
Abstract
Study Design
Retrospective cohort.
Objectives
To assess the incidence, time to presentation, and independent risk factors for retropharyngeal hematoma causing airway obstruction following anterior cervical discectomy and fusion (ACDF).
Methods
The PearlDiver national database was queried for patients who underwent one- to four-level ACDF. Patients who underwent concomitant posterior fusion or had surgical indications related to malignancy, trauma, or infection were excluded. Patients were stratified based on the development of a retropharyngeal hematoma causing airway obstruction within 7 days. Descriptive statistics assessed differences in patient demographics and comorbidities. Univariable and multivariable regression analyses identified independent predictors.
Results
Among 430,542 patients, 140 (0.03%) developed postoperative retropharyngeal hematoma leading to acute airway obstruction. A significant proportion of patients presented within 1 day of surgery (45 patients, 32.14%), with 23 (16.43%) on day zero and 22 (15.71%) on day 1. Notably, 40.71% of cases occurred after discharge. Independent predictors included ossified posterior longitudinal ligament (OPLL) (aOR: 8.07, P < 0.001), male gender (aOR: 2.30, P < 0.001), hypertension (aOR: 1.67, P < 0.05), viral hepatitis (aOR: 1.57, P < 0.05), and comorbidity index (aOR: 1.14, P < 0.001).
Conclusion
This study identified a 0.03% incidence of retropharyngeal hematoma leading to acute airway obstruction and several independent predictors, including comorbidity index, male gender, hypertension, viral hepatitis, and OPLL. Surgeons should consider overnight admission for observation in patients with these risk factors, as a significant proportion of hematomas present within 1 day of surgery.
Introduction
Anterior cervical discectomy and fusion (ACDF) is a widely performed surgical procedure for the treatment of cervical myelopathy and/or radiculopathy. 1 Due to its efficacy and low complication rates, many surgeons have adopted outpatient ACDF to reduce health care costs, with research demonstrating its safety and high satisfaction rate among patients.2,3 However, retropharyngeal hematoma, while rare, remains a feared complication due to its potential to rapidly cause airway obstruction. If not promptly recognized and managed, it can lead to anoxic brain injury or death.
Prior studies have reported the incidence of retropharyngeal hematoma following ACDF ranging from 0.2% to 5.6%.4-11 Risk factors for this complication include hypertension, multi-level fusions, ossified posterior longitudinal ligament, and preoperative anticoagulation use.9,11 However, previous research has been limited to single-institution studies with small sample sizes, often identifying fewer than 20 cases of this complication. Given the rarity of retropharyngeal hematomas, single-institution data may not provide an accurate estimate of its true incidence or comprehensively identify independent predictors.
Recognizing risk factors for this complication is essential for developing mitigation strategies to reduce its incidence. Since retropharyngeal hematomas frequently develop within the first 24 hours postoperatively, understanding these risk factors ensures careful patient selection for outpatient ACDF and helps determine which patients may benefit from overnight admission. 11 Therefore, this study leverages a large national database to determine the incidence and independent predictors of retropharyngeal hematoma causing airway obstruction following ACDF.
Methods
Data Source and Study Population
The patient sample was identified through a query of the PearlDiver Mariner Database (PearlDiver Technologies, Fort Wayne, IN, USA). PearlDiver is a comprehensive, nationwide dataset that includes approximately 170 million deidentified patient records, encompassing demographics, diagnostic, and procedural data from all payer types and both inpatient and outpatient settings. Given that all patient data is deidentified, patient consent was waived, and Institutional Review Board approval was not required.
Using Current Procedural Terminology (CPT) codes, the database was queried for patients who underwent primary or revision 1 to four-level ACDF (CPT-22551 & CPT-22554) between 2010 to April 2023. Exclusion criteria included patients with surgical indications for malignancy, trauma, or infection. Additionally, to exclude circumferential cervical fusions, which are typically performed on an inpatient basis, patients who underwent posterior cervical fusion within 14 days of ACDF were also excluded.
Using International Classification of Disease ninth (ICD-9) and 10th (ICD-10) edition codes, patients were stratified based on the presence or absence of a retropharyngeal hematoma causing airway obstruction within 7 days of the index procedure (Supplemental Table 1). As there are no specific ICD codes for retropharyngeal hematoma, patients were identified using a proxy definition: a concomitant diagnosis of hematoma and acute airway obstruction.
Study Endpoints
The endpoints of this study were to determine the incidence of retropharyngeal hematoma causing airway obstruction, the time from surgery to presentation, and to identify associated risk factors, including age, Elixhauser Comorbidity Index (ECI), gender, tobacco use, coagulopathy, hypertension, coronary artery disease (CAD), alcohol abuse, deficiency anemia, obesity, chronic kidney disease (CKD), liver disease, diabetes, viral hepatitis, ossified posterior longitudinal ligament (PLL), preoperative anticoagulation, and the number of spinal segments fused. Preoperative anticoagulation was defined as the use of Heparin, Warfarin, Clopidogrel, Aspirin, Rivaroxaban, or Factor Xa inhibitors within 7 days of the index procedure.
Statistical Analysis
Differences in patient demographics and comorbidities were assessed using Pearson’s Chi-squared test of independence for categorical variables and Student’s t test for continuous variables. Univariable and multivariable regression analyses were performed to identify independent predictors of retropharyngeal hematoma resulting in airway obstruction. The multivariable model included covariates to control for confounding variables, such as age, gender, ECI, and the number of spinal segments fused. All statistical analyses were performed using RStudio (Version 4.4.2) within the PearlDiver Mariner Database. A P-value of <0.05 was considered statistically significant. To protect patient anonymity, any groups containing less than eleven patients are denoted with an asterisk.
Results
Patient Population and Characteristics
A total of 430,542 patients who underwent ACDF during the study period were identified, of whom 140 (0.03%) developed postoperative retropharyngeal hematoma leading to acute airway obstruction.
Demographic and Comorbidity Differences.
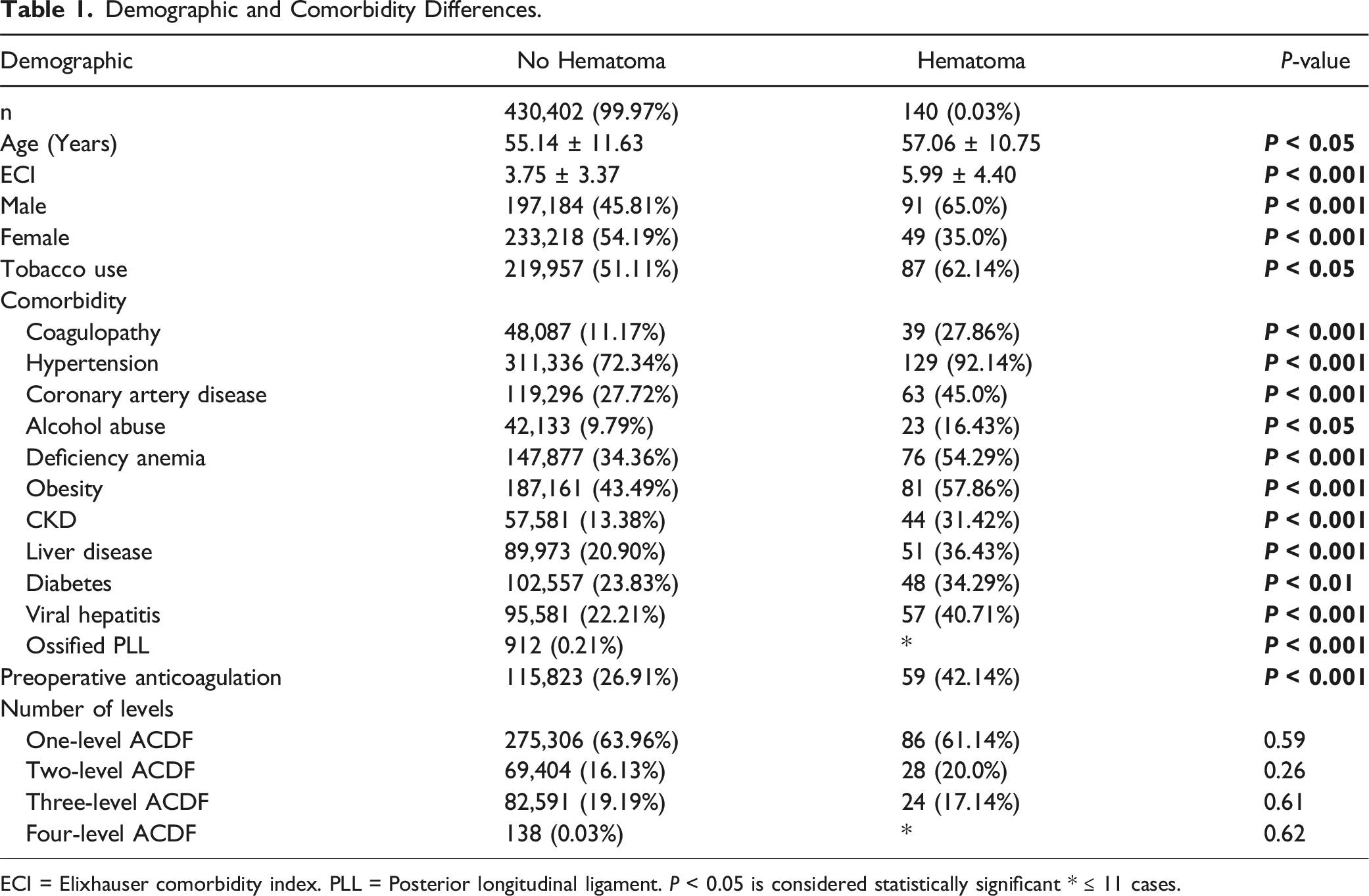
ECI = Elixhauser comorbidity index. PLL = Posterior longitudinal ligament. P < 0.05 is considered statistically significant * ≤ 11 cases.
There were no significant differences in the number of one- (61.14% vs 63.96%, P = 0.59), two- (20.0% vs 16.13%, P = 0.26), three- (17.14% vs 19.19%, P = 0.61), and four-level fusions (<11 cases vs 138 cases, P = 0.62) (Table 1).
Patients most frequently presented within 1 day of surgery (45 patients, 32.14%), with 23 (16.43%) presenting on postoperative day zero and 22 (15.71%), presenting on postoperative day 1. The mean time from ACDF to hematoma presentation was 2.82 ± 2.06 days. The distribution of patients presenting across each postoperative day is summarized in Figure 1. Time from ACDF to retropharyngeal hematoma presentation.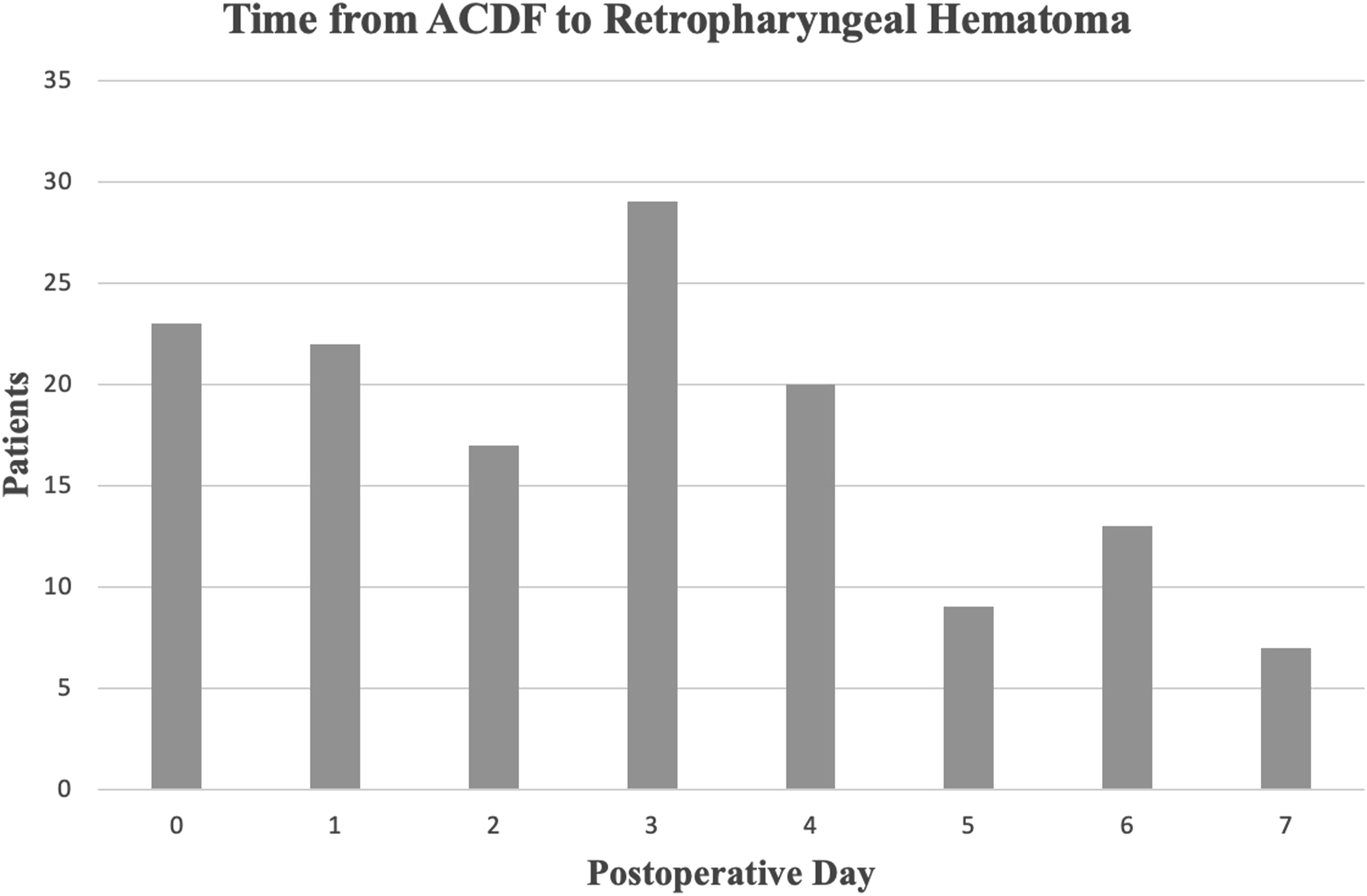
Additionally, 57 cases (40.71%) were classified as readmissions, while 83 (59.29%) represented extended initial hospitalizations.
Predictors of Retropharyngeal Hematoma
Univariable and Multivariable Analyses of Risk Factors.
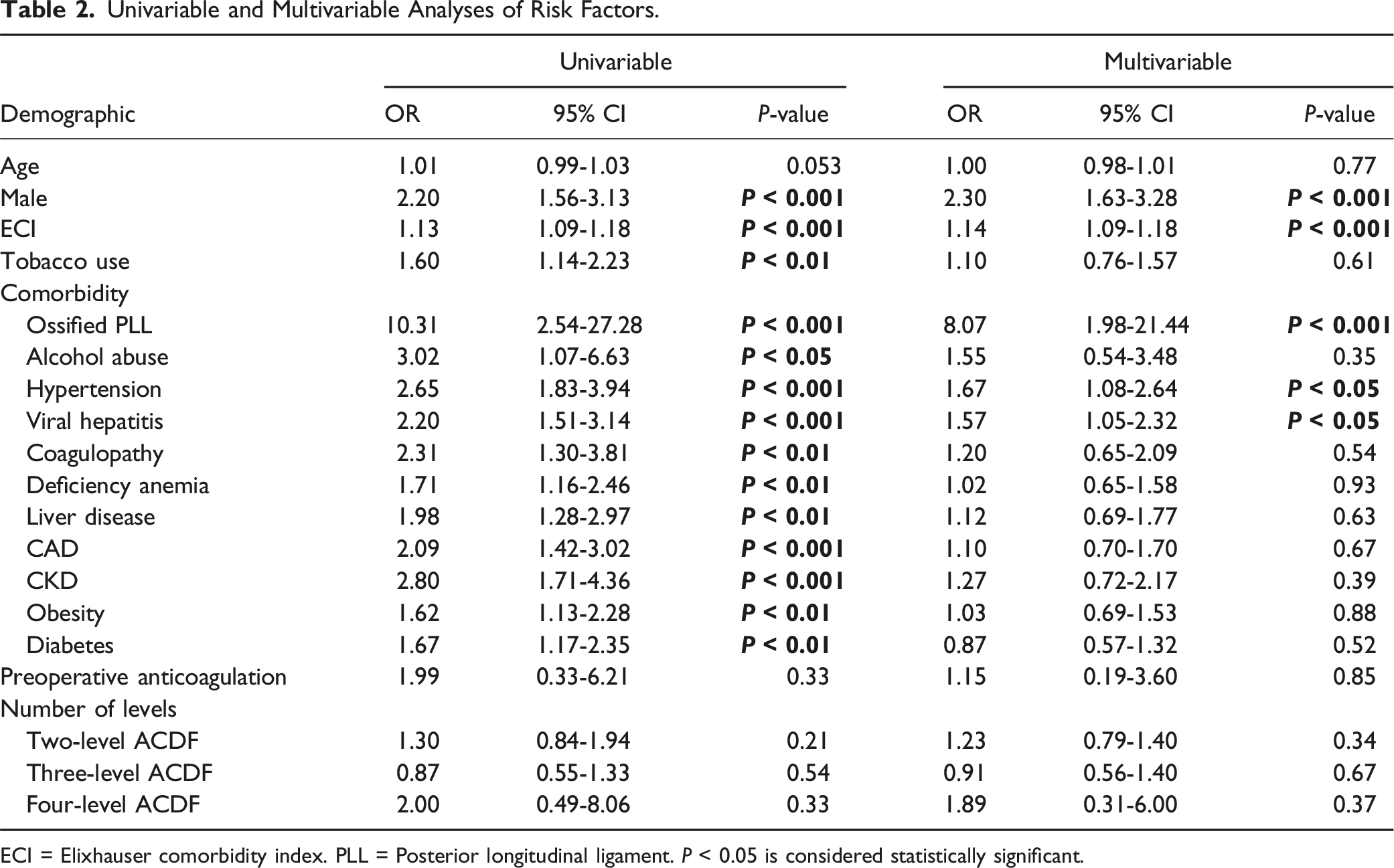
ECI = Elixhauser comorbidity index. PLL = Posterior longitudinal ligament. P < 0.05 is considered statistically significant.
Multivariable regression analysis identified independent predictors of retropharyngeal hematoma, including ossified PLL (aOR: 8.07, [1.98-21.44], P < 0.001), male gender (aOR: 2.30, [1.63-3.28], P < 0.001), hypertension (aOR: 1.67, [1.08-2.64], P < 0.05), viral hepatitis (aOR: 1.57 [1.05-2.32], P < 0.05), and ECI (aOR: 1.14, [1.09-1.18], P < 0.001) (Figure 2, Table 2). Predictors of Retropharyngeal Hematoma following ACDF. ECI = Elixhauser comorbidity index. PLL = Posterior longitudinal ligament.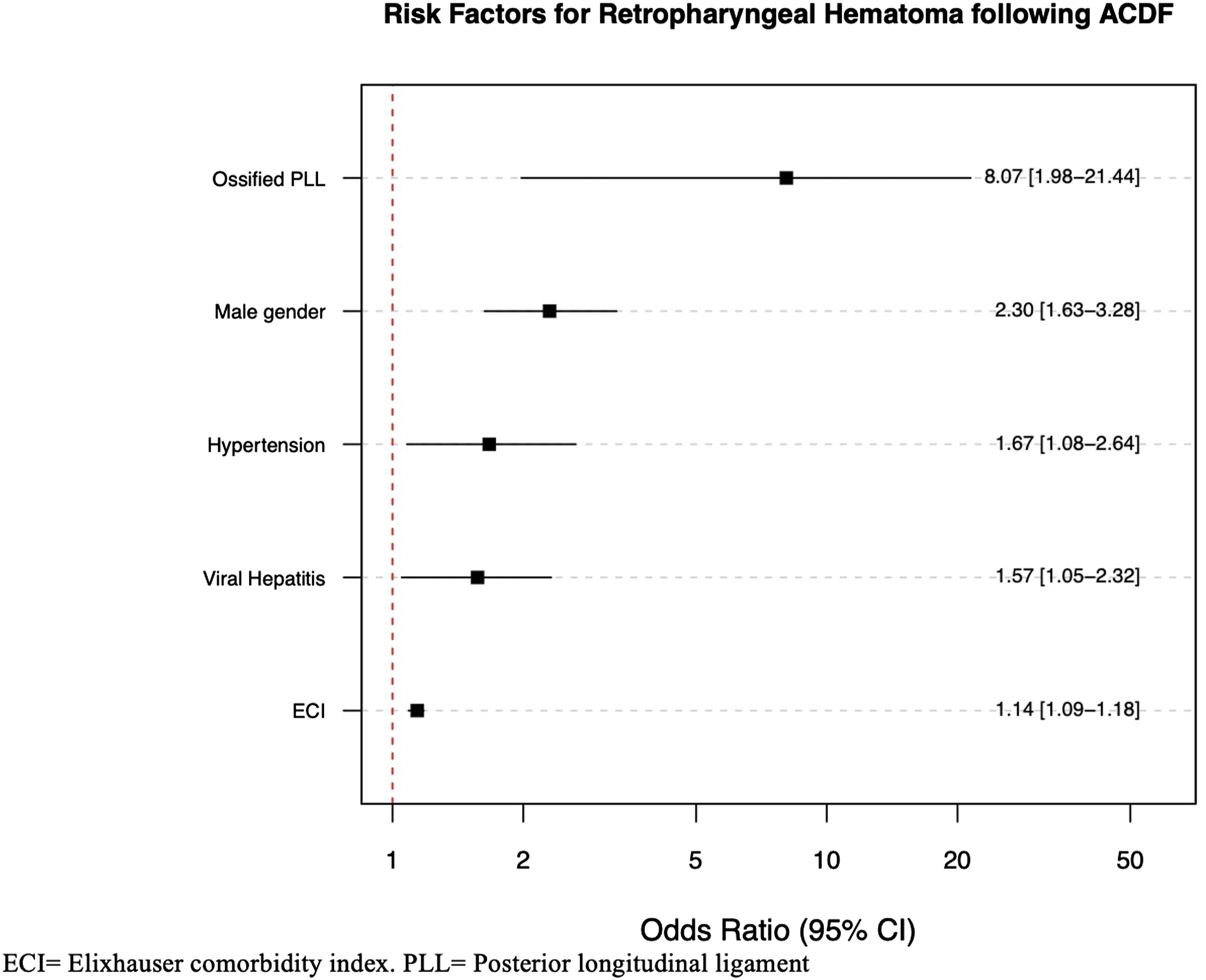
Discussion
Retropharyngeal hematoma following ACDF is a rare but life-threatening complication. Due to its low incidence, studying this complication using a single-institution database presents significant challenges. This study aimed to determine the incidence of retropharyngeal hematoma leading to airway compromise following ACDF. We identified a 0.03% incidence with patients most frequently presenting within 1 day of surgery, and several independent predictors, including ECI, male gender, hypertension, viral hepatitis, and ossified PLL. This study represents the first national-level investigation into this complication and the largest analysis to date. Our findings provide insights into risk mitigation strategies, potentially helping to prevent this life-threatening complication and enabling surgeons to identify patients who may benefit from inpatient observation.
The reported incidence of this complication in the literature ranges from 0.2% to 5.6%; however, our reported incidence falls below this range.4-10 Our lower incidence is likely due to the fact that we focused exclusively on cases that resulted in acute airway obstruction, as not all cases of retropharyngeal hematoma lead to airway compromise. With this approach, this study identified more clinically significant cases, as smaller hematomas can be managed with observation and steroids. For instance, in a retrospective review of 1015 consecutive ACDF cases, Fountas et al reported that 57 patients (5.6%) developed retropharyngeal hematoma. Of these, only 24 (2.4%) required emergent surgical evacuation, while the remaining 33 patients (3.2%) were managed conservatively with close observation. 4 Furthermore, the larger sample size employed in our study likely provides a more precise estimate of the true incidence, reinforcing that the risk of life-threatening retropharyngeal hematoma following ACDF is lower than previously thought and further supporting the overall safety of the procedure.
Among patient demographics, we identified male gender as a significant predictor of retropharyngeal hematoma. Hardman et al. reported higher rates of all-cause airway obstruction following ACDF in males compared to females. 12 Although this finding could be influenced by unmeasured confounders, such as higher BMI among male patients, we attempted to account for these factors in the multivariable analysis by adjusting for comorbidity burden. Additionally, prior institutional studies with more granular clinical data have identified male gender as a risk factor for hematoma formation following other anterior neck surgeries, such as thyroidectomy, further supporting its role as a contributing factor in this complication.13,14 While the specific mechanism remains unclear, it may be due to sex-related anatomical differences in the upper airway, predisposing males to pharyngeal collapse. 15 Some have also suggested that this could be attributed to stronger neck musculature in men, which may lead to tearing of sutures or of previously ligated vessels upon awakening from anesthesia. 13 This may be further influenced by the greater prevalence of hypertension among males, which was also identified as a significant predictor in our analysis. 14
Our findings regarding hypertension as a risk factor align with prior studies. Qu et al identified a 1.06-fold increased likelihood of retropharyngeal hematoma formation following ACDF in patients with elevated diastolic blood pressure, while Hardman et al reported an almost 2-fold increased risk of airway obstruction in hypertensive patients.11,12 Patients with hypertension have vascular stiffness and impaired autonomic control of vessel size, leading to intraoperative hypotension due to the vasodilatory effects of anesthetic agents, followed by postoperative hypertension. 16 This rebound to elevated pressures may result in re-bleeding that was not apparent at the time of incision closure. Surgeons should ensure preoperative hypertension is well-managed, coordinating with primary care physicians when necessary. Additionally, blood pressure should be closely monitored postoperatively, especially in hypertensive patients, and those with elevated pressures should be strongly considered for admission and treated accordingly. Beta-blockers and calcium channel blockers have been shown to be effective and safe for perioperative blood pressure management. 17 Furthermore, measures should be taken to prevent postoperative elevation of blood pressure, such as facilitating a smooth extubation process to prevent triggering coughing or retching and maintaining adequate pain management. 18
The relationship between viral hepatitis and retropharyngeal hematoma risk has not yet been fully established, but it may be related to its coagulopathic effects. Hepatitis can lead to thrombocytopenia through mechanisms such as hypersplenism, decreased thrombopoietin production, and platelet destruction. 19 Additionally, hepatic parenchymal disease associated with viral infection can impair coagulation factor synthesis, further increasing bleeding risk. 20 Hepatopulmonary syndrome, which affects 16% to 34% of the cirrhotic population, can potentially cause postoperative dyspnea and coughing, which may elevate postoperative pressures. 21 Careful attention should be paid to preoperative liver function tests, particularly since hepatitis infection can be asymptomatic while still causing liver damage. 22 The MELD-Na score, which reliably predicts postoperative outcomes in patients with liver damage, can be calculated using routine preoperative lab values such as creatinine, BUN, bilirubin levels, sodium, and serum AST. 23 This patient population should be strongly considered for overnight admission.
With an 8-fold increased risk, ossified PLL was the strongest predictor in our analysis. Similarly, Qu et al reported a 4.06-fold increased risk, and O’Neil et al reported a 6.8-fold increase in relative risk for retropharyngeal hematoma in this patient population following ACDF.9,11 Surgical treatment of OPLL through ACDF is technically challenging and carries higher complication rates compared to techniques like laminoplasty. This is due to the difficulty in separating the ossified ligament from the dura, leading to high rates of durotomy, and subsequent prolonged intraoperative time, a known risk factor for retropharyngeal hematoma.24-26 It is important to acknowledge however, that the prolonged surgical duration and elevated blood loss in these cases may lead to a consumptive coagulopathy, which could serve as an unmeasured confounding variable in our analysis.
Regarding surgical variables, we did not identify an association between the number of levels fused and hematoma risk. However, O’Neil et al reported a 2.6-fold increased risk in multi-level fusions, and Sagi et al. identified an elevated risk of laryngeal edema causing postoperative airway obstruction in multi-level procedures, particularly those involving the C2, C3, and C4 vertebrae. 24 These findings may be related to the extended operative times and increased intraoperative blood loss. For instance, Sagi et al. associated operative times exceeding 5 hours with an increased risk of airway obstruction following ACDF. 24
The timing of retropharyngeal hematoma onset is critical in determining its clinical severity and guiding postoperative management. While our study showed that a substantial proportion of cases occurred within the first 24 hours following ACDF, the database did not allow for precise identification of onset within that period. However, prior research has shown that the most life-threatening hematomas typically present within the first 6 hours postoperatively. 6 Taken together, our findings and those of prior studies suggest that the overall incidence of clinically significant hematoma is lower than previously reported and reinforce the safety of ACDF. However, surgeons should consider a six-hour postoperative observation period in patients with the identified risk factors. Such an approach may optimize early detection while supporting safe outpatient practices in appropriately selected patients. This recommendation is further supported by our finding that over 40% of hematomas occurred after discharge, further underscoring the importance of short-term monitoring in at-risk patients.
Limitations
This study is not without limitations. The PearlDiver database relies on accurate ICD coding to capture relevant patients; thus, inaccuracies in coding could result in misclassification and underreporting of cases. This limitation also applies to potential miscoding by surgeons during medical charting. Another limitation inherent to the database is that we could not quantify the severity of the diseases that were identified as independent risk factors. Additionally, because our study focused only on patients with airway obstruction due to hematoma, minor hematomas that did not cause significant airway compromise may have been excluded, potentially underestimating the true incidence of this complication.
Furthermore, due to the limitations of the database, we were unable to account for key intraoperative variables such as operative time, surgical approach, estimated blood loss, surgeon experience, and vertebral level involvement, all of which may influence outcomes. Moreover, as a retrospective study, these findings provide observational data and do not establish causality. Despite these limitations, the greatest strength of this study lies in its large sample size, making it the most comprehensive national analysis to date on the incidence and risk factors for retropharyngeal hematoma causing airway obstruction following ACDF.
Conclusion
This study identified a 0.03% incidence of retropharyngeal hematoma leading to acute airway obstruction and several independent predictors, including ECI, male gender, hypertension, viral hepatitis, and ossified PLL. Since retropharyngeal hematoma most commonly presents on postoperative day 1, surgeons should strongly consider overnight admission for observation in patients with these risk factors. Further research is needed to develop evidence-based risk mitigation protocols to further decrease its incidence.
Supplemental Material
Supplemental Material - Retropharyngeal Hematoma Following Anterior Cervical Discectomy and Fusion: Identifying Risk to Prevent a Life-Threatening Complication
Supplemental Material for Retropharyngeal Hematoma Following Anterior Cervical Discectomy and Fusion: Identifying Risk to Prevent a Life-Threatening Complication by Henry Avetisian, William Karakash, Camille Flynn, Atishay Mathur, Mirbahador Athari, Marc A. Abdou, Dil Patel, Jeffrey C. Wang, Raymond J. Hah, and Ram K. Alluri in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Henry Avetisian, William Karakash, Camille Flynn, Athishay Mathur, Mirbahador Athari, Marc A. Abdou, and Dil Patel have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccential Robotics for lectures and presentations.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
ORCID iDs
Data Availability Statement
Data is not publicly available but can be available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.