
Abstract
Study Design:
Retrospective study.
Objectives:
To investigate the effect of paraspinal muscle degeneration on the maintenance of local and global alignment among degenerative lumbar scoliosis (DLS) patients after corrective surgery.
Methods:
98 DLS patients with a mean follow-up period of 38.3 months after corrective surgery were included. The T1 pelvic angle (TPA), lumbar lordosis (LL), pelvic incidence were measured preoperatively, immediate postoperatively and at last follow-up. All patients were divided into LL maintenance group (n = 21) and LL loss group (n = 77). For patients with well-aligned correction (immediate postoperative TPA ≤ 20°, n = 73), they were divided into TPA maintenance group (last follow-up TPA ≤ 20°) and TPA loss group (last follow-up TPA > 20°). The relative gross cross-sectional area (rGCSA) and fat infiltration (FI) of multifidus (MF) and erector spinae (ES), and the relative functional CSA (rFCSA) of psoas major (PS) were measured at L3, L4 and L5 on preoperative magnetic resonance imaging.
Results:
MF rGCSA were significantly smaller in LL loss group than in LL maintenance group. Both MF rGCSA and PS rFCSA were significantly smaller and MF FI was significantly higher in TPA loss group than in TPA maintenance group. Binary logistic regression revealed that the MF rGCSA was an independent factor of LL loss; Large immediate postoperative TPA was an independent risk factor of TPA loss, but not the parameters of paraspinal muscles.
Conclusion:
The effect of paraspinal muscles in lower lumbar segments might be mainly focused on the maintenance of local alignment rather than the global alignment.
Keywords
Introduction
For degenerative lumbar scoliosis (DLS), maintaining sagittal correction alignment after surgery is crucial to a satisfactory clinical outcome. 1 The relevance between sagittal malalignment and postoperative symptoms and functional status has been widely reported.2-4 It is common that patients persistently lose the sagittal alignment even after an appropriate restoration. 5
Local and global alignment are both important for the evaluation of sagittal balance. Loss of lumbar lordosis (LL) is associated with several spinal diseases that require surgical intervention. 6 Studies have shown that obtaining an appropriate LL can improve patients’ quality of life and reduce the incidence of adjacent segment degeneration.7,8 The T1 pelvic angle (TPA), which provides combined information of truncal inclination and pelvic tilt (PT), can reflect the global sagittal alignment more precisely. TPA is also closely related to health-related quality of life in patients with adult spinal deformity.9,10
Multifarious factors such as patient demographics and surgical factors may affect the sagittal alignment.11,12 It is widely accepted that paraspinal muscles should also be considered during the management of spinal deformity.13-15 Some studies have revealed the correlation between paraspinal muscle degeneration and long-term loss of sagittal alignment.5,16,17 However, Yagi et al did not performed a multifactor analysis 5 and Dohzono et al did not take the correction alignment into account. 16 To our knowledge, no report has elucidated the role of paraspinal muscle degeneration in the deterioration of sagittal alignment from well-aligned to poorly-aligned after corrective surgery.
As a consequence, this study was conducted to investigate the difference of paraspinal muscle profiles between DLS patients who maintained the correction alignment and who loss the correction alignment in local and global curve after corrective surgery.
Methods
This was a single-institution retrospective study approved by the relevant institutional Ethics Committee with the requirement for informed consent being waived (M2020497). A total of 98 patients with DLS treated with corrective surgery in our hospital from January 2010 to December 2016 were included. The mean last follow-up duration was 38.3 months. The inclusion criteria were (1) Age > 50 years old at the time of surgery; (2) Cobb angle > 10° which was located in the lumbar spine; (3) Without any history of scoliosis up to adolescence, former spinal surgery and neuromuscular diseases (4) Had complete preoperative and postoperative data. All patients underwent posterior approach and long instrument with fusion ≥ 3 vertebral segments. They were also encouraged to exercise by themselves in the hospital and at home. No 1 received a revision surgery in the final follow-up.
Surgical Procedure
Surgeries were performed by senior surgeons for all included cases. All surgical strategies and approaches were discussed and decided before surgery. Using the posterior midline approach, meticulous exposure of the spine and posterior decompression fusion and fixation with pedicle screw was performed. Then the neural decompression by laminectomy and discectomy was performed after pedicle screws had been implanted. If corrective surgery was needed, Smith-Peterson osteotomy (SPO, n = 23), Ponte osteotomy (n = 5) and pedicle subtraction osteotomy (PSO, n = 3) were applied. After the cage with autogenous bone granules tamponade placed appropriately and rod assembly, posterolateral fusion was performed in all patients.
Sagittal Alignment Evaluation
The preoperative, immediate postoperative, and last follow-up radiographic assessments were analyzed by standing posteroanterior and lateral whole spine X-ray. The parameters including TPA, LL, pelvic incidence (PI) were measured (Figure 1). TPA was defined as the angle subtended by a line from the femoral heads to the center of the T1 vertebral body and a line from the femoral heads to the center of the superior sacral end plate. 10 Considering TPA is the combination of sagittal vertical axis (SVA) and PT and is less affected by variations in standing compensation, we did not conduct the measurement of SVA and PT.
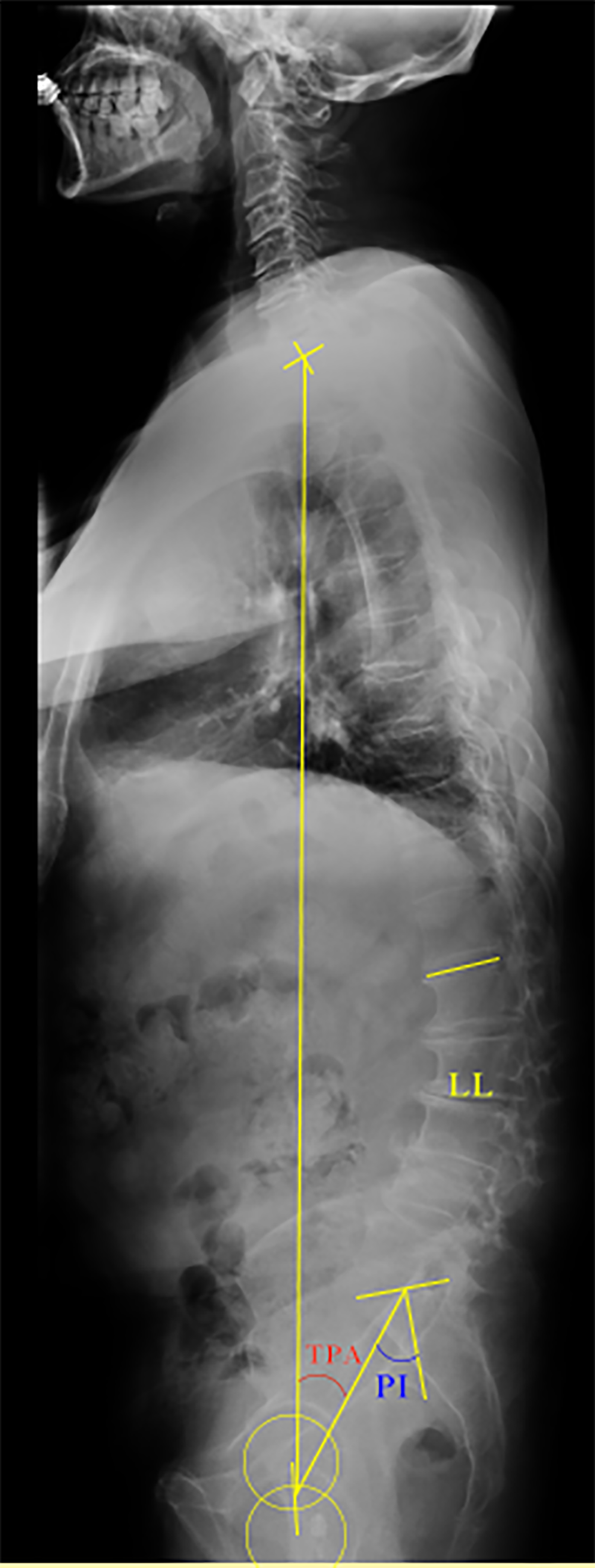
Illustration showing the sagittal alignment parameters, including TPA, LL and PI (a 60-year-old man before corrective surgery).
For local alignment evaluation, all 98 patients were divided into LL maintenance group (last follow-up LL ≥ immediate postoperative LL, n = 21) and LL loss group (last follow-up LL < immediate postoperative LL, n = 77). Due to the indeterminate range of LL reconstruction for Asian people reported by previous studies,18,19 we did not set an operative target of LL and only focused on the decrease of LL after surgery. Banno et al reported that TPA 20° or lesser was the proper target value for corrective surgery in Asian patients. 9 Therefore, for global alignment evaluation, patients with well-aligned correction (immediate postoperative TPA ≤ 20°, n = 73) were then divided into 2 groups: TPA maintenance group (last follow-up TPA ≤ 20°, n = 50) and TPA loss group (last follow-up TPA > 20°, n = 23).
The complications were evaluated on spine radiograph at final follow-up by 2 observers blinded to clinical information. We defined the screw loosening as a 1 mm or wider circumferential radiolucent line around the pedicle screw. 20 Subsidence was defined as greater than 2 mm of cage protrusion through the vertebral endplates. 21 PJK was defined as proximal junctional angle 10° or greater and at least 10° greater than the corresponding preoperative measurement. 22
Back pain visual analog scale (VAS) score, Oswestry disability index (ODI), Japanese Orthopedic Association (JOA) score (29 points) were employed to evaluate symptoms and functional status preoperatively.
Paraspinal Muscle Evaluation on MRI
All enrolled patients had undergone preoperative MRI of thoracolumbar area. MRIs were required with Signa HDxt 3.0 T (General Electric Company). The slice thickness was 3 mm with a 3-mm gap between each slice and the axial MRI was parallel to the inferior endplate of the vertebral body. We measured the multifidus (MF), erector spinae (ES) and psoas major (PS) bilaterally from T2-weighted images at the inferior vertebral endplate of L3, L4 and L5 level. The following parameters were measured on each level by the Image J software (Figure 2): gross cross-sectional area (GCSA, including muscle, intramuscular fat and soft tissue) of MF, ES and intervertebral disc; fat infiltration (FI) of MF and ES was measured by the previously reported thresholding technique16,23; For PS, only functional cross-sectional area (FCSA) was measured in view of the outline of intramuscular fat and soft tissue was not clearly defined. 20 We calculated the mean value of cross-sectional area (CSA) and FI of L3, L4 and L5 to reflect the whole picture in lower lumbar.16,24 To reduce the effect of body shape on muscular parameters, relative cross-sectional area (rCSA, the ratio of cross-sectional area of muscle to that of disc at the same level) was introduced.20,25 rCSA of both gross muscle (G) and functional muscle (F) were measured as rGCSA and rFCSA.
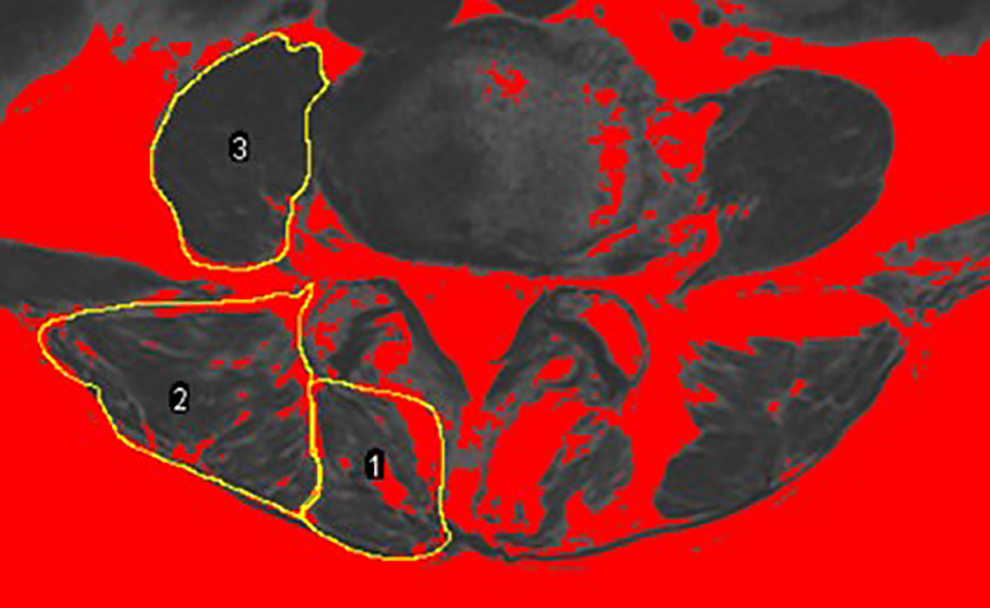
Measurements of paraspinal muscular parameters on axial T2-weighted MRI (a 62-year-old woman). Regions of multifidus (1), erector spinae (2) and psoas muscle (3) at L4 level were outlined by yellow lines. For psoas muscle, only functional muscle was outlined. Thresholding technique to highlight lean muscle area (red area).
To test the reliability, all muscular parameters of 15 patients randomly selected were measured by 2 observers independently. After 3 weeks, the same measurements were performed by 1 observer.
Statistical Analysis
Intraclass correlation coefficient was calculated to test the intra- and inter-rater reliability. Demographic and clinical information, radiographic parameters and paraspinal muscle characteristics were compared between patients with and without maintenance of alignment at final follow-up. The Mann-Whitney U test or ANOVA (for continuous data) and Chi-square test (for categorical data) were conducted to determine the statistical difference. Binary logistic regression model was used to identify the independent risk factors of loss of alignment. Age, gender, follow-up duration, muscular parameters that had significant differences between groups (MF rGCSA, MF FI and PS rFCSA), and immediate postoperative LL and TPA were included in the regression model. Receiver operating characteristic (ROC) curve was utilized to find out the most optimum cut-off point of which presented the largest Youden index. Statistical significance was set at P value < .05. All statistical analyzes were performed using SPSS 22.0 (IBM Corp).
Results
78.6% (77/98) of the patients developed LL loss and 31.5% (23/73) of the patients developed TPA loss after corrective surgery at final follow-up. The follow-up duration showed a significant difference between the patients with and without loss of LL (P < .05). However, the age, gender, body mass index (BMI), the number of osteotomies, fusions extending to the sacrum, number of fusion levels and interbody fusions were not significantly different between LL maintenance group and LL loss group (all P > .05), or between TPA maintenance group and TPA loss group (all P > .05) (Table 1). Moreover, there was no significant difference of preoperative VAS, ODI and JOA scores between LL maintenance group and LL loss group (all P > .05), or between TPA maintenance group and TPA loss group (all P > .05) (Table 1).
Descriptive Summary of Patients Between Alignment Maintenance Group and Alignment Loss Group.
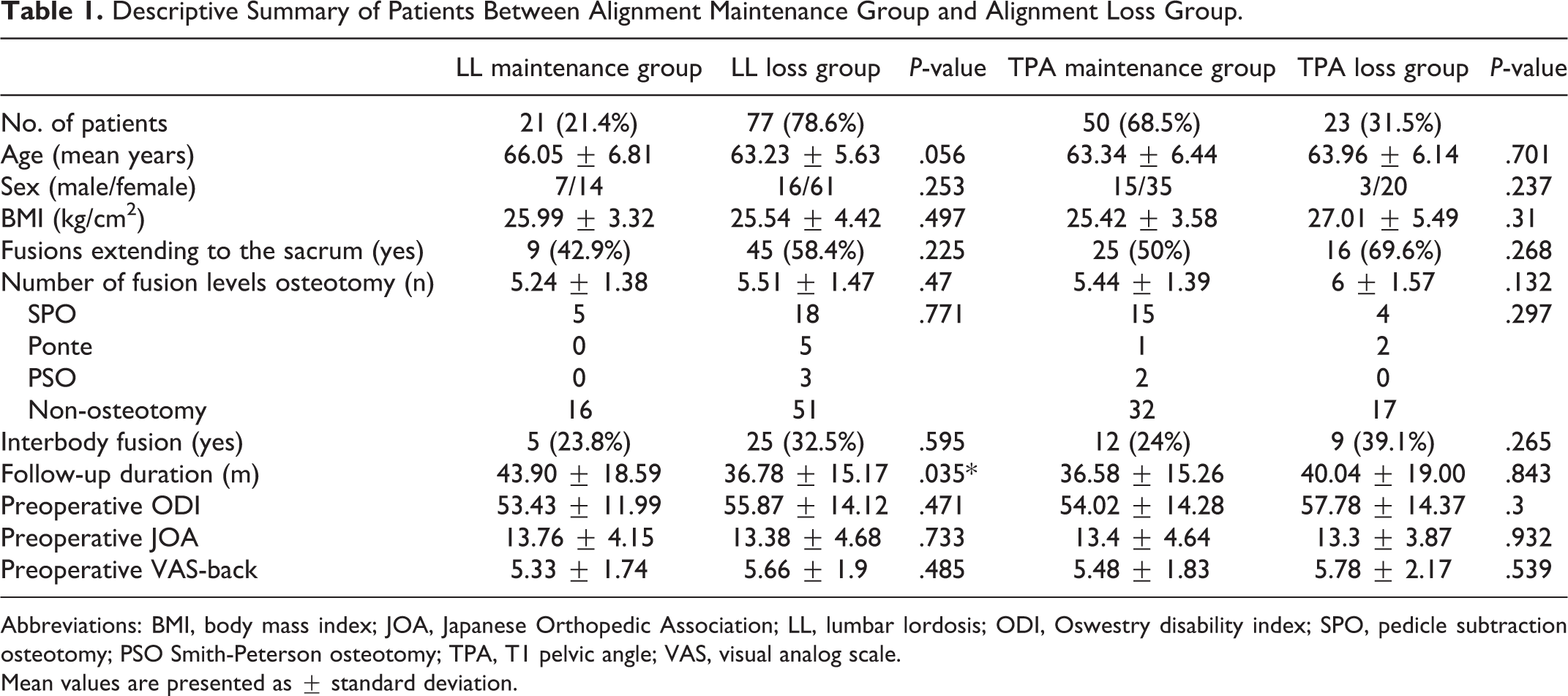
Abbreviations: BMI, body mass index; JOA, Japanese Orthopedic Association; LL, lumbar lordosis; ODI, Oswestry disability index; SPO, pedicle subtraction osteotomy; PSO Smith-Peterson osteotomy; TPA, T1 pelvic angle; VAS, visual analog scale.
Mean values are presented as ± standard deviation.
*P < .05.As shown in Table 2, immediate postoperative TPA, LL and PI had no significant difference (all P > .05) between LL maintenance group and LL loss group. However, TPA loss group had a greater TPA and smaller LL than TPA maintenance group immediately after the surgery (all P < .05). At the final follow-up, both LL loss group and TPA loss group had a greater TPA loss and greater LL loss than LL maintenance group and TPA maintenance group respectively (all P < .05). Besides, there was no significant difference in screw loosening rate at last follow-up between LL maintenance group and LL loss group (P > .05), or between TPA maintenance group and TPA loss group (P > .05).
Comparison of Sagittal Alignment, Screw Loosening and Paraspinal Muscle Characteristics Between Alignment Maintenance Group and Alignment Loss Group.
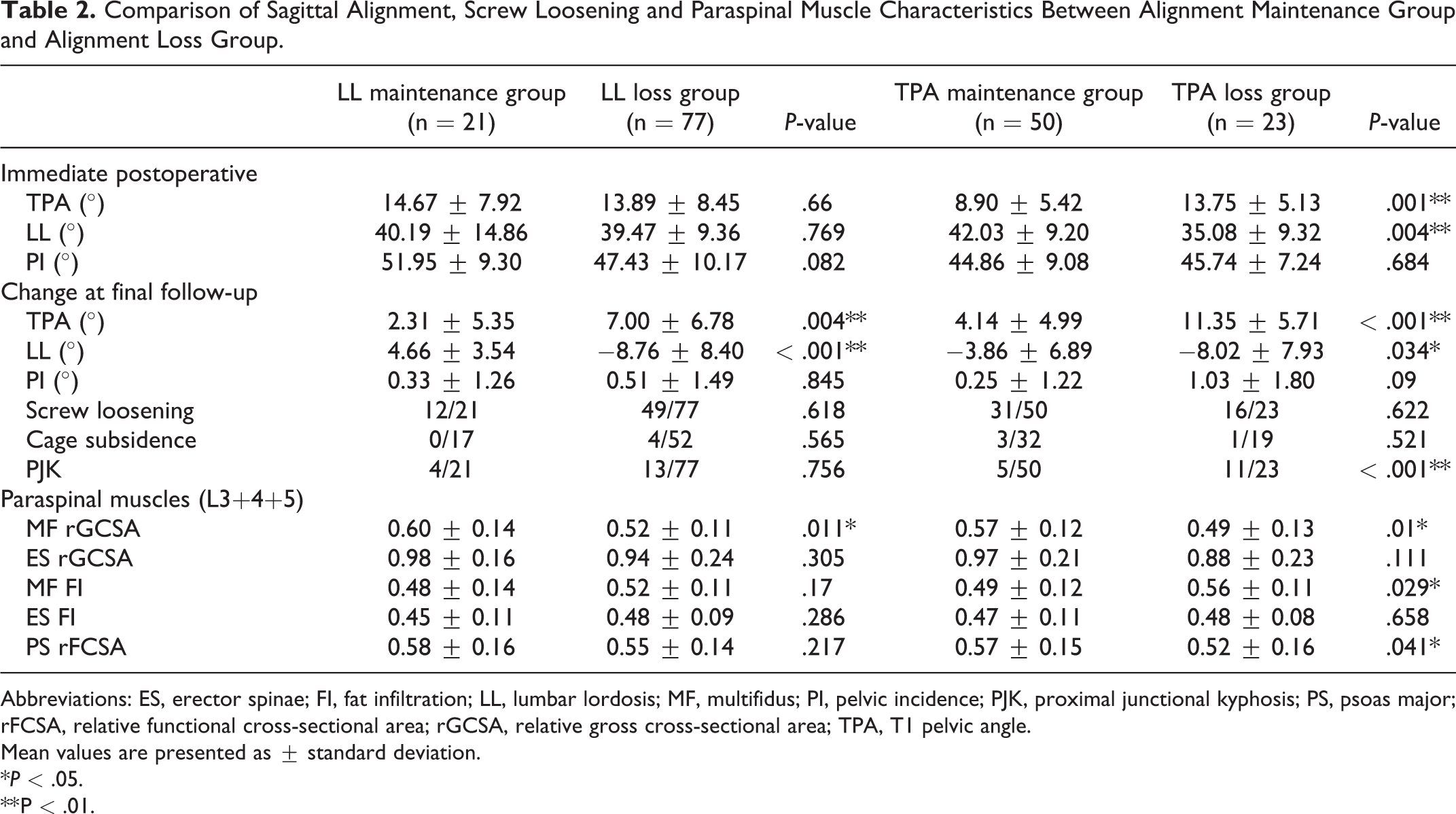
Abbreviations: ES, erector spinae; FI, fat infiltration; LL, lumbar lordosis; MF, multifidus; PI, pelvic incidence; PJK, proximal junctional kyphosis; PS, psoas major; rFCSA, relative functional cross-sectional area; rGCSA, relative gross cross-sectional area; TPA, T1 pelvic angle.
Mean values are presented as ± standard deviation.
*P < .05.
** P < .01.
In LL maintenance group and LL loss group, MF rGCSA showed a significant difference between the 2 groups (P = .011), whereas the parameters of ES and PS did not (all P > .05). In TPA loss group, MF rGCSA was significantly smaller (P = .01) and MF FI was significantly higher (P = .017) than in TPA maintenance group. Besides, PS rFCSA was also significantly smaller in patients with loss of TPA (P = .041) (Table 2).
Binary logistic regression revealed that the MF rGCSA was an independent factor of LL loss (P = .014, OR = 0.94; Table 3); Large immediate postoperative TPA was an independent risk factor of TPA loss (P = .014, OR = 0.94), but not the parameters of paraspinal muscles (Table 4). With the use of ROC curve and the Youden index, we found that the best cut-off value of MF rGCSA for predicting the postoperative loss of LL was 0.56 (AUC = 0.672, sensitivity = 0.688, specificity = 0.677) (Figure 3). According to the best cut-off value, patients were divided into MF rGCSA ≥ 0.56 group and MF rGCSA ≤ 0.56 group. For MF rGCSA < 0.56 group, the percentage of patients with loss of LL was 88.1% (52/59), while it was 64.1% (25/39) for MF rGCSA ≥ 0.56 group, which showed a significant difference (P = .005).
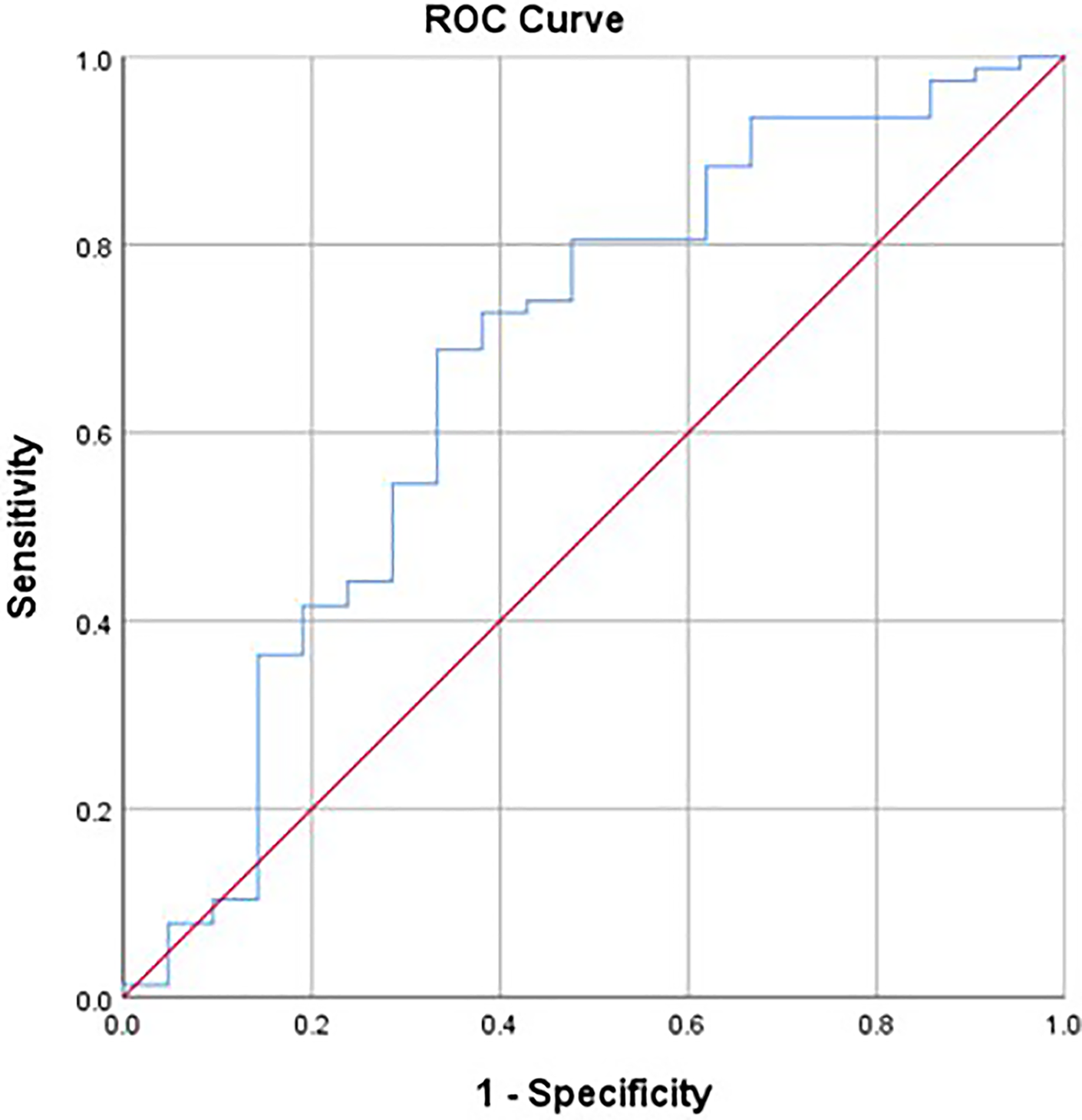
ROC curve to find the optimum cut-off point of MF rGCSA to predict the postoperative loss of local alignment.
Independent Risk Factors of Postoperative Loss of LL Identified by Logistic Regression.
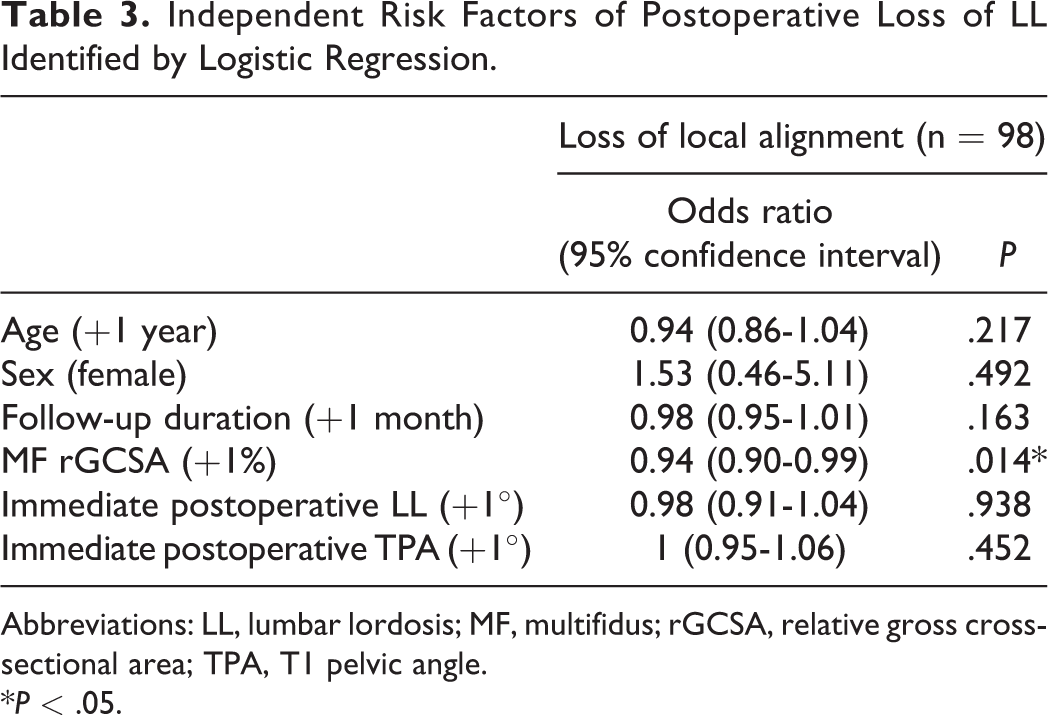
Abbreviations: LL, lumbar lordosis; MF, multifidus; rGCSA, relative gross cross-sectional area; TPA, T1 pelvic angle.
*P < .05.
Independent Risk Factors of Postoperative Loss of TPA Identified by Logistic Regression.
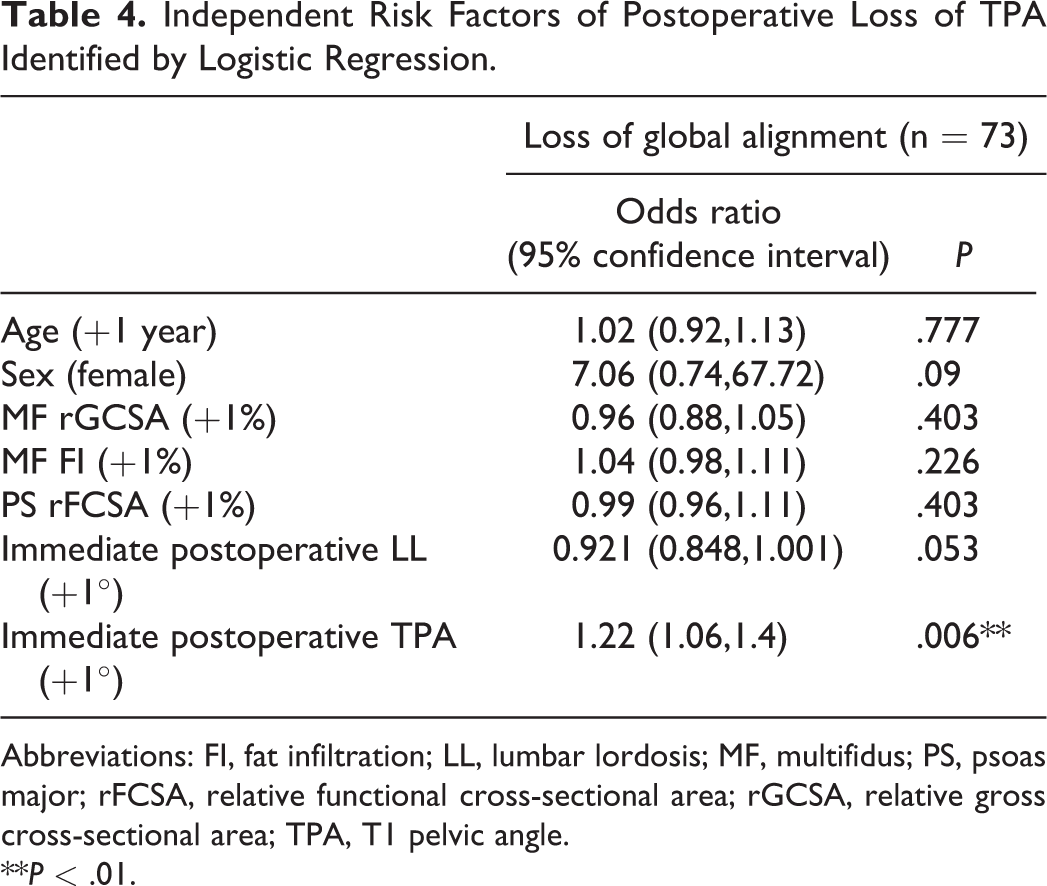
Abbreviations: FI, fat infiltration; LL, lumbar lordosis; MF, multifidus; PS, psoas major; rFCSA, relative functional cross-sectional area; rGCSA, relative gross cross-sectional area; TPA, T1 pelvic angle.
**P < .01.
The intraclass correlation coefficient for both intra-rater and inter-rater reliability of MF rGCSA, ES rGCSA, MF FI, ES FI and PS rFCSA were > 0.8 (Table 5).
Intra-Rater and Inter-Rater Reliability of Paraspinal Muscle Parameters Using Intraclass Correlation Coefficient.
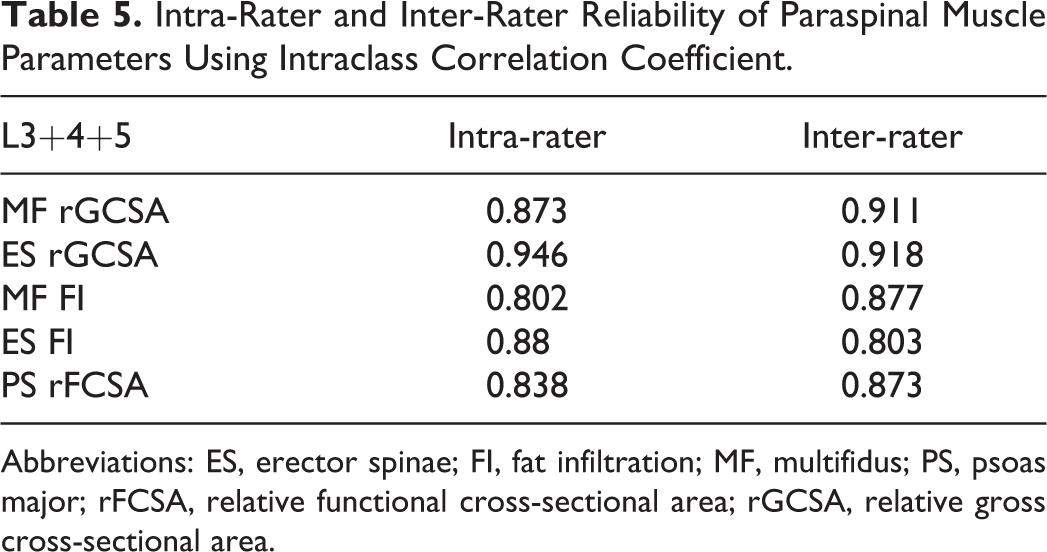
Abbreviations: ES, erector spinae; FI, fat infiltration; MF, multifidus; PS, psoas major; rFCSA, relative functional cross-sectional area; rGCSA, relative gross cross-sectional area.
Discussion
Compared to coronal deformity, maintaining an appropriate sagittal curve after corrective surgery is more important to achieve a desired outcome in DLS patients. However, the role of paraspinal muscle degeneration in sagittal malalignment development is poorly understood. In this study, we focused on the DLS patients who maintained the corrective curve and who lost the curve after obtaining an appropriate restoration. We found out some important clinical observation. First, MF rGCSA was an independent factor of LL loss; the best cut-off value of MF rGCSA for predicting the postoperative loss of local alignment was 0.56. Second, immediate postoperative TPA was an independent risk factor of TPA loss, whereas the parameters of paraspinal muscles were of no effect.
In our study, 78.6% DLS patients developed LL loss at final follow-up. While Gao et al have reported that DLS patients who lost LL were 46.4% (32/69) at final follow-up. They defined LL loss group as patients losing LL above the average. In addition, TPA loss after correction occurred in 31.5% DLS patients. Ryan et al investigated patients with preoperative TPA>20° and found that 13 of the 73 poor-aligned patients (3 months TPA > 20°) developed TPA loss between 3 months and 1 year after surgery, while only 4 of the 63 well-aligned patients (3 months TPA < 15.9°) deteriorated between 3 months and 1 year after surgery. 26
Our study revealed that MF rGCSA was smaller in both LL loss group and TPA loss group. MF plays an important role in maintaining the posterior stability, which contributes approximately 2 thirds of the active stabilizing effect on the vertebral column. 27 According to a previous study, decreased CSA of paraspinal muscles coincided with reduced muscle strength, thus resulting in difficulty in maintaining posture. 28 Besides, we found that MF FI was higher in patients with loss of TPA. Apart from decreasing in muscularity, high-proportioned intramuscular fat was also associated with poor muscle strength. 29
In our study, rGCSA of ES was also lower in patients with local and patients with global alignment loss, whereas no significant difference has been found. ES, as 1 of back extensor muscles, can also antagonize the abdominal muscles flexion. 30 However, the reason why the ES was not effective in maintaining balance required further work to explain. A study reported that ES morphology was poorly related to back function. 31 Wang et al also demonstrated that MF had an effect on postoperative functional status, but ES did not. 23 Univariate analysis showed that patients with maintenance of TPA had a larger PS rFCSA than patients with loss of TPA. A study demonstrated that smaller PS CSA was significantly correlated with decreased relative flexion strength. 29 The abundant lean muscle of PS can better reflect the powerful strength to support the spine when standing upright, as fatty component could not provide contractile forces.
In multivariate analysis, the finding that MF rGCSA was independently associated with LL loss indicated that patients who had a small size of MF before surgery were prone to loss the appropriate local alignment. Previous studies have demonstrated that graft subsidence, hardware failure and adjacent level issues could also cause LL loss.32,33 In our study, there was no difference of cage subsidence, screw loosening and PJK between LL maintenance group and LL loss group. Besides, the correction of alignment also had no significant difference between two groups (Supplemental Table S1). The findings could reveal that the stability supported by paraspinal muscles was important and independent of instruments. While Lee et al found that paraspinal muscle degeneration was not correlated with postoperative change of LL in patients with degenerative flat back. 34 The cause of the discrepancy with our results might be interpreted by the different diseases and study design. Besides, we found that the MF rGCSA ≥ 0.56 was the optimum cut-off value to predict the loss of LL. Therefore, when performing corrective surgery for patients with a small MF muscularity at lower lumbar segments, the risk of postoperative development of malalignment and more rigid fixation in surgery might be considered.
As for the prediction of postoperative TPA loss, we found that all paraspinal muscles parameters were not independent risk factors. Therefore, it can be speculated that paraspinal muscles in lower lumbar mainly work for the maintenance of local alignment rather than the global alignment. Lee et al reported that the lower paraspinal muscle condition was not associated with upper spinal alignment improvement, since the supporting function exerted by paraspinal muscles might not extend beyond the upper part of the spine. 34 Yagi et al’s study and Dohzono et al’s study might also verify our hypothesis. They have demonstrated that preoperative paraspinal muscle degeneration was not corelated to the SVA improvement.5,16
Of note, we found that both immediate postoperative LL and TPA were not factors influencing the maintenance of LL after surgery in univariate and multivariate analysis. Whether a patient could maintain local alignment was more affected by muscles than the correction of sagittal parameters. Furthermore, our analysis clearly demonstrated a significant correlation between immediate postoperative TPA and loss of TPA after corrective surgery. It reminded us that a patient with a large TPA, even when a desired global balance (TPA ≤ 20°) was obtained after correction, would still be inclined to global imbalance. However, considering that TPA is affected by the unfused segments, it is difficult to control it during the surgery.
We recognized limitations in the present study. Firstly, there were no postoperative MRIs to evaluate the condition of muscle injury after the operation, which might reduce the predictive value of paraspinal muscles on the development of malalignment. Secondly, the final follow-up was approximately 3 years after surgery, and during this period of time various factors might affect the sagittal alignment. Thirdly, this was a retrospective study that had the inherent bias. In spite of that, our study was conducted with the use of quantitative parameters of paraspinal muscles on MRI, which have a good intra-rater and inter-rater reliability.
Conclusions
The MF rGCSA was an independent factor of LL loss, and a large immediate postoperative TPA was an independent risk factor of TPA loss in DLS patients that underwent corrective surgery and interbody fusion. However, the preoperative paraspinal muscle morphology was not related to TPA loss in the multivariate analysis. The effect of paraspinal muscles in lower lumbar segments might be mainly focused on the maintenance of local curve rather than the global curve.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_21925682211022284 - Paraspinal Muscle Degeneration as an Independent Risk for Loss of Local Alignment in Degenerative Lumbar Scoliosis Patients After Corrective Surgery
Supplemental Material, sj-docx-1-gsj-10.1177_21925682211022284 for Paraspinal Muscle Degeneration as an Independent Risk for Loss of Local Alignment in Degenerative Lumbar Scoliosis Patients After Corrective Surgery by Gengyu Han, Wei Wang, Siyu Zhou, Wei Li, Bo Zhang, Zhuoran Sun and Weishi Li in Global Spine Journal
Footnotes
Authors’ Note
Gengyu Han, Wei Wang, and Siyu Zhou contributed equally to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No.81 871 807).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.