
Abstract
Study Design
Retrospective cohort study.
Objective
Reciprocal changes (RCs) in unfused spinal segments can significantly affect the global alignment after corrective surgery. Identifying radiographic thresholds for guiding surgical strategies is critical for optimizing the outcomes.
Materials and Methods
Ninety-eight ASD patients who underwent staged surgeries, including lateral lumbar interbody fusion (LLIF) and posterior spinal fusion (PSF), were analyzed. According to the final follow-up image, the patients were classified into balanced (BG) and imbalanced (IG) groups, with IG further stratified into proximal junctional kyphosis/failure (IG-PJK/PJF) and non-PJK/PJF (IG-NPJK/PJF). Radiographic and clinical data were collected preoperatively, postoperatively, and at 2-year follow-up.
Results
The IG exhibited greater RCs in thoracic kyphosis (TK) and PI-LL mismatch from postoperative to follow-up than the BG (P = .030, P = .008). Significant predictors included Age >65.5 y/o (AUC: .672) and Post-PT >17.5° (AUC: .852) for imbalance and Post-TK >34.5° (AUC: .755) for IG-PJK/PJF. IG-PJK/PJF showed poorer ODI scores than BG and IG-NPJK/PJF (P = .021 and P = .022, respectively). IG-PJK/PJF showed poorer total SRS-22 scores than IG-NPJK/PJF (P = .021).
Conclusion
Increased RCs in TK was associated with adverse outcomes. Extending the upper instrumented vertebra (UIV) to the upper thoracic spine and addressing excessive TK (>34.5°) may improve alignment and reduce complications. Radiographic thresholds can provide actionable guidance in surgical planning.
Keywords
Introduction
Adult spinal deformity (ASD) encompasses a wide spectrum of spinal malalignment patterns, ranging from simple biplanar and segmental deformities to complex three-dimensional global deformities characterized by significant disruptions in coronal and sagittal alignment.1,2 In surgical management, spine deformity surgeons typically focus on correcting the most rigid and deformed portion of the curvature to preserve flexibility and facilitate more physiological motion in the non-fused spinal segments.3,4 However, the non-fused segments remain dynamic, permitting ongoing changes in spinal alignment postoperatively. These adaptive modifications in the unfused regions, commonly referred to as Reciprocal Changes (RCs), can serve as compensatory mechanisms to achieve optimal global spinal alignment.5-7 The potential for RCs and their clinical impact must be carefully considered, particularly in cases where significant deformity corrections are achieved with fusion levels terminating in the lower thoracic spine. Recognizing and accounting for RCs is critical for optimizing surgical outcomes and maintaining spinal balance in the long-term.
This study aimed to evaluate whether compensatory changes in the unfused thoracic spine after staged corrective surgery and long fusion extending from the lower thoracic spine to the pelvis have a favorable or unfavorable impact on global spinopelvic alignment. It hypothesizes that changes in the unfused thoracic spine will significantly influence sagittal alignment, which was analyzed using stratified patient groups.
Materials and Methods
Study Population
The study protocol was approved by the Institutional Review Board of the university hospital. Consecutive patients who underwent a week interval of two-stage corrective spinal fusion surgery for ASD at our institution over a 6-year interval between March 2017 and December 2023 were included in this study. ASD was defined as the presence of at least one of the following indicators: adult degenerative (de novo scoliosis) or degenerative kyphosis (degenerative kyphosis with scoliosis of a less than 10° Cobb angle) or adult idiopathic scoliosis (continuation of adolescent idiopathic scoliosis) or iatrogenic spinal deformity without instrumentation but with spinal curvature greater than 20° in the coronal plane, C7 sagittal vertical axis greater than 50 mm, pelvic tilt greater than 25°, and/or thoracic kyphosis greater than 60°.
The inclusion criteria were as follows: (1) age >20 years, (2) availability of a complete set of preoperative full-length standing radiographs, and (3) number of fused vertebrae totaling 6 or more segments. (4) Patients in whom distal fixation was achieved using S2-alar-iliac (S2AI) screws for pelvic stabilization. Standardized data collection forms were used to collect patient demographic variables including age, sex, body mass index (BMI), and etiology.
The exclusion criteria were as follows: (1) patients with neuromuscular disorders diagnosed preoperatively or postoperatively; (2) a history of infection or tumors affecting the pelvis or spine; (3) patients in whom distal fixation was achieved using iliac screws for pelvic stabilization; (4) patients whose proximal fixation was instrumented above T9; and (5) patients who underwent three-column osteotomy (3-CO). (6) Patients with less than 2 years of postoperative follow-up or those lost to follow-up within 2 years, resulting in incomplete imaging or clinical data, were excluded. Finally, 98 patients were included in the final analysis. The detailed data are presented in Figure 1. 286 patients were enrolled. 25 patients with less than 6 segments fusion; 28 patients with LIV was not ilium; 36 patients with incomplete imaging; 16 patients with spinal tumors or neuromuscular disorders; 30 patients with 3-CO; 53 patients with UIV above T9 were excluded. Finally, 98 patients were included.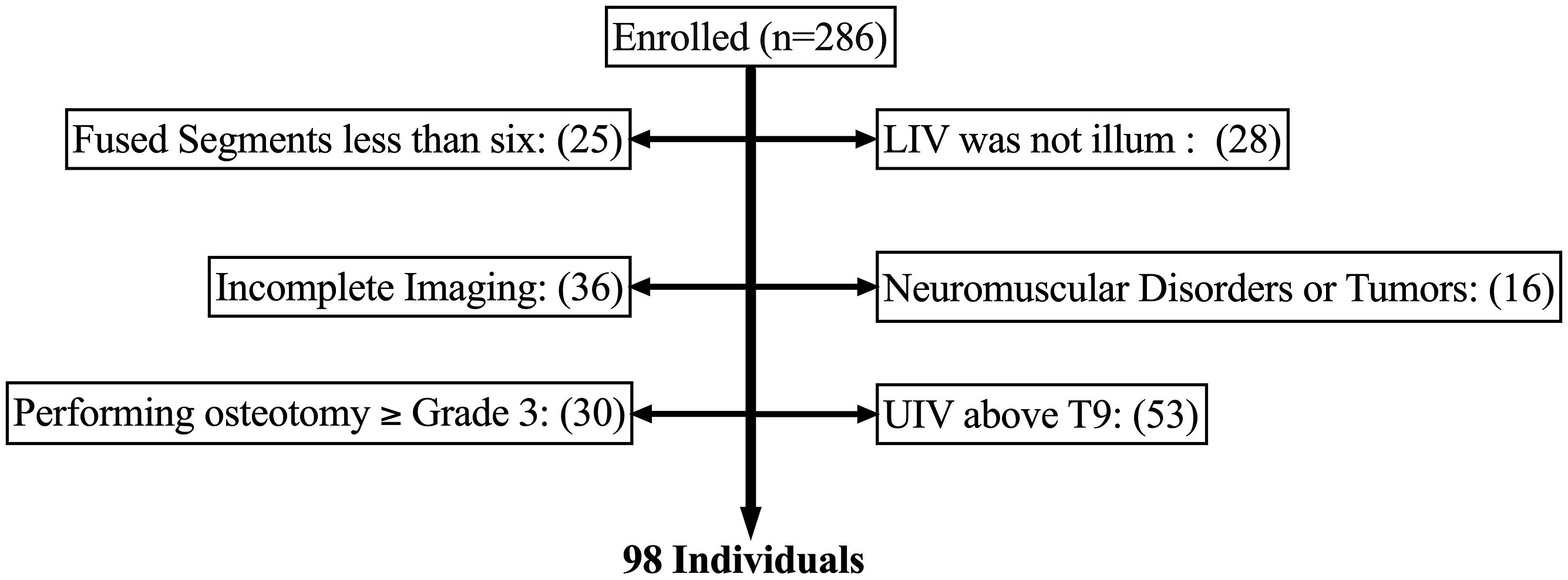
Surgical Procedure
All patients underwent staged spinal corrective fusion surgeries spaced one week apart. The first stage (1st) involved lateral position and multilevel lateral lumbar interbody fusion (LLIF) via an anterior approach from L1/2 to L5/S1. The second stage (2nd) was performed in the prone position and consisted of multilevel corrective osteotomy and posterior instrumented corrective fusion (PSF) surgery with a pedicle screw-based system from the lower thoracic spine to the pelvis. Spinal osteotomies were classified according to the Schwab spinal osteotomy classification as follows: grade 1, multiple facetectomies; grade 2, multiple posterior column osteotomies (PCO). The perioperative surgical data collected included estimated blood loss (EBL), operative time (OPT), surgical approach, number of instrumented vertebrae, and levels of lateral lumbar interbody fusion (LLIF). The detailed procedure is illustrated in Figure 2. Schema describing the correction in the two-stage surgery in ASD. (a) Preoperative to the 1st stage LLIF surgery (pre); (b) postoperative following the 1st stage LLIF surgery; (c) postoperative following the 2nd stage PCO/PSF surgery (post); LLIF, lateral lumbar interbody fusion; PCO, posterior column osteotomy; PSF, posterior spinal fusion.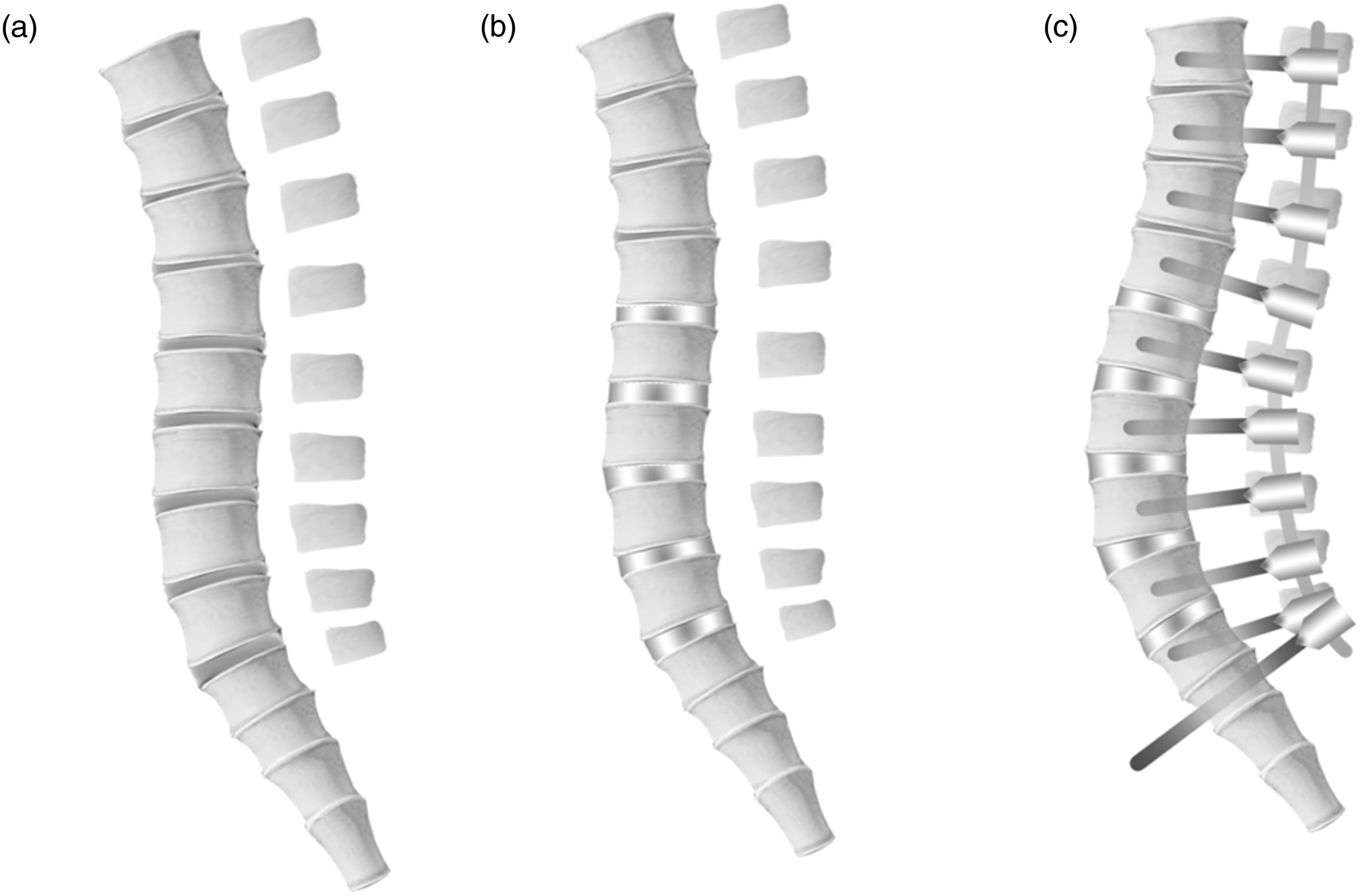
Radiographic Measurements
All radiographic measurements were performed using a Picture Archiving and Communications Systems (PACS) workstation by 2 experienced spine surgeons with double-blinded analysis. The following parameters were measured on full-length standing sagittal radiographs: T1 slope (T1S), thoracic kyphosis (TK), lumbar lordosis (LL), pelvic tilt (PT), sacral slope (SS), pelvic incidence (PI), PI minus LL mismatch (PI-LL), and C7 sagittal vertical axis (C7 SVA). The detailed radiographic measurements are shown in Figure 3. Illustration of measurements of spinal and pelvic parameters in sagittal radiograph, including (a) T1S, TK, LL, C7 SVA; (b) PI, PT, SS; T1S, T1 slope; TK, thoracic kyphosis; LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; C7 SVA, C7 sagittal vertical axis.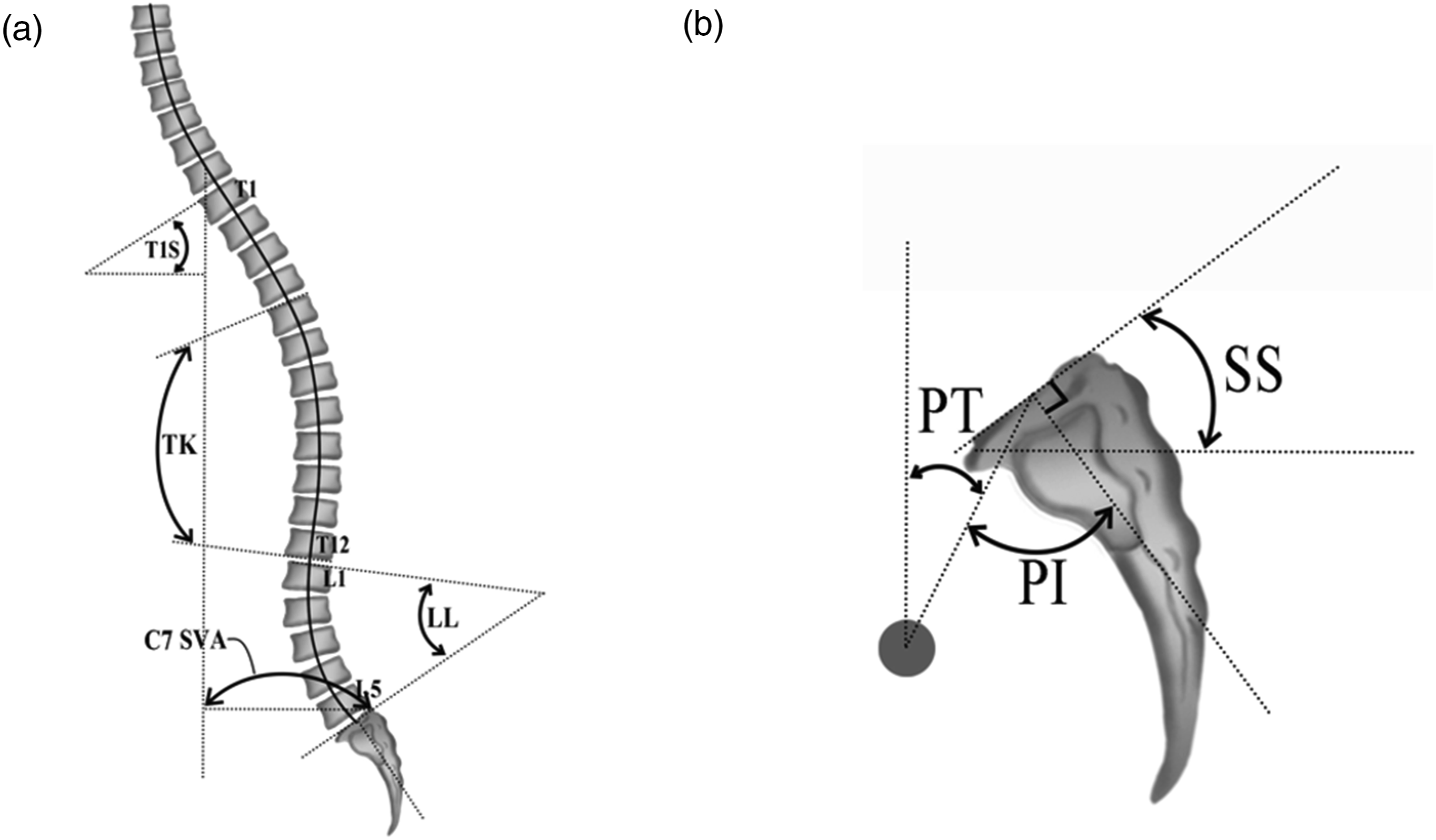
The measurement time points for all imaging parameters were as follows: preoperative to the 1st stage LLIF surgery (Pre), postoperative following the 2nd stage PCO/PSF surgery (Post), and the 2-year postoperative follow-up (F). Standardized radiographic parameter collection forms were used to record patient values at each preoperative, postoperative, and follow-up time point.
Based on the postoperative follow-up full-length standing spine sagittal radiographs obtained at 2 years (F), patients were classified into the balanced group (BG) or the imbalanced group (IG) depending on whether successful realignment was achieved, defined as a C7 sagittal vertical axis (C7 SVA) <50 mm and pelvic tilt (PT) <25°.
Furthermore, the cases within the imbalance group (IG) were further stratified into the PJK/PJF group (IG-PJK/PJF) and non-PJK/PJF groups (IG-NPJK/PJF) and analyzed based on the following definitions: (1) Proximal Junctional Kyphosis (PJK), defined as a ≥20° increase in kyphosis across the 2 vertebrae proximal to the upper instrumented vertebrae (UIV + 2 to UIV), 8 and (2) Proximal Junctional Failure (PJF), defined as fractures of the UIV or UIV + 1 or loosening of the UIV instrumentation. 9
Clinical Assessments
Quality of life was assessed during the preoperative assessment (Pre) and the 2-year postoperative follow-up visit (F) using the SRS-22 questionnaire and Oswestry Disability Index (ODI). Standardized questionnaire forms were used to record patient values at each preoperative (Pre) and 2-year follow-up time point (F).
Statistical Analysis
Categorical variables were expressed as case counts and compared between groups using the chi-square test. Continuous variables with normal distribution were expressed as mean ± standard deviation. Differences between the postoperative imbalance and non-imbalance groups and between the PJK/PJF and non-PJK/PJF subgroups within the non-imbalance group were analyzed using independent sample t-tests. For comparisons among the postoperative balanced group, imbalanced group with PJK/PJF, and imbalanced group without PJK/PJF, one-way analysis of variance (ANOVA) was performed for SRS-22 scores and Oswestry Disability Index (ODI).
Radiographic parameters with statistically significant differences were analyzed using binary logistic regression to identify preoperative and postoperative risk factors for sagittal imbalance, as well as risk factors for PJK/PJF within the imbalance group. Critical values were determined using receiver operating characteristic (ROC) curve analysis. Statistical significance was set at P ≤ .05.
Statistical analyses were conducted using IBM SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA), and forest plots and receiver operating characteristic (ROC) curves were generated using GraphPad Prism 10.
Results
Demographics, Operative Parameters of Balanced Group vs Imbalanced Group
Among the 98 patients included in this study, 89 were female (90.8%) and 9 were male (9.2%). Within the balanced group (BG), there were 11 females and two males, whereas in the imbalanced group (IG), there were 78 females and seven males, with no statistically significant difference between the groups (P = .411). The mean age was significantly different between the groups, at 62.2 ± 14.6 years for the BG and 69.9 ± 7.5 years for the IG (P = .004). The mean body height was 153.0 ± 7.8 cm in the BG and 150.3 ± 7.2 cm in the IG, while the mean body mass index (BMI) was 22.7 ± 4.0 kg/m2 for the BG and 23.1 ± 3.6 kg/m2 for the IG; both showed no statistically significant differences (P = .210 and P = .691, respectively). The preoperative T-score averaged −1.2 ± 1.4, the BG and −1.4 ± 1.0 in the IG, with no statistically significant difference between the groups (P = .481).
All 98 patients underwent a staged surgery. The mean operative time for the 1st lateral lumbar interbody fusion (LLIF) was 146.5 ± 41.9 min for the BG and 131.4 ± 30.0 min for the IG, while the second posterior column osteotomy/posterior spinal fusion (PCO/PSF) procedures averaged 296.5 ± 71.9 min for the BG and 305.8 ± 52.4 min for the IG, with no statistically significant differences between the groups (P = .115 and P = .571, respectively). The estimated blood loss (EBL) during the 1st stage was 58.8 ± 43.5 mL for the BG and 65.7 ± 95.4 mL for the IG, and during the 2nd stage, it was 795.5 ± 570.2 mL for the BG and 822.3 ± 476.4 mL for the IG, again showing no significant differences between the groups (P = .801 and P = .855, respectively).
Demographics, Operative Parameters of Balanced Group (BG), Imbalance Group (IG), and Imbalanced With PJK/PJF Group (IG-PJK/PJF).
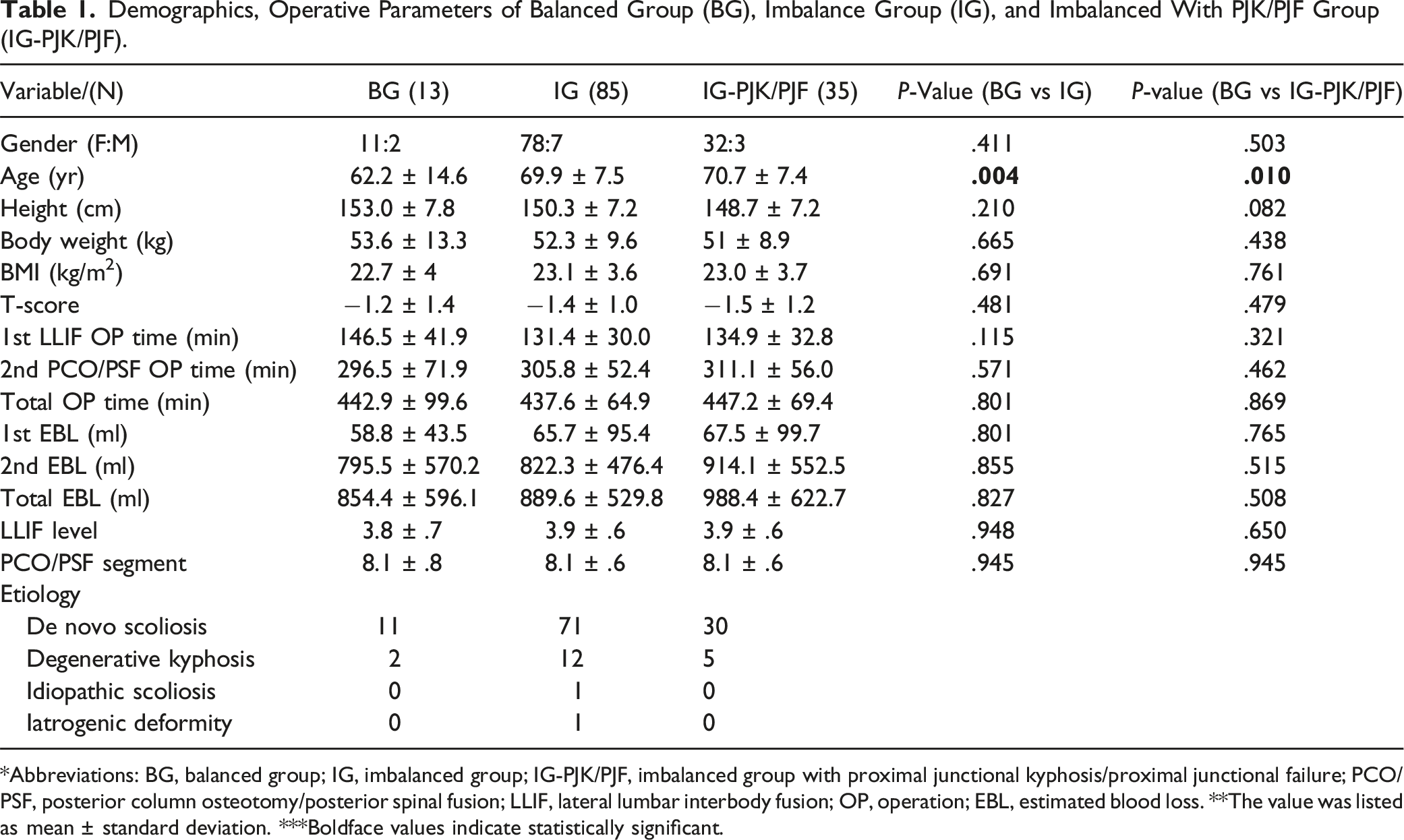
*Abbreviations: BG, balanced group; IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/proximal junctional failure; PCO/PSF, posterior column osteotomy/posterior spinal fusion; LLIF, lateral lumbar interbody fusion; OP, operation; EBL, estimated blood loss. **The value was listed as mean ± standard deviation. ***Boldface values indicate statistically significant.
Pre- to Postoperative and Final Radiographic Comparison of BG vs IG
The analysis of preoperative imaging parameter means demonstrated statistically significant differences between the balanced and imbalanced groups for Pre-PT and Pre-PI. The Pre-PT values were 28.5 ± 7.1 in the balanced group compared to 35.3 ± 11.1 in the imbalanced group (P = .037), while the Pre-PI values were 40.8 ± 13.5 and 53.1 ± 10.6, respectively (P = .001). These results suggest that the imbalanced group exhibited a greater angular tendency than the balanced group did.
Radiographic Comparison Between Preoperative (Pre), Postoperative (Post), and Two-Year Follow-Up (F).
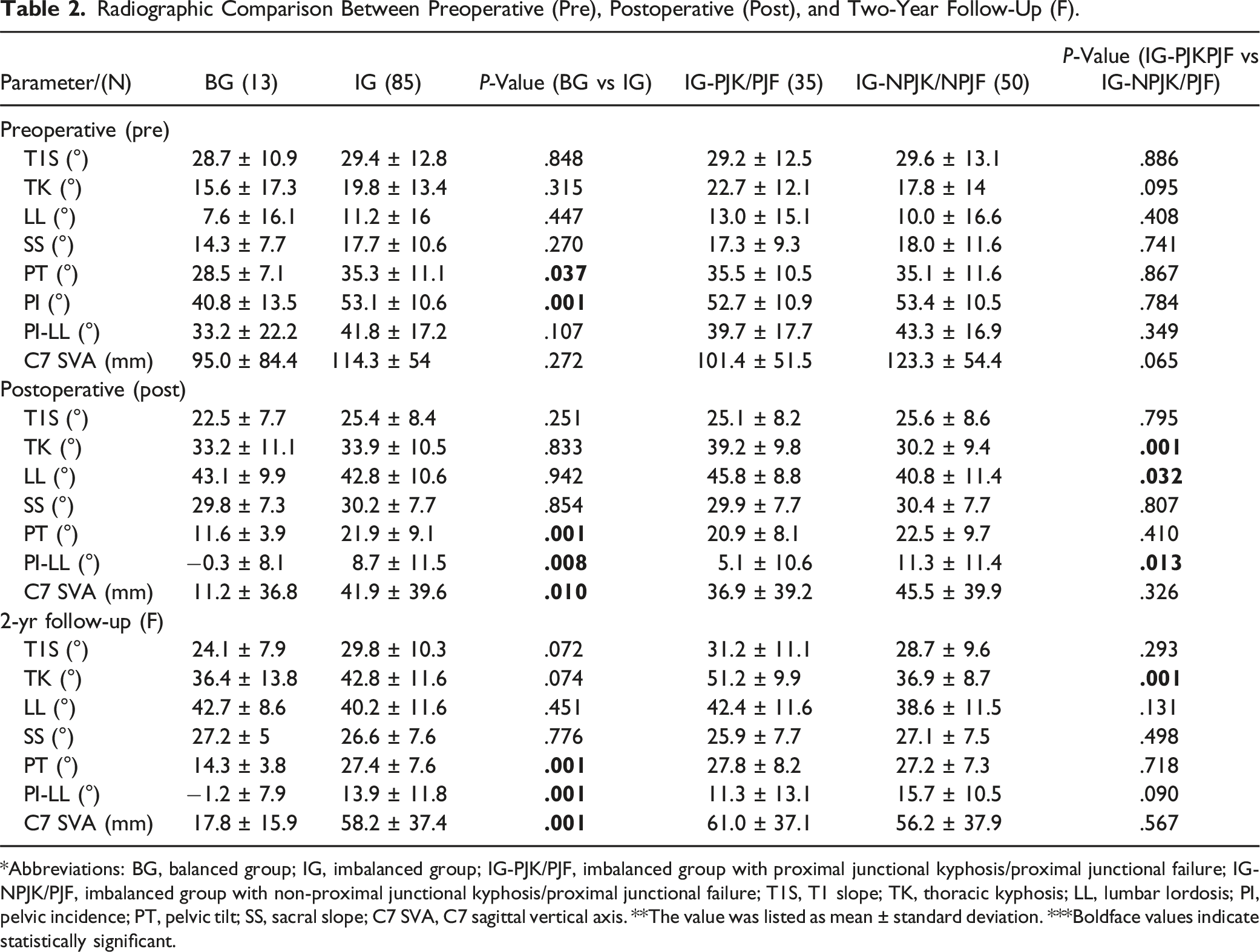
*Abbreviations: BG, balanced group; IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/proximal junctional failure; IG-NPJK/PJF, imbalanced group with non-proximal junctional kyphosis/proximal junctional failure; T1S, T1 slope; TK, thoracic kyphosis; LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; C7 SVA, C7 sagittal vertical axis. **The value was listed as mean ± standard deviation. ***Boldface values indicate statistically significant.
Pre- to Postoperative and Final Radiographic Comparison of IG-PJK/PJF vs IG-NPJK/PJF
In the imbalanced group, 35 patients (41.2%) were classified as PJK/PJF (IG-PJK/PJF), while 50 patients (58.8%) were classified as non-PJK/PJF (IG-NPJK/PJF). Preoperative imaging parameter comparisons between these subgroups showed no significant differences (P > .05). However, the postoperative imaging parameters demonstrated significant differences: Post-TK (IG-PJK/PJF: 39.2 ± 9.8 vs IG-NPJK/PJF: 30.2 ± 9.4; P = .001), Post-LL (IG-PJK/PJF: 45.8 ± 8.8 vs IG-NPJK/PJF: 40.8 ± 11.4; P = .032), and Post PI-LL (IG-PJK/PJF: 5.1 ± 10.6 vs IG-NPJK/PJF: 11.3 ± 11.4; P = .013). However, at the final follow-up, a statistically significant difference was observed only in the F-TK (IG-PJK/PJF: 51.2 ± 9.9 vs IG-NPJK/PJF: 36.9 ± 8.7, P = .001) between 2 groups. Detailed data are presented in Table 2.
Pre- to Postoperative and Final Reciprocal Changes Comparison of BG vs IG and IG-PJK/PJF vs IG-NPJK/PJF
In the comparison between the BG and IG groups, no statistically significant differences were observed in the changes in the imaging parameters between the preoperative and postoperative assessments (Post-Pre) (P > .05). However, significant differences were noted between the 2 groups in the changes from postoperative to 2-year follow-up (F-Post) in PI-LL (BG: −.8 ± 5.6 vs IG: 5.2 ± 7.6, P = .008) and TK values (BG: 3.2 ± 7.2 vs IG: 8.9 ± 9, P = .030). The imbalanced group exhibited greater angular changes in PI-LL and TK between the immediate postoperative period and final follow-up.
Reciprocal Changes Comparison Between Preoperative (Pre), Postoperative (Post), and Two-Year Follow-Up (F).
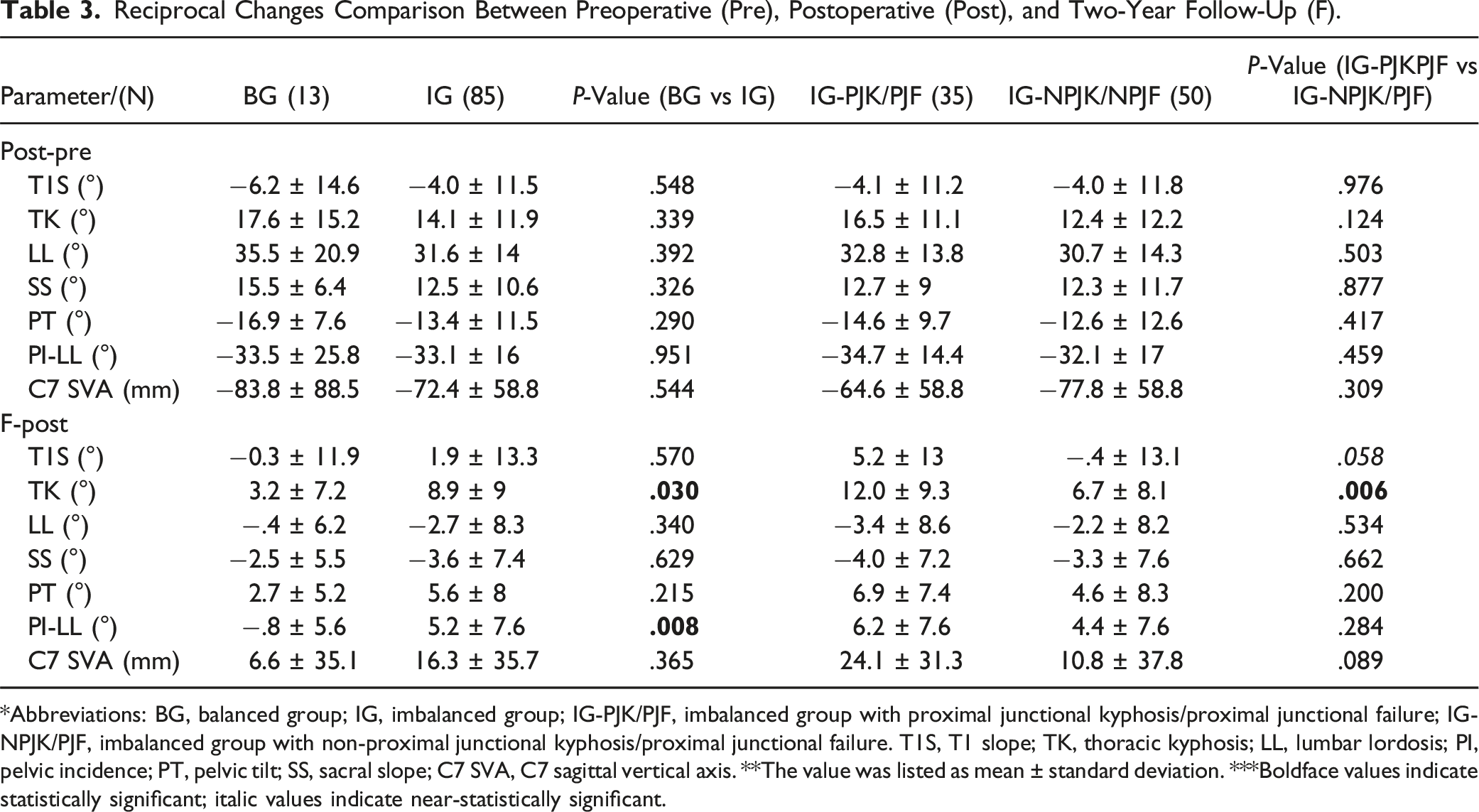
*Abbreviations: BG, balanced group; IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/proximal junctional failure; IG-NPJK/PJF, imbalanced group with non-proximal junctional kyphosis/proximal junctional failure. T1S, T1 slope; TK, thoracic kyphosis; LL, lumbar lordosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; C7 SVA, C7 sagittal vertical axis. **The value was listed as mean ± standard deviation. ***Boldface values indicate statistically significant; italic values indicate near-statistically significant.
Clinical Comparison Between BG vs IG-PJK/PJF vs IG-NPJK/PJF
According to the SRS-22 total scores at the final follow-up, there were no statistically significant differences between the BG and IG-NPJK/PJF groups (3.7 ± .7 vs 3.7 ± .7, P = .900). However, a statistically significant difference was observed in the self-image domain, with the BG group scoring higher than the IG-PJK/PJF group (3.6 ± .9 vs 2.9 ± .8, P = .008). Within the imbalanced group, the IG-PJK/PJF subgroup demonstrated significantly lower scores compared to the IG-NPJK/PJF subgroup in the self-image (2.9 ± .8 vs 3.6 ± .7, P = .001) and total domains (3.3 ± .8 vs 3.7 ± .7, P = .021), with a near-significant difference in the mental health domain (3.1 ± 1.1 vs 3.6 ± 1.0, P = .053).
Clinical Comparison Between Balanced Group (BG), Imbalance With Non-PJK/PJF Group (IG-NPJK/PJF), and Imbalanced With PJK/PJF Group (IG-PJK/PJF).
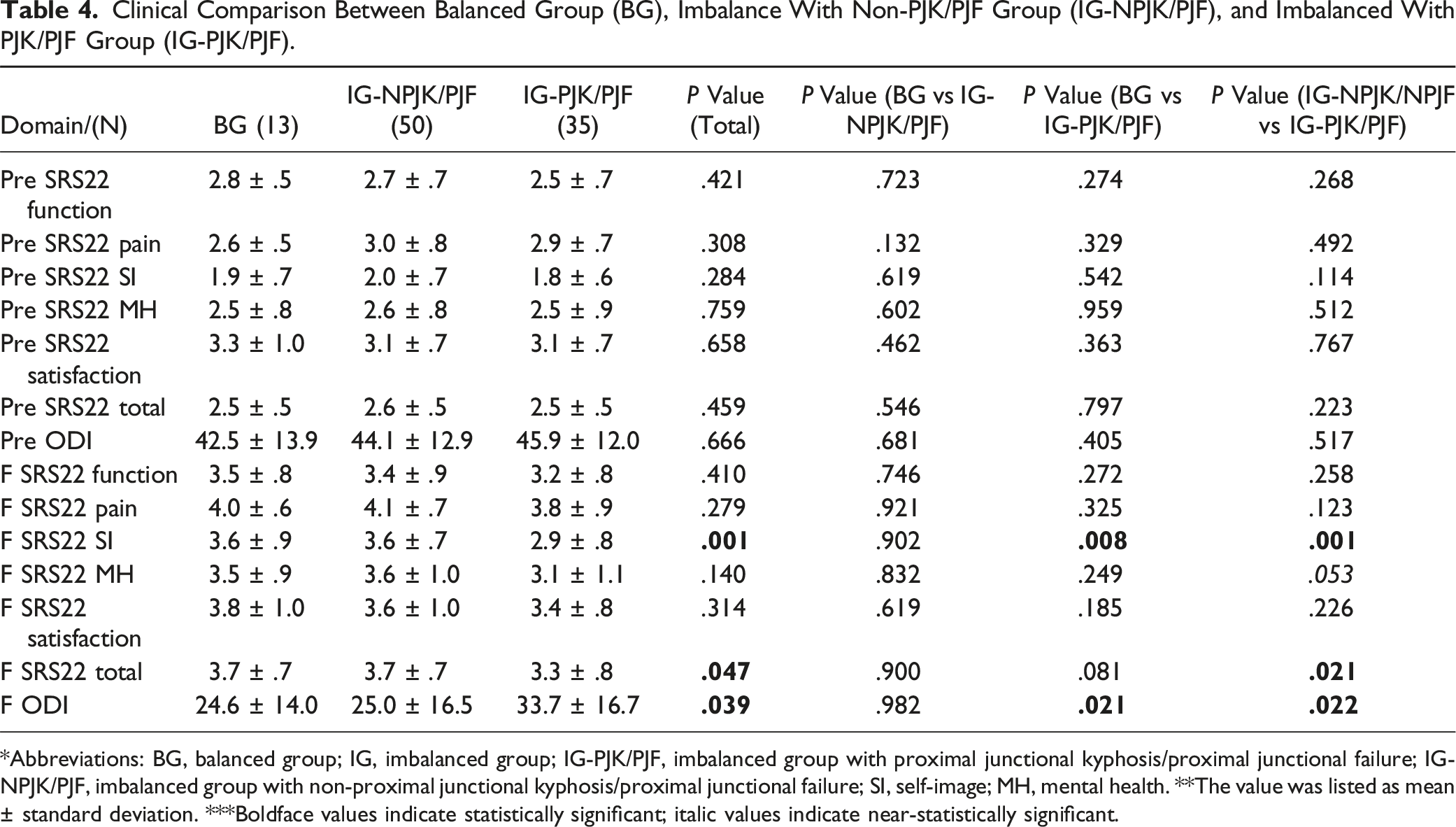
*Abbreviations: BG, balanced group; IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/proximal junctional failure; IG-NPJK/PJF, imbalanced group with non-proximal junctional kyphosis/proximal junctional failure; SI, self-image; MH, mental health. **The value was listed as mean ± standard deviation. ***Boldface values indicate statistically significant; italic values indicate near-statistically significant.
Discussion
Elderly patients with adult spinal deformity (ASD) often present with multiple comorbidities, and corrective fusion surgery for spinal deformities is frequently associated with various complications.10-12 In recent years, the development of lateral lumbar interbody fusion (LLIF) techniques has led to the proposal of staged correction strategies to reduce surgical risks and complications.13-15 However, despite these advancements, cases of correction imbalance and proximal junctional kyphosis/failure (PJK/PJF) remain observable during follow-up.16-18 Consequently, the study of staged correction strategies for ASD continues to be a topic of significant interest.19,20
This study aimed to explore whether compensatory changes in the unfused thoracic spine after staged corrective surgery and long fusions have a favorable or unfavorable impact on global spinopelvic alignment. However, the findings from this study revealed that the majority of compensatory changes led to poorer overall sagittal alignment, which could be attributed to changes that occurred through the unfused segments, such as F-Post TK and F-Post T1S. Over half—85 of 98 (86.7%)—of the unfused segments exhibited these unfavorable changes, whereas only 13 of 98 instances (13.3%) of changes led to improved global alignment.
The IG and IG-PJK/PJF group had a higher mean age than BG groups (69.9 ± 7.5 vs 62.2 ± 14.6 years, P = .004; 70.7 ± 7.4 vs 62.2 ± 14.6 years, P = .010). No differences were observed in other physiological parameters, surgical parameters, or bone mineral density. Kim et al 21 also identify age as a risk factor for sagittal decompensation after long fusion in ASD surgery. Hyun and Rhim, 22 identified that patients with postoperative TK progression were older than those with stable kyphosis. The etiology of imbalance and proximal junctional failure in older patients is likely to be multifactorial. As aging, the ability to compensate for positive sagittal alignment decreases. This may be partly due to muscular atrophy in the multifidus. In a series of 25 patients with iatrogenic kyphosis, Husson et al 23 found that half of them had evidence of fatty degeneration of the multifidus. Older patients may lack the muscular reserve needed to counteract flexion loading of the thoracic spine because of generalized age-related muscular weakness or muscle degeneration. Muscle mass and muscular strength have both been shown to progressively decline with age. 24
In our study, no statistically significant differences were observed in the preoperative TK and reciprocal changes (RCs) when comparing the preoperative and postoperative values (Post-Pre) within each group. However, there was a significant difference in reciprocal changes (RCs) when comparing postoperative and 2-year follow-up values (F-Post) within each group about the change in TK (3.2 ± 7.2° vs 8.9 ± 9°, P = .030; 12.0 ± 9.3° vs 6.7° ± 8.1°, P = .006). As significant differences were observed in the RCs of TK in the unfused segments among the groups from the postoperative period to the 2-year follow-up, we believe this warrants further investigation into its potential role in contributing to sagittal imbalance and development of proximal junctional kyphosis (PJK) or proximal junctional failure (PJF) at the 2-year follow-up.
The Impact of Reciprocal Changes in Thoracic Kyphosis (TK) for IG-PJK/PJF
According to the SRS-22 and ODI questionnaire, the IG-PJK/PJF group demonstrated poorer clinical outcomes than those of the BG and IG-NPJK/PJF groups. Therefore, in the IG-PJK/PJF group, certain radiographic RCs from the postoperative to the final follow-up period contributed to adverse clinical outcomes. According to our analysis, when comparing RCs at the final follow-up to the immediate postoperative period, the IG group showed consistently greater and positively correlated changes in thoracic kyphosis (TK) than the BG group, and IG-PJK/PJF demonstrated similar trends to IG-NPJK/PJF. Based on these findings, we conclude that during follow-up after staged corrective surgery for ASD, greater changes in reciprocal TK adjustments were associated with adverse clinical outcomes.25-28
Discriminative Value and Odds Ratio for IG and IG-PJK/PJF
Risk Factors for IG and IG-PJK/PJF Based on Logistic Regression and Receiver Operating Characteristic Curve.
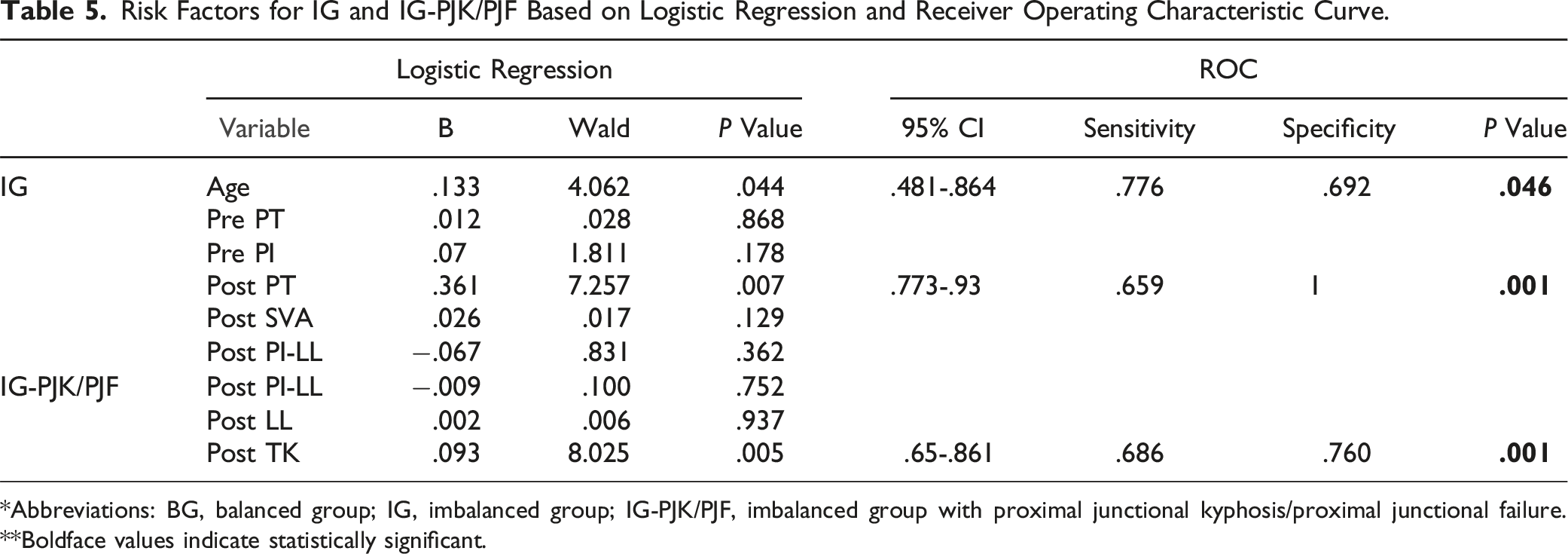
*Abbreviations: BG, balanced group; IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/proximal junctional failure. **Boldface values indicate statistically significant.
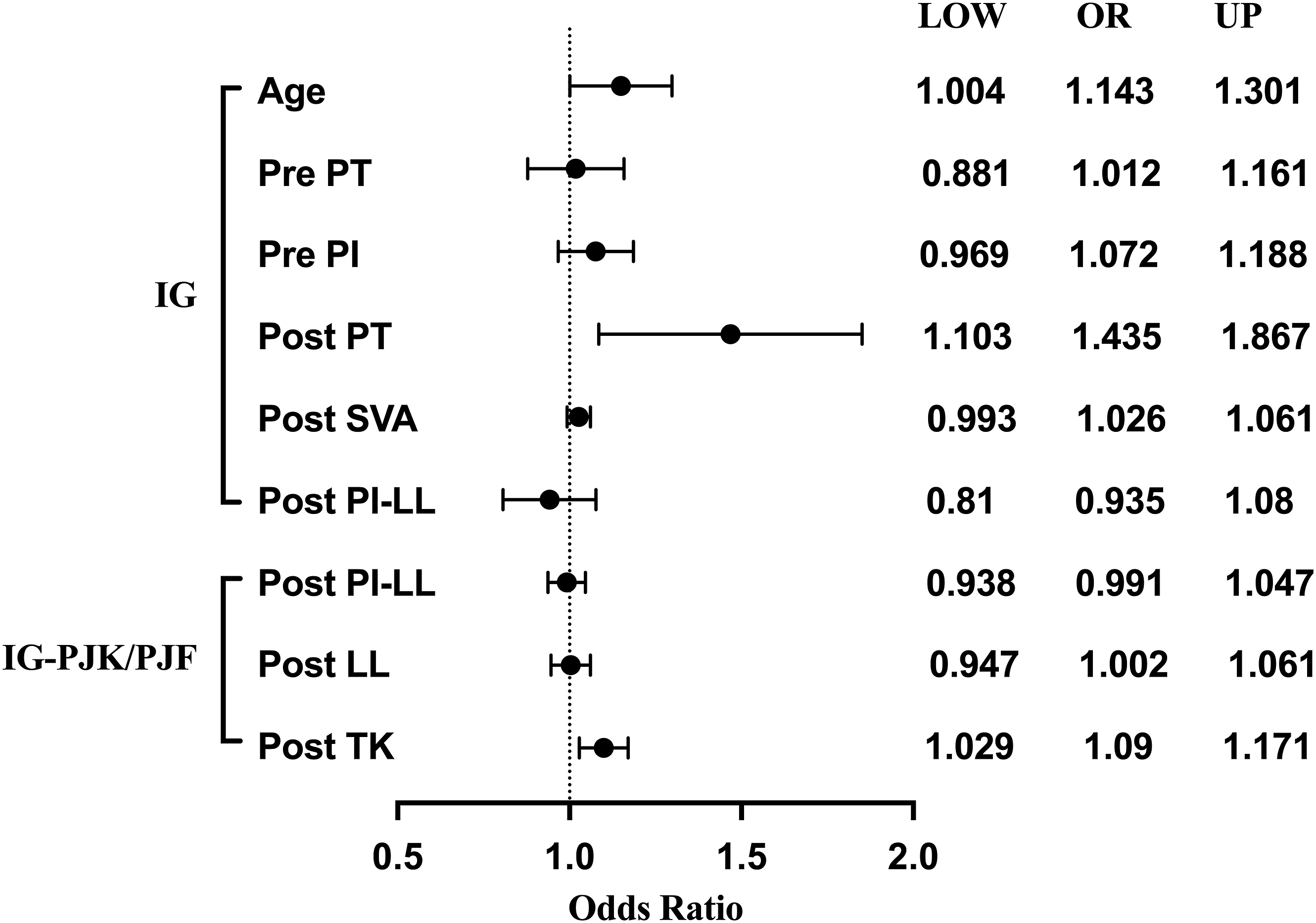
Forest plot of odds ratio for IG and IG-PJK/PJF based on logistic regression. (IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/failure).
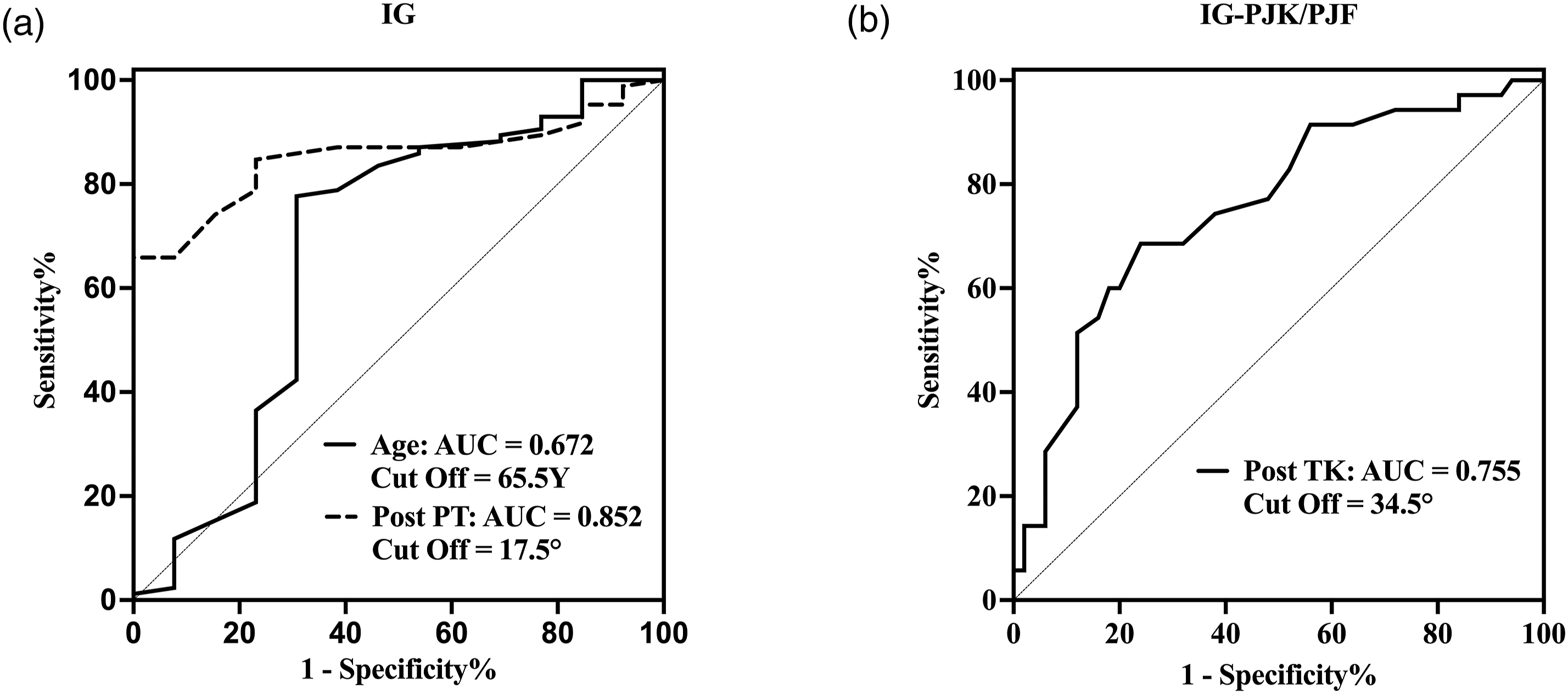
Preoperative and postoperative discriminative value for IG and IG-PJK/PJF based on receiver operating characteristic curve. (IG, imbalanced group; IG-PJK/PJF, imbalanced group with proximal junctional kyphosis/failure).
Correction of sagittal spinal deformity has been shown to significantly improve health related quality of life. Conversely, proximal junctional kyphosis has been shown to diminish global corrections and PJK is more prevalent in larger corrections.31-33 So a balance exists between performing the corrections necessary to attain good global alignment while avoiding the overcorrections that may predispose to the development of PJK. Therefore, careful preoperative planning of sagittal spinal deformity corrections may aid in the attainment of postoperative alignments within the optimal range for a given patient. One of the problems with developing an effective preoperative plan is the difficulty in predicting the postoperative response of preoperative compensatory mechanisms. Compensation through thoracic kyphosis reciprocal changes (TK RCs) have not been well investigated. 34
In the case of adult spinal deformity, some patient will decrease their thoracic kyphosis to compensate for the loss of lumbar lordosis.34,35 Diebo et al 34 found that patients with larger pelvic incidence/lumbar lordosis mismatches have less thoracic kyphosis, however, the magnitude of thoracic hypokyphotic compensation was not quantified in that study. Klineberg et al 36 demonstrated increased reciprocal thoracic kyphosis occurs after lumbar pedicle subtraction osteotomy (PSO) and this may diminish the global correction. Protopsaltis et al 37 were the first to quantify preoperative thoracic compensation through hypokyphosis as a primary contributing factor to the development of postoperative reciprocal thoracic kyphosis. These patients were also found to be at a higher risk of developing proximal junctional kyphosis. Previous studies25-28 have demonstrated a correlation between thoracic radiographic parameters and clinical outcomes after surgery for ASD. Our research on staged corrective surgery for ASD has revealed similar findings. Furthermore, this study identified clinically relevant radiographic thresholds based on the differences in clinical outcomes, thereby providing guidance for surgical planning. These thresholds aim to prevent adverse effects caused by reciprocal changes in unfused segments. The study by Lafage et al 6 demonstrated that the postoperative unfavorable RC group exhibited a greater change in thoracic kyphosis (TK), with a mean postoperative TK of 36 ± 13°.
The study by Protopsaltis et al 37 reported that the postoperative thoracic kyphosis (TK) in the Reciprocal Kyphosis group with proximal junctional kyphosis (PJK) was 47.2 ± 14.7°. The most previously published studies on this topic have focused on single-stage osteotomy correction procedures, rather than staged anterior-posterior correction surgeries. Single-stage osteotomy correction procedures commonly utilize three-column osteotomy (3-CO) techniques, which differ from the anterior release approach employed in the present study through anterior realignment surgery. This methodological difference may contribute to the variation in the TK cut-off values observed across studies. Another potential contributing factor is that our study population consisted of individuals from an Eastern cultural background, where daily activities frequently involve squatting or kneeling. This contrasts with Western cultural practices and lifestyle habits, which may, in part, account for the observed differences in cutoff values.
Although some scholars have proposed that prophylactic vertebroplasty at UIV + 1 or prolonged bracing may reduce the risk of proximal junctional kyphosis (PJK) or proximal junctional failure (PJF) following deformity corrective surgery with long fusion, the findings remain inconclusive. A study by Raman et al 38 indicated that while prophylactic vertebroplasty may minimize the risk of junctional failure during the early postoperative period, it does not appear to decrease the incidence of PJK at the 5-year follow-up. Similarly, a large systematic review by Rahmani et al 39 concluded that the evidence regarding whether prophylactic vertebroplasty reduces the incidence of PJK, proximal junctional fractures (PJFx), and PJF after spinal fusion remains inconclusive and conflicting. The study by Lord et al 40 demonstrated that postoperative orthoses had no significant impact on the incidence of proximal junctional kyphosis (PJK). Similarly, research conducted by Shahi et al 41 reported no difference in the rate of proximal junctional failure between patients who received postoperative bracing and those who did not. Given the lack of long-term evidence and ongoing controversy surrounding alternative interventions for the prevention of PJK/PJF, we advocate for a proactive approach in older patients. When postoperative thoracic kyphosis (TK) exceeds the discriminative threshold in adult spinal deformity staged corrective surgery, attention should be directed toward optimizing sagittal alignment distribution. In such cases, early revision surgery extending the upper instrumented vertebra (UIV) to the upper thoracic spine, combined with multiple-level thoracic posterior column osteotomies (PCOs) to reduce thoracic kyphosis, may be warranted. This strategy aims to prevent the development of PJK/PJF and the potential for subsequent irreversible neurological deficits.
Limitations
A limitation of this study is the small number of male participants, which may introduce gender-related bias in the analysis. Another limitation is that all patients underwent two-stage corrective procedures, precluding direct comparison with the effects of single-stage correction on reciprocal changes.
Conclusions
Significant postoperative alignment changes can occur in unfused thoracic spinal segments after staged corrective lumbar surgery. Risk factors for final follow-up imbalance include age >65.5 years-old, postoperative PT >17.5°, and increased RCs for TK >34.5°. Following staged corrective surgery for ASD, increased TK reciprocal changes (TK RCs) have been associated with PJK/PJF and adverse clinical outcomes. Therefore, in older patients, when postoperative TK exceeds the discriminative value, extending the UIV to the upper thoracic region and performing thoracic PCO to reduce TK should be considered to mitigate the risk associated with PJK/PJF.
Footnotes
Acknowledgments
The authors acknowledge the help of Professor Hsien-Te Chen’s supervision.
Author Contributions
X.-P. X., Y.-S. L. designed and performed experiments, Y.-S. L. developed this algorithm. X.-P. X. assisted in data analysis and figures, X.-P. X., Y.-S. L., and Y.-H. H. prepared the manuscript. All authors contributed to the manuscript and approved the submitted version. We declare that AI-assisted technologies were not used to generate scientific or interpreted data. AI technologies were only used to perform grammar checks on the completed manuscripts to improve linguistic accuracy under the supervision of all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
IRB Approval
Approval obtained from the Institutional Review Board at China Medical University Hospital (CMUH111-REC1-128).
Data Availability Statement
Data supporting the findings of this study are available upon request from Dr Yuan-Shun Lo.