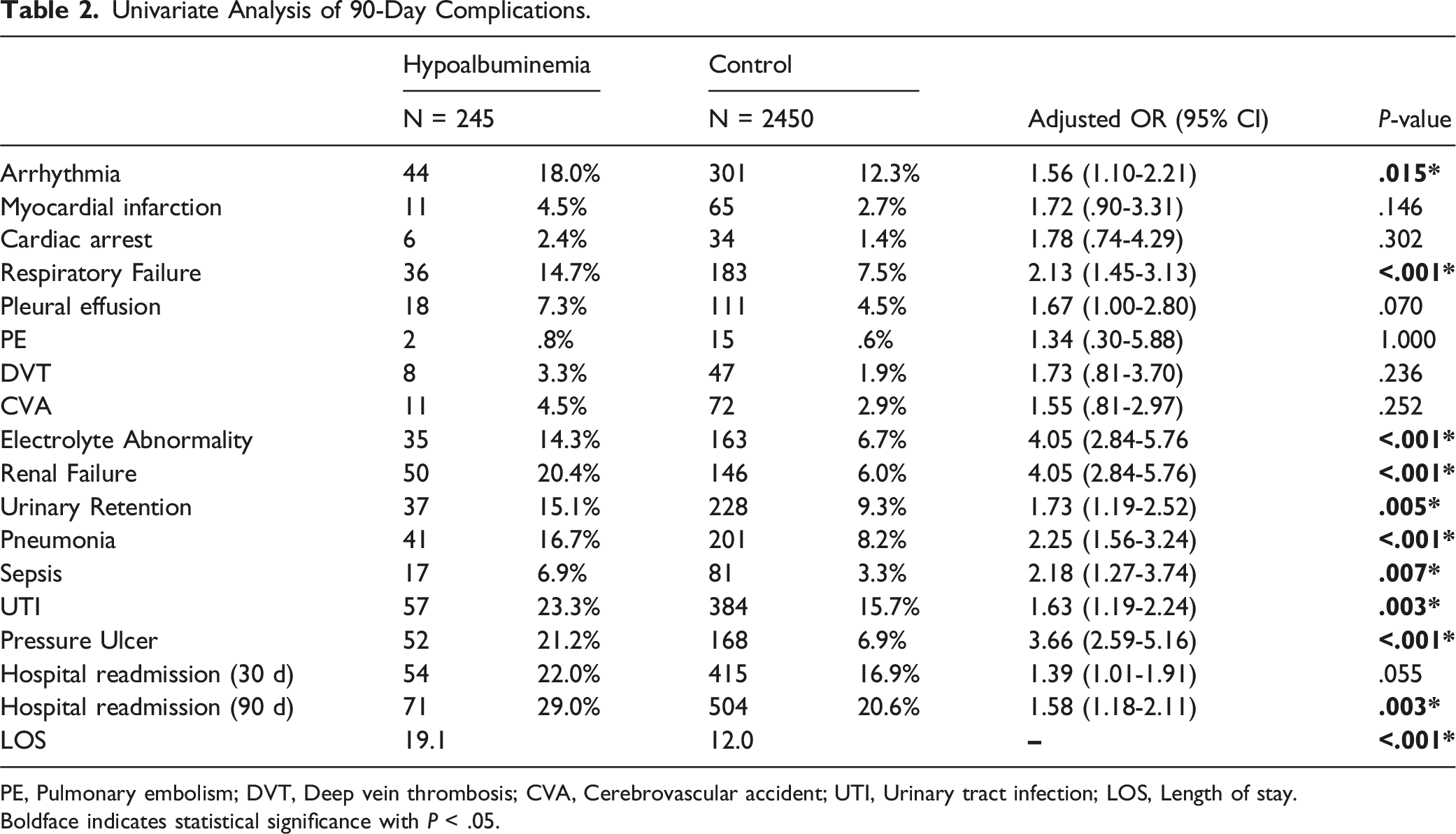
PE, Pulmonary embolism; DVT, Deep vein thrombosis; CVA, Cerebrovascular accident; UTI, Urinary tract infection; LOS, Length of stay.
Boldface indicates statistical significance with P < .05.
Multivariate Analysis of 90-Day Complications.
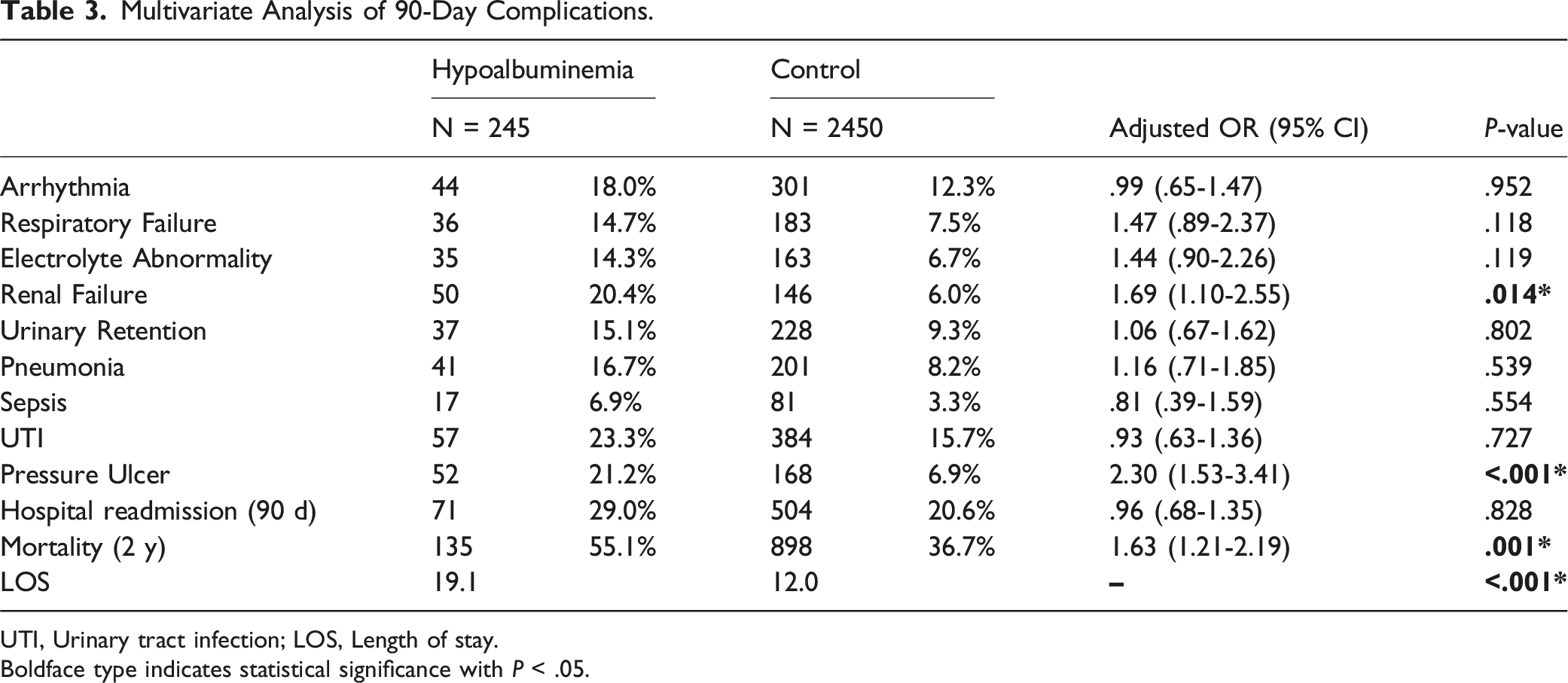
UTI, Urinary tract infection; LOS, Length of stay.
Boldface type indicates statistical significance with P < .05.
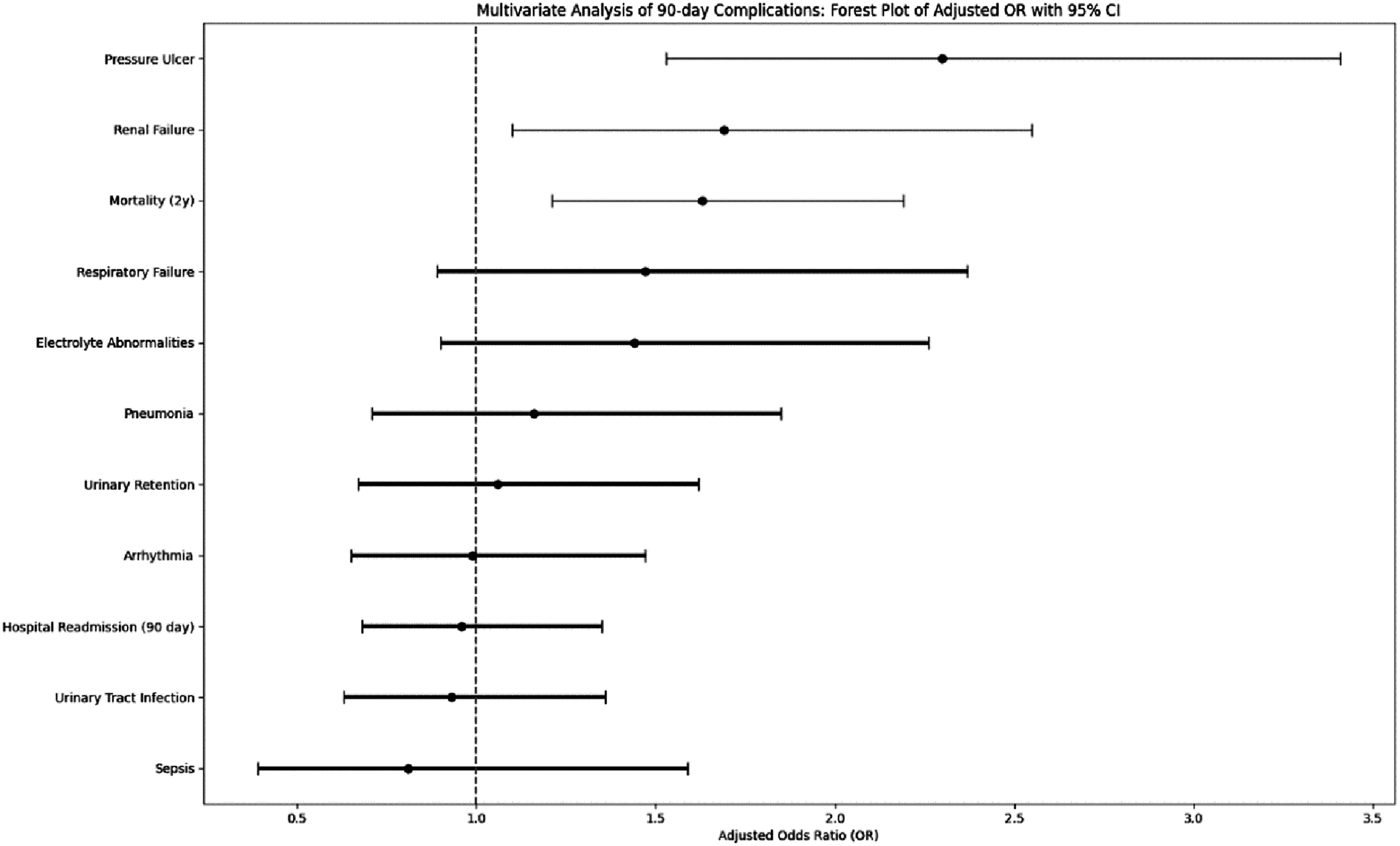
Forest plot of adjusted OR with 95% CI.
Discussion
First described by Schneider et al, in 1954, 3 central cord syndrome is the most common incomplete spinal cord injury in the United States.9,10 Understanding of the neuropathophysiology of atCCS has changed over time, with the more recent explanation revolving around a more diffuse shear pattern of injury rather than representing trauma to a specific columnar somatotopic organization of the corticospinal tract in the spinal cord.10-12 Hypoalbuminemia has previously been associated with poor outcomes following acute spinal cord injury in general.13-15 From a serologic standpoint, albumin plays a critical role in maintaining intravascular osmotic pressure and serving as a transport protein for hormones, drugs, and other molecules while also participating in immune and inflammatory responses. 16 Historically, serum albumin levels have been used as a simple yet non-specific surrogate marker for poor nutritional status without actually by itself being diagnostic of the multifactorial pathoentity of malnutrition. 17 More recently, albumin has been viewed as a negative acute phase reactant, complicating the assumption that hypoalbuminemia is directly related to nutritional status.18,19 To date, the association between serum albumin and atCCS has not yet been explored.
In our study, hypoalbuminemia (HA) was associated with an increased likelihood of renal failure in patients with atCCS compared to the control group, with an odds ratio of 1.69. Hypoalbuminemia in patients with pre-existing renal failure is attributed to both a reduced synthesis and increased degradation. 20 However, previous studies have reported low albumin to be a risk factor for the development of renal complications 21 with a 2010 meta-analysis reporting a causal relationship between hypoalbuminemia and the development of acute kidney injury or acute renal failure. 22 With regard to potential prevention and treatment, previously, administration of human albumin has been found to be nephroprotective in some cases,20,23,24 but mechanisms are not understood, and this has not been studied in the context of spinal cord injury. Future studies may explore the use of serum albumin as a prevention of complications in patients with hypoalbuminemia and atCCS.
Patients in the analysis with hypoalbuminemia were also more likely to develop pressure ulcers compared to control. In the past, HA has been found to be directly correlated with the development of pressure ulcers in patients in the intensive care unit. 25 Furthermore, albumin administration has been found to both prevent pressure ulcers from developing and progressing to advanced stages. 26 However, a more recent study found that HA alone was not a risk factor for pressure ulcers in surgical patients, but rather the associated comorbidities of HA were causing the ulcers. 27
Hypoalbuminemia has been found to increase mortality with other spinal pathologies 28 This is supported by our results as overall mortality differed significantly between the two study groups, with an odds ratio of 1.63 for the HA compared to the control group. In practice, serum albumin is screened on routine bloodwork 13 and can thus be a relatively simple way to help aid in the prognostic evaluation of patients presenting with atCCS.
Of note, HA was not found to be associated with an increased risk of developing respiratory failure, though respiratory complications are common in patients with spinal cord injuries.29-32 The cause of respiratory failure in SCI is attributed to weakness of respiratory muscles resulting in an inability to cough and clear secretions from the respiratory system; higher level and completeness of injury are associated with a greater risk of respiratory complications.30-32 One study found that 74% of patients with complete spinal cord injury required mechanical ventilation, with an increased risk with Asia A complete cervical spinal cord injuries. 14 Extent of severity of deficits in atCCS and association with respiratory complications may be explored further. Furthermore, hypoalbuminemia is itself a risk factor for the development of pulmonary complications such as ARDS, and it is thus overall surprising that our results did not support the existing evidence. 33 Additionally, patients with HA were not found to have an increased risk of developing pneumonia or sepsis, despite hypoalbuminemia being a known risk factor for the development of both complications. 34 However, we cannot elucidate these findings, which are contradictory to the literature.
Database studies have inherent limitations. Pearldiver, as a private analytics database, includes patients primarily 65 and older with a predilection for the Southern United States 35 and includes patients that are not randomly sampled. As with any database study, there is also the potential for coding error, either clerical or a result of annual updates to ICD-10 code definitions. 36 Furthermore, severity of deficits and neurologic level of injury following central cord injury was not explored and may be related to the development of complications following injury. A potential interrelation of baseline HA and atCSS on outcomes vs acquired HA during hospitalization could not be explored with the data as available. We decided to minimize variables introduced by spine surgery care in spinal cord injury by reducing our investigation to those patients who received nonsurgical treatment only. Patients placed into nonsurgical care as treatment choice may have been afflicted by poor medical baseline conditions, thus creating a selection bias. Lastly, there may be other variables that were not measured or included in the analysis that influence outcomes. Future case-controlled, prospective studies might be more suitable to parse out potential relationships between HA and atCCS complications.
Conclusion
Patients presenting with hypoalbuminemia after acute traumatic central cord injury treated non-surgically are at an increased risk of developing certain complications such as renal failure and decubital pressure ulcers and also have longer lengths of stay, higher longer term readmissions risk after 90 days as well as an increase in overall mortality. Surprisingly, respiratory failure, pneumonia, and sepsis were not found to be statistically different between patients with atCCS with and without HA. This database study has a significant size and claims to have high data quality standards does have limitations, but future case-controlled, prospective studies may further explore complications in atCCS patients and hypoalbuminemia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.