
Abstract
Study Design
Retrospective study.
Objective
The aim of this study is to evaluate the radiological, neurological and clinical outcomes of single-stage posterior unilateral transpedicular corpectomy (PUTC) technique for severe thoracic and lumbar complete burst fractures.
Methods
Sixteen patients with thoracic and lumbar burst fractures characterized by the involvement of both endplates and thoracolumbar injury score such as a Load Sharing Classification (LSC) point 7 or greater and the Thoracolumbar AO Spine Injury Score (TL AOSIS) 9 or more treated with PUTC technique were retrospectively reviewed. Preoperative and the final follow-up radiological parameters were measured. Demographic data, neurologic function, clinical outcomes and surgery-related complications were further analyzed.
Results
The mean age was 40.3 years with the average follow-up of 25.6 months. The mean estimated blood loss and operating time were 685.7 ± 268.6 mL and 312.5 ± 50.4 min. Loss of vertebral body height and segmental kyphosis were 59.9% and 14.6° before surgery, which significantly improved to 18.6% and −6.8° at the final follow-up. Solid fusion was achieved in all patients. ASIA grade improvement was significantly observed in 15 patients with incomplete neurologic deficits. The preoperative pain and function level showed a mean VAS score of 8.7 and ODI of 90.6% that improved to 1.6 and 23.7%. None of patients developed iatrogenic nerve root injury.
Conclusions
Single-stage PUTC technique with circumferential reconstruction can achieve sufficient spinal canal decompression, improvement of neurological deficit, ideal kyphosis correction with ventral column reconstruction and the avoidance of anterior approach in patients with severe thoracic and lumbar complete burst fractures.
Keywords
Introduction
Vertebral burst fractures of the spine result from axial loading and are frequently with the concomitant flexion, which result in spinal canal encroachment, collapse of the fractured vertebral column and kyphotic deformity.1,2 Thoracic and lumbar burst fractures with minimal instability and no associated neurological deficit may be effectively managed by the nonoperative means. However, patients with unstable burst fractures including marked retropulsion of bone fragments causing exceeding 50% canal encroachment, severe vertebral collapse more than 50%, local kyphotic angle more than 20° and/or neurologic deficits can benefit from surgical management. 2 The surgical goals in such unstable cases include adequate decompression of the spinal canal, restoration of spinal realignment and reconstructive stabilization of the thoracic or lumbar spine. 3
There is also no consensus on the ideal surgical treatment strategy for severe thoracic and lumbar burst fractures. Suggested surgical options include an anterior approach, a posterior approach, or combined anterior-posterior surgery.4-6 The advantages and disadvantages of each surgical technique and approach should be carefully considered. An anterior approach can provide direct decompression of the spinal canal that could potentially yield better neurological outcomes. 7 However, the anterior approach is associated with a longer operative time, greater blood loss and potential injury to the great vessels.4,7 Moreover, realignment of the kyphotic spine may be difficult with this anterior approach. 2 For such severe thoracic or lumbar burst fractures, another surgical procedure is a traditional posterior vertebral column resection (PVCR) with circumferential reconstruction as previously described.8-17 The benefit of the PVCR technique is that it allows complete decompression of the spinal canal and circumferential reconstructive stabilization from a single posterior-only approach which is more familiar to the majority of spine surgeons. However, this PVCR technique may require total laminectomy, bilateral pediculectomy and subtotal corpectomy followed by anterior column reconstruction via a mesh cage or artificial vertebral body, which is technical-demanding and can be associated with an excessive blood loss and a high complication rate.8-17 In addition, refinements of this traditional procedure can make this challenging procedure safer and more effective. There is limited information in the literature about posterior-only unilateral transpedicular corpectomy (PUTC) technique with circumferential reconstructive stabilization for the treatment of severe thoracic and lumbar burst fractures. Therefore, the aim of this study is to evaluate the clinical, neurological, and radiological outcomes of PUTC technique for the management of such severe complete burst fractures of the thoracic and lumbar spine.
Patients and Methods
Study Population
Patients with severe thoracic and lumbar complete burst fractures, characterized by the involvement of both endplates 18 and thoracolumbar injury score such as a Load Sharing Classification (LSC) point 7 or greater, 19 the Thoracolumbar AO Spine Injury Score (TL AOSIS) 9 or more, 18 and vertebral body spread exceeding 62.7%, 20 were retrospectively collected at the department of spinal surgery in our hospital through January 2019 and June 2024. Surgical indications for this PUTC surgery were complete burst fractures (AOSpine type A4) with severe vertebral body comminution and fragment displacement. The inclusion criteria were as follows: (1) a single unstable complete burst fracture (A4), or combined with a posterior ligamentous complex injury (B) or a translational injury (C) using AOSpine classification system 18 ; (2) a fracture severity score 7 or greater using the load sharing classification (LSC) 19 ; (3) vertebral body spread exceeding 62.7%. 20 The exclusion criteria were: (1) a stable burst fracture, or incomplete burst fracture (A3); (2) a LSC point 6 or less, or a TL AOSIS of 9 or less; (3) vertebral body spread less than 62.7%; (4) skeletal immaturity, an insufficiency fracture. In each case, X-rays and three-dimensional CT were scanned through the affected level to show fracture morphology, vertebral comminution and fragment displacement and canal encroachment. MRI was done before surgery to assess the integrity of posterior ligamentous complex (PLC) and abnormal intramedullary cord signaling. These criteria were suitable to 16 patients, and the medical records, radiographic images and neurologic status determined by the American Spinal Injury Association (ASIA) Impairment Scale, 21 were accessible for all. Intraoperative data including estimated blood loss, operative time and intraoperative findings such as dural tear were noted. The average follow-up was 25.6 months (range 12-42 months). All patients were included based on written informed consent. Institutional review board approval and patient informed consent to participate in this study were obtained (IRB approval number 2022902).
Surgical Technique
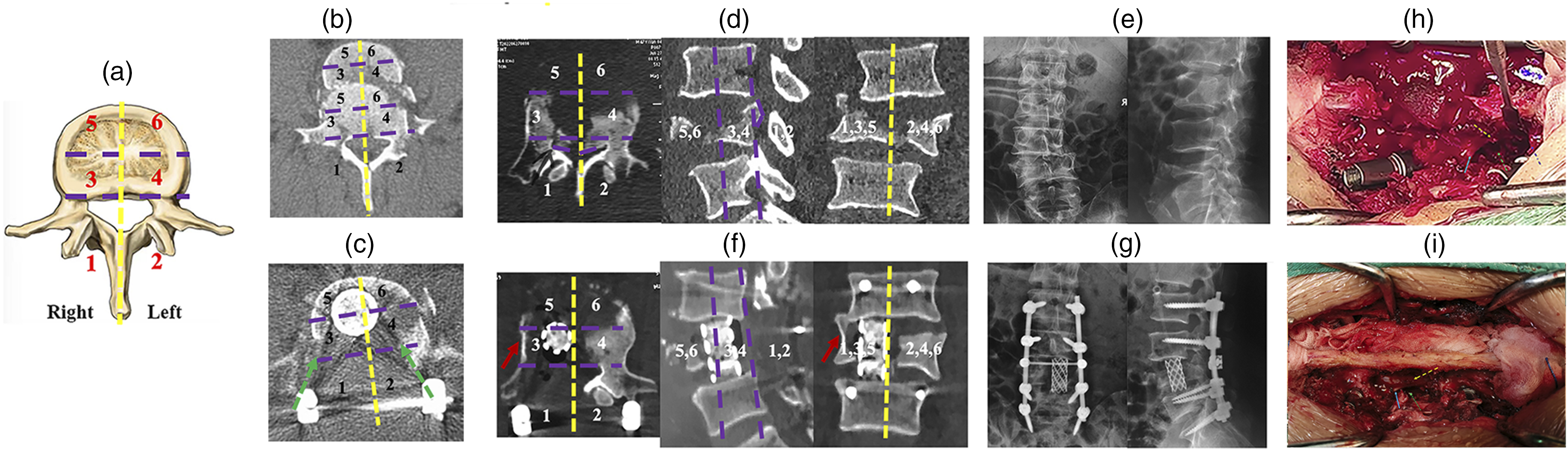
All operations were performed by the senior author (C. C) as shown in Figure 1. Under general anesthesia, a posterior midline incision was made and the posterior elements were subperiosteally exposed. All pedicle screws were placed using the free hand technique at least 2 levels cephalad and caudal to the fracture to minimize the length of the fusion. A shorter pedicle screw construct such as one level cephalad and caudal to the fracture (Short segment pedicle fixation, SSPF) was used in two patients (Case 14, 15) with severe lumbar complete burst fractures (A4) in this series. In this study, SSPF was defined as fixation extending not more than 1 level proximal and distal to fractured vertebra. Any fixation extending beyond this was considered as long segment pedicle fixation (LSPF). In cases where severe osteoporosis (T-score < −3.0) on DEXA (dual-energy X-ray absorptiometry) or quantitative CT scan (QCT <80 HU) or with additional compression fractures adjacent to the burst fracture, instrumentation was performed 3 levels above and below the main fracture. Then, the temporary titanium rod was placed contralateral to the side to maintain alignment and prevent translation before performing pediculectomy and corpectomy via a unilateral transpedicular corridor. A unilateral semi-laminectomy and facetectomy were unilaterally drilled or rongeured out, exposing the relevant disc space, pedicle and the nerve roots. A unilateral pediculectomy was subsequently drilled, and the corpectomy through a unilateral transpedicular corridor in a piecemeal fashion gradually was performed using a high-speed drill, large curettes and Kerrison. To achieve sufficient decompression of the spinal canal and ventral column reconstruction, the proposed concept of six spinal zones can guide the optimal corpectomy via a unilateral transpedicular corridor as shown in Figure 2. Briefly, the middle zone 3 on the right resected side and the small portion of middle zone 4 on the contralateral left side including retropulsed bony fragments can be resected while preserving both anterior zones 5, 6 and the contralateral most portion of middle zone 4, keeping a thin shell of bony vertebral wall beneath the dural tube that protected the neural elements as shown in Figure 2F. Next, discectomies both above and below were performed using curettes. In the process of resection of the fractured vertebra and disc, the lateral cortex of the fractured vertebra and the corresponding rib in thoracic vertebra was preserved to prevent injury to segmental vessels and pleura, respectively (Figures 2F and 4D). The last step will be the posterior vertebral wall, the portion of retropulsed bony fragments just ventral to the cord, which was gently removed with a posterior wall punch. Ventral column reconstruction was performed by insertion of a nonexpendable titanium mesh packed with autograft and allograft bone. For safe insertion of a mesh between the neural elements parallel to the exiting nerve roots, the nerve root was sufficiently mobilized. Lateral and anteroposterior fluoroscopy were used to confirm mesh positioning as shown in Figure 1D and E. After the mesh was placed satisfactorily, posterior compression was applied across the pedicle screw fixation so that the mesh fit snugly and remained in contact with the endplates on either side. The posterior bony elements were then decorticated, and the autograft and allograft were placed over these bony elements. The wound was thoroughly washed with saline, and hemostasis was then achieved. After bone graft, the incision was closed in the standard fashion layer by layer. Surgical procedure of posterior unilateral transpedicular corpectomy (PUTC) technique with a limited laminotomy (ALL). (A) Diagram showing technical aspects of posterior unilateral transpedicular corpectomy (PUTC) technique with a limited laminotomy (ALL) included a unilateral semi-laminectomy and facetectomy, pediculectomy, corpectomy via a unilateral transpedicular corridor, discectomies, removal of posterior wall of the fractured vertebral body, and a medial half of laminotomy and resection of the root of spinous process followed by a titanium mesh cage placement. (B-E) The intraoperative fluoroscopic films in the PUTC technique guided the optimal corpectomy. Four neural probes were used to detect the resection extent of corpectomy including the inferior and superior endplate of the adjacent vertebra above and below the fractured vertebra, and the resection depth at the fluoroscopic lateral film (B), and the one neural probe to detect the contralateral resection extent showing that the neural probe surpassed the midline and reached the contralateral vertebral column at the fluoroscopic anteroposterior film (C). A titanium mesh cage with autogenous and allograft bone inside was inserted into the ventral column through a unilateral transpedicular corridor at the fluoroscopic lateral (D) and anteroposterior films (E). (F) Intraoperative photograph of this PUTC technique with a limited laminotomy (ALL) preserved all lumbar nerve elements such as the nerve root (the blue arrow), the dural sac (the yellow dotted arrow), the unilateral transpedicular corridor (the green dotted arrow), and the posterior tension band including spinous process, interspinal ligament, supraspinal ligament, and the contralateral pedicle, lamina, par interarticularis and facet joint. The proposed concept of six spinal zones in the thoracic or lumbar spine can guide the optimal resection of 2-3 of 6 spinal zones during the PUTC technique. (A) Anatomic description of six spinal zones in the transverse section of thoracic or lumbar spine was characterized by the vertical midline of the vertebral body along the spinous process, the posterior wall line of the vertebral body and the horizontal midline of the vertebral body. The posterior zone (1, 2), middle zone (3, 4) and anterior zone (5, 6) were defined by the posterior elements such as pedicle, laminae, par interarticularis, facet joints and spinous processes, the posterior half portion of the vertebral body including fractured bone fragments and the anterior half portion of the vertebral body, respectively. (B and C) The traditional posterior vertebral column resection (PVCR) with a massive resection of the fractured vertebral body via the bilateral transpedicular approach. The sagittal translational injury with severe vertebral body comminution was presented in a patient with severe lumbar complete burst fracture (B). In this patient, a wide laminectomy followed by a subtotal resection of the fractured vertebral body (5-6 of 6 spinal zones) was achieved through the bilateral transpedicular approach (the green arrow, C), while preserving a small portion of anterior and middle zones (C). (D-G) The proposed six spinal zones can guide the optimal corpectomy via a unilateral transpedicular corridor to achieve circumferential decompression and ventral column reconstruction. Clinical case example with the involvement of 5-6 spinal zones at the computed tomography (D) and X-rays (E) in Case 8 with severe lumbar complete burst fractures. The optimal resection of 3 zones (the posterior zone and middle zone on the right resected side; the medial half of lamina and a small portion of middle zone on the left side) was performed through a unilateral transpedicular corridor, which preserved the anterior zone on the right resected side (Zone 5), and the contralateral anterior zone (Zone 6) and the most portion of middle zone (Zone 4), and the posterior elements (Zone 2) – pedicle, the lateral half of lamina, pars interarticularis and facet joint (F, G). This PUTC technique with a wide laminectomy (AWL) also preserved the lateral cortex of the fractured vertebral body preventing the damage to segmental vessel (the red arrow, F). (H-I) All lumbar nerves including the lumbar exiting nerve roots were preserved in this PUTC technique. Intraoperative photograph showed the nerve roots (the blue arrow), the dural sac (the yellow dotted arrow) and the unilateral transpedicular corridor (the green dotted arrow) in Case 7 and Case 9 underwent this PUTC technique with a wide laminectomy (AWL), and a limited laminotomy (ALL), respectively.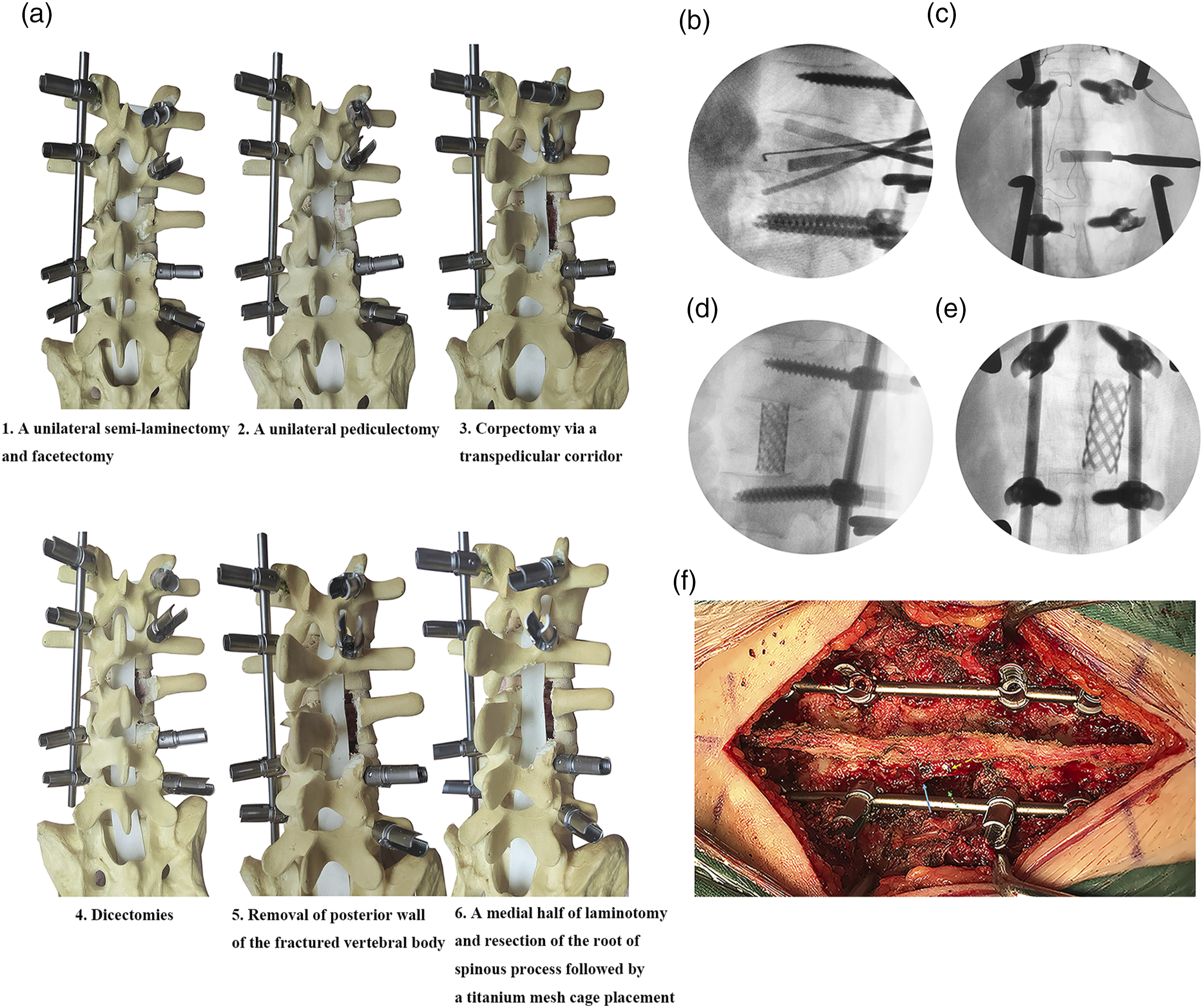
Postoperative Management and Follow-Up
The follow-up radiographs were obtained in the immediate postoperative period, 6 months after surgery and at the most recent follow-up. CT scan was performed six months following surgery to evaluate fusion status (Figure 3H). Radiographic parameters included the collapse of the fractured vertebra that was defined as the percentage of the height of the fractured vertebra with respect to the next adjacent intact vertebra, above and below the fractured vertebra,
22
and local kyphosis via the Cobb angle that was measured above and below the fractured vertebra preoperatively and at the last follow-up.
22
Back pain and functional outcomes were determined on the basis of Visual Analog Scale (VAS) and Oswestry Disability Index score (ODI), respectively.
23
The more bone structures and the lateral cortex of the fractured vertebral column were preserved during this PUTC technique with a wide laminectomy (AWL) to maintain spinal stability and prevent the damage to segmental vessel (Case 5). (A-C) Preoperative X-rays and computed tomography (CT) of 23-year-old female patient with severe L4 complete burst fracture with retro-displacement of L3 to L5 vertebra. (D-F) Postoperative CT and X-rays showed sufficient spinal canal decompression, restoration of height of L4 vertebra and segmental lordosis. (G-H) Postoperative CT image confirmed the maintenance of circumferential reconstruction, lumbar lordosis and the solid fusion after 6 months follow-up.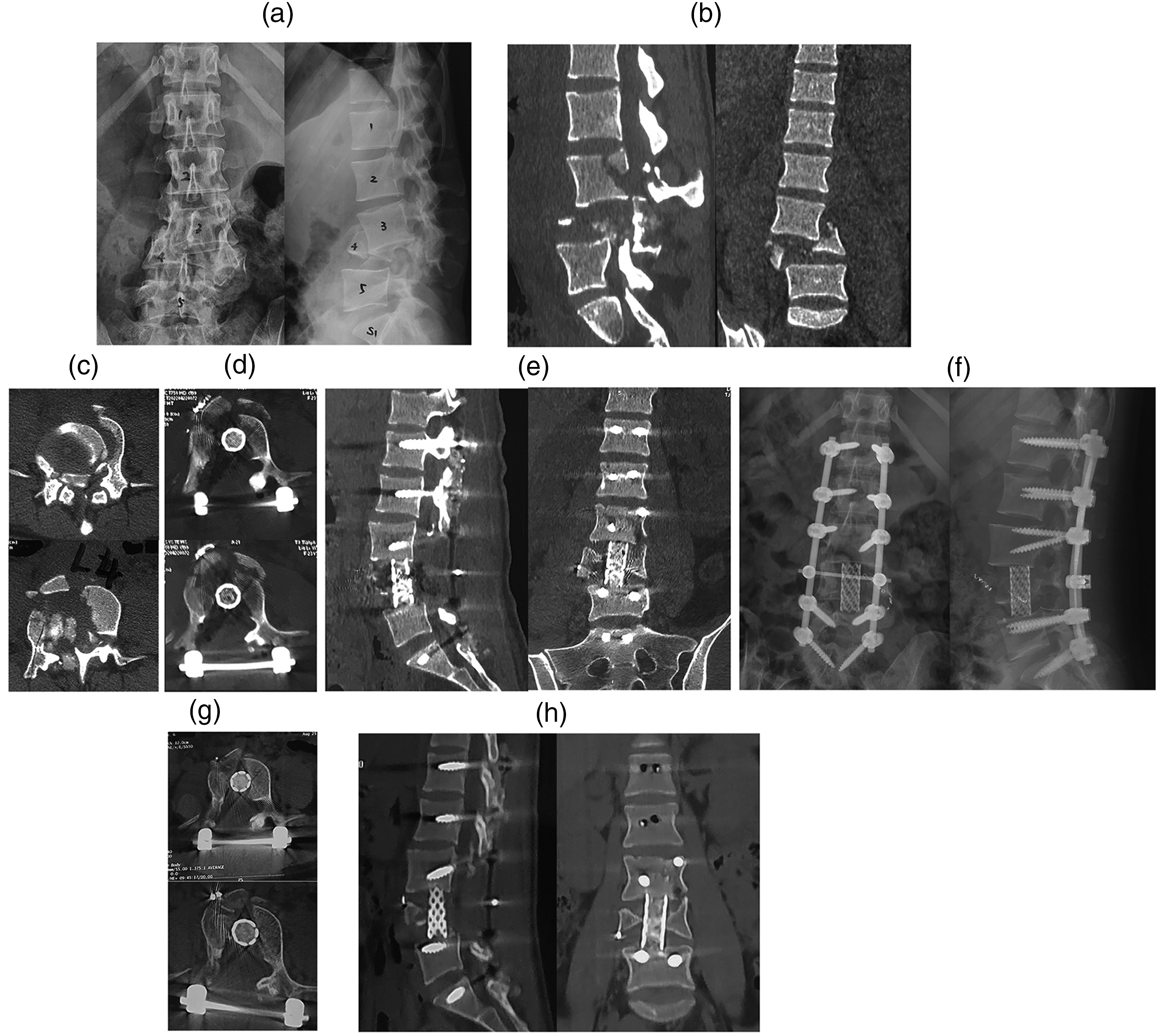
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD). Categorical variables were expressed as the number of cases. Differences were analyzed by Student t test for continuous variables or Pearson’s Chi-square/ Fisher’s exact tests for categorical variables. Statistical analyses were performed by SPSS software (SPSS, Chicago, IL). The level of significance was set at P < 0.05. All reported P values were two-sided.
Results
Clinical Characteristics of the Study Population
Summary of Demographics and Thoracolumbar Injury Score in 16 Patients With Severe Thoracic and Lumbar Complete Burst Factures.
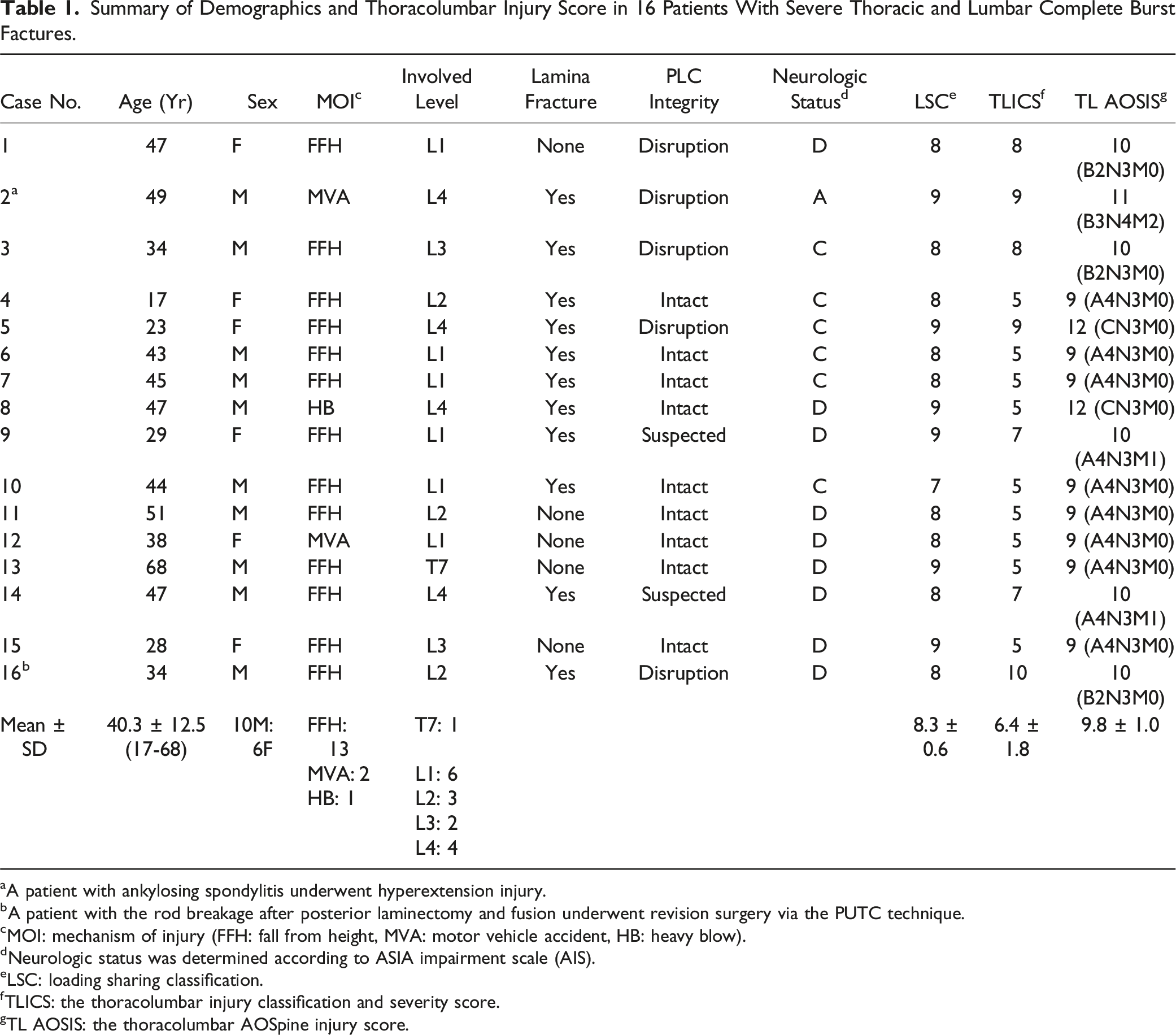
aA patient with ankylosing spondylitis underwent hyperextension injury.
bA patient with the rod breakage after posterior laminectomy and fusion underwent revision surgery via the PUTC technique.
cMOI: mechanism of injury (FFH: fall from height, MVA: motor vehicle accident, HB: heavy blow).
dNeurologic status was determined according to ASIA impairment scale (AIS).
eLSC: loading sharing classification.
fTLICS: the thoracolumbar injury classification and severity score.
TL AOSIS: the thoracolumbar AOSpine injury score.
Surgical Procedures, Perioperative Characteristics and Follow-Up Data in all 16 Patients Undergoing the PUTC Technique With Circumferential Reconstruction.
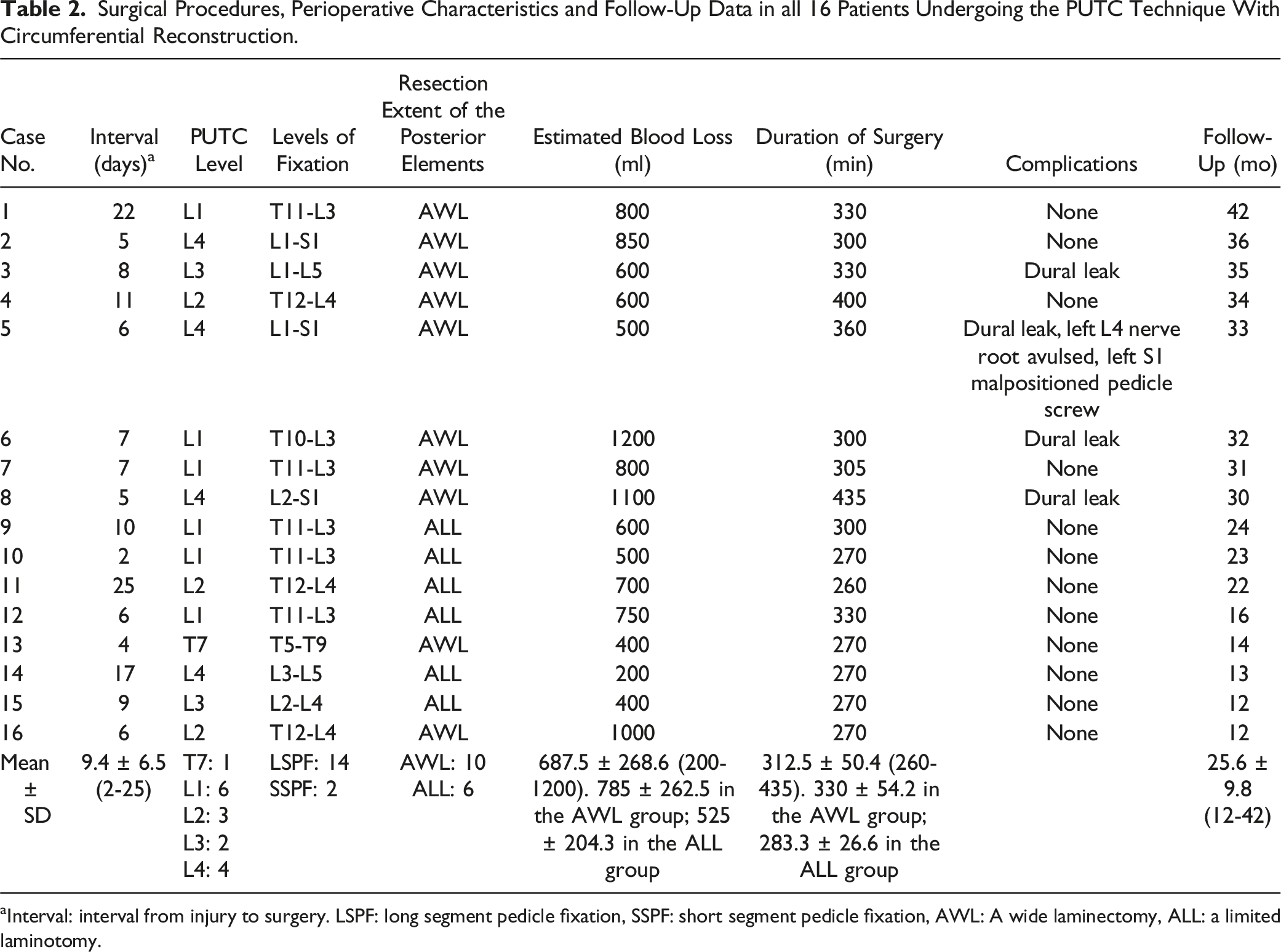
aInterval: interval from injury to surgery. LSPF: long segment pedicle fixation, SSPF: short segment pedicle fixation, AWL: A wide laminectomy, ALL: a limited laminotomy.
Assessment of Radiographic Parameters
Radiographic Data in 16 Patients Undergoing the PUTC Technique With Circumferential Reconstruction.
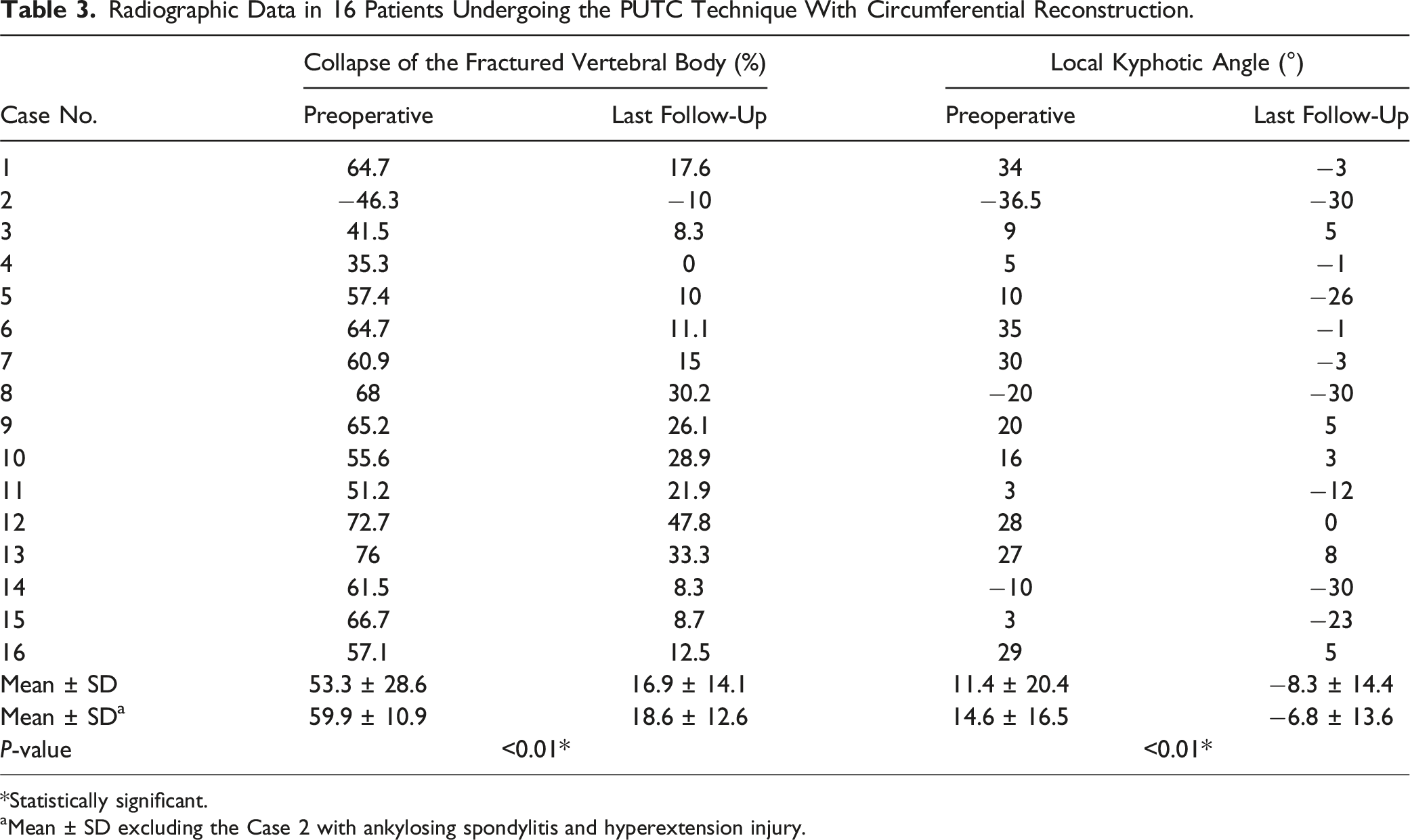
*Statistically significant.
aMean ± SD excluding the Case 2 with ankylosing spondylitis and hyperextension injury.
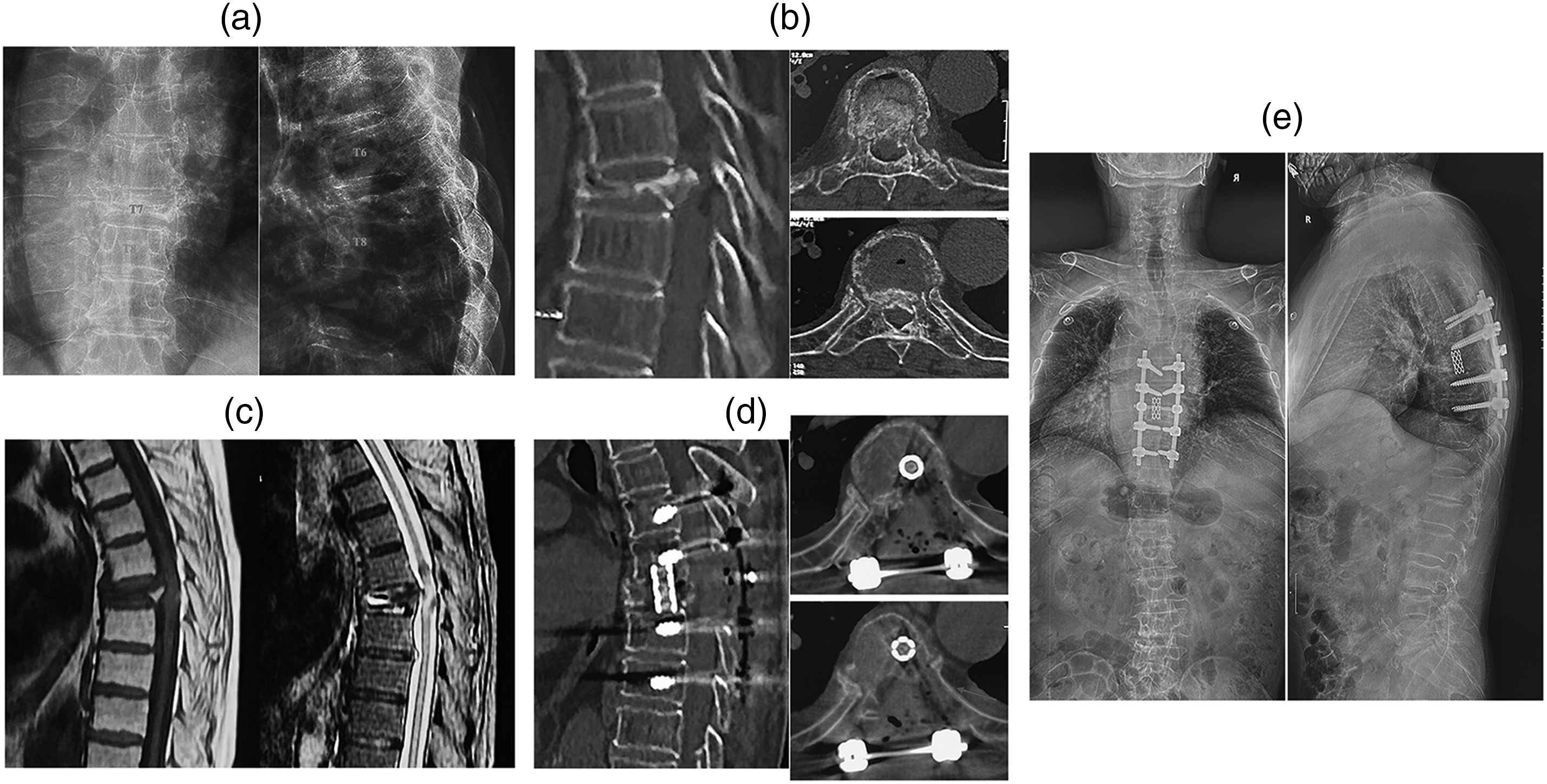
The lateral cortex of the corresponding rib in severe thoracic complete burst fracture was preserved during this PUTC technique with AWL to avoid the damage to pleura (Case 13). (A-C) Preoperative X-rays, computed tomography (CT) and MRI of 68-year-old male patient with severe T7 complete burst fracture. (D) Postoperative CT showed sufficient spinal canal decompression, segmental thoracic alignment and the preservation of the more bone structures and the lateral cortex of the seventh rib (the red arrow) to avoid the damage to pleura. (E) Postoperative anteroposteior and lateral standing radiographs confirmed the maintenance of thoracic alignment and circumferential reconstruction after 14 months follow-up.
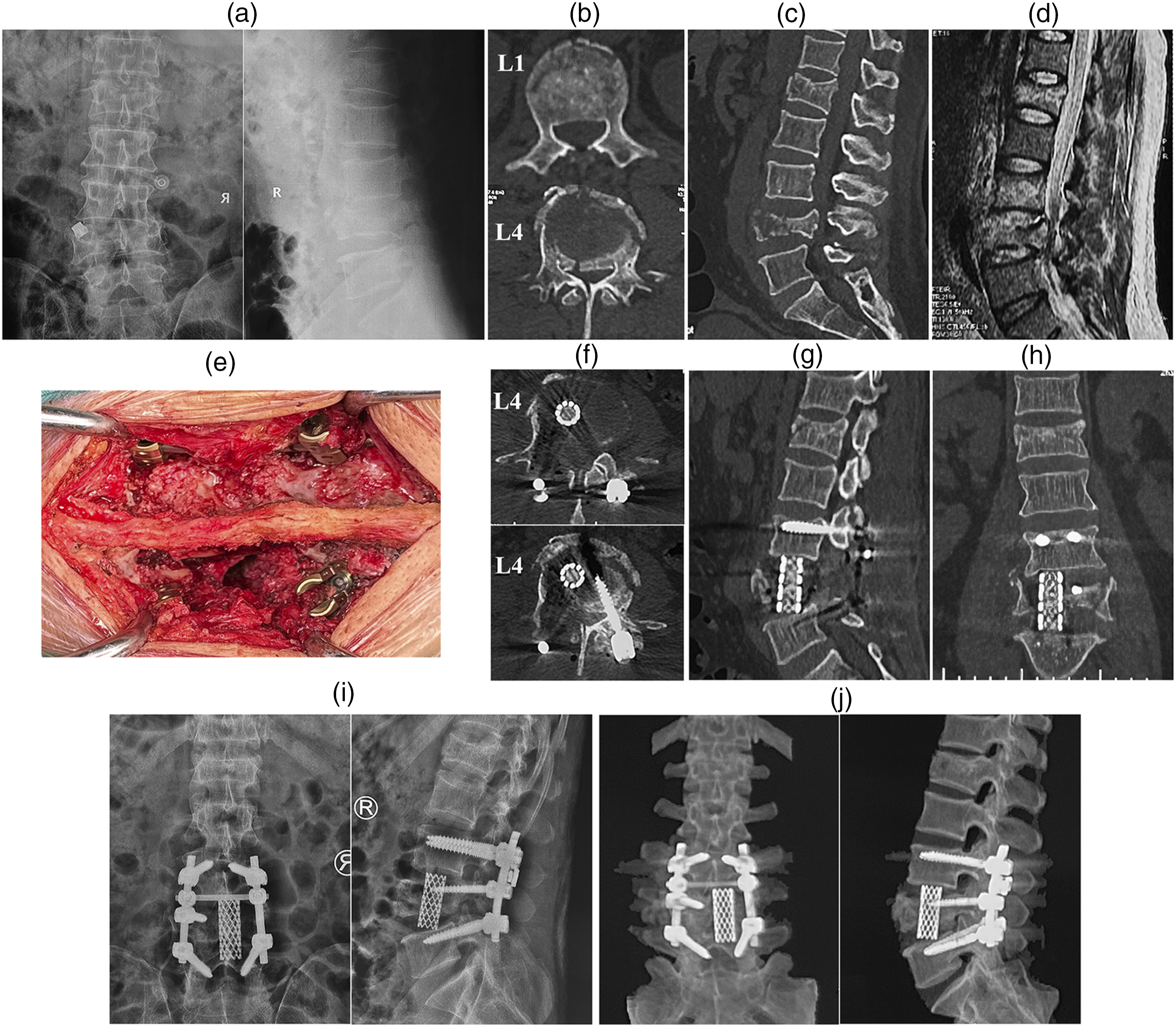
The posterior tension band was preserved in this PUTC technique with ALL to maintain spinal stability (Case 14). (A-D) Preoperative X-rays, computed tomography (CT) and MRI of 47-year-old male patient with severe L4 complete burst fracture and mild L1 incomplete burst fracture. L1 incomplete burst fracture was conservatively managed, and short-segment pedicle-rod system and intermediate screw stabilization with L4 corpectomy were successfully accomplished while preserving the posterior tension band (E). (F-I), Postoperative CT and X-rays showed sufficient spinal canal decompression, segmental lumbar lordosis and ventral column reconstruction by a nonexpendable titanium mesh cage. (J) Postoperative CT image confirmed the solid union and circumferential reconstruction after 13 months follow-up.
Neurologic Recovery and Clinical Functions
Neurological Function and Clinical Outcomes According to VAS and ODI.
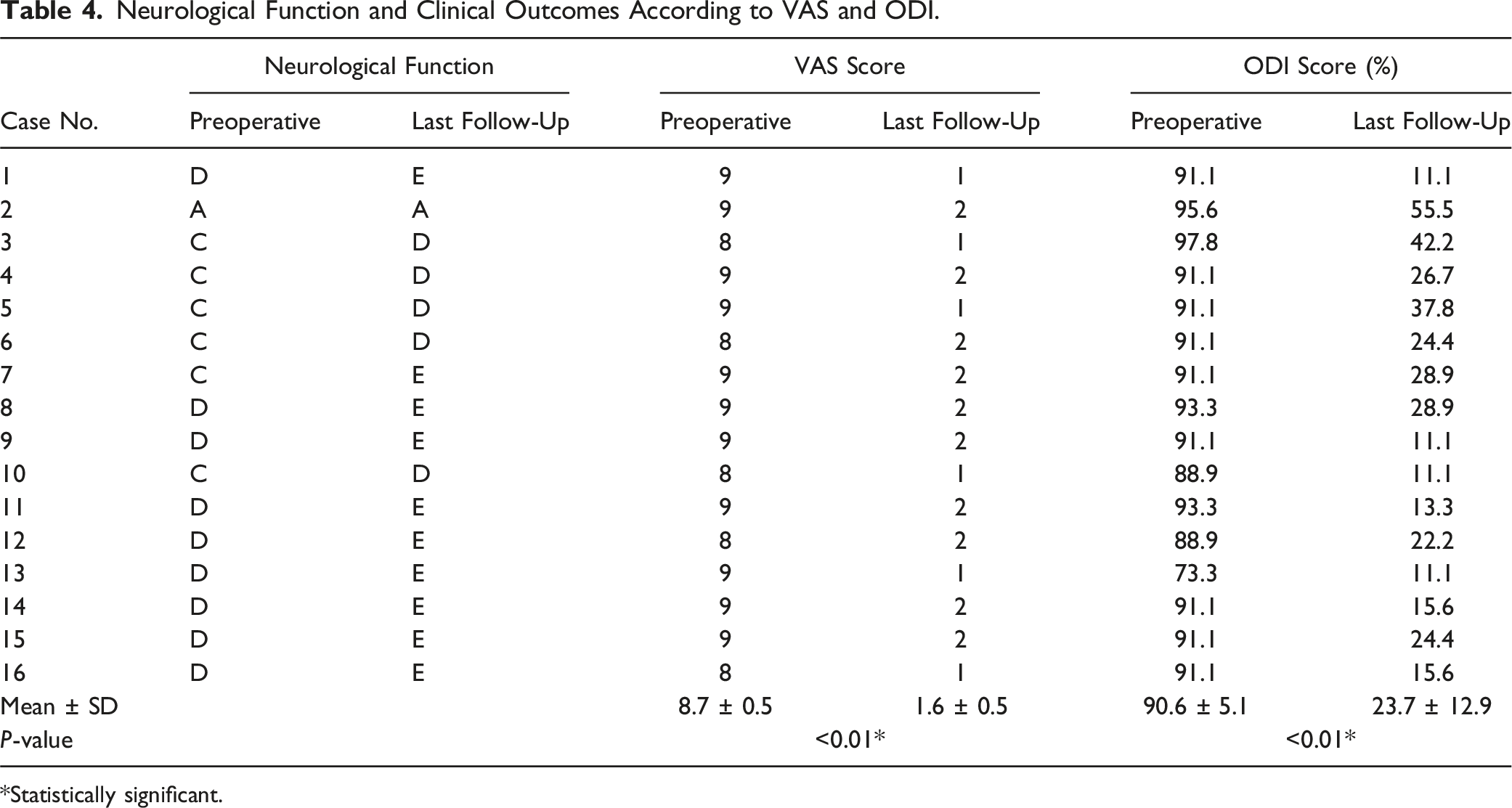
*Statistically significant.
Surgery-Related Complications
Comparison With the Previously Published Data of the Traditional PVCR Procedure and This PUTC Technique in the Treatment of Unstable Thoracic or Lumbar Burst Fractures.
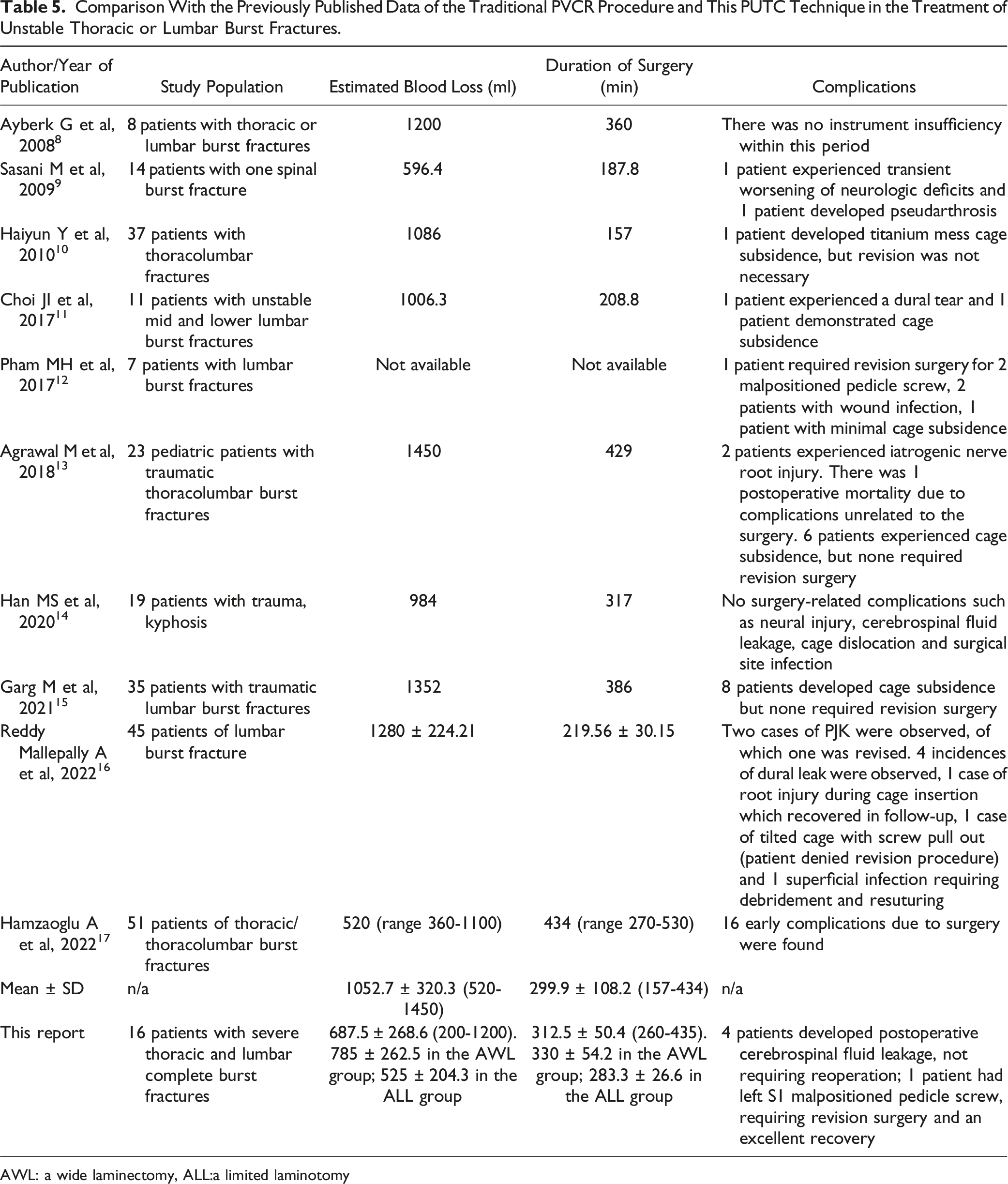
AWL: a wide laminectomy, ALL:a limited laminotomy
Discussion
Much debate exists over anterior-only, posterior-only vs combined anterior-posterior approach for patients with severe thoracic and lumbar burst fractures.4-6 Recently, several authors have demonstrated that the traditional procedure of posterior vertebral column resection (PVCR) has several advantages over the combined approaches such as less estimated blood loss and lower complications. 7 However, this traditional PVCR technique requiring extensive resection including total laminectomy, bilateral pediculectomy and subtotal corpectomy via the bilateral transpedicular approach was associated with a high trauma, an overall estimated blood loss of 1052.7 mL and a high complication rate as shown in Table 5,8-17 which may be attributed to a massive amount or subtotal resection of the fractured vertebral body and a wide resection of the posterior elements such as spinal processes, laminar and interarticular joint as shown in Figure 2B and C. Thus, to reduce surgery-related complications, the optimal resection of the fractured vertebral body or the preservation of the posterior elements or both in the premise of sufficient spinal canal decompression and ventral column reconstruction can be an ideal treatment strategy for severe thoracic and lumbar complete burst fractures.
To better execute the optimal resection of the fractured vertebral body (Zone 3-6) or the preservation of the posterior elements (Zone 1 and 2) during this PUTC technique, we initially introduce the concept of spinal zone in the thoracic or lumbar spine as posterior zone (1, 2), middle zone (3, 4), and anterior zone (5, 6) as shown in Figure 2A. As such, our proposed PUTC technique can be approached via a unilateral transpedicular corridor with the optimal resection of 2-3 spinal zones including the posterior and middle zone on the resected side, and the contralateral small portion of middle zone (Figure 2F), wherein the subtotal resection of 5-6 spinal zones were required in our previous traditional PVCR procedure (Figure 2C). Both anterior zones, the contralateral most portion of middle zone and posterior zone are preserved (Figure 2F), which can better maintain the spinal stabilization and confer robust posterolateral fusion. In addition, we also preserve the lateral cortex of the fractured lumbar spine and the corresponding rib in the fractured thoracic spine (Figures 2F and 4D), which can prevent the damage to the segmental vessels or pleura, respectively. Notably, the traditional PVCR procedure requires a wide laminectomy (AWL) as shown in Figure 2H, exposing the spinal canal for subtotal corpectomy, which will cause severe damage to spine stability and increase surgical trauma. In our retrospective study, a wide laminectomy (AWL) or a limited laminotomy (ALL) was firstly performed, depending on whether posterior column fractures caused spinal canal encroachment. For requiring ligamentotaxis and a sufficient reduction for a translational injury, the use of AO-USS fracture system and the double-threaded Schanz screws were quite helpful at the strategic positions based upon our previous clinical report.24,25 10 patients underwent AWL (Figure 2H) while 6 underwent a limited laminotomy (ALL) as shown in Figure 2I. The estimated blood loss (525 ± 204.3 mL) and operative time (283.3 ± 26.6 min) in patients with the ALL group were less than those in patients with the AWL group (Table 2). Furthermore, a less complication including dural tear and leakage was noted in patients with the ALL group (Table 2). These results supported that the ALL group had several advantages over the AWL group. However, when neural compression is attributed to the laminar fractures or a translational injury, AWL should be peformed to achieve sufficient decompression of spinal canal. Thus, our results have illustrated this PUTC technique with ALL can preserve the posterior tension band (Figure 5) and improve clinical and radiographic outcomes, with a less incidence of surgery-related complications than the AWL group.
Indications of supplemental ventral column reconstruction after short segment pedicle fixation (SSPF) for severe vertebral comminution are controversial. A LSC score of 7 or greater indicates severe vertebral comminution and fragment displacement, requiring ventral column reconstruction. 19 However, severe authors have documented that the relevance of LSC in the management of unstable burst fractures may be questionable.24,26 To better predict the posterior-only construct failure, De Iure et al have presented that vertebral body spread more than 62.7% require supplementary anterior supports. 20 In this study, we select this PUTC technique with circumferential reconstruction rather than vertebroplasty plus SSPF as our previously reported, 24 because complete burst fractures with severe vertebral comminution and spread exceeding 62.7% cause loss of anterior support and require ventral column reconstruction. After the optimal resection of 2-3 spinal zones, we reconstruct ventral column via a titanium mesh cage of a diameter of 14-16 mm filled with local autograft and allograft. Notably, placement of a mesh cage in the lumbar spine is usually difficult from the posterior approach owing to the need to navigate around the lumbar nerve roots. Our experience reveals that wide dissection and thorough mobilization of the lumbar nerve roots create a corridor for cage insertion, and cage placement requires oblique insertion. In this circumstance, all lumbar nerve roots were preserved in all patients (Figures 1F and 2H and I), and none of patients underwent neurological injury during cage insertion. Although a small fusion bed and possible implant failure could be drawbacks to the use of smaller cage compared to lumbar endplate footprint, we preserved the more bone structures and placed bone chips on the contralateral posterior zone (Figures 2F-G, 3–5). The lack of fusion failure or cage subsidence in our series demonstrates the relatively excellent stability and safety of the construct. In addition, in the SSPF group as shown in Figure 5F, we used the intermediate screws to further enforce the spinal stabilization after a mesh cage was successfully inserted. Similar to the previous report, 16 our overall clinical and radiographic results are promising, avoiding the need for anterior approach. However, for a translational injury, multiple consecutive vertebral fractures or severe osteoporosis that the BMD T-score is below −3.0, we select LSPF in these 14 patients.
Our proposed PUTC technique demonstrates the following advantages over the traditional PVCR technique. Above all, the optimal resection in this PUTC technique limited to 2-3 spinal zones vs 5-6 zones in the traditional PVCR, preserving the contralateral pedicle, the lateral half of lamina, pars interarticularis and facet joint (Figure 2F). The mean blood loss (685.7 ± 263.4 mL) decreased by 35% compared to PVCR (1052.7 mL), with lower complication rates (Table 5). In addition, the ALL group preserving the posterior elements (525 ± 204.3 mL; Figure 5) showed 33.1% less blood loss than the wide laminectomy (AWL) group (785 ± 262.5 mL) and lower dural tear rates, underscoring the importance of preserving the posterior tension band. The less resection extent, less blood loss, lower complication rates and the more preservation of bone structures demonstrate minimally invasive profile and enhanced intraoperative safety of the PUTC technique. Furthermore, neurological improvement in this PUTC technique was significantly observed in 15 patients with incomplete spinal cord injury, with VAS scores decreasing from 8.7 to 1.6, outperforming the literature-reported range of 1-3 points. 16 Oblique titanium mesh cage placement (14-16 mm diameter) combined with pedicle fixation can restore the fractured vertebral body height without cage subsidence (Figures 2–5). Our technique can achieve solid biomechanical stability via local bone grafting and intermediate screw augmentation in the short-segment pedicle fixation (SSPF) group, eliminating the need for combined anterior-posterior approaches. These satisfactory results support functional recovery and biomechanical superiority of the PUTC technique. Last but not least, our PUTC technique can be applicable to thoracic and lumbar complete burst fractures with severe comminuted fractures (LSC ≥7; TL AOSIS≥9) and vertebral body spread >62.7%, but its contraindications of the PUTC technique with the SSPF group are severe osteoporosis (T-score < −3.0) or multilevel fractures. However, because the single-center small sample size (n = 16) and the average 25.6 months follow-up may limit generalizability and underestimate late complications (eg, adjacent segment degeneration), further investigation of a larger patient population and the long-term efficacy should be necessary. Prospective, randomized studies may be required to adequately investigate these issues.
Conclusions
In conclusion, this current study has demonstrated that severe thoracic and lumbar complete burst fractures with a LSC point 7 or greater and a TL AOSIS score 9 or more can be circumferentially decompressed and reconstructed using this proposed PUTC technique with the optimal corpectomy and ventral column reconstruction. This PUTC surgery can significantly improve clinical and radiographic outcomes and eliminate the need of an anterior approach in patients with such severe complete burst fractures of the thoracic and lumbar spine, offering remarkable advantages over the traditional PVCR procedure. However, larger studies are warranted to conclusively establish this promising results.
Footnotes
Acknowledgments
This work was partly supported by grants from TianJin Youth Medicine Talents Plan. All experiments and manuscript were designed and performed by our authors, and the funder has not been involved in these experiments and manuscript preparation and submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.