
Abstract
Study design
Prospective analysis of retrospective data.
Objectives
To analyse the clinical and radiological outcomes of thoracic and thoracolumbar TB kyphosis by a posterior-only approach using kyphosis classification.
Methods
Patients with thoracic and thoracolumbar spinal TB who underwent posterior-only surgical correction for kyphotic deformity >30° were categorized into Group: A (Active TB) and Group B (Healed TB). Demographic, clinical and radiological data were collected, and kyphotic deformity was classified according to Rajasekaran classification.
Results
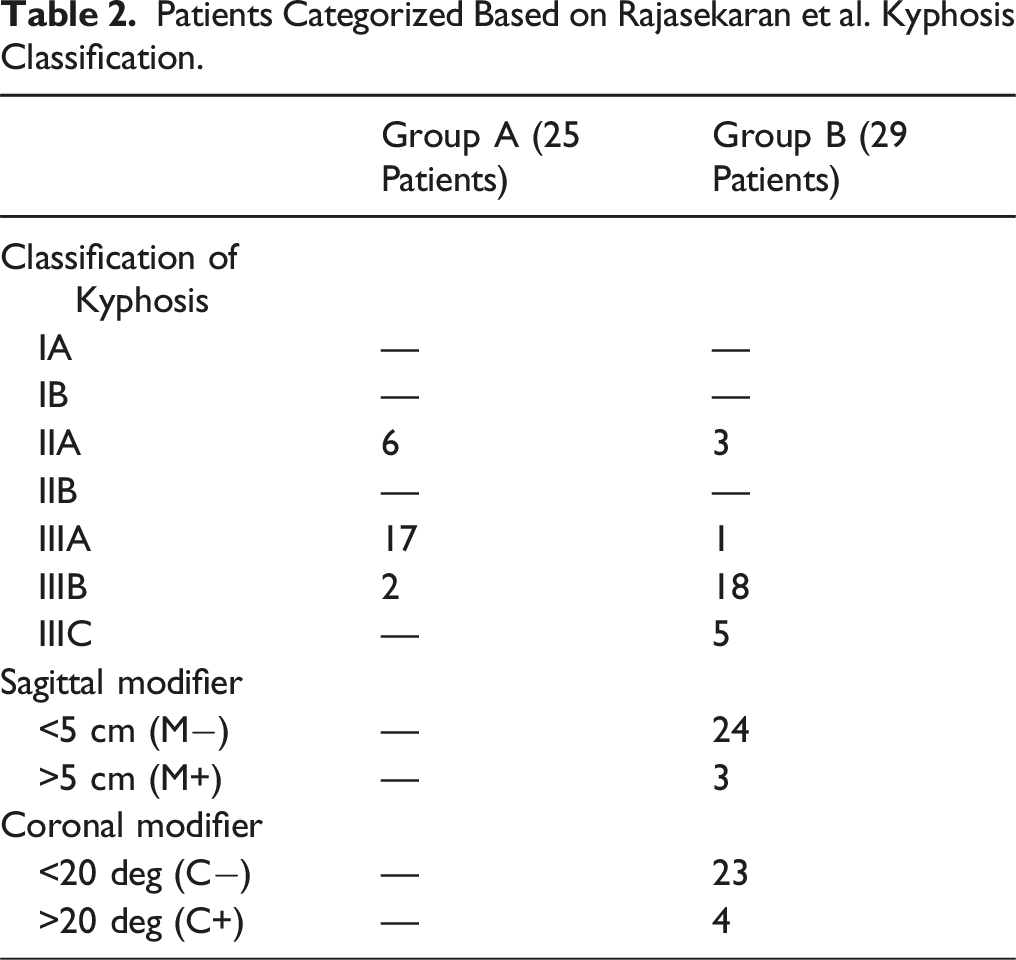
52 patients with a minimum 2-year follow-up were included. Group A included 25 patients with mean preop kyphosis of 39.5° (31.2°-53.7°), and Group B included 27 patients with mean preop kyphosis of 85° (44.2°-125.2°). Among 25 patients in Group A, 19 were Type IIIA, and 6 were Type IIA kyphosis. In Group B, 18 patients were Type IIIB, 5 were Type III C, 3 were Type IIA, and 1 was IIIA kyphosis. All patients in group A underwent posterior column shortening by Smith-Peterson Osteotomy, with 14 patients requiring additional anterior column reconstruction. Patients in Group B required Closing-Opening Wedge Osteotomy (18), Halo followed by vertebral column resection (6), disc bone osteotomy (2) and pedicle subtraction osteotomy (1). Mean kyphosis at 2 years follow-up was 20.8° (11.2°-32.8°) in Group A and 53.5° (8.1°- 96.4°) in Group B.
Conclusions
Correction of kyphosis in spinal TB involves completely different strategies in active and healed disease. Hence, a posterior-only treatment approach using Rajasekaran’s kyphosis classification can help surgeons in appropriate decision-making.
Keywords
Introduction
Spine is the most common site of osteoarticular tuberculosis, accounting for 50% of the cases.1,2 Anterior column is affected in about 90% of patients with spinal tuberculosis, and natural healing of the disease results in kyphotic spinal deformity. Progressive kyphosis could result in neurological deficits, mechanical instability, pain, and psychosocial problems. Tuberculous kyphosis can progress during both the active and healed phases of the disease, especially in children. 3 Surgical correction of kyphosis in the active stage involves less extensive procedures and is relatively safer compared to kyphosis in the healed phase. Though there are clear surgical indications for patients with active and healed disease, there are many discrepancies in the literature regarding the surgical correction of kyphotic deformities in these patients.4,5 Our study aims to analyse various surgical procedures performed in our institute for tuberculous kyphosis based on Rajasekaran’s kyphosis classification and propose a treatment approach for the management of kyphotic deformity in thoracic and thoracolumbar spinal TB.
Materials and Methods
Following approval from the institutional review board (IRB No: 2021/09/10) and informed written consent from all participants, we performed a prospective analysis of retrospective data of 52 patients with thoracic and thoracolumbar spinal TB and a deformity of more than 30° who underwent surgical treatment in our institute between 2010- 2019 was performed. Biopsy-proven active tuberculous spondylodiscitis patients who underwent surgery were considered in the active group (Group A). Patients with longstanding deformity following a healed tuberculous lesion and seeking treatment for pain/neurodeficit/respiratory difficulty/cosmesis due to the deformity were included in the healed group (Group B). Only patients with a minimum follow-up of 2 years were included in the study. Kyphosis angle of more than 30° was identified as one of the risk factors for severe progression of deformity in spinal TB, and hence, those patients were included. 6 Data collection was performed using the hospital information system (HIS), operative registry and PACS. This included the patient’s demographic data, radiological data including pre and post-operative radiographs, computed tomography (CT) scan, Magnetic Resonance Imaging (MRI) scan and surgical data. In all patients, level of involvement, number of vertebrae involved and the magnitude of deformity were noted. In healed cases, additional data, including flexibility of the deformity (using dynamic radiographs) and coronal and sagittal balance (using full-length standing radiographs), were also assessed. Pre-, post-operative and follow-up kyphotic angles were calculated in lateral X-rays by the method described by Konstam and Blesovsky. 7 Vertebral body loss (VBL) was calculated by dividing the total vertebral body height into ten equal fractions and measuring the number of fractions lost. In multiple vertebral involvements, the VBL of each vertebra was added up to give the vertebral body loss. 8 Anterior and posterior column integrity was also assessed, and patients were classified according to the Kyphosis Classification proposed by Rajasekaran et al. 9 All the surgeries were performed by three senior surgeons in our institute (SR, APS and RMK). All patients underwent a standard posterior-only approach for the correction of kyphosis deformity. In Group A patients with active lesions, the kyphosis was mobile and hence, a unilateral costotransversectomy from the side of maximum vertebral body collapse was performed to facilitate the insertion of an adequate-sized cage for kyphosis correction. In Group B patients where there was fixed kyphosis, bilateral costotransversectomy was necessary to mobilise and correct the kyphosis.
In group A patients, Antituberculous therapy (ATT) was started after the bacteriological confirmation by gene xpert from tissues obtained during surgery with histological validation. Hence, in cases presenting without any prior intervention, there was no antitubercular therapy prior to surgery. It is now well established that a neo-adjuvant antituberculous therapy is unnecessary in spinal tuberculosis surgery.10,11 In group B patients with healed tuberculosis, antituberculous therapy was not reinitiated unless the tissues obtained during surgery showed suspicion of reactivation in histopathology or gene xpert.
Patients were followed up at 1, 3, 6 and 9 months and 2 years. Loss of correction at follow-up was calculated as the difference between the deformity angle measured at 2 years follow-up and that of immediate postoperative radiograph. Clinical outcomes were assessed using Frankel grading for neurological outcomes and Visual Analogue Score (VAS) for postoperative pain at the final follow-up.
Results
Demographic and Clinical Data
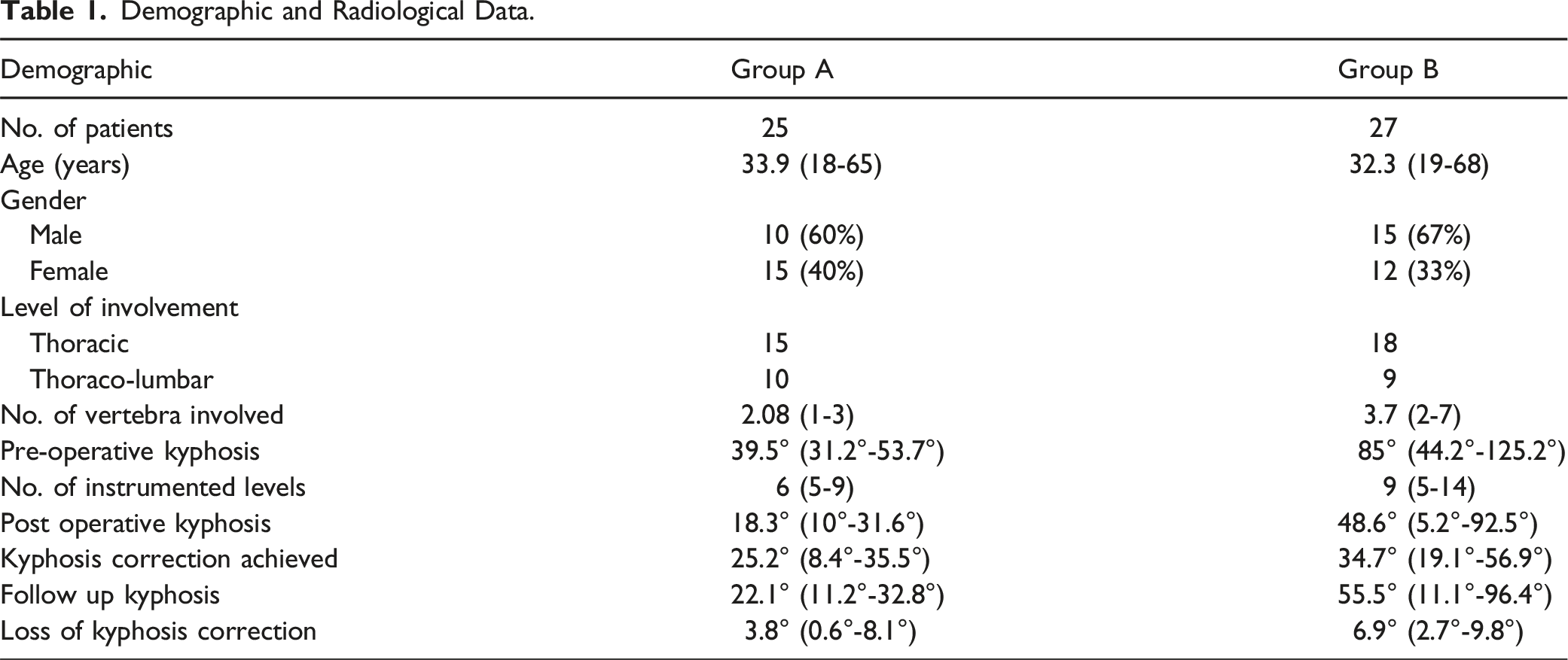
A total of 52 patients with a mean age of 33.08 (10-68) years were included in the study. Group A included 25 patients with active spinal TB. Group B included 27 patients with healed spinal TB. In Group A, of the 25 patients, 10 patients (40%) were males. Pain was the most common presenting symptomatology in all (100%) patients in the group. 16 patients also had neurological involvement (Frankel D: 11 patients, Frankel C: 4 patients and Frankel B: 1 patient). In Group B, of the 27 patients, fifteen (56%) were males. 9 patients presented with neurological involvement (Frankel D: 5 patients, Frankel C: 3 patients and Frankel B: 1 patient), and seven patients presented with cardio-respiratory symptoms. Six patients had back pain and five patients had cosmetic concerns. The mean pre-operative VAS scores in Groups A and B are 6.3 (5-8) and 4.7 (2-6) respectively.
Radiological Data
In Group A, thoracic level and thoracolumbar involvement were seen in 15 (60%) and 10 (40%) patients respectively. Average number of vertebrae involved was 2 (1-3). The mean pre-operative vertebral body loss was 0.8 (0.5-1.8) and the mean pre-operative kyphosis was 39.5° (31.2°-53.7°).
Demographic and Radiological Data.
Kyphosis Classification
Patients Categorized Based on Rajasekaran et al. Kyphosis Classification.
Surgical Data
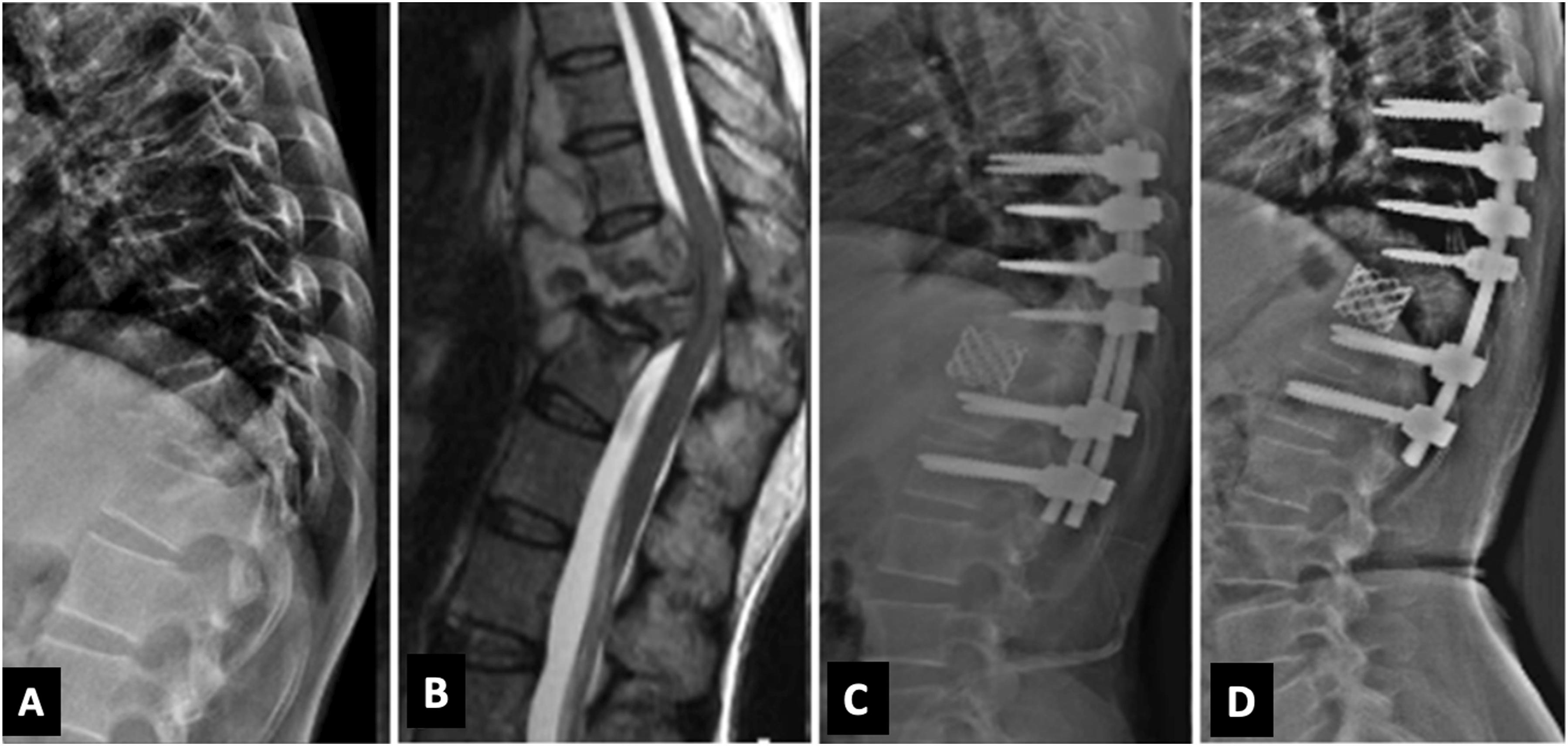
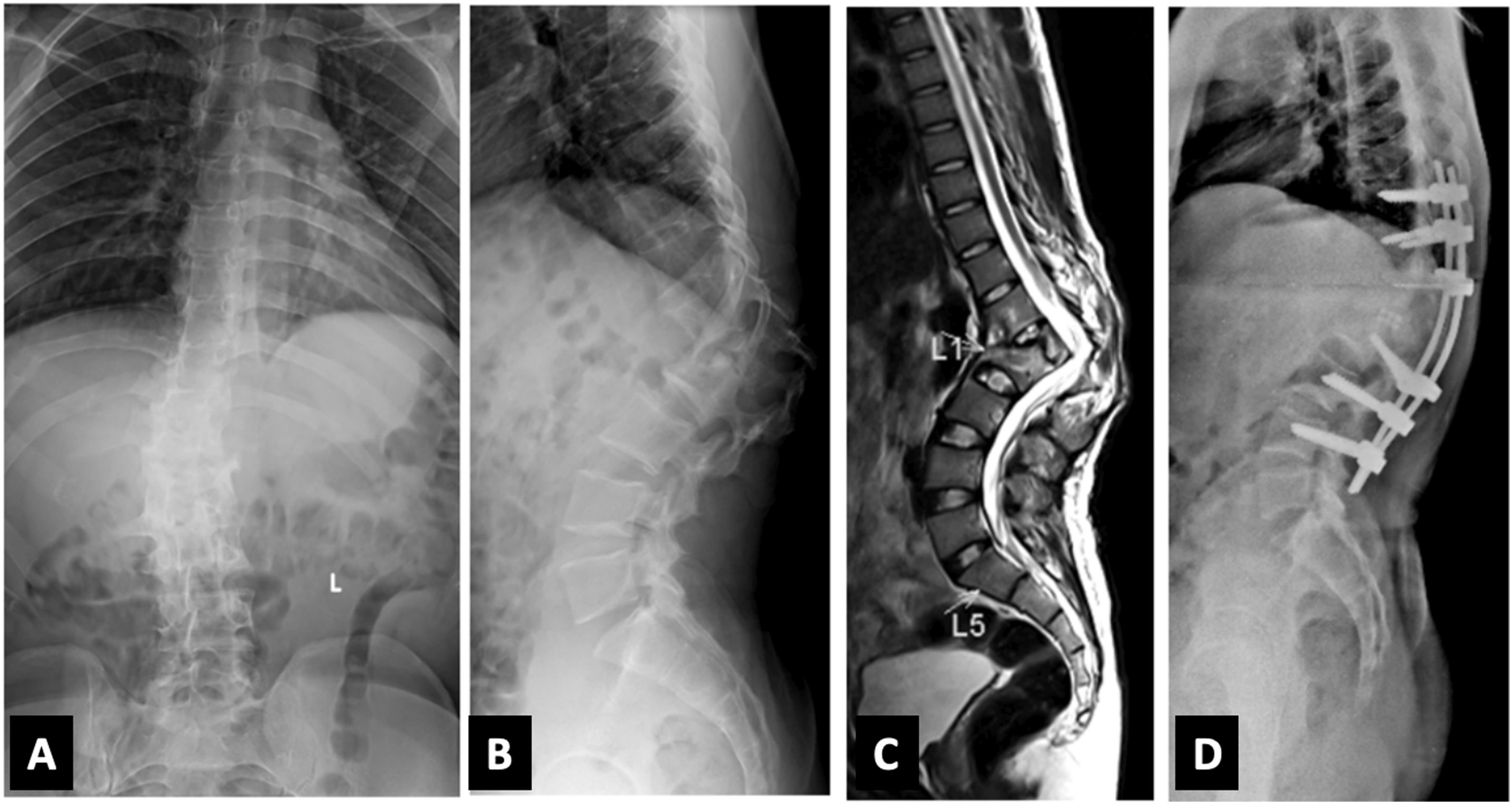
All the patients in our study underwent a posterior-only approach. In Group A, 9 patients (2 patients: Type IIA, 7 patients: IIIA) underwent only instrumented decompression with posterior column shortening (Smith Peterson osteotomy) (Figure 1). Total Vertebral Body loss in these 9 patients was 0.5 to 0.9. In 16 patients (3 patients: Type IIA, 13 patients: IIIA), an additional anterior column reconstruction using a titanium metallic cage was performed (Figure 2). In these 13 patients, 5 patients had a total vertebral body loss >1. The average number of levels instrumented was 6 (5-9). (A) Lateral radiograph of thoracolumbar spine in Group A patient showing kyphosis of 31.2°; (B) Mid Sagittal T2W MRI showing collapse prevertebral and epidural abscess; (C) Sagittal CT cuts showing destruction of the endplate and collapse of the vertebra (D) Lateral postoperative radiograph after posterior column shortening showing good deformity correction with post-op kyphosis of 6.5°. (A) Lateral radiograph of lower thoracic spine in Group A patient showing involvement collapse of T10 and T11 vertebrae; (B) Mid Sagittal T2W MRI showing epidural abscess causing spinal cord compression with prevertebral abscess; (C) Lateral post-operative radiograph showing posterior instrumented stabilisation with anterior column reconstruction; (D) 2 years follow up lateral radiograph showing good implant position with no significant loss of correction.
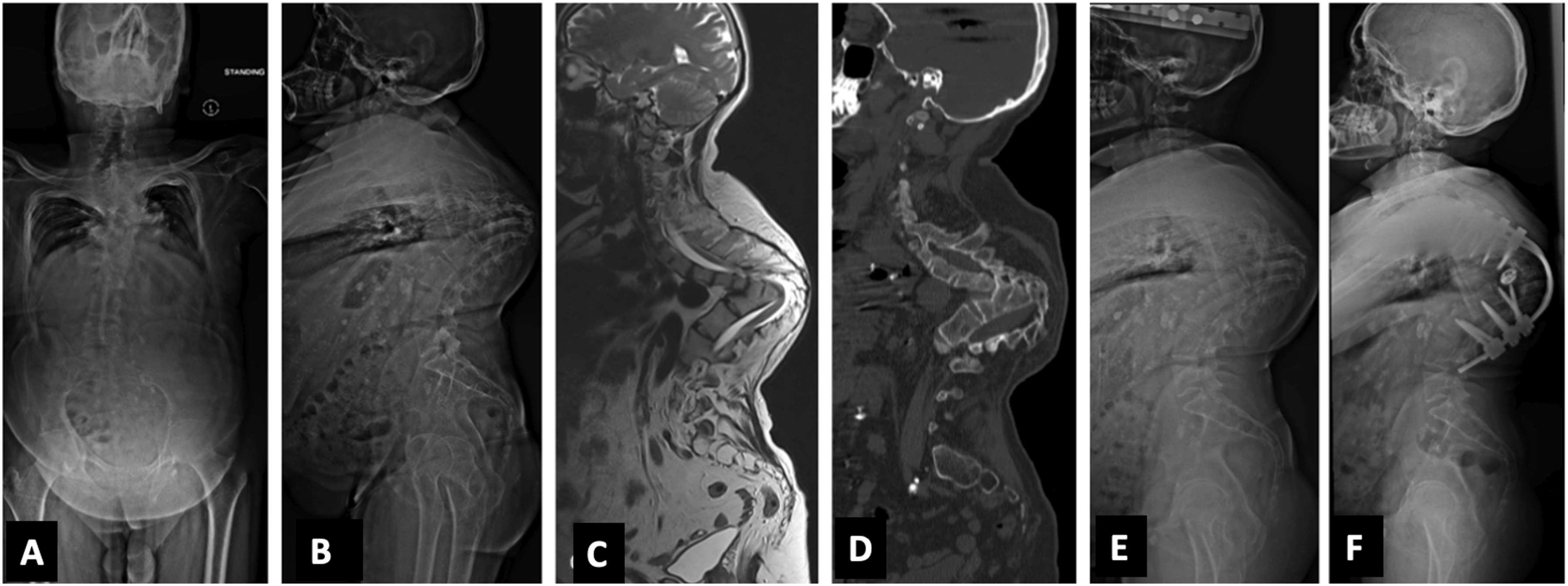
In Group B, the deformities were rigid and not flexible. The average number of levels instrumented in the group was 9 (5-14). Pedicle Subtraction Osteotomy (n = 1) and Disc-Bone osteotomy (n = 2) (Figure 3) were performed on a total of three patients and they were classified as kyphosis Type IIA. Their mean preoperative kyphosis was 50°. The mean kyphosis correction achieved in these patients was 34.7°. Eighteen patients (17 patients: type IIIB, 1 patient: IIIA) underwent Closing-opening wedge osteotomy (COWO) (Figure 4). In patients, with C+ modifier (4 patients), asymmetric osteotomy and wedge resection on the convex side was performed. Mean kyphosis correction of 40.2° (25.1°-59.9°) was achieved with COWO. Six patients (5 patients: type IIIC, 1 patient: IIIB) had a kyphosis of over 100° and, halo gravity traction was applied preoperatively for a mean duration of 4.8 (3-6) weeks and underwent vertebral column resection (multiple vertebrectomy) (Figure 5). Mean kyphosis correction of 49.3°. One of our patients in Group B with thoracic kyphosis (apex at T8-T9) of 95° (type IIIB) had a loss in neuromonitoring signals intra-operatively, during kyphosis correction manoeuvre (COWO) and further deformity correction was not attempted. The surgical treatment in both groups is enumerated in Tables 3 and 4. (A, B) Anteroposterior and lateral radiographs in Group B patient showing kyphosis deformity (59.4°) at the T4-T5 level (Type IIA); (C, D, E) Sagittal CT cuts showing complete anterior column loss with intact posterior column (Type IIA); (F) Postoperative radiograph after Disc- Bone Osteotomy with kyphosis correction, postoperative kyphosis reduced to 23.4°. (A, B) AP and Lateral radiograph in Group B patient showing a lateral translation and focal kyphosis at the T12-L1 level. Both the anterior and posterior columns have failed, resulting in kyphotic deformity (Type IIIB). (C) Sagittal T2W MRI showing stretching of the conus at the level of T12. (D) Postoperative radiograph after COWO showing good kyphosis correction. (A, B) Anteroposterior and lateral radiograph in Group B patient showing healed TB with buckling collapse (Type IIIC) at the thoracic spine with kyphosis of 125.2°. (C) Sagittal T2W whole spine MRI showing stretching of the cord at the level of internal gibbus; (D) Sagittal CT scan images showing completely healed TB with fusion of multiple vertebrae forming a single mass anteriorly; (E) Lateral Postoperative radiograph after 6 weeks of Halo traction; (F) Post-operative radiograph showing reduction in the kyphotic deformity to 92.5°. Type of Surgery in Group a Patients. Type of Osteotomy Performed in Group B Patients.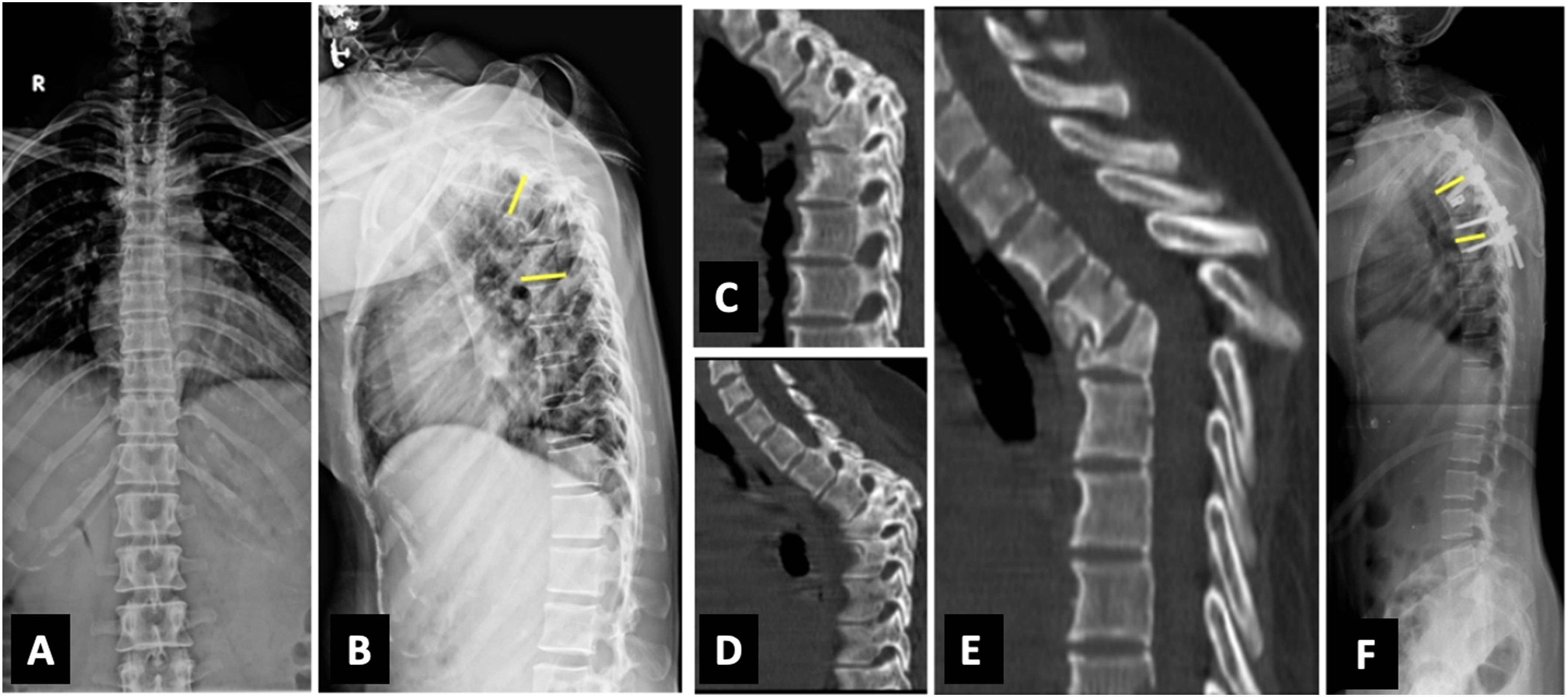


Outcome and Follow-Up Data
The immediate Postoperative kyphosis in Groups A and B was 17.3° (10°-30.9°) and 48.6° (5.2°-92.5°) respectively. Kyphosis Correction achieved in each group was- Group A: 22° (8.4°-35.5°) and Group B: 34.7° (25.1°-59.9°). All our patients had a minimum follow-up of 2 years. The mean follow-up duration was 3.7 (2-6) years. The mean post-operative VAS scores at final follow-up in Groups A and B are 0.6 (0-2) and 2.4 (2-3) respectively. All the patients in Group A had achieved fusion at the final follow-up. Neurology improved (Frankel E) in all 11 patients with deficits. In group B, there was complete neurological recovery (Frankel E) in 4 patients and partial in two patients (Frankel D). The patient with intra-operative neuromonitoring signal change underwent rehabilitation and had only partial recovery of her motor function at the final follow-up (Frankel B to Frankel C). The mean kyphosis at the final follow-up was 20.8° (11.2°-32.8°) and 53.5° (8.1°-96.4°) in Groups A and B respectively. Loss of correction in Groups A and B was 3.2° (0.6°-8.3°) and 6.9° (2.7°-9.8°) respectively. One patient in Group A and three patients in Group B had wound dehiscence, for which resuturing was performed. One of the patients in Group B needed a flap cover for wound breakdown and exposed implant. He also had a rod breakage needing revision at 4 4-month follow-up.
Discussion
Tuberculosis is one of the most common causes of kyphotic deformity in the spine. 12 This is because it is primarily a disease of the anterior column of the spine and healing occurs by collapse of the anterior column. 13 Progression depends on factors like level of involvement, degree of vertebral body loss, the number of vertebral bodies involved, the magnitude of the initial deformity and the age of the patient. Conservatively treated patients have an average increase in deformity of 15°.14,15 However, in about 3%–5% of patients, deformities progress more than 60°. 16 In active disease, destruction of the spinal column by the disease process, mechanical effects of the granulation tissue/ abscess and deformity are the cause of symptoms. In healed disease with severe kyphosis, the lever arm of the centre of gravity is shifted anteriorly with respect to the affected vertebral segment, resulting in failure of the anterior column in compression and the posterior column in tension. This causes pain, spinal cord compression, and reduction in thoracic volume, causing cardiopulmonary dysfunction, costopelvic impingement and cosmetic concerns. In our study, pain was present in all patients in the active phase (Group A) and 16 patients had neurological involvement. In Group B, neurological deficit and cardiopulmonary symptoms were the common presenting symptoms in nine and six patients respectively.
The surgical approaches for TB kyphosis include anterior only, posterior only, and combined anterior-posterior. The benefits of the anterior approach include better exposure, complete debridement and the ability to achieve anterior fusion. However, the anterior approach in the lower lumbar spine does have an increased risk of neurovascular injury. Rajasekaran, in his study, observed graft slippage, fracture, absorption, or subsidence in 59% of cases with anterior body fusion without instrumentation, and these complications were common when the graft spanned 2 or 3 vertebral bodies. Anterior fusion technique alone also has been reported to have the risk of increased kyphosis angle in the follow-up period, particularly if there is involvement of multiple segments. 17
Posterior approaches are commonly performed due to ease, familiarity of approach, and the lesser learning curve involved. Moreover, it helps to achieve adequate exposure for circumferential spinal cord decompression, better deformity correction through pedicle screws, and the possibility of extension of instrumentation in addition to avoidance of thoracotomy-related complications. Combined anterior and posterior approaches, either as single or two stages, may offer the advantage of decreasing the incidence of kyphosis at a long-term follow-up. However, it is associated with increased cost, longer stay, and more incidence of post-operative complications. Zhang et al. performed two-stage surgery for spinal TB, where in first stage, posterior stabilisation was done, followed by anterior column debridement and use of allografts in stage 2. Their study reported that the combined approach helped in better restoring spinal alignment and preventing kyphosis progression. 18 Yin et al. compared the posterior-only approach with the combined approach in thoracolumbar spinal TB in children. They concluded blood loss, surgical time and hospital stay were reduced perceptibly in patients who underwent a posterior-only surgical approach. 19 In a similar study, Zhang et al. compared the posterior with the posteroanterior approach in 51 children with lumbar TB and concluded that the posterior-only approach provides a satisfactory outcome in experienced hands. 20
Because there are less associated morbidity procedural steps with the posterior-only approach, its utilisation has been rapidly expanding recently. 21 Wang et al. performed single-stage debridement, interbody grafting, posterior instrumentation and posterior fusion of DL spine TB and achieved good results. 22 In our study, all the patients in Group A and Group B underwent a posterior-only approach and achieved good mean kyphosis corrections of 22° (8.4°-35.5°) in groups A and in Group B 34.7° (25.1°-59.9°) respectively”.
In patients with active spinal TB, the deformity is always flexible and mobile at the involved segment. So, a shortening of the posterior column alone is adequate for the correction of the kyphosis. However, in patients with significant anterior column loss, shortening can cause delirious effects on the cord. In our previous prospective study on patients with active spinal TB (with vertebral body loss of less than 1), undergoing surgical fixation using all posterior-only approach, we observed that only posterior column shortening resulted in comparable functional, radiological and neurological outcomes to global reconstruction. 23 In active spinal TB, we wouldn’t recommend a radical debridement of the disease focus. Instead, the debridement should be limited only to achieve adequate decompression of the spinal cord. This would ensure that the anterior void is not large enough to necessitate reconstruction. Fourteen patients in our study had an anterior reconstruction with a titanium metallic cage and nine patients underwent only posterior column shortening. We observed that irrespective of the type in kyphosis classification, the necessity of anterior column reconstruction was based on the extent of total vertebral body loss. We recommend anterior reconstruction when total vertebral body loss (VBL >1). Overall mean correction achieved in group A was 22°. This is comparable with the study by Zeng et al., where in 34 patients with active thoracic TB treated by posterior-only approach, they reported a kyphosis correction of 25.9°. 24
In patients with kyphosis in healed spinal TB, the deformity is rigid and less mobile. Few surgeons have suggested a staged approach for deformity correction, as it is associated with a significant complication rate. Even with staged procedures, Yau et al. reported a mortality rate of 10%. 25 With the advancements in surgical techniques and rigid three-column fixation provided by pedicle screws, single-stage correction has been advocated recently. Bezer et al. in their study of 16 patients with post-TB kyphosis, concluded that single-stage correction of the established deformity is relatively safe, with good outcomes. 26 In patients where only the anterior column is lost, posterior shortening procedures like pedicle-subtraction osteotomy (PSO) and Disc-bone osteotomy (DBO) can be performed. In our study, three patients were in kyphosis Type IIA. Two patients underwent DBO (Figure 2) (mean correction achieved: 36.1°), and 1 underwent a PSO (correction achieved: 32.7⁰). In all these cases, the pre-operative kyphosis rarely exceeded 60° as the posterior column remains intact. In patients with kyphosis Type III deformity, there can be a disproportionate loss of the anterior column relative to the posterior column and hence, a technique that provides adequate deformity correction without causing shortening of the spinal canal is necessary in these patients.
Closing-opening wedge Osteotomy (COWO) was initially described for deformity correction in patients with post-traumatic kyphosis.
27
We performed COWO in one patient in Type IIIA and 17 patients in Type IIIB (Figure 3). In our study, we achieved a mean kyphosis correction of 40.2° (25.1°-59.9°) in patients undergoing COWO. Kawahara et al, in their series of seven patients with post-traumatic kyphosis, reported a higher average deformity correction (49°) with COWO.
27
Compared to post-traumatic kyphosis, in post-TB kyphosis, there are multiple vertebral involvements and also significant adhesions between the dura and the anterior column. Hence, attempts to make gross correction of the deformity are potentially dangerous. Secondly, the mean preoperative kyphotic Cobb’s angle in our series was also higher (81.7°) compared to their study (Cobb’s angle: 67°). One of the patients in our study had an intraoperative neurological deterioration (Frankel D to Frankel B) following the deformity correction. She was a case of thoracic kyphosis (Cobb’s angle: 95°) with the apex at T8-T9 with stretched and thinned cord over the apex of the deformity (Figure 6). Though there was controlled correction of the deformity after wide decompression, there was a loss of neuromonitoring signals intra-operatively. Hence, the planned correction was not attempted, and the deformity was under-corrected. At 6 months follow-up, there was a partial recovery in her neurological function (Frankel B to Frankel C). Anatomically, the lower thoracic cord is a potential watershed vascular zone with poor communication between the anterior and posterior vascular channels.
28
In a study by Kalidindi et al., 105 patients with kyphotic deformity due to varied etiologies were included, and they identified that the apex of kyphosis in the lower thoracic region, magnitude of pre-operative kyphosis, signs of myelopathy and are risk factors of neurological worsening during kyphosis correction surgeries.
29
(A, B) Anteroposterior and lateral whole spine standing radiograph of a 54-year-old female in Group B with kyphotic deformity (Kyphosis Type IIIb M (−) C (−); (C) Sagittal CT scan images showing apex of the deformity at lower thoracic spine; (D) Whole spine MRI scan showing thinned, stretched out spinal cord draping the vertebral body at the apex of the deformity.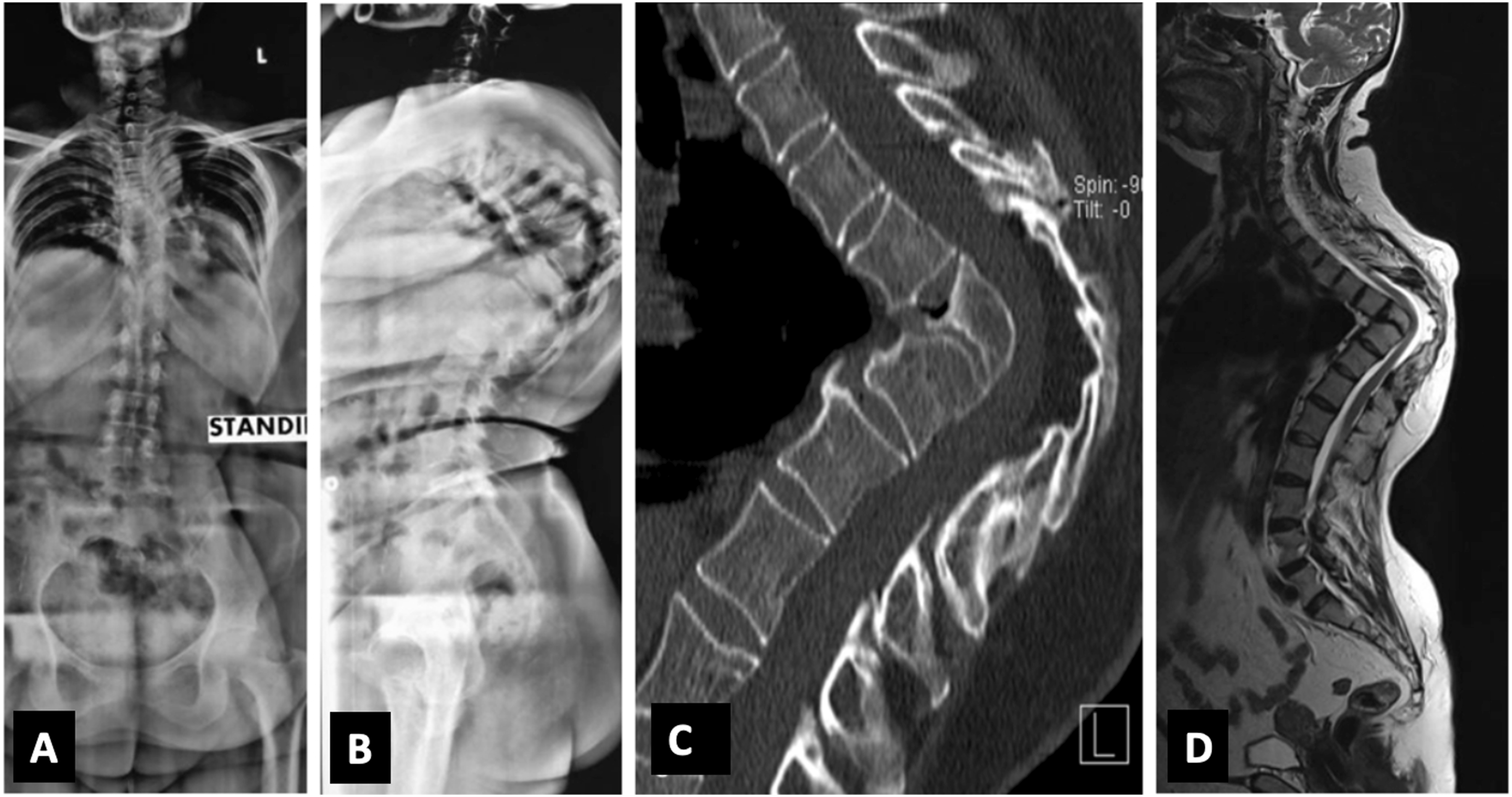
Five patients in our study had a Buckling collapse (Type IIIC). In all these patients, kyphosis was more than 100°, and vertebral column resection (multiple vertebrectomies) was planned. Five patients with Type IIIC and one patient with Type IIIB underwent this procedure. Preoperatively, halo gravity traction was applied in all these patients. The mean duration of traction was 4.8 (3-6) weeks. Halo gravity traction works by tissue creep phenomenon due to the viscoelastic property of the spinal column. It also provides time for pre-operative optimisation (breathing exercises and nutritional supplements) of these patients, as most of these patients are poorly nourished with a very low respiratory capacity due to reduced mediastinal volume. 30 The overall correction achieved by vertebral column resection in our study was 49.3°.
Based on our experience, we formulated a treatment approach based on kyphosis classification for thoracic and thoracolumbar TB kyphosis, which can help surgeons in appropriate decision-making (Figure 7). Limitations of our study include a relatively smaller sample size in each group, including both thoracic and thoracolumbar spine, which are subjected to different loading patterns and biomechanical behaviours. Pelvic parameters (pelvic incidence, pelvic tilt and sacral slope) were not analyzed and included in the protocol. Further, multi-centred trials involving a larger sample size and longer follow-up duration are necessary to validate our findings. Flowchart showing management of thoracic and thoracolumbar TB kyphosis based on kyphosis classification.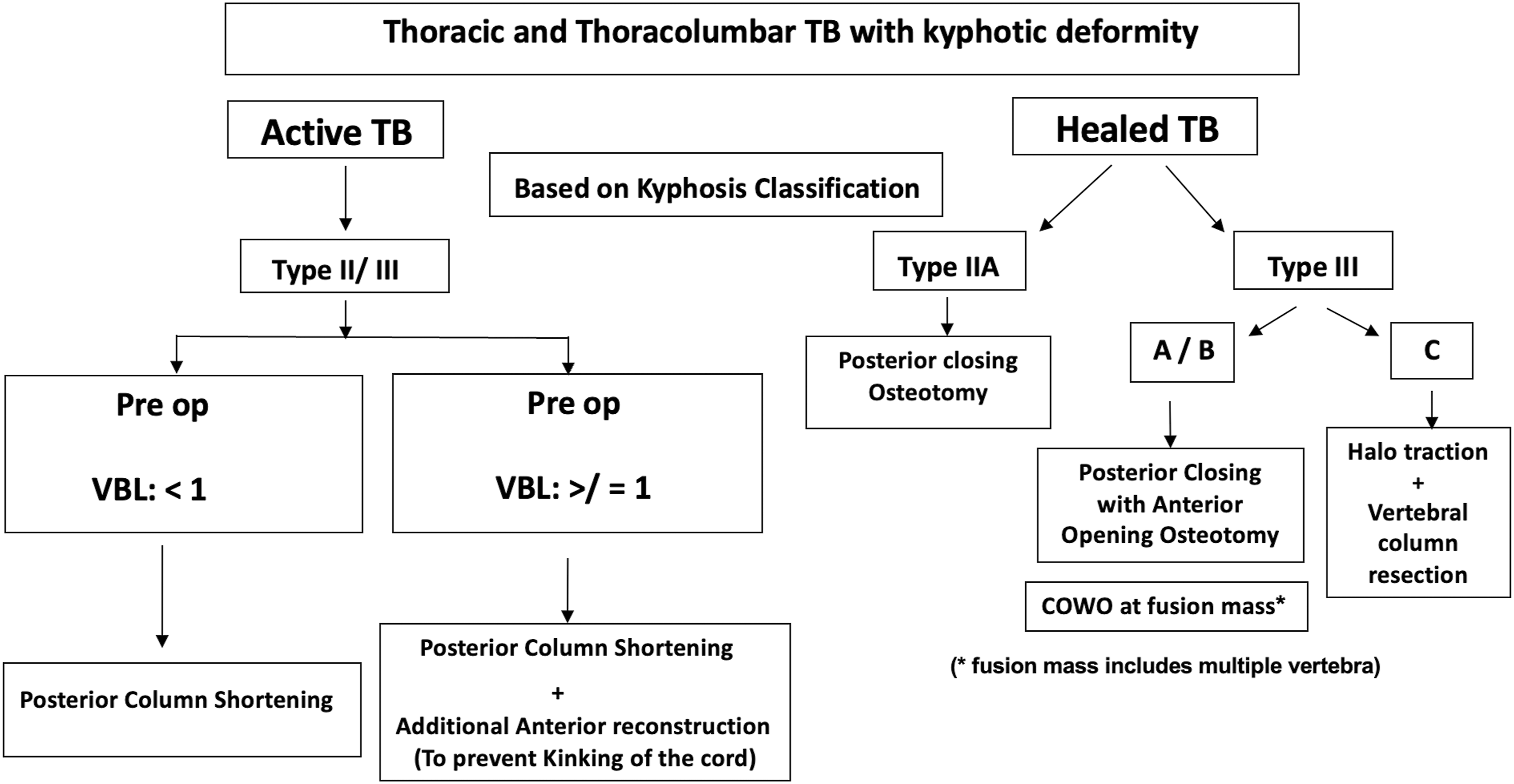
Conclusion
Kyphosis in spinal TB needs appropriate management to avoid long-term complications. Surgical management of these deformities in active and healed TB is two different entities with varied surgical challenges. The posterior-only approach can be a reliable option for treating such deformity, provided an appropriate preoperative analysis and classification of such deformity is performed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.