
Abstract
Objective
To assess the association between the systemic inflammation response index (SIRI) and the prognosis in patients with sepsis-associated acute kidney injury (SA-AKI).
Methods
In this observational study, adult patients with SA-AKI were categorized into three groups based on SIRI tertiles. Survival outcomes were compared across the three groups using Kaplan–Meier survival curves. Various Cox proportional hazards regression models were developed to determine the association between the SIRI and mortality in patients with SA-AKI. Subgroup analyses were also performed to explore the association between different SIRI tertiles and all-cause mortality.
Results
After adjusting for several confounders, the second SIRI tertile (2.5 < SIRI < 7.6) was found to be an independent risk factor for 30-day mortality [hazard ratio (95% confidence interval): 1.19 (1.01–1.40)], 90-day mortality [1.22 (1.06–1.41)], and 365-day mortality [1.24 (1.09–1.40)]. Furthermore, high SIRI values were associated with increased risks of 30-day, 90-day, and 365-day mortality in patients with SA-AKI across all three models. The third tertile showed a significant association with adverse outcomes in most subgroups.
Conclusions
The SIRI serves as a comprehensive biomarker for predicting all-cause mortality of critically ill patients with SA-AKI.
Keywords
Introduction
During the past few years, sepsis has consistently shown high incidence and mortality rates worldwide. Sepsis was estimated to be responsible for approximately 11 million deaths in 2017, constituting 20% of the total global mortality. 1 The complex interplay of immune, inflammatory, and hemodynamic responses in patients with sepsis can lead to multiple organ dysfunction. Among various affected organs, the kidneys are particularly susceptible, 2 and their involvement may lead to sepsis-associated acute kidney injury (SA-AKI). More than half of AKI cases are attributed to sepsis, with associated mortality rates as high as 40%. 3 Hence, it is imperative to effectively identify patients with SA-AKI who have an unfavorable prognosis and implement timely intervention.
Sepsis is characterized by uncontrolled inflammation stemming from diverse pathogenic microorganisms and their toxins. AKI can be triggered by various factors, with inflammation being a significant contributor. SA-AKI refers to a sudden decline in kidney function when sepsis is present. During inflammation, the immune system releases a variety of cytokines and inflammatory mediators that can directly damage the kidneys. 4 Additionally, sepsis can cause a drop in blood pressure, compromising renal perfusion and resulting in the development of AKI. 5 Therefore, the severity of the inflammatory response significantly impacts the prognosis of SA-AKI.
Numerous studies have proposed that inflammatory indices, such as the neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio, can serve as prognostic markers for infectious diseases.6–8 Additionally, the systemic inflammation response index (SIRI) has garnered increasing attention in recent years. Cai et al. 9 reported that higher SIRI levels independently predicted adverse outcomes in patients with infective endocarditis. Jin et al. 10 found that the SIRI was independently associated with the occurrence of ischemic stroke in patients with rheumatoid arthritis. Given the potential significance of the SIRI in infectious and inflammatory conditions, this raises the intriguing possibility that the SIRI can be applied as a valuable indicator in patients with SA-AKI. Importantly, although researchers have noted the prognostic value of the SIRI in patients with sepsis, 11 its role in patients with SA-AKI has not been specifically explored. The aim of the present study was to bridge this gap, focusing on the potential of the SIRI to serve as a prognostic marker in this population.
Materials and methods
Data source and study population
This retrospective study utilized data from the MIMIC-IV database (version 2.0), which encompasses records of 76,943 unique intensive care unit (ICU) admissions from 2008 to 2019 at the Beth Israel Deaconess Medical Center located in Boston, MA, USA. Rigorous de-identification measures were applied to anonymize the patient and hospital information in this database. The primary author, Jia Tang, has obtained full access to the database (record ID: 52759164). The study inclusion criteria were occurrence of the initial ICU admission during the first hospitalization, age of ≥18 years, ICU length of stay of ≥2 days, satisfaction of the Sepsis-3 criteria, and diagnosis of AKI. Patients with pre-existing chronic kidney disease or congestive heart failure and patients lacking SIRI data within 24 hours of ICU admission were excluded.
Data extraction
We extracted patients’ demographic data, clinical parameters, and prognosis information, including the following: age, sex, race, ICU type, vital signs (heart rate, mean blood pressure, respiratory rate, and temperature), comorbidities (chronic obstructive pulmonary disease, diabetes, cancer, acute pancreatitis, burns, and rhabdomyolysis), AKI stage, illness severity scores [Sequential Organ Failure Assessment (SOFA) score and Simplified Acute Physiology Score II], interventions (renal replacement therapy, mechanical ventilation, and vasoactive agents), laboratory results (anion gap, serum creatinine, blood urea nitrogen, neutrophils, monocytes, lymphocytes, and SIRI), and clinical outcomes (30-day, 90-day, and 365-day mortality and hospital length of stay). Missing values for all variables were imputed by the random forest method with the R package “mice.” 12 Variables with >20% missing data were removed from the analysis. All vital signs and laboratory data included in the study were derived from measurements taken during the first 24 hours following patients’ admission to the ICU. When multiple measurements occurred within a 24-hour window, only the initial recording was considered. All data within this database were extracted using Structured Query Language (SQL) with PostgreSQL (version 14.7).
Definitions and outcomes
Satisfaction of the Sepsis-3 criteria necessitated documented or suspected infection in combination with a ≥2-point increase in the SOFA score. 13 In accordance with the Kidney Disease Improving Global Outcomes (KDIGO) guideline, 14 AKI was defined as follows: an increase in serum creatinine by ≥0.3 mg/dL within 48 hours, an increase in serum creatinine to a magnitude of ≥1.5 times the baseline within 7 days, or a urine volume of <0.5 mL/kg/hour for 6 hours. The SIRI was calculated as follows: SIRI = N × M/L, where N, M, and L were the peripheral neutrophil, monocyte, and lymphocyte counts, respectively.
The primary outcome of this study was 30-day all-cause mortality following ICU admission. The secondary outcomes were 90-day all-cause mortality, 365-day all-cause mortality, and hospital length of stay for patients with SA-AKI.
Statistical analysis
The baseline characteristics of eligible patients were categorized into three groups based on the tertiles of SIRI. The Shapiro–Wilk normality test was conducted to assess the normality of all continuous variables. Continuous variables with a normal distribution are presented as mean and standard deviation, while non-normally distributed variables are presented as median and interquartile range. Categorical variables are expressed as numerical values and percentages. Group distinctions were assessed using the t test or Wilcoxon rank-sum test for continuous variables and the chi-square test for categorical variables. Survival outcomes across the three groups were analyzed using Kaplan–Meier survival curves and compared by the log-rank test. Additionally, we employed three adjusted Cox proportional hazards regression models to determine the association between the SIRI and all-cause mortality in patients with SA-AKI. The results are reported as hazard ratio (HR) with 95% confidence interval (CI). We performed a subgroup analysis to further enhance the robustness of our data. This was conducted using stratified Cox proportional hazard regression models to explore the association between SIRI tertiles and all-cause mortality. Group 1 (SIRI of ≤2.5) was set as the reference group. Statistical significance was established at a P-value of <0.05 with a two-tailed test. We conducted all statistical analyses using R Software Version 4.3.1 (www.r-project.org). The reporting of this study conforms to the STROBE guidelines. 15
Ethical approval and informed consent
This research adhered to the Declaration of Helsinki and was approved by the ethics committees of both the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center (researcher certification number 52759164). The requirement for written informed consent was waived because of the anonymized information collection process and retrospective study design.
Results
Population and patient characteristics
In total, 4617 patients with SA-AKI were included in the final analysis (Figure 1). Missing data for all variables were <5% (Figure S1). After five iterations of multiple imputation on the dataset, we selected the dataset from the first imputation, which displayed a distribution strikingly similar to that of the original data (Figure S2). The baseline characteristics of all selected patients are listed in Table 1. The patients were then categorized into three groups: Group 1 (SIRI ≤ 2.5), Group 2 (2.5 <SIRI < 7.6), and Group 3 (SIRI ≥ 7.6). As shown in the table, there were significant differences in all variables except for age, burns, diabetes, and mechanical ventilation. Most patients were male [2627 (56.9%)] and of White ethnicity [2947 (63.8%)]. Most patients diagnosed with stage 1 AKI were within the first SIRI tertile, most diagnosed with stage 2 AKI were within the second SIRI tertile, and most diagnosed with stage 3 AKI were within the third SIRI tertile. Patients in the third tertile had higher neutrophil and monocyte counts and lower lymphocyte counts than patients in the first and second tertiles. The third tertile also exhibited the highest 30-day, 90-day, and 365-day mortality and longest hospital stay among the three groups (Table S1).

Flowchart of patient selection.
Baseline characteristics of the study population.

Data are expressed as median [interquartile range] or n (%).
SIRI, systemic inflammation response index; ICU, intensive care unit; CCU, coronary care unit; MICU, medical intensive care unit; SICU, surgical intensive care unit; MBP, mean blood pressure; RR, respiratory rate; COPD, chronic obstructive pulmonary disease; SOFA, Sequential Organ Failure Assessment; SAPSII, Simplified Acute Physiology Score II; RRT, renal replacement therapy; MV, mechanical ventilation; SCr, serum creatinine; BUN, blood urea nitrogen.
Kaplan–Meier curves for SIRI tertiles
The Kaplan–Meier survival curves (Figure 2) showed the incidence of 30-day, 90-day, and 365-day all-cause mortality across the groups based on SIRI tertiles. During the three observation periods, patients with high SIRI levels showed a lower probability of survival. Patients in the first and second tertiles exhibited similar survival probabilities, whereas patients in the third tertile showed a substantial decline in survival probability. By the end of the 365-day observation duration, approximately 50% of the patients in the third tertile were still alive, whereas the other two groups had a greater percentage of survivors.
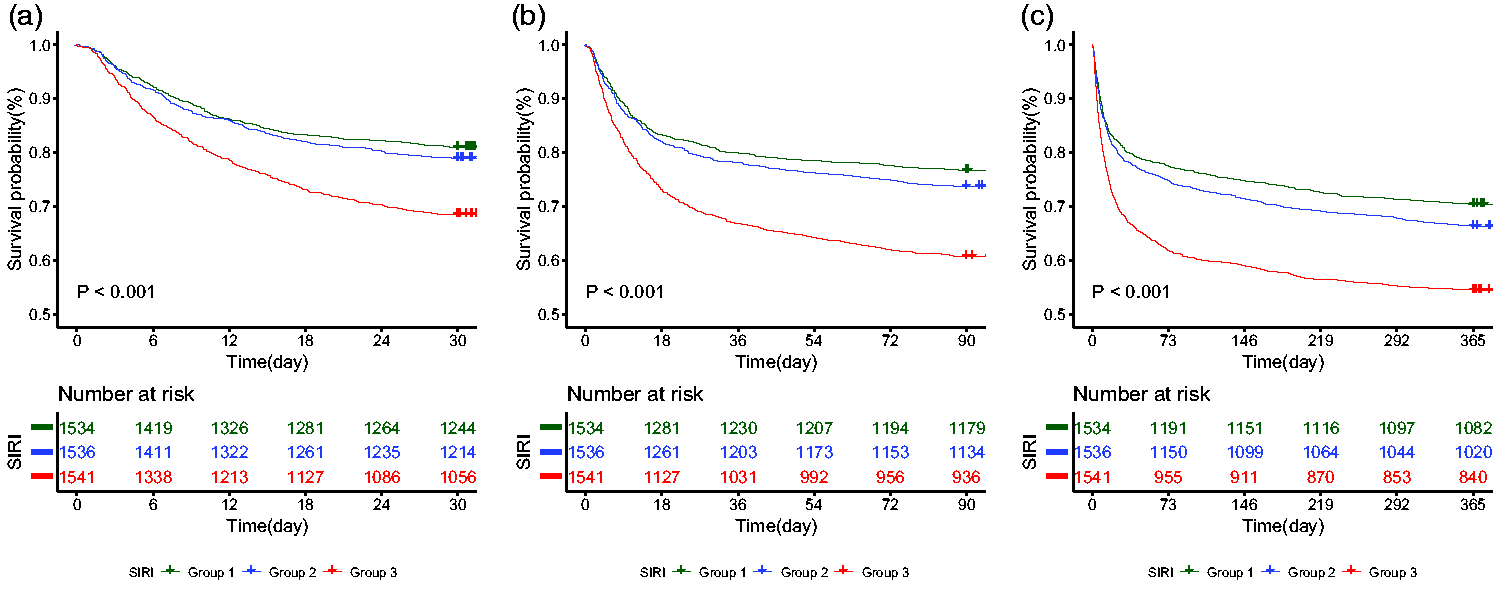
Kaplan–Meier survival curves across three groups. (a) 30-day follow-up period. (b) 90-day follow-up period and (c) 365-day follow-up period.
Multivariate Cox regression analysis between SIRI and all-cause mortality
Table 2 shows the results of the association analysis between SIRI and 30-day, 90-day, and 365-day all-cause mortality. Three models were constructed: Model I, adjusted only for age, sex, race, and ICU type; Model II, further adjusted for heart rate, mean blood pressure, respiratory rate, temperature, chronic obstructive pulmonary disease, diabetes, cancer, acute pancreatitis, burns, and rhabdomyolysis; and Model III, further adjusted for AKI stage, anion gap, serum creatinine, blood urea nitrogen, renal replacement therapy, mechanical ventilation, vasoactive agent, and SOFA score. Group 1 (SIRI ≤ 2.5) served as a reference. The results demonstrated that a high SIRI (SIRI ≥ 7.6) was associated with a greater risk of 30-day, 90-day, and 365-day mortality in patients with SA-AKI in all three models. In the model that adjusted for the maximum number of confounding factors, Group 2 (2.5 < SIRI < 7.6) emerged as an independent risk factor for 30-day mortality [HR (95% CI): 1.19 (1.01–1.40), P = 0.032], 90-day mortality [1.22 (1.06–1.41), P = 0.006], and 365-day mortality [1.24 (1.09–1.40), P = 0.001].
Multivariable Cox regression to assess association of SIRI with all-cause mortality among patients with SA-AKI.
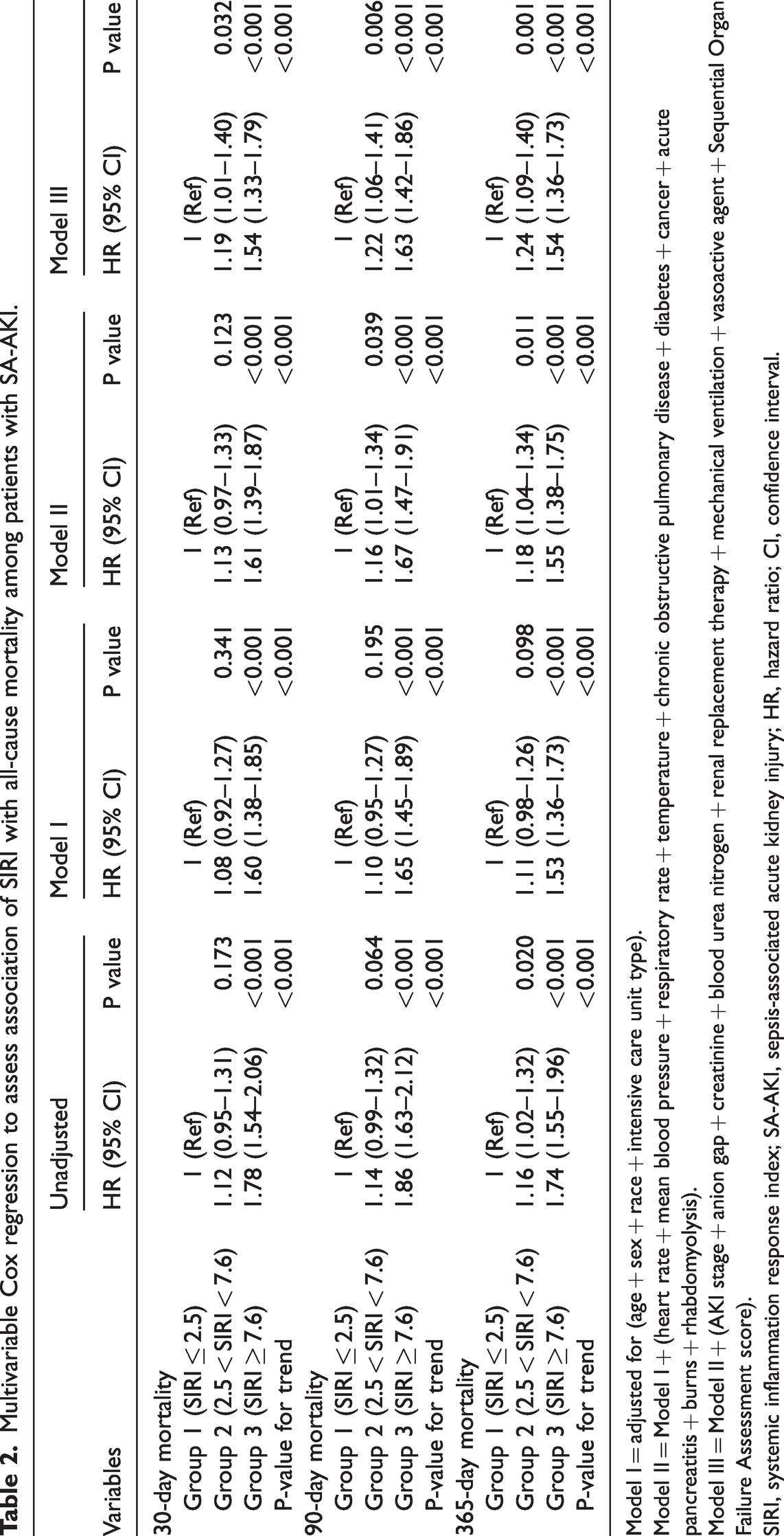
Model I = adjusted for (age + sex + race + intensive care unit type).
Model II = Model I + (heart rate + mean blood pressure + respiratory rate + temperature + chronic obstructive pulmonary disease + diabetes + cancer + acute pancreatitis + burns + rhabdomyolysis).
Model III = Model II + (AKI stage + anion gap + creatinine + blood urea nitrogen + renal replacement therapy + mechanical ventilation + vasoactive agent + Sequential Organ Failure Assessment score).SIRI, systemic inflammation response index; SA-AKI, sepsis-associated acute kidney injury; HR, hazard ratio; CI, confidence interval.
Subgroup analyses of association between SIRI and all-cause mortality
The association between different SIRI tertiles and 30-day mortality in different subgroups is shown in Table 3. Subgroup analyses were also performed for both 90-day mortality (Table S2) and 365-day mortality (Table S3). A significant association was observed between the second SIRI tertile (2.5 < SIRI < 7.6) and 30-day mortality in the female subgroup [HR (95% CI): 1.40 (1.10–1.78), P = 0.006] and stage 3 AKI subgroup [HR (95% CI): 1.28 (1.02–1.61), P = 0.032]. The third SIRI tertile (SIRI ≥ 7.6) was an independent risk factor for patients from the medical ICU [HR (95% CI): 1.45 (1.20–1.76), P < 0.001] and surgical ICU [HR (95% CI): 1.50 (1.14–1.98), P = 0.004]. However, no significant association was observed between the third SIRI tertile and 30-day mortality in the acute pancreatitis subgroup [HR (95% CI): 1.62 (0.42–6.26)] or rhabdomyolysis subgroup [HR (95% CI): 0.92 (0.37–2.29)]. Given the small number of patients in both groups, this finding requires verification in a larger sample in the future. With longer follow-up durations, a significant correlation between the second SIRI tertile and mortality became apparent in an expanding set of subgroups. Furthermore, our analyses revealed that no significant interaction was observed for short-term mortality (30 days) in all subgroups. For 365-day mortality, however, there was a statistically significant interaction effect among different ICU types with a P-value for interaction of <0.05.
Association between SIRI and 30-day all-cause mortality in different subgroups.

Multivariable Cox regression analysis in subgroups adjusted for the same covariates as for Model III in Table 2.
SIRI, systemic inflammation response index; HR, hazard ratio; CI, confidence interval; ICU, intensive care unit; CCU, coronary care unit; MICU, medical intensive care unit; SICU, surgical intensive care unit; COPD, chronic obstructive pulmonary disease; AP, acute pancreatitis; AKI, acute kidney injury.
Discussion
Sepsis, widely characterized as a systemic infection, presents a significant threat to patients’ well-being and lives. AKI, one of the most common complications of sepsis, manifests early in patients with sepsis and substantially increases the risks of mortality and morbidity. Approximately two-thirds of patients with sepsis are susceptible to developing SA-AKI. 16 During sepsis, the body triggers an overly aggressive inflammatory response to combat infection. Similar to this, one pathological feature of AKI is inflammation in the renal interstitium. 17 This inflammatory response represents the primary host defense mechanism against infection and plays a crucial role in initiating and supporting the necessary repair processes for functional recovery following injury. 18 Classic inflammatory indicators, including the white blood cell count and its subtypes, notably the neutrophil and lymphocyte counts, have a well-established place in clinical practice.19,20 By combining these counts, the SIRI emerges as a comprehensive biomarker for evaluating the body’s inflammatory state.
In the present study, we found that the 30-day, 90-day, and 365-day mortality rates increased as the SIRI became higher in patients with SA-AKI. Moreover, Cox regression analysis demonstrated that a high SIRI was an independent predictor of all-cause mortality regardless of whether the confounders were adjusted. Our findings corroborate a prior study’s conclusion that the SIRI serves as an independent prognostic biomarker for sepsis-related mortality. 11 Another study suggested that the SIRI may be a valuable biomarker for predicting the occurrence of AKI in patients with acute pancreatitis. 21 Although we observed an association between elevated mortality and the SIRI, it is imperative to acknowledge that various factors may contribute to these outcomes. Consequently, we conducted subgroup analyses that considered these variables. Our findings revealed a significant association between a high SIRI and adverse outcomes in most subgroups. Additionally, patients with moderate SIRI levels were not completely free from the risk of mortality, and appropriate management of these patients should not be overlooked. A high SIRI did not qualify as a risk factor for short-term outcomes in patients in the coronary care unit, but it emerged as a risk factor for long-term outcomes. Moreover, we found that the role of the SIRI as a risk factor varied among patients from different ICUs. In particular, a high SIRI exhibited the greatest risk for patients in the coronary care unit. Therefore, it may be necessary to implement different management strategies for patients with a high SIRI in various ICU settings, especially in the coronary care unit.
Neutrophils serve as front-line defense in the innate immune system. 22 They are vital in combating infectious diseases because they identify and engulf pathogens, release cytokines and free radicals, produce enzymes, and clear debris and necrotic tissue, thus boosting the immune response and guarding against infection. 23 Under normal circumstances, neutrophils in the circulation have a brief half-life (usually 7–12 hours) 24 ; however, their longevity is increased during the onset of sepsis. One key signaling pathway contributing to neutrophil resistance to apoptosis involves the activation of extracellular regulated protein kinases 1/2 and phosphoinositide-3 kinases in neutrophils. This ultimately leads to upregulated expression of the anti-apoptotic protein Bcl-xL. 25 In various inflammatory diseases, neutrophils release a range of metabolites that damage normal cells, such as reactive oxygen species and proteases. These can mediate dissolution of the extracellular matrix, leading to acute and potentially irreversible damage. 26
The mononuclear phagocyte system theory posits that macrophages in the bloodstream are primarily derived from monocytes. 27 Macrophages play a crucial role in innate immunity by phagocytizing and digesting pathogens as well as participating in the activation of adaptive immunity through antigen presentation. Monocytes and their successor cells, such as macrophages, produce a variety of inflammatory mediators, including tumor necrosis factor-α and monocyte chemoattractant protein-1. 28 These mediators can enhance inflammatory responses and exacerbate tissue and organ damage. Animal models have indicated the pivotal role of macrophages in the AKI-associated inflammatory response. 29 Monocytes not only differentiate into macrophages but also into dendritic cells, which are involved in inducing specific immune responses through antigen presentation. 30 However, the dynamics of lymphocytes differ. Anti-inflammatory cytokines in the bloodstream can induce immunosuppression, leading to apoptosis of a significant number of lymphocytes. 31 Evidence from clinical studies indicates that sepsis is associated with a decrease in the blood lymphocyte count, which may persist at low levels for up to 28 days.32,33
The SIRI serves as an indicator of systemic inflammation. As the SIRI increased in the present study, we observed a notable rise in the neutrophil and monocyte counts accompanied by a reduction in the lymphocyte count. The SIRI not only reflects patients’ inflammatory status but also quantifies the degree of inflammation, offering valuable insights for healthcare professionals to better understand patients’ health status. The neutrophil, monocyte, and lymphocyte counts are routine laboratory tests performed in patients with sepsis or AKI upon admission to the ICU, facilitating practical and cost-effective use of the SIRI in clinical settings. Therefore, we recommend considering the SIRI as a systemic inflammatory ischemic marker, given its potential to provide a more comprehensive portrayal of the disease characteristics of SA-AKI.
To the best of our knowledge, this study represents the first attempt to elucidate the association between the SIRI and adverse outcomes in patients with SA-AKI. Our study had a relatively large sample size of >4000 patients. Nevertheless, several limitations merit attention. Conducting retrospective studies based on established databases often involves limited data access constraints, impeding comprehensive investigation. Furthermore, because of incomplete follow-up renal function data in the public database, the ability to conduct a detailed analysis of the development of acute and chronic kidney disease was limited. Consequently, we could not perform a comprehensive assessment of the proportion of patients with AKI transitioning to acute or chronic kidney disease and examine its impact on 1-year mortality. The SIRI was assessed only once upon admission to the ICU, without dynamic monitoring during the entire hospitalization. Consequently, whether dynamic changes in the SIRI can offer additional insights for patients with sepsis remains uncertain. To gain a more profound understanding of the relationship between the SIRI and the prognosis of patients with SA-AKI, further in-depth and multicenter research is warranted.
Conclusion
This study showed that the SIRI is a comprehensive biomarker for predicting all-cause mortality of critically ill patients with SA-AKI. Patients with a higher SIRI at ICU admission had a higher risk of mortality.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241235758 - Supplemental material for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study
Supplemental material, sj-pdf-1-imr-10.1177_03000605241235758 for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study by Jia Tang, Zhenguang Zhong, Muyesai Nijiati and Changdong Wu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241235758 - Supplemental material for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study
Supplemental material, sj-pdf-2-imr-10.1177_03000605241235758 for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study by Jia Tang, Zhenguang Zhong, Muyesai Nijiati and Changdong Wu in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605241235758 - Supplemental material for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study
Supplemental material, sj-pdf-3-imr-10.1177_03000605241235758 for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study by Jia Tang, Zhenguang Zhong, Muyesai Nijiati and Changdong Wu in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605241235758 - Supplemental material for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study
Supplemental material, sj-pdf-4-imr-10.1177_03000605241235758 for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study by Jia Tang, Zhenguang Zhong, Muyesai Nijiati and Changdong Wu in Journal of International Medical Research
Supplemental Material
sj-pdf-5-imr-10.1177_03000605241235758 - Supplemental material for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study
Supplemental material, sj-pdf-5-imr-10.1177_03000605241235758 for Systemic inflammation response index as a prognostic factor for patients with sepsis-associated acute kidney injury: a retrospective observational study by Jia Tang, Zhenguang Zhong, Muyesai Nijiati and Changdong Wu in Journal of International Medical Research
Footnotes
Author contributions
JT: Writing—original draft. ZZ: Writing—review & editing. MN: Writing—review & editing. CW: Writing—review & editing.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.