
Abstract
Study Design
Cross-sectional study.
Objective
To examine the association between SIRI and spinal BMD and assess the influence of age, hypertension, and diabetes.
Methods
We analyzed data from 13,950 participants aged ≥20 years. SIRI was calculated using neutrophil, monocyte, and lymphocyte counts, and spinal BMD was measured by DXA. Linear regression, generalized additive models, and segmented regression were used, with subgroup analyses based on age, hypertension, and diabetes.
Results
A threshold effect was observed at SIRI = 0.68. Below this threshold, SIRI negatively correlated with spinal BMD (β = −0.0412, P = 0.0494), while above it, a positive correlation was found (β = 0.0079, P < 0.0001). Subgroup analyses showed stronger positive associations in older adults (≥65 years, β = 0.0136, P < 0.0001), and those with hypertension (β = 0.0089, P = 0.0004) and diabetes (β = 0.0187, P < 0.001).
Conclusion
A segmented nonlinear relationship exists between SIRI and spinal BMD, with age, hypertension, and diabetes as significant modifiers. SIRI may serve as a biomarker for osteoporosis risk.
Keywords
Introduction
Osteoporosis is a prevalent global public health issue, particularly among older adults, 1 leading to increased risks of fractures, restricted mobility, and a substantial decline in quality of life, thereby placing a significant burden on patients, families, and health care systems.2-6 As a crucial indicator of bone health, spinal bone mineral density (BMD) is not only a primary criterion for diagnosing osteoporosis but is also directly linked to fracture risk. Understanding the factors that influence spinal BMD and the underlying biological mechanisms is therefore essential for the early prevention and intervention of osteoporosis.7,8 In recent years, inflammation has gained considerable attention as an influential factor in bone health. Numerous studies indicate that chronic low-grade inflammation is closely associated with various metabolic diseases and may play an essential role in bone metabolism, particularly by accelerating bone loss and consequently reducing bone density.9,10 However, the specific mechanisms linking inflammation to bone health remain unclear, warranting further investigation.
The Systemic Immune-Inflammation Response Index (SIRI), calculated from neutrophil, monocyte, and lymphocyte counts, is an integrative marker of inflammation.11,12 In recent years, SIRI has shown high sensitivity and reliability as a marker of systemic inflammation burden in assessing and predicting risks for cardiovascular disease, metabolic syndrome, diabetes, and cancer.13-16 Despite its promising applications in these fields, the relationship between SIRI and spinal BMD, especially in terms of osteoporosis risk, has yet to be thoroughly explored and widely discussed. The purpose of this study is to investigate the association between SIRI and spinal BMD in a large population sample, with a specific focus on potential segmented nonlinear relationships and threshold effects. This study aims to provide new insights and perspectives on the role of inflammation in bone health.
This study draws on data from the 2005-2018 cycles of the National Health and Nutrition Examination Survey (NHANES), a nationally representative program employing a multistage stratified sampling design. 17 By analyzing the relationship between SIRI and spinal BMD in a large general population, we aim to assess the independent impact of systemic inflammation on bone health after adjusting for key demographic and clinical variables. Using multivariable regression and nonlinear modeling approaches, we further explore whether this association follows a threshold or segmented pattern. These findings may offer new insights into the inflammatory mechanisms of osteoporosis and support the potential utility of SIRI as a biomarker for bone health monitoring.
Methods
Data Source
We used demographic data from the NHANES database in the United States. Conducted every two years since 1999, this survey employs a multi-stage, stratified sampling method to ensure representation across all age groups in the U.S. population. During the survey, participants provide informed consent and complete questionnaires with assistance from trained staff, followed by physical examinations conducted in mobile labs. Ethical approval is provided by the National Center for Health Statistics (NCHS). For our analysis, we selected data from the 2005 to 2018 cycles, which included demographic information, questionnaire responses, physical exam findings, lab results, and imaging data. This publicly accessible data is available at https://www.cdc.gov/nchs/nhanes/about_nhanes.htm.
Study Design
This study utilized data from five NHANES cycles: 2005-2006, 2007-2008, 2009-2010, 2013-2014, and 2017-2018, with a total of 50,463 participants. Initially, individuals without spinal BMD data from Dual-Energy X-ray Absorptiometry (DXA) were excluded, as well as those lacking the required data to compute SIRI (neutrophil, monocyte, and lymphocyte counts). Participants under 20 years of age were also excluded. The final analysis included 13,950 participants (Figure 1). Flowchart of participant selection and analytical steps.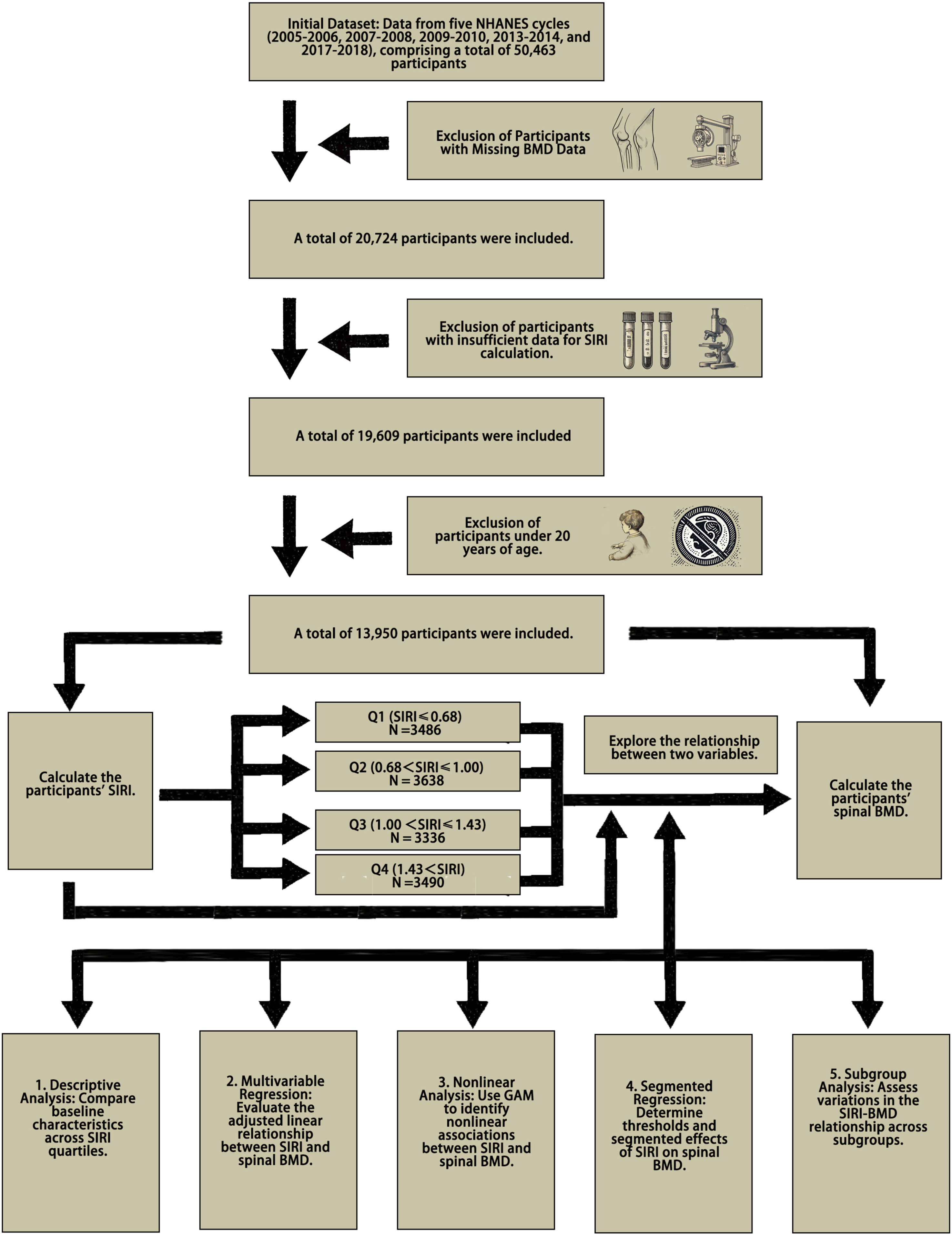
Exposure and Outcome Variables
SIRI is calculated as (neutrophil count × monocyte count)/lymphocyte count, with these cell counts obtained from laboratory blood tests. Total spinal BMD is measured by DXA. Based on SIRI quartiles, the 13,950 participants were divided into four groups: Q1, Q2, Q3, and Q4. This study examined variations in different variables across these quartiles. Although converting continuous variables into quartiles may reduce statistical precision, this approach helps to limit bias, particularly in cases of skewed distributions. Additionally, it facilitates the identification of potential relationships between independent and dependent variables at different levels.
Assessment of Other Covariates
Other covariates included age, sex, race, marital status, education level, smoking status, drinking status, history of hypertension, history of diabetes, waist circumference, weight, height, and body mass index (BMI, kg/m2). Some variables were collected using standardized questionnaires: smoking was defined as having smoked at least 100 cigarettes in one’s lifetime; drinking was defined as consuming at least 12 alcoholic beverages of any type within a single year. Participants who answered “Yes” to the question “Has a doctor ever told you that you have diabetes/hypertension?” were classified as having diabetes or hypertension. Blood samples were analyzed in the laboratory to determine total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C).
Statistical Analysis
In this study, continuous variables are presented as means (standard deviation [SD]) or medians with interquartile ranges (25th and 75th percentiles), while categorical variables are expressed as frequencies and percentages (n, %). Differences in normally distributed continuous variables were evaluated using independent-sample T-tests or one-way ANOVA. For non-normally distributed continuous variables, the Wilcoxon-Mann-Whitney rank-sum test was used. Chi-square tests were applied to assess differences in categorical variables. Differences across SIRI quartiles were examined. To investigate the association between SIRI and total spinal BMD, multivariable stepwise regression models were used to estimate β coefficients and 95% confidence intervals (CIs). Additionally, GAM and curve fitting, implemented with the mgcv package in R, were used to assess the potential impact of SIRI on total spinal BMD. The segmented package in R was applied to explore potential saturation effects and to identify breakpoint values via threshold analysis. Subgroup analyses were performed to evaluate whether the relationship between SIRI and spinal BMD varied across specific population characteristics, including age, gender, smoking, alcohol consumption, hypertension, and diabetes. Interaction terms were included to assess statistical significance for effect modification. The log-likelihood ratio test was conducted to compare the standard linear model with the segmented generalized additive model. All statistical analyses were performed in R (version 4.2.3), with statistical significance set at a two-sided P < 0.05. Data management and supplementary statistical analyses were performed using IBM SPSS Statistics 25.
Results
Baseline Characteristics
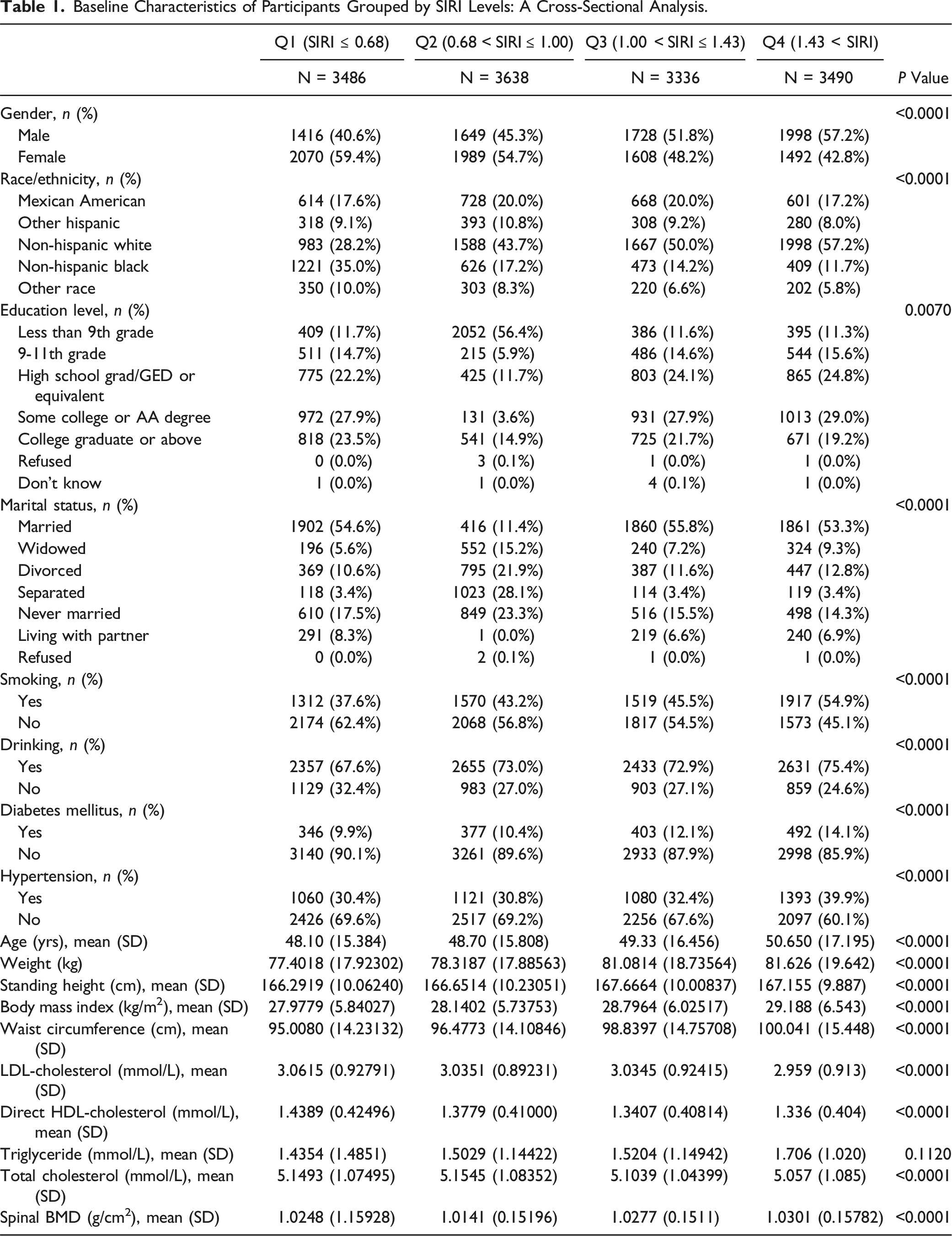
Baseline Characteristics of Participants Grouped by SIRI Levels: A Cross-Sectional Analysis.
Exploring Linear and Nonlinear Relationships of SIRI with Spinal BMD
Multivariable Regression Analysis Results of the Relationship Between SIRI and Spine BMD.
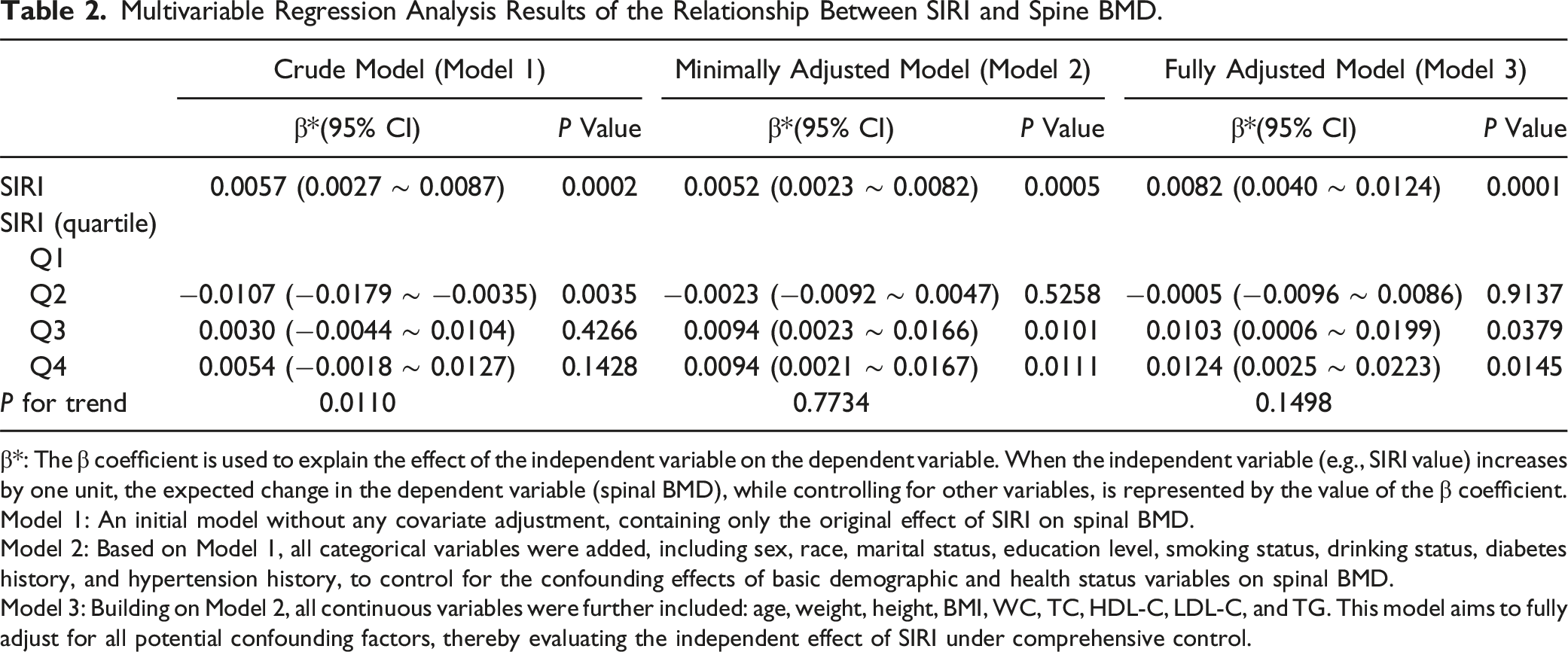
β*: The β coefficient is used to explain the effect of the independent variable on the dependent variable. When the independent variable (e.g., SIRI value) increases by one unit, the expected change in the dependent variable (spinal BMD), while controlling for other variables, is represented by the value of the β coefficient.
Model 1: An initial model without any covariate adjustment, containing only the original effect of SIRI on spinal BMD.
Model 2: Based on Model 1, all categorical variables were added, including sex, race, marital status, education level, smoking status, drinking status, diabetes history, and hypertension history, to control for the confounding effects of basic demographic and health status variables on spinal BMD.
Model 3: Building on Model 2, all continuous variables were further included: age, weight, height, BMI, WC, TC, HDL-C, LDL-C, and TG. This model aims to fully adjust for all potential confounding factors, thereby evaluating the independent effect of SIRI under comprehensive control.
Although the multivariable regression models indicated a significant relationship between SIRI and spinal BMD, the linear trend test (Table 2) suggested that this association might not be strictly linear. In the crude model, the linear trend P-value was 0.011, reaching statistical significance. However, in the minimally adjusted model (P = 0.7734) and the fully adjusted model (P = 0.1498), this trend did not reach significance. To further explore the potential nonlinear relationship between SIRI and spinal BMD, we employed a GAM (Figure 2). Adjusted associations between SIRI and spinal BMD using GAM (A) unadjusted model - The smooth function displays the baseline association between SIRI and spinal BMD without adjustment for any covariates. (B) Minimally adjusted model - Adjusted for basic demographic characteristics, including sex, race, marital status, education level, smoking and drinking status, history of diabetes, and hypertension. Shows the independent effect of SIRI on spinal BMD. (C) Fully adjusted model - Adjusted for all key covariates, including sex, race, marital status, education level, lifestyle factors (smoking and drinking), diabetes and hypertension history, as well as age, weight, height, BMI, WC, TC, HDL-C, LDL-C, and TG, showing the effect of SIRI on spinal BMD with comprehensive variable control.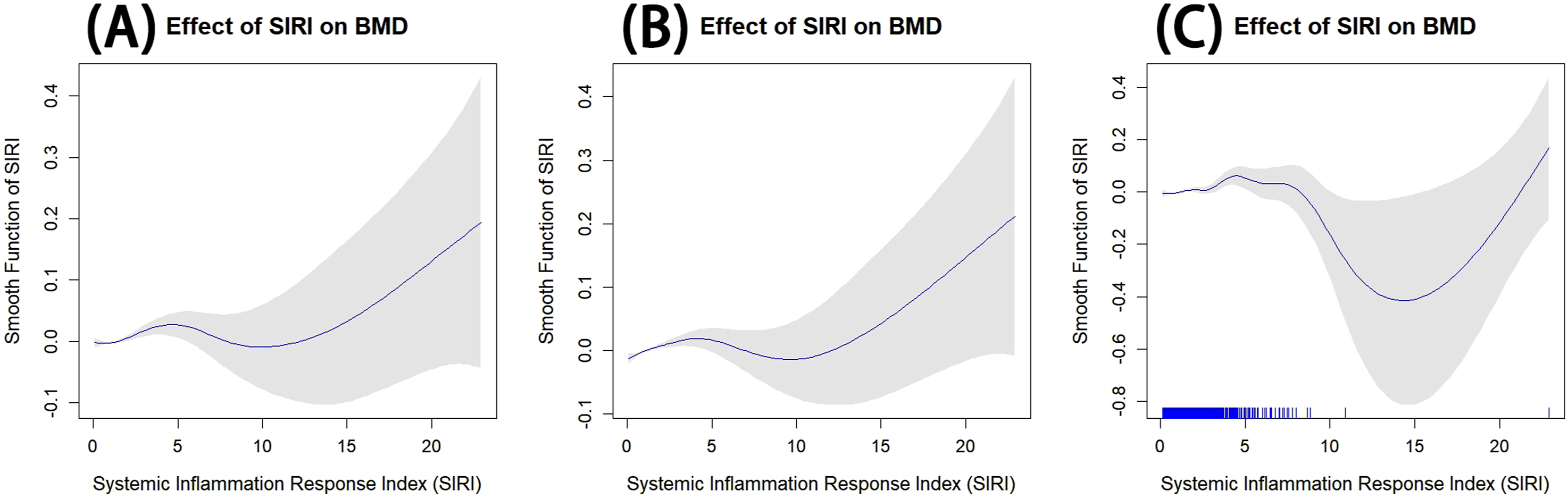
The GAM results revealed a significant nonlinear association between SIRI and spinal BMD (P < 0.001). As shown in panels (A), (B), and (C) of Figure 2, different levels of adjustment produced subtle variations in the trend. In the unadjusted model (Figure 2A), spinal BMD showed a slight increase at lower SIRI levels, followed by a more consistent upward trend at higher SIRI values. The minimally adjusted model (Figure 2B) indicated a similar pattern, with spinal BMD showing an initial dip at moderate SIRI levels before trending upward. The fully adjusted model (Figure 2C) confirmed a more complex nonlinear relationship, with spinal BMD initially decreasing and then sharply increasing as SIRI levels rose. This trend suggests that higher SIRI levels may have a more pronounced positive effect on spinal BMD, particularly when other covariates are comprehensively controlled for.
Segmented Regression and Nonlinear Analysis Results
Results of Standard Linear Regression and Segmented Regression Analysis of SIRI and Total Spine BMD.
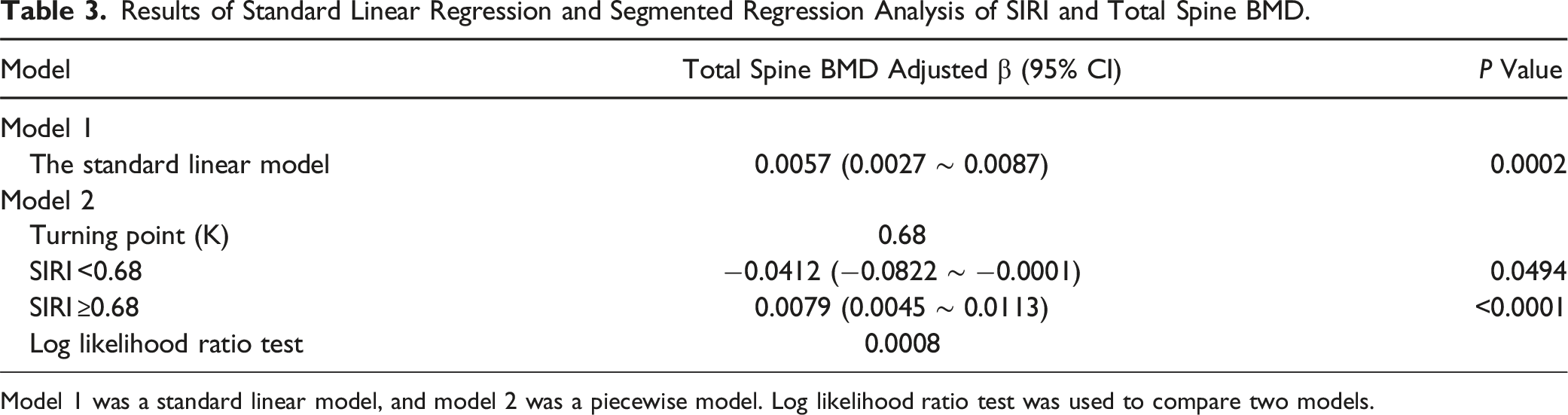
Model 1 was a standard linear model, and model 2 was a piecewise model. Log likelihood ratio test was used to compare two models.
Overall, the standard linear model, GAM, and segmented regression models consistently indicated a positive association between SIRI and spinal BMD, with this effect becoming more apparent at higher SIRI levels (Figure 2). The segmented regression analysis showed that at lower SIRI levels (<0.68), the effect of SIRI on spinal BMD was negative, but beyond this threshold (≥0.68), the effect turned positive and significantly increased. This finding supports the hypothesis of a nonlinear or segmented effect of SIRI on spinal BMD, suggesting that the impact becomes more pronounced as SIRI levels rise.
Subgroup Analysis Results
Subgroup Analysis of the Association Between SIRI and Spinal BMD.
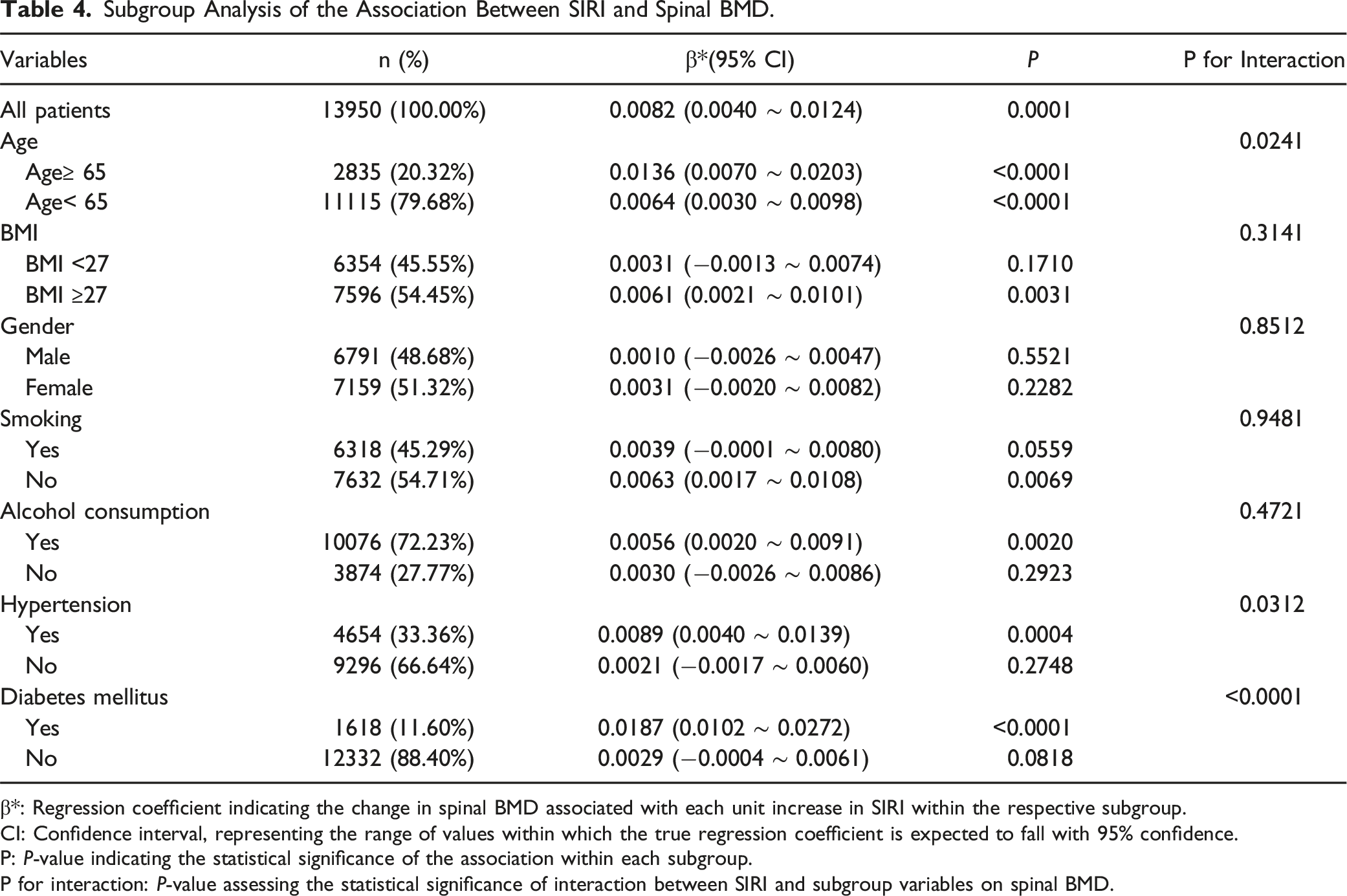
β*: Regression coefficient indicating the change in spinal BMD associated with each unit increase in SIRI within the respective subgroup.
CI: Confidence interval, representing the range of values within which the true regression coefficient is expected to fall with 95% confidence.
P: P-value indicating the statistical significance of the association within each subgroup.
P for interaction: P-value assessing the statistical significance of interaction between SIRI and subgroup variables on spinal BMD.
The relationship between SIRI and spinal BMD also varied significantly by hypertension status (P for interaction = 0.0312). In participants with hypertension, a significant positive association was identified (β = 0.0089, 95% CI: 0.0040 ∼ 0.0139, P = 0.0004), while no significant association was observed in those without hypertension (P = 0.2748). Similarly, diabetes mellitus emerged as a key modifier (P for interaction <0.0001). Among participants with diabetes, the association was particularly pronounced (β = 0.0187, 95% CI: 0.0102 ∼ 0.0272, P < 0.001), whereas no significant relationship was observed in non-diabetic individuals (P = 0.0818).
For other subgroup variables, including gender, smoking status, alcohol consumption, and BMI categories, no significant interaction effects were observed (P for interaction >0.05). However, the general trends remained consistent across these groups. These findings underscore the potential role of age, hypertension, and diabetes as modifiers of the relationship between SIRI and spinal BMD, while also suggesting that this association remains robust across different levels of body weight. Together, they highlight the complex and multifactorial influence of systemic inflammation on bone health.To further investigate age-specific and sex-specific variations, we stratified participants into four age groups (<60, 60-69, 70-79, and ≥80 years) and conducted subgroup analyses by sex within each age group. As presented in Supplemental 2, a significant positive association between SIRI and spinal BMD was observed among females aged <60 years (β = 0.0093, 95% CI: 0.0035 to 0.0150, P = 0.0016), while no significant associations were found in older female subgroups. Among males, the associations across age groups were generally weaker and nonsignificant. Notably, in the 70-79 years subgroup, the direction of the association differed between males (β = −0.0030, 95% CI: −0.0160 to 0.0101, P = 0.6524) and females (β = 0.0010, 95% CI: −0.0148 to 0.0167, P = 0.9045), although no significant interaction effect by sex was detected (P for interaction = 0.7052). These results suggest that the SIRI–BMD relationship may vary subtly across age and sex strata, particularly among younger female participants.
Discussion
BMD is a crucial indicator of bone health, widely used for diagnosing osteoporosis and assessing fracture risk.18-21 In recent years, attention has increasingly focused on the impact of inflammation on bone metabolism, especially with the SIRI as a comprehensive marker reflecting an individual’s inflammatory burden.22,23 SIRI has demonstrated high sensitivity in predicting the risk of several diseases, including cardiovascular disease, metabolic syndrome, diabetes, and cancer.24-26 However, the relationship between SIRI and spinal BMD, particularly any potential nonlinear associations, remains underexplored. This study is the first to uncover a segmented nonlinear relationship between SIRI and spinal BMD, identifying a significant threshold effect, thus providing new insights into the mechanisms by which inflammation influences bone metabolism.
This study utilized a large population sample from the NHANES database to systematically analyze the relationship between SIRI and spinal BMD, revealing a complex association in a stepwise manner. Initially, we employed linear regression analysis, progressively adjusting for variables to examine the overall impact of SIRI on spinal BMD. Results indicated that the initial unadjusted model showed a significant positive correlation between SIRI and spinal BMD. After adjusting for categorical variables such as sex, race, and marital status, the positive trend remained significant. Further adjustments for continuous variables like age, weight, BMI, and waist circumference strengthened the positive impact of SIRI on spinal BMD. Subsequently, we used a GAM to explore the nonlinear relationship between SIRI and spinal BMD. Results demonstrated that SIRI’s effect on spinal BMD exhibited a nonlinear pattern: within the lower SIRI range, spinal BMD showed minimal change with SIRI variations, whereas at higher SIRI levels, spinal BMD increased significantly. To further confirm this segmented characteristic, we conducted a segmented regression analysis, dividing SIRI into two intervals for linear fitting. The analysis revealed that when SIRI was below 0.68, it was negatively correlated with spinal BMD, whereas above 0.68, the correlation was significantly positive.
In addition to these findings, subgroup analyses further illuminated how specific population characteristics modified the association between SIRI and spinal BMD. The positive relationship was stronger among older adults (≥65 years), individuals with hypertension, and those with diabetes, suggesting that these populations may experience heightened or more complex inflammatory responses influencing bone metabolism. For example, the association in participants aged ≥65 years (β = 0.0136) was more pronounced than in younger individuals (β = 0.0064). Similarly, participants with hypertension or diabetes showed stronger positive correlations compared to those without these conditions, highlighting potential population-specific differences in how inflammation impacts bone density. These subgroup findings underscore the multifaceted nature of inflammation’s effects on bone metabolism, which may be influenced by underlying health conditions or age-related changes in inflammatory responses.
Collectively, these findings support the hypothesis of a segmented association between SIRI and spinal BMD, offering new perspectives on the complex and bidirectional role of inflammation in bone metabolism. They also underscore the need to consider individual characteristics, such as age and comorbidities, when evaluating the skeletal impact of systemic inflammation. From a clinical standpoint, inflammation-driven ossification plays a key role in conditions such as spondylodiscitis and cervical arthroplasty, where excessive bone formation may complicate healing and spinal fusion outcomes. Anti-inflammatory medications are commonly employed in the acute phase to minimize such complications. These observations reinforce the potential utility of inflammatory biomarkers like SIRI, not only for risk stratification in osteoporosis, but also for guiding individualized treatment decisions in inflammation-related spinal disorders. To more intuitively demonstrate the nonlinear relationship between SIRI and spinal BMD, we created a scatter plot and fitted curve in Figure 3 to further validate the segmented association observed in our analysis. Figure 3 illustrates the overall trend between SIRI and spinal BMD, as well as the segmented relationships at different SIRI levels. In Figure 3A, a slight upward trend is observed across the overall range of SIRI and spinal BMD. To examine this segmented effect more closely, we further divided the data, as presented in Figure 3B and C. Figure 3B shows the situation when SIRI is below 0.68, where the relationship between SIRI and spinal BMD is slightly negative, aligning with our threshold effect hypothesis. Figure 3C displays the relationship when SIRI is above 0.68, showing a significant positive correlation between SIRI and spinal BMD, suggesting that higher SIRI levels may promote bone density. These visualizations clearly support the segmented nonlinear association between SIRI and spinal BMD, providing key visual evidence to enhance our understanding of their relationship. Scatter plot of the segmented relationship between SIRI and Spinal BMD (A) Displays the overall association between SIRI and spinal BMD, illustrating the general trend across the full range of SIRI values. (B) Shows the relationship between SIRI and spinal BMD for SIRI values below the identified threshold of 0.68. This segment indicates a slight negative association, aligning with the threshold effect observed in the analysis. (C) Illustrates the association for SIRI values equal to or above 0.68, where a positive relationship between SIRI and spinal BMD becomes evident, supporting the hypothesis that higher SIRI levels are associated with higher spinal BMD values.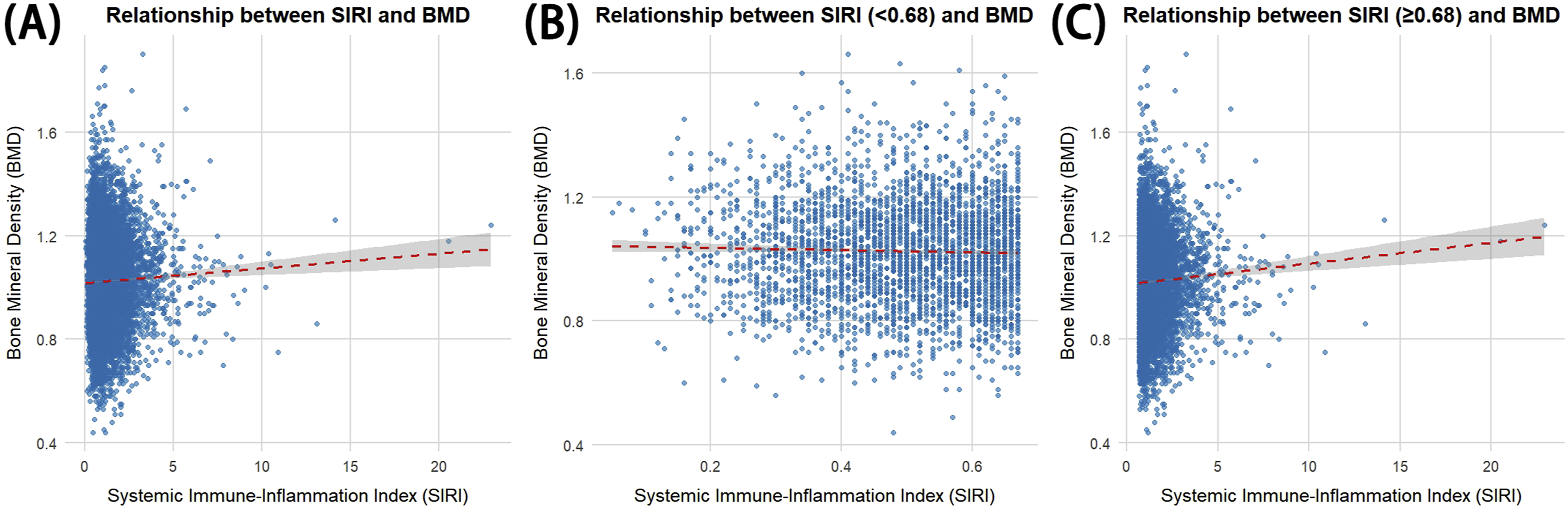
This study provides significant insights into the relationship between inflammation and bone metabolism, marking the first to reveal a segmented nonlinear relationship between SIRI and spinal BMD. This finding not only suggests a potential biomarker for osteoporosis screening and individualized risk assessment but also highlights the complex, multi-level impact of inflammatory burden on bone density.
We propose that low-level inflammation may contribute to bone resorption by activating osteoclast activity, thereby accelerating bone loss and reducing spinal BMD. Chronic low-grade inflammation has been shown to promote osteoclast differentiation, enhancing bone resorption without adequate compensatory bone formation, which can negatively impact bone density. 27 Inflammatory cytokines, such as TNF-α and IL-6, are often induced by low levels of inflammation and have been observed to activate osteoclasts, contributing to bone loss and supporting the view that low-level inflammation detrimentally affects spinal BMD.28,29 Additionally, pro-inflammatory cytokines like IL-1β and IL-6 are known to enhance osteoclast differentiation and activity under low inflammatory conditions, reinforcing the idea that low-grade inflammation increases bone resorption by influencing osteoclast activity.30-34
However, when inflammation reaches higher levels, compensatory mechanisms may be triggered within the bone microenvironment. For instance, increased osteoblast activity or the upregulation of anti-inflammatory factors may regulate bone metabolism and mitigate some of the negative effects of inflammation.34,35 At this stage, the adverse impact of inflammation on bone density may be reduced or even reversed, potentially resulting in an increase in spinal BMD. High levels of pro-inflammatory cytokines can, in some cases, trigger a compensatory osteoblastic response, promoting bone formation and potentially enhancing spinal BMD.36,37 Furthermore, elevated inflammatory markers have been shown to stimulate adaptive responses within the skeletal system, enhancing osteoblast activity and raising spinal BMD. At higher inflammation levels, specific cytokines, such as IL-1β and RANKL, may simultaneously activate both osteoblasts and osteoclasts, with adaptive responses making osteoblast activity more prominent under these conditions.38,39
This segmented relationship suggests that the impact of inflammation on bone metabolism exhibits dual characteristics depending on its intensity. Low-level inflammation may accelerate bone resorption, whereas high-level inflammation may under certain conditions promote bone formation. Given SIRI’s sensitivity to inflammatory burden, it may serve as an effective biomarker for dynamically monitoring these varied effects on bone density. This discovery provides new insights into the complex role of inflammation in bone health and lays a scientific foundation for the application of inflammatory biomarkers in osteoporosis prevention and management.
In future research, validating this mechanism will further deepen our understanding of the complex role of inflammation in bone metabolism. Specifically, future studies could utilize longitudinal designs to observe the relationship between changes in SIRI and dynamic spinal BMD variations, thereby determining a causal relationship between the two. Additionally, experimental studies could focus on the regulatory mechanisms of osteoclast and osteoblast activity under varying levels of inflammation, especially examining the specific roles of pro-inflammatory and anti-inflammatory factors within the bone marrow microenvironment. Further exploration of the synergistic effects between SIRI and other inflammatory markers (such as NLR and PLR) would also help clarify the multifaceted impact of inflammation on bone metabolism. Through animal models and in vitro experiments, specific molecular pathways (such as the RANKL/OPG and Wnt signaling pathways) can be observed in inflammatory conditions to delineate the precise influence of inflammation on bone resorption and formation. Additionally, with the advancement of multi-omics technologies, future research could integrate genomics, proteomics, and metabolomics to construct a comprehensive map of the effects of different inflammation levels on bone health. This approach could help identify potential molecular biomarkers and advance novel strategies for osteoporosis prevention and treatment, moving toward more personalized management of bone health.
Despite revealing a segmented nonlinear association between SIRI and spinal BMD, this study has certain limitations. First, as a cross-sectional study, it cannot establish causality, making it unclear whether changes in SIRI directly lead to changes in spinal BMD. Second, although several confounding variables (such as age, sex, ethnicity, lifestyle, and history of chronic disease) were controlled, there may still be unmeasured confounders, such as diet, nutritional intake, and physical activity, that could influence spinal BMD. Third, as this study is based on a U.S. population sample from the NHANES database, its generalizability may be limited, especially in applicability to other ethnicities and regions. Finally, the study relies on SIRI as a single indicator; future research could incorporate multiple inflammation-related markers to better understand the complex impact of inflammation on bone density.
In conclusion, this study identifies a segmented nonlinear relationship between SIRI and spinal BMD, with a significant threshold effect that offers new insights into the role of inflammation in bone health. Although there are certain limitations, this study provides a scientific basis for applying inflammatory biomarkers in osteoporosis risk assessment. Future longitudinal and mechanistic studies are needed to further validate and expand upon these findings.
Conclusion
This study reveals a segmented nonlinear relationship between SIRI and spinal BMD, highlighting a threshold effect that offers new insights into how inflammation may impact bone health. While low levels of SIRI were associated with decreased spinal BMD, likely through increased osteoclast activity, higher SIRI levels appeared linked to compensatory osteoblast activation. Although causality cannot be confirmed due to the cross-sectional design, these findings suggest SIRI’s potential as a biomarker for osteoporosis risk. Future longitudinal studies are encouraged to validate this relationship and explore targeted strategies for bone health management based on individual inflammatory profiles.
Supplemental Material
Supplemental Material - Deciphering the Threshold and Segmented Nonlinear Association Between Systemic Inflammation Response Index and Spinal Bone Density: Insights From a Large-Scale Population Study
Supplemental Material for Deciphering the Threshold and Segmented Nonlinear Association Between Systemic Inflammation Response Index and Spinal Bone Density: Insights From a Large-Scale Population Study by Muradil Mardan, Zeyu Lu, Qingyin Xu, Shaokuan Song, Huoliang Zheng, Hui Deng, Hao Cai, Qizhu Chen, Pengbo Chen, Bo Li, Shengdan Jiang, Leisheng Jiang, and Xin-Feng Zheng in Global Spine Journal.
Footnotes
Acknowledgments
We would like to express our gratitude to all those who contributed to this work. We also acknowledge the helpful discussions and insights provided by colleagues in the field. No specific acknowledgments are required for this study.
Author Contributions
Each author has participated in the drafting and critical revision of the manuscript and has given approval for the final version.
Declaration of Conflicting Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Shanghai Sailing Program (23YF1425900) and the National Natural Science Foundation of China (82272535).
Ethical Statement
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.