
Abstract
Study Design
Retrospective observational cohort study.
Vertebral body collapse with subsequent kyphosis, compression of neural structures usually requires surgical treatment; spinal fixation, corpectomy, decompression and realignment of the spine.
The objective was to present results of corpectomies using a unilateral minimally invasive posterolateral transpedicular approach (MITPA) in patients with metastatic or posttraumatic kyphosis.
Material and Methods
The study included 28 patients: 23 with osteolytic vertebral body metastases, 5 posttraumatic kyphosis. All patients were operated by 2 surgeons, all had percutaneous pedicle fixation and unilateral single-level corpectomy using MITPA, followed by insertion of an expandable cage. Perioperative parameters were noted and radiological analysis based on CT performed before, after surgery and on the last follow up in 12 months.
Results
The mean age of patients was 62 years, average length of surgery 263 min, with mean EBL 648 mL and average length of hospital stay 9.3 days. The local kyphosis, measured on end-plates of adjacent vertebrae, was corrected by 14.3° (from 13.1° [±9] to −1.2° [±8], P < .05). Complications occurred in 11 patients (39%), most of them minor, only 2 complications were major (7%): 1 deteriorated neurological deficit and 1 deep vein thrombosis. In 8 cases of preoperative paresis, 7 showed postoperative neurological improvement. In 12 months follow up, no serious mechanical complications were observed, beside minor cage subsidence in 5 cases and adjacent vertebral fracture. The anterior fusion was noted in all cases followed.
Conclusions
MITPA corpectomy allows for significant correction of kyphosis, both in metastatic and posttraumatic vertebral body collapse with relatively low rate of major complications.
Introduction
Vertebral body resection, also known as corpectomy, is often necessary when the vertebral body is significantly damaged and cannot adequately support the anterior spinal column or transfer loads. This condition can lead to deformity, instability, or spinal cord compression, which can have serious consequences. Vertebral body destruction is most commonly observed in patients with spinal tumors, traumatic injuries, or infections.
Vertebral body resection is an extensive surgical procedure that carries a high risk of complications and often requires a long recovery period for patients.1,2 This extended recovery can be particularly detrimental for cancer patients with metastases in the spine, as open, invasive surgery may disrupt ongoing oncological treatments.3,4 For these patients, minimally invasive techniques may facilitate and speed up the implementation of systemic cancer treatment and radiotherapy following surgery.
The main principles of minimally invasive surgery (MIS) aim to achieve the same objectives as open surgery but with reduced tissue damage and less surgical trauma. Research indicates that minimally invasive spinal procedures are associated with less blood loss, fewer healing complications, lower rates of infection, and faster recovery times. However, these procedures may also carry a higher risk of non-union, a steep learning curve for surgeons, and increased intraoperative radiation exposure.5,6
The combined anteroposterior approach to vertebral body excision is very extensive and risky procedure. 7 Therefore, a single approach is recommended whenever possible. The posterior transpedicular corpectomy has been documented in the literature, and it can also be performed using minimally invasive or mini-open techniques, each with its own benefits and drawbacks.8,9 Many authors have demonstrated the advantages of minimally invasive or mini-open surgery compared to traditional open surgery. These benefits are particularly significant for cancer patients due to their need for further treatment.10-12
Previously described minimally invasive transpedicular corpectomies have used a posterior midline approach to access the spinal canal through laminectomy.9,13 While this method allows for extensive decompression and provides a clear view of the spinal canal, it presents challenges when accessing the vertebral body and positioning the cage, especially when the dura cannot be retracted.
In this paper, the authors present the results of corpectomies with unilateral minimally invasive posterolateral transpedicular approach (MITPA) performed on a consecutive series of patients with vertebral body collapse and local kyphosis, whether due to trauma or a metastatic osteolytic process.
Methods
The study included 28 patients who underwent the procedure between January 2020 and October 2022. All procedures were performed by 2 surgeons from the same institution using the exact same technique.
The indications for the surgeries included osteolytic lesions due to neoplastic metastases in 23 patients, and spinal fractures with vertebral body collapse in 5 patients. The reason for performing corpectomy with Minimally Invasive Transforaminal Percutaneous Approach (MITPA) in all patients was local kyphosis resulting from traumatic or metastatic destruction of the vertebral body, which caused an improper spinal profile that required realignment (Figure 1A–C). Illustrative case. Patient with metastasis to the spine from breast cancer; presented with weakness of both legs, right sided more pronounced, mild urinal incontinence, severe back pain. (A) and (B) MRI scans showing pathological fracture of L1 vertebral body due to osteolytic process, significant canal encroachment with conus medullaris compression by tumour masses. (C) CT scans obtained prior to operation, showing L1 wedged vertebral body. Yellow lines show measurement of local kyphosis (130), red - regional kyphosis (100). (D) CT scans after surgical realignment of the spine, decompression of spinal canal, percutaneous transpedicular fixation with cement augmentation, MITPA corpectomy with implantation of expandable PEEK cage. Yellow - local lordosis (120), red - regional lordosis (120), correction by 250 and 220 respectively.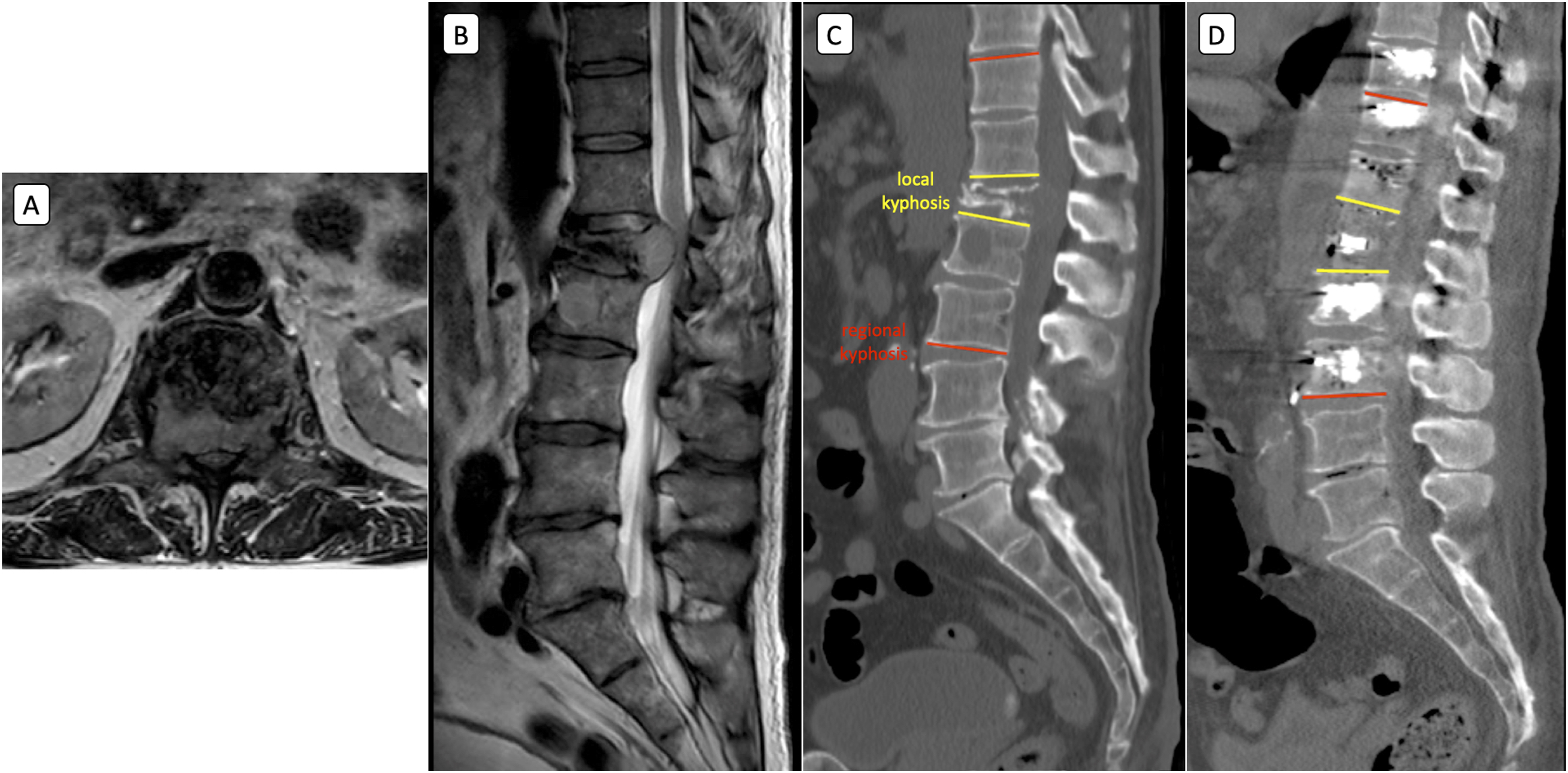
All patients diagnosed with metastases had their Spinal Neoplastic Instability Score (SINS) calculated. Patients undergoing multilevel corpectomies and bilateral MITPA were excluded from the study. Authors analyzed perioperative parameters; length of the procedure, estimated blood lose (EBL), radiation but also complications which occurred up to 12 months postoperatively. The main radiographical analysis was based on CT scans performed preoperatively and early postoperatively. Local kyphosis was defined as an angle between end plates of adjacent vertebral bodies to fractured/collapsed vertebra (Figure 1C), and regional kyphosis – angle between end plates of vertebral bodies 2 levels below and 2 levels above. The same way after kyphosis restoration (Figure 1D). Analysis was done separately for corpectomies in thoracic spine T1-T9 (13 patients), thoracolumbar junction and lumbar spine T10-L5 (15 patients). On the last follow up in 12 months CT scans were obtained and fusion and implant integrity was assessed.
Technical Description of the Procedure
The surgery was performed with the patient in a prone position. The first step involved the percutaneous insertion of pedicle screws, followed by cement augmentation of the screws if necessary, particularly for patients with known or suspected decreased bone quality. On the contralateral side to the planned excision, a rod was inserted and fixed in place using set screws. Next, a paracentral longitudinal skin incision was made between the extenders of the screws at the required level. After incising the fascia, the paraspinal muscles were split, exposing the facet joint, lamina, and transverse process (TP) on one side. Following the removal of the TP and paraspinal rib, the lateral wall of the affected vertebral body was dissected, typically to the medial line anteriorly. A protective spatula was inserted in front of the spine. Facetectomies of the upper and lower facets were performed, along with a hemilaminectomy, and the pedicle was removed down to the level of the vertebral body. Then, the vertebral body was removed in a piecemeal fashion, and a PEEK expandable cage was inserted. The cage was then distracted to achieve stable fixation with the end plates (see Figure 2A and B). If needed, the set screws of the contralateral rod were loosened to facilitate this maneuver. Occasionally, nerve roots were ligated (from T2 to L1) to create additional space for inserting the vertebral body cage. Intraoperative pictures. Percutaneous pedicular fixation, with left sided rod mounted, right sided MITPA for L1 corpectomy with vertebral body reconstruction with PEEK expandable cage. (A) General view of the surgical field, (B) magnification of MITPA.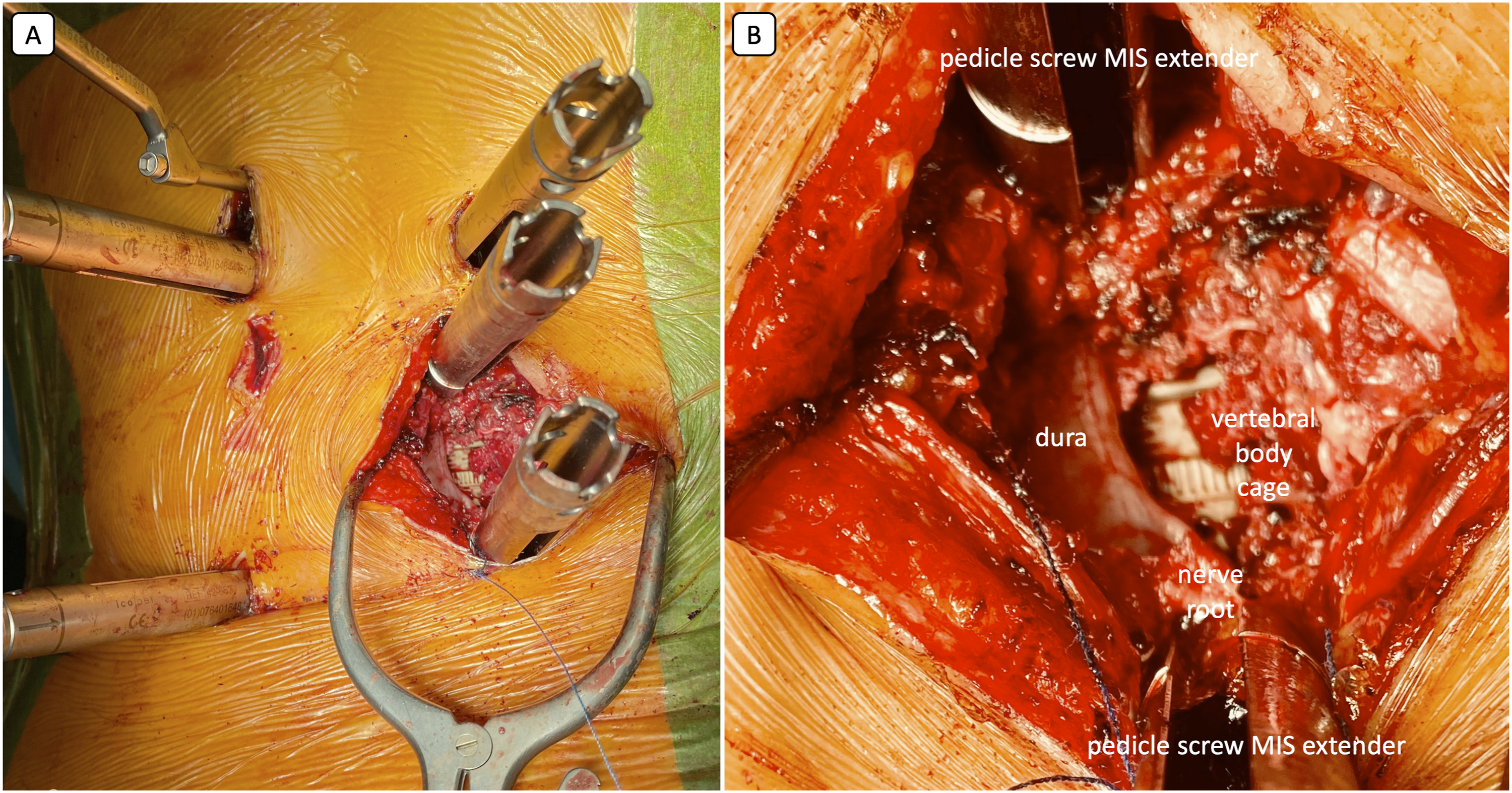
Data were presented as means with standard deviation (±), along with ranges in brackets when available. Statistical analyses were performed to compare groups using the Student’s t-test If there was a lack of homogeneity in variance and/or the data did not follow a normal distribution (P > .05), the Mann-Whitney test was employed instead of the Student’s t-test. A P-value of less than .05 was considered statistically significant.
Informed consent from the patients included in the study was not obtained, as the study design was retrospective. The study protocol was approved and registered by the Bioethics Committee of Wroclaw Medical University (KBkanc. 172/2024) and was conducted in accordance with the principles of the Helsinki Declaration.
Results
Among 28 patients who underwent minimally invasive corpectomies with percutaneous pedicle screw fixation, 5 had post-traumatic kyphosis, while 23 presented with metastasis and pathologic vertebral body fractures. The mean age of the patients was 62 years, with a range from 18 to 76. The group included 15 men (12 with tumors and 3 with trauma) and 13 women (11 with tumors and 2 with trauma).
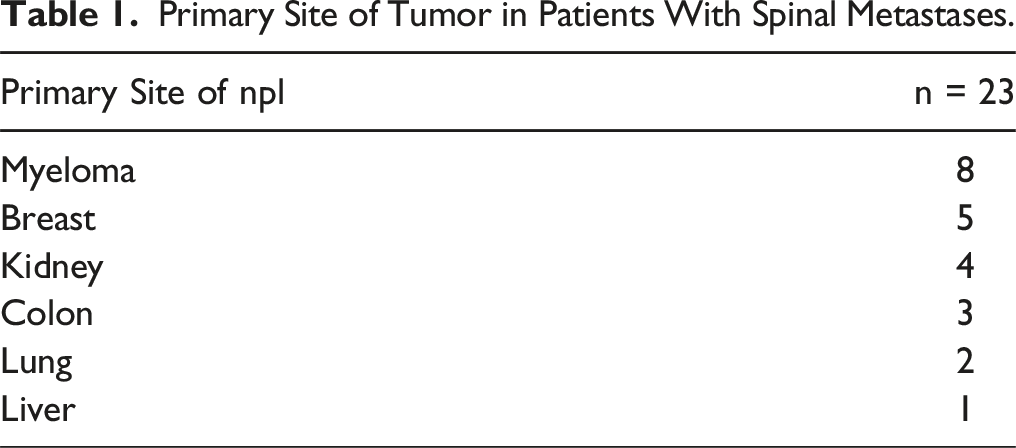
Primary Site of Tumor in Patients With Spinal Metastases.
The average SINS (Spine Instability Neoplastic Score) in this group was 14.3. Two patients had indeterminate stability of the spine according to the SINS criteria, scoring 11 and 12 points, while the remaining patients were classified as unstable with SINS scores of 13 and above.
Perioperative Characteristics.

Radiographic Parameters; Bold P Values Indicate Statistical Significance.

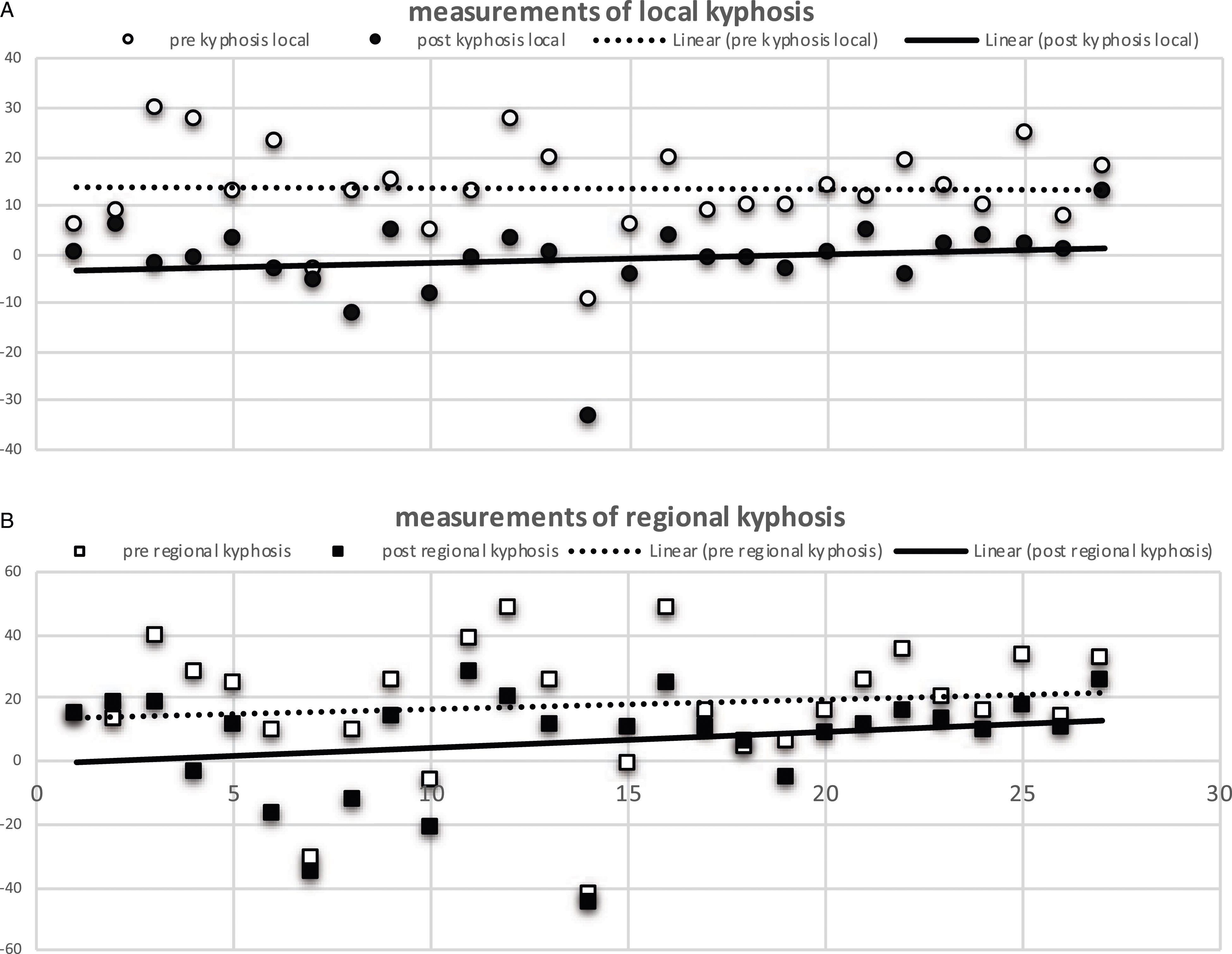
Measurements of local (A) and regional (B) kyphosis. The higher number the bigger kyphosis, 0 indicates neutral, parallel endplates, numbers with minus stand for lordosis.
Complications.
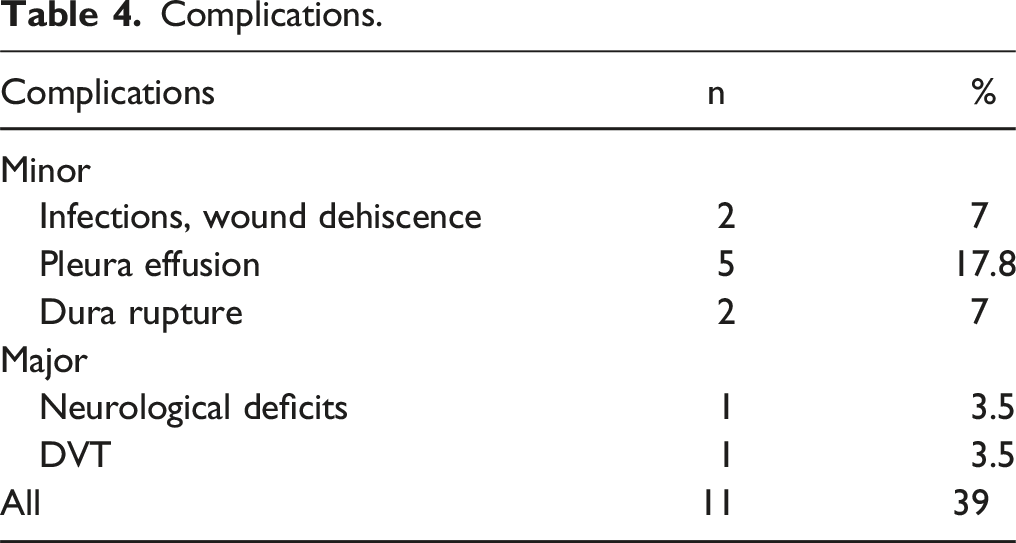
Out of 8 cases of preoperative paraparesis (6 patients grade D and 2 grade C according to the ASIA scale), 7 patients improved to ASIA E at follow-up. Only one patient from the trauma group had a neurological deficit (ASIA C), which fully resolved to grade E. However, one case showed a deterioration in neurological status; this patient had preoperative paraparesis (ASIA D) and developed paraplegia (ASIA A) on the second day post-surgery.
Six patients were lost to follow-up after 12 months, all of whom had metastases, with 4 confirmed deaths due to metastatic disease. We did not observe any implant failures, including breakage, loosening, or cage migration. There was only minor cage subsidence in 5 cases (up to 2 mm), which did not affect the spinal profile. One patient experienced an adjacent fracture 6 months post-surgery, which was managed with vertebroplasty. No other surgical revisions were necessary, and signs of anterior fusion were noted in all cases.
Discussion
In this series of patients with kyphotic deformity resulting from traumatic or metastatic vertebral body collapse, the authors described the technique and demonstrated the results of minimally invasive transpedicular posterolateral corpectomy (MITPA). The data presented shows a positive overall outcome, a relatively low complication rate, an improvement in spinal alignment, and satisfactory spinal canal decompression, with most patients experiencing significant improvements in neurological function.
The authors highlighted the effectiveness of MITPA corpectomy technique for restoring proper spinal alignment, indicating that the correction of kyphosis achieved in this study is better or comparable to that seen with open surgical methods described in existing literature. Specifically, Rustagi et al and Joubert et al reported an average kyphosis improvement of 6.5° degrees with open procedures, while this series achieved a mean correction of kyphosis of 11° degrees.14,15 There is currently no available literature showing the restoration of spinal alignment in corpectomies using minimally invasive techniques. To our knowledge this is the first report documenting kyphosis correction using these techniques.
In this series, the authors reported a relatively high overall complication rate of 39%. However, most of these complications were minor; only 7% (2 patients) experienced major complications. In contrast, studies on open transpedicular corpectomies have reported higher rates of major complications: 11% according to Rustagi et al and 14% according to Wang et al, while minor complication rates were similar, ranging from 24% to 39%.12,14,16 Lau and Chou, in their mini open case series, reported a surprisingly low complication rate of 7%, which included only 2 wound infections. This rate is significantly lower than what is found in the literature and the data presented in this paper, although it is worth noting that their series was smaller than the current one.9,13 Minor complications were reported in this paper, however these did not impact the systemic oncologic treatment or significantly affect the overall outcomes for the patients. The pleural effusions observed were likely associated with rib removal and were probably due to irritation of the pleura during the procedure. The authors currently prefer to perform rib osteotomies instead of rib resections when possible; however, the available corridor for cage insertion is not always adequate, making rib removal necessary at times.
The average length of the operation reported in this article was 263 min (4.3 h). This duration is shorter or at least comparable to other studies, such as Lau’s report of 7.5 h (452.4 min), Zhou’s et al 5.9 h (354 min), and Alshareef’s et al 4.6 h. It is also significantly shorter than traditional open procedures; Lau et al reported 6.8 h and Alshareef et al 6 h of surgery.12,13,17
The mean estimated blood loss (EBL) in this study was 648 mL, which is quite low given the extensive nature of the procedure. At our institution, all highly vascularized tumors are embolized prior to surgery; in the group presented, only 4 patients with renal tumor metastases underwent the procedure. Our results indicated significantly less blood loss compared to what has been reported in open corpectomies: Alshareef et al reported an EBL of 1600 mL, Lau et al reported an EBL of 1925.8 ± 1530.1 mL, and Rustagi et al reported 2000 mL. Furthermore, our EBL was even lower than that observed in minimally invasive techniques reported by other surgeons: Alshareef et al documented an EBL of 900 ± 800 mL, Lau reported 1150.0 ± 716.6 mL, and Zhou noted an EBL of 1416.94 mL.12-14,17
Corpectomy is an extensive surgical procedure that typically requires a long recovery period and an extended hospital stay, which can be particularly undesirable for cancer patients. Patients who underwent MITPA for corpectomy had an average hospital stay of 9.3 days, significantly shorter than that associated with open surgery. This duration is comparable to data reported by Lau (7.1 ± 3.5 days) and Zhou (9.28 ± 6.28 days).12,13
As it is a MIS procedure, a certain amount of radiation is necessary. In this study, the average radiation exposure was 42 mGy; however, in one case, the radiation levels reached as high as 121 mGy, which is quite excessive. There are currently no available reports on minimally invasive corpectomies and intraoperative radiation. However, numerous articles comparing open and MIS methods have noted an increase in radiation exposure with the latter. 6 So far, at the authors’ institution, fluoroscopy has been the primary method used for these procedures. Nevertheless, the authors are considering the use of navigation technology to reduce radiation exposure for the theatre staff.
We observed significant improvement in neurological recovery among all patients with primary deficits, except for one who experienced deterioration (7 improved, 1 deteriorated). All the patients who improved were able to walk at the 3-month follow-up after surgery. The one patient who deteriorated developed paraplegia on the second postoperative day, likely due to decreased spinal cord perfusion related to drops in mean arterial pressure (MAP).
Previously described minimally invasive spinal transpedicular corpectomies were based on accessing the spinal canal through the posterior midline with a laminectomy.9,12,13,18 The paramedian skin incision and oblique posterolateral trajectory towards the spinal canal, pedicle, and vertebral body through hemilaminectomy allowed for better handling of the spinal cord, eliminating the need for retraction or any manipulations to the dural sac. MITPA provides visualization of the contralateral side of the spinal canal and vertebral body - tilting the table contralaterally, undercutting the contralateral lamina, in an over-the-top decompression fashion allows access to the other side of the spinal canal but also vertebral body from the inside. The authors have demonstrated that this modified technique enables effective decompression and facilitates the placement of a vertebral body cage.
Authors currently regard this technique as a mainstay treatment for patients with vertebral body destruction. They consider corpectomy with MITPA as an extension of separation surgery for patients with tumors. At their institution, this procedure is offered to patients who show a better prognosis and have experienced significant collapse of the vertebral body, accompanied by kyphotic deformity.
However, there are limitations to this study. The analyzed group is relatively small and not homogeneous, comprising patients with both tumors and trauma. Additionally, the study design is retrospective with a limited duration of observation. Therefore, there is a clear need for longer-term observation and further research on this technique, particularly in comparison to open procedures or minimally invasive anterior corpectomies with posterior pedicle fixation.
Conclusions
The minimally invasive posterolateral transpedicular approach (MITPA) for thoracolumbar corpectomy provides significant correction of kyphosis in cases of both metastatic and posttraumatic vertebral body collapse, with a relatively low rate of major complications. Compared to open procedures, MITPA significantly enhances patient recovery, resulting in less blood loss, shorter operation times, and reduced hospital stays. This is especially important for oncology patients who need to undergo additional radiotherapy or systemic treatments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.