
Abstract
Study design
Comparative study.
Objective
The vertebral bone quality (VBQ) score is a validated opportunistic screening tool for bone mineral density (BMD). Obesity, often associated with hyperlipidemia and fat infiltration, may result in lower VBQ-derived BMD. However, studies have shown that dual-energy x-ray absorptiometry (DXA)-derived BMD tends to increase in obesity. Given this paradox, the aim of this study was to evaluate the effect of obesity on the utility of VBQ in opportunistic osteopenia/osteoporosis screening.
Methods
A total of 310 consecutive patients with degenerative cervical myelopathy were included. Body mass index (BMI) classified patients into underweight/normal, overweight, and obesity groups. Pearson’s correlation assessed the associations of BMI with VBQ score, Hounsfield unit (HU) values, and T-score. The utility of VBQ score and HU values to discriminate normal BMD from osteopenia/osteoporosis was analyzed using receiver operating characteristic curve analysis and area under the curve (AUC).
Results
BMI was associated with lower VBQ score and higher T-score, but not with HU values. The correlation between VBQ score and T-score decreased with increasing BMI, eventually becoming nonsignificant in the obesity group (r = 0.241, P = .082). The VBQ score was not effective in identifying osteopenia/osteoporosis in the obese group (AUC = 0.59, P = .282). Compared with VBQ score, HU values were effective in several BMI subgroups (AUC = 0.75 to 0.88, P < .001).
Conclusion
The Cervical VBQ score is no longer a reliable indicator of DXA-derived BMD in obese patients. Even when the VBQ-derived BMD appears normal, it should not be solely relied upon to preclude further DXA evaluation.
Keywords
Introduction
Osteoporosis is a common disease characterized by systemic impairment of bone mass, strength, and microarchitecture, which increases the risk of instrumentation-related complications in spine surgery.1,2 The prevalence of osteoporosis has been reported to be as high as 12.9% in patients over 50 years of age undergoing cervical spine surgery, and this number is likely to increase further with the ageing of the population. 3 Despite this, poor preoperative bone health is often underestimated and undermanaged.2,4,5 A recent survey of spine surgeons reported that less than half perform preoperative dual-energy x-ray absorptiometry (DXA) scans to evaluate bone mineral density (BMD) in practice. 5 Furthermore, DXA scans involve additional costs and radiation exposure. 6 As a complement to DXA, Hounsfield unit (HU) values based on computed tomography (CT) scans have become reliable for assessing BMD. 7 Recently, the magnetic resonance imaging (MRI)-based vertebral bone quality (VBQ) score has been introduced as a novel approach to assess BMD without additional radiation. 8 This scoring system has been validated for the diagnosis of osteopenia/osteoporosis and the prediction of fragility fractures, instrumentation-related complications, and clinical outcomes, leading to its increasing clinical application.9-13
However, individual physiological factors can influence the clinical applicability of the VBQ score. 14 With obesity continuing its relentless global spread, 15 it is crucial to consider its impact. Obesity induces ectopic accumulation of adipocytes in bone marrow cavities, 16 potentially resulting in an increased VBQ score (i.e., decreased BMD). However, numerous studies have pointed that BMD is actually higher in obese individuals.17,18 In addition, obesity is strongly associated with hyperlipidemia, which can further inflate the VBQ score, leading to false positive predictive results.14,19 As a result, spine surgeons must account for the effects of obesity on VBQ score to avoid misinterpretations.
Body mass index (BMI) is easily accessible and most commonly used to define obesity. Some scholars have reported that BMI is an influencing factor for VBQ score, but shows no association with HU values.14,20 Therefore, the objective of this study was to determine whether increased BMI is associated with decreased utility of the cervical VBQ score in the assessment of BMD and to compare the utility of the VBQ score with HU values in BMI subgroups.
Methods
Patient Population
Ethical approval of this retrospective study was given by the Shanghai Changzheng Hospital ethics committee review board (2024SL037). We evaluated patients with degenerative cervical myelopathy (DCM) operated at our institution from September 2022 to July 2024. Inclusion criteria were: (1) availability of imaging data, including DXA, CT, and MRI scans, with all exams performed within one month; (2) males >50 years of age or postmenopausal females. Patients with any of the following were excluded: (1) cervical segmental insufficiency, malignancy, tuberculosis, ankylosing spondylitis, or metabolic bone disease other than osteoporosis; (2) history of surgery and fracture of the cervical spine, lumbar spine, or hip; and (3) documented long-term use of thyroid hormones, glucocorticoids, or anti-osteoporosis medications.
Detailed demographic data were obtained from electronic medical records. We divided the patients into three groups according to the regionally relevant BMI thresholds established by the Working Group on Obesity in China: underweight/normal (≤23.9), overweight (24.0-27.9), obesity (≥28.0).21-23 In addition, a sub-analysis based on the WHO classification system was conducted to increase the generalizability of our findings. 24
Bone Density Measurements
All lumbar and hip DXA scans were performed using the GE Lunar iDXA (GE Healthcare, Waukesha, WI, USA). T1-weighted MRI images were obtained using Siemens and GE Medical Systems. CT images of the cervical spine were obtained using two 64-row CT scanners (Philips and Siemens).
The T-score information was extracted from our institutional bone density facility for the lumbar spine, femoral neck, and total hip. Patients were stratified into two categories based on the lowest DXA T-score: normal BMD (T-score ≥ −1.0) and osteopenia/osteoporosis (T-score < −1.0).
25
Cervical VBQ score and HU values were calculated as described in previous studies.
26
Signal intensity (SI) of the medullary portion of each vertebral body and cerebrospinal fluid (CSF) at the cisterna magna were obtained by placing regions of interest (ROI) on T1-weighted MRI images (Figure 1A). The VBQ score was calculated by dividing the SI of the C2-C7 by the SI of the CSF. ROIs were placed in the mid-sagittal, mid-axial, and mid-coronal planes of the C2-C7 medulla to obtain HU values (Figure 1B–D). The VBQ score and HU values were measured by two observers with excellent intra- and inter-rater reliability. Calculation of the vertebral bone quality (VBQ) score and Hounsfield unit (HU) values.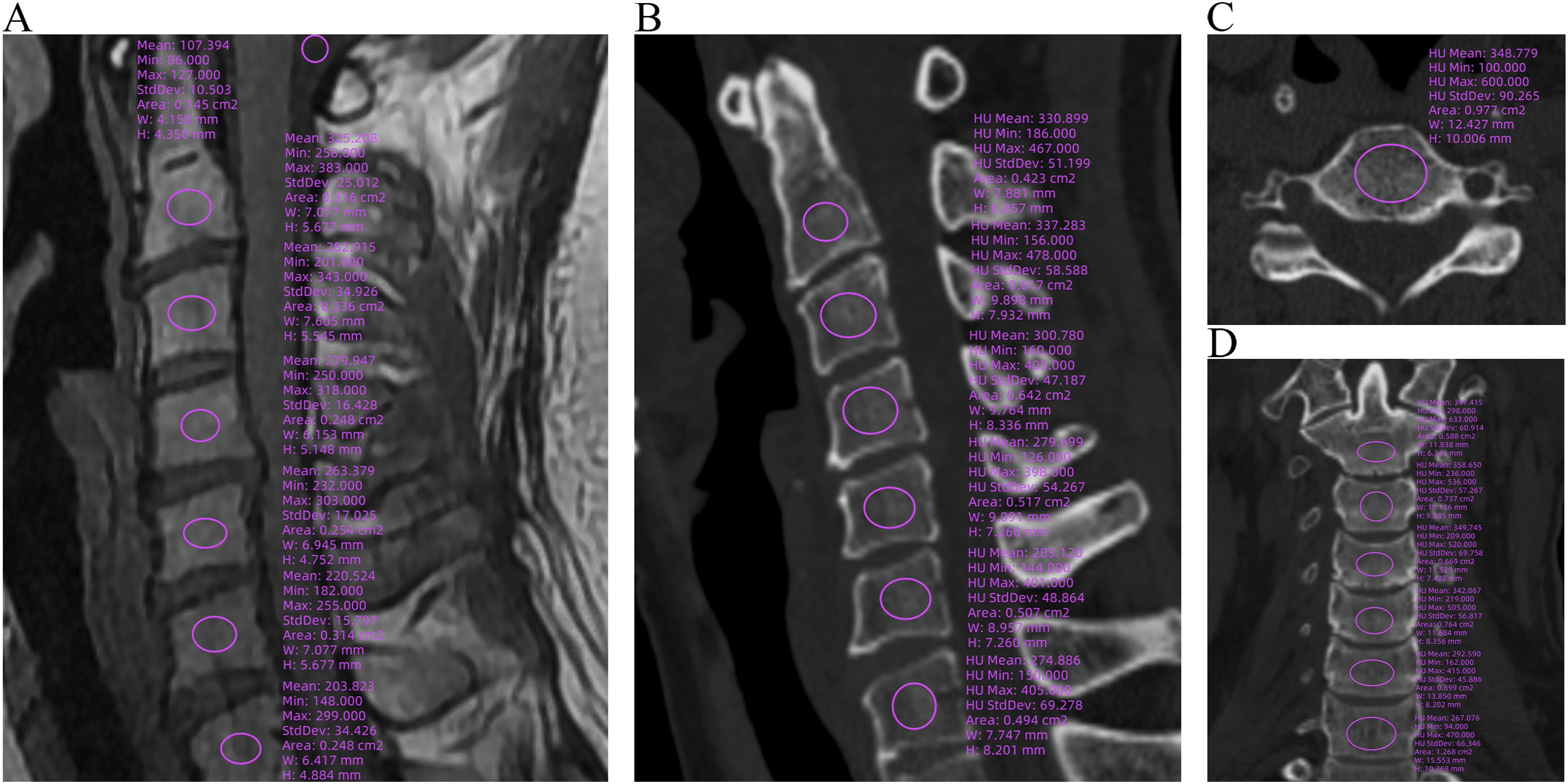
Statistical Analysis
Statistical analysis was performed with use of SPSS Statistics (version 27.0, IBM). Normality of data was assessed by the Shapiro-Wilk test. Continuous variables are presented as mean (SD) and analyzed using independent samples t-test or ANOVA. Categorical variables are presented as numbers and proportions of events and were assessed using either chi-squared or Fisher exact tests. The relationships between T-score, VBQ score, HU values, and BMI were further characterized using Pearson correlations. The impact of BMI on VBQ score was evaluated through multiple linear regression analysis. Receiver operating characteristic (ROC) curve analysis with Youden index was used to find a cut-off value of VBQ score and HU values that predicted osteopenia/osteoporosis. The area under the curve (AUC) reflects the ability of the score to discriminate between normal BMD and osteopenia/osteoporosis. An AUC value of ≥0.70 is acceptable. 27 The level of significance was defined as P < .05.
Results
Characteristics of Normal BMD and Osteopenia/Osteoporosis Groups.
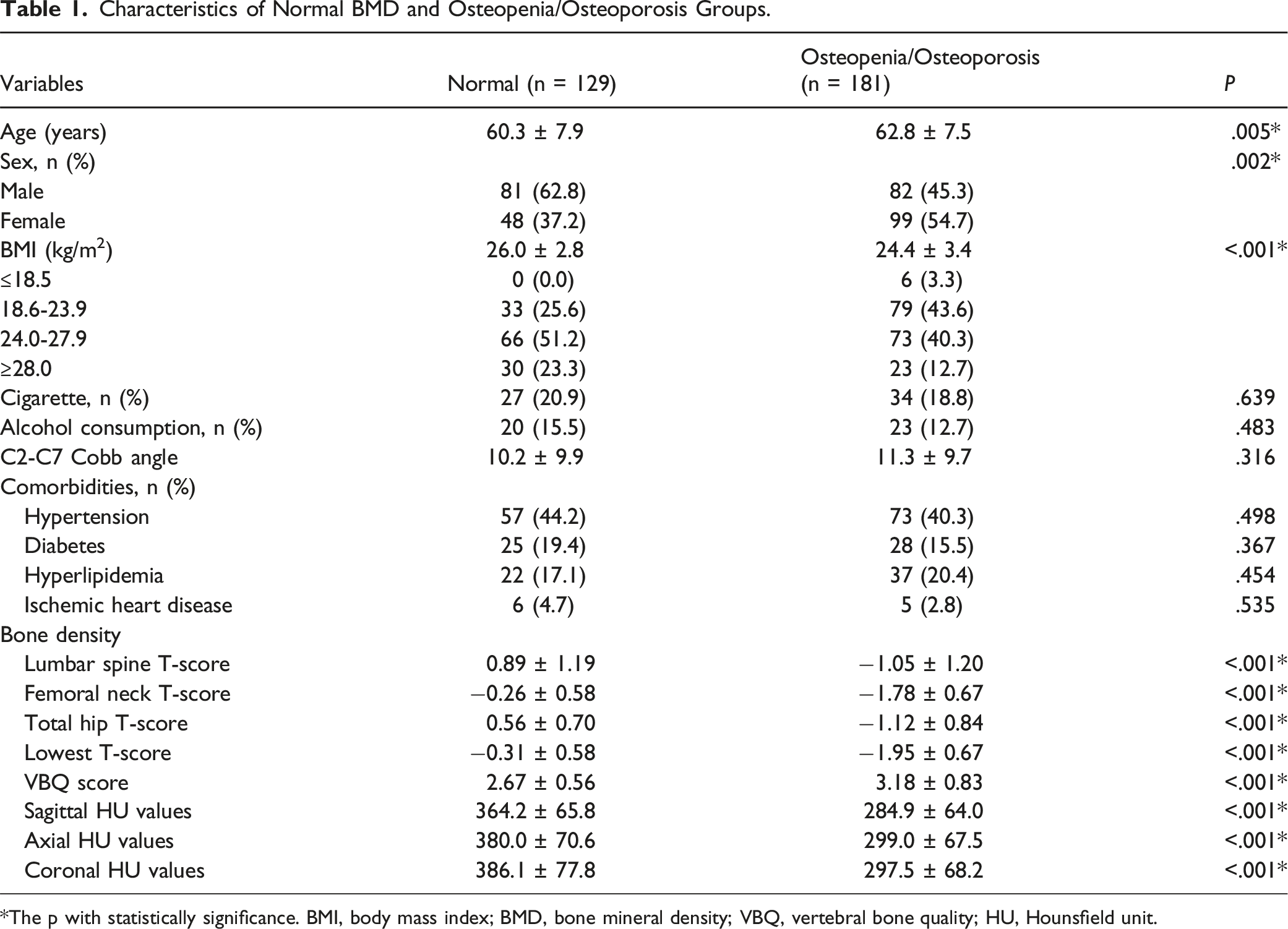
*The p with statistically significance. BMI, body mass index; BMD, bone mineral density; VBQ, vertebral bone quality; HU, Hounsfield unit.
Correlations Between BMI and VBQ Score
Characteristics of Various BMI Subgroups.
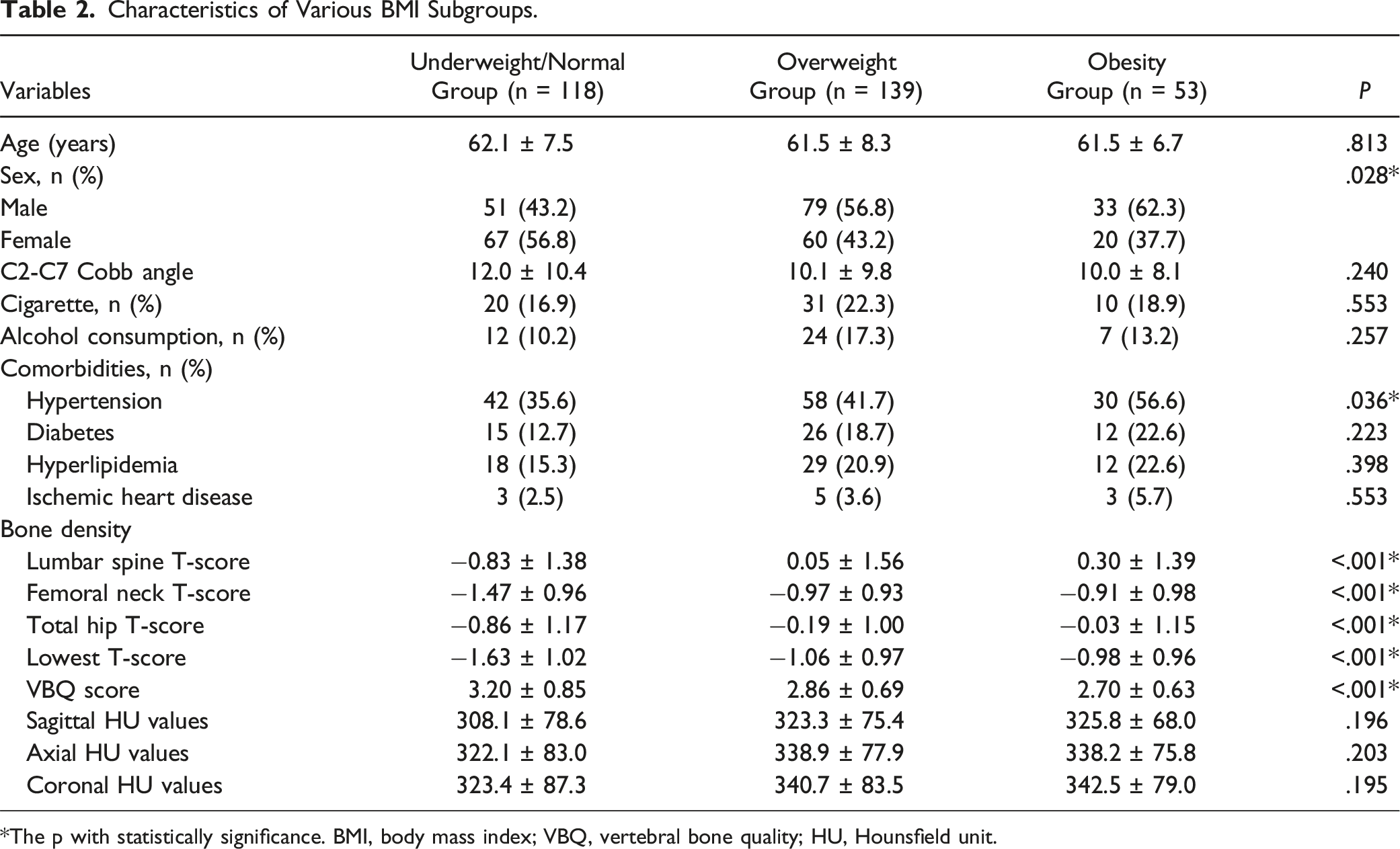
*The p with statistically significance. BMI, body mass index; VBQ, vertebral bone quality; HU, Hounsfield unit.
Multiple Linear Regression Analysis of the Effect of BMI on VBQ Score.
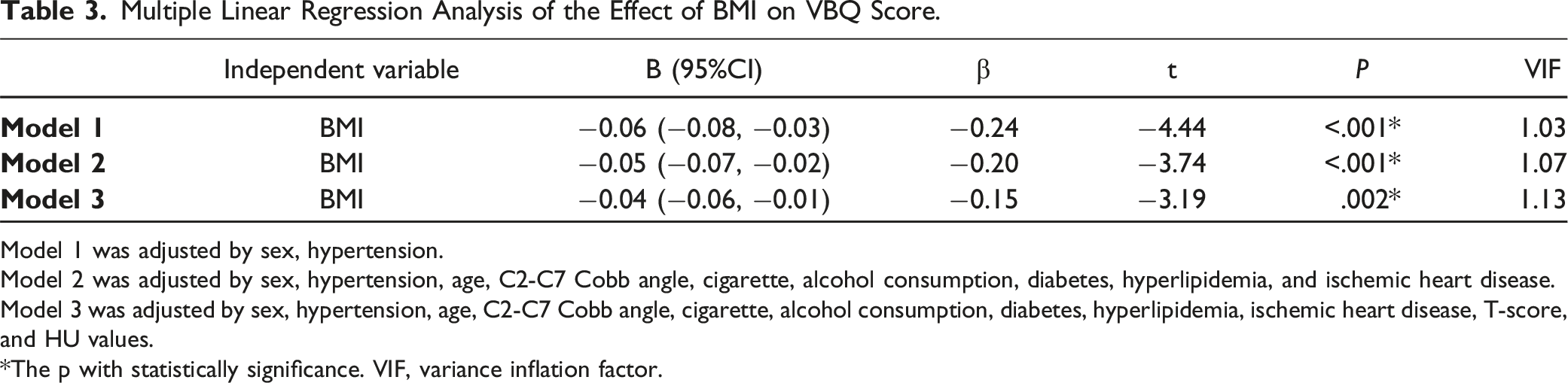
Model 1 was adjusted by sex, hypertension.
Model 2 was adjusted by sex, hypertension, age, C2-C7 Cobb angle, cigarette, alcohol consumption, diabetes, hyperlipidemia, and ischemic heart disease.
Model 3 was adjusted by sex, hypertension, age, C2-C7 Cobb angle, cigarette, alcohol consumption, diabetes, hyperlipidemia, ischemic heart disease, T-score, and HU values.
*The p with statistically significance. VIF, variance inflation factor.
Correlations Between VBQ Score and T-Score in BMI Subgroups
In the underweight/normal group, the VBQ score was significantly correlated with the lowest T-score (r = −0.47, P < .001) (Figure 2). Correlation values between VBQ score and lowest T-score were lower in the overweight group, but still significant (r = −0.39, P < .001). However, in the obesity group, there was no significant association between the VBQ score and the lowest T-score (r = −0.24, P = .082). In the various BMI subgroups, the correlation coefficients between HU values and the lowest T-score ranged from 0.52 to 0.71 (P < .001 for all). Correlation coefficients between VBQ score, HU values, and T-score in different BMI subgroups. *, The p with statistically significance. VBQ, vertebral bone quality; HU, Hounsfield unit.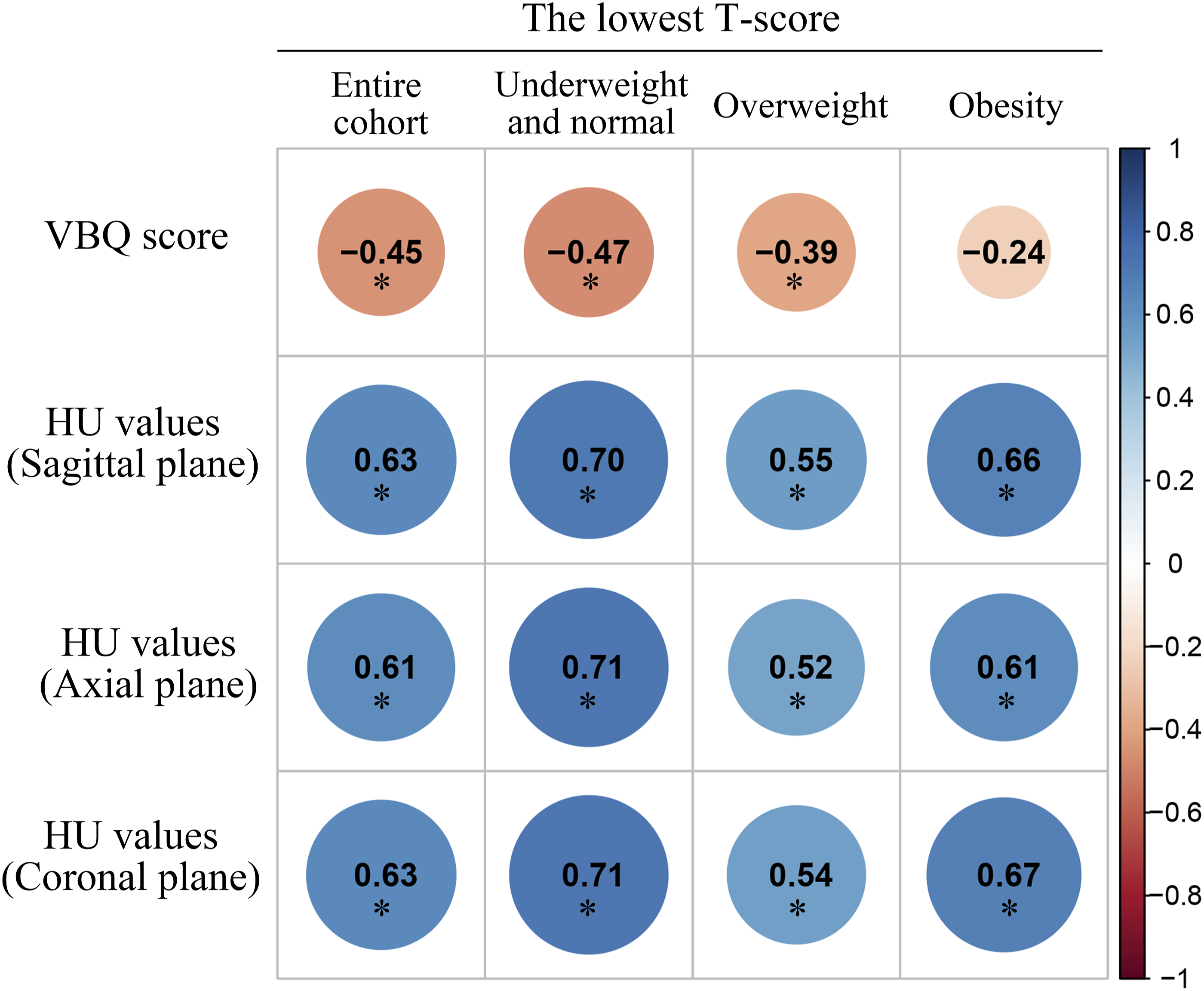
ROC Curve Analysis Associated with BMI Subgroups
Diagnostic Accuracy and Optimal Cut-Off Value of VBQ Score for Detection of Osteopenia/Osteoporosis in Different BMI Subgroups.
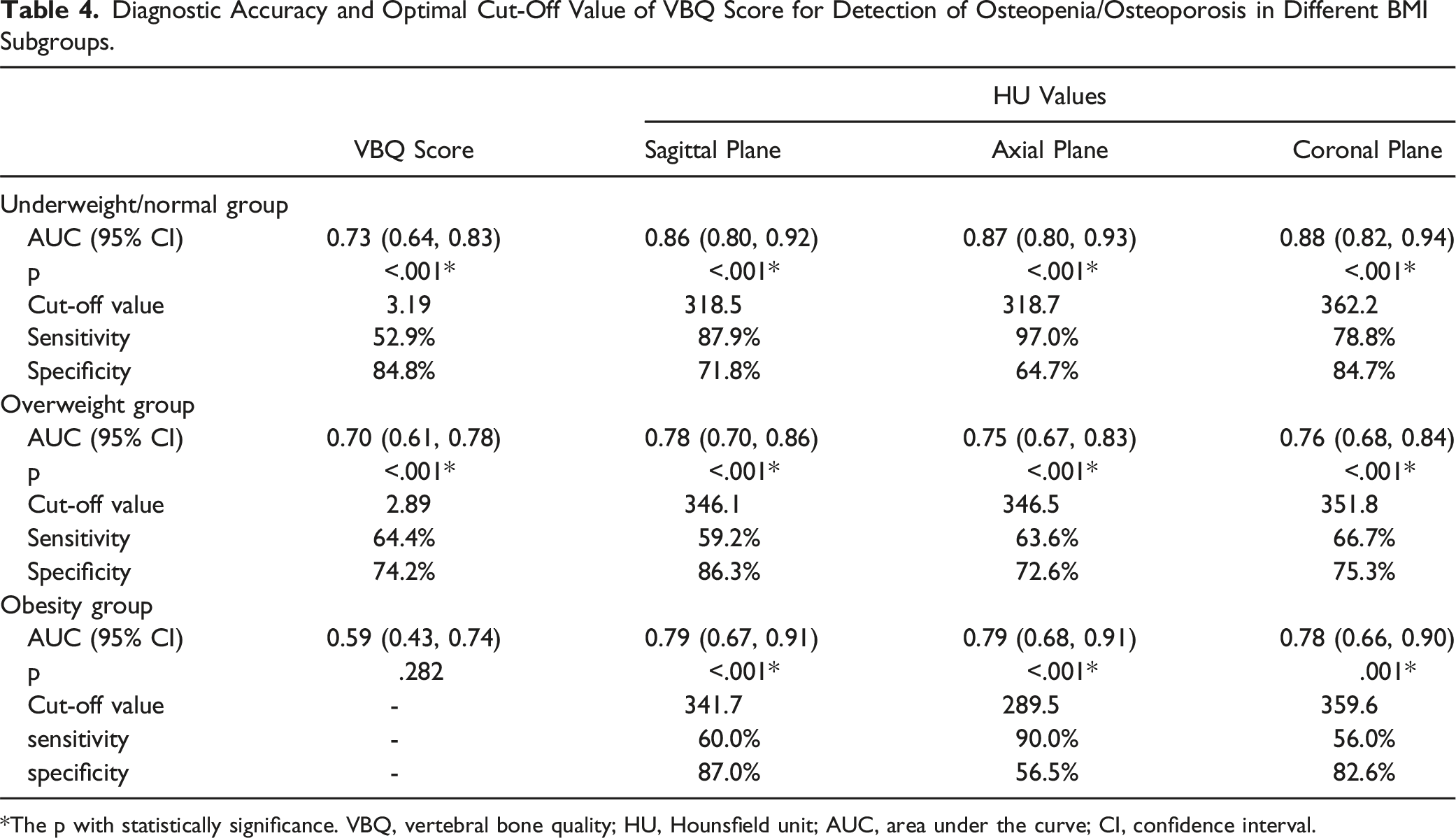
*The p with statistically significance. VBQ, vertebral bone quality; HU, Hounsfield unit; AUC, area under the curve; CI, confidence interval.
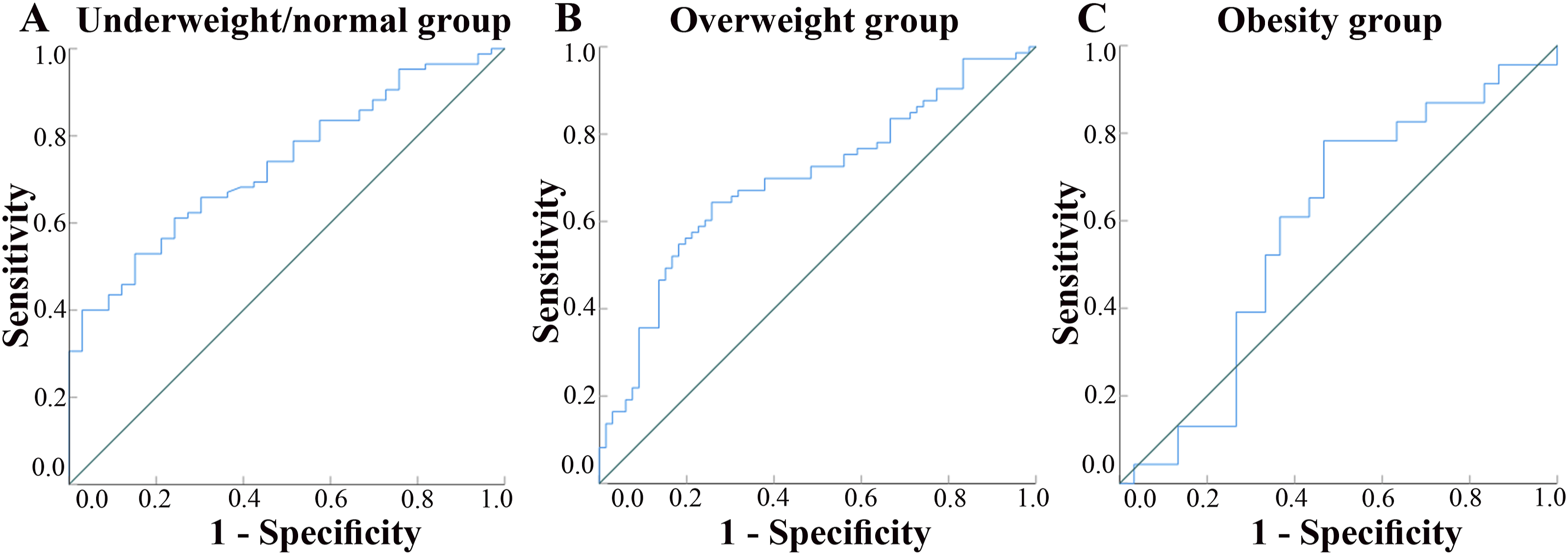
Receiver operating characteristic curve (ROC) analysis of VBQ score under different BMI subgroups. The diagonal line is the reference line indicating no predictive ability.
Discussion
To our knowledge, this is the first study to investigate the limitations of using VBQ score in obese populations. The primary finding was the negative effect of BMI on cervical VBQ score, rendering VBQ score less effective in differentiating between normal and osteopenia/osteoporosis in obese patients. In contrast, HU values consistently demonstrated efficacy in differentiating bone conditions across various populations, with no significant association between BMI and HU values.
Since the introduction of the VBQ score by Ehresman et al, 28 its application has expanded from lumbar spine assessment to the cervical spine for osteopenia/osteoporosis screening.9,29,30 Previous research by Huang et al. reported an accuracy of 0.78 for identifying osteopenia/osteoporosis using the cervical VBQ score in patients with undifferentiated DCM. 9 In our study, accuracy levels were 0.73 and 0.70 in underweight/normal and overweight groups, respectively. However, a reliable model could not be developed for the obesity group, highlighting the potential limitations of VBQ in this population. This finding should be interpreted with caution, especially considering the growing use of VBQ score in spine surgery.
Preferential differentiation of bone marrow mesenchymal stem cells (BM-MSCs) into adipocytes reduces osteogenesis, and bone marrow adipocyte progenitor cells have been shown to contribute to osteoclastogenesis.31,32 The inverse relationship between bone marrow adipose tissue content and BMD forms the basis for the VBQ score, which uses T1-weighted MRI to indirectly assess BMD by evaluating bone marrow adiposity. 8 High BMI promotes the differentiation of BM-MSCs into adipocytes, 31 which typically increases bone marrow fat content and may contribute to lower VBQ-derived BMD. However, our study found that higher BMI was associated with increased BMD, as assessed by both DXA and VBQ score. This is consistent with the broader literature, which indicates that obesity can impact the skeleton through several pathways, typically resulting in higher BMD.18,33-35 Specifically, mechanical loading associated with increased BMI triggers a cascade of transduction signals that increase bone mass via osteoblast activity and the Wnt/β-catenin signaling pathway.31,36 At the same time, adipose tissue, as an endocrine organ, affects bone metabolism via endocrine pathways, potentially exerting both positive and negative effects. 35 These opposing influences may account for variations in the correlation between VBQ- and DXA-derived BMD across different BMI subgroups.
The gold standard, DXA uses two different X-ray energies to pass through bone and soft tissue and measures the difference in their attenuation to calculate BMD. 37 However, the precise bone composition changes measured by the VBQ score, and the factors influencing it, remain poorly understood. Haffer et al. have proposed that the VBQ score captures both organic and inorganic components of the vertebral body, reflecting bone quality and mass, whereas DXA measures primarily inorganic material to calculate BMD. 38 Despite the general trend for obesity to increase DXA-derived BMD, the “obesity paradox” indicates that this does not necessarily translate into reduced fracture risk. 35 This suggests that DXA may fail to capture the full extent of bone changes associated with obesity. In contrast, several studies have reported that the VBQ score outperforms T-score in predicting fragility fractures and osteoporotic vertebral compression fractures.11,39 Thus, the VBQ score has the potential to identify compositional changes in the bone marrow and reflect real bone changes in the vertebral body. Unfortunately, the present study could not discern whether the altered VBQ scores in obese patients reflect inaccuracies in the scoring system or reflect localized changes in bone quality that are not detectable by DXA.
The HU values reflect the X-ray absorption properties of bone tissue as measured by CT. They are less affected by changes in body size and therefore may provide a more direct reflection when assessing bone density. In this study, unlike T-score or the VBQ score, HU values do not appear to fluctuate with changes in BMI. This independence may also mean that it is insensitive to certain pathological or physiological changes associated with obesity. Nevertheless, HU value provides a relatively stable method of opportunistic bone density assessment independent of BMI. It may be more appropriate for evaluating patients in certain specific clinical situations, such as individuals with extreme body sizes that may affect the accuracy of other methods.
The VBQ score is a valuable tool; however, its accuracy for BMD screening is limited in obese patients, highlighting the need for cautious interpretation of results. Specifically, VBQ score is no longer a reliable indicator of DXA-derived BMD in obese patients. Even when the VBQ-derived BMD appears normal, it should not be solely relied upon to preclude further DXA evaluation, as this is likely to lead to underdiagnosis of compromised bone health. Notably, our study does not aim to discredit the VBQ score. Rather, it may provide insights about bone quality that DXA can’t capture. The complex effects of obesity on bone metabolism and marrow composition further emphasize the need for a multimodal approach. We recommend integrating VBQ results with CT-based HU measurements, and clinical risk factors to enhance diagnostic accuracy and guide treatment decisions more effectively.
This study has several limitations. First, this study only highlights the impact of obesity on the use of the cervical VBQ score for osteoporosis/osteoporosis screening. However, whether this impact exists in predicting adverse outcomes, including fracture, nonunion of instruments, is unknown. Second, to validate our findings, multicenter studies with large sample sizes are needed. Third, although BMI is the most commonly used indicator of obesity, it cannot distinguish between fat and lean body mass, or between subcutaneous and visceral fat. Further research is needed to explore what body composition changes associated with higher BMI affect VBQ score. Finally, this study was conducted in a cervical spine surgery population. The applicability of opportunistic use of thoracic and lumbar VBQ score for osteoporosis screening in the obese population requires further investigation.
Conclusion
The VBQ score may not be appropriate for screening for osteopenia/osteoporosis in an obese population. Even if the VBQ-derived BMD appears normal, it cannot be solely relied upon to preclude further DXA assessment. This does not imply that the VBQ score is inherently advantageous or disadvantageous. Future research should focus on evaluating the clinical utility of the VBQ score in predicting fracture risk and device failure in different populations.
Supplemental Material
Supplemental Material - Obesity Limits Utility of Vertebral Bone Quality Score for Opportunistic Osteopenia/Osteoporosis Screening in Cervical Surgery Patients
Supplemental Material for Obesity Limits Utility of Vertebral Bone Quality Score for Opportunistic Osteopenia/Osteoporosis Screening in Cervical Surgery Patients by Mingliang Shi, Cheng Ye, Baocheng Niu, Dong Xie, Qing Chen, Qi Zhao, Hao Wu, and Lili Yang in Global Spine Journal
Footnotes
Author Contributions
Conceptualization: Mingliang Shi, Cheng Ye, Baocheng Niu
Formal Analysis: Cheng Ye, Qi Zhao, Hao Wu
Investigation: Cheng Ye, Baocheng Niu, Dong Xie
Methodology: Mingliang Shi, Dong Xie, Qing Chen, Qi Zhao, Project Administration: Lili Yang
Writing – Original Draft: Mingliang Shi
Writing – Review & Editing: Mingliang Shi, Qi Zhao, Hao Wu, Lili Yang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was sponsored by National Natural Science Foundation of China (82372431), the Shanghai Municipal Health Commission Health Leading Talents Program (2022LJ007), the Natural Science Foundation of the Science and Technology Commission of Shanghai Municipality (22ZR1476700), Shanghai Municipal Annual Innovative Medical Device Application Demonstration Project (23SHS05700-06), the Fifth Round Innovation Team of Shanghai Changning District, “Open bidding for selecting the best candidates” cultivation project of Shanghai Changzheng Hospital (2023YJBF-PY10).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.