
Abstract
Study Design
Single-blind, prospective controlled trial.
Objective
While physiotherapy scoliosis-specific exercise improves spinal deformities in mild adolescent idiopathic scoliosis, evidence for early-onset idiopathic scoliosis (EOIS) is limited. This study proposed comprehensive spinal correction rehabilitation (CSCR) and evaluated its efficacy in EOIS.
Methods
44 EOIS patients aged 7-10 years were divided into 2 groups matching for age and gender. The interventional group (n = 22) underwent CSCR, and the control group (n = 22) was followed up for observation. Bracing was added if the patients’ Cobb angle reached 25° and above. All enrolled patients were evaluated at the initial visit and after the 6-month intervention, including baseline condition, the major curve Cobb angle, lung function, balance function, and quality of life, respectively.
Results
After the intervention, the amount of change in the main curve Cobb angle, forced vital capacity (FVC) and forced expiratory volume in the first second (FEV1) (△Cobb angle, △FVC, △FEV1) in the intervention group increased significantly compared with the control group (P = .001, P = .001, P = .002); in the intervention group, the main curve Cobb angle decreased, and FVC and FEV1 increased significantly after the intervention (P = .001 P = .007, P = .003), but there was no significant difference compared with the control group; and the difference in balance function and quality of life between the 2 groups after the intervention was also not significant (all P > .01).
Conclusion
CSCR could effectively improve the spinal deformity of patients with EOIS and simultaneously increase their lung function.
Keywords
Introduction
Early-onset idiopathic scoliosis (EOIS) is defined as idiopathic scoliosis with onset before 10 years old. 1 Nouri et al 2 found that the prevalence of early-onset scoliosis was .077%, with idiopathic scoliosis second only to neuromuscular scoliosis, accounting for 37.1% of all cases of early-onset scoliosis. Although the incidence of EOIS in children is low, its progression remains a significant concern in clinical practice. Untreated EOIS can result in severe spinal deformity, impeding the normal development of alveoli and thoracic contour, thereby posing permanent damage to cardiorespiratory function in children with EOIS.3-7 This underscores the importance of early detection and timely intervention for EOIS.
Currently, the variability in treatment efficacy for EOIS poses a challenge given the unclear etiology of EOIS. Standard treatments for EOIS typically include a series of serial casting, bracing, Halo-gravity traction, surgery, and rehabilitation.8-12 While serial casting and bracing are commonly employed as primary treatments for EOIS, the extended pressure exerted by the cast and brace on the skin, along with issues of poor compliance in younger patients, remain potential factors impacting the efficacy of treatment.8,13 As an invasive treatment requiring anesthesia, Halo-gravity traction may pose neurological risks to children and warrant caution when considering young patients. 14 Furthermore, surgery is used as an alternative when conservative treatment fails due to the occurrence of postoperative complications and significant medical expenses involved. 11 An increasing number of studies have demonstrated the effectiveness of physiotherapy scoliosis-specific exercise (PSSE) in decelerating the progression of scoliotic deformity, of which exercise therapies for EOIS mainly include Schroth, Scientific Exercise Approach to Scoliosis (SEAS), Functional Individual Therapy of Scoliosis approach (FITS), Barcelona Scoliosis Physical Therapy School approach (BSPTS) and Lyon.15-19 However, it has been suggested that PSSE has a limited effect on improving lung function, balance, and quality of life in children with scoliosis, and there is still a lack of high-level evidence on the effectiveness of PSSE in the treatment of EOIS.1,20
To address the limitations of exercise therapy in improving lung function and to validate its efficacy in children with EOIS, an individualized treatment approach, named Comprehensive Spinal Correction Rehabilitation (CSCR), was developed, integrating deformity correction with physical fitness enhancement within developmental characteristics of pediatric patients. This study aimed to investigate the therapeutic effect of CSCR on lung function, balance, and quality of life in children with EOIS. We hypothesized that CSCR would serve as a precision rehabilitation program targeting the delay of scoliosis progression, improvement of lung function, and enhancement of the quality of life in children with EOIS.
Methods and Materials
Study Design
44 children were enrolled and evenly divided into 2 groups matching for age and gender. The interventional group (n = 22) underwent CSCR, and the control group (n = 22) was followed up for observation. If the patients’ Cobb angle reached 25° and above, bracing treatment would be added. Because of the different methods of intervention in this study, therapists and patients were not allowed to be blinded when providing or receiving treatment. However, after patients were informed of their subgroups, they were asked not to disclose their subgroups to ensure that all assessors were blinded. This clinical trial has been approved by the Xinhua Hospital Ethics Committee Affiliated to Shanghai Jiao Tong University School of Medicine (XHEC-C-2022-081-3) and registered in the Chinese Clinical Trial Registry (ChiCTR2300074420). Parents or legal guardians of all recruited children signed an informed consent form before participating in the study.
Participants
Children with EOIS who attended the outpatient clinic of the Department of Re-habilitation Medicine, Xinhua Hospital, Shanghai Jiaotong University School of Medi-cine, Shanghai, China, between December 2022 and December 2023, were recruited. Those who met the eligibility criteria would be included in the study. Inclusion criteria were that the children met the diagnostic criteria for EOIS and were between 7 and 10 years old.
1
The exclusion criteria included children with (1) scoliosis attributed to neuromuscular disorders, congenital disorders, specific syndromes, (2) a history of thoracic, abdominal, pelvic, or spinal surgery, (3) mental illness or rheumatic diseases, (4) contraindications to exercise or inability to tolerate exercise therapy, (5) previous rehabilitation, and (6) insufficient comprehension to cooperate with treatment. The flowchart of the patients recruited for this study is shown in Figure 1. The sample size was calculated using G-Power software (Version 3.1 for Windows, Universität Düsseldorf, Düsseldorf, Germany). The effect size was determined based on the findings of the previous study, where the interventional group exhibited a change of (−1.55 ± 4.39)° in the major curve Cobb angle compared to (2.9 ± 2.60)° in the control group,
21
with α set at .01 and β = .2, which yielded a total of 19 children with EOIS in each group. It was anticipated that the trial might have a 10% loss-to-follow-up rate, with a required sample size of at least 21 patients in each group. Flow diagram of the patients through the trial. CSCR, comprehensive spinal correction rehabilitation.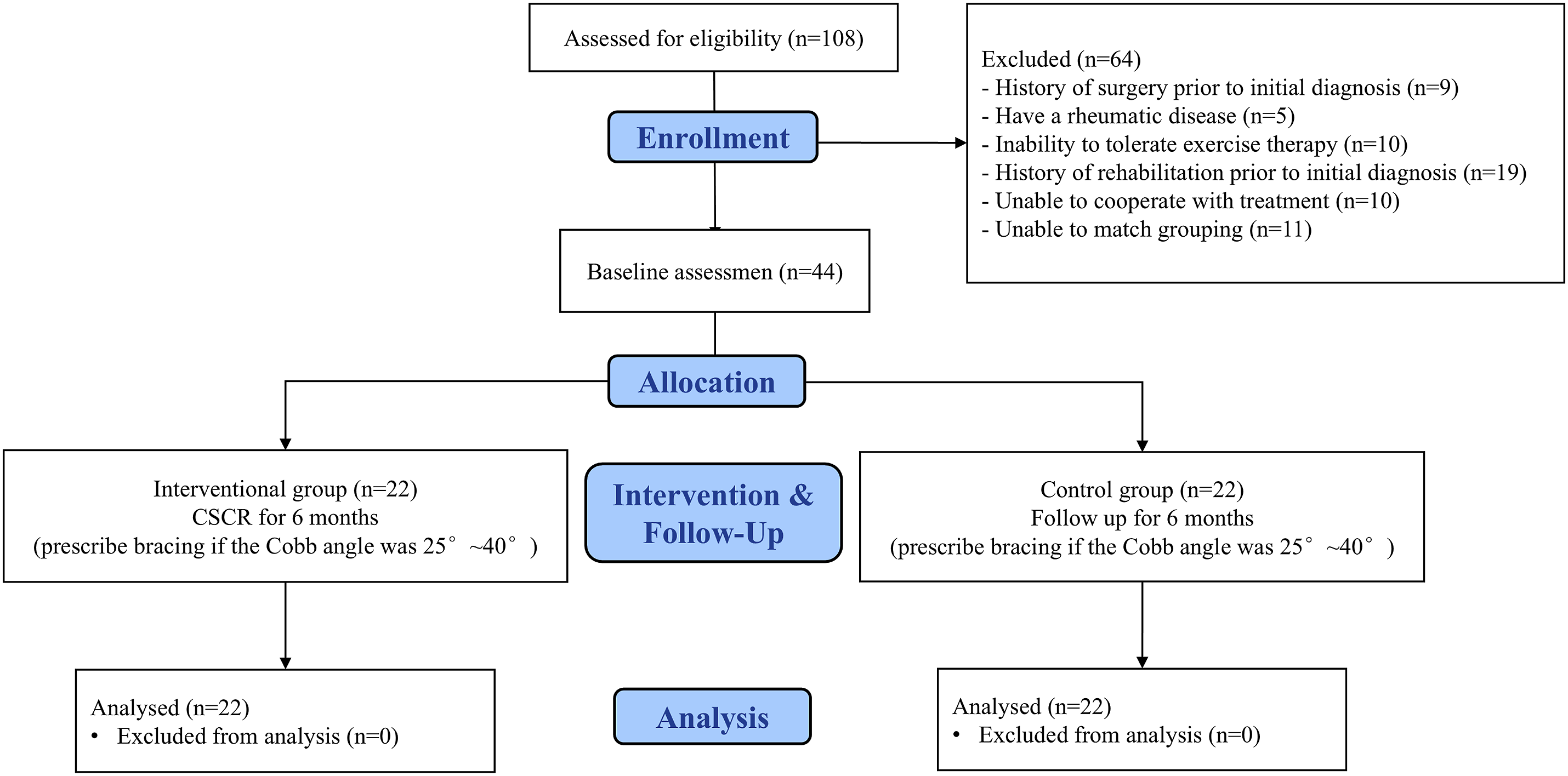
Treatment Protocol
The interventional group received CSCR, which is an innovative therapy that incorporates the characteristics of developing children and adolescents. It is based on PSSE and includes specific exercise therapy, balance and stability training, breathing training, strength training, home-based exercise, and bracing. The details of the treatment are as follows: (1) Specific exercise therapy includes three-dimensional self-correction, manipulation, and distraction therapy. 22 Among them, three-dimensional self-correction involves self-correction exercises in different positions according to the scoliosis condition to correct the abnormal posture and at the same time correct the spinal deformity in 3 planes: sagittal, coronal, and horizontal planes; manipulative therapy can adjust the small spinal joints, relax the tense muscles, and improve the vertebral flexibility; and distraction therapy can achieve the effect of the reversal of correction through axial stretching of spinal paravertebral muscles. (2) Balance and stability training is performed using a static balancing instrument (Tetrax, Sunlight Medical Ltd, Israel). Tetrax would adjust the height and tilt of the display according to the height and weight of patients, using visual feedback for the centre of gravity control. During training, the patient needs to move the light point representing the centre of gravity on the display to the indicated light point. The system records the speed and accuracy of the movement, and the patient’s centre of gravity movement and bipedal weight bearing while standing are accurately captured by the force platform. 23 (3) During the breathing training, patients need to take slow, deep breaths under the guidance of the therapist. When inhaling, try to fill the chest cavity with gas as much as possible, especially to make the concave side of the collapsed lungs fully expanded; when exhaling, try to exhaust all the gases as much as possible, especially to minimize the residual gases in the convex side of the lungs, and the patients who are wearing the braces can carry out the above breathing training while bracing. (4) Strength training mainly includes training of the spinal muscles as well as the core muscles. It can be incorporated into home-based exercises to train core strength, with specific movements including abdominal breathing and plank support, in addition to diagonal support and unilateral bridge movements. (5) Home-based exercises are taught to all patients by the same therapist, with parents able to observe. The patients could perform three-dimensional spinal self-correction by performing several sets of specific gymnastic movements in different positions. During the home treatment, parents assisted in monitoring the accuracy and standardization of the corrective exercises. (6) Bracing would be used when the Cobb angle is 25°∼40° and the brace is worn for 20 or more hours per day. At the initial consultation, health education was conducted to inform the patients and their parents of the risks and dangers of scoliosis progression, to teach the patients to pay attention to daily postural management, to instruct the parents to recognize the progression of the deformity in time and to emphasize the importance of regular follow-up. The intensity of treatment was set according to the individual tolerance level, and the treatment lasted for 6 months. The frequency of treatment was 60 min for outpatient treatment once a week and 30 min for home-based exercise once a day.
The control group was followed up for observation and health education. If the Cobb angle was 25°∼40°, bracing would be prescribed. The content of health education was the same as that of the interventional group.
Outcome Measures
Patients were assessed twice by the same assessor at the time of the initial visit and 6 months after the intervention. Assessments included the major curve Cobb angle, lung function, balance function, and quality of life.
Cobb Angle
The major curve Cobb angle was obtained by measuring the coronal plane of the whole spine radiographs. 24
Lung Function
Evaluators used the QuarkPFT4 spirometer (COSMED, Italy) to perform lung function tests on patients. 25 At the start of the test, the subject was placed in a natural standing position, holding the blowing device in one hand and ensuring that the lips were wrapped tightly around the disposable cartridge bite, and mouth breathing was used throughout the test. The assessor then instructed the subject to breathe calmly according to the instructions of the instrument. After at least 5 steady tidal breaths appeared on the display, the subject was instructed to take a maximal inhalation until the total lung volume was reached, and then immediately exhale as fast as possible up to the residual air level, followed by another inhalation up to the total lung volume, and then finally, the measurement was obtained. The above test was repeated 3 times and the average of the 3 measurements was taken as the result. The indices for evaluating lung function are forced vital capacity (FVC), percentage of forced vital capacity predicted (FVCpred%), forced expiratory volume in the first second (FEV1), percentage of forced expiratory volume in the first second predicted (FEV1pred%), and percentage of forced expiratory volume in the first second to forced vital capacity (FEV1/FVC%).
Balance Function
The balance function of the patients was tested using Tetrax. 23 During the measurement, the patient has to keep 8 positions (eyes open normal position [NO], eyes closed normal position [NC], eyes open while standing on a footpad [PO], eyes closed while standing on a footpad [PC], eyes closed with head turned to the right [HR], eyes closed with head turned to the left [HL], eyes closed with head tilted back 30° [HB], eyes closed with head tilted forward 30° [HF]) on the balance tester, and the force platform can feel the weight-bearing situation and the movement of the centre of gravity of the human body when standing, and the signal can be processed to obtain the Fall index (FI). A high FI was related to a decline in balance function.
Quality of Life
Quality of life was assessed utilizing the Scoliosis Research Society-22 item questionnaire (SRS-22). 26 The SRS-22 questionnaire consists of twenty-two items covering 5 dimensions, each with a score range of 1∼5, including functional activity, pain, self-image, mental health, and satisfaction with treatment, with higher scores indicating better quality of life for patients.
Data Analysis
Data were processed and analyzed using SPSS (version 25.0; Armonk, NY, USA, IBM Corporation) statistical software after collecting data from both assessments. The Shapiro-Wilk test would be used to determine whether the data conform to a normal distribution; normal distribution will be expressed as the mean ± standard deviation (x̅ ± s) for measures, median and quartiles [M (P25, P75)] for nonnormal distribution, and enumeration data (constitutive ratios) for counts. When comparing between groups, the independent samples t test or Mann-Whitney U test was used to compare the differences in the major curve Cobb angle before and after the intervention; the Fisher’s exact test was used to compare the differences in the lung function indices, the balance function indices, and the indices related to the quality of life before and after the intervention between the 2 groups. Paired samples t test or paired samples or Wilcoxon signed-rank test was used for within-group comparisons, with Fisher’s exact test for count data. The significance level was set at P < .01 after the Bonferroni correction.
Results
Basic Information
Baseline Demographic and Clinical Characteristics for Control and Interventional Groups.
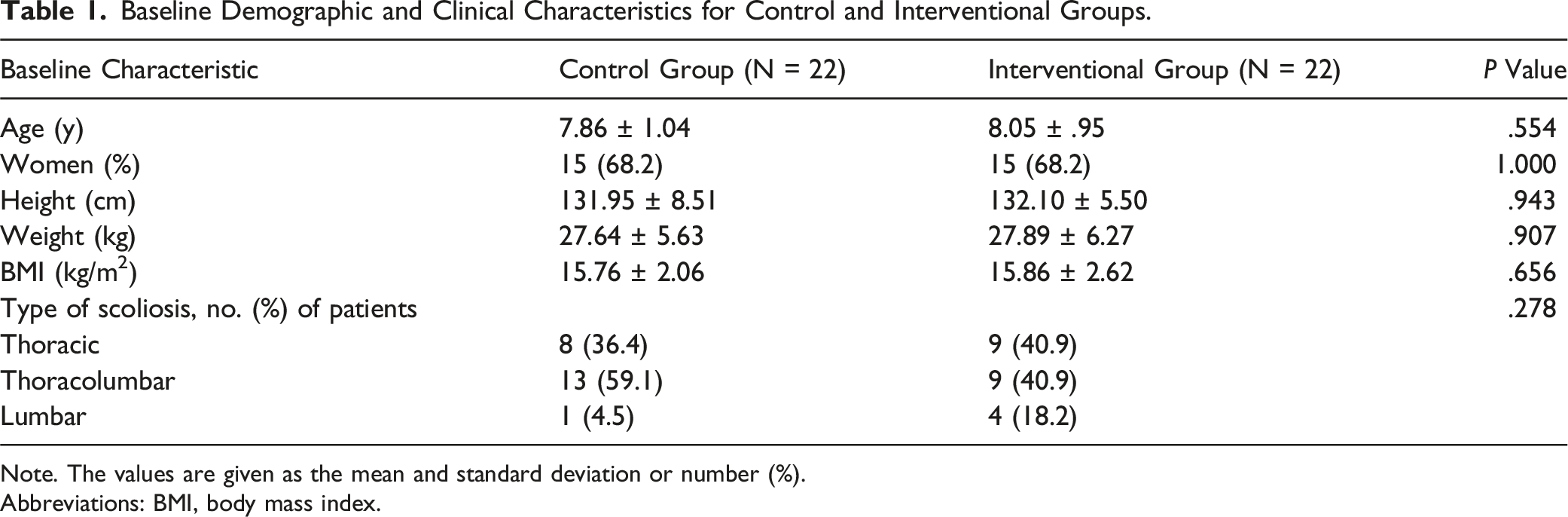
Note. The values are given as the mean and standard deviation or number (%).
Abbreviations: BMI, body mass index.
Comparison of the Major Curve Cobb Angle
Comparison of the Major Curve Cobb Angle Before and After Intervention in Both Groups.

Note. The values are given as the mean and standard deviation.
*Statistical analysis for comparison: P < .01, statistical significance.
Comparison of the Amount of Change in the Major Curve Cobb Angle
The pre-intervention major curve Cobb angle was subtracted from the post-intervention major curve Cobb angle to express the amount of change in the major curve Cobb (△Cobb) angle before and after the intervention. The △Cobb angle in the control group was (−.2 ± 2.9)°, and the △Cobb angle in the interventional group was (3.2 ± 3.7)°. Before and after the intervention, the △Cobb angle in the interventional group was significantly greater than that of the control group, and this difference was statistically significant (P = .001), as shown in Figure 2. Comparison of the amount of change in the major curve Cobb angle before and after intervention in both groups.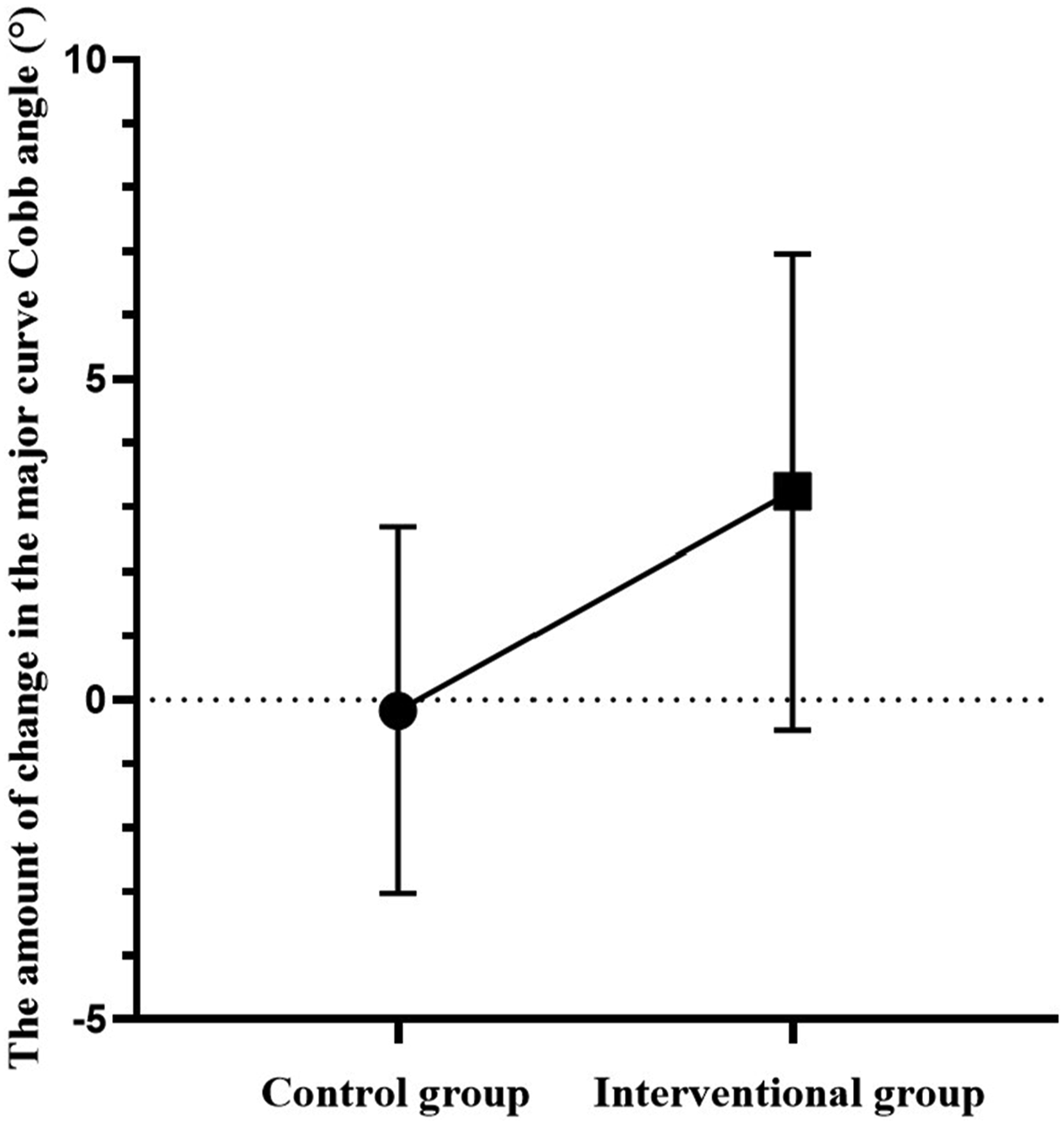
Comparison of Lung Function
Comparison of Lung Function Before and After Intervention in Both Groups.
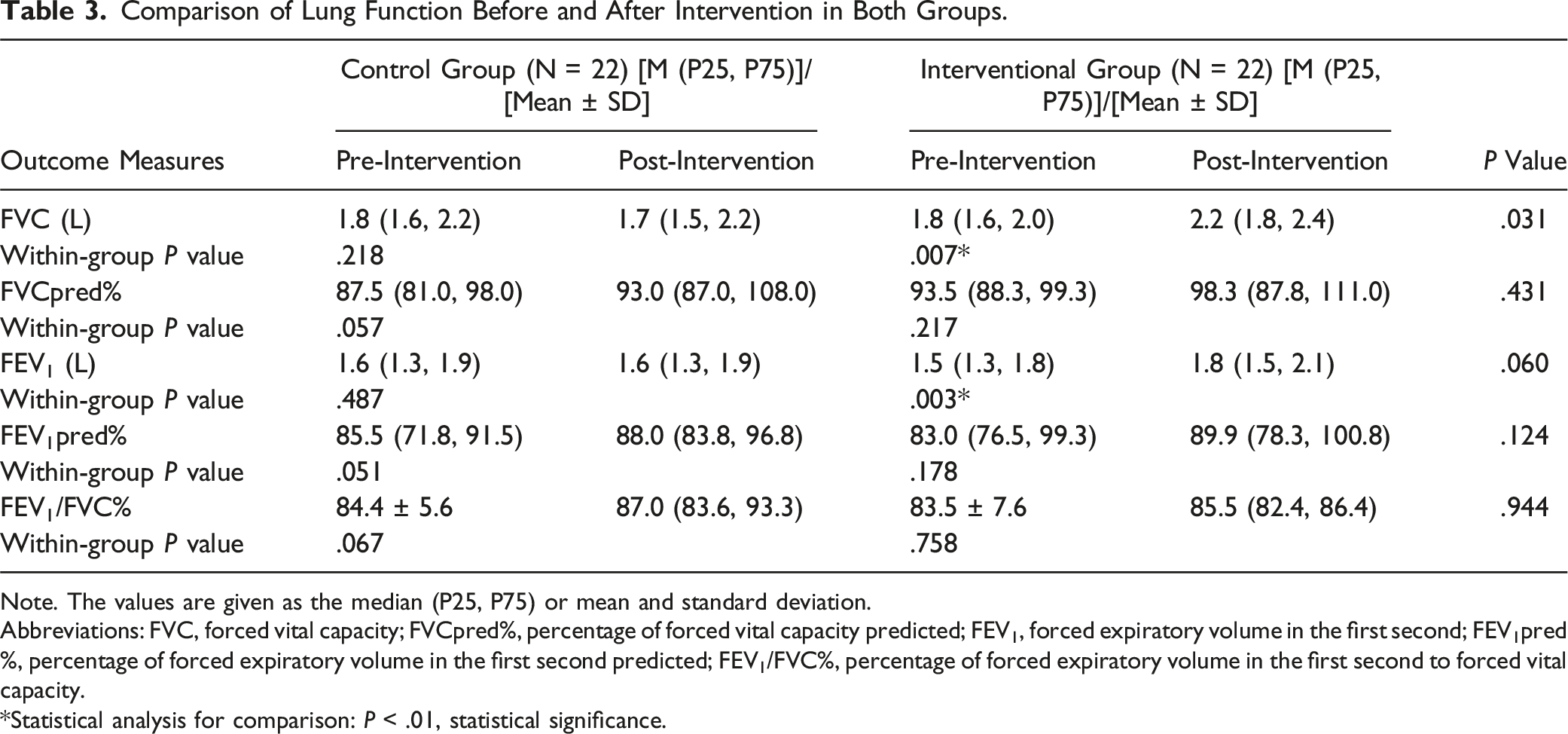
Note. The values are given as the median (P25, P75) or mean and standard deviation.
Abbreviations: FVC, forced vital capacity; FVCpred%, percentage of forced vital capacity predicted; FEV1, forced expiratory volume in the first second; FEV1pred%, percentage of forced expiratory volume in the first second predicted; FEV1/FVC%, percentage of forced expiratory volume in the first second to forced vital capacity.
*Statistical analysis for comparison: P < .01, statistical significance.
Comparison of the Amount of Change in Lung Function
Comparison of the Amount of Change in Lung Function Before and After Intervention in Both Groups.
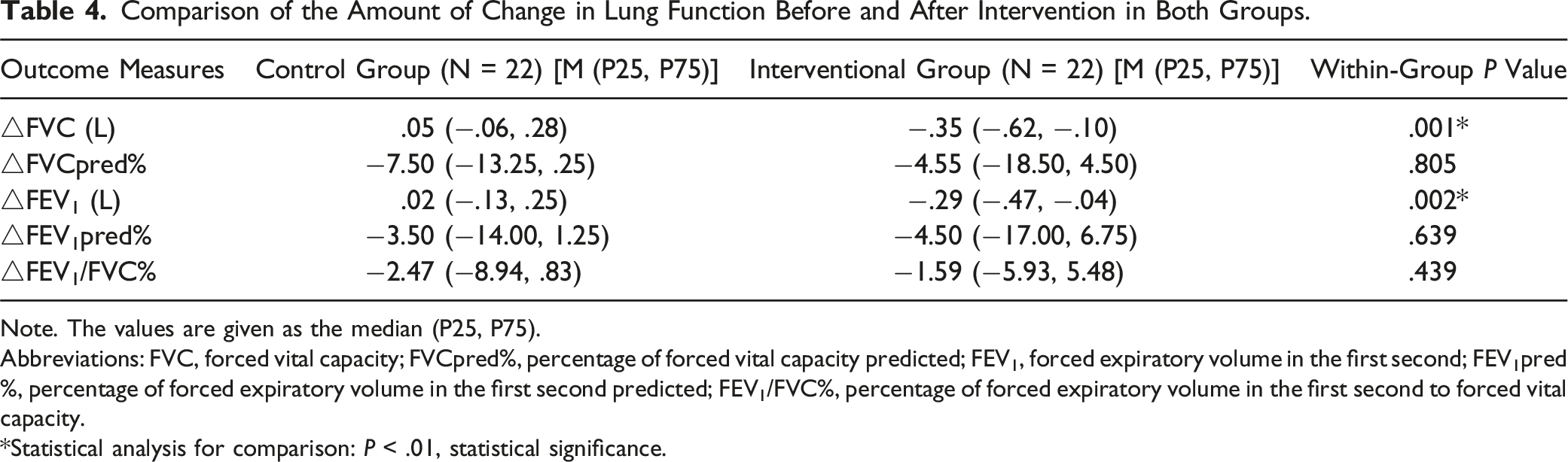
Note. The values are given as the median (P25, P75).
Abbreviations: FVC, forced vital capacity; FVCpred%, percentage of forced vital capacity predicted; FEV1, forced expiratory volume in the first second; FEV1pred%, percentage of forced expiratory volume in the first second predicted; FEV1/FVC%, percentage of forced expiratory volume in the first second to forced vital capacity.
*Statistical analysis for comparison: P < .01, statistical significance.
Comparison of Balance Function
Comparison of Balance Function Before and After Intervention in Both Groups.

Note. The values are given as the median (P25, P75).
Abbreviations: FI, fall index.
Comparison of Quality of Life
Comparison of SRS-22 Scores Before and After Intervention in Two Groups.
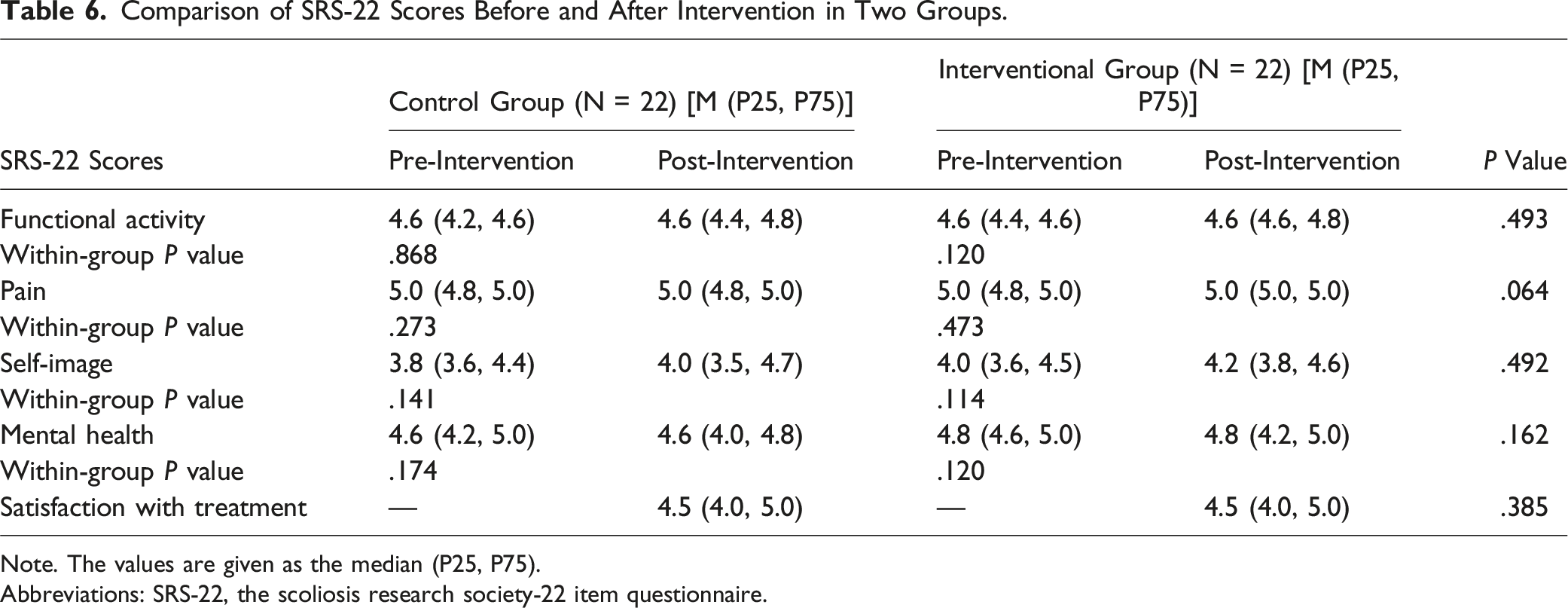
Note. The values are given as the median (P25, P75).
Abbreviations: SRS-22, the scoliosis research society-22 item questionnaire.
Comparison of SRS-22 Scores Before and After Intervention in Two Groups With Thoracic Curvature Type of Scoliosis.
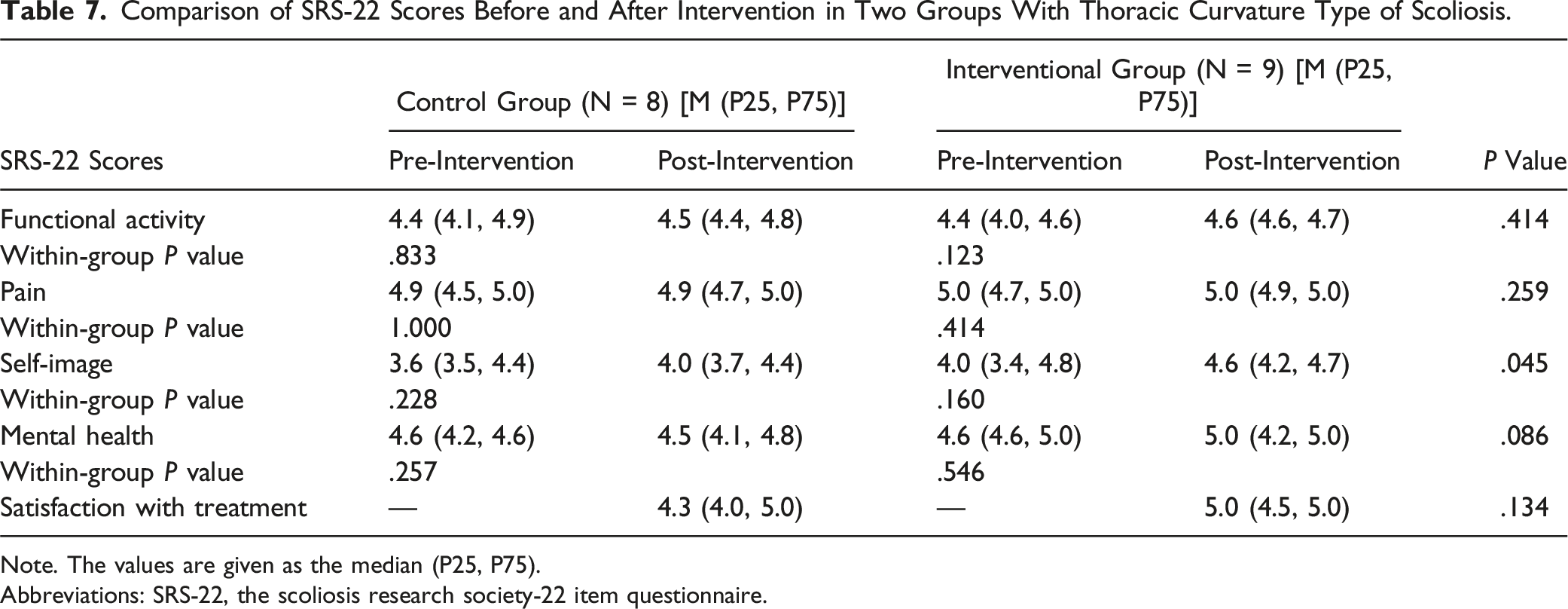
Note. The values are given as the median (P25, P75).
Abbreviations: SRS-22, the scoliosis research society-22 item questionnaire.
Comparison of SRS-22 Scores Before and After Intervention in Two Groups With Thoracolumbar Curvature Type of Scoliosis.
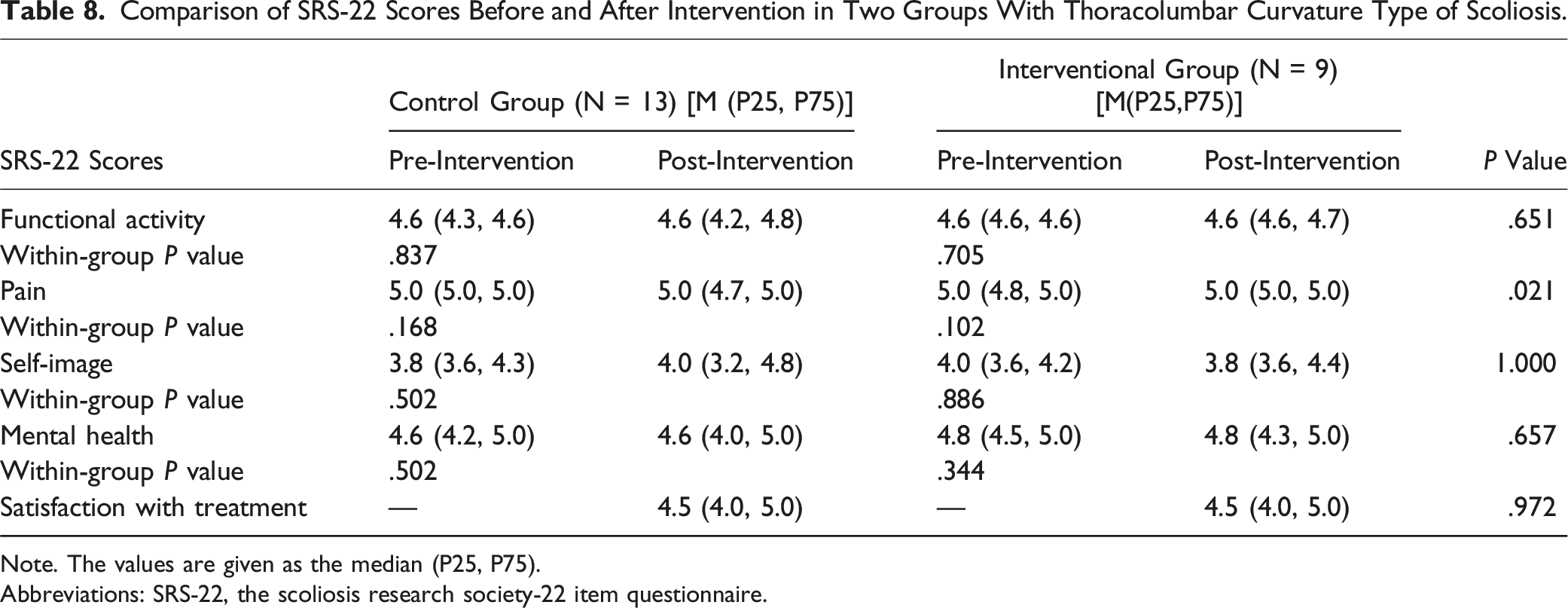
Note. The values are given as the median (P25, P75).
Abbreviations: SRS-22, the scoliosis research society-22 item questionnaire.
Discussion
Due to the high progression and variability of EOIS in young children, there is currently a lack of evidence regarding the effectiveness of general exercise therapy for children with EOIS. CSCR is based on PSSE and also incorporates balance and stability training, breathing training, strength training, home-based exercise, and bracing. CSCR is based on PSSE and incorporates balance/stability, breathing, strength training, home exercises, and bracing. The design of CSCR focuses on correcting spinal deformities while also improving essential daily functions such as lung capacity and balance. In this study, we found that the major curve Cobb angle of the interventional group decreased significantly compared to the pre-intervention period, and the △ Cobb angle in the intervention group increased significantly compared with the control group, which is consistent with previous findings. In Białek et al, 16 exercise therapy was used in 41 patients aged 4 to 9 years with EOIS and Cobb angle ranging from 11° to 30°, and the results showed a significant decrease in Cobb angle post-intervention after a 4.8-year follow-up. The CSCR used in the study was effective in delaying the deformity by providing targeted training to characterize the children’s spinal deformity. However, it should be noted that most of the patients in this study belonged to mild and moderate scoliosis, and the efficacy for patients with severe scoliosis needs to be verified by further studies.
Abnormal curvature and rotation of the spine and distortion of thoracic structures can lead to compromised lung function in patients with scoliosis. Especially in children with EOIS, the thorax and lungs are developing in childhood, and the spinal deformity that occurs at this time may result in reduced thoracic volume, reduced thoracic mobility, and ultimately reduced lung function.21,27 Tang et al 28 performed Halo-gravity traction and breathing training preoperatively on 34 children with thoracic curvature type of scoliosis aged 4∼8 years and found that breathing training helped to improve the lung function of the children and reduce perioperative complications. Moramarco et al 29 performed a multimodal exercise program for 5 to 7 days in 36 patients with IS and found that patients with scoliosis who underwent a multimodal exercise program showed a significant improvement in lung function indicators of FVC and FEV1 compared to the previous period, which is consistent with the findings of this study. The results of this study showed that FVC and FEV1 were significantly improved in the interventional group after the intervention compared to the pre-intervention period, and the △FVC and △FEV1 were significantly greater in the interventional group than in the control group. The results of the above show that CSCR is effective in improving the lung function of EOIS, especially for the FVC and FEV1 indicators. Breathing training can make the thoracic cavity reach its maximum limit as much as possible, prompting the lungs to fully expand, thus improving the compliance of the lungs and thorax and improving lung function. During breathing training, the child could actively inhale and exhale deeply under the guidance of the therapist to maximize the activation of the diaphragm and auxiliary respiratory muscles, thus increasing the strength and endurance of the respiratory muscles. It is also important to be aware that wearing a brace for a long period of time has a negative effect on lung function. 30 However, most of the patients in this study did not need to be treated with braces, so more in-depth studies are required to determine the effect of CSCR on improving lung function in patients with scoliosis who wear braces.
Balance function is a critical aspect of daily activities, especially in children. 31 Good balance is strongly linked to enhanced mobility performance and health promotion in children.32,33 Scoliosis patients have low balance stability, and most of them have moderate or higher fall risk. 34 A study showed that there was a positive correlation between coronal balance on the side of the major curvature and weight bearing on the forefoot in patients with idiopathic scoliosis. 35 Shen et al 36 found that adding balance training to Schroth therapy significantly improved balance function in patients with IS. In this study, there was no significant difference between the interventional and control groups in balance function before and after the intervention. Since different visual conditions may affect the children’s balance control. 37 This study did not investigate the patients’ vision condition in detail and urged them to wear corrective glasses during assessment and practice, which may be one of the reasons why no significant difference in balance function was observed. In the follow-up study, in addition to prolonging the intervention time, we will pay attention to the patient’s vision condition and remind them to wear appropriate corrective glasses in time during balance function assessment and balance/stability training.
The appearance of back deformity, pain, and abnormal body posture caused by scoliosis may cause various adverse psychosocial reactions in children, affecting their quality of life. 38 A Meta-analysis shows that exercise therapy alone could improve the quality of life in scoliosis patients in the short term. 39 However, in the study by Kuru et al, 15 no benefits of exercise therapy in terms of the quality of life of scoliosis patients were found, which was consistent with the findings of our study. In this study, we found that the difference in the dimension scores of the SRS-22 between the 2 groups was not statistically significant in the post-intervention period; even when different scoliosis types analyzed subgroups, no significant differences were found. This result may be related to the ceiling effect of the SRS-22 questionnaire. In our study, the percentage of patients who scored not less than 4 on the SRS-22 for which the best score is 5 was high (functional activity = 93.2%, pain = 100%, self-image = 45.5% and mental health = 100%), as mild and moderate scoliosis have less of an impact on the quality of life of patients, resulting in generally high baseline values, and high scores may have compromised the questionnaire’s ability to measure the effect of the intervention.40,41 In addition, an important factor causing a decrease in the quality of life of scoliosis patients is bracing. Prolonged bracing can lead to unhealthy psychological states such as low self-esteem in children, and the constraints on movement and breathing imposed by braces can reduce the quality of life and well-being of scoliosis patients. 42 However, only 2 patients included in this study were treated with braces, which may also have contributed to the lack of significant change in quality of life after the intervention.
The present study has several limitations. First, a 6-month follow-up period may not capture the long-term effects of CSCR on the severity of spinal deformity, functional mobility, and quality of life in children with EOIS in the long term or after pubertal development. Second, this study was a single-centre, nonrandomized, controlled design, which may impact the level of the evidence. In addition, when measuring balance function and performing balance/stability training, the patient’s vision condition was not considered, which may have affected the study results. Finally, the sample size of this study was relatively small, and most of the children with EOIS included in this study had mild scoliosis, with only 2 of all patients treated with braces. These factors limited the statistical power to detect significant changes in the outcomes of measures before and after the intervention.
Conclusion
CSCR has been shown to be effective in correcting spinal deformity and improving lung function, especially for the FVC and FEV1 indicators, but is less effective in improving balance function and quality of life. In the future, attention needs to be paid to the patient’s vision condition during balance assessment and training, and consideration could be given to the inclusion of more children with severe EOIS as well as those treated with braces, a longer duration of intervention, and a multicenter randomized controlled design to further validate the effectiveness of CSCR.
Footnotes
Acknowledgments
We thank Xi Zhang for her valuable advice on statistical methodology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Shanghai Hospital Development Center Foundation (No. SHDC 12023118) and the Medical Innovation Research of Shanghai Science and Technology Commission (No. 22Y21900600).