
Abstract
Study Design
Retrospective study.
Objectives
Our objective is to create comprehensible machine learning (ML) models that can forecast bone cement leakage in percutaneous vertebral augmentation (PVA) for individuals with osteoporotic vertebral compression fracture (OVCF) while also identifying the associated risk factors.
Methods
We incorporated data from patients (n = 425) which underwent PVA. To predict cement leakage, we devised six models based on a variety of parameters. Evaluate and juxtapose the predictive performances relied on measures of discrimination, calibration, and clinical utility. SHapley Additive exPlanations (SHAP) methodology was used to interpret model and evaluate the risk factors associated with cement leakage.
Results
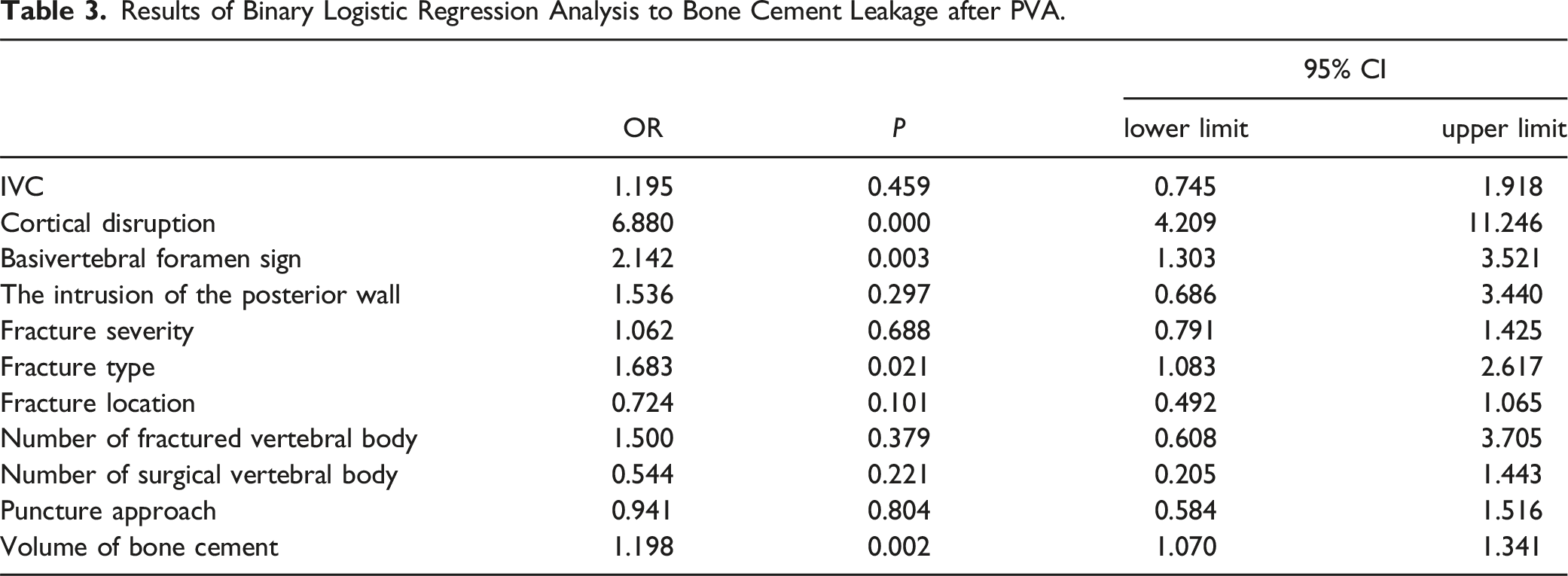
The occurrence rate of cement leakage was established at 50.4%. A binary logistic regression analysis identified cortical disruption (OR 6.880, 95% CI 4.209-11.246), the basivertebral foramen sign (OR 2.142, 95% CI 1.303-3.521), the fracture type (OR 1.683, 95% CI 1.083-2.617), and the volume of bone cement (OR 1.198, 95% CI 1.070-1.341) as independent predictors of cement leakage. The XGBoost model outperformed all others in predicting cement leakage in the testing set, with AUC of .8819, accuracy of .8025, recall score of .7872, F1 score of .8315, and a precision score of .881. Several important factors related to cement leakage were drawn based on the analysis of SHAP values and their clinical significance.
Conclusion
The ML based predictive model demonstrated significant accuracy in forecasting bone cement leakage for patients with OVCF undergoing PVA. When combined with SHAP, ML facilitated a personalized prediction and offered a visual interpretation of feature importance.
Keywords
Introduction
Percutaneous vertebral augmentation (PVA), including vertebroplasty (PVP) and kyphoplasty (PKP), is an established procedure for treating osteoporotic and partially tumor-related vertebral fractures, although it carries the risk of potential catastrophic outcomes. 1 Osteoporotic vertebral compression fracture (OVCF) pose a significant hazard and are a major cause of disability and mortality in elderly patients. 2 PVA is widely utilized in patients with OVCF due to its minimally invasive nature, ability to relieve pain, capacity to maintain or restore vertebral height, and promotion of early ambulation. However, several complications associated with PVA have been identified in previous studies, including bone cement leakage, 3 fractures at adjacent or remote levels, 4 infections, and hidden blood loss. 5 Among these complications, the leakage of bone cement is receiving increasing attention as the most common complication of PVA, with prevalence ranging from 5% to 80%. 3 While the majority of bone cement leakages are asymptomatic, they can occasionally lead to serious consequences, such as nerve or spinal canal compression, as well as intravascular embolism, particularly pulmonary embolism, which can be catastrophic and even fatal. The long-term prognosis of asymptomatic bone cement leakage remains uncertain. Therefore, early recognition and intervention are crucial for bone cement leakage. Unfortunately, effective methods for early identification of bone cement leakage are still lacking in clinical practice.
Clinical prediction models, which assess the probability of specific outcomes based on patient characteristics, 6 are increasingly popular in orthopedics for predicting complications associated with surgical procedures. With the recent advancements in artificial intelligence (AI), machine learning (ML) algorithms have been introduced into prediction models. Some researchers have developed ML models to predict bone cement leakage and have selected the best-performing model to create a web calculator. 7 However, previous models did not incorporate comprehensive evaluations of ML models’ performance and neglected the inclusion of multifaceted related variables. Furthermore, the interpretability of ML models is limited due to their “black box” nature, where only input and output are visible without any insight into the intermediate process. Consequently, their applicability in clinical practice is restricted because they lack intuitive interpretation.
To address these issues, our study integrates additional radiology and surgery-related information to develop ML models, utilizing SHapley Additive exPlanations (SHAP) to provide intuitive explanations of individual predictions and risk factors. Our aim is to build more robust ML-based predictive models for bone cement leakage in PVA and assist clinicians in recognizing the early-stage risk of bone cement leakage, analyzing risk factors, and implementing interventions to reduce its occurrence.
Method
Study Participants
We conducted a retrospective analysis of patients (n = 425) who underwent PVA for OVCF at the Department of Spine Surgery, Zhongda Hospital affiliated with Southeast University, from May 2020 to December 2022. This study was approved by the Institutional Ethics Committee of Zhongda Hospital affiliated with Southeast University (reference number: 2022ZDKYSB121) and the application for exemption from informed consent was granted.
Inclusion criteria were as follows: (1) diagnosis of OVCF based on clinical manifestations and radiological characteristics; (2) presence of back pain, with or without trauma, related to OVCF; (3) meeting the indications for PVP/PKP.
Exclusion criteria were as follows: (1) age below 45 years; (2) presence of spinal cord, cauda equina, or nerve root injuries; (3) chronic vertebral compression fracture with negative MRI results, burst fractures, or malignant fractures; (4) Loss and fault of raw clinical data and incomplete imaging data (complete data including preoperative plain radiography, CT and MRI, postoperative plain radiography or CT).
Clinical and Radiological Data
All variables were obtained from patients’ medical records, radiological data (including DXA, preoperative MRI, CT scan, and plain anteroposterior and lateral radiography of the spine), and operative documents. The variables collected were as follows: (1) Baseline characteristics: age, sex, height, weight, body mass index (BMI), and bone mineral density (BMD) T-scores obtained from dual-energy X-ray absorptiometry (DXA); (2) Medical history-related variables: time interval from injury to admission, time interval from admission to surgery, history of OVCF, surgical history of PVP/PKP, history of chronic diseases (including hypertension, diabetes, coronary heart disease, cerebrovascular disease), use of steroid medication, use of anti-osteoporosis medication, surgical history of pedicle screw fixation, number of fractured vertebral bodies, number of surgically treated vertebral bodies, and location of fracture (thoracic, thoracolumbar (T11-L2), lumbar; (3) Operation-related variables: type of operation (PVP or PKP), puncture approach (unipedicular or bipedicular technique), the volume of bone cement, length of surgery time, and anesthesia technique. (4) Radiology-related variables: intervertebral cleft (IVC), cortical disruption, fracture type and severity, basivertebral foramen sign, the intrusion of the posterior wall.
The radiology-related variables were assessed by three spinal experts from the Department of Spine Surgery. The experts were blinded to both the participants’ characteristics and the statistical analysis.
Surgery Procedures
All surgeries were performed by skilled and experienced spinal surgeons from the Department of Spine Surgery, Zhongda Hospital affiliated with Southeast University. Preoperative preparation involved positioning the patient in a prone position and determining the puncture point and angle for the responsible vertebral body by preoperative fluoroscopic imaging. The skin was marked, followed by routine disinfection and draping. Anesthesia approaches included local anesthesia, intravenous anesthesia, and general anesthesia. The vertebroplasty needle was inserted into the vertebral body using either the unipedicular or bipedicular technique, based on the surface projection of the pedicles. Once the needle position was deemed satisfactory under lateral fluoroscopy, the needle core was withdrawn.
For patients undergoing PVP, the appropriate cement material (polymethyl methacrylate, PMMA) was injected into the responsible vertebral body using a pressure syringe under C-arm fluoroscopic guidance. For patients undergoing PKP, a working cannula was inserted into the vertebral body using the PKP surgical system. A balloon was then placed through the working cannula and inflated with a contrast medium until the vertebral body achieved the desired height. Once the desired height was reached, the balloon was deflated and withdrawn, and bone cement was introduced to fill the space in the vertebral body.
During cement injection, the “wiredrawing” or “toothpaste-like” phase was initiated. The distribution of bone cement was confirmed to be satisfactory under C-arm fluoroscopy.
The evaluation of bone cement leakage was based on intraoperative fluoroscopy.
Reference Standard
Definition of Radiology-Related Variables
1. IVC defined as an intravertebral transverse, linear, or cystic radiolucent shadow on preoperative CT; as a hypointense area similar to air on T1-weighted MRI sequences and on T2-weighted MRI sequences, or as a hyperintense area similar to cerebrospinal fluid on MRI STIR sequences.
8
2. Cortical disruption was characterized by clear discontinuity observed at the endplates or vertebral body wall on preoperative MRI or CT scans. 3. Fracture type and severity were assessed using Genant’s semi-quantitative classification based on lateral X-ray imaging.
9
Fracture type was classified into three types: wedge, biconcave, and crush. Fracture severity was categorized into mild, moderate, and severe based on the reductions of 20-25%, 26-40%, and >40%, respectively. In this study, reductions of less than 20% were also classified as mild. 4. The basivertebral foramen sign is characterized by the passage of the vertebrobasilar vein through the center of the vertebral body’s posterior wall, resulting in a triangular or irregular quadrilateral bone defect on CT sagittal images or a porous defect in the bone on CT axial images.
10
5. The intrusion of the posterior wall considered when the part of the posterior wall of the vertebral body protruded into the spinal canal on the axial CT image.
11
Definition of Bone Cement Leakage
Cement leakage was characterized as the presence of any cement outside the vertebral body. 3 Intraoperative fluoroscopy was performed for all patients during the procedure, and plain anteroposterior and lateral radiography or CT scans of the spine were conducted postoperatively to assess the occurrence of bone cement leakage.
Data Processing
Prior to developing the ML models, it was necessary to address missing data and normalize the data. For missing data imputation, variables with a missing value percentage exceeding 30% were excluded, while those below 30% were imputed using the k-nearest neighbors imputation strategy with a value of k set to 5. The dataset was then randomly split into a training set and a testing set, with an 8.5:1.5 ratio. Data normalization was performed by standardizing quantitative variables to have a mean of zero and a unit variance. The testing set was standardized based on the parameters derived from the training set. Categorical variables were encoded using the LabelEncoder functions from Scikit-Learn library.
Model Development and Interpretation
Model Development
We developed six ML models to predict bone cement leakage in PVA procedures. The models utilized the Extreme Gradient Boost classifier (XGBoost), Decision tree classifier (Decision Tree), Random Forest classifier (Random Forest), Gaussian Naive Bayes Classifier (GaussianNB), and support vector machines classifier (SVM), implemented using the Sci-Kit Learn package in Python (version 3.7.6).
To optimize the models’ performance, we employed a grid search approach to tune the parameters using the training set. The models were built based on the best parameters obtained from the grid search. Specifically, GaussianNB, Decision Tree, Random Forest, and SVM models were tuned manually, while the XGBoost model required parameter tuning for each parameter individually. Additionally, we implemented artificial neural networks (ANN) using the TensorFlow (version 2.3) Keras package. The ANN architecture comprised dense layers with a ReLU activation function. Dropout layers were incorporated after the dense layers to prevent overfitting. The gradient descent method was employed to minimize the loss function in the ANN model.
Evaluation of Performance
Various performance measures were calculated to assess the models’ performance on the test set: These measures included accuracy, precision, F1-score, recall, and the area under the receiver operating characteristic curve (AUC), which collectively provided a comprehensive evaluation of the discrimination ability of the ML models. To evaluate the predictive accuracy, calibration plots were utilized to compare the actual probability with the predicted probability. Furthermore, clinical decision curve analysis (DCA) was employed to evaluate the clinical utility of the ML models.
Interpretation and Visualization of the Model
Due to the inherent “black-box” nature of ML algorithms, understanding the underlying process and obtaining meaningful interpretations can be challenging. To address this limitation, we utilized SHapley Additive exPlanations (SHAP) to provide both global and local interpretations of the model.
For the best-performing model, we calculated the SHAP values for all features and obtained the mean SHAP values. These values were then utilized to create visual representations, including single sample force plots and summary plots. These plots were instrumental in visualizing the relationship between the prediction outcomes and each individual feature.
Statistical Analysis
The normality of distribution for continuous variables was assessed using the Shapiro-Wilk or Kolmogorov-Smirnov test. If a continuous variable followed a normal distribution, it was expressed as the mean ± standard deviation (SD), and the independent-sample t-test was used for the comparative analysis. However, if the variable did not conform to a normal distribution, it was presented as the median and interquartile range (IQR), and the Mann-Whitney U test was employed for the comparative analysis. Categorical variables were presented as frequencies and percentages, and the chi-square test was used for analysis. To identify independent risk factors for the occurrence of bone cement leakage, binary logistic regression analysis was conducted. A P-value <.05 was considered statistically significant. IBM SPSS Statistics version 24.0 (SPSS Inc, Chicago, IL, USA) was employed to perform the aforementioned statistical analyses.
Result
Patient Characteristics
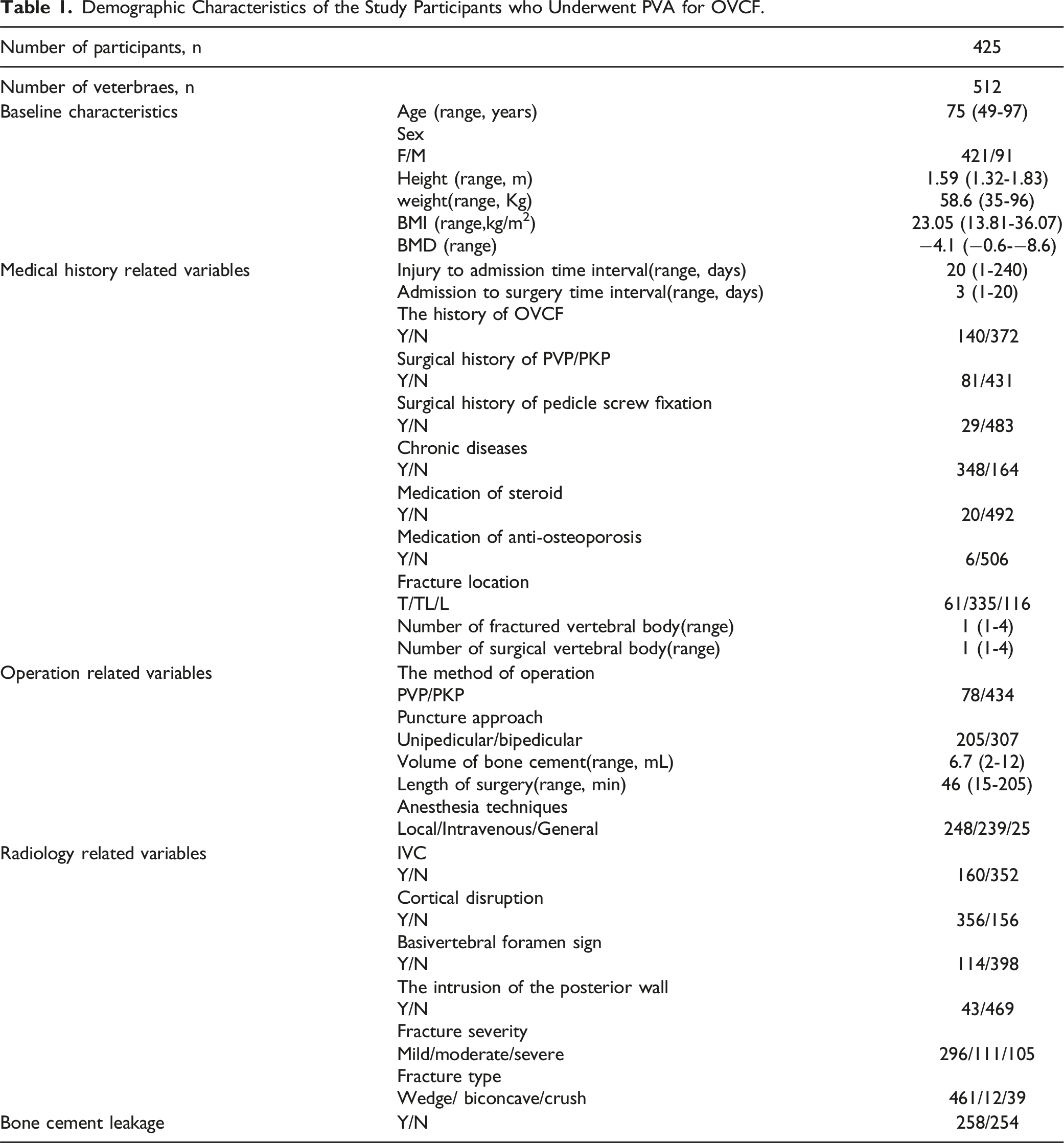
Demographic Characteristics of the Study Participants who Underwent PVA for OVCF.
Risk Factors
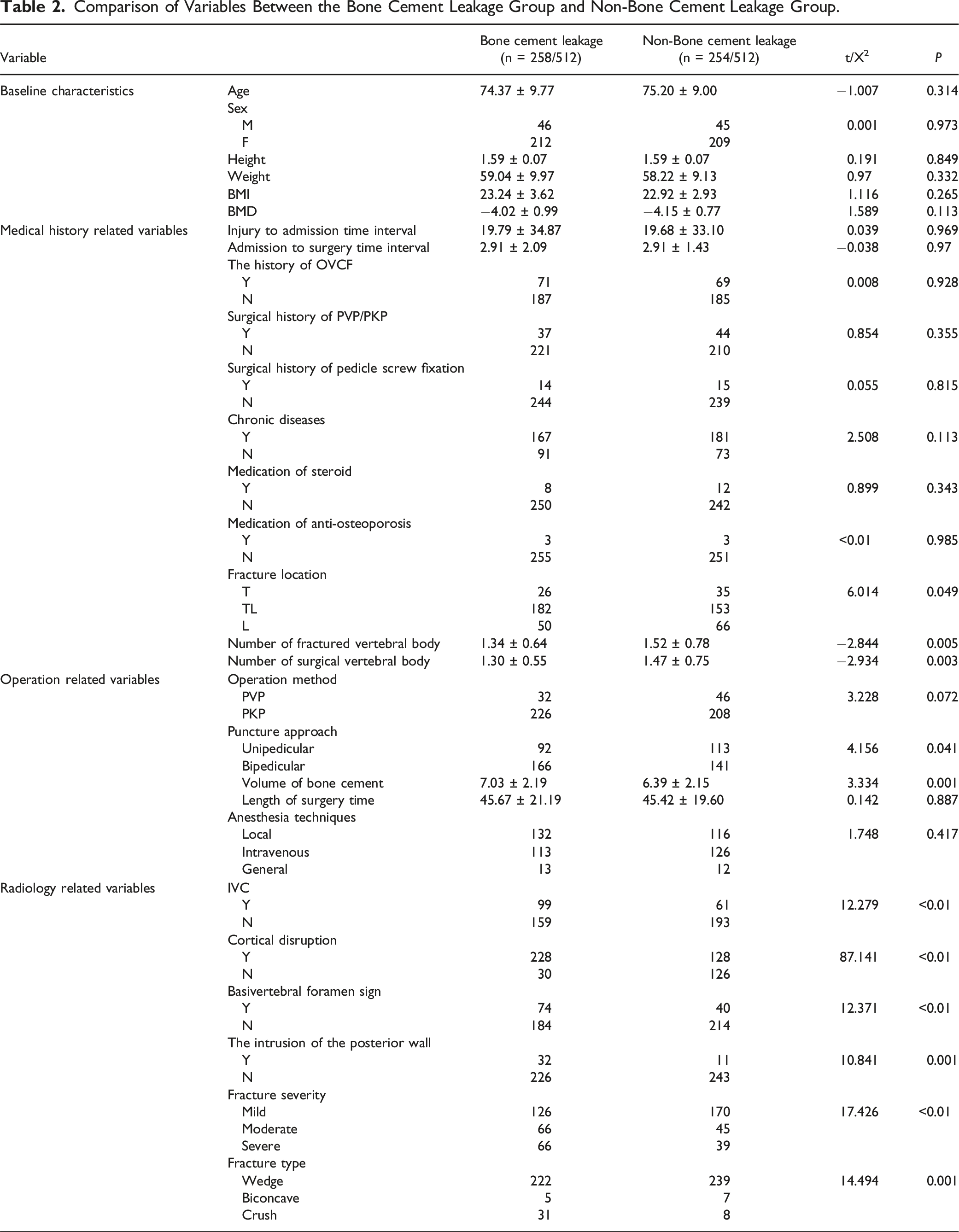
Comparison of Variables Between the Bone Cement Leakage Group and Non-Bone Cement Leakage Group.
Results of Binary Logistic Regression Analysis to Bone Cement Leakage after PVA.
Performance of Prediction Model
Results of Models for Bone Cement Leakage in PVA for OVCF.

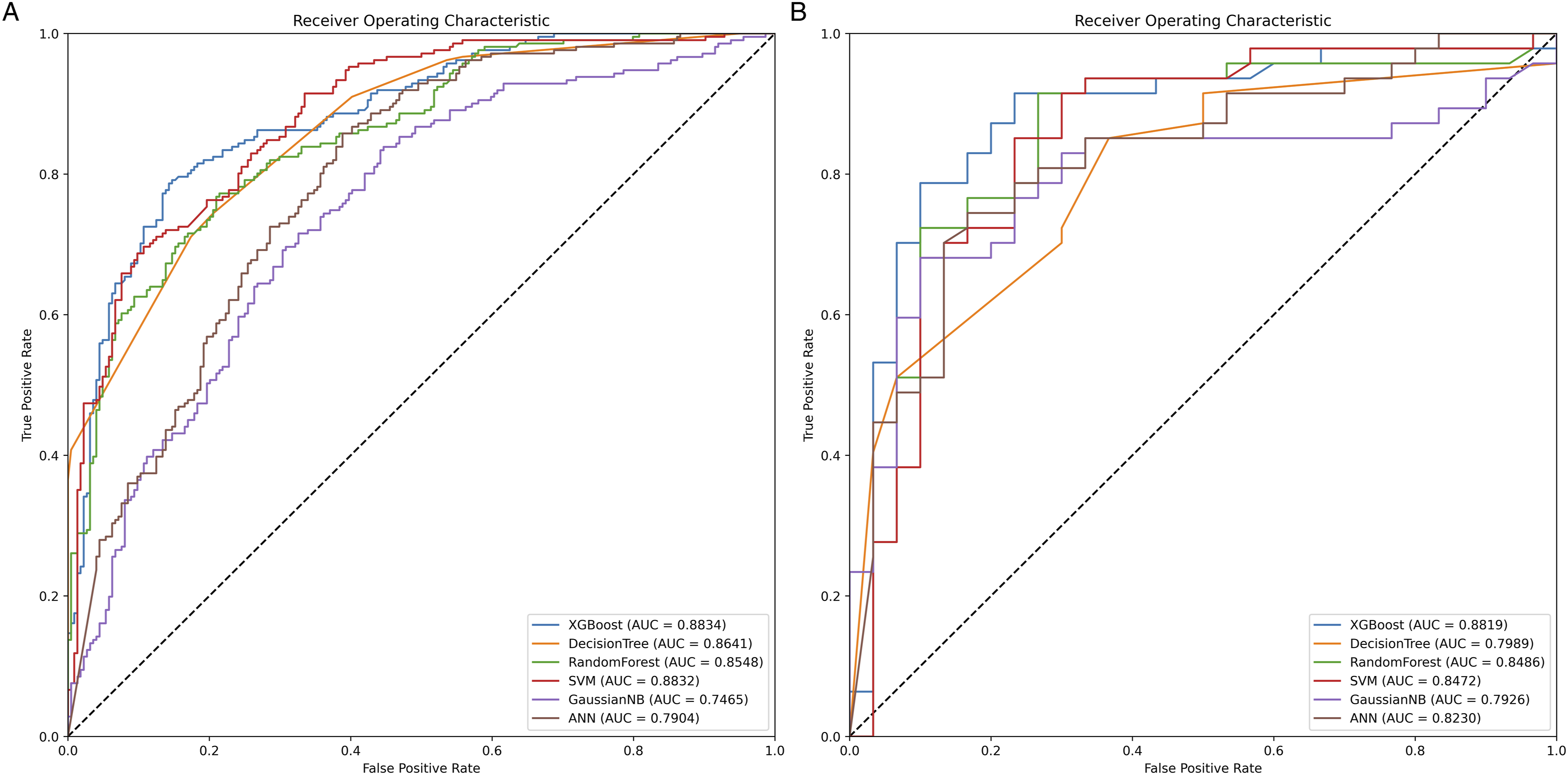
Receiver Operating Characteristic (ROC) Curves for 5 Machine Learning Models and 1 Deep Learning Model. The XGBoost model achieved a better Area Under the ROC Curve (AUROC) compared to the other models. (a) ROC curve for the training set; (b) ROC curve for the testing set.
The calibration plot in Figure 2 demonstrates a favorable predictive accuracy between the actual probability and the predicted probability. Calibration Plots of 5 mL Models and 1 dL Model.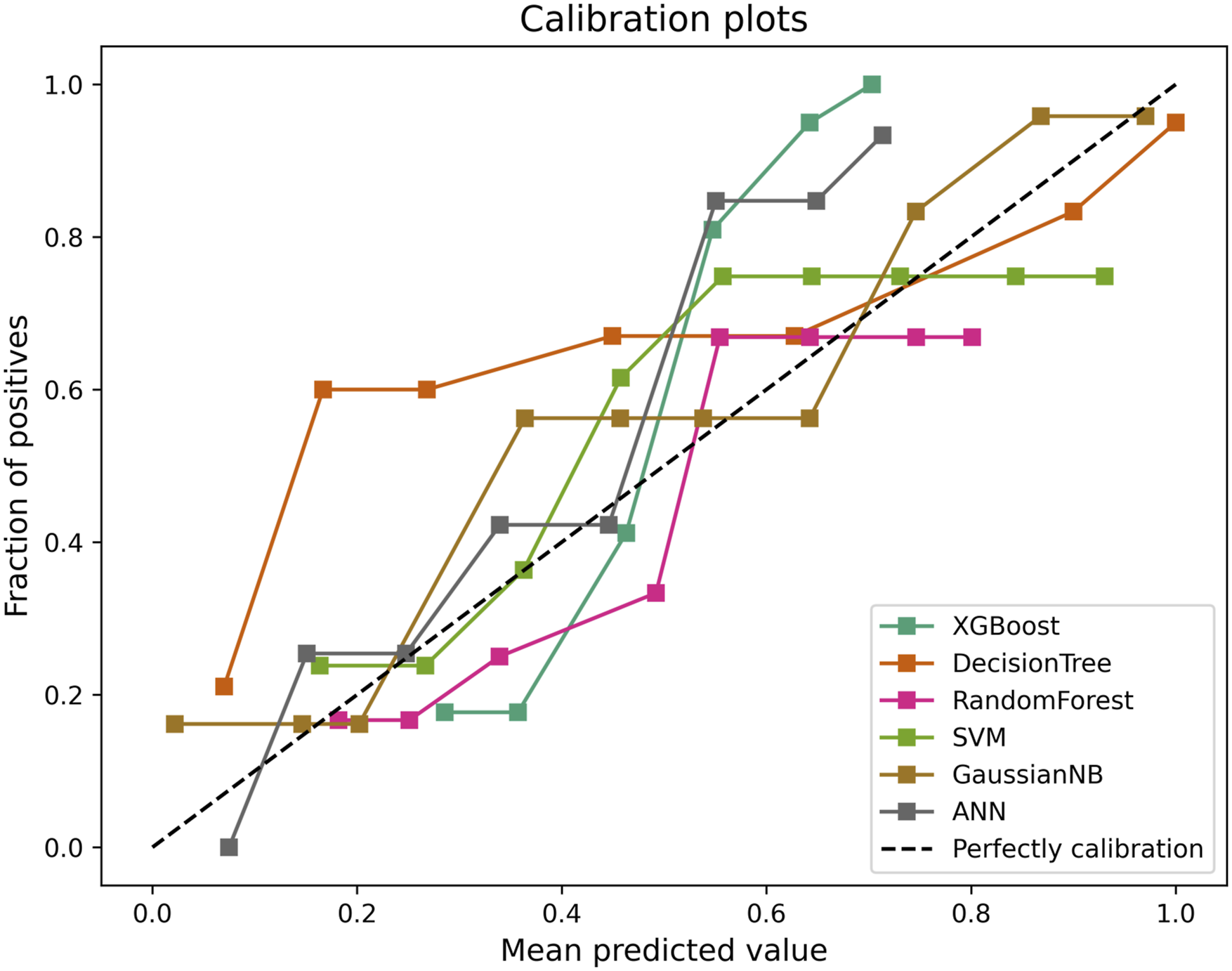
To assess the clinical utility of the predictive model, the DCA curve was employed. Figure 3 presents the comparison of the six models. Decision Curve Analysis for 5 mL Models and 1 dL Model. (a) ANN; (b) Decision tree; (c) GaussianNB; (d) Random Forest; (e) SVM; (f) XGBoost.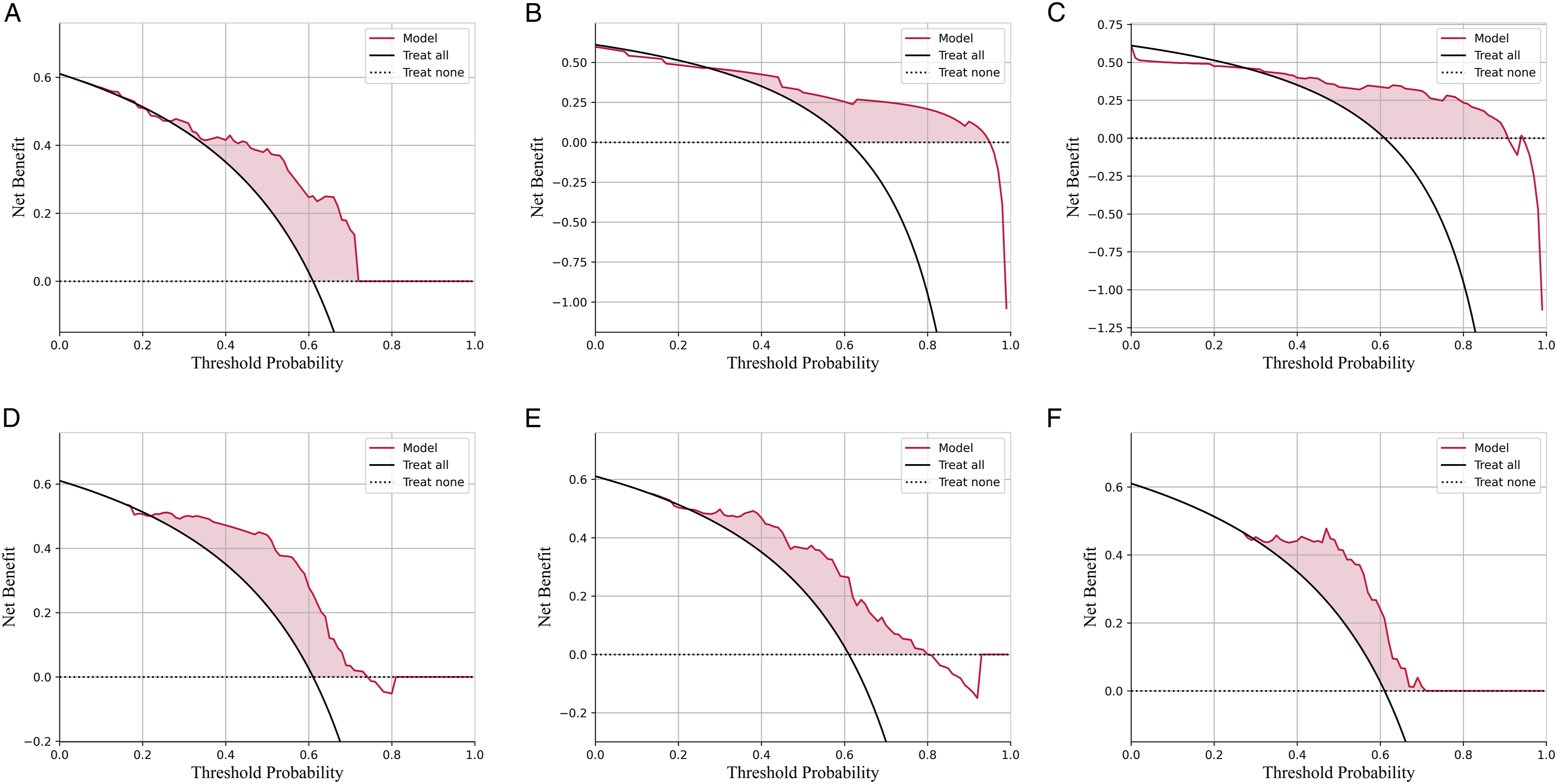
In summary, the XGBoost model exhibited the best performance in this study.
Visualized Interpretation of Feature Importance and Personalized Predictions
Visualized Interpretation of Feature Importance
The XGBoost model was selected to calculate the SHAP values for all features using the SHAP package. Based on these results, summary plots and force plots were generated to visually explore the relationship between the prediction outcomes and each individual feature. Figure 4(a) depicts all the evaluated risk factors by their average absolute SHAP values, while Figure 4(b) showcases the top 10 most important features in our model. Model Interpretation. (a) Importance ranking of the top 10 risk factors with stability and interpretation using the optimal model. (b) Importance ranking of the top 10 variables based on the mean |SHAP value.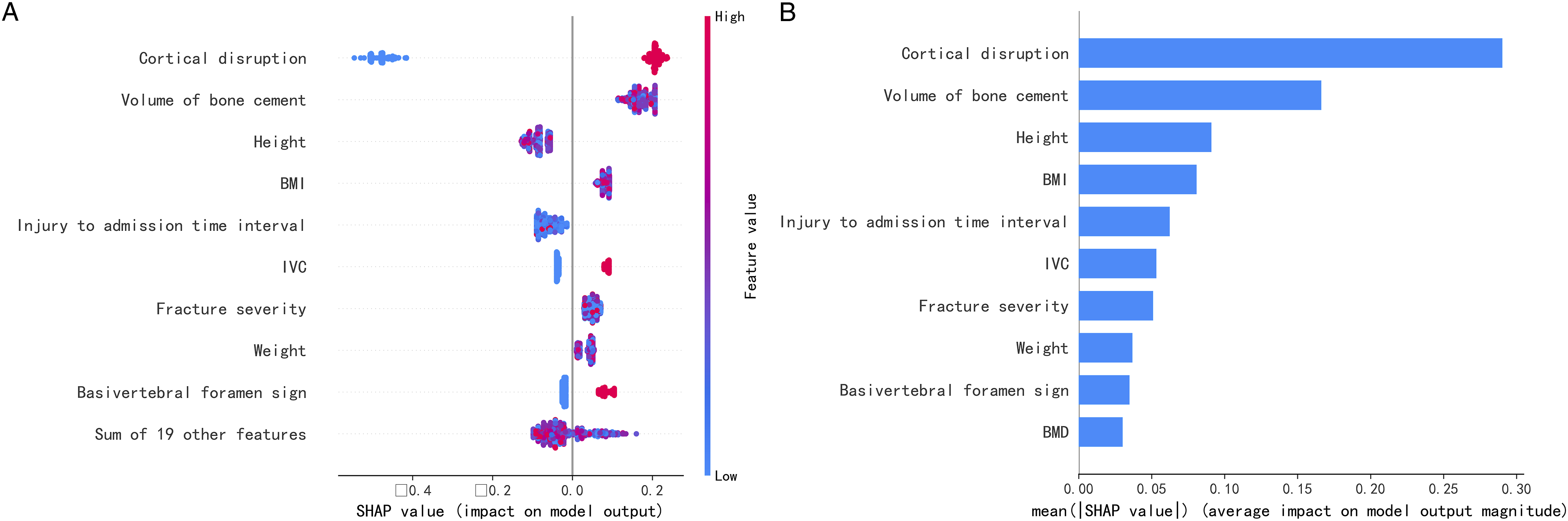
According to the summary plot, features such as cortical disruption, volume of bone cement, height, BMI, injury to admission time interval, IVC, fracture severity, weight, basivertebral foramen sign, and BMD played decisive roles in the predictive models.
Risk factors were assessed by examining the scatter plot generated by the SHAP package in combination with their clinical significance. The scatter plot revealed relatively high absolute SHAP values for cortical disruption, IVC, and basivertebral foramen sign, with clear distinctions in the distribution of SHAP values. It is important to note that a SHAP value of zero for a feature indicates that it had no impact on the model’s output.
Interpretation of Personalized Predictions
The force plot for a single patient, depicted in Figure 5, illustrates the influence of each feature on the predictive outcomes in terms of high risk and low risk of bone cement leakage. The blue and red arrows represent the impact of each feature. A blue arrow indicates that the feature reduces the risk of bone cement leakage, while a red arrow indicates an increased risk. The width of the arrow corresponds to the contribution made to the predictive value. To demonstrate the interpretability of the model, we provide two random examples: one patient who experienced bone cement leakage following PVA, and another patient who did not. Interpretation of Model Prediction Results Using Two Sample Cases (a) a patient who didn’t experience bone cement leakage following PVA; (b) a patient who experienced bone cement leakage following PVA.
Discussion
This study developed interpretable ML models that integrate clinical features and radiographic signs to predict the risk of bone cement leakage after PVA in OVCF. All models demonstrated favorable performance, with the XGBoost model outperforming GaussianNB, Decision Tree, Random Forest, SVM, and ANN models. The superior predictive performance of the XGBoost model indicates its potential for accurate and reliable risk assessment in clinical settings. By computing SHAP values and mean values, the XGBoost model enabled both global and local interpretations. The key features found to play a decisive role in the predictive models, considering their clinical significance, include cortical disruption, volume of bone cement, BMI, injury to admission time interval, IVC, fracture severity and type, basivertebral foramen sign, and BMD. Additionally, two examples are provided to illustrate the model’s capability in predicting cement leakage and assessing the relative importance of each variable. These findings empower clinicians to identify high-risk bone cement leakage patients, enhance their understanding of the significance of features in overall and individual prediction models, and support clinical decision-making aimed at reducing the incidence of bone cement leakage while improving patient outcomes.
As populations age, there is a concomitant rise in the prevalence of osteoporosis and the subsequent risk of osteoporotic fractures. PVA is a minimally invasive surgical procedure that is recommended and extensively employed for patients experiencing acute symptomatic OVCF. Nevertheless, the postoperative complication of bone cement leakage poses a significant concern, given its potential to result in severe complications or even fatalities when symptoms emerge. This drawback contradicts the procedure's benefits, such as minimal invasiveness, rapid recovery, and early discharge from bed rest. Literature reports an incidence of bone cement leakage varying between 5-82%. 7 Our study, which retrospectively evaluated 512 fractured vertebrae, found an incidence of bone cement leakage at 50.4%. This result aligns with studies that utilized postoperative radiography to assess leakage, although it is slightly less than those that exclusively relied on postoperative CT scanning.
Numerous prior studies that have compared the incidence of bone cement leakage by employing different surgical strategies 12 or by accounting for specific factors (like the volume and viscosity of bone cement 13 ) have identified a lower occurrence of cement leakage in certain situations. This suggests a potential for prevention. Consequently, the preoperative prediction of bone cement leakage carries substantial clinical importance. The study by Li et al demonstrated that predictive models using nomograms and ML can be developed to forecast bone cement leakage after PVP, based on the associated risk factors.7,14 Deng et al retrospectively examined 374 cases of thoracolumbar OVCFs treated with single-level PVP. They sifted through data and variables using four ML algorithms and formulated a nomogram prediction model based on six variables, which demonstrated reliable predictive power. 15 There was a similar study on prediction models for constructing nomograms for intradiscal type leakage. 16
Previous models, however, do not integrate radiographic signs, which align more closely with the clinical process, and lack comparison among various deep learning models. In our research, we included 28 features, encompassing radiographic-related variables, into our predictive models. The AUC in the testing set spanned from .7926 to .8819. The predictive performance of our model resembles the ML model used in earlier studies, 7 surpassing the performance of nomogram predictive models.14,15 The SHAP package underscored the importance of features, with imaging indicators distinctly contributing in a manner that diverges from prior models. Examining the imaging features carrying significant weight in the predictive results reveals that adjusting the puncture angle and depth, along with optimizing the timing and volume of cement injection, could effectively minimize the risk of bone cement leakage during PVA.
In this study, 5 ML model classifiers and 1 deep learning model classifier were used, and the above models are widely used in spinal diseases, including the field of diagnosis, treatment and prognosis for spinal degenerative diseases, trauma, spinal tumors, etc. In diagnosis, the application of ML algorithm achieved high diagnostic accuracy in disease prediction and differentiation, primarily utilizing radiological imaging. Hao Zhang et al 17 established Gaussian naïve Bayes (GNB), K-nearest neighbor (KNN), logistic regression, multilayer perceptron (MLP), Decision Tree, linear discriminant, and gradient-boosting decision tree classifiers models, combined radiomics to differentiate benign from malignant indistinguishable vertebral compression fractures with improved diagnostic efficacy. Jun Zhang et al have differentiated acute and chronic vertebral compression fractures by similar ML models combined radiomics features and deep transfer learning features. ML has been incorporated into treatment decision-making processes such as surgical grade, instrumental vertebrae, and correction range. 18 For surgical correction of thoracolumbar adult spinal deformity, an ANN successfully mimicked lead surgeons’ decision making in selection of the upper instrumented vertebra. 19 An increasing number of ML models have been used to predict prognosis, such as clinical outcomes and complications. Sung Tan Cho et al 20 have used Decision Tree and Random Forest models to analysis prognostic factors for the progression of OVCF following conservative treatment. Zhang et al 21 have built XGBoost, logistic regression, Random Forest, AdaBoost, GNB, ComplementNB, MLP, SVM, and KNN machine learning models to predict delirium in patients after surgery for degenerative spinal disease. Among them, XGBoost models was practical and had a good performance. Ren et al 22 also established similar ML models to predict Recurrent Lumbar Disc Herniation Following Percutaneous Endoscopic Lumbar Discectomy. Based on the previous literatures review and the experience of our group, we chose the above models to predict bone cement leakage. Of the models used in our study, the XGBoost model displayed superior predictive performance, even surpassing deep learning algorithms. Despite deep learning models’ strengths in areas such as images, language, and audio, some researchers have posited that, with tabular data, it is simpler to achieve robust predictions using tree-based methods rather than deep learning. 23
Binary logistic regression analysis in our research showed that cortical disruption, basivertebral foramen, fracture type, and the volume of bone cement were independently linked with bone cement leakage post-PVA in OVCF. The interpretation of SHAP demonstrated that features such as cortical disruption, volume of bone cement, BMI, injury to admission time interval, IVC, fracture severity, basivertebral foramen, and BMD play a pivotal role in the predictive model. This does not completely align with the results of previous studies, as shown in the feature importance analysis.7,24,25 Radiology-related variables such as cortical disruption, IVC, fracture severity and type, and basivertebral foramen hold a key position in the predictive model, underscoring the necessity of their inclusion.
When considering risk factors for bone cement leakage following PVA, prior studies have not provided definitive evidence, leaving some risk factors contentious. Drawing from the results of binary logistic regression analysis and feature importance analysis conducted in this research, in conjunction with their clinical significance, we can deduce that factors such as cortical disruption, IVC, fracture severity and type, basivertebral foramen, BMI, BMD, volume of bone cement, and injury to admission time interval play a significant role in contributing to bone cement leakage in PVA.
Cortical disruption emerged as the primary risk factor, aligning with previous research findings. 26 A higher degree and certain types of fractures indicate more severe cortical disruption which amplifies the risk of bone cement leakage. This is particularly the case with end plate-associated intradiscal types, which heighten the risk of new adjacent vertebral fractures. 6 The concept of IVC was initially proposed in relation to Kummell’s disease, where it is considered a hallmark feature, 27 indicating avascular necrosis of the vertebral body and severe collapse. According to Zhang, K et al, IVC is not only a risk factor for type-C leakage but also acts as a protective factor against type-S leakage (segmental venous leakage). 10 This is possibly attributable to the lower stress within the vertebral body spaces during cement injection as compared to a compressed vertebral body, thereby allowing room for the cement to fill, and consequently reducing cement leakage. 28 This phenomenon may also be associated with the phase of IVC, which contains liquid or gas. 29 The basivertebral foramen is an independent risk factor for type-B leakage, 10 as the bone defect in the posterior wall of the vertebral body provides a natural passage for bone cement leakage. 30 A study by Wang et al 31 uncovered a link between the basivertebral foramen and IVC, which can directly cause bone cement leakage after PKP in elderly OVCF patients. The volume of bone cement emerged as a risk factor for bone cement leakage in both binary logistic regression analysis and feature importance ranking. There is no positive correlation between the volume of bone cement and clinical effectiveness, including pain relief and restoration of vertebral body height. However, an increase in bone cement volume elevates the risk of bone cement leakage. As such, selecting the optimal volume of bone cement is imperative to maximize clinical effectiveness and minimize bone cement leakage. The volume fraction percentage (VF%), which represents the ratio of intravertebral cement volume (IVCV) to fractured vertebral body volume (FVBV), has been proposed to assess the optimal volume of bone cement. 32 Nieuwenhuijse et al 33 suggested an optimal value of 24%. Clinicians should undertake an individualized evaluation of each patient to determine the suitable volume of bone cement. A lower BMD, indicative of a higher grade of osteoporosis, suggests larger trabecular space for bone cement injection and lower injection pressure, thus, facilitating the reduction of bone cement occurrence. 34 However, a higher degree of osteoporosis also leads to more severe fracture damage, potentially resulting in leakage from the weaker cancellous bone into the venous system. 35 In recent years, the Subcutaneous fat index (SFI) has been proven to be a more important evaluated variable for obesity than BMI. 36 It was not used in the study because previous literatures did not analyze it as a risk factor for bone cement leakage. Further studies will be conducted to objectively evaluate the image-related features including SFI, and create more efficient predictive and generalized model by using deep learning and radiomics techniques.
This study does come with several limitations. Firstly, as a single-center retrospective study, the data were exclusively sourced from the Department of Spine Surgery, Zhongda Hospital affiliated with Southeast University, warranting further validation of generalizability and potential recalibration when implemented by other medical institutions. Secondly, data from multiple centers should be incorporated into the model development and its internal and external validation. Thirdly, in this study, considering the high-risk population of osteoporotic vertebral compression fracture, only over 45 years of age patients were included in the analysis, which resulted in a certain degree of bias, and subsequent studies will further expand the population to improve the generalizability of the model. Fourthly, Fewer male patients were included in this retrospective study, as a proof of concept, the limited gender proportion and sample size demonstrated the effectiveness of the ML model, but a more rational gender ratio and the sample size expansion need in future research. Fifthly, this study predominantly assessed bone cement leakage using postoperative radiography, with CT not routinely employed. Although postoperative radiography can evaluate bone cement leakage, the gold standard for bone cement leakage assessment remains postoperative CT, which should be more frequently applied in future studies.
Conclusion
In our investigation, we formulated six distinct prediction models for bone cement leakage following PVA in OVCF patients. The XGBoost model demonstrated superior predictive capacity for bone cement leakage. This interpretable model can offer a visual representation of feature importance and individualized prediction. The predictive outcomes could aid medical practitioners in preoperative assessment of the risk of bone cement leakage, allowing comprehensive consideration of clinical characteristics. This, in turn, could help the development of more tailored treatment strategies or preoperative interventions to decrease the occurrence of cement leakage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the National Natural Science Foundation of China (82202768), Jiangsu Provincial medical Key Discipline (Laboratory) Cultivation Unit (JSDW202222).