
Abstract
Study Design
A systematic review and meta-analysis.
Objectives
This systematic review and meta-analysis aim to evaluate the diagnostic accuracy of CT in detecting PLC injuries in traumatic thoracolumbar fractures.
Methods
A comprehensive search of PubMed/MEDLINE, Embase, and Web of Science was conducted up to January 2025. Studies were included if they examined the diagnostic validity of CT for PLC injuries compared with MRI with predefined outcomes (true/false positives/negatives). Quality assessment was performed using the QUADAS-2 tool, and statistical analysis involved bivariate binomial regression to generate summary receiver operating characteristic (SROC) curves and pooled estimates of sensitivity and specificity.
Results
Eight studies involving 1440 patients were included. The pooled sensitivity and specificity of CT for PLC injury detection were 75% (95% CI: 68 to 80, P = 0.00) and 87% (95% CI: 71 to 95, P = 0.00), respectively. The area under the curve (AUC) from the SROC analysis was 0.81 (95% CI: 0.78 to 0.84), indicating fair diagnostic accuracy. Meta-regression analysis revealed that sensitivity and specificity remained consistent across advanced CT techniques, multiplanar reconstruction, and full MRI protocol, but extensive trauma, CT 16-64 or ≥128 slices, and 3.0 T MRI scanner influenced it. No significant publication bias was detected.
Conclusion
This meta-analysis demonstrates that CT has fair diagnostic accuracy for detecting PLC injuries in traumatic thoracolumbar fractures, supporting its clinical utility. Future research should explore integrating advanced imaging technologies to enhance CT’s diagnostic precision.
Keywords
Introduction
The Posterior Ligament Complex (PLC) is a key stabilizing structure of the spine, and the lesions could cause persistent pain, neurological deficit and late spine kyphosis. 1 Magnetic Resonance Imaging (MRI) is currently the gold standard for assessing PLC integrity. 2 However, its routine use is not available in all centers due to its higher costs, poor feasibility for polytraumatic patients, and longer scanning time compared to other imaging modalities. 3
Computed Tomography (CT) is considered a secondary option for detecting PLC lesions. It is a faster method and is available in more medical centers compared to MRI. 4 However, it has limitations in assessing ligament structures compared to MRI, even though it has been used to infer PLC injuries based on vertebral body translation, facet diastasis, and interspinous widening (ISW). 5
Earlier reviews failed to demonstrate adequate diagnostic accuracy of CT for PLC injuries and presented poor interobserver reliability. 6 Recent studies were successful in showing very good agreement between CT and MRI in the diagnosis of PLC injuries. Khurana et al 7 used accuracy analysis and reported that 2 positive CT findings were sufficient to provide a positive predictive value (PPV) high to confirm PLC, excluding the necessity for subsequent MRI.
Thus, whether CT is equally useful in diagnosing PLC injuries compared to MRI is still an issue that has not been completely answered in the scientific field. Therefore, this systematic review and meta-analysis aim to elucidate this question.
Methods
Search Strategy and Data Extraction
We conducted a comprehensive search of PubMed/MEDLINE, Embase, and Web of Science (Clarivate) from their inception to January 2025. The search used the following keywords: (Tomography OR Computed Tomography OR X-ray) AND (“posterior ligamentous complex” OR “posterior ligament*”) AND (“injury” OR “trauma” OR “traumatic” OR “fracture”). No specific filters were applied during the search process. Two authors (R.A.S.S. and P.Q.M.) extracted independent data using predefined criteria. Disagreements were resolved by a third author (L.F.). The data collection followed a standardized approach, capturing information on study design, patient baseline characteristics, and the outcomes of interest.
Inclusion and Exclusion Criteria
Two authors (R.F.O.S.M and A.N.) evaluated the studies for inclusion based on the following criteria: prospective or retrospective design examining the diagnostic validity of CT in PLC injuries and at least having one pre-set outcome of interest, such as (1) True Positives, (2) True Negatives, (3) False Positives, or (4) False Negatives.
Exclusion criteria were: (1) not full-text available studies, (2) animal or pre-clinical studies without human patients, (3) duplicate publications with only the most complete version included, (4) studies with less than four enrolling patients, ie, case reports or small series, (5) abstracts or conference proceedings.
Quality Assessment
The methodological quality assessment was made by one independent reviewer (I.R.M.) using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool. 8 Studies with QUADAS points above nine were considered with high heterogeneity.
Statistical Analysis
The analysis was performed using Stata 14.2 with the midas package. 9 A summary ROC (SROC) curve was generated through bivariate binomial regression to evaluate diagnostic accuracy. Forest plots provided pooled estimates of the area under the curve (AUC), sensitivity, and specificity, with 95% confidence intervals (CIs). A binormal mixed model was applied to assess diagnostic performance across different studies.
A scatter plot was used to illustrate the distribution of studies based on positive (LR+) and negative likelihood ratios (LR−). A Fagan nomogram estimated post-test probabilities of malignancy based on pre-test probabilities, contextualizing the clinical utility of the diagnostic test.
Publication bias was examined using Deek’s funnel regression test, where a P-value <.05 indicated significant asymmetry. Heterogeneity was assessed through the I2 statistic, with thresholds of <25% for low and >75% for high heterogeneity. A funnel plot and Deek’s test were used to further investigate potential reporting bias.
Bivariate analysis was used in an attempt to model sensitivity and specificity simultaneously, as well as their natural association. Goodness-of-fit was assessed utilizing deviance, Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC) in order to test model adequacy as well as compare competitive models. Bivariate normality was tested to confirm that the assumption of normally distributed logit-transformed sensitivity and specificity was valid and, thus, the bivariate binomial regression model. Detection of outliers was done by applying influence diagnostics and leverage analysis to detect studies having disproportionate effects on the pooled estimates to ascertain the robustness of the meta-analysis outcomes.
Results
Study Selection
The flow diagram in Figure 1 summarizes the study selection process. A total of 483 records were identified from PubMed (223), EMBASE (165), and Web of Science (95). After removing 168 duplicate records, 315 studies were screened based on title and abstract, leading to the exclusion of 295 studies. Of the remaining twenty studies, ten were excluded due to the following reasons: studies involving animal models (n = 4), case reports (n = 1), lack of a defined population (n = 1), or absence of relevant outcomes (n = 6). Ultimately, eight studies were included in the final review.10–17 Prisma flow diagram.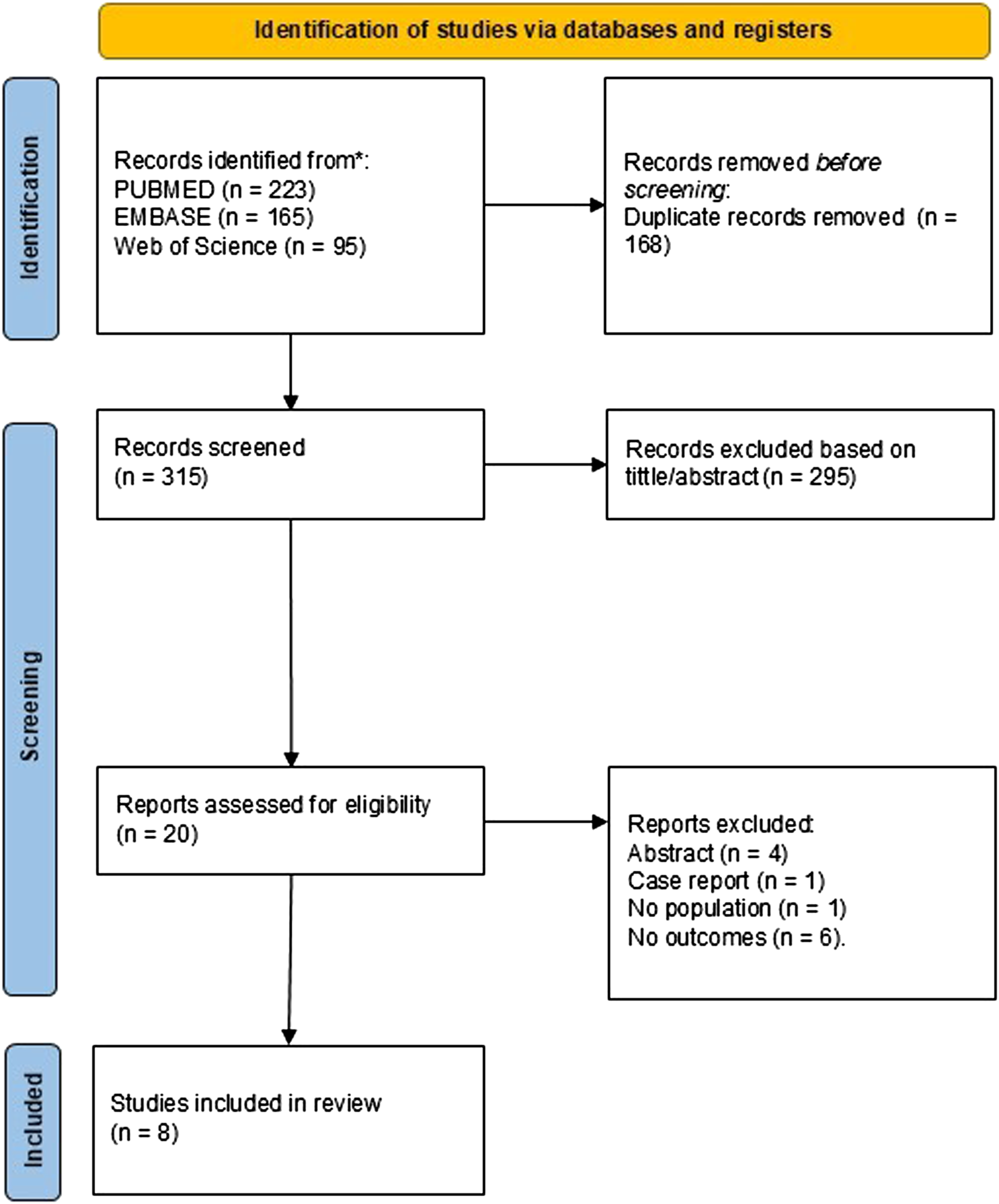
Baseline Characteristics of Included Studies and Population.
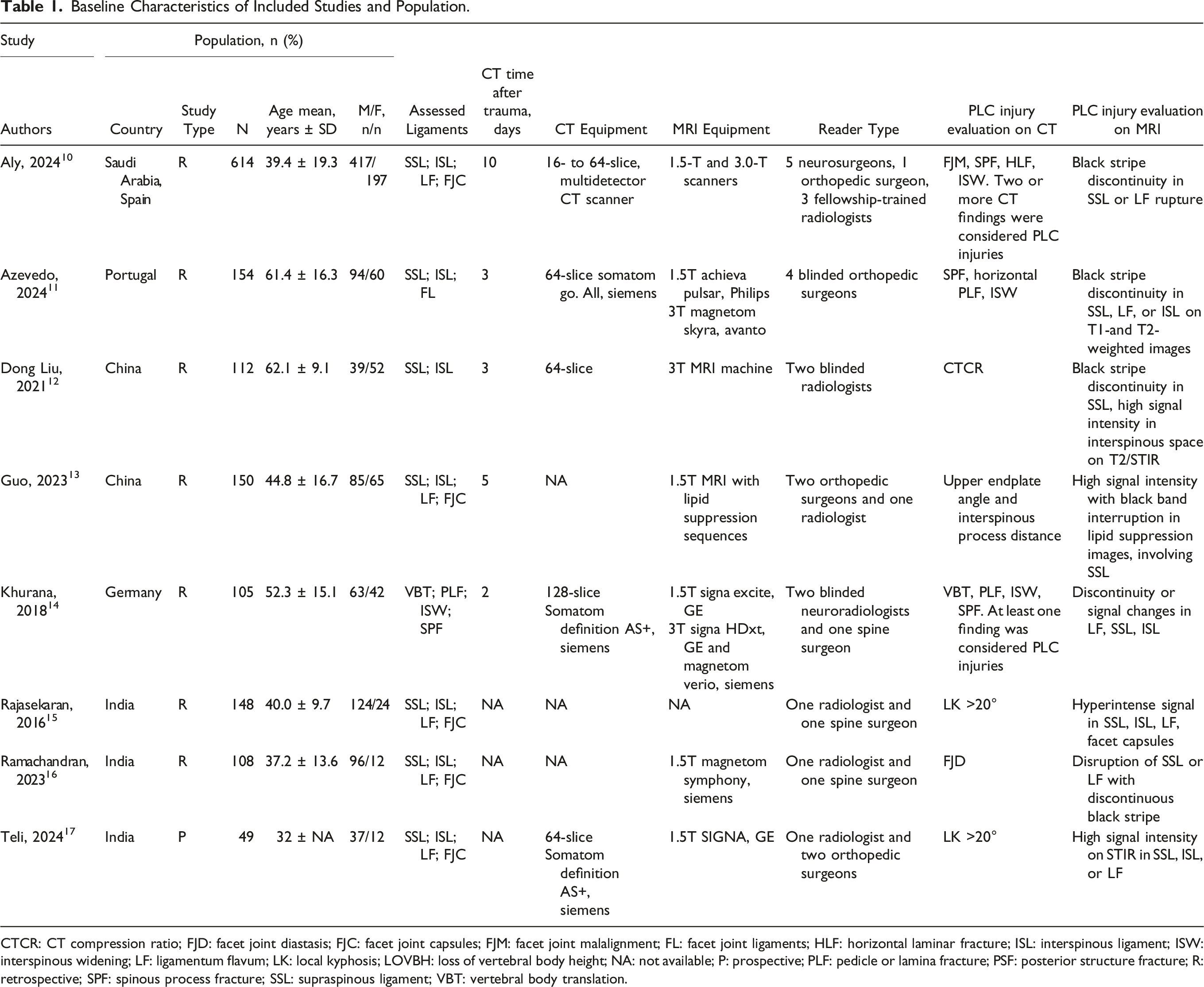
CTCR: CT compression ratio; FJD: facet joint diastasis; FJC: facet joint capsules; FJM: facet joint malalignment; FL: facet joint ligaments; HLF: horizontal laminar fracture; ISL: interspinous ligament; ISW: interspinous widening; LF: ligamentum flavum; LK: local kyphosis; LOVBH: loss of vertebral body height; NA: not available; P: prospective; PLF: pedicle or lamina fracture; PSF: posterior structure fracture; R: retrospective; SPF: spinous process fracture; SSL: supraspinous ligament; VBT: vertebral body translation.
Quality Assessment
Based on Figure 2, most domains showed a low risk of bias, indicating a strong methodological quality in patient selection, index test application, reference standard, and flow/timing. However, some studies presented unclear risks in specific domains due to insufficient reporting of blinding or case selection criteria. A few studies had a high risk of bias in patient selection, mainly due to retrospective designs or lack of consecutive patient inclusion. Regarding applicability concerns, most studies aligned well with the review question, with only minor concerns in patient selection and reference standard applicability. These findings suggest that the overall evidence is robust but highlights the need for clearer methodological reporting in future studies. Quality assessment.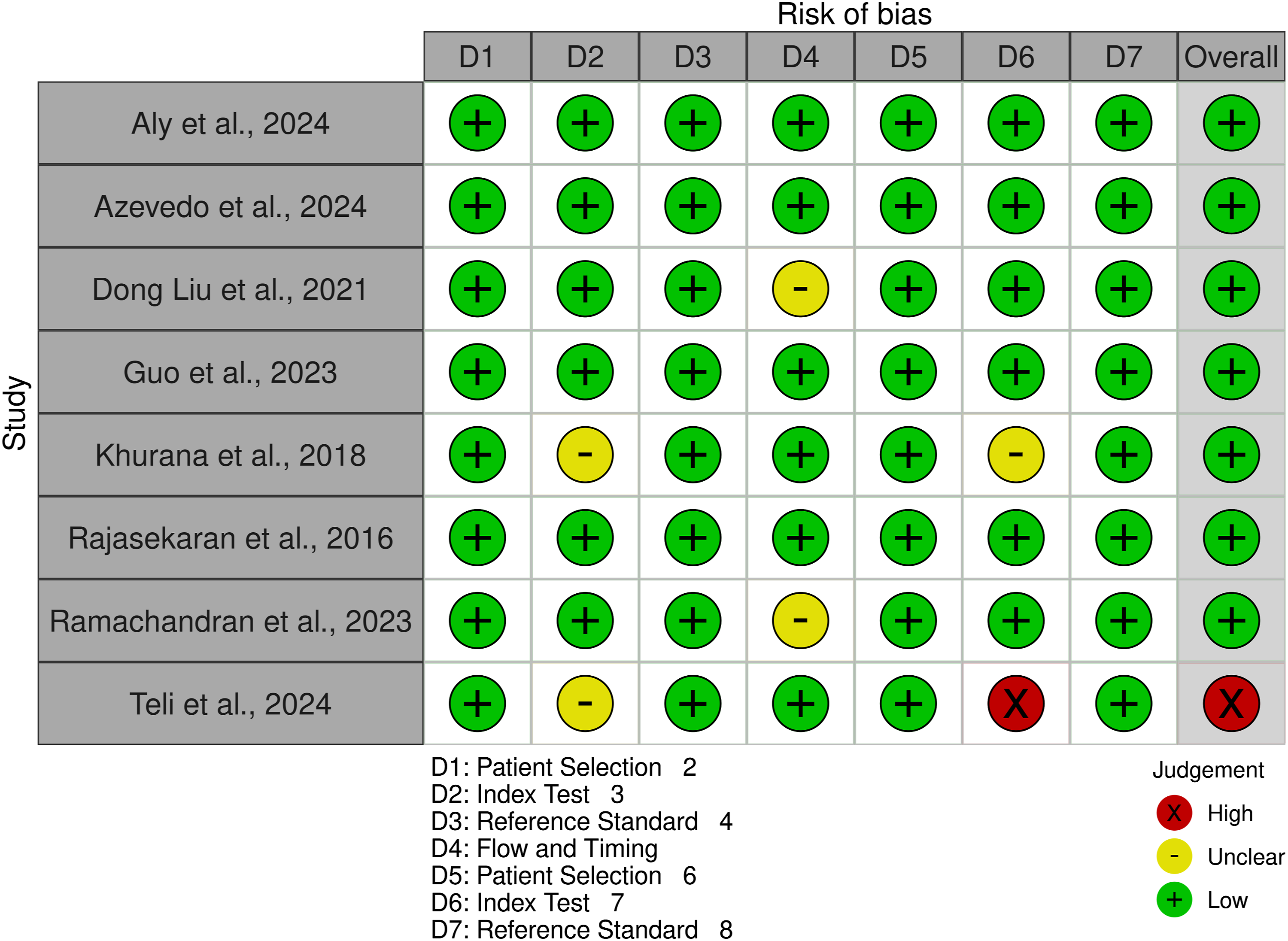
Diagnostic Accuracy
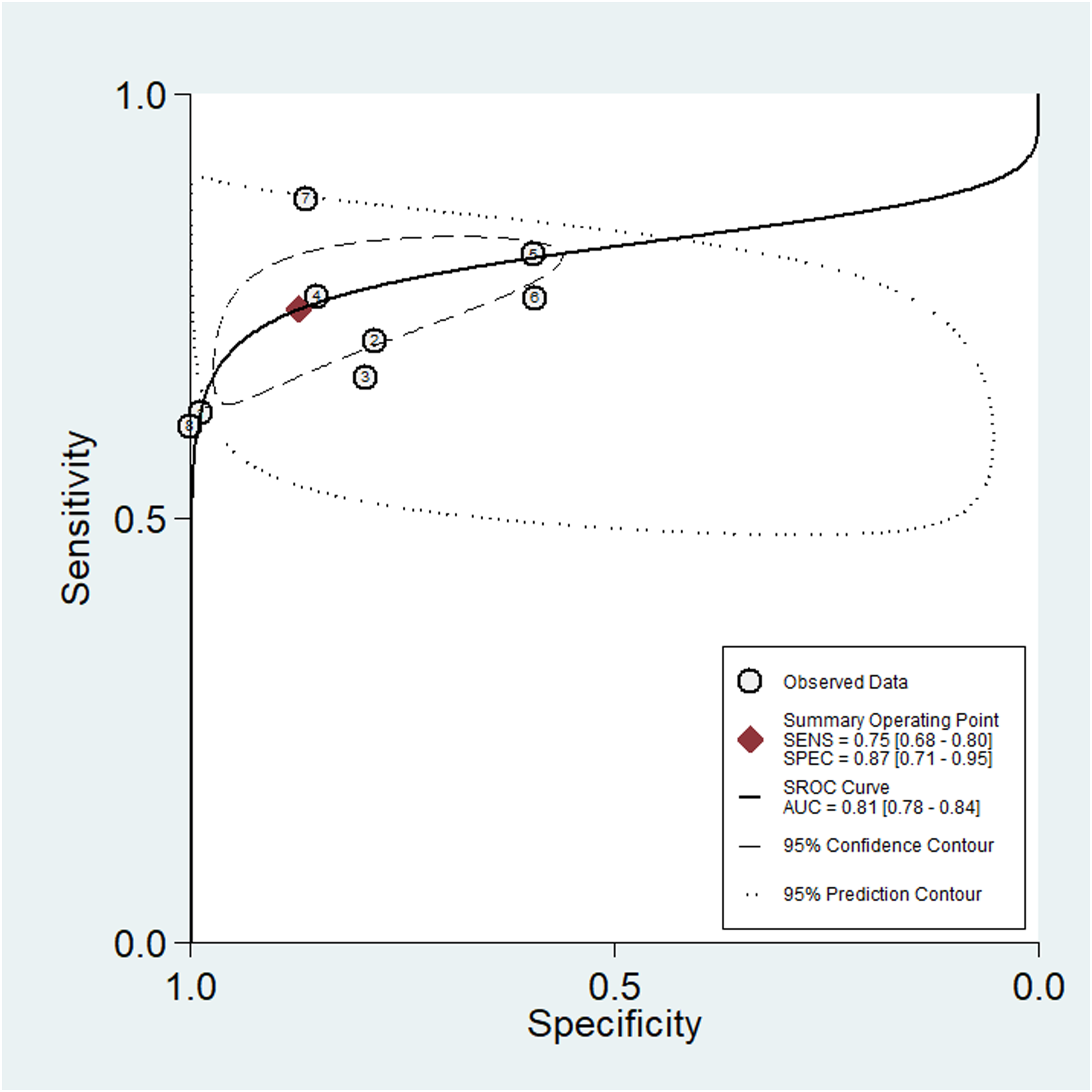
A meta-analysis of CT scans for detecting PLC injuries in the thoracic and lumbar spine provided the following summary estimates (Figure 3): Sensitivity, 0.75 (95% CI: 0.68 to 0.80, P = 0.00, I2 = 82.46); specificity, 0.87 (95% CI: 0.71 to 0.95, P = 0.00, I2 = 97.29), Positive Likelihood Ratio, 5.85 (95% CI: 2.53 to 13.54), Negative Likelihood Ratio 0.29 (95% CI: 0.24 to 0.35). The diagnostic odds ratio (DOR) was 20 (95% CI: 9 to 46). The AUC from the summary receiver operating characteristic (SROC) analysis was 0.81 (95% CI: 0.78 to 0.84), as shown in Figure 4. Plots of diagnostic accuracy measures of sensitivity and specificity. Summary ROC plot.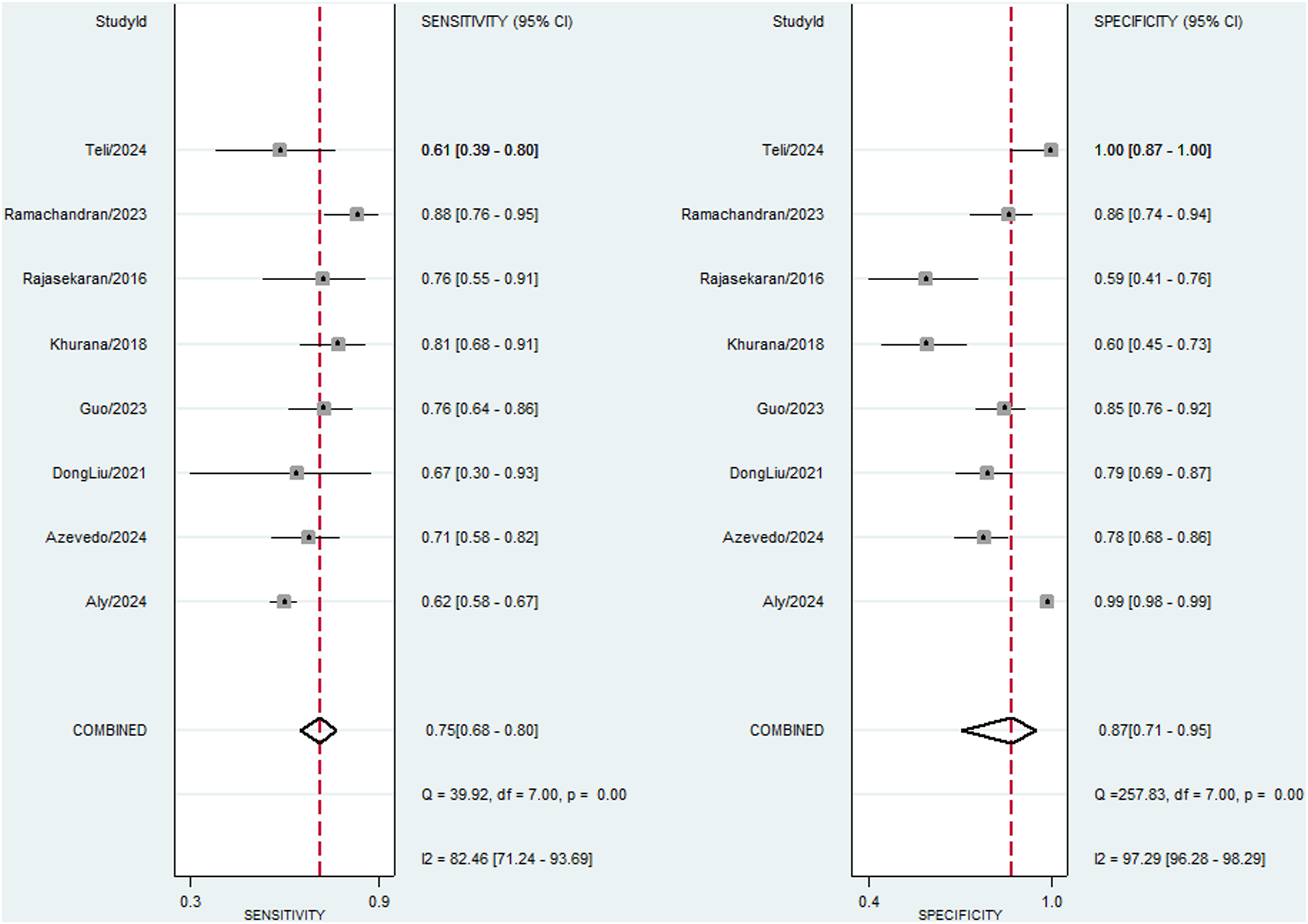
The Fagan nomogram (Figure S1, Supplementary Material) illustrates the clinical effectiveness of CT scans in detecting PLC injuries. With a pre-test probability of 25%, the positive likelihood ratio (LR+) of 6 raised the post-test probability of trauma to 66%. Conversely, the negative likelihood ratio (LR-) of 0.29 decreased the post-test probability to 9%. Additionally, the posterior probability analysis (Figure S2, Supplementary Material) further emphasizes the diagnostic value of CT scans. The test achieved an unconditional negative predictive value (NPV) of 0.76 (95% CI: 0.69 to 0.83) and an unconditional PPV of 0.84 (95% CI: 0.76 to 0.92) across a prevalence range of 25% to 75%.
The scatter plot (Figure S3) illustrates the positive and negative likelihood ratios (LRP and LRN) for CT in diagnosing PLC injuries. The summary point, located within the quadrant of high LRP (>10) and low LRN (<0.1), highlights CT’s diagnostic reliability, with strong evidence suggesting it effectively confirms the presence of PLC injuries while minimizing the likelihood of false negatives. The spread of individual data points reinforces the consistency of CT’s diagnostic performance across studies.
Quality Assessment and Publication Bias
The meta-regression analysis (Figure 5) revealed that study design significantly influenced sensitivity (P < 0.001) and specificity (P < 0.01). Extensive trauma revealed a statistically significant influence on sensitivity (P < 0.05) but not in specificity. CT scanner with 16-64 slices or ≥128 slices revealed a statistically significant influence in sensitivity (P < 0.001) but not in specificity. 3.0 T MRI scanner revealed a statistically significant influence in sensitivity (P < 0.001) but not in specificity. No significant effect was observed for the advanced CT techniques (Soft tissue and bone algorithms, multiplanar reconstruction - MPR, including axial, coronal, sagittal planes), full protocol (T1, T2, and STIR sequences), confirmed PLC injury (Findings include ISW >4 mm, fracture markers such as FMA, HLF, SPF, LK, PSF), reinforcing the robustness of CT’s diagnostic performance in PLC injuries. Meta-regression analysis of CT sensitivity and specificity.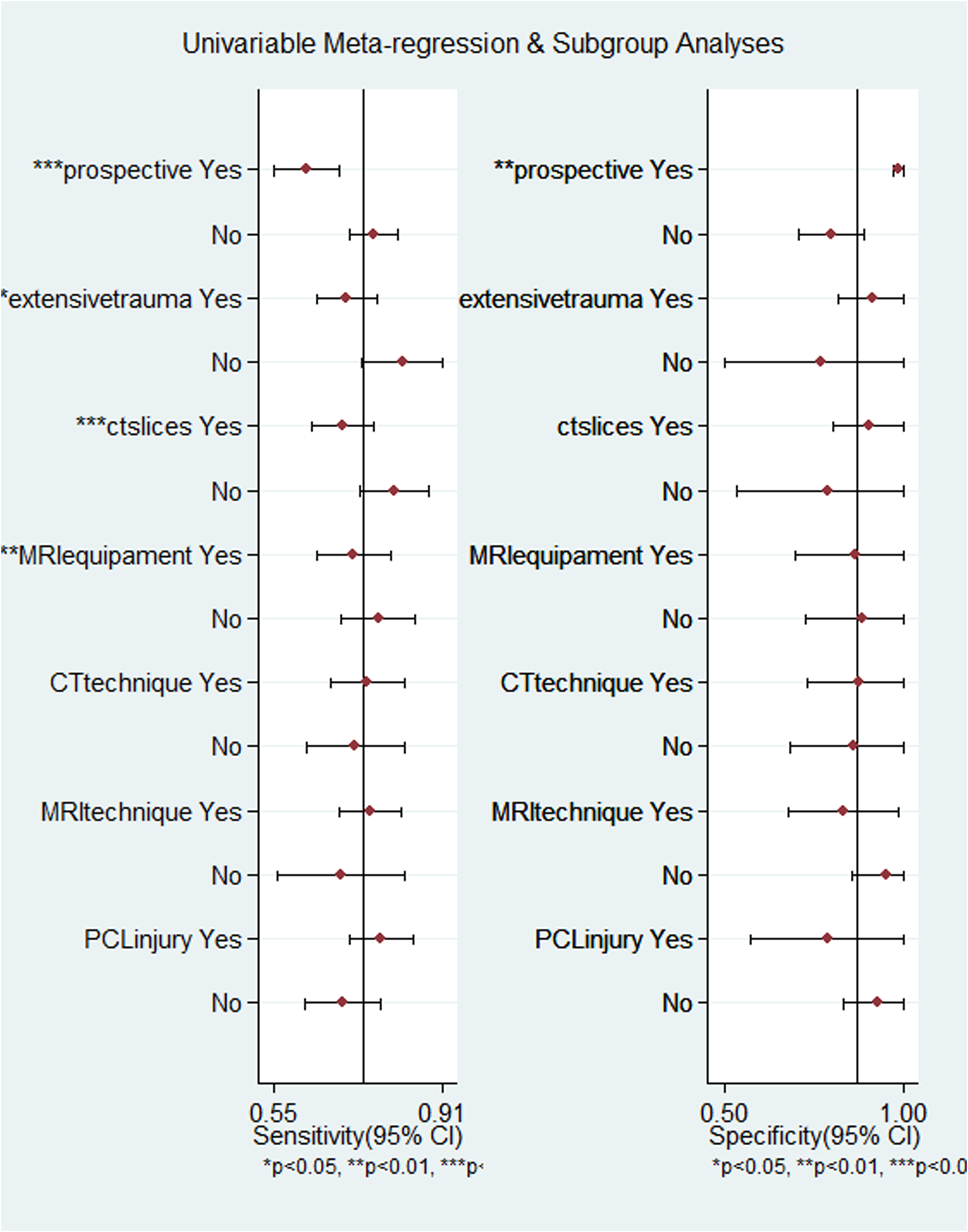
The Deeks’ Funnel Plot analysis (Figure 6) yields a significant (P = 0.01) deviation from symmetry. The presence of asymmetry, indicated by the non-random distribution of studies around the regression line, suggests potential publication bias Deeks’ funnel plot asymmetry test.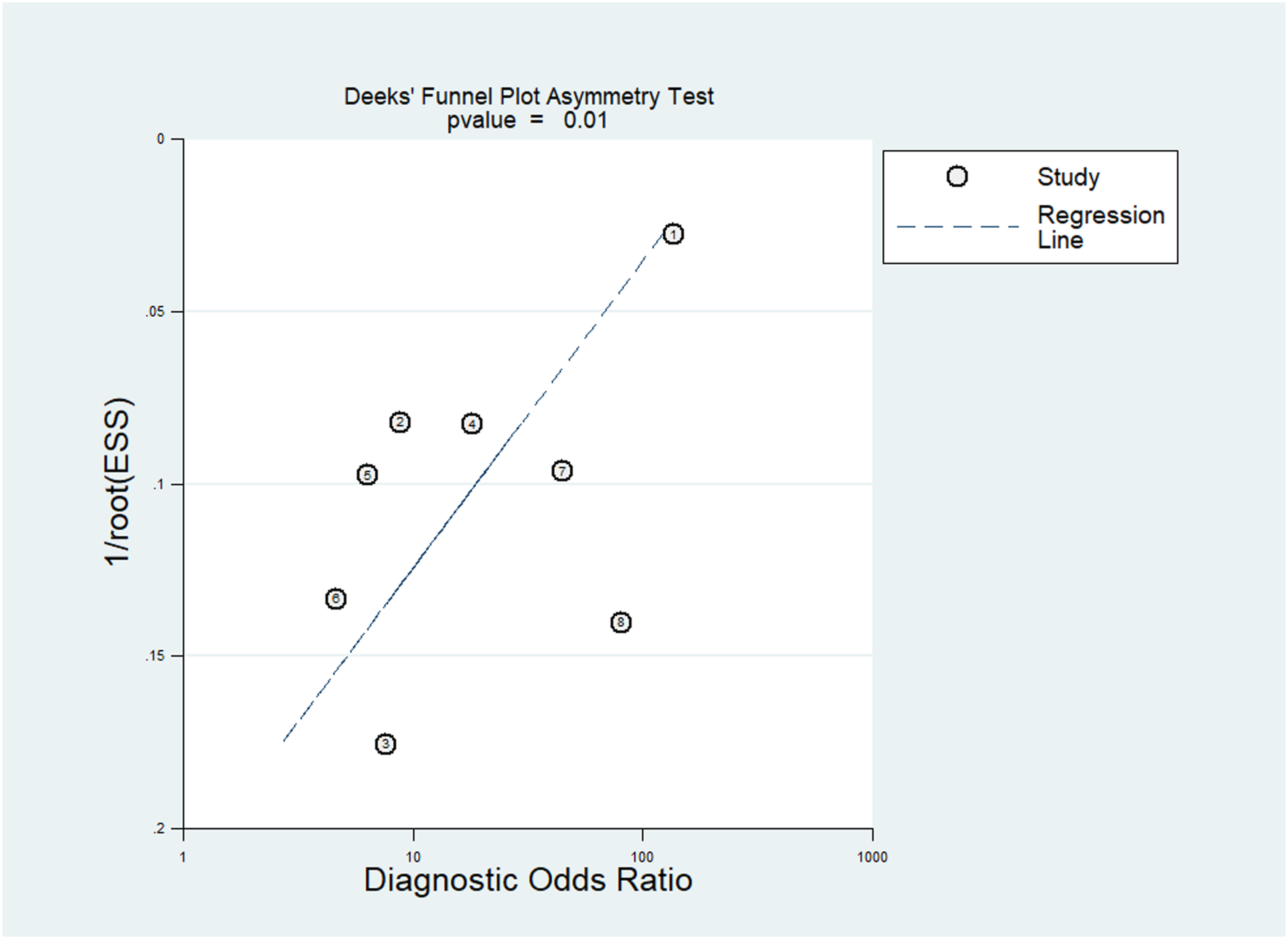
Our study on detecting PLC injuries using CT in thoracolumbar fractures reveals fair diagnostic accuracy, as evidenced by the bivariate boxplot analysis (Figure 7). Notably, the absence of significant outliers implies minimal heterogeneity among the studies, reinforcing the overall confidence in CT’s diagnostic capability. The influence analysis (Figure S4, Supplementary Material) demonstrates a well-fitting model with bivariate normality, minimal outliers, and some influential studies, indicating fair diagnostic accuracy for detecting PLC injuries using CT in thoracolumbar fractures. Bivariate boxplot.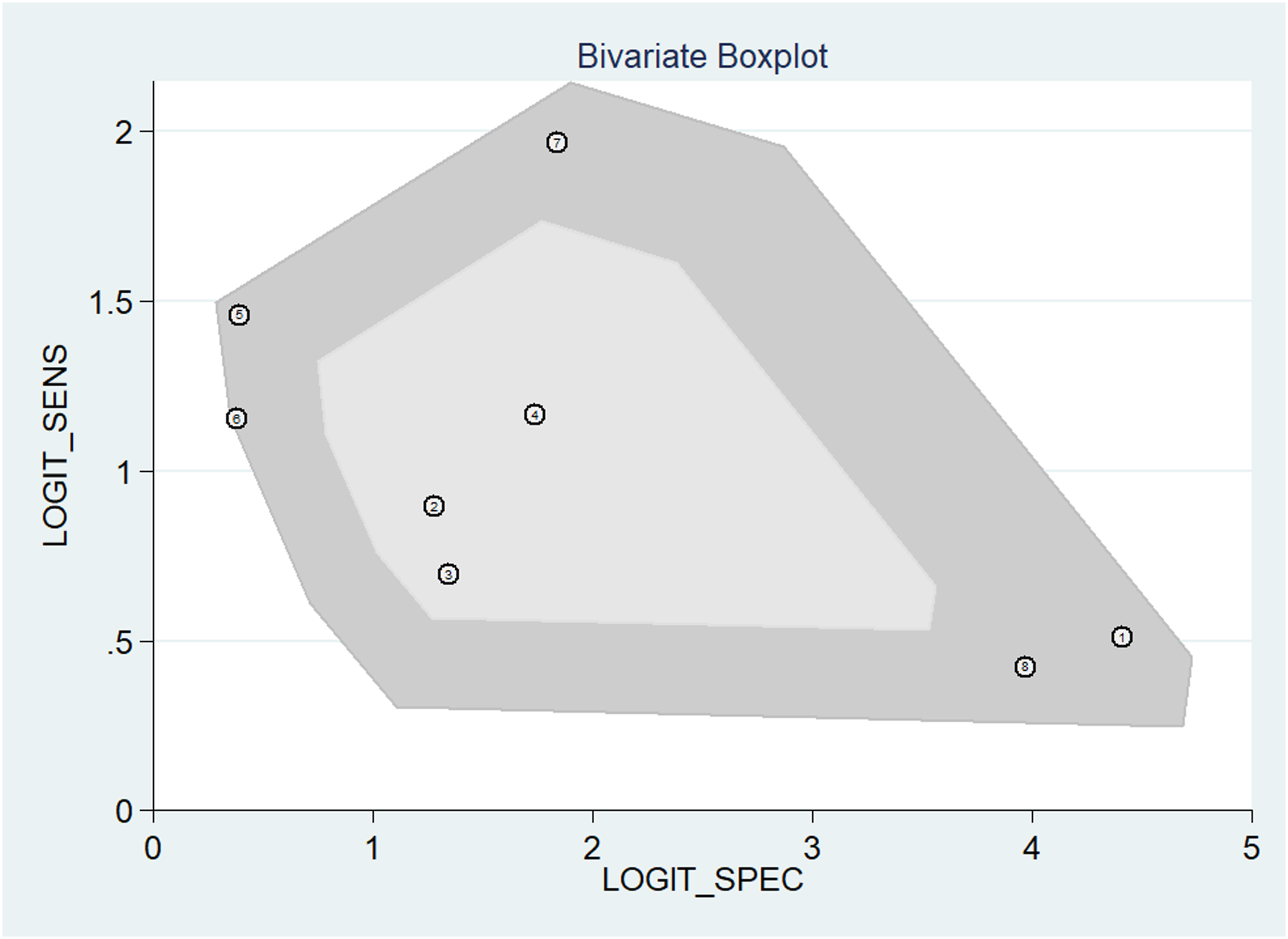
Discussion
We analyzed data from a total of 1440 patients across eight studies to evaluate the accuracy of CT in diagnosing PLC injuries in thoracolumbar fractures. CT had a pooled sensitivity of 75% (95% CI: 68 to 80, P = 0.00), specificity of 87% (95% CI: 71 to 95, P = 0.00), and DOR of 20 (95% CI 9 to 46). The AUC from the SROC analysis was 0.81 (95% CI: 0.78 to 0.84), suggesting effective overall diagnostic capability. The PLC plays a key role in stabilizing the spine, particularly the thoracolumbar spine. PLC damage directly affects the stability of the spine and requires accurate diagnosis to be effectively treated. MRI is considered the gold standard in PLC injury diagnosis due to its sensitivity. However, MRI’s long acquisition time is a significant drawback, particularly in emergencies, as it may delay critical decision-making. For instance, in acute situations where there is a need for quick evaluation, the time taken by MRI can hinder urgent treatment decisions, and therefore, other imaging techniques, such as CT scans, are also used.15,18
MRI’s high cost limits its routine use in resource-constrained settings and contributes to overall healthcare expenses. 6 CT scans play a crucial role in diagnosing PLC injuries in the thoracolumbar spine, especially in low-resource settings where access to advanced imaging modalities like MRI may be limited. CT scans provide reliable indirect measures of PLC disruption, such as interspinous distance widening, facet joint widening, and vertebral subluxation or dislocation.19,20 These features are essential for assessing the stability of the spine and determining the need for surgical intervention.
CT plays a critical role in the classification and operative planning of thoracolumbar fractures. Evidence has shown that CT enhances fracture classification accuracy more than plain radiographs. For instance, spine surgeons would correctly classify 43.4% of fractures from radiographs alone but increase this by 18.2% with the addition of CT scans.3,21 CT is particularly beneficial in identifying AO type B fractures, which are often missed in radiographs alone.3,21 The similarity between radiographs and CT is good for A-type fractures and poor for B-type, but maximal for CT and MRI, indicating CT’s central role in correct fracture classification.3,21
CT is also instrumental in identifying clinically significant thoracolumbar fractures, meaning those fractures that require operative fixation, bracing, or spine rehabilitation. CT scanning of the chest, abdomen, and pelvis (CTCAP) has been demonstrated to be sufficient to identify these significant fractures, with no clinical benefit of thoracolumbar reformatted imaging on outcome.22,23 CT reformats can, nevertheless, minimize missed injury at the expense of increased hospital stay and resource utilization.22,24 Studies have demonstrated that certain CT findings, such as vertebral translation, facet joint malalignment (FJM), and interspinous widening, are significant predictors of PLC injury. 25 The occurrence of multiple CT features can be utilized to enhance diagnostic precision, with two or more positive features significantly increasing the likelihood of PLC injury. 26 However, a single CT feature typically lacks predictive utility, and further confirmation by MRI is necessary. 26
The reliability of CT in PLC injury diagnosis is generally acceptable, with evidence suggesting that CT can accurately diagnose PLC injury in most cases, especially type B or C injuries, according to the AOSpine classification. 27 Rajasekaran et al 15 and Aly et al 10 indicate that MRI may only modestly increase the sensitivity for certain fracture subtypes, such as B2 injuries, but does not significantly alter the need for surgical intervention or the overall classification in most cases. However, it is important to note that the diagnosis of ligamentous injury can shift the classification from Type A to Type B, underscoring the relevance of accurate CT-based evaluation of ligamentous status. Therefore, CT remains a critical tool in the initial assessment and classification of thoracolumbar fractures, especially for AO Type B and severe Type A injuries. There is considerable interobserver variability in CT-based grading, suggesting that MRI must be used to verify PLC injury in doubtful cases. 29 This heterogeneity is emphasized by the necessity for standardized imaging protocols to increase the consistency of PLC assessments. 30 For instance, in one study, MRI was found to have good diagnostic performance for PLC injuries, with very good interobserver agreement, particularly for the interspinous ligament. 31 However, another study reported lower sensitivity and specificity than in earlier studies, suggesting that MRI appearance cannot be an exclusive basis for clinical decision-making.32,33 This inconsistency in the accuracy of MRI is evidence of its value in additional diagnostic approaches.
Clinical decision-making can be greatly impacted by CT findings. While CT is extremely good at diagnosing PLC injuries in low lumbar fractures, addition of MRI does not appreciably change fracture classification or clinical decisions and suggests minimal additional MRI value in certain cases. 28 Yet, CT parameters such as local kyphosis and canal compromise can detect MRI findings, mandating additional MRI evaluation in neurologically intact patients. 18 The combination of CT and MRI results may increase diagnostic accuracy and reliability. A proposal for an imaging algorithm suggests the use of both modalities to assess PLC injuries, leveraging each modality’s strengths to provide a comprehensive evaluation. 30 This method seeks to standardize the diagnostic procedure and minimize variations in assessment results. 30
There are a few limitations of this systematic review and meta-analysis that should be stated. While the study provides valuable data on the diagnostic accuracy of CT for detecting PLC injuries in thoracolumbar fractures, its findings are affected by heterogeneity in PLC injury evaluations in CT and MRI images, differences in study design, variations in imaging protocols, disparities in equipment specifications (eg, 1.5T vs 3T MRI), and inconsistencies in the criteria used to define PLC injury across studies. Despite high heterogeneity, sophisticated statistical methods and sensitivity analyses gave assurance of the reliability of CT diagnostic accuracy for PLC injury. It also describes considerable interobserver variability in CT-based measurements, with the implication that there could be variability in the way PLC injuries are graded between studies. In addition, comments that although CT has reasonable reliability for the diagnosis of PLC injuries, particularly in more complex fracture patterns, its soft tissue visualization is less than MRI, and MRI confirmation is still required in doubtful cases. Future studies should aim to standardize imaging protocols and definitions of PLC injuries, establish uniform diagnostic criteria, and improve interobserver agreement, ensuring more consistent and reliable assessments of PLC injuries across different clinical settings.
Conclusion
This meta-analysis demonstrates fair diagnostic accuracy of CT for diagnosing posterior PLC injuries in traumatic thoracolumbar fractures. Statistically fair sensitivity, specificity, and AUC confirm that CT is an effective imaging method for the diagnosis of these injuries. The Fagan nomogram analysis also supports its clinical utility, with a significant rise in post-test probability when PLC injury is suspected. These findings support the role of CT as a valuable diagnostic tool, facilitating early and accurate assessment of trauma-related PLC injuries. Given its solid performance, more research into CT-based evaluation is warranted, exploring the integration of new imaging technologies and artificial intelligence software to further enhance diagnostic precision. The expansion of comparative studies with MRI and delineation of the place of CT in different clinical contexts will result in improved imaging plans for PLC injury detection.
Supplemental Material
Supplemental Material - Accuracy of CT Scan for Detecting Posterior Ligamentous Complex Injury in Traumatic Thoracolumbar Fractures: A Systematic Review and Meta-Analysis
Supplemental Material for Accuracy of CT Scan for Detecting Posterior Ligamentous Complex Injury in Traumatic Thoracolumbar Fractures: A Systematic Review and Meta-Analysis by Luciano Falcão, Victor Arthur Ohannesian, Philippe Quadros Monteiro, Rafael Andrade Sampaio Silva, Isabelle Rodrigues Menezes, Ricardo Fonseca Oliveira Suruagy Motta, Kenzo Ogasawara Donato, André Nishizima, Andrei Fernandes Joaquim, and Danilo Gomes Quadros in Global Spine Journal.
Footnotes
Author Contributions
Luciano Falcão - Conceptualization, validation, writing - original draft, writing - review & editing, Supervision, Project administration; Victor Arthur Ohannesian - Methodology, Software, formal analysis, visualization; Philippe Quadros Monteiro - Investigation, data curation; Rafael Andrade Sampaio Silva - Investigation, data curation; Isabelle Rodrigues Menezes - Investigation, data curation, visualization; Ricardo Fonseca Oliveira Suruagy Motta - Validation; Kenzo Ogasawara Donato - Writing - original draft; André Nishizima - Writing - review & editing, Visualization; Andrei Fernandes Joaquim - Writing - review & editing; Danilo Gomes Quadros - Writing - review & editing, Supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.