
Abstract
Study Design
Human Cadaveric Biomechanical Study
Objectives
Lumbar Lateral Interbody Fusion (LLIF) utilizing a wide cage has been reported as having favorable biomechanical characteristics. We examine the biomechanical stability of unilateral pedicle screw and rod fixation after multilevel LLIF utilizing 26 mm wide cages compared to bilateral fixation.
Methods
Eight human cadaveric specimens of L1-L5 were included. Specimens were attached to a universal testing machine (MTS 30/G). Three-dimensional specimen range of motion (ROM) was recorded using an optical motion-tracking device. Specimens were tested in 3 conditions: 1) intact, 2) L1-L5 LLIF (4 levels) with unilateral rod, 3) L1-L5 LLIF with bilateral rods.
Results
From the intact condition, LLIF with unilateral rod decreased flexion-extension by 77%, lateral bending by 53%, and axial rotation by 26%. In LLIF with bilateral rods, flexion-extension decreased by 83%, lateral bending by 64%, and axial rotation by 34%. Comparing unilateral and bilateral fixation, LLIF with bilateral rods reduced ROM by a further 23% in flexion-extension, 25% in lateral bending, and 11% in axial rotation. The difference was statistically significant in flexion-extension and lateral bending (P < .005).
Conclusions
Considerable decreases in ROM were observed after multilevel (4-level) LLIF utilizing 26 mm cages supplemented with both unilateral and bilateral pedicle screws and rods. The addition of bilateral fixation provides a 10-25% additional decrease in ROM. These results can inform surgeons of the incremental biomechanical benefit when considering unilateral or bilateral posterior fixation after multilevel LLIF.
Keywords
Introduction
Lateral lumbar interbody fusion (LLIF) is a minimally invasive technique of lumbar arthrodesis with reported fusion rates as high as 97.9%. 1 The disc space can be accessed via a retroperitoneal trans-psoas or anterior-to-psoas approach.1-4 Both are usually performed with the patient in the lateral decubitus position to permit the approach, disc space preparation, and implantation of the interbody cage. Supplemental internal fixation is often combined with the interbody device to afford greater construct stability, with pedicle screws instrumentation being most commonly described.
Repositioning the patient to the prone position for placement of pedicle screws and rods can add considerable time spent in the operating room, with some authors reporting 44.4 minutes of increased operative time. 5 Risks during posterior pedicle screw fixation include potentially violating the adjacent facet joint and, in the case of percutaneous pedicle screws, guidewire migration through the anterior vertebral body cortex, potentially leading to vascular injury.6,7 Percutaneous pedicle screw fixation is associated with increased surgical site pain, morbidity, intraoperative bleeding, and operative time compared to stand-alone constructs. 8 So-called “single position surgery” has been described using robotics, intraoperative CT, or specialized bolsters for positioning and may carry a unique risk profile that has yet to be fully characterized.9-12
Previous biomechanical studies have highlighted the substantial stabilizing effect of extra-wide lateral interbody cages. Pimenta et al. reported that 26 mm LLIF cages without any supplemental fixation showed stability that exceeded transforaminal lumbar interbody fusion (TLIF) with bilateral pedicle screws and rods and 18 mm LLIF cages with unilateral screws and rods. 13 They attributed the stability to the preservation of the posterior tension band structures and enhanced loading of the apophyseal ring. However, their study was limited to single-level fusion. The biomechanical performance of 26 mm cages for multilevel fusion has not been well characterized.
The purpose of the current study was to evaluate the biomechanical stability of extra-wide 26 mm lateral cages in a multilevel fusion construct (L1-L5, 4 levels) in flexion-extension, lateral bending, and axial rotation with unilateral or bilateral pedicle screw and rod fixation. We hypothesized that, due to the stability conferred by 26 mm wide interbody cages, the unilateral rod construct would provide similar biomechanical stability as the bilateral rod construct.
Methods
Specimen Preparation
Eight fresh-frozen human cadaveric specimens of L1-L5 were included. A priori power analysis (alpha of .05, beta of .2, power of .80) showed a minimum sample size of 6 to 8 specimens, depending on the range of motion tested. Specimens were prepared by cleaning surrounding soft tissue and muscle, taking care to preserve the discs and spinal ligaments (supraspinous, interspinous, facet capsules, posterior longitudinal ligament, and anterior longitudinal ligament). The mean specimen age was 66.5 ± 11.5 years. There were 7 male and 1 female specimens. The average BMI was 31.1 ± 7.32 kg/m2. All specimens were visually inspected to confirm no fracture, deformity, previous surgery, or severe spondylosis. A CT scan (120 kV, 20 mA, .62 mm resolution, GE Brightspeed, Boston MA) was performed on all specimens to investigate the bone quality and to produce measurements to plan optimal implant size. For testing, the sacrum and T12 vertebra were embedded in a metal cup using fast-curing resin (Bondo, fiberglass, 3M) and positioned with the L3-L4 level horizontal. Specimens were kept moisturized and wrapped in plastic foil during the curing process until tested.
Instrumentation
Lateral interbody cages were implanted with the specimen in the lateral decubitus position utilizing the LLIF surgical technique and instrumentation specific to this technique (Extreme Lateral Interbody Fusion (XLIF), Nuvasive, San Diego, California). All interbody cages were 26 mm in width (anterior-posterior dimension) and polyetheretherketone (PEEK) material (CoRoent, Nuvasive, San Diego, California). The height (superior-inferior) and length (medial-lateral) of each implant was determined by CT scan and adjusted if necessary.
Pedicle screws (Armada, Nuvasive, San Diego, California) were placed with the specimen in the prone position. Screws were implanted bilaterally at every level from L1-L5 utilizing standard freehand technique with anatomic landmarks. Screw size was determined by CT scan and adjusted if necessary. Pilot holes were tapped and probed, in addition to visual inspection of the specimens, to detect any breach. Rods were 5.5 mm titanium and placed unilaterally or bilaterally. For the unilateral rod condition, the rod was placed on the left-sided screws.
Order of Testing
Specimens were tested in the following 3 conditions: 1) intact, 2) 26 mm lateral interbody cages with unilateral rod L1-L5 (LLIF + unilateral rod), 3) 26 mm lateral interbody cages with bilateral rods L1-L5 (LLIF + bilateral rods).
Biomechanical Testing
Specimens were attached to a universal testing machine (MTS 30/G) using specially designed holding jigs. Flexion, extension, and lateral bending were attained by applying a 200 N load at a rate of 2 mm/s to the loading arm connecting the cup containing the thoracic end of the spine while the cup with the sacral end was fixed to the base of the loading frame. Axial rotation of ± 8° of the specimen was achieved by coupling the thoracic end to a servo motor rotating at 2 deg/s with the sacral end fixed. A 50 N pre-load (follower load) was applied from L1 to L5. During all the tests, three-dimensional specimen motion from L1 to L5 was recorded using a motion-tracking device (Optotrak, Northern Digital Inc., Waterloo, Ontario, Canada).
Statistical Analysis
Range-of-motion measurements in flexion/extension, lateral bending, and axial rotation were measured at each segment (L1-L2, L2-L3, L3-L4, L4-L5) and combined. Descriptive statistics were reported as mean ± standard deviation degrees. Change in ROM after instrumentation was reported as percentage change from the intact specimen. Paired t-tests were used to compare ROM between instrumentation conditions. Statistical analyses were performed using Microsoft Excel Version 2013 with significance set at P < .05.
Results
Bone quality was determined by CT scan as previously described. 14 The mean Hounsfield unit (HU) was 143 ± 29.4 (range, 84 to 169.4). Only one specimen was below the suggested threshold for osteoporosis of less than 110 HU. 15
Lateral interbody cages were 26 mm in width and ranged from 8 to 14 mm. The most common heights were 10 mm (n = 13). Length ranged from 45 to 60 mm. The most common length was 55 mm (n = 14). Pedicle screw diameters ranged from 6.5 mm to 8.5 mm in diameter and 40 to 60 mm in length. The diameters of the screws implanted were 6.5 mm (n = 10), 7.5 mm (n = 45), and 8.5 mm (n = 25). The screw diameter was a mean 72.3 ± 14.4% (median, 70.2%) of the inner diameter of the pedicle as measured on CT scan.
Axial rotation was measured in all 8 specimens. Flexion/extension and lateral bending are presented for 7 of the specimens because of a change in methodology for acquiring these measurements.
Comparison with Intact Condition
Comparison of range-of-motion of intact spine specimens with specimens after lumbar lateral interbody fusion (LLIF) with unilateral or bilateral pedicle screw and rod fixation.
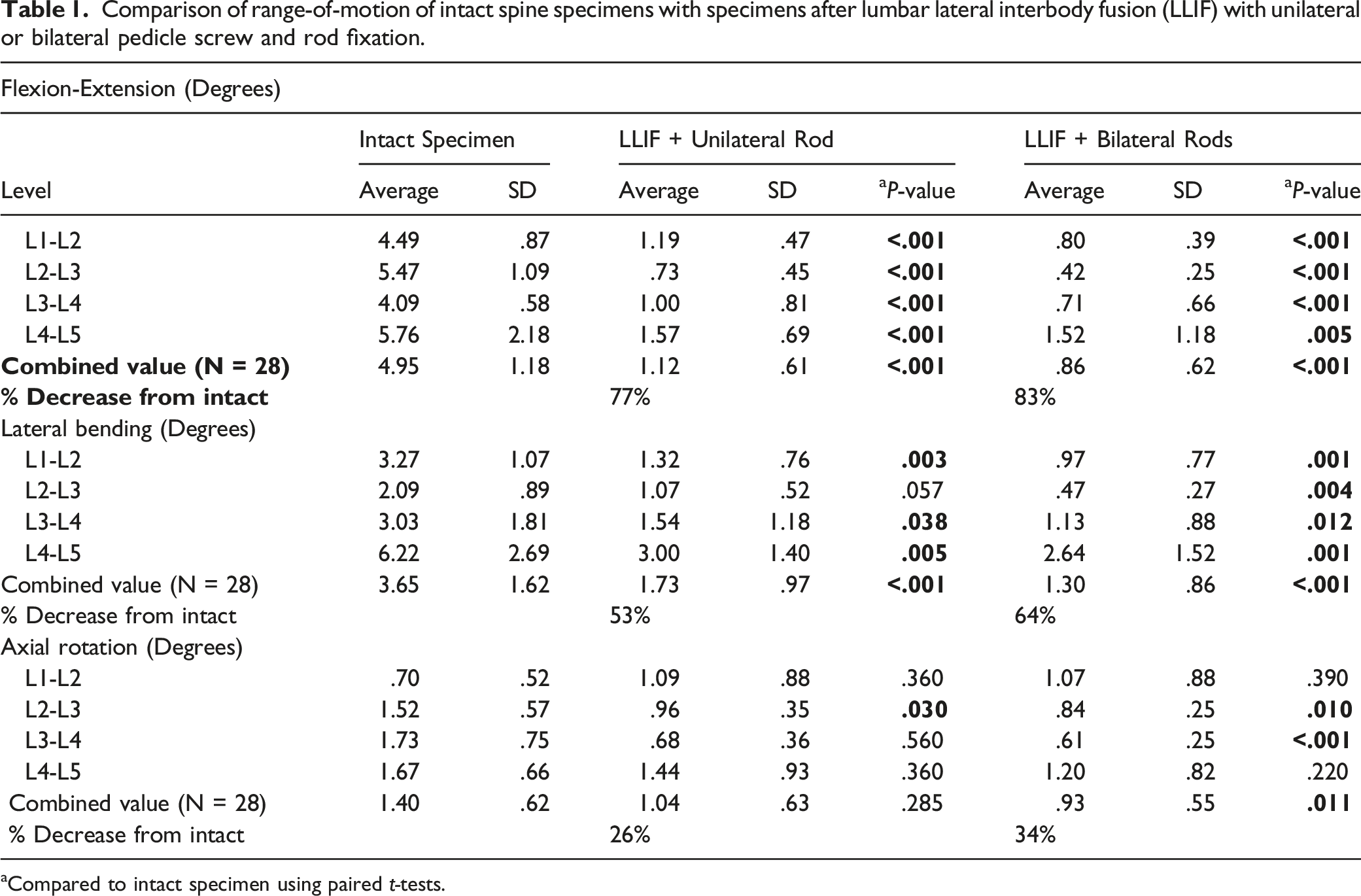
aCompared to intact specimen using paired t-tests.
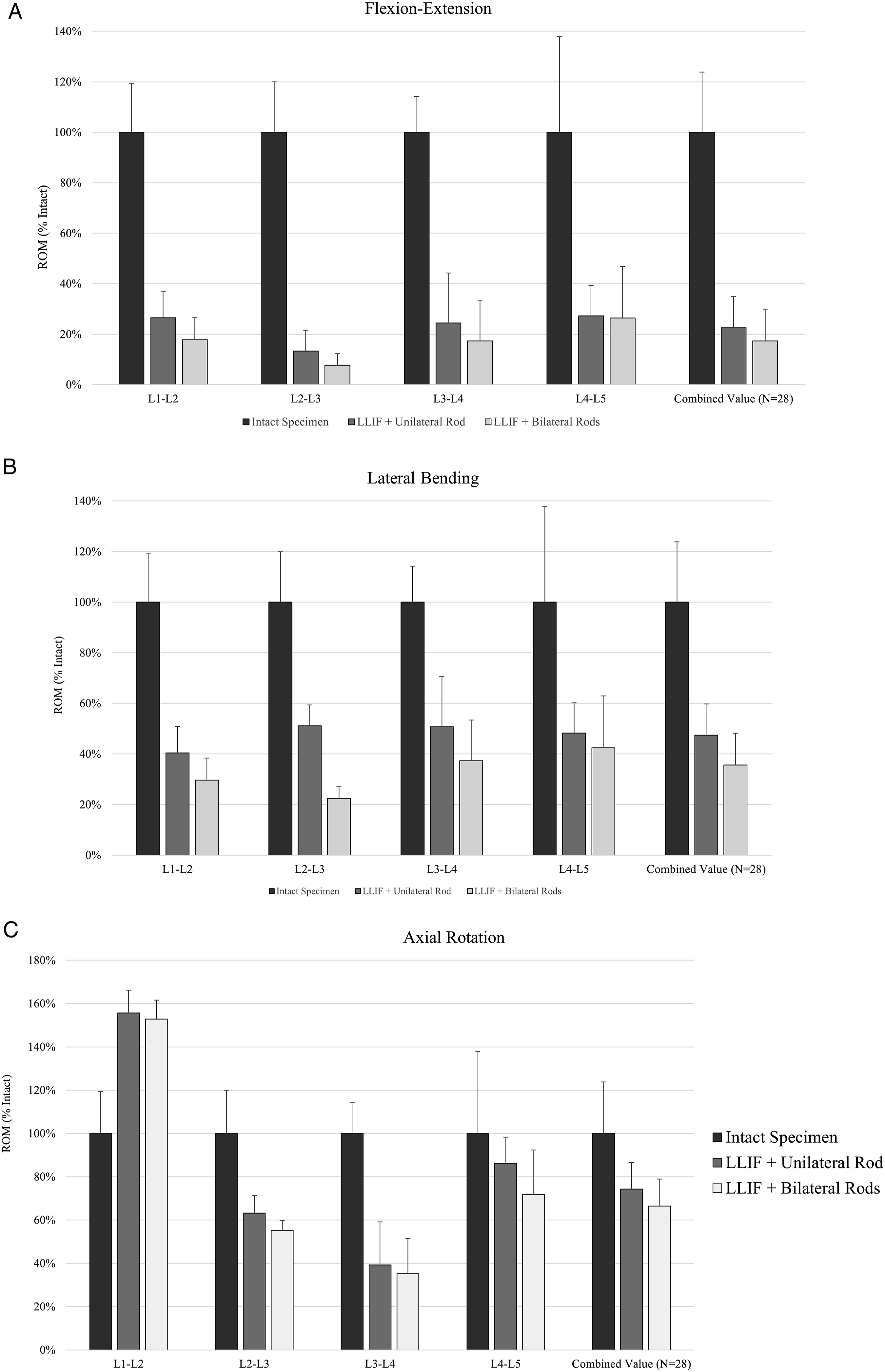
Bar graphs depicting the range-of-motion achieved by the intact spine specimen and specimens instrumented with lumbar lateral interbody (LLIF) cages with unilateral and bilateral pedicle screw and rod fixation. Range-of-motion was compared in A) flexion-extension, B) lateral bending, and C) axial rotation. Paired t-test: *P < .05, **P < .01, ***P < .001.
For axial rotation, the intact specimen mean ROM was 1.4° ± .62°. With LLIF + unilateral rod, axial rotation decreased 26% to 1.04° ± .63°. With LLIF + bilateral rods, axial rotation decreased 34% to .93° ± .55°. The difference was statistically significant only for LLIF + bilateral rods (P = .01).
Comparison between Unilateral and Bilateral Rods
Comparison of range-of-motion of specimens after lumbar lateral interbody fusion (LLIF) with unilateral or bilateral pedicle screw and rod fixation.
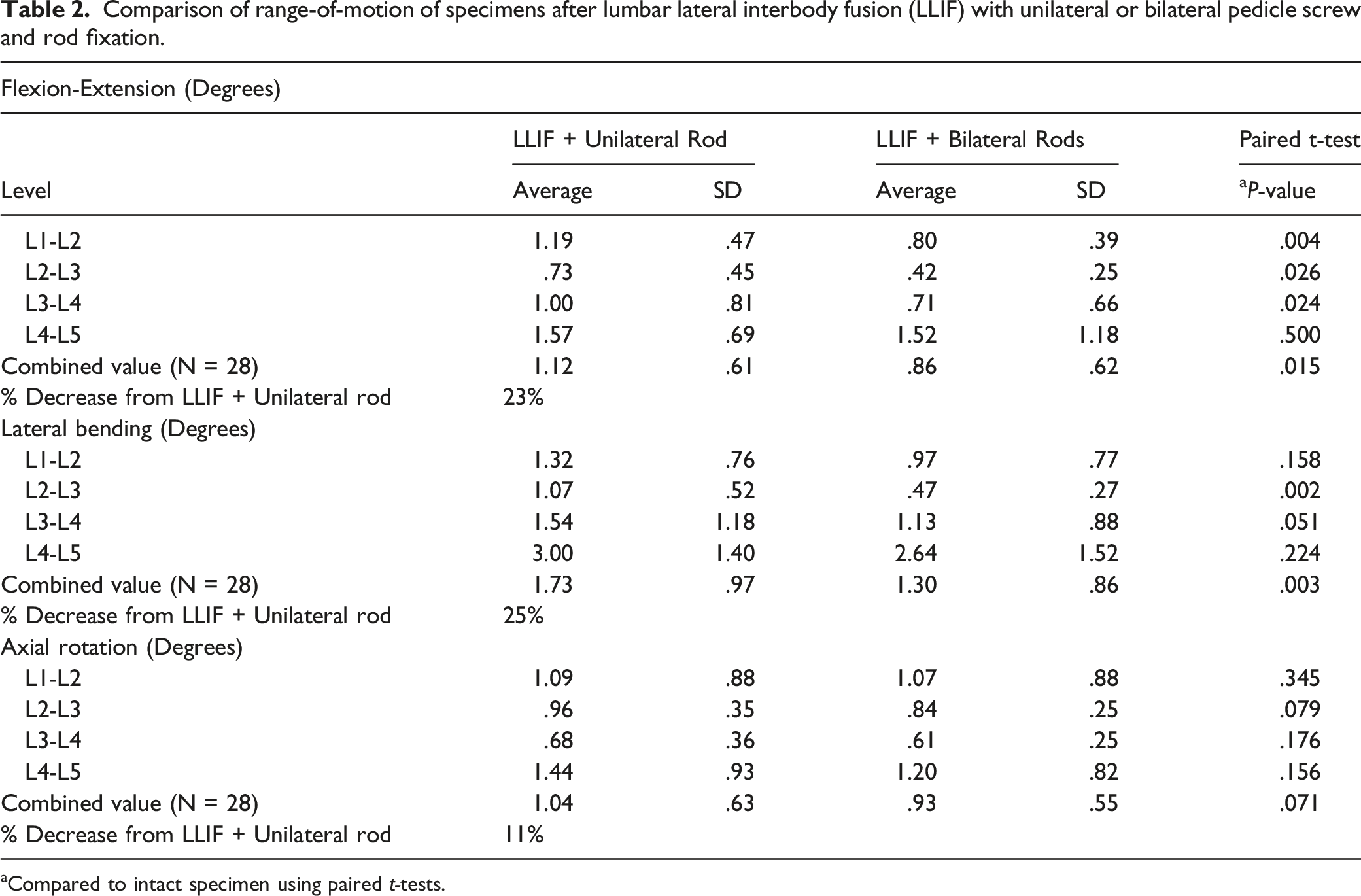
Compared to intact specimen using paired t-tests.
Discussion
The Current Study
Revealed that, after multilevel placement of 26 mm lateral interbody cages, bilateral pedicle screw and rod fixation showed statistically significant reductions in flexion-extension and lateral bending motions compared to unilateral rod fixation. Bilateral screws and rods also demonstrated lower axial rotation than unilateral screws and rods, although the difference did not reach statistical significance. Despite the purported biomechanical advantages conferred by the lateral interbody technique and extra wide (26 mm) cages, the addition of bilateral posterior instrumentation nevertheless showed demonstrably higher stability, defined here as a lower ROM. It should be noted that the results reflect differences in ROM, rather than construct stiffness; however, values of intervertebral displacement are valuable as they are indicative of the resistance that is provided by the structure’s stiffness.
Lateral interbody fusion performed with transpsoas or anterior to psoas access is biomechanically favorable due to the approach. Lateral access of the disc preserves the posterior tension band that is disrupted with posterior-based interbody fusion, which imparts increased stability. 16 The anterior longitudinal ligament (ALL) is a significant stabilizer of the spinal column, which is resected during anterior-based interbody fusion but is preserved with LLIF.17,18 Combining LLIF with open posterior techniques for adult deformity surgery has been reported to have decreased complications, faster recovery, and fewer levels fused compared to the use of all-posterior techniques. 19
The large footprint of LLIF cages provides enhanced loading of the apophyseal ring. Subsidence has been associated with cage width < 22 mm and cage height >11 mm, osteoporosis, and multilevel surgery. 20 Lang et al. reported a near-complete elimination of late subsidence with the use of extra-wide 26 mm cages. 21 A biomechanical study of single-level interbody fusion by Pimenta et al. compared the stabilizing effect of 26 mm LLIF cages, 18 mm LLIF cages, and TLIF cages either stand-alone or combined with bilateral or unilateral pedicle screw-rod fixation. 13 They found that stand-alone 26 mm cages demonstrated statistically greater stability in axial rotation and similar stability in flexion-extension and lateral bending as TLIF with bilateral pedicle screws and rods. This highlights the biomechanical importance of preserving the posterior tension band, which is removed with posterior-based open and minimally invasive interbody fusion techniques. 22 In addition, the stand-alone 26 mm LLIF cage construct was statistically more stable in axial rotation, flexion-extension, and lateral bending than the 18 mm LLIF cage with unilateral posterior supplemental fixation. This study demonstrated the substantial stability conferred by the greater apophyseal ring engagement of 26 mm cages, even in the stand-alone condition. Based on these findings, we hypothesized that unilateral rod fixation would provide similar biomechanical stability as bilateral screws and rods in a multilevel LLIF model utilizing extra-wide 26 mm cages.
Unilateral, as opposed to bilateral, pedicle screw and rod instrumentation as supplemental posterior fixation has important advantages including decreased blood loss, decreased operating room time, and short-term improvement in postoperative pain.23-26 Multiple large series of patients undergoing TLIF have reported lower cost and equivalent clinical outcomes with unilateral screw and rod fixation, although rates of non-union and cage migration may be higher.24-26
The use of unilateral pedicle screw fixation for LLIF has been described with good clinical and radiographic results. Wen et al. retrospectively compared 74 patients undergoing single-level LLIF supplemented with either unilateral or bilateral screw fixation and reported significantly decreased medical expenses ($11,044.80 vs $15,018.40) and lower Oswestry Disability Index (ODI) and visual analog pains scores (VAS) at 7-days postoperatively in the unilateral fixation group. 27 Unilateral screw fixation did not affect rates of fusion (86.8% vs. 91.7%) or cage subsidence. A prospective cohort study by Fukushima et al. of 100 patients similarly found shorter operative times with unilateral screw fixation with equivalent fusion rates (87.8% vs 84.7%) and subsidence rates between the study groups. 28 However, there was a higher rate (5 cases vs. 1 case) of reoperation in the unilateral screw group mostly due to cage loosening. A 20-patient case series by Du et al. reported excellent radiographic and clinical outcomes for single-level adjacent segment disease treated with LLIF and unilateral screw fixation. 29 Collectively, these studies suggest that unilateral screw fixation for LLIF in single-level disease may be sufficient.
We are not aware of any clinical reports of unilateral screw fixation after multilevel LLIF. If this is found to be an acceptable surgical strategy, the benefits of unilateral fixation in terms of time savings and decreased morbidity30,31 could potentially be amplified in the setting of multilevel LLIF. The use of unilateral fixation could facilitate single-position surgery, in which the patient remains in the lateral decubitus position after LLIF and pedicle screws are placed in this position. The technical feasibility of percutaneously instrumenting one side of the spine in the lateral position (usually the superior side) is considerably less challenging than bilateral instrumentation. The perceived need to place bilateral pedicle screws and rods has given rise to the concept of single position LLIF surgery in the prone position. However, the potential complications of placing only unilateral constructs (e.g., pseudoarthrosis, late deformity, decreased correction, etc.) could be multiplied in multilevel LLIF, so characterization of the biomechanical properties is critical.
Previous biomechanical studies on unilateral fixation after LLIF have been limited to single-level fusion and/or narrow interbody cages (18 mm or less in width). We chose 26 mm cages in a 4-level LLIF model because the extra wide cages possess important biomechanical advantages. 13 Godzik et al. evaluated single-level LLIF at L2-3 or L3-4 with unilateral and bilateral pedicle screw fixation in 13 human specimens utilizing 18 mm cages. 32 They reported statistically similar stiffness in flexion-extension, lateral bending, and axial rotation. A similar study from the same institution by Reis et al. evaluated LLIF in seven cadaveric specimens at L3-4 combined with multiple supplemental fixation methods. 33 The bilateral pedicle screw fixation construct afforded a 91% decrease in flexion, 82% decrease in extension and lateral bending, and 74% decrease in axial rotation compared with intact specimens. They reported a significant decrease in stability with unilateral screw fixation, which was roughly one-half the stiffness of bilateral screw fixation. Our findings were similar in the multilevel setting, in which we observed an 83% decrease in flexion-extension, 64% decrease in lateral bending, and 34% decrease in axial rotation with bilateral screws and rods, as well as significant decreases in construct stiffness with unilateral screw fixation. A multilevel LLIF cadaveric study utilizing 17 mm wide cages by Lai et al. tested six T12-L5 human specimens with LLIF at L2-5 combined with either unilateral screws, bilateral screws, or lateral plate fixation. 34 The authors found bilateral pedicle screw fixation significantly reduced overall lumbar motion in flexion-extension (3° vs. 5.93°), lateral bending (3.69° vs. 7.37°), and axial rotation (6.46° vs. 9.82°) compared to unilateral screws. Nevertheless, they concluded that unilateral screw or plate fixation may provide sufficient biomechanical stability for multilevel LLIF. The reported reductions in ROM are larger than our results, which may be attributable to differences in experimental technique and the notably high baseline ROM of the intact specimens reported by Lai et al. We utilized a high proportion (87.5%) of relatively large diameter 7.5 and 8.5 mm screws. Screw diameter has been shown to have a significant effect on stiffness. 35
In conclusion, we observed considerable decreases in ROM from the intact condition after 4-level LLIF utilizing 26 mm cages for both unilateral and bilateral pedicle screws and rods. The addition of bilateral posterior fixation provides a 10-25% additional decrease in ROM. The stability afforded by unilateral screws and rods after multilevel LLIF may be adequate to achieve a solid arthrodesis for select patients, such as those with minimal risk factors for cage subsidence or non-union. The results of this study can inform surgeons as they consider unilateral or bilateral posterior fixation regarding the incremental biomechanical benefit that can be expected from additional instrumentation. Our results concluded that the construct with maximum stability, regardless of the use of extra-wide cages, remains LLIF with bilateral screws and rods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs. James Mok and Farid Amirouche disclose in-kind product donation by Nuvasive. Dr. James Mok discloses that he receives consulting fees and royalties from MiRus. Drs. Craig Forsthoefel, Roberto Leonardo Diaz, and Ye Lin have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.