
Abstract
Study Design
A retrospective cohort study.
Objective
To evaluate the utility of routine preoperative urinalysis as a predictor of postoperative complications following elective lumbar fusion surgery (ELFS).
Methods
This study included a retrospective review of patients aged ≥18 years-old who underwent ELFS for degenerative pathology between 2018 to 2022 at a single academic institution. Patients were categorized into 3 groups: No Urinalysis (No-UA), Negative Urinalysis (Negative-UA), and Positive Urinalysis (Positive-UA). A retrospective review of medical records was conducted including patient characteristics and clinical factors of interest. Emergency department (ED) visits and return to the operating room (OR) within 3-months postoperatively were recorded. Statistical analyses were performed using bivariate and multivariate analysis.
Results
A total of 493 patients were included. Despite having higher rates of preoperative antibiotics administered, patients with a positive urinalysis were significantly more likely to present with postoperative urinary tract infections (UTIs) than the No-UA and Negative-UA groups. No significant differences were seen in other types of complications including pneumonia, bacteremia, superficial wound infections, deep wound infections, and wound dehiscence between the 3 groups. Additionally, rates of return to OR, return to ED, reinsertion of foley catheters, duration of indwelling catheterization, and hospital length of stay had no significant differences between the groups.
Conclusion
This study suggests there may be a limited role in performing routine preoperative urinalysis prior to ELFS. This study may help further improve preoperative assessment guidelines and assist with patient counseling and considerations prior to elective lumbar fusion surgery.
Introduction
Preoperative assessments with urinalysis (UA) are commonly performed for risk stratification of patients undergoing elective lumbar fusion surgery. This preoperative screening method aims to help reduce potential postoperative complications such as urinary tract infections and wound complications. 1 However, the utility of preoperative UA prior to surgical procedures continues to be debated. Current guideline consensus does not recommend patients to undergo routine UA prior to surgery, unless the operation involves urologic procedures or the placement of foreign material such as prosthetic joints or valves. 2 Previous case series have reported abnormal UA results in up to 34% of patients; however, less than 1% of these patients experienced an adverse postoperative outcome. 3 Prior research has also reported a poor predictive value of routine preoperative UA in assessing an increased risk of postoperative complications. 4
Furthermore, there has been a 62.3% increase in the number of elective lumbar fusion procedures for degenerative pathologies over the past 2 decades between 2004 and 2019.5,6 With this significant increase in volume, there are growing concerns of unnecessary antibiotic prescription and utilization for asymptomatic bacteriuria prior to surgical operations, leading to increased risks of antibiotic resistance, adverse drug reactions, and increased healthcare costs. 7 Previous data reports approximately $50 million in 10-year aggregate savings with the elimination of unnecessary UAs and an additional $5 million in savings with the reduction of inappropriate antibiotic treatment. 8 In addition to increased hospital costs, both patients and hospital systems are at increased risks of C. difficile spread and infection following unnecessary antibiotic utilization.9,10
Despite limited evidence in the literature suggesting significant benefits for performing preoperative UAs prior to surgical procedures, this routine screening method continues to be implemented in elective lumbar fusion surgeries. However, the benefits of UAs in predicting postoperative complications remains unclear within this context. The purpose of this study was to assess the utility of routine preoperative UA as a predictor of postoperative infections, wound dehiscence, and short-term return to the emergency department (ED) or operating room (OR) in patients undergoing elective lumbar spine fusion surgery.
Methods
This retrospective study was approved by the Institutional Review Board (IRB ID: 2139637-1). Informed consent was not required for this study. Patients aged ≥ 18 years undergoing elective, instrumented lumbar or lumbosacral fusion surgery for degenerative pathology at a single academic institution between 2018 to 2022 met the inclusion criteria. Patients who underwent surgery for trauma, tumor, and/or deformity were excluded from the study. Patients who met the inclusion criteria were classified into 3 groups: No Urinalysis (No-UA), Negative Urinalysis (Negative-UA), and Positive Urinalysis (Positive-UA). A Positive-UA criteria was met if the patient had at least one of the following: positive nitrites, positive leukocyte esterase, presence of bacteria, and >10 WBC HBF. Patients with a Positive-UA were further categorized by either a positive or negative urine culture. For patients who had a Positive-UA, a confirmatory UA demonstrating negative UA after antibiotic treatment was not obtained prior to proceeding with surgery. A retrospective review of medical records was conducted including patient characteristics, rates of intervention due to urinalysis, and rates of postoperative infections and wound dehiscence. Postoperative complications within 3-months after surgery were categorized into 6 groups: urinary tract infections (UTIs), pneumonia, bacteremia, deep wound infection, superficial wound infection, and wound dehiscence. Postoperative UTIs were diagnosed with symptomatic testing and not routine testing. Emergency department utilization and return to the operative room within 3-months postoperatively were recorded. The primary outcome of this study assessed for significant differences in postoperative infections based on whether the patients had No-UA, Negative-UA, or Positive-UA. Secondary outcomes included evaluating for differences in return to ED, return to OR, hospital length of stay, and use of foley catheters.
Statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS). Bivariate and multivariate analyses were performed to determine the utility of routine preoperative urinalysis and whether it was associated with postoperative complications. Univariate and multivariate analyses were performed using Chi-Square (categorical variables), ANOVA (comparison of means, continuous variables) and logistic regression, respectively. For each statistical model, a P-value of less than 0.05 (P < 0.05) was considered statistically significant.
Results
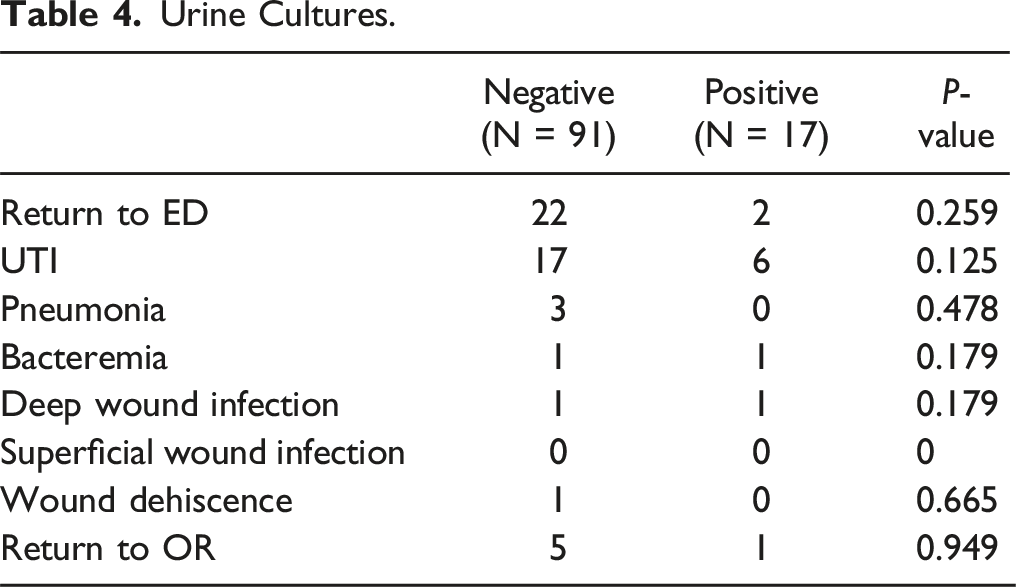
This study included 493 patients who met the inclusion criteria: 53 No-UA, 333 Negative-UA, and 107 Positive-UA. 440 (89.2%) patients underwent a preoperative urinalysis screening. The average age of patients was 65.3 years and 267 (54.2%) were male. The average time between preoperative UA and operative date was 13.9 days. In patients with a positive urinalysis, 18 (16.8%) of them returned a positive culture. Patients in the positive-UA group (N = 21; 19.6%) were significantly more likely to receive preoperative antibiotics than patients in the No-UA (N = 1; 1.9%) and Negative-UA (N = 0; 0%) groups (P < 0.05). Patients with a positive UA (N = 23; 21.5%) also presented with higher rates of postoperative urinary tract infections than patients in the No-UA (N = 2; 3.8%) and Negative-UA (N = 17; 5.1%) groups (P < 0.05). However, there were no significant differences in the rates of pneumonia, bacteremia, deep wound infections, superficial wound infections, and wound dehiscence between the 3 groups (P > 0.05). There were also no significant differences in return to OR, return to ED, reinsertion of foley catheters, duration of indwelling catheterization, and hospital length of stay (P > 0.05). The rate of catheterization in the patient group was 453 patients (91.8%), with 24 patients (4.9%) requiring replacement after surgery.
Demographic Characteristics Between Three Groups.
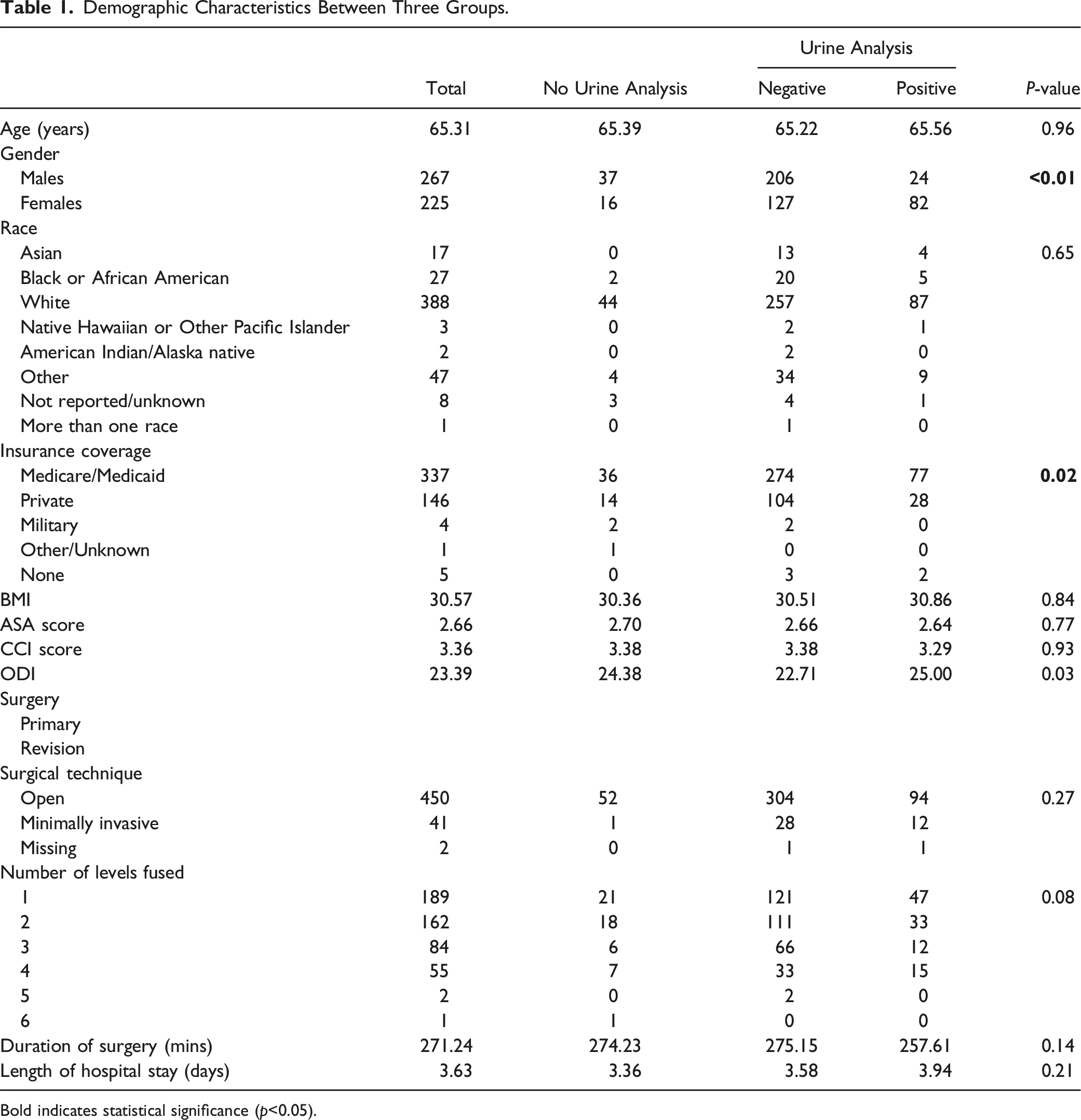
Bold indicates statistical significance (p<0.05).
Interventions.
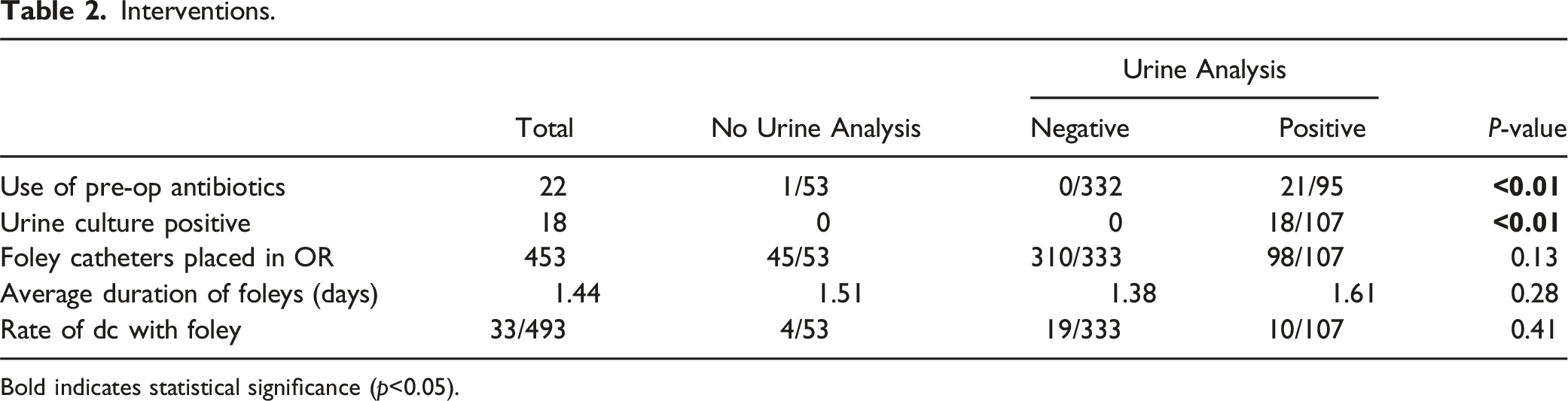
Bold indicates statistical significance (p<0.05).
Complications.
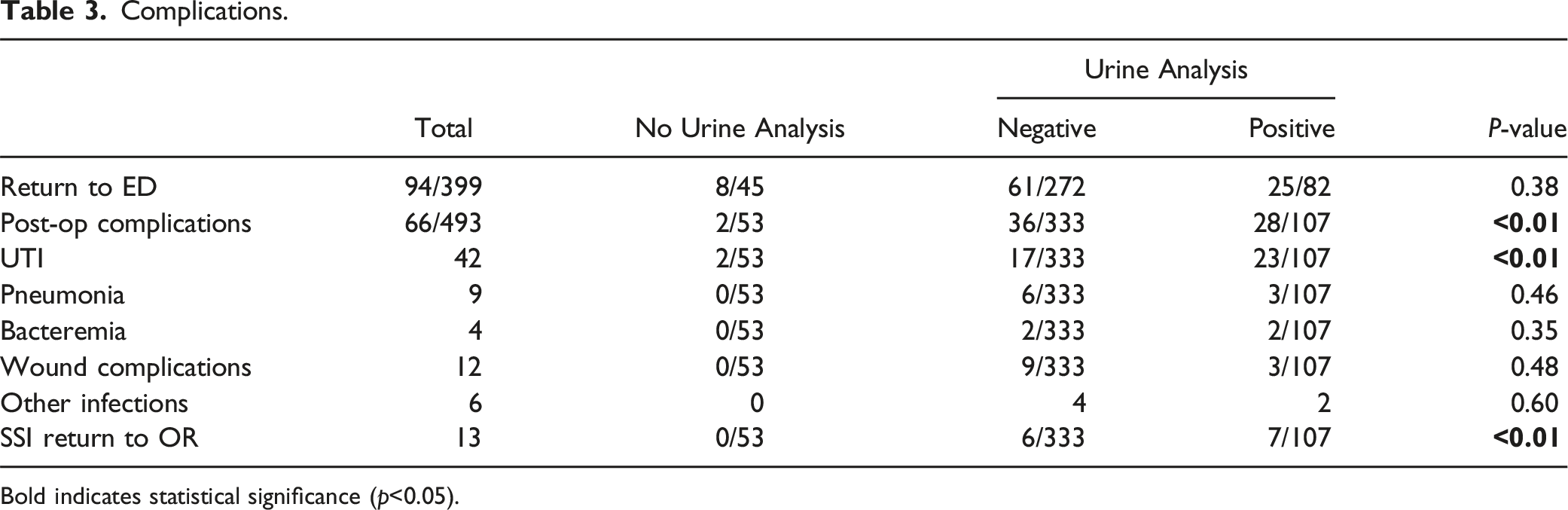
Bold indicates statistical significance (p<0.05).
Urine Cultures.
Antibiotics.
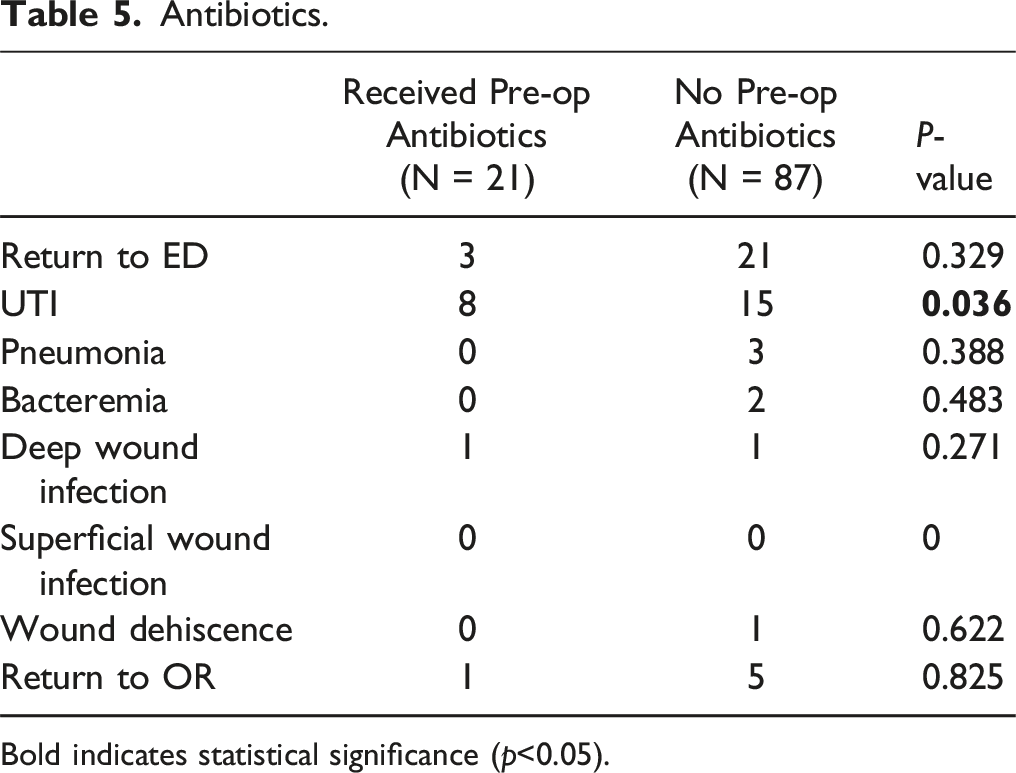
Bold indicates statistical significance (p<0.05).
Univariate and Multivariate Analyses: UTI Complications.
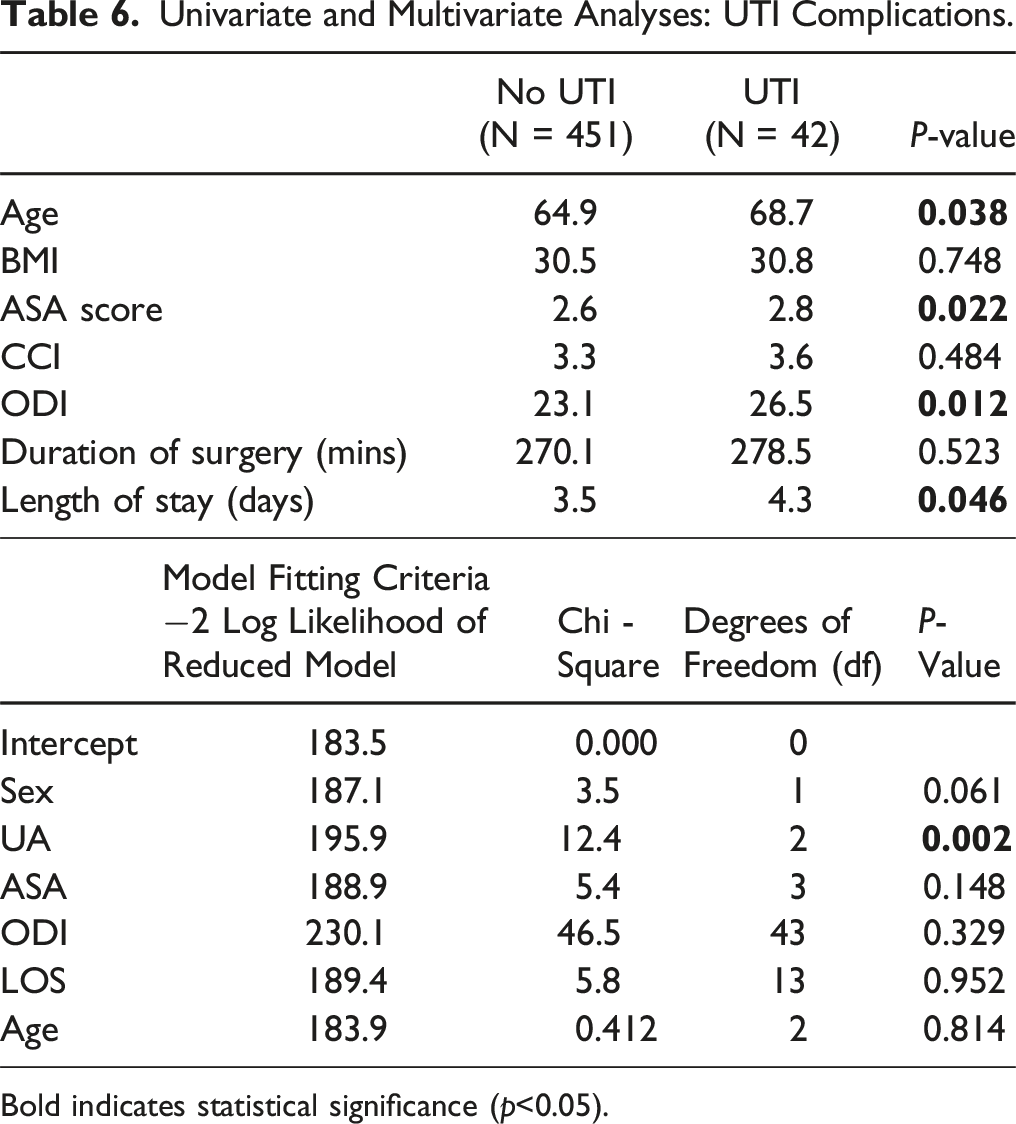
Bold indicates statistical significance (p<0.05).
Univariate Analyses: Surgical Site Infections.
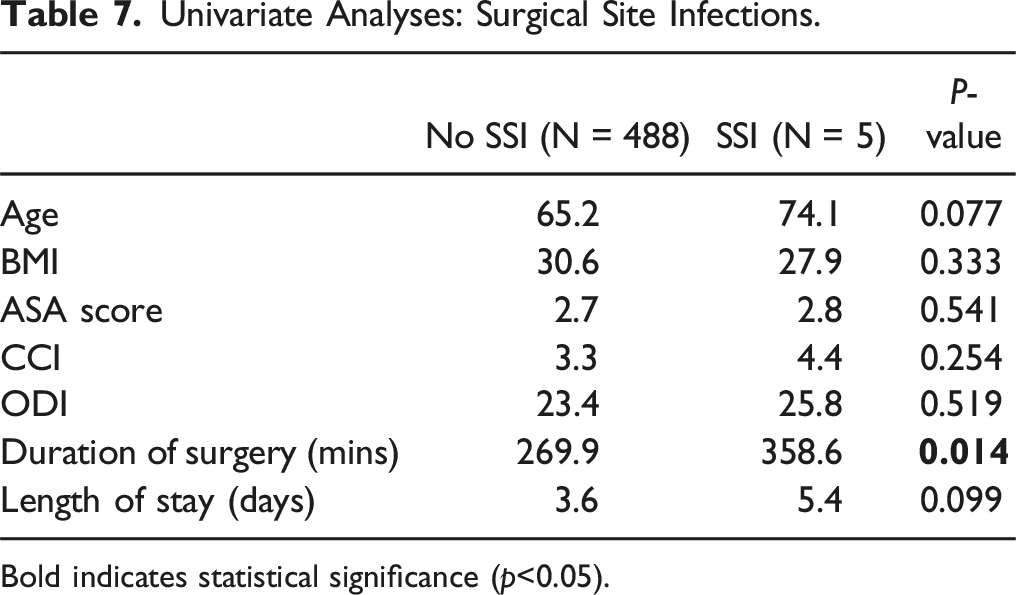
Bold indicates statistical significance (p<0.05).
Univariate Analyses: ‘Other’ Complications.
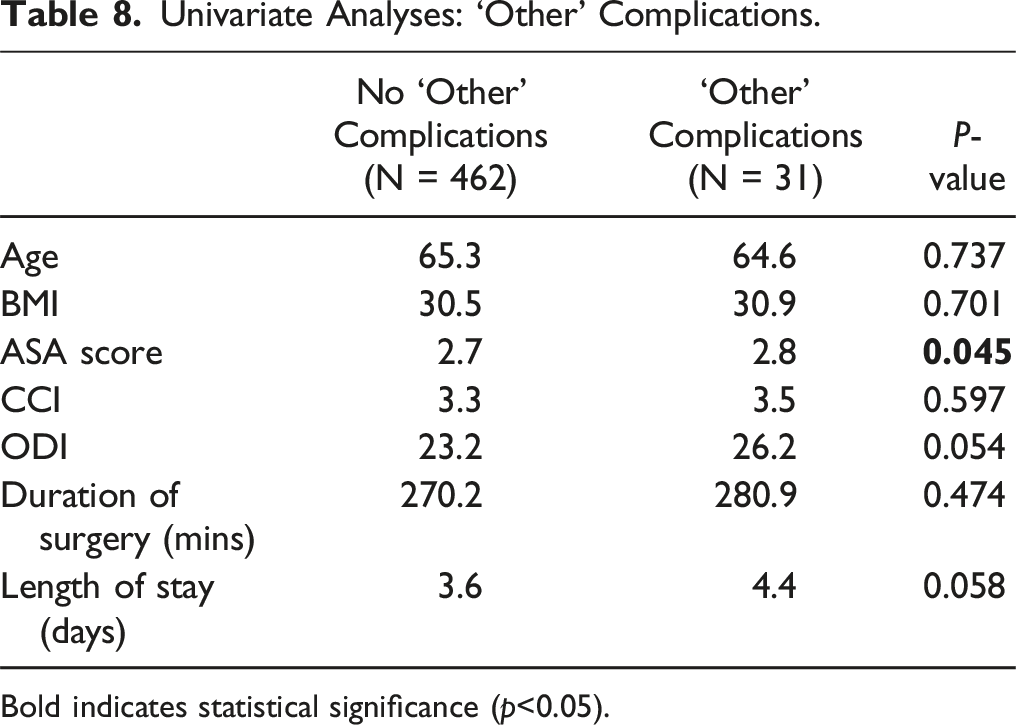
Bold indicates statistical significance (p<0.05).
Discussion
In this study, we aimed to assess whether routine preoperative urinalysis tests were predictive of postoperative complications following elective lumbar fusion surgery. Current guidelines supported by the Infectious Disease Society of America and the American Society of Anesthesiologists do not recommend preoperative urinalysis screening prior to non-urologic operations in asymptomatic patients.11-13 However, routine preoperative urinalysis screening methods continue to be widely used in orthopaedic practices. In this study, 89.4% of the patients had a preoperative urinalysis done prior to surgery. The results indicate that routine preoperative urinalysis tests are often limited in predicting postoperative complications following elective lumbar fusion surgery. Although patients in the positive-UA group did present with a higher rate of postoperative UTIs, this increase did not translate to increased risks for other postoperative complications (e.g. return to ED, return to OR, pneumonia, SSIs) compared to negative-UA and No-UA groups. Amongst patients in the positive UA group that returned to the OR for surgical site infections, only one patient had an intraoperative wound culture that matched the preoperative urine culture. The lack of differences found between these groups when considering postoperative complications supports current guidelines that do not recommend preoperative UAs prior to surgery under most cases. With the increased risks of postoperative UTIs seen in the positive-UA group, it is also unclear if the use of a UA as a screening tool helped prevent the increased risk of postoperative UTIs that was identified in this analysis.
Preoperative antibiotic usage was also significantly increased in the positive-UA group (N = 21; 19.6%) when compared to the other two groups. Although this may have been noted as necessary to help reduce the risk of postoperative UTIs, only one patient in our sample had a postoperative urine culture that matched the preoperative urine culture for urinary tract complications. Additionally, there were no significant differences in other types of postoperative complications, regardless of whether the patients received preoperative antibiotics. This highlights the potential overutilization of antibiotics in patients without a clear benefit or reduction in postoperative complications, which may result in antibiotic resistance, increased costs, and adverse side effects in patients. 11 Previous research has also explored the utility of routine preoperative urinalysis in a variety of surgical procedures. In a study by Hollenbeck et. al, the authors explored whether the rates of surgical site infections, catheter-associated UTIs, and antibiotic prescriptions changed following the elimination of routine urinalysis screening for elective total joint arthroplasty patients. The results of their study indicated a 93% reduction in antibiotic utilization with no significant differences in surgical site infections and catheter-associated UTIs postoperatively. 7 Additionally, a study by Sousa et al. found that majority of the prosthetic joint infections following elective total joint arthroplasty procedures were due to microorganisms different than the isolates identified on preoperative UA screening. 14 A similar study by Honkanen et al. also reports a lack of association between preoperative bacteriuria and increased risks of periprosthetic joint infections. In the case of a periprosthetic joint infection, their study indicated the causal pathogen was different from the pathogen identified in the preoperative urine culture. 15 Furthermore, the results in a study conducted by Hellinger et al. reports a 82.8% decrease in inappropriate antibiotic treatment for asymptomatic bacteriuria following the cessation of screening urine cultures, which was associated with no increase in surgical site infections after spinal fusion, laminectomy, knee replacement, and hip replacement operations. 16 In agreement with the prior studies, our study further supports the notion that there is limited utility in performing routine preoperative UA screening in asymptomatic patients.
Two previous studies reported in the literature indicated a significant association between asymptomatic bacteriuria and postoperative prosthetic joint infection.17,18 However, in the study by Sousa et al., the results showed that preoperative antibiotic treatment had no benefit in reducing the risk of prosthetic joint infection between patients with asymptomatic bacteriuria and those without. Both studies also report that the microorganisms identified in the prosthetic joint infections did not correlate with the urine isolates. These findings further suggest that routine preoperative urinalysis and urine culture screening is likely unnecessary and contributes to the overutilization of antibiotics. As the culture isolate in the postoperative infection is frequently different from the preoperative urine culture, it may be important to identify other preoperative risk factors that can mitigate these complications.
Besides preoperative UAs in elective lumbar spine fusion surgeries, other factors may offer more insight into the predictive risk of postoperative complications. In our study, increased ASA scores were significant in increased risks of postoperative “other complications” (return to ED, return to OR, pneumonia, wound dehiscence, and bacteremia). Increased ODI and length of hospital stay were also nearly significant in higher rates of these other complications. These preoperative factors signify potential ways postoperative risks can be assessed for in patients undergoing elective lumbar spine fusion surgeries that may be more beneficial than preoperative urinalysis screening. Unlike UAs, which may cost the hospital and patients both time and money without clear indication of predicting postoperative risks and complications, these variables are obtained and measured without the required burden on healthcare systems that UAs present with. Furthermore, these variables may help curb the overutilization of antibiotics that has been seen correlated with the administration of UAs.
There were several limitations in our study. This study was conducted retrospectively at a single academic center which limits the generalizability of the data. Additionally, there were a handful of patients in our data that had a positive preoperative urinalysis, but did not have a follow-up urine culture. This may potentially skew the data, as we were unable to compare the microorganisms isolated between the preoperative and postoperative cultures in the case of a postoperative infection. Postoperative complications were also limited to within 3-months, so a longer time frame may potentially reveal greater risks of other complications over time.
Conclusion
Overall, our findings align with previous studies exploring the utility and predictive value of preoperative UAs. These findings put into question the utility and need for routine UAs before elective lumbar spine fusion surgeries. This information can assist in further establishing guidelines for the usage of preoperative UAs prior to elective lumbar spine fusion surgery, as well as open up further exploration into variables that may also predict postoperative complications, such as ASA, that can be analyzed without the burden and cost that UAs place onto the healthcare system. As a prior study by Winkler et al. reported an estimated cost savings of $8090 following the removal of preoperative UA and urine culture in cardiac surgery without an increase in postoperative surgical site infections, catheter-associated urinary tract infections, and C. diff infections, we recommend this practice be followed in patients undergoing spine surgery as there is limited benefit and can help reduce healthcare costs. 19
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.