
Abstract
Study Design
Observational study.
Objective
To evaluate representation of countries and gross national income (GNI) at major international spine conferences.
Methods
The 50 most attended spine conferences were identified via ChatGPT. Conferences were excluded if they (1) reference/are held in a single country, (2) emphasize one technique, (3) emphasize neurosurgery or orthopaedic spine, (4) have <2 years of conference programs available. Programs were reviewed (2022-2024) to identify invited speakers/award recipients, executive board members, and committee members and their country of practice. Countries were assigned GNI/capita from World Bank data.
Results
Eurospine, GSC, IMAST, ISASS, NASS, and SRS met inclusion criteria (1462 unique invited speakers/awardees). Other than Eurospine, board members were predominantly from Northern America. Speakers were most commonly from Northern America (56.2%), with no representation from Southern Africa and Central Asia. Speakers were overwhelmingly from high-income countries (89.7%) with none from low-income countries. Speakers at GSC were the most globally representative, with 68.8% from countries diverse from GSC’s executive board. GSC and NASS had the greatest representation from lower-middle (9.7%) and upper-middle income countries (30.4%), respectively. USA and Germany had 867 (59.4%) invitees, while all of Africa had four. Committee members followed similar trends compared to invited speakers for region, country, and GNI/capita representation.
Conclusions
Amongst major international conferences, a preponderance of invited speakers and committee members were from a small number of regions, particularly Northern America and Western Europe. Most speakers and committee members practice in high-income countries, with no representation from low-income countries.
Keywords
Introduction
Disorders of the spine can have a substantial impact on quality of life, and are a major source of global disability.1,2 These disorders affect patients across a wide range of ages and socioeconomic statuses, and can be particularly impactful for individuals from low- and lower-middle income countries.3,4 Country income level designations are calculated by the World Bank, and are based on gross national income (GNI) per capita.5,6 Low and lower-middle income countries are especially vulnerable to spinal disorders for a variety of reasons. These include an increased prevalence of degenerative spine disease, suboptimal outcomes for spine and spinal cord trauma, and commonly endemic tuberculosis.7-14 Tuberculosis spinal infection in particular can lead to deformity, prolonged treatment, and frequently incomplete resolution of symptoms.15-18 Finally, spinal disorders can be costly—effective strategies for cost containment and sustainability of spine treatment in low and lower-middle income countries have not been well researched. 19
Due to these challenges of treating spinal disease in low- and lower-middle income countries, there has been a call for additional research, greater collaboration with upper-middle and high-income countries, and improved education and information-sharing.20,21 Despite this, a recent review by Lin et al. noted that literature on spine-focused clinical partnerships between high-income and low- and middle-income countries is sparse. 22 One potentially impactful intervention to address these disparities is international spine surgery conferences. Medical conferences represent an important source of career advancement, collaboration, education, and sharing of clinical and research experiences. 23 In particular, when these conferences have an international or global footprint, they offer unique opportunities for reducing disparities and promoting equity. However, there is minimal data in the literature characterizing the representation of different countries and country income levels at the major international spine conferences.
For these reasons, the purpose of the current work was to identify the most prominent spine surgery conferences with an international presence, and characterize the degree to which they actively engage spine surgery providers and researchers from other countries, especially those from lower-middle and lower-income levels. These data are important in order to continue guiding efforts amongst the international spine community to facilitate truly global collaboration, clinical research, publication output, and education.
Methods
The current work exclusively utilized publicly available data, and thus was deemed Institutional Review Board exempt. The initial list of spine surgery conferences was generated by the prompt “Can you list the top 50 attended spine conferences globally?”, which was entered into ChatGPT 4.0. This list was narrowed through a series of exclusions including: (1) use of a singular country in the conference name (eg, The Irish Spine Society), and/or mention on the conference website of an emphasis on local rather than global involvement; (2) conference meetings predominantly being held in the same country (eg, Cervical Spine Research Society); (3) emphasis on a single surgical technique (eg, International Society for Minimal Intervention in Spinal Surgery), or non-surgical techniques; (4) emphasis on neurosurgery or orthopaedic spine surgery (ie, exclusive of the other specialty); (5) focus on multi-specialty orthopaedic surgery (eg, American Academy of Orthopaedic Surgeons); (6) Less than 2 years of conference programs and/or lack of consecutive years available online. For each included conference, all available annual meeting programs were collated from 2022-2024 for review.
Identification and Characterization of Attendees
The primary outcome was the degree of intentional inclusion of international involvement at the selected major spine surgery conferences. Thus, the available annual meeting programs were analyzed to identify all invited speakers, award recipients, and committee members. Additionally, the executive board members of each conference were obtained from conference/society websites. Departmental websites, society websites, and publicly available social/professional media were examined for country identification of current practice/work location. Additionally, each current practice/work location was assigned a geographic region. This region was based on the 22 United Nations geoschemes, which were condensed to 14 geographic regions to facilitate descriptive statistics.24,25 The final 14 geographic regions were (1) Northern America, (2) Central America, (3) Caribbean and South America, (4) Western, Middle, and Eastern Africa, (5) Southern Africa, (6) Northern Africa, (7) Northern, Western, and Southern Europe, (8) Eastern Europe, (9) Central Asia, (10) Western Asia, (11) Southern Asia, (12) Eastern Asia, (13) Southeastern Asia, Micronesia, Polynesia, and Melanesia, and (14) Australia and New Zealand.
Each invited speaker/award recipient was defined as either concordant with or diverse from the conference to which they were invited. Conferences were assigned a region based on the most common country of practice (mode) amongst their executive board members. Additionally, the current practice/work country of each invited speaker/award recipient was assigned a gross national income (GNI) per capita based on the most recent data from the World Bank.6,26 Finally, each current practice/work country was assigned a designation as a low-income, lower-middle income, upper-middle income, or high-income country based on GNI per capita data and income cut-offs established by the United Nations, which have been utilized previously in the spine literature. 27
Invited speakers/award recipients who appeared more than once at the same conference in the same year were counted only once. In contrast, the same individual serving on more than one committee was counted for each committee appointment. Additionally, invited speakers/award recipients/committee members were excluded if (1) no information was found online regarding their current practice/work location; (2) they were non-physician conference speakers (eg, physical therapists, attorneys, etc.); or (3) they were not directly involved in the care or research of spinal disorders.
Results
Amongst the 50 initially identified conferences, six met inclusion criteria for further analysis. These conferences were (1) the Eurospine Annual Meeting, (2) AO Spine’s annual meeting, the Global Spine Congress (GSC), (3) the International Meeting on Advanced Spine Techniques (IMAST), (4) the International Society for the Advancement of Spine Surgery (ISASS) Annual Conference, (5) the North American Spine Society (NASS) Annual Meeting, and (6) the Scoliosis Research Society (SRS) Annual Meeting. The total number of unique invited speakers/award recipients counted amongst all included conference data was 1462. The total number of committee member positions was 399. The inclusion and exclusion criteria flow diagram is summarized in Figure 1. Flow diagram summarizing inclusion and exclusion criteria for conferences, invited speakers, and committee members.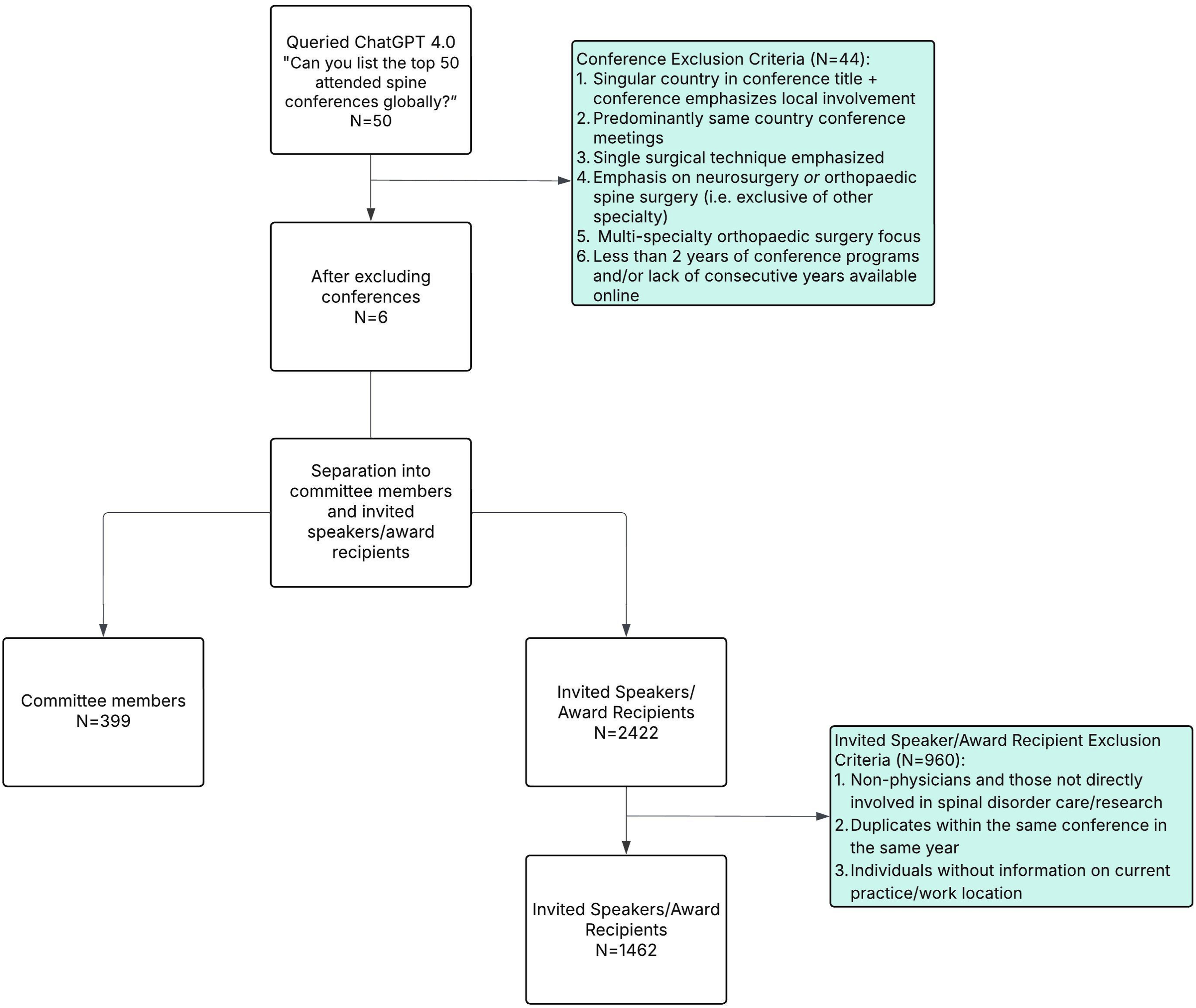
Geographic and Economic Characteristics of Invited Speakers and Awardees’ Country of Employment at Six International Spine Surgery Conferences.
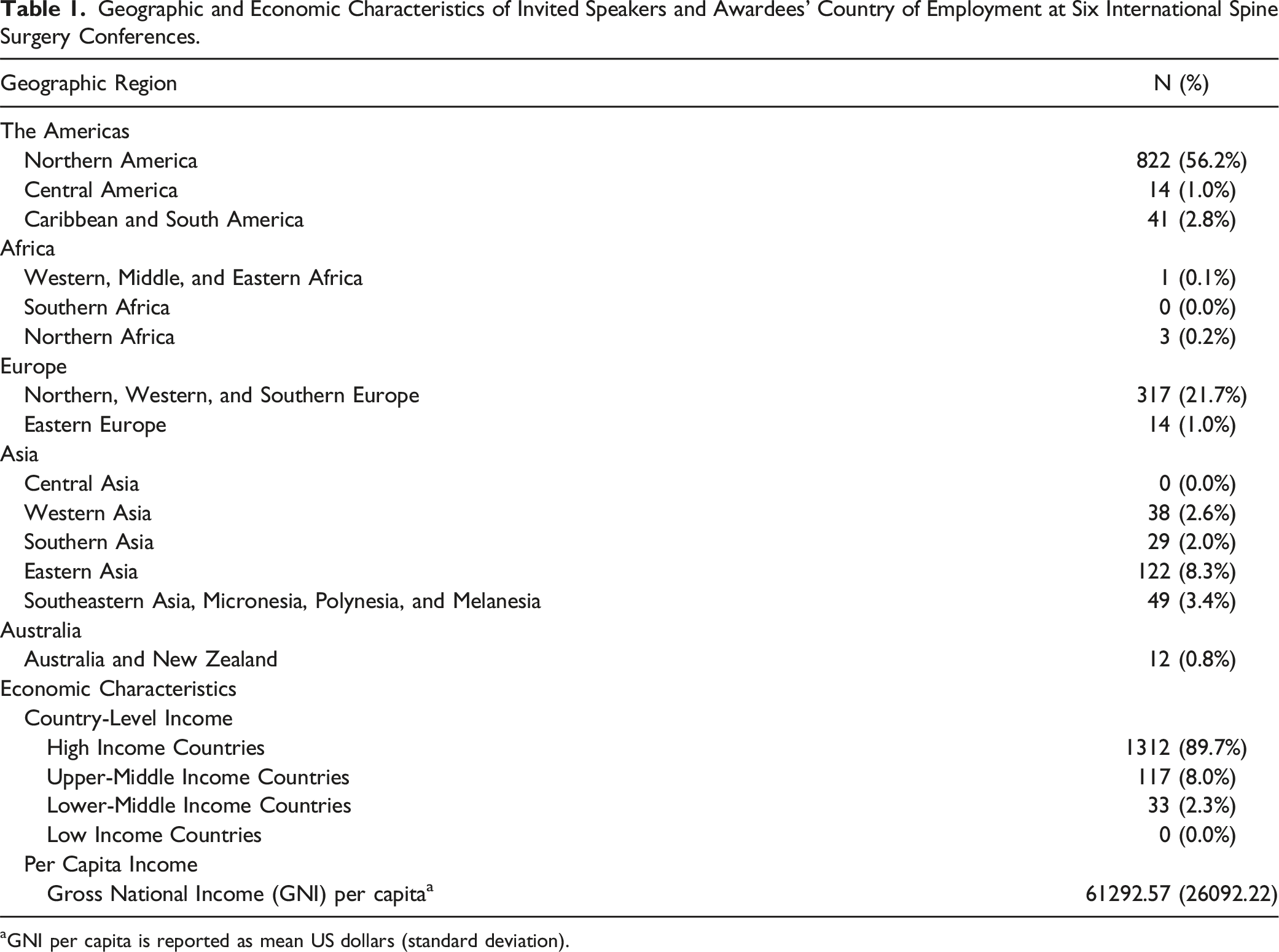
aGNI per capita is reported as mean US dollars (standard deviation).
Geographic Representation of Invited Speakers and Awardees’ Country of Employment Stratified by Spine Surgery Conference.
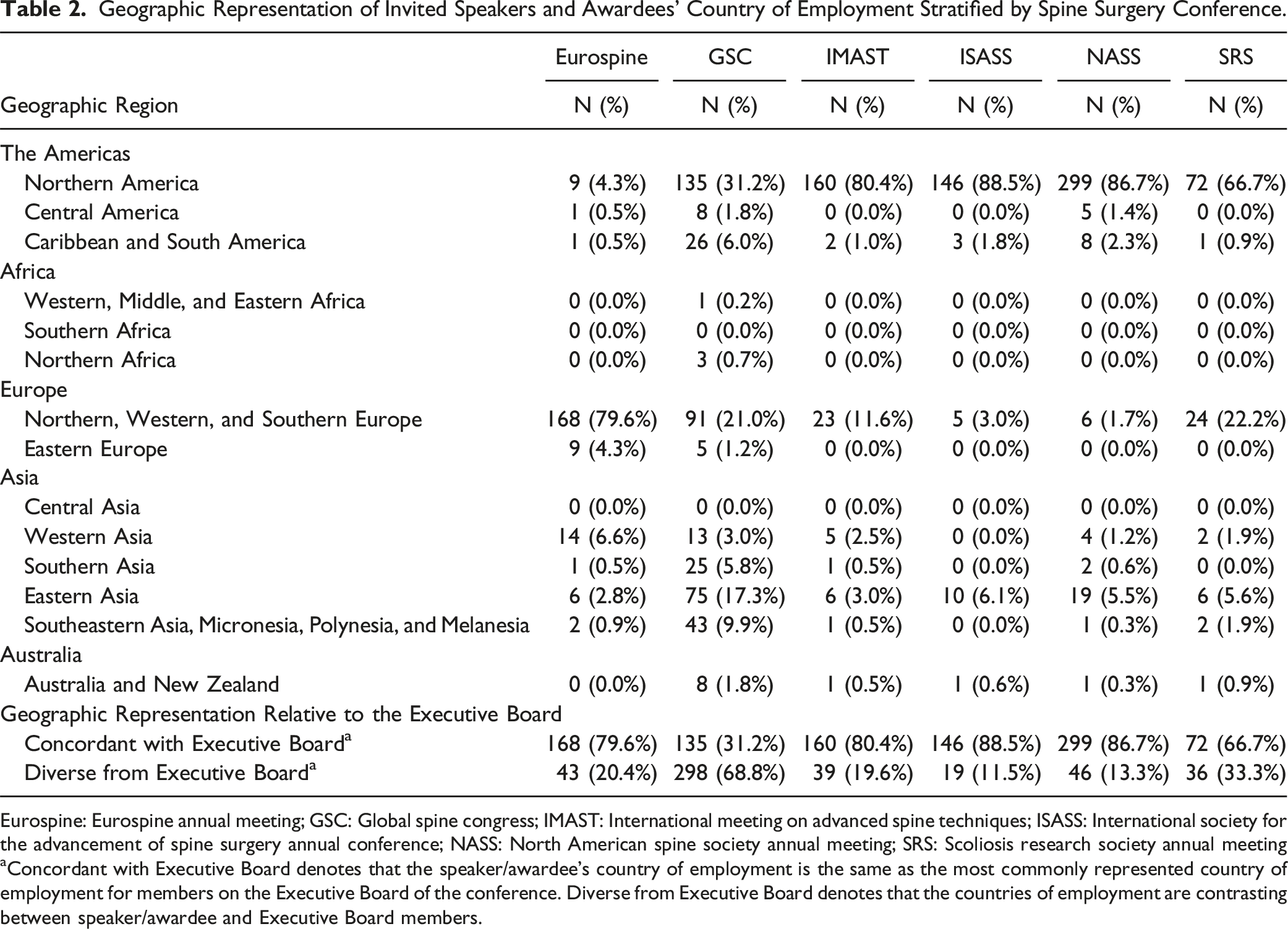
Eurospine: Eurospine annual meeting; GSC: Global spine congress; IMAST: International meeting on advanced spine techniques; ISASS: International society for the advancement of spine surgery annual conference; NASS: North American spine society annual meeting; SRS: Scoliosis research society annual meeting
aConcordant with Executive Board denotes that the speaker/awardee’s country of employment is the same as the most commonly represented country of employment for members on the Executive Board of the conference. Diverse from Executive Board denotes that the countries of employment are contrasting between speaker/awardee and Executive Board members.
Economic Characteristics of Invited Speakers and Awardees’ Country of Employment Stratified by Geographic Representation Relative to the Executive Board and Spine Surgery Conference.
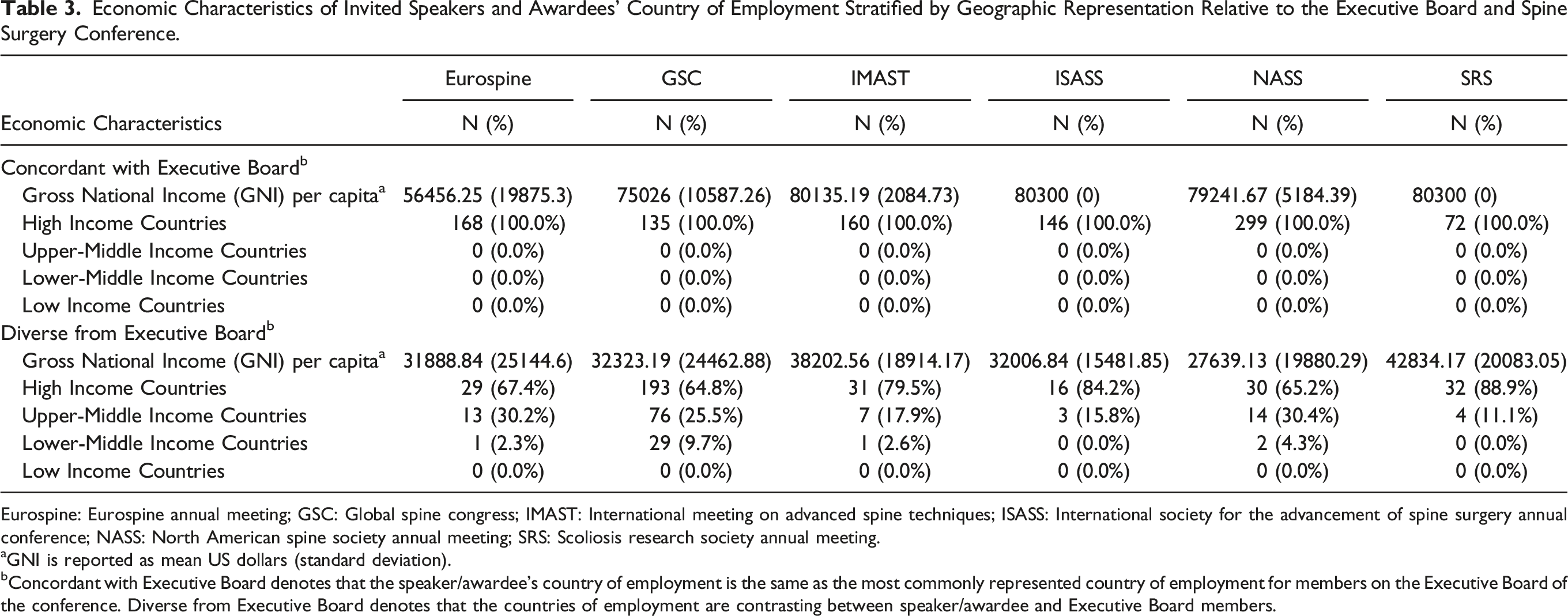
Eurospine: Eurospine annual meeting; GSC: Global spine congress; IMAST: International meeting on advanced spine techniques; ISASS: International society for the advancement of spine surgery annual conference; NASS: North American spine society annual meeting; SRS: Scoliosis research society annual meeting.
aGNI is reported as mean US dollars (standard deviation).
bConcordant with Executive Board denotes that the speaker/awardee’s country of employment is the same as the most commonly represented country of employment for members on the Executive Board of the conference. Diverse from Executive Board denotes that the countries of employment are contrasting between speaker/awardee and Executive Board members.
Invited Speakers and Awardees’ Country of Employment Stratified by Spine Surgery Conference.
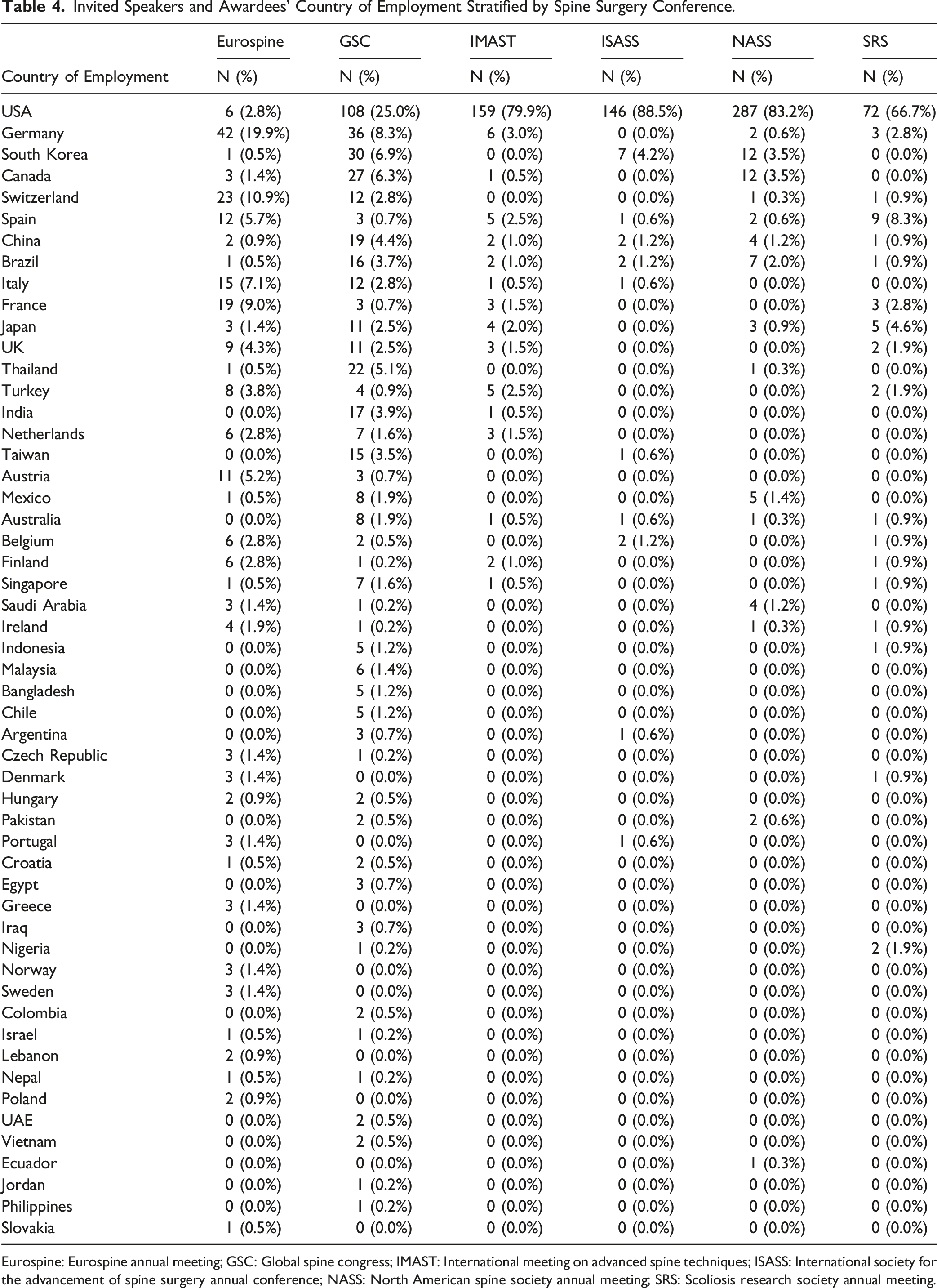
Eurospine: Eurospine annual meeting; GSC: Global spine congress; IMAST: International meeting on advanced spine techniques; ISASS: International society for the advancement of spine surgery annual conference; NASS: North American spine society annual meeting; SRS: Scoliosis research society annual meeting.
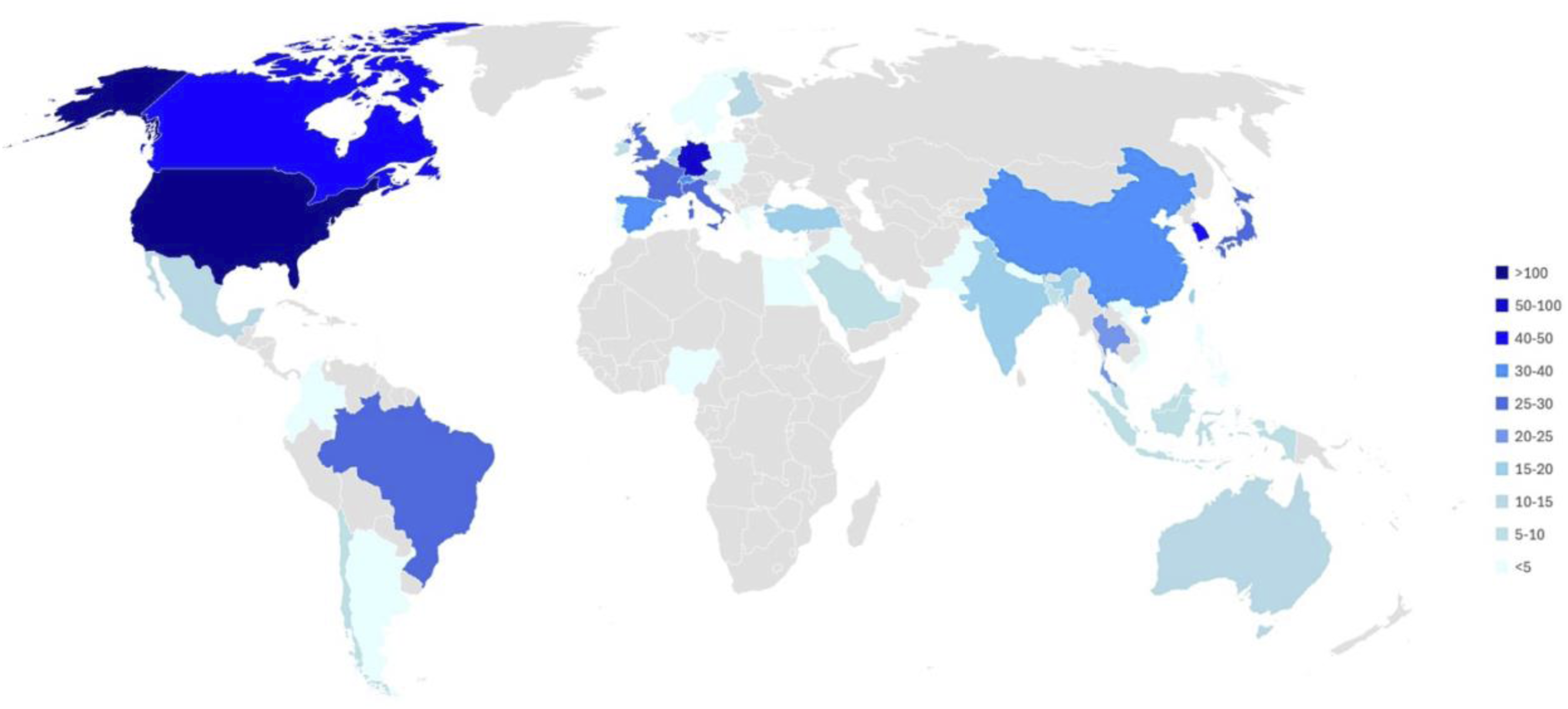
Countries with invited speakers/award recipients at the six conferences, graded by number invited.
Geographic and Economic Characteristics of Committee Members’ Country of Employment at Six International Spine Surgery Conferences.
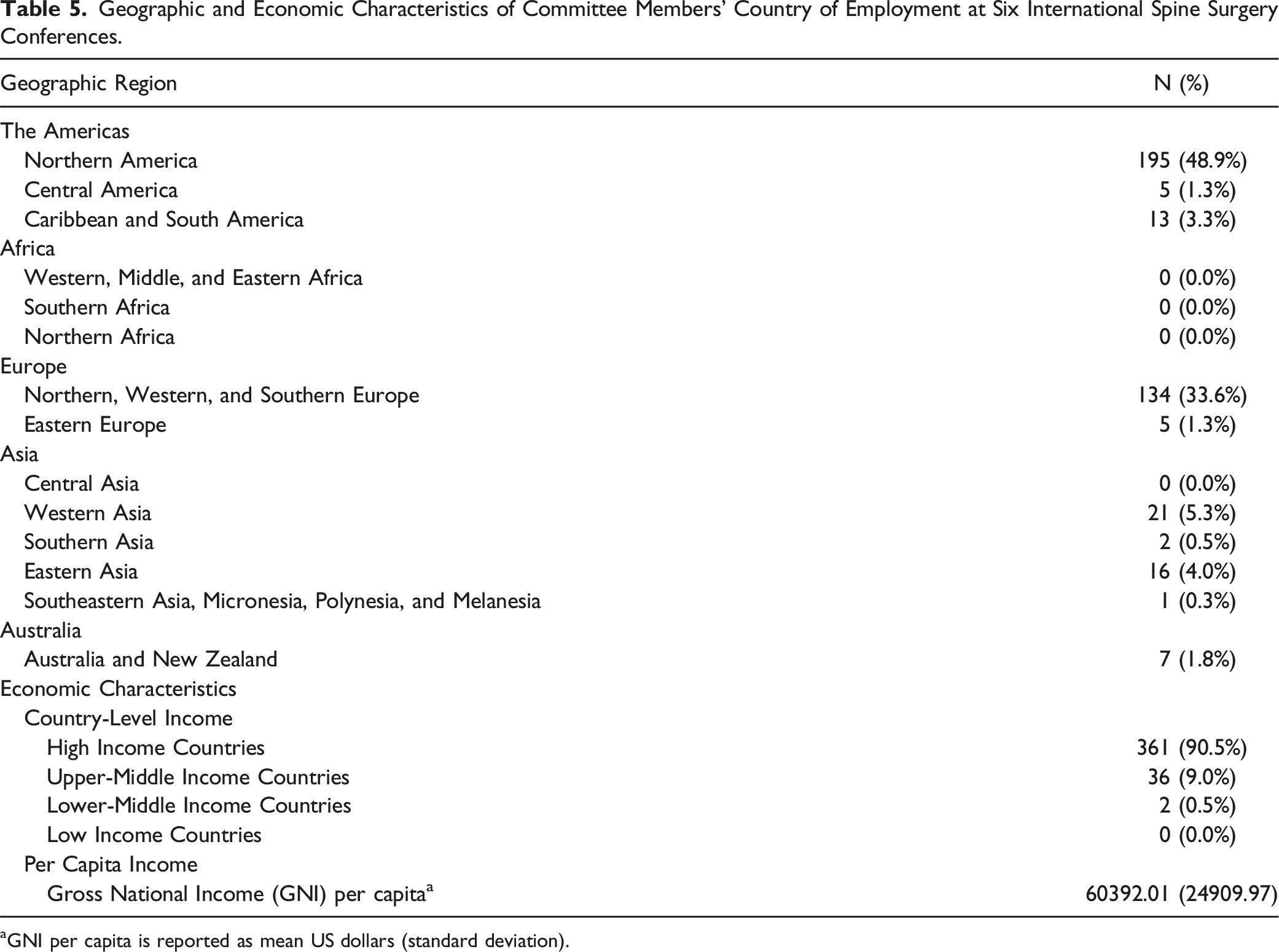
aGNI per capita is reported as mean US dollars (standard deviation).
Geographic Representation of Committee Members’ Country of Employment Stratified by Spine Surgery Conference.
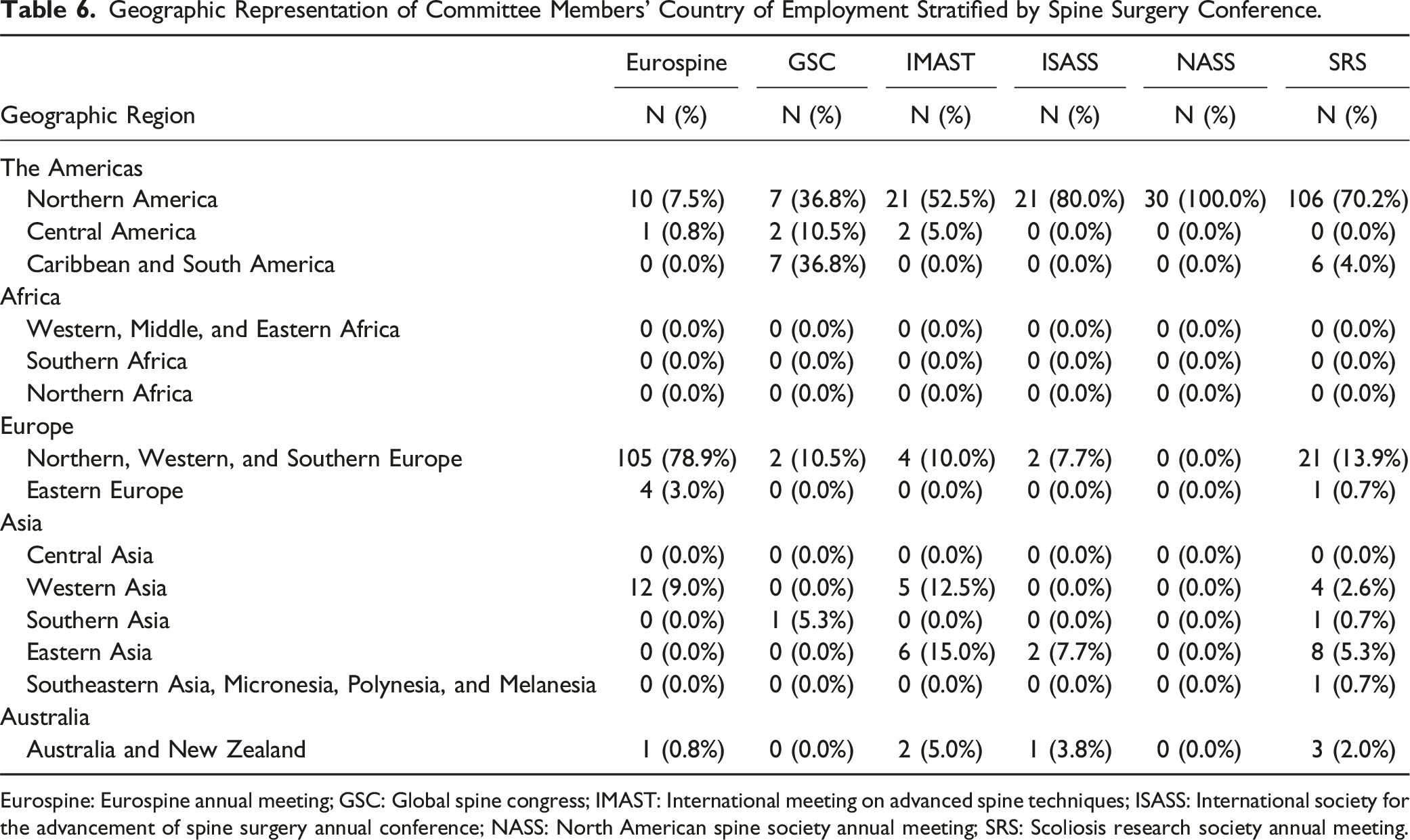
Eurospine: Eurospine annual meeting; GSC: Global spine congress; IMAST: International meeting on advanced spine techniques; ISASS: International society for the advancement of spine surgery annual conference; NASS: North American spine society annual meeting; SRS: Scoliosis research society annual meeting.
Economic Characteristics of Committee Members’ Country of Employment Stratified by Geographic Representation Relative to the Spine Surgery Conference.
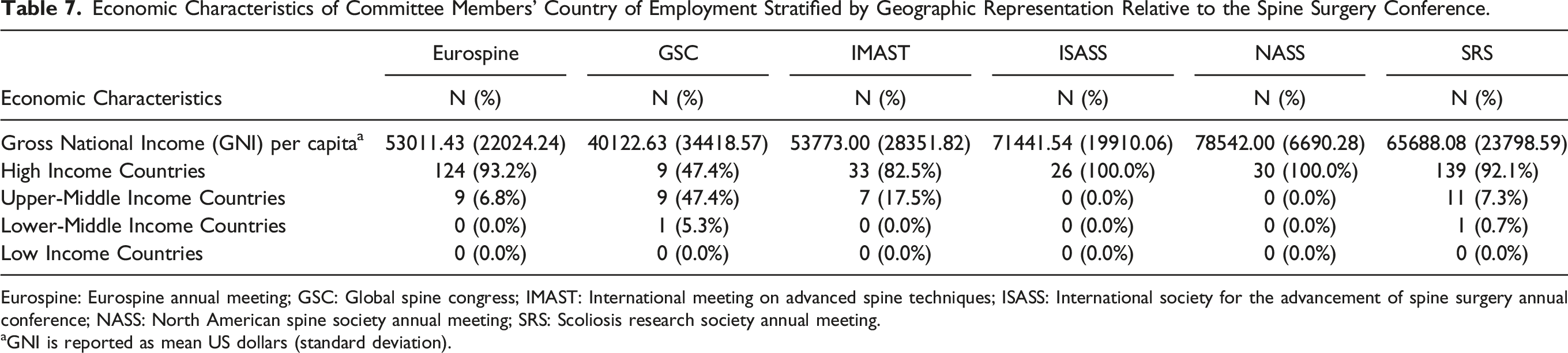
Eurospine: Eurospine annual meeting; GSC: Global spine congress; IMAST: International meeting on advanced spine techniques; ISASS: International society for the advancement of spine surgery annual conference; NASS: North American spine society annual meeting; SRS: Scoliosis research society annual meeting.
aGNI is reported as mean US dollars (standard deviation).
Committee Members’ Country of Employment Stratified by Spine Surgery Conference.
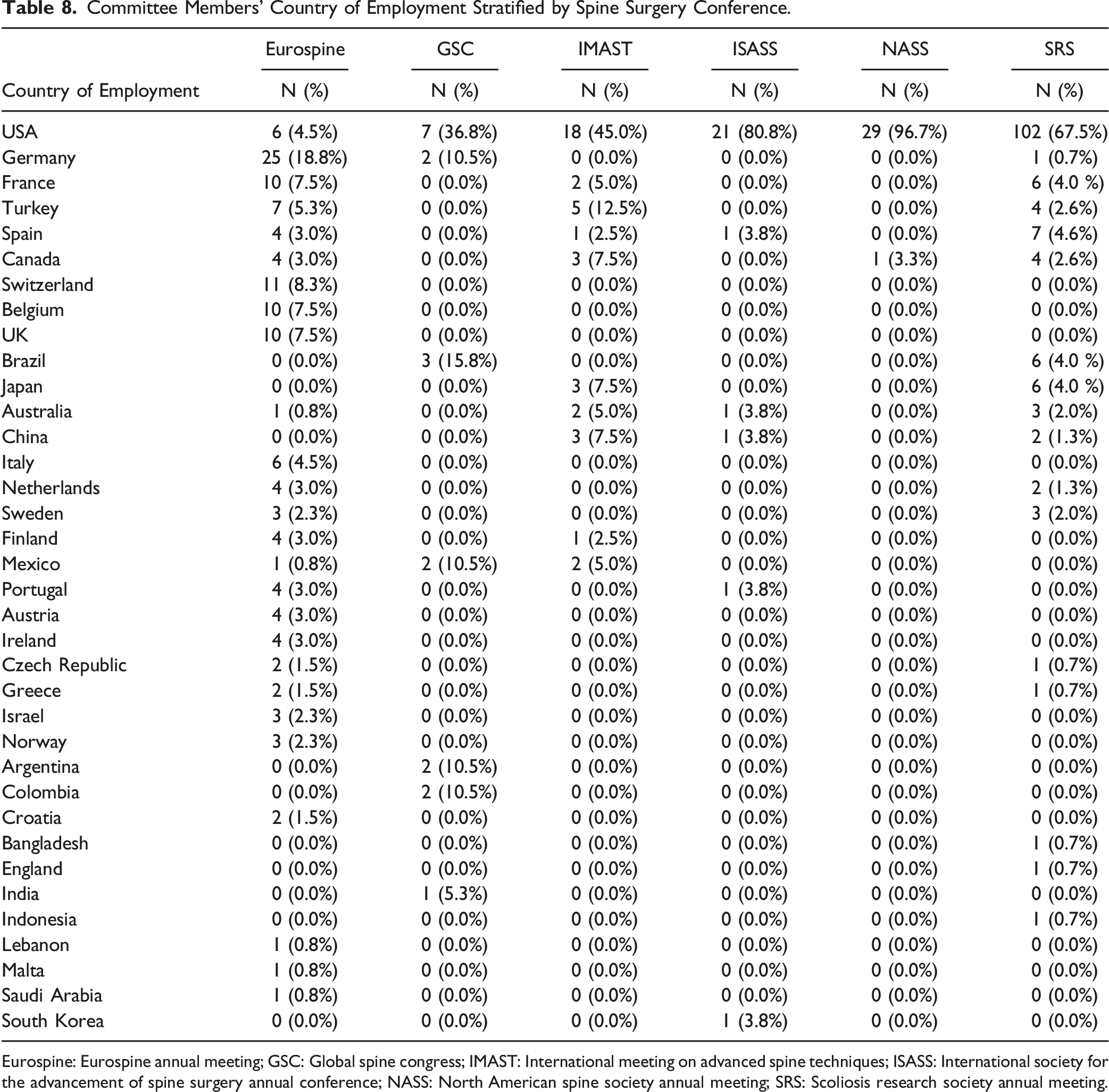
Eurospine: Eurospine annual meeting; GSC: Global spine congress; IMAST: International meeting on advanced spine techniques; ISASS: International society for the advancement of spine surgery annual conference; NASS: North American spine society annual meeting; SRS: Scoliosis research society annual meeting.
Discussion
The goal of access for all individuals and regions to high-quality medical care by the year 2030 has been posited previously in the literature.27-29 This endeavor extends beyond provision of material resources, and externally trained providers, and includes collaboration across the spectrum of different regions and income designations of countries. To this end, several important undertakings have been initiated within the field of spinal disorders, including the Global Spine Care Initiative, the SRS Global Outreach Program, and World Spine Care.30,31 These efforts emphasize the importance of collaboration in order to provide evidence-based practices, sustainability and scalability. Ideally, these collaborative efforts should involve exchange of perspectives and techniques, research, and education. International conferences, in particular, represent critical opportunities for such collaboration. Unfortunately, data on the diversity of country involvement, and representation from lower-middle, and low-income nations at international conferences is severely lacking.
The current study utilized publicly available data from several of the most prominent international conferences to identify important trends amongst invited speakers, award recipients, and members of conference committees. Most notably, the overwhelming majority of invitees to the six international conferences surveyed in the present work come from high-income countries, with no invitees coming from low-income countries. Additionally, with the exception of GSC, all conferences analyzed had a large majority of invited speakers/award recipients coming from a country that was similar to the national composition of the conference’s executive board. Africa, Central Asia, Eastern Europe, and South and Central America all had very low percentages of invited speakers/award recipients. All of these trends were similarly reflected amongst the membership of various conference-related committees.
Low and middle income countries are disproportionately affected by musculoskeletal disease.22,32,33 In the current work, no invitees to conferences or members of conference committees came from low-income countries, and only 33 invited speakers/awardees (2.3%) came from lower-middle income countries, and 2 committee members (0.5%) came from lower-middle income countries. Notably, these numbers are spread across the multiple years surveyed in this project, and across six major conferences—thus, the representation per year and per conference is even lower. The reasons for these disparities are undoubtedly multi-factorial, and it is beyond the scope of the current work to perform an exhaustive global economic analysis. However, a few factors potentially at play warrant further discussion. While a recent estimate proposed that low and middle income countries represent nearly half of the global population, these countries account for less than 20% of the world’s surgeons. 34 This constitutes a ratio of providers per 100,000 people that is over ten times lower than high-income countries. 34 Due to additional barriers regarding limitations of resources, training and education programs, the equity of distribution of surgical specialists, such as spine providers, is even more disproportionate. 29 Thus, one of the primary reasons for disparities amongst low- and lower-middle income countries being invited to speak at major international conferences could simply be the limited number of these professionals in those countries.
Another reason could be the cost of attending conferences and language barriers. A recent article assessing 46 surgical societies across multiple continents noted that total cost of conference attendance including registration, travel, and board could be substantial. The authors concluded specifically that these costs could be a significant barrier for individuals from lower and middle income countries. 35 Previous work, especially during and after the COVID-19 pandemic, has suggested virtual conference options as both a cost and carbon-footprint saving option. 36 Unfortunately, one possible drawback of this strategy is a decrease in skill transfer opportunities for virtual attendees. However, virtual speaking options for invited speakers may also provide a means of circumventing language barriers via digital translation and subtitles. Additional potential solutions proposed for individuals from low and middle income countries include discounts by the conferences themselves. 37 These strategies have been posited as a way to ameliorate financial barriers and improve equity. Within the context of the current work, this could represent a solution, but would potentially require some degree of financial collaboration in order to off-set cost. This may take the form of industry sponsorship or levying additional registration fees on high-income country conference attendees. Further research is needed within the field of spine surgery in order to identify best practices for registration and travel fees for major international conferences.
The current work showed a substantial asymmetry for invitees not only in terms of GNI per capita, but also in terms of world regions. Large swathes of South America, Africa, and Asia were not well represented as invited speakers. This is important within the context of spine surgery for a number of reasons. The burden of degenerative, and especially traumatic spine disease are substantial in low and middle income countries relative to high-income countries. 12 Research in several regions of Africa and Southeast Asia have emphasized the prevalence and impact of spine disorders.7-11 Long-term data from a Nigerian hospital, for example, reported that over half of all surgical cases were indicated for degenerative spine disorders. 38 Addressing these issues in a way that incorporates both the resources of high-income countries, and the perspectives and specific socioeconomic, geopolitical, and cultural needs of low- and middle-income countries is a hugely challenging enterprise. International spine conferences represent one of the few opportunities for this type of intensive collaboration to take place. Thus, improving invited representation at spine conferences for these underrepresented regions may be a promising strategy for improving equitable provision of spine treatment, research, and care. This could have both clinical implications, in terms of providing educational and collaborative avenues for standardizing clinical spine care globally, and scientific implications, in terms of facilitating global multicenter research.
In addition to the more economically focused discussion above, there are several potential reasons for the decreased regional representation across certain aspects of the globe at spine conferences. First, conferences may differ in terms of their specific mission-statements and focus. GSC, for instance, had the most diversity both amongst its executive board, and amongst its invited speakers. This correlation may indicate a particular emphasis by AO Spine and/or GSC to address international spine issues. The impact of the diversity of a spine executive board on international representation and focus has been proposed by Xu et al. in a prior research work related to leading spine journals. 39 In contrast, if other spine conferences are more purely research-driven in terms of their invited speakers, this may lead to an otherwise unintentional decreased emphasis on certain regions. A recent work by Pascual-Leone et al. noted that while non-USA research output continues to increase each year, the overwhelming majority of work is still produced by a relatively small number of high-income countries. 40 Thus, one of the factors limiting additional invitations to surgeons from lower-middle and low income countries could be related to the relatively decreased academic output from these nations. It is certainly not the intention of the current work to assess or critique a particular society or conference’s mission. Rather, the goal of the present study is to broadly assess representation from a diverse array of national and economic backgrounds at the major spine surgery conferences in order to encourage further thought and research on this important topic.
The current work has several limitations, beyond those inherent to retrospective studies. Firstly, this investigation relied entirely on publicly available data, and required evaluation of websites from all over the world. Thus, it is possible that some of the reported information was incomplete or inaccurate. This was hopefully ameliorated by the relatively large size of the dataset, and by the use of only major conferences as sources of subjects. Secondly, this study was intended to be a relatively broad overview of trends amongst major spine conferences. Thus, it does not represent a rigorous economic or geopolitical evaluation that would add further context or granularity to the presented data. Future work will potentially aim to address this in collaboration with experts outside of the field of spine surgery in order to strengthen the statistical rigor. Finally, the authors concede that there are a wide variety of spine conferences not evaluated by this work. Thus, the conclusions cannot be applied generally to all spine conferences. This was intentional in order to focus only on the representation of diverse countries and economic backgrounds at major conferences with an international presence. Evaluating less prominent or regional conferences would have been outside the scope of the current project. Future work may broaden the analysis to include a more extensive list of global spine conferences.
Conclusions
The current work indicates that amongst the six major international spine conferences analyzed, there is a preponderance of invited attendees from a relatively small number of regions and countries. There was some variance between conferences in terms of the extent to which the decision-making bodies of the respective conferences were similar vs dissimilar from their invitees. However, the overwhelming majority of invited individuals were from high-income countries, with no representation from low-income countries. These findings are important, because international conferences represent an important avenue for relationship-building and collaboration between spine surgical professionals from different countries. Thus, understanding the current amount of representation from different countries at international conferences may encourage future outreach and inclusion. Substantial further research is needed on this important topic.
Footnotes
Acknowledgements
The authors would like to acknowledge ChatGPT (version 4.0) for its assistance in identifying the initial top 50 most attended global spine conferences.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JAC: Accelus – research support, Cervical Spine Research Society – board or committee member, PathKeeper Surgical – stock or stock options; unpaid consultant, Wolters Kluwer Health – Lippincott Williams & Wilkins – editorial or governing board. ASH: Biomet – IP royalties, CTL America – IP royalties, Paradigm spine – stock or stock options. ARV: Receives royalties from Stryker, Globus, Medtronic, Atlas Spine, Alphatech Spine, SpineWave, Spinal Elements, Elsevier, Jaypee, Taylor Francis/Hodder and Stoughton, and Thieme; has stock or stock options in Accelus, Advanced Spinal Intellectual Properties, Atlas, Avaz Surgical, AVKN Patient Driven Care, Cytonics, Deep Health, Dimension Orthotics LLC, Electocore, Flagship Surgical, FlowPharma, Rothman Institute and Related Properties, Globus, Harvard MedTech, Innovative Surgical Design, Jushi (Haywood), Nuvasive, Orthobullets, Parvizi Surgical Innovation, Progressive Spinal Technologies, Sentryx, Stout Medical, ViewFi Health; and is a consultant for Stryker, Globus, Spinal Elements, Accelus, and Ferring Pharmaceutical; Serves on Scientific Advisory Board / Board of Directors / Committee for National Spine Health Foundation (NSHF), Sentryx, and Accelus. CKK: Clinical Spine Surgery – editorial or governing board, Inion – IP royalties, Regeneration Technologies, Inc. – research support. GDS: Advance Medical – paid consultant, Bioventus – paid consultant, Surgalign – paid consultant, AOSpine – board or committee member, AOSpine – other financial or material support, Cervical Spine Research Society – board or committee member, Cerapedics – research support, DePuy, A Johnson & Johnson Company – research support, Medtronic Sofamor Danek – research support, Wolters Kluwer Health – Lippincott Williams & Wilkins – editorial or governing board. All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
ORCID iDs
Data Availability Statement
Data available upon reasonable request.