
Abstract
Study Design
This study is part of the AO Spine Metastatic Tumor Research and Outcomes Network [MTRON], an international multicenter prospective observational registry including patients with spinal metastases.
Objectives
This study aims to elucidate the incidence of surgical complications, their risk factors and consequent effects on survival outcomes, hospital length of stay, and overall health-related quality of life (HRQOL) parameters in a large cohort of patients affected by spinal metastases who were surgically treated.
Methods
Available data from February 2017 to July 2023 were analyzed. The primary outcome of this study was the evaluation of the incidence of intraoperative and postoperative adverse events (AEs). The secondary outcomes included the assessment of risk factors for surgery-related AEs and the impact of AEs on survival, length of hospital stay and quality of life.
Results
Among the 1267 patients analyzed, 6.9% experienced intraoperative AEs and 19.3% experienced at least 1 postoperative AE. Several factors resulted to be associated to the occurrence of postoperative AEs: age, smoking habit, poor Eastern Cooperative Oncology Group (ECOG) Performance status, previous radiation therapy at the index target, duration of surgery, number of instrumented levels, simultaneous anterior and posterior approach, presence of metastases at other sites, multiple spinal metastases. Postoperative AEs were associated with reduced survival rates, increased hospital length of stay and poorer HRQOL outcomes, particularly in domains such as neurological function and mental health. In general, surgery substantially improves HRQOL across multiple domains, with these benefits persisting over time despite the occurrence of AEs. However, patients with preoperative risk factors, including comorbidities, smoking, neurological impairment, and prior radiation therapy, experienced less improvement.
Conclusions
The negative impact of AEs on overall survival and HRQOL could be associated with the presence of some preoperative parameters of frailty that are detected as risk factors for AEs occurrence. This finding emphasizes the need for personalized preoperative assessments and optimized perioperative care strategies.
Keywords
Introduction
Recent years have witnessed a notable rise in the incidence of spinal metastases, attributed to advancements in cancer therapeutics and prolonged patient survival. 1 Collectively, spinal metastases afflict 70% of cancer patients, with 10% to 20% experiencing skeletal-related events, including refractory pain, pathological vertebral fractures, and spinal cord compression, culminating in neurological impairment, compromised ambulatory function, diminished quality of life, and reduced survival rates.2-4 Accordingly, surgical intervention is often warranted to alleviate symptoms, restore functional integrity and improve health-related quality of life (HRQOL).5,6
Surgical treatments for spinal metastases encompass palliative resections employing anterior, posterior, or anteroposterior approaches in general, and are often accompanied by conventional or stereotactic radiation. 7 Less invasive techniques, such as percutaneous stabilization and cement augmentation, are also utilized regularly. Given the primarily palliative nature of treatment and the considerable vulnerability of these patients, surgical interventions carry a significant risk of complications and thus decision making is complex. 7 Various studies have reported complication rates ranging from 10% to 76.2% following spine surgery for metastases.8-27 In a retrospective study of 987 patients, the overall complication rate during the index hospital admission/surgery and subsequent admissions was 39%, with 27% experiencing one major complication and 12% encountering 2 or more postoperative complications. 22 A large administrative database retrospective study, inherently providing less detail, involving 26,233 patients reported an in-hospital complication rate of 21.9%. 15 A more recent systematic literature review indicated a 29% risk of complications associated with spine surgery for metastases, with infections and pulmonary complications being the most prevalent. 23 Finally, a rigorous prospective study on complications in emergency surgery for metastatic spine diseases reported a very high rate of complications, with 76.2% of patients experiencing at least 1 adverse event (AE). 27 Complications lead to prolonged hospital stays, additional diagnostic tests, treatments, and the need for rehabilitation services. Importantly, AEs in this patient population may also interrupt or delay systemic or radiation therapy. Furthermore, readmission rates within 3 months post-discharge range from 9.7% to 16.8%, with corresponding rates of reoperations for complications.12,22 This AE profile contributes to significant healthcare costs and suffering to patients with oftentimes limited life expectancy.
Making inroads to reduce complications depends on first improving data quality and then acting on these data. The extreme variability in complication rates displayed in the literature and thus inaccuracy rests almost entirely on the process of the surveillance, capture, reporting and research methodology; an administrative vs research registry, dedicated surveillance personal, standardized psychometrically sound classification and severity grading, retrospective vs prospective collection and detailed follow-up. Furthermore, multicenter and multicultural collection is essential to optimize generalizability.
The Metastatic Tumor Research and Outcomes Network (MTRON) (National Clinical Trial n. NCT02830451) is part of the AO Spine Knowledge Forum Tumor’s global network of surgeons and oncologists dedicated to improving care and outcomes in these unique and deserving patients. MTRON has acted on many of the afore mentioned limitations inherent to the literature by developing a comprehensive prospective, multicenter, multicountry registry of patients who have undergone surgical intervention for spine metastases. Utilizing this registry the primary outcome of this study is to determine the incidence of AEs in patients with spine metastases requiring surgery with or without radiation. Secondary outcomes are first to assess the relationship of complications to survival, hospital length of stay, and overall HRQOL and second to identify risk factors for developing complications in this patient cohort.
Methods
Study Design
This study is part of the AO Spine Knowledge Forum Tumor’s Metastatic Tumor Research and Outcomes Network [MTRON], an international multicenter prospective observational registry including patients with spinal metastases. The trial is registered at ClinicalTrials.gov with ID number NCT02830451.
Each participating center’s local Ethics board approved the study protocol and IRB approval numbers for each center are reported in the title page.
Patients were eligible to be enrolled into the registry if they were 18 years or older and were diagnosed with a metastatic spinal tumor. All patients signed a study-specific informed consent before the enrolment for the study.
For this predefined research question, patients were eligible for inclusion in the analysis if they were prospectively treated with surgery for metastatic spine disease. Available data from February 2017 to July 2023 were analyzed.
Outcome Measures
Prospectively collected data included the following: demographic and clinical data at baseline, number and location of spinal lesions, primary tumor location, histology and subtype, presence of other distant metastases, prior treatments of index metastasis.
Baseline functional status was assessed with preoperative American Spinal Injury Association (ASIA) for neurological assessment and Eastern Cooperative Oncology Group (ECOG) for performance status. The degree of spinal cord compression and instability were assessed by Bilsky grade epidural compression classification and Spinal Instability Neoplastic Score (SINS) at the time of treatment, respectively. Surgical and radiotherapy treatment details were collected. Pain was assessed at baseline and at all follow-up visits with the pain NRS. Health-related Quality of Life (HRQOL) metrics included the Spine Oncology Study Group Outcomes Questionnaire (SOSGOQ2.0) 28 and Euro-QoL 5D (EQ-5D-3L), 29 which were performed at baseline and all follow-up visits. Surgery-related AEs were collected using the Spine Adverse Events Severity system version 2 (SAVES V2) and were classified as minor if grade was ≤3 and severe if grade was >3. 30
The primary outcome of this study was the evaluation of the incidence of intraoperative and postoperative AEs, in patients requiring surgical intervention for spinal metastases. The secondary outcomes included the impact of surgery-related AEs on survival, length of hospital stay and HRQOL. All patients’ data were collected and stored in a de-identified format in a secure web-based database [REDCap v6.5.2, Vanderbilt University, Nashville, TN, USA]. Only patients who had at least half of the digital forms completed in the REDCap database were included in the analysis to ensure data quality.
Statistical Analysis
Descriptive statistics were used to summarize baseline population characteristics, including demographic variables, stratified by the occurrence and severity of AEs. For the primary endpoint—incidence of intraoperative and postoperative AEs—percentages with 95% confidence intervals (CIs) were reported. Subjects experiencing multiple AEs of the same type were counted once.
For secondary endpoints, such as survival and length of stay, Kaplan-Meier analysis was employed to compare patient groups with and without AEs. Differences in survival between these groups were assessed using a stratified log-rank test. To adjust for covariates, we applied the Cox proportional hazards model to estimate hazard ratios (HRs) with their corresponding 95% CIs.
Longitudinal data, such as repeated measurements of patient-reported outcomes across timepoints, were analyzed using a mixed model for repeated measures (MMRM). Model estimates were presented with their associated 95% CIs. Additionally, lasso regression was conducted to explore the relationships between potential covariates (eg, age, ECOG performance status, smoking history) and AE occurrence, identifying key predictors. The final model included selected variables along with their coefficients.
Missing data was addressed using multiple imputation techniques. A two-sided P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SAS (version 9.4, SAS Institute Inc, Cary, NC, USA) and R (version 4.1.2 or later, R Core Team, 2021).
Results
Descriptive Analysis of the Study Population
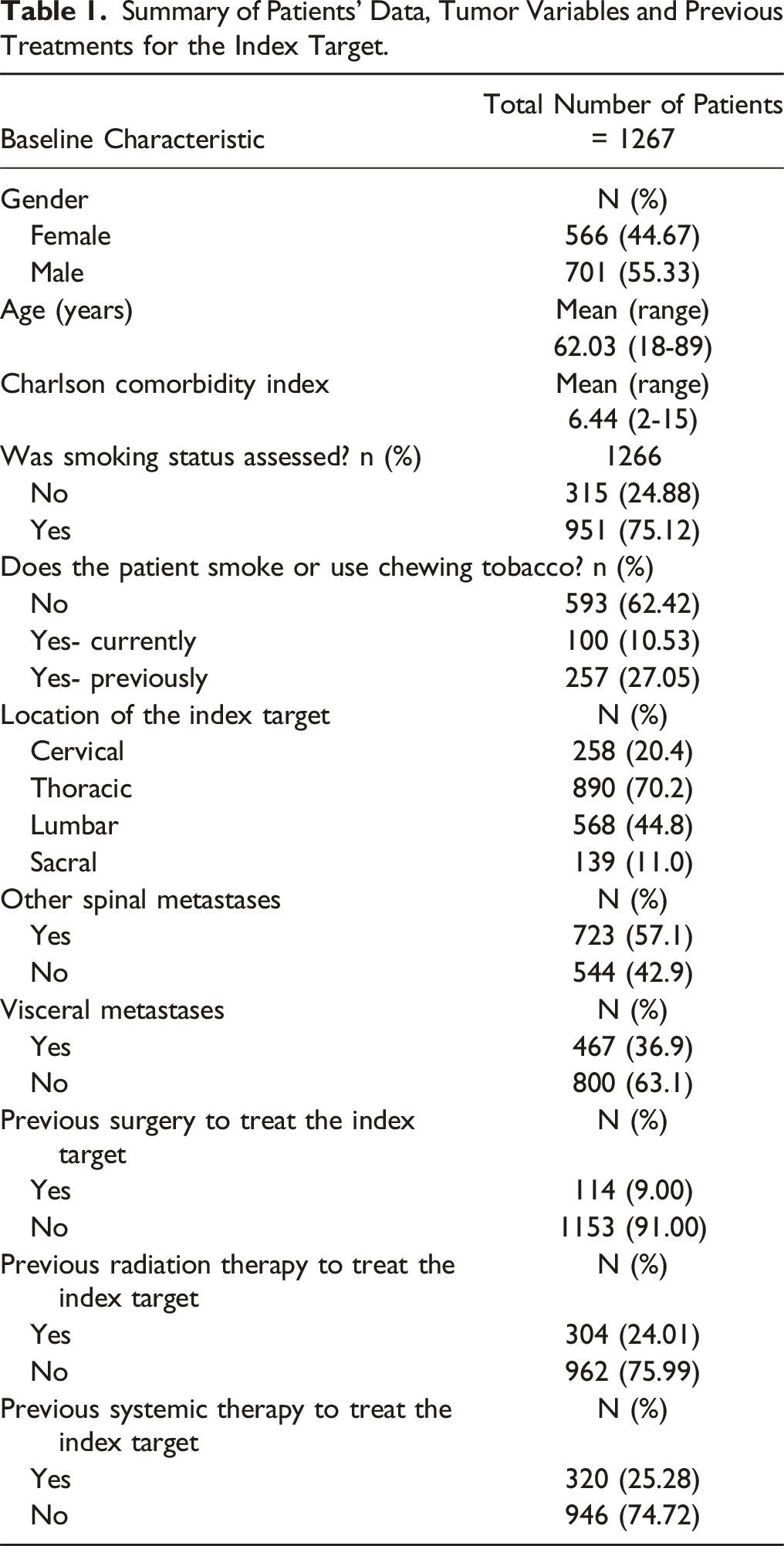
Summary of Patients’ Data, Tumor Variables and Previous Treatments for the Index Target.
As shown in Figure 1, 1158 patients (90.8%) were followed up to 30 days after surgery, 1066 patients (84.1%) were followed up to 60 days (2 months) after surgery and 752 patients (59.4%) to 180 days (6 months) after surgery. Number of patients at follow-up at 1 month, 2 months, 3 months, and 6 months after surgery.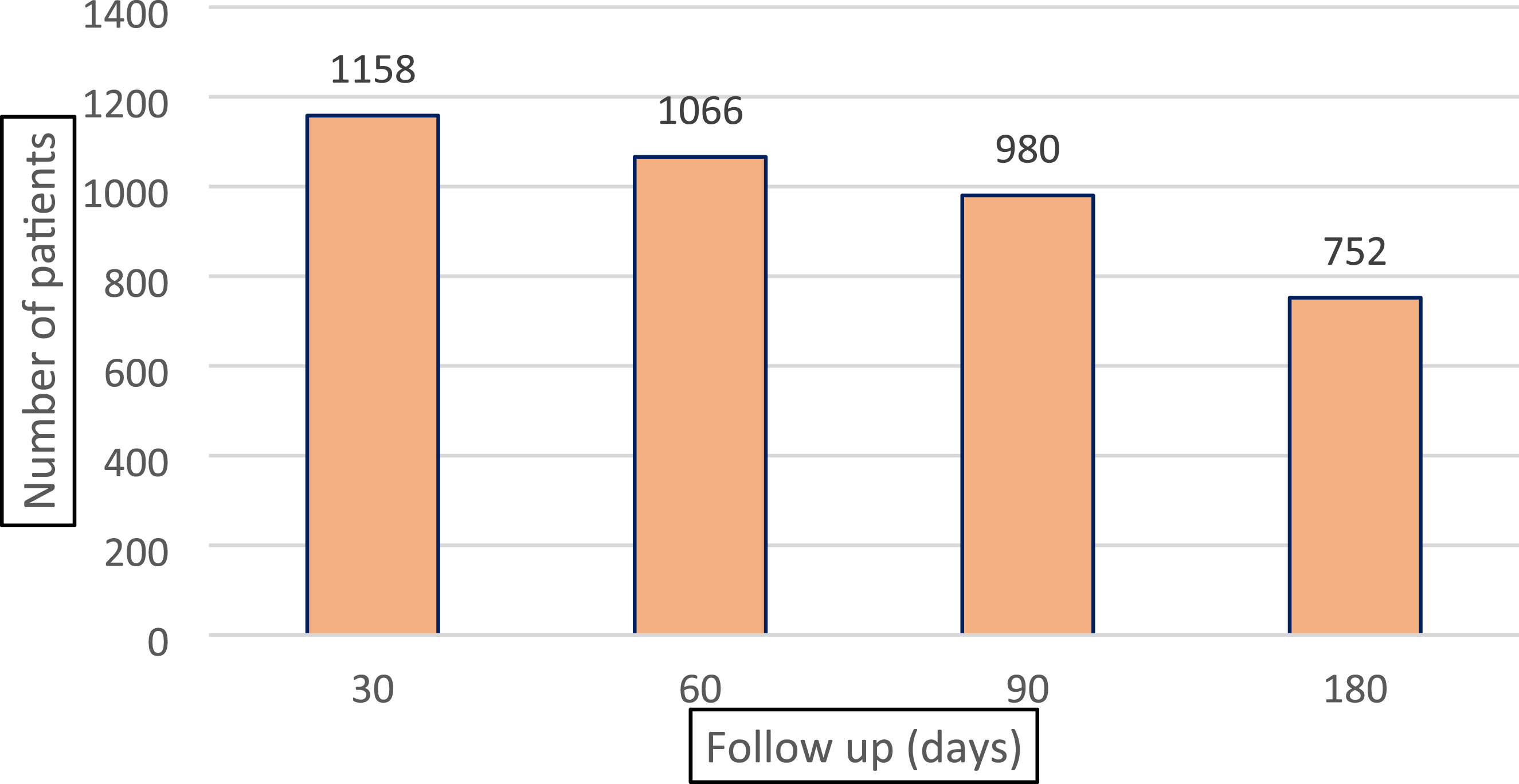
The distribution of primary tumors is shown in Figure 2. Most of metastatic index targets were in the thoracic spine (890, 70.2%); other spinal metastases were present in 723 patients (57.1%) and visceral metastases were present in 467 patients (36.9%). 114 patients (9%) were previously treated with surgery at the index target, while 304 patients (24.0%) underwent previous radiation therapy at the index target, and 320 patients (25.3%) underwent previous systemic therapy. Type of primary tumors in the overall cohort of 1267 patients.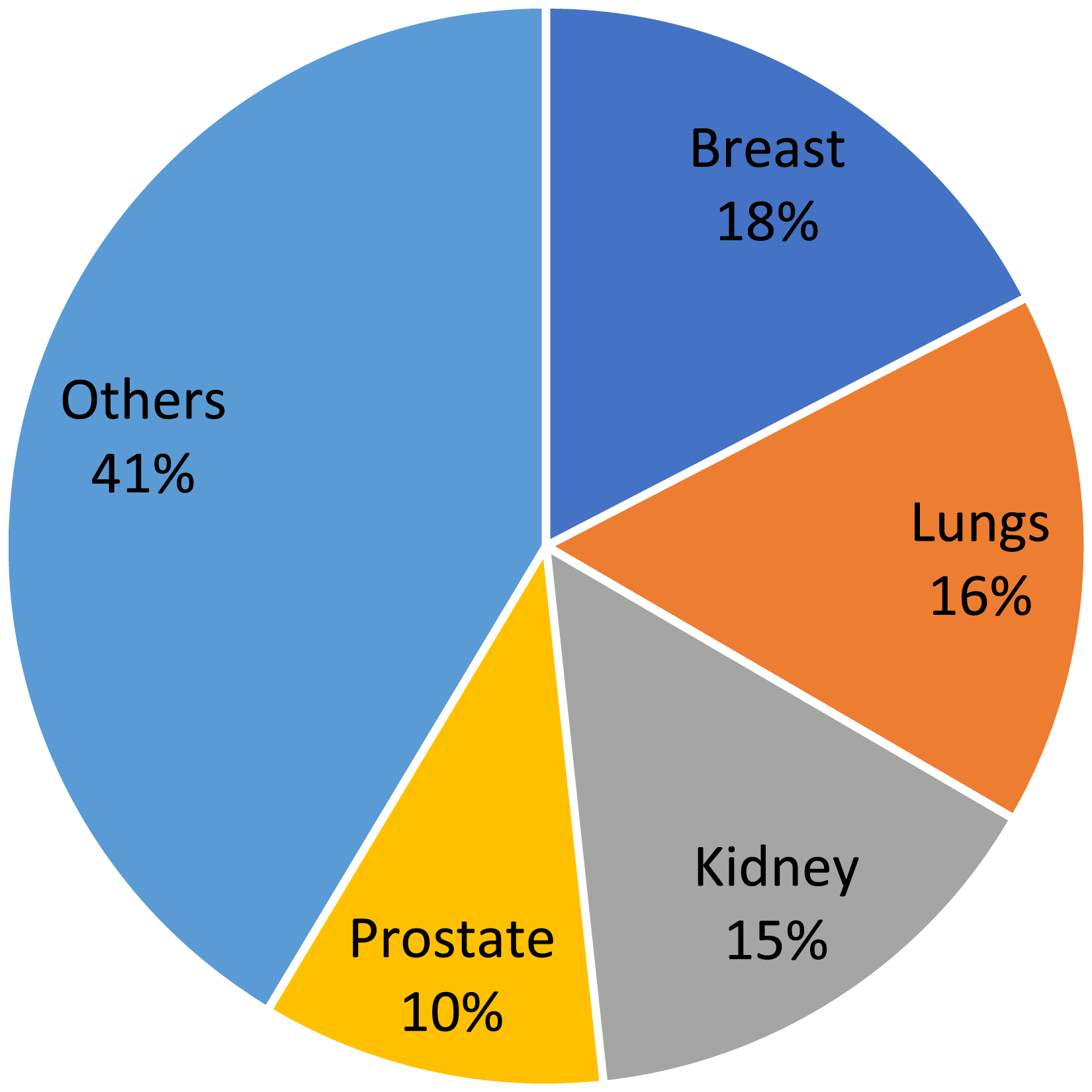
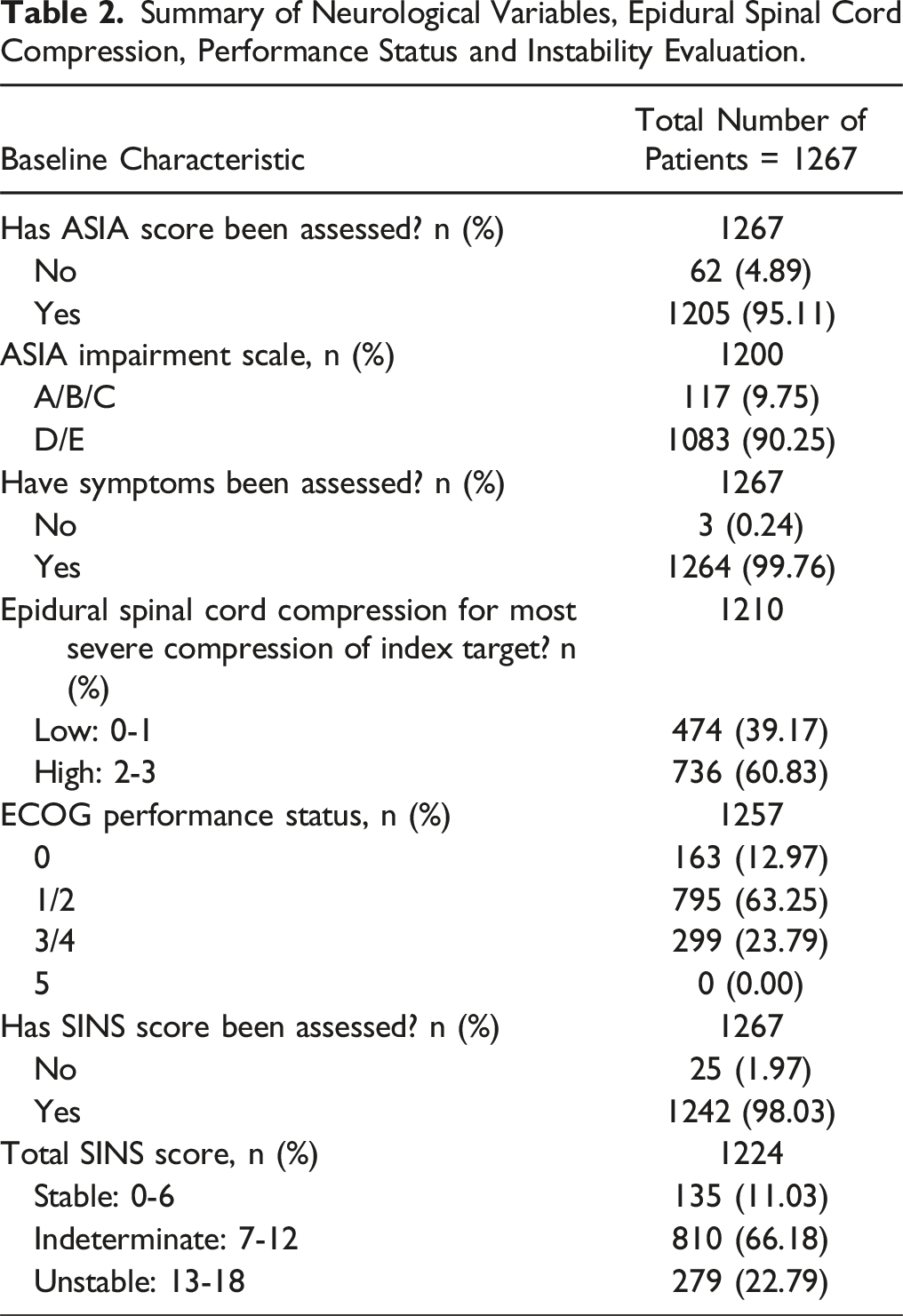
Summary of Neurological Variables, Epidural Spinal Cord Compression, Performance Status and Instability Evaluation.
Summary of Surgical Variables.
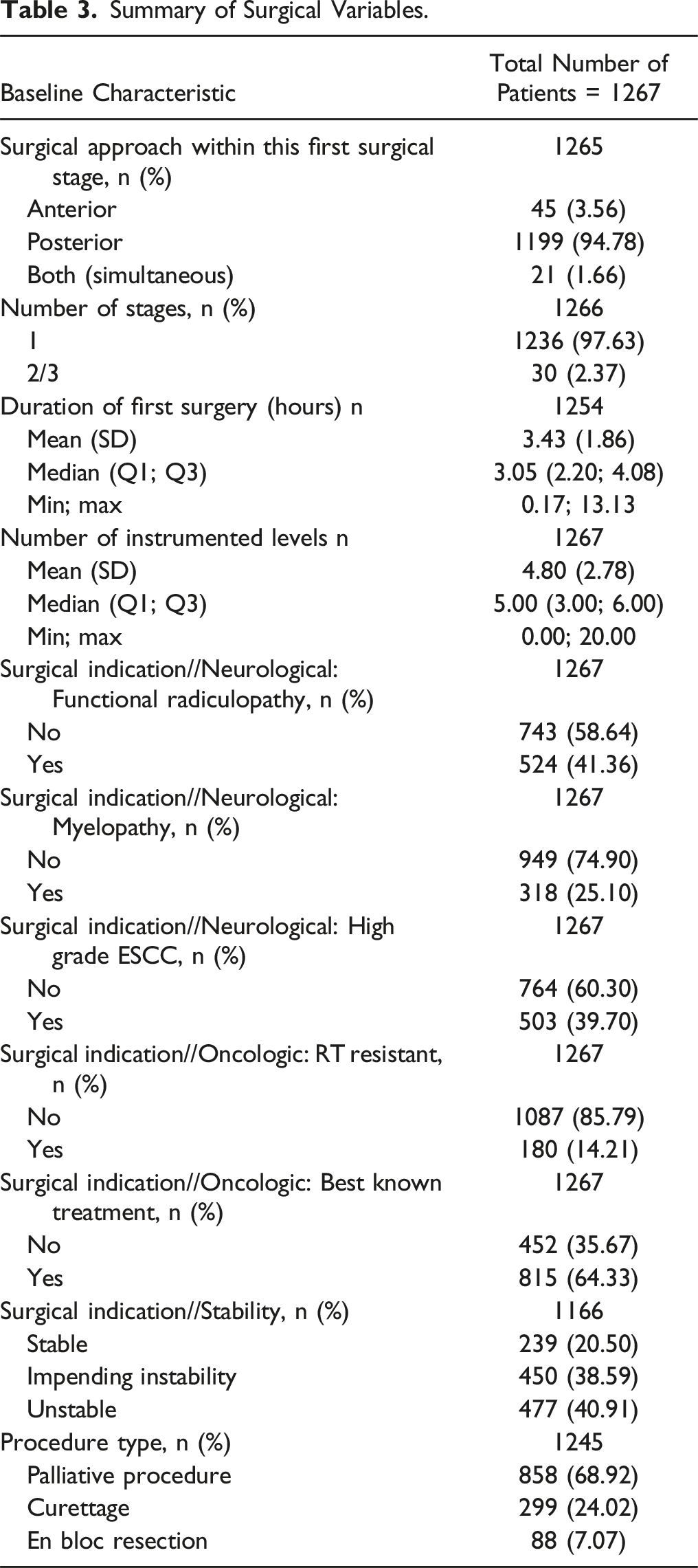
Most of the surgical procedures (68.9%) had palliative intent, debulking was performed in 24.0% of cases and en-bloc resection in 7.1% of cases.
Adverse Events Collection
Intraoperative Adverse Events (Patient Level), Worst Severity Grade and Severity Group.
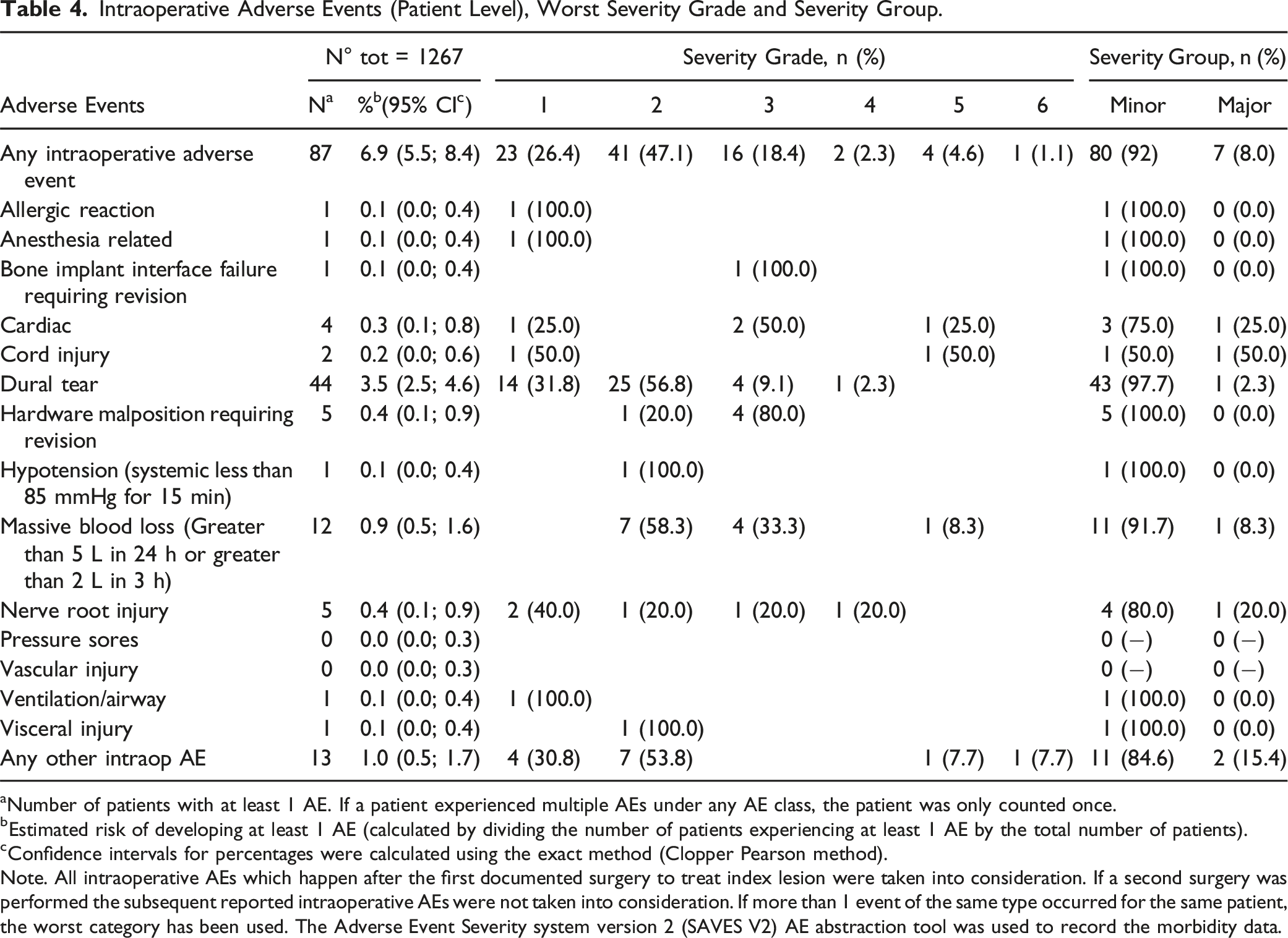
aNumber of patients with at least 1 AE. If a patient experienced multiple AEs under any AE class, the patient was only counted once.
bEstimated risk of developing at least 1 AE (calculated by dividing the number of patients experiencing at least 1 AE by the total number of patients).
cConfidence intervals for percentages were calculated using the exact method (Clopper Pearson method).
Note. All intraoperative AEs which happen after the first documented surgery to treat index lesion were taken into consideration. If a second surgery was performed the subsequent reported intraoperative AEs were not taken into consideration. If more than 1 event of the same type occurred for the same patient, the worst category has been used. The Adverse Event Severity system version 2 (SAVES V2) AE abstraction tool was used to record the morbidity data.
Postoperative Adverse Events (Patient Level), Worst Severity Grade and Severity Group.
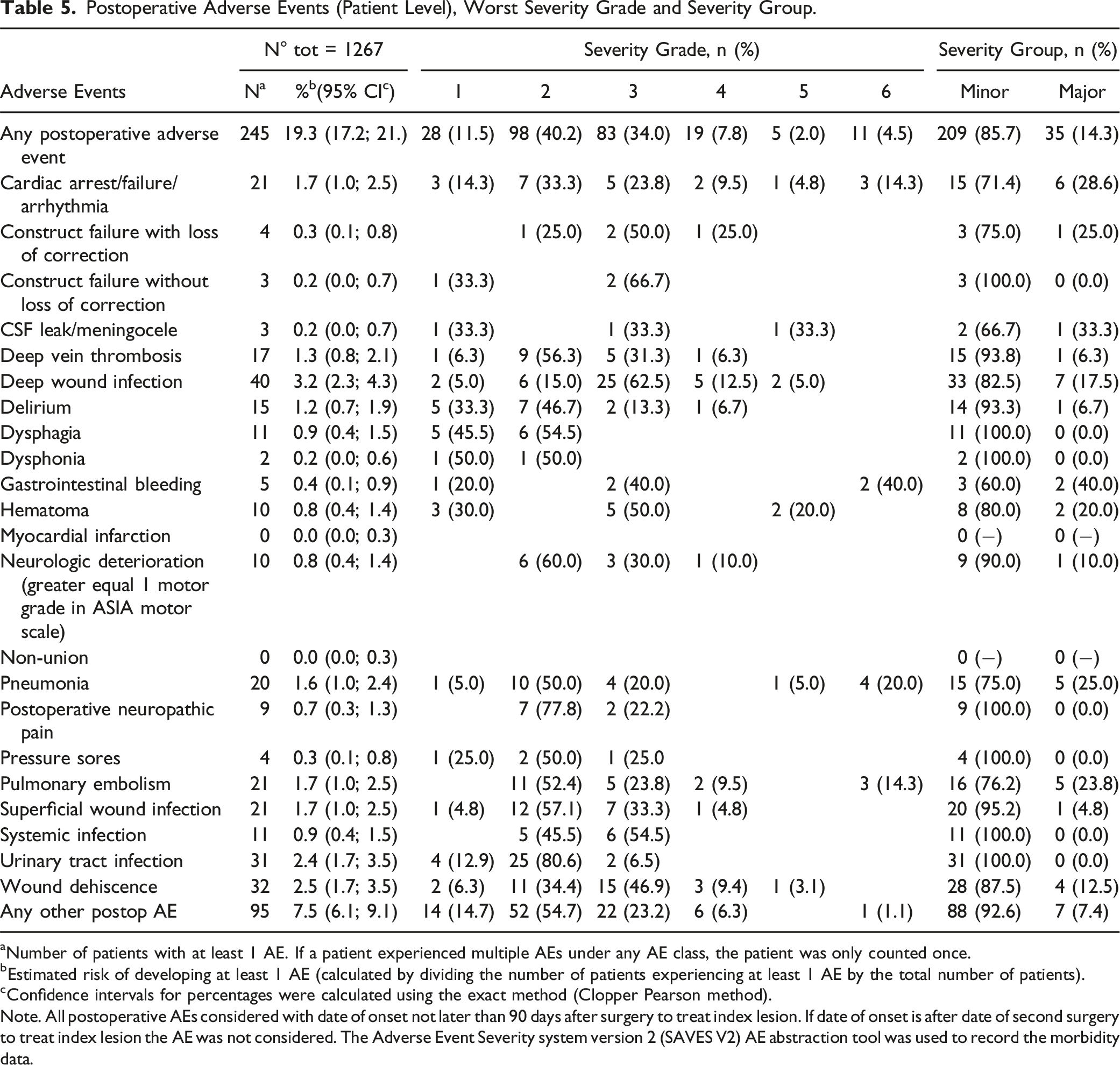
aNumber of patients with at least 1 AE. If a patient experienced multiple AEs under any AE class, the patient was only counted once.
bEstimated risk of developing at least 1 AE (calculated by dividing the number of patients experiencing at least 1 AE by the total number of patients).
cConfidence intervals for percentages were calculated using the exact method (Clopper Pearson method).
Note. All postoperative AEs considered with date of onset not later than 90 days after surgery to treat index lesion. If date of onset is after date of second surgery to treat index lesion the AE was not considered. The Adverse Event Severity system version 2 (SAVES V2) AE abstraction tool was used to record the morbidity data.
Number of Adverse Events per Subject (Patient Level).
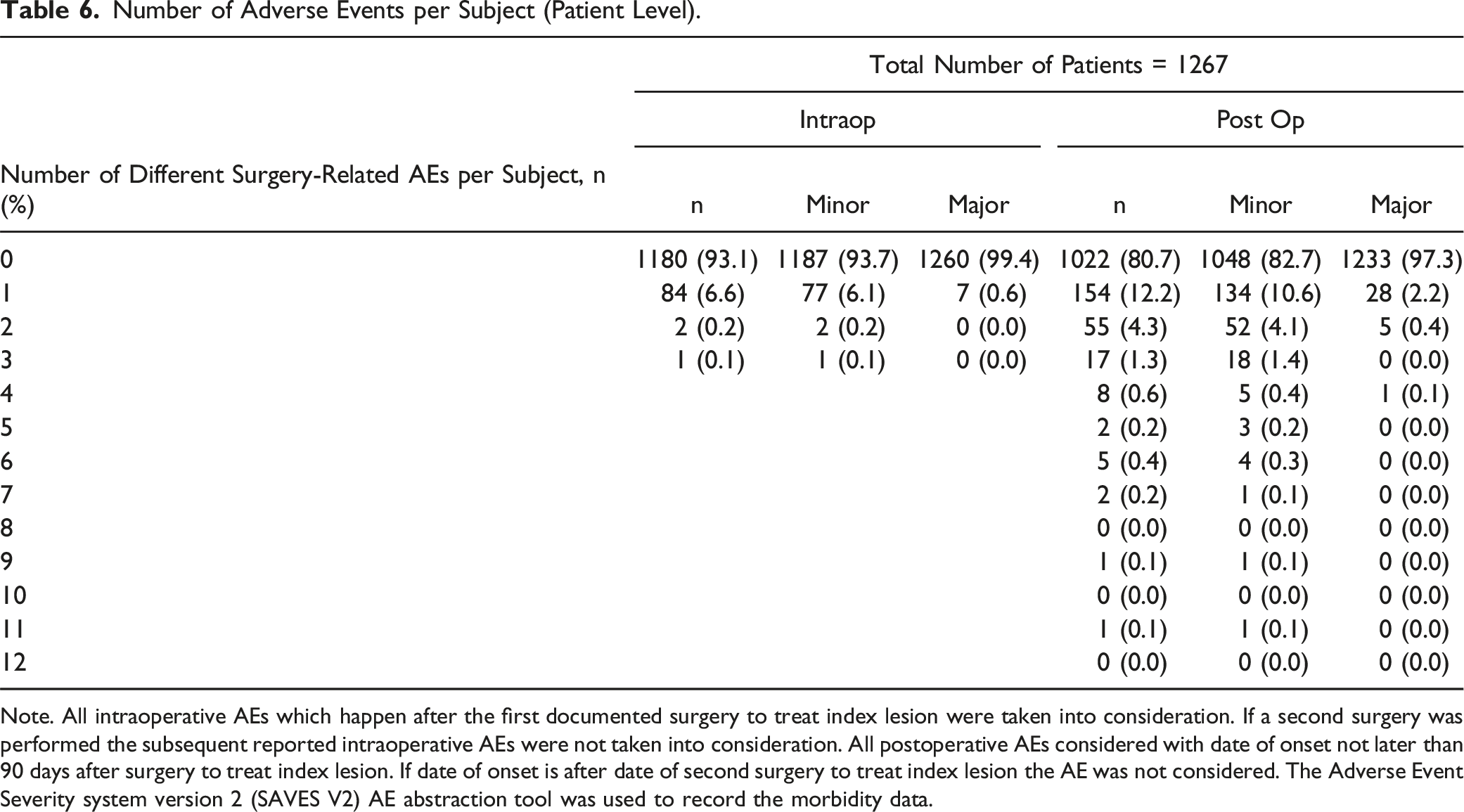
Note. All intraoperative AEs which happen after the first documented surgery to treat index lesion were taken into consideration. If a second surgery was performed the subsequent reported intraoperative AEs were not taken into consideration. All postoperative AEs considered with date of onset not later than 90 days after surgery to treat index lesion. If date of onset is after date of second surgery to treat index lesion the AE was not considered. The Adverse Event Severity system version 2 (SAVES V2) AE abstraction tool was used to record the morbidity data.
The population characteristics (demographic variables, tumor variables, neurological variables, symptoms, surgical variables and previous treatments) were stratified in relation to the occurrence of intraoperative and postoperative AEs, as reported in Supplemental Materials (Tables I-X).
Logistic Regression Models for the Occurrence of Adverse Events
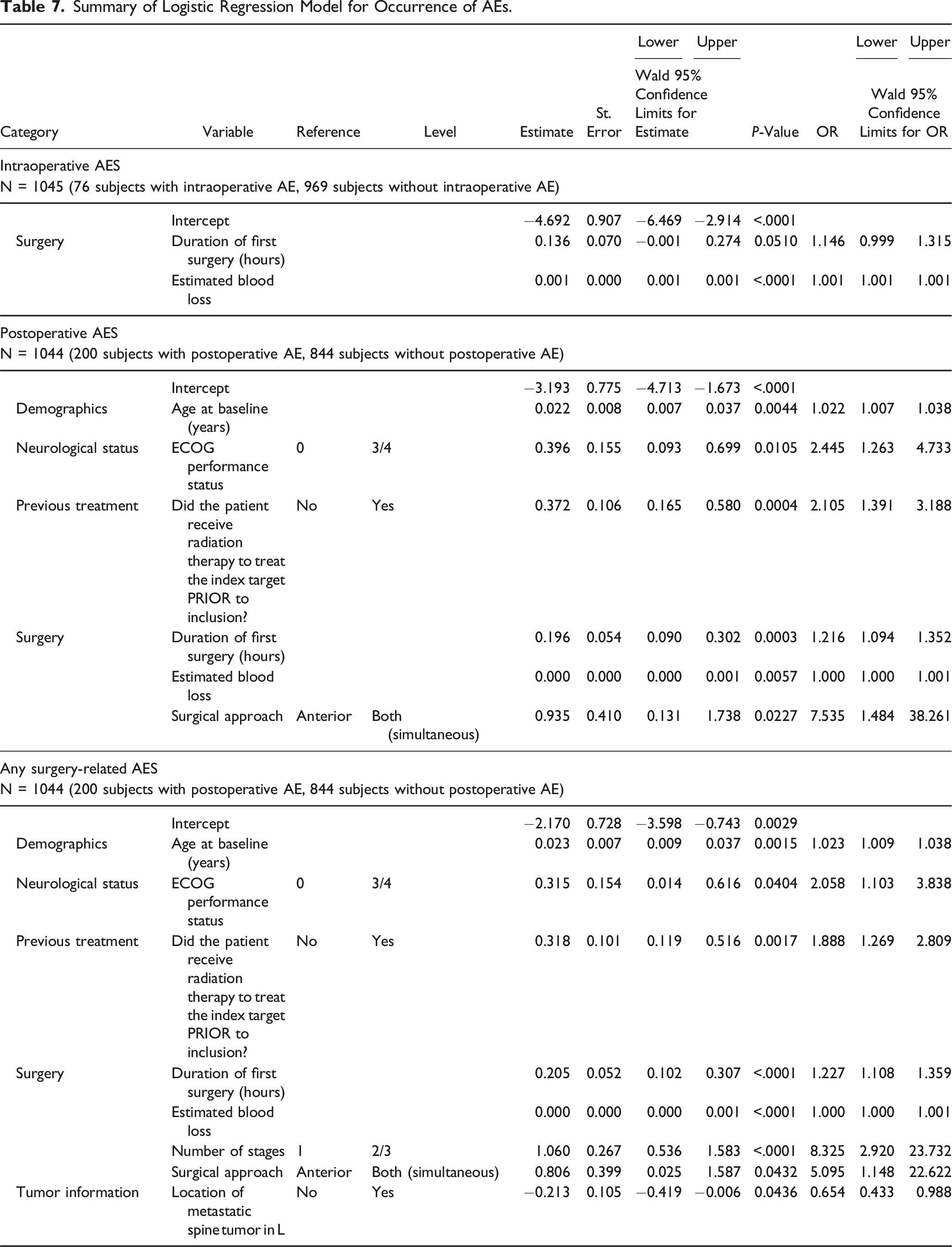
Summary of Logistic Regression Model for Occurrence of AEs.
Impact of AEs on Survival
The impact of surgery-related AEs on patients’ survival was evaluated by Kaplan-Meier analysis and the plots are reported in Figures 3 and 4. Kaplan-Meier plot for comparison of survival by occurrence of AE. (A) Any intraoperative AE; (B) Any postoperative AE; (C) Any surgery-related AE. Kaplan-Meier plot for comparison of survival by occurrence of major AE. (A) Any major postoperative AE; (B) Any major surgery-related AE.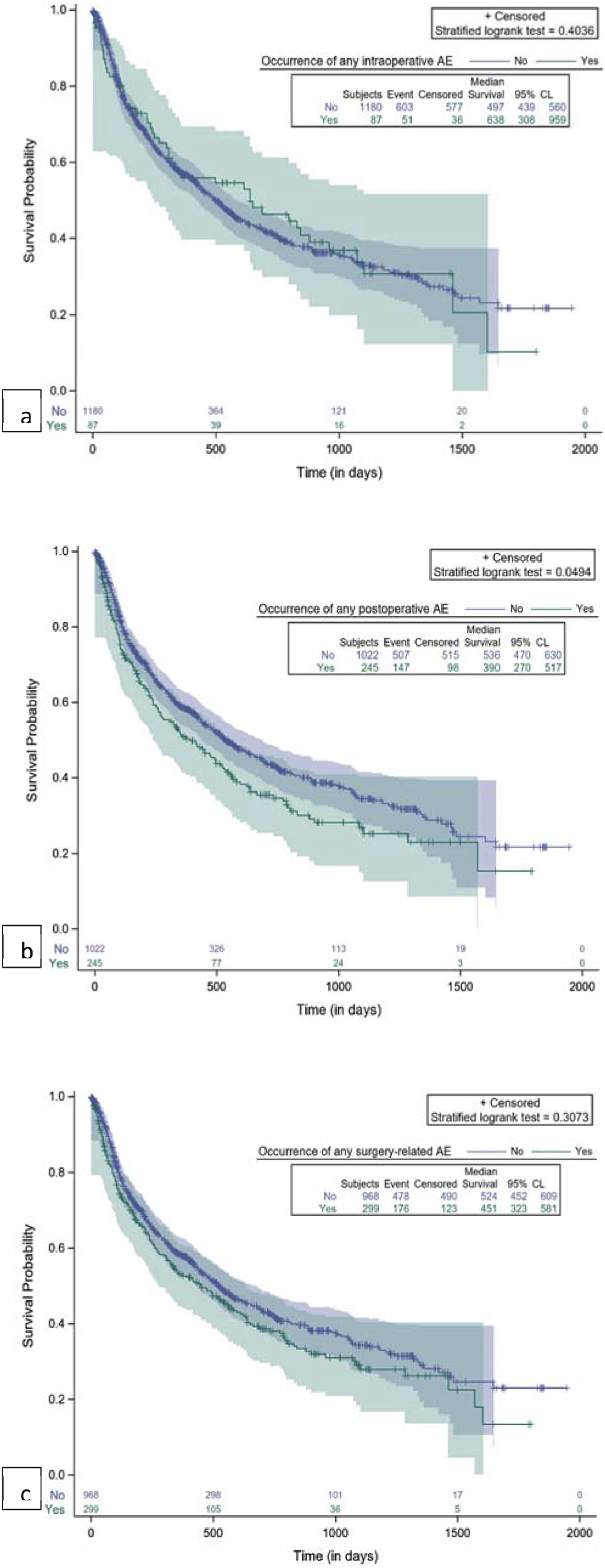
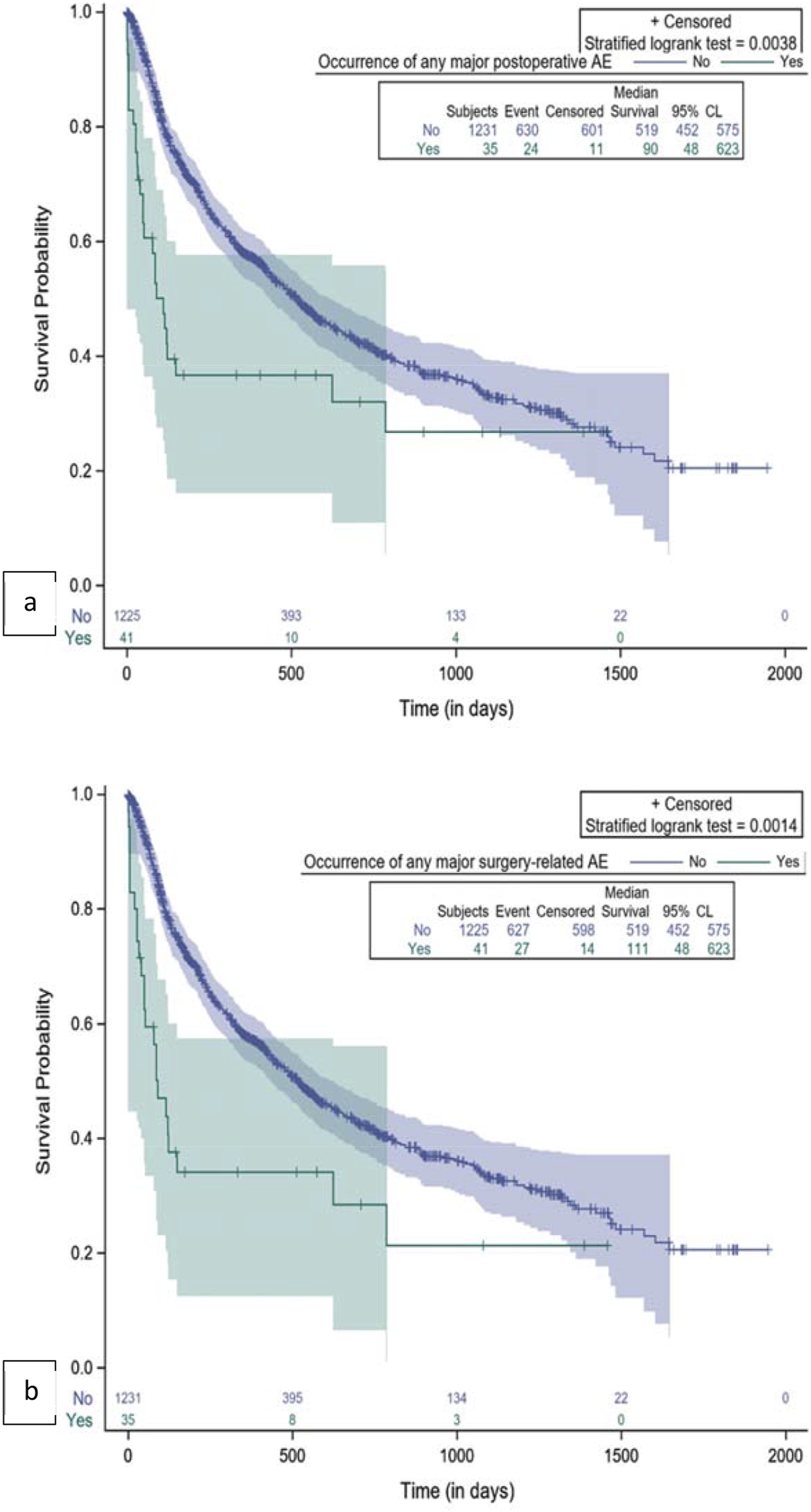
Any intraoperative AEs and major intraoperative AEs had no significant impact on survival (Figure 3A), while any postoperative AEs, and in particular major postoperative AEs, were significantly associated with shorter survival, as shown in Figure 3B and 4A. If we consider all surgery-related AEs, only major events had a significant association with survival time (Figure 4B. Patients without any major surgery-related AE had a median survival of 519 days (17.3 months) (95% CL: 452; 575). The occurrence of major surgery-related AEs was correlated with a significant decrease in survival (P = 0.0014), specifically a median survival of 111 days (3.7 months) (95% CL: 48; 623) (Figure 4B).
Cox Regression Models for Survival
Summary of Cox-Model for Survival With Occurrence of AEs as Input Variable.
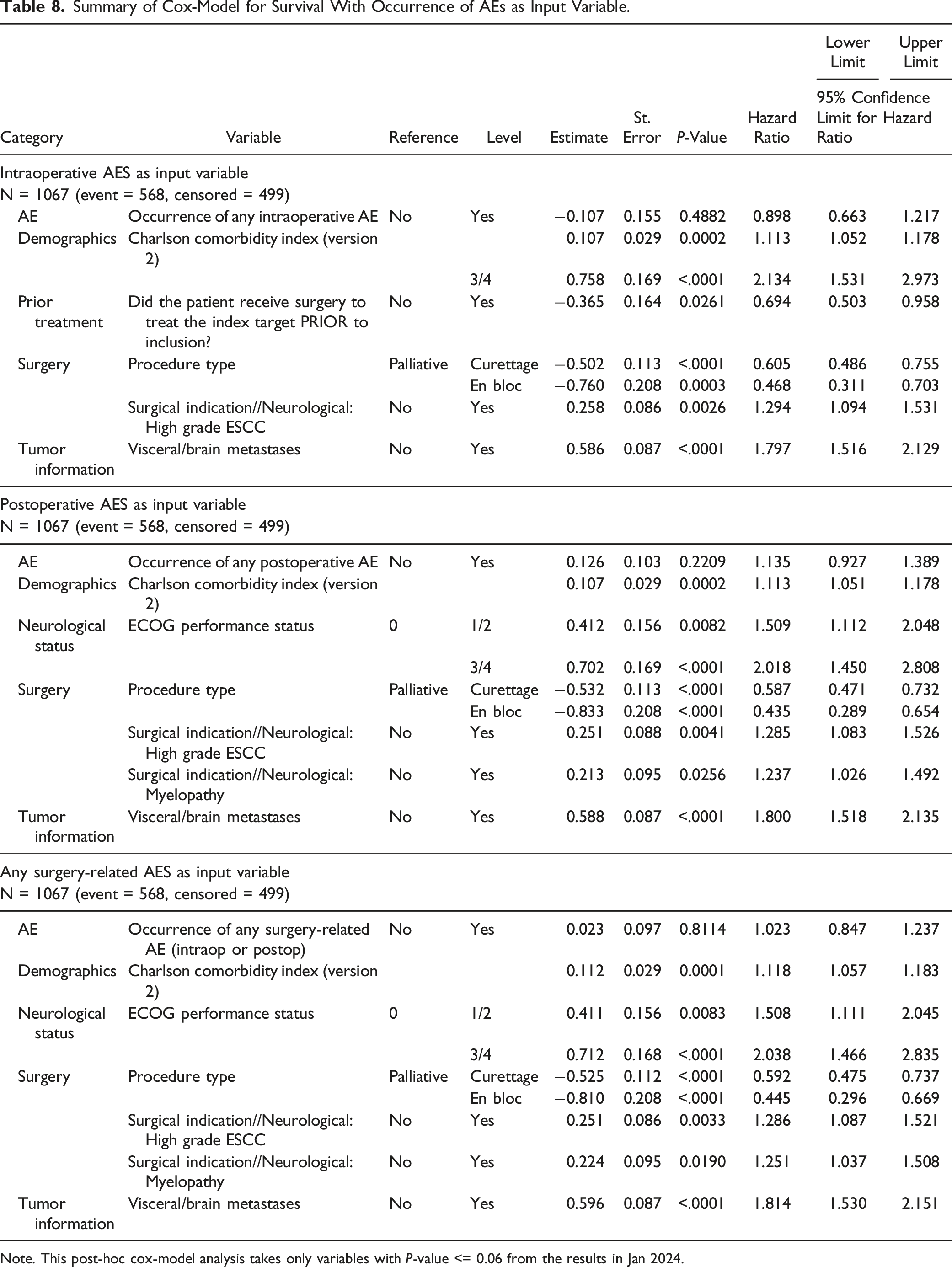
Note. This post-hoc cox-model analysis takes only variables with P-value <= 0.06 from the results in Jan 2024.
Impact of Surgery-Related AEs on Length of Hospital Stay
The impact of surgery-related AEs on patients’ length of stay (LOS) was evaluated by Kaplan-Meier analysis. As shown in Figure 5, both intraoperative and postoperative AEs during the hospitalization period were associated with longer LOS. The small number of AEs occurring after surgery and before patients’ discharge may have affected the results. Kaplan-Meier plot for comparison length of hospital stay by occurrence of AE. (A) Any intraoperative AE; (B) Any postoperative AE (within the hospitalization time).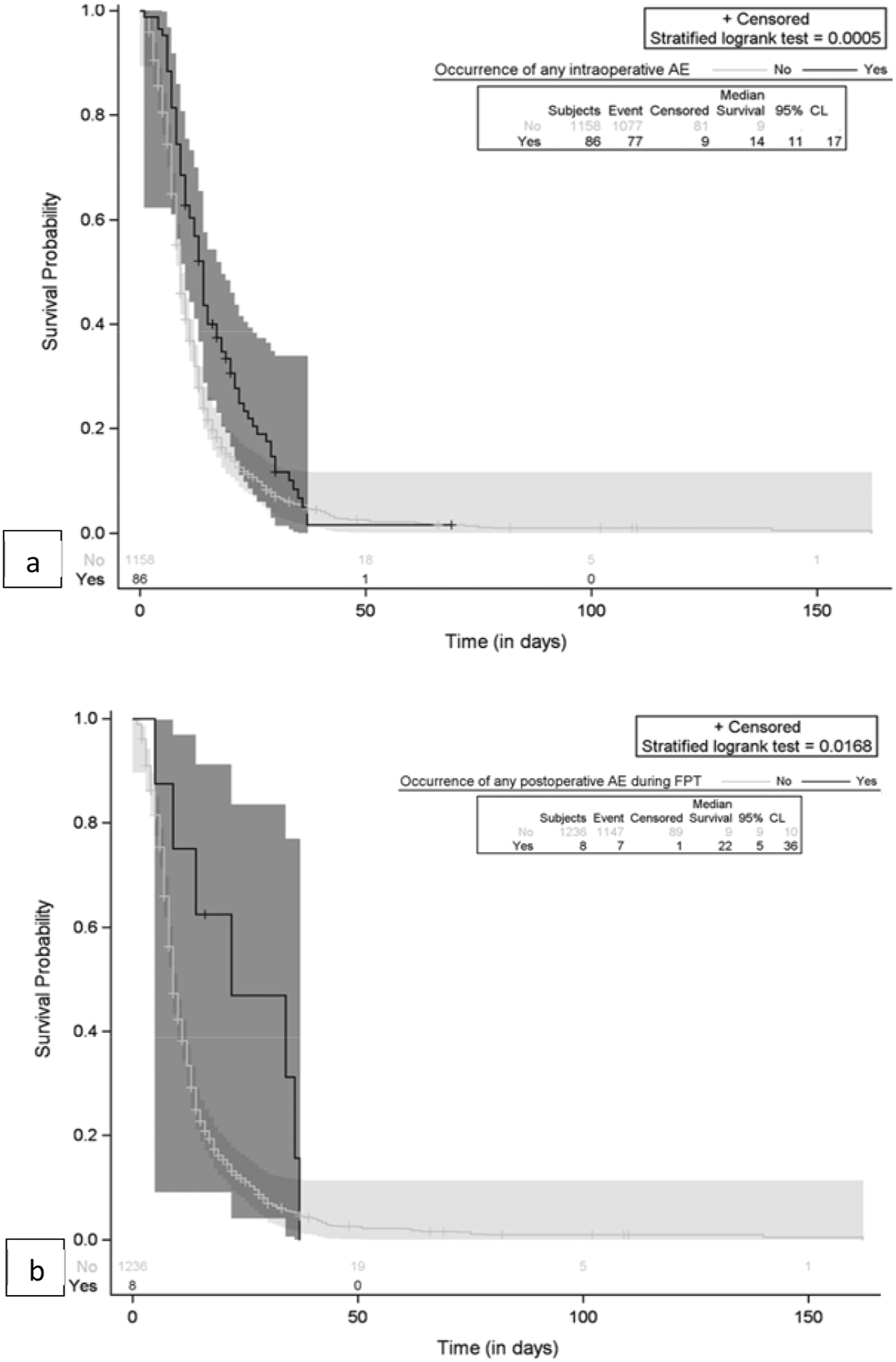
Cox Regression Models for Length of Stay
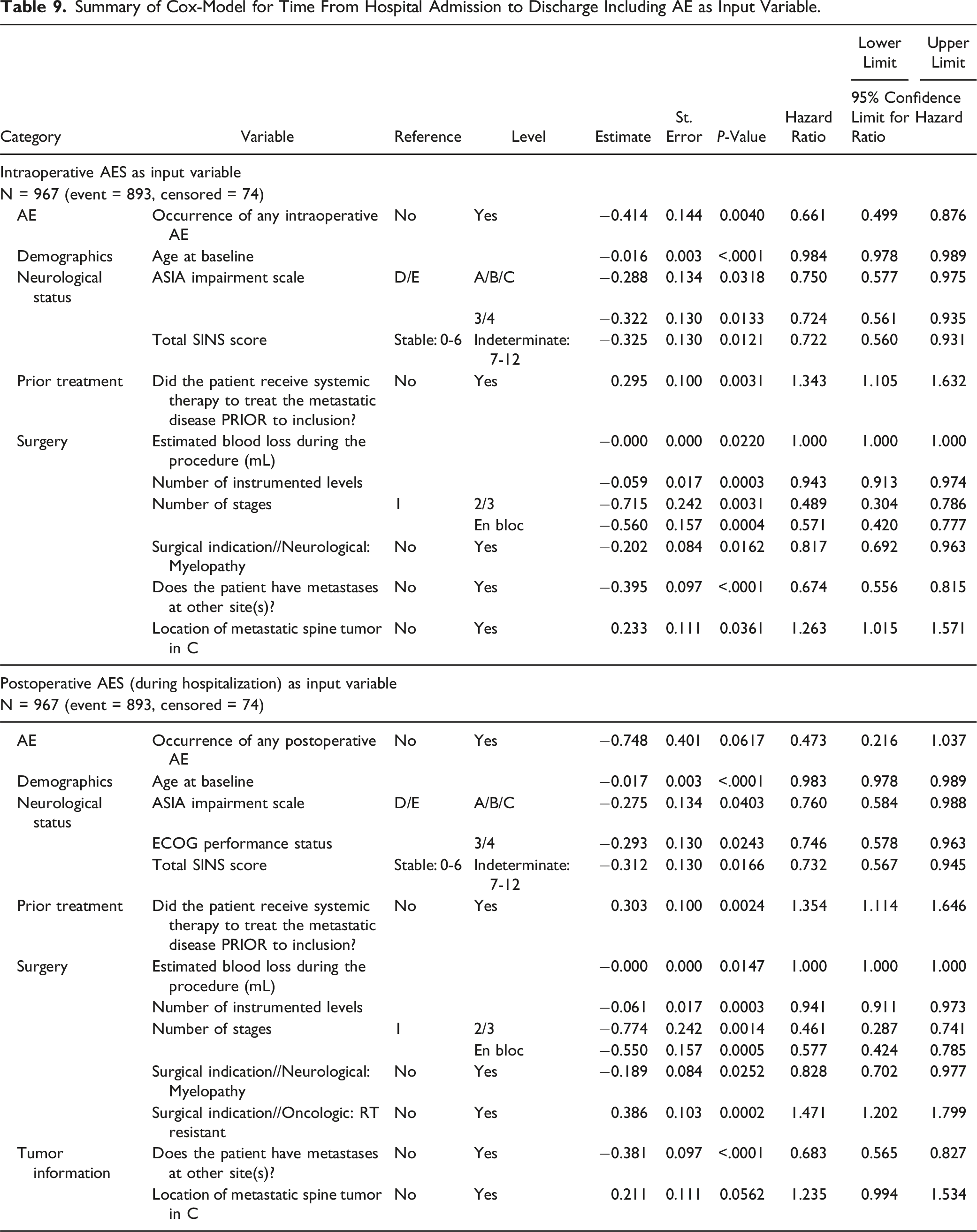
Summary of Cox-Model for Time From Hospital Admission to Discharge Including AE as Input Variable.
Effect of Surgery and AEs on Patients’ Quality of Life
The effect of surgery on HRQOL was evaluated by patient-reported outcomes measures (PROMs). In particular, EQ-5D and SOSGOQ questionnaires were self-administered, and the results obtained at baseline, 2 months follow up and 6 months follow up were compared. Moreover, the impact of AEs on HRQOL was analyzed.
As shown in Figures 6 and 7 and in Tables 10 and 11, both EQ-5D score and SOSGOQ total score significantly improved immediately after the surgery, and the improvement increased during the follow up period. The improvement of EQ-5D and SOSGOQ values immediately after the surgery was recorded also in the presence of intraoperative and/or postoperative adverse events, even if no significant increase was recorded between 2 months and 6 months FU (Tables 10 and 11). Mean EQ-5D scores by occurrence of AEs. (A) Intraoperative AEs; (B) postoperative AEs; (C) any surgery-related AEs. Mean SOSGOQ scores by occurrence of AEs. (A) Intraoperative AEs; (B) postoperative AEs; (C) any surgery-related AEs. Summary of EQ5D-3L Mean Values Including Standard Deviations and P-values by Occurrence of AEs. P values are calculated by t test. Bold values represent p < 0.05 (statistically significant). Summary of SOSGOQ Total Score Mean Values Including Standard Deviations and P-values by Occurrence of AEs. P values are calculated by t test. Bold values represent p < 0.05 (statistically significant).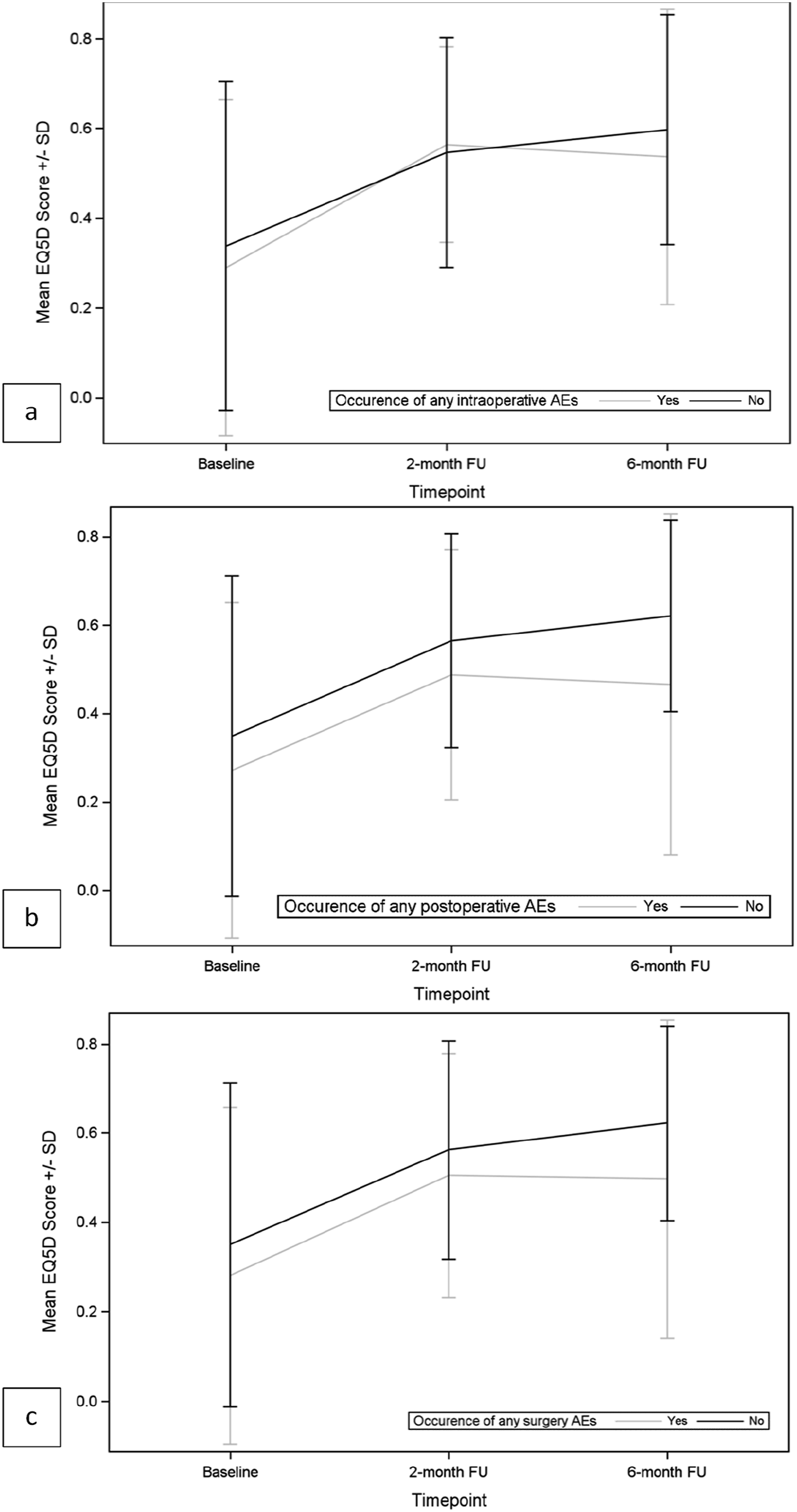
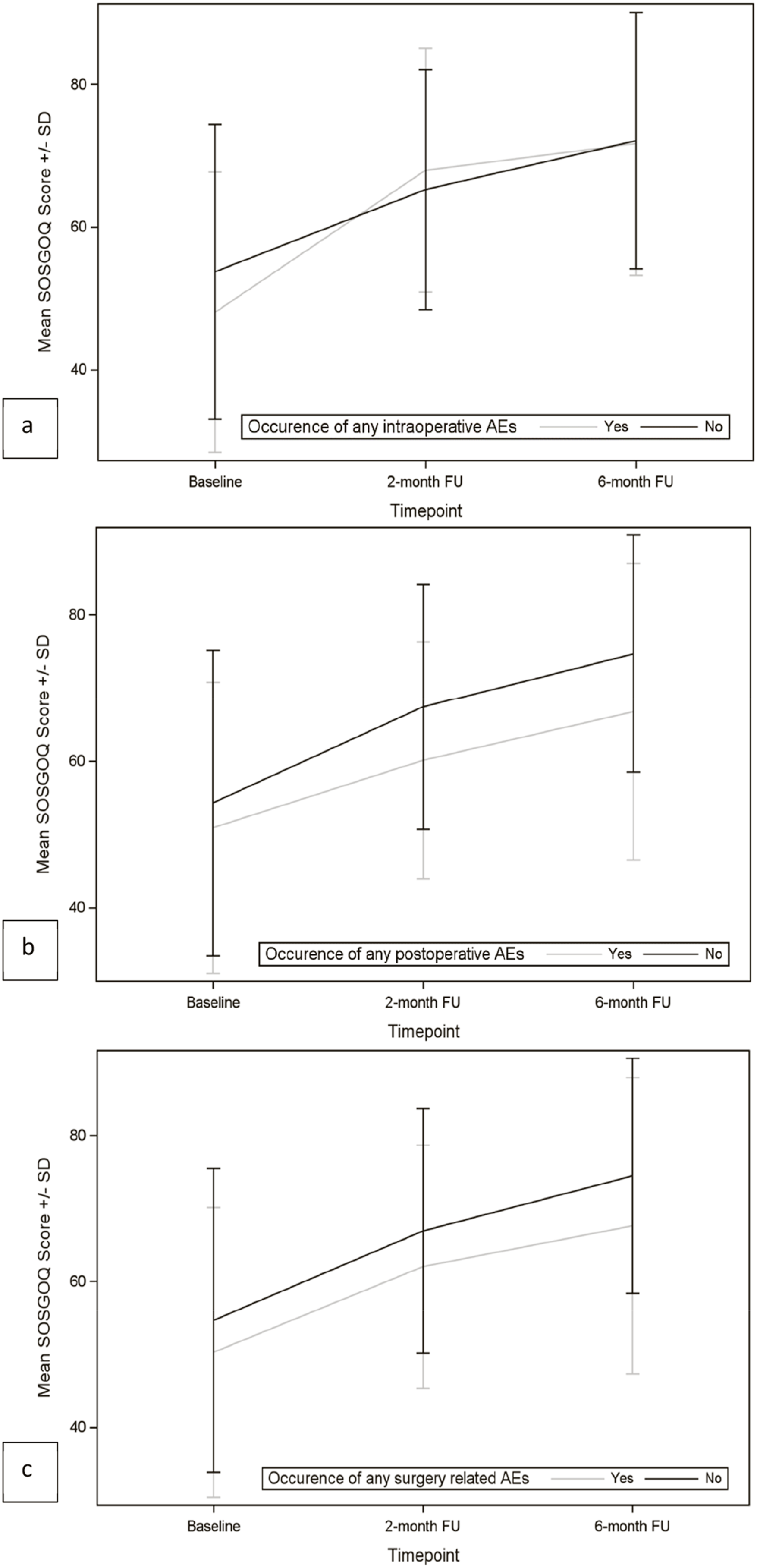
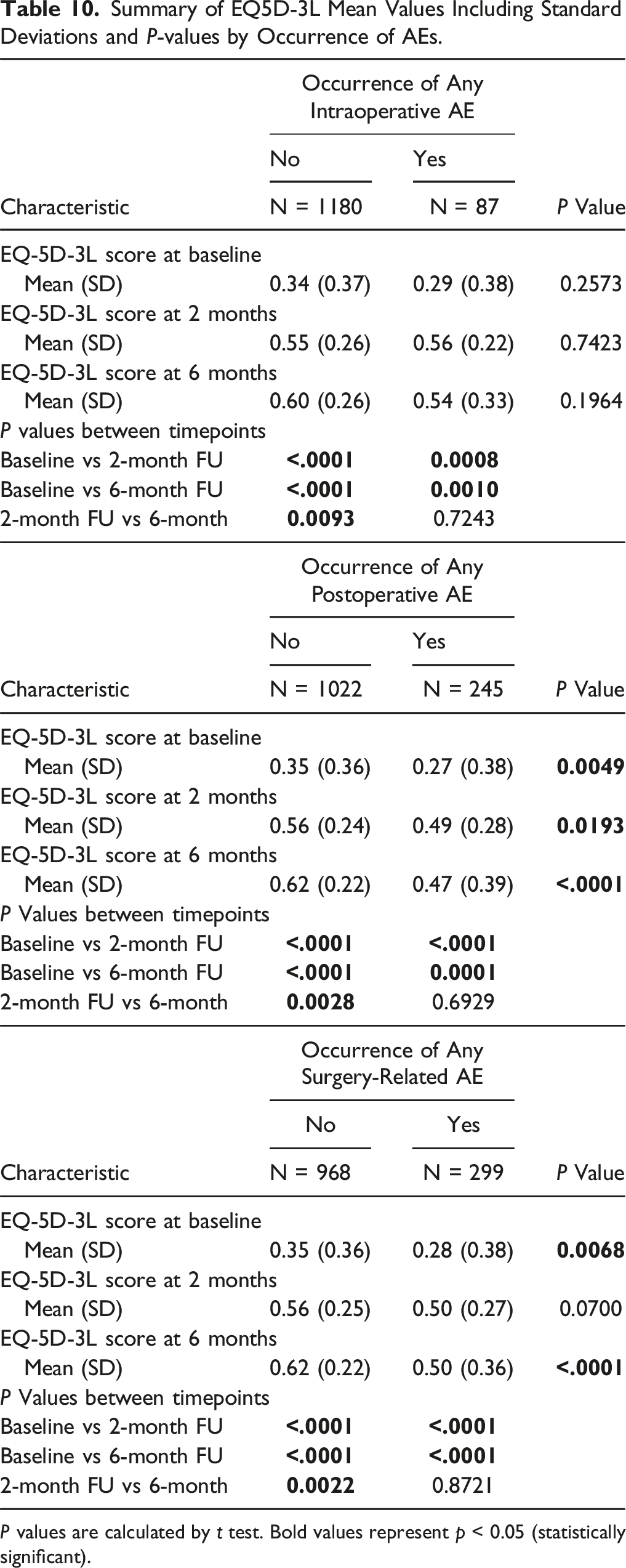
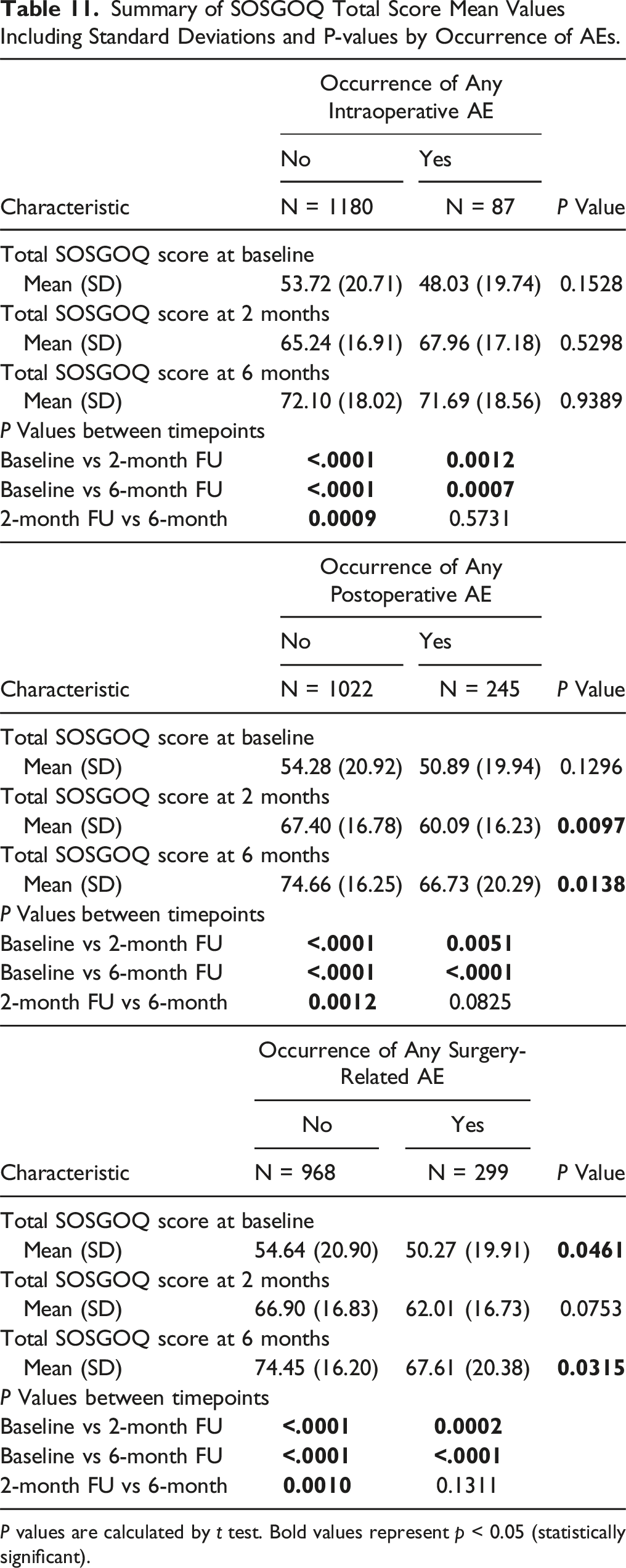
Comparing the mean values of EQ-5D and SOSGOQ scores between the 2 groups of patients with or without intraoperative AEs, we observed no significant differences at baseline and at follow-up timepoints (2 months or 6 months) (Tables 10 and 11). However, in the group of patients suffering postoperative or any surgery-related AEs, significantly different baseline values were detected for EQ-5D and SOSGOQ scores compared to the population without postoperative or any surgery-related AEs. The difference was confirmed also at follow-up timepoints (Tables 10 and 11).
Analyzing in detail the different domains of SOSGOQ (Supplemental Materials Table XVII), we observed a significant improvement for the Pain domain score, the Mental domain score and the Social domain score immediately after the surgery, and the improvement increased during the follow up period. The Physical function domain score improved starting from 2 months after surgery, while the Neurological domain score improved later, starting from 6 months FU. The occurrence of intraoperative AEs did not impair the trend of different SOSGOQ’s domain scores during time, while the occurrence of postoperative AEs significantly affected SOSGOQ’s domain scores during time, in particular the Neurological function domain and the Mental domain, where no significant improvements were registered after surgery and during follow up in the presence of postoperative adverse events.
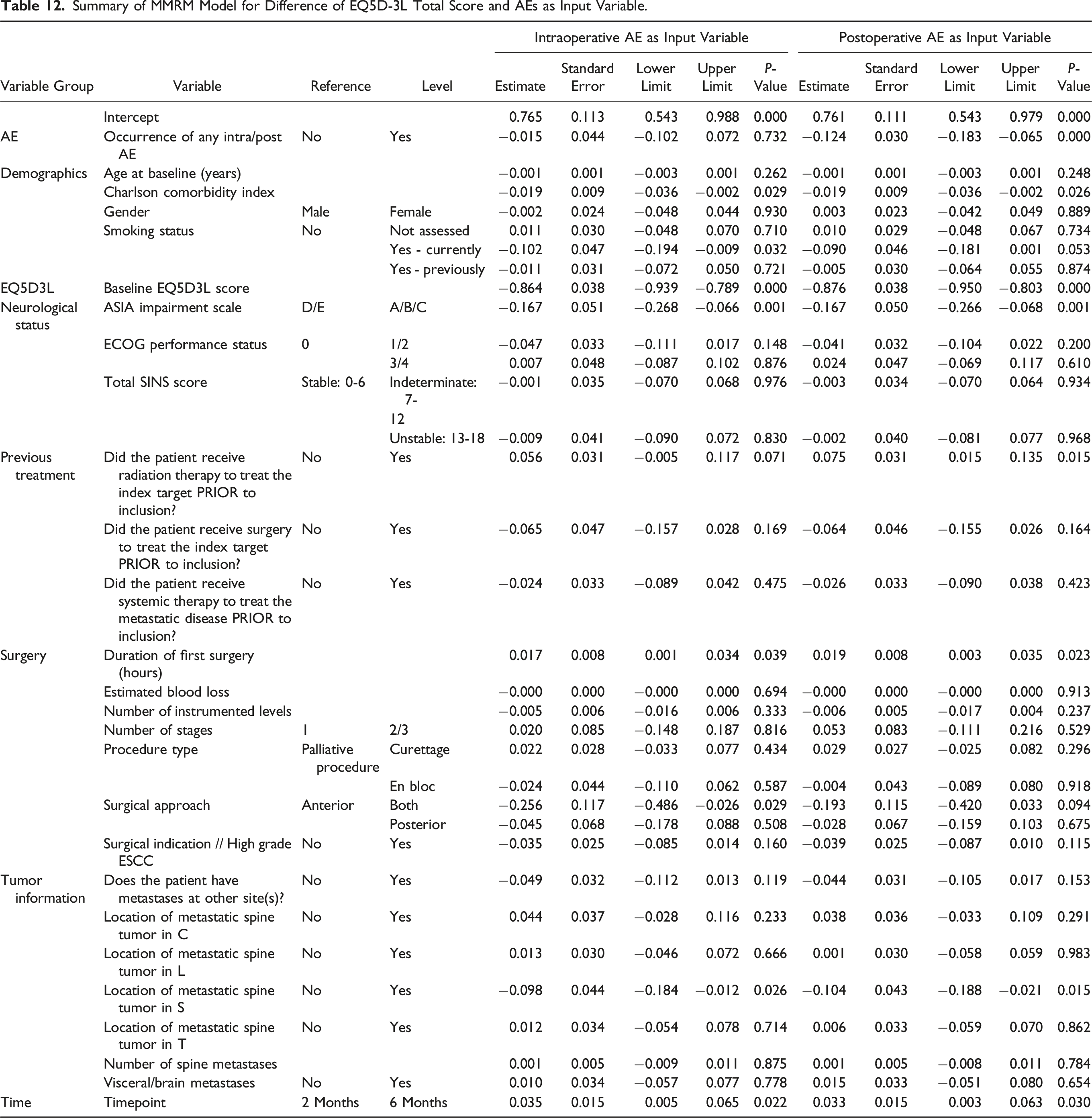
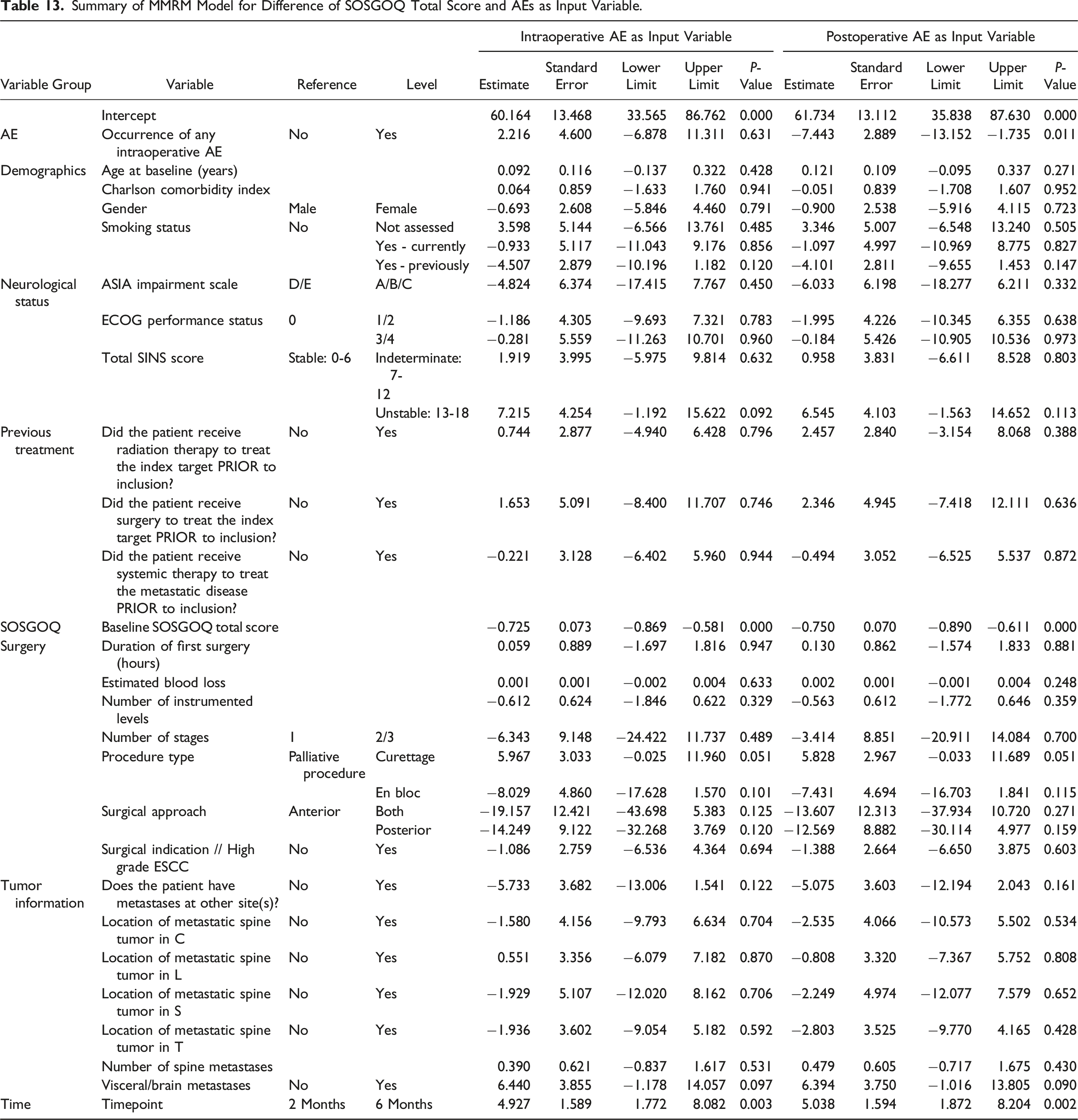
Analysis of Risk Factors for HRQOL Improvement by Mixed Models for Repeated Measures (MMRM)
Summary of MMRM Model for Difference of EQ5D-3L Total Score and AEs as Input Variable.
Summary of MMRM Model for Difference of SOSGOQ Total Score and AEs as Input Variable.
Discussion
In this large multicentric study, we analyzed data specific to AEs in a cohort of patients, who were predominantly potentially unstable, neurologically intact, with high grade epidural disease and good performance status, and underwent surgery for spinal metastases. Our focus was on the incidence and impact of both intraoperative and postoperative AEs. Importantly, we also examined the main clinical and procedural variables that could play a role in increasing the likelihood of AEs, their effect on quality of life and survival, and their influence on hospital length of stay.
Adverse Events and Risk Factors
The study revealed that, among the 1267 patients who underwent surgery for spinal metastases, 6.9% experienced intraoperative AEs, with unintended durotomy being the most frequent complication (3.5%). Most of these intraoperative events (92%) were minor (severity grade ≤3), indicating that intraoperative complications were relatively well managed within this cohort. The incidence of durotomy observed in our patient cohort aligns with existing literature, which reports an intraoperative durotomy incidence ranging from 2% to 16%.24,31-35
In this context, it is important to emphasize that patients with spinal metastases who undergo surgery for spinal metastases that were previously radiated show a significantly increased risk of dural tears 36 due to the presence of epidural fibrosis, adhesions, and dura thinning. In our cohort 24% of patients had a history of prior radiation at the index target.
Postoperative AEs were more common (19.3%) than intraoperative AEs and primarily consisted of deep wound infections, wound dehiscence, and urinary infections. Notably, patients with postoperative events were more likely to experience multiple AEs (37% of those with postoperative AEs). This finding is also consistent with the literature; in spinal surgery for tumors and metastases, wound infection is 1 of the most reported complications, with an incidence ranging from 1.5% to 30%.37-41 Such infections often lead to multiple reoperations, increased costs, prolonged disability, and, occasionally, sepsis or even death. 42 The clinical spectrum of wound infections is broad: they may be treatable with antibiotics alone, may require multiple wound debridement and revision surgeries, or may present with persistent dehiscence leading to sepsis and/or death.37-41 However, in our patient cohort, only 7/33 patients (21.2%) had a severe wound infection. As previously reported, cancer patients may frequently receive postoperative spinal radiation, and are potentially undergoing chemotherapy, all of which are risk factors for wound healing complications.43,44 In addition to radiotherapy and systemic therapies, other risk factors for wound infection include prior spinal surgeries, complex plastic reconstructions, an increasing number of comorbidities (in our study cohort, the Charlson Comorbidity Index was 6.44, range, 2-15), prolonged hospital stays, underlying neurological disorders, smoking, drug or alcohol abuse, underlying cardiac disorders (other than hypertension), diabetes, and obesity. 45
Through logistic regression models our study also found that intraoperative blood loss is a significant risk factor for intraoperative AEs, whereas several factors are associated with postoperative AEs, including age, smoking habits, ECOG performance status (score 3-4), prior radiation therapy, surgery duration, number of instrumented levels, multiple surgical stages, and simultaneous anterior and posterior approaches. These findings underscore the influence of both patient-specific clinical conditions and procedural complexity on the likelihood of postoperative complications. The identification of these risk factors is crucial as it can guide preoperative planning, help healthcare providers anticipate potential issues, and implement targeted strategies to improve patient outcomes and reduce complications.
Impact of AEs on Survival, Length of Stay and HRQOL
Concerning the impact of surgery-related AEs on survival, it was shown that intraoperative AEs, including major ones, do not significantly affect survival. However, as reported for other clinical studies, in this study postoperative AEs, especially major events, are significantly associated with reduced survival.22,46 In our study, patients without surgery-related AEs have a median survival of 524 days, while patients with major AEs show a survival reduction to 111 days. However, multivariable analyses suggested that the negative impact of postoperative AEs on survival could be associated with the presence of other factors having a significant impact on the survival of patients suffering from vertebral metastases: the presence of comorbidities, the poor ECOG Performance Status, the occurrence of a previous surgery to treat the index lesion (indicating presence of a recurrence), the neurological status (presence of high grade ESCC, presence of myelopathy), the presence of visceral/brain metastases. All these factors can create a frailty condition that (i) increases the risk of complications and (ii) impairs life expectancy. Moreover, the occurrence of complications can delay or prevent the possibility of adjuvant therapies (radiotherapy and systemic therapy), with consequent impact on survival.
Moreover, both intraoperative and postoperative AEs are also significantly associated with prolonged LOS. This effect on LOS is further confirmed by Cox regression models, where variables such as advanced age, spinal instability, neurological impairment (ASIA score A-C), and high ECOG performance status scores are also significant predictors of extended LOS. These results indicate that surgery-related complications can lead to a higher healthcare burden and extended hospitalization, which may have implications for patients’ recovery and quality of life and for healthcare costs.
The findings of this study also demonstrate that surgery significantly improves HRQOL, as measured by EQ-5D and SOSGOQ scores, with benefits becoming evident immediately after the procedure and continuing to increase over time. These results align with the existing literature, which consistently highlights the positive impact of surgical interventions on HRQOL for patients with complex conditions, such as metastatic disease or musculoskeletal tumors.47-49
However, the study also highlights a notable distinction between the impact of intraoperative AEs and postoperative AEs on patients’ HRQOL. Specifically, no significant differences were observed in the EQ-5D and SOSGOQ scores between patients with or without intraoperative AEs at baseline or at follow-up timepoints. This suggests that intraoperative AEs, at least within this cohort, may not have a detectable immediate or long-term effect on these HRQOL measures. Potential explanations include effective intraoperative management or a generally low severity of these events.
Conversely, patients who experienced postoperative AEs demonstrated significantly lower baseline EQ-5D and SOSGOQ scores compared to those without such events. This disparity persisted across follow-up timepoints, indicating a likely pre-existing vulnerability to postoperative AEs and a prolonged negative impact of these preoperative characteristics and the associated AEs on recovery trajectories. In other words, these patients not only started from a worse health status but were also more likely to experience a less favorable recovery process, highlighting the compounded burden of postoperative complications. 50 From a clinical perspective, these findings underscore the importance of preoperative risk stratification to identify vulnerable patients who may require tailored care to mitigate the risks of postoperative AEs.
Analyzing the specific domains of SOSGOQ provides a deeper understanding of these dynamics. The Pain domain, along with the Mental and Social domains, showed significant improvements immediately after surgery. These findings are consistent with reports by other authors51,52 who documented rapid improvements in pain and psychological well-being following surgical interventions for spinal metastases. In contrast, the Physical Function domain improved starting at 2 months post-surgery, while the Neurological domain only began to improve at 6 months, suggesting that some domains require longer recovery periods. The delayed improvement in the Physical Function domain reflects the time required for musculoskeletal healing and the gradual adaptation to physical rehabilitation. 53 The physical recovery process often involves wound healing, resolution of inflammation, and regaining strength and mobility, which take weeks to months. 54 The even later improvement in the Neurological domain, observed at 6 months post-surgery, suggests that nerve function recovery is a longer and more complex process. Neurological improvements are dependent on factors such as the duration and degree of preoperative nerve compression, the extent of decompression achieved during surgery, and the inherent regenerative capacity of the nervous system, which is often slow. 55 In cases where preoperative neurological deficits were severe, recovery may require extended periods for neural plasticity and regeneration to occur. 56
Using Mixed Models for Repeated Measures (MMRM), several baseline factors emerged as significant predictors of HRQOL improvement, independent of AEs. These included comorbidities, smoking status, baseline neurological impairment, longer surgery duration, and sacral metastases. Patients with more comorbidities or who smoked demonstrated less robust improvements, reflecting the broader detrimental effects of systemic health conditions and lifestyle factors on recovery. Longer surgeries and sacral metastases likely represent more complex clinical cases, which are inherently associated with more demanding surgeries and greater challenges in achieving optimal outcomes. Additionally, baseline neurological impairment was a strong determinant, as reflected in the burden on patients’ quality of life and prolonged recovery periods. These findings align with reports from the AO Spine Knowledge Forum Tumor, 57 which similarly highlighted the negative impact of comorbidities and smoking on surgical outcomes in cancer patients.
Highlights and Limitations
The results of this study provide a comprehensive analysis of AEs associated with spinal metastases surgery, offering important insights into the incidence, nature, and impact of both intraoperative and postoperative complications. The prospective collection of a large cohort of cases in different clinical centers around the world increases the variability and generalizability of results. However, although the broad sample increases the potential for generalization, it does not inherently eliminate biases that may arise from the study’s design and the intrinsic limitations of the registry. The main limitation of this study is the possibility of different recordings of AEs in clinical centers, the presence of missing data and “lost to follow up” that may cause an underestimation of the incidence of AEs. Moreover, although our regression models identified certain variables associated with an increased risk of AEs, we cannot establish direct causation. The association between specific variables, such as advanced age or comorbid conditions, and AEs does not exclude the possibility that other factors not considered in our study may contribute to the observed outcomes.
Despite these limits, this study highlights some relevant findings for the management of patients with spinal metastases. The surgical treatment, which is indicated to restore the neurological function, treat spinal instability and/or pathological fracture and improve quality of life, results in a high rate of adverse events, in particular postoperative AEs, that have a pronounced effect on patient recovery, quality of life, and survival. The findings underscore that postoperative AEs, especially severe ones, significantly reduce survival rates and adversely impact HRQOL, particularly in domains such as neurological function and mental health. However, our analysis also reveals that some parameters indicating a frailty status (comorbidities, poor ECOG Performance Status, presence of recurrences, impaired neurological status, presence of visceral/brain metastases) are associated to the occurrence of surgery-related AEs, suggesting that these factors can contribute to the effect of AEs on survival and quality of life.
This finding is relevant as it underscores the importance of an accurate preoperative assessment to identify vulnerable patients who are more likely to experience surgical complications with consequent impact on recovery, quality of life, and survival.
Strategies to minimize the incidence and severity of postoperative complications, such as precise surgical planning, effective wound management, and timely adjuvant therapies, are crucial. Additionally, integrating tailored rehabilitation programs and addressing mental health challenges in postoperative care can further enhance outcomes and recovery trajectories.
Conclusion
This large, multicentric study highlights the delicate balance required in treating complex conditions like spinal metastases, where the benefits of surgery must be weighed against the risks of complications. By identifying key risk factors for complications and their implications, this research underscores the importance of preoperative risk stratification to identify vulnerable patients who may require tailored perioperative care to mitigate the risks of postoperative AEs and their negative impact on survival and quality of life.
Supplemental Material
Supplemental Material - Evaluation of Adverse Events and the Impact on Health-Related Outcomes in Patients Undergoing Surgery for Metastatic Spine Tumors: Analysis of the Metastatic Tumor Research and Outcomes Network (MTRON) Registry Dataset
Supplemental Material for Evaluation of Adverse Events and the Impact on Health-Related Outcomes in Patients Undergoing Surgery for Metastatic Spine Tumors: Analysis of the Metastatic Tumor Research and Outcomes Network (MTRON) Registry Dataset by Giovanni Barbanti Brodano, Cristiana Griffoni, Francesca Salamanna, Luigi Emanuele Noli, Annalisa Monetta, Alessandro Luzzati, Alexander C. Disch, Aron Lazary, Ori Barzilai, Ilya Laufer, Ziya L. Gokaslan, Michael G. Fehlings, Jorrit-Jan Verlaan, Dean Chou, Laurence D. Rhines, John H. Shin, William G. J. Teixeira, Daniel M. Sciubba
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was promoted and funded by AO Spine through the AO Spine Knowledge Forum Tumor, a focused group of international spine tumor experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research and the AO Innovation Translation Center, Clinical Evidence.
IRBs Approval Numbers
Universitätsspital Basel, Basel, n. 2018-00129; Johns Hopkins University School of Medicine, Baltimore, n. CR00036868/IRB00150703; Massachusetts General Hospital, Boston, n. 17-144; Istituto Ortopedico Rizzoli, Bologna, n. 0007178 / 439; National Center for Spinal Disorders, Budapest, n. 10848-2/2018/EKU; Universitätsklinikum Cal Gustav Carus, Dresden, n. EK 61022017; Duke University Medical Center, Durham, PRO00102543 (Reference ID: 315416); The University of Texas M.D. Anderson Cancer Center; Houston, n. PA18-0742; Kanazawa Medical University, Kanazawa, n. 1234; Monash University, Melbourne, n. 17-0000-469A; Istituto Ortopedico Galeazzi, Milano, n. 265/2017; McGill University Health Centre, Montreal, n. 2018-3949; Memorial Sloan-Kettering Cancer Center, New York, n. 18-153; Philadelphia, n. 827848; Brown University, Providence, n. RIH IRB 1-00000396, RIH IRB 2-00004624, TMH IRB -00000482; Mayo Clinic, Rochester, n. 16-009684; University of Rochester Medical Center, Rochester, n. RSRB00067541; Rush University Medical Center, Chicago, n. 16112101-IRB02; National University of Singapore, Singapore, n. NUH/2017/0006; Instituto do Cancer do Estado Sao Paulo, Sao Paulo, n. 26813119.5.0000.0065; Toronto Western Hospital, Toronto, n. 16-6225; Sunnybrook Health Sciences Center, Toronto, n. 336-2017; The UCSF Spine Center University of California, San Francisco, n. 17-22044; Universitair Medisch Centrum Utrecht , Utrecht, n. 18-314/C; UBC, Vancouver General Hospital , UBC, Vancouver General Hospital, Vancouver, n. H17-00283; Valhalla, n. 12410; Winnipeg, n. HS21103 (H2017:292).
Ethical Statement
ORCID iDs
Data Availability Statement
Data are collected in a secured RedCap database under the supervision of AO Network Clinical Research and the AO Innovation Translation Center, Clinical Evidence.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.