
Abstract
Postpartum osteoporosis (PO) is a rare condition characterized by low bone mineral density (BMD) and an increased risk of vertebral fragility fracture. We encountered a 34-year-old woman who developed back pain 1 week after delivery. Magnetic resonance imaging of the lumbar spine revealed three vertebral compression fractures. Pretreatment BMD evaluation by dual-energy X-ray absorptiometry revealed a low T-score and Z-score (−2.0 and −2.0, respectively; BMD, 0.876 g/cm2) in the affected region of the spine. The patient was diagnosed with PO and treated with subcutaneous injection of denosumab 60 mg (Prolia; Amgen, Inc., Thousand Oaks, CA, USA) every 6 months. After two treatments, the BMD had significantly increased and the back pain was improved; the patient therefore decided to terminate the treatment. Two months later, her back pain worsened and BMD decreased as measured by dual-energy X-ray absorptiometry examination of the lumbar spine. Therefore, the patient resumed treatment with denosumab, and the BMD of the lumbar spine increased after another two treatments. Therefore, we consider denosumab to be promising in the management of PO with respect to increased BMD and decreased pain.
Keywords
Introduction
Postpartum osteoporosis (PO) is a rare type of osteoporosis that affects women during the early postpartum period. The reported prevalence of PO is approximately four to eight patients per million population. 1 Back pain is one of the most common complaints in patients with PO, and many affected patients develop vertebral fractures. Multiple osteoporotic vertebral compression fractures can lead to height decreases in some patients. The mechanism of PO remains unknown, and a standard treatment strategy has not been established. A general consensus on PO management is currently lacking, and treatment tends to focus on both pain reduction and BMD gain to prevent the occurrence of fragility fractures.2,3 Treatments for PO include breastfeeding cessation, calcium and vitamin D supplementation, bisphosphonates, and teriparatide (TPT). Denosumab is effective in treating postmenopausal osteoporosis. In recent reports, denosumab also showed efficacy in the treatment of PO, which is an uncommon form of secondary osteoporosis. We herein report a case of PO with multiple lumbar fractures treated with denosumab and provide a review of the related literature.
Case presentation
A 34-year-old woman presented with severe low back pain 1 week after the birth of her child. She did not seek medical attention immediately and presented to our institution 5 weeks after the onset of pain. Her medical history was unremarkable. Physical examination revealed tenderness of the back. Her height had decreased by approximately 1 cm since the delivery of her child. Magnetic resonance imaging of the lumbar spine revealed three vertebral compression fractures (L2, L3, and L4) and height loss (Figure 1). All laboratory data were within the reference ranges except for a high N-osteocalcin (N-MID fragment) concentration (Table 1). Pretreatment BMD measurements determined by dual-energy X-ray absorptiometry (DXA) revealed a low T-score and Z-score (−2.0 and −2.0, respectively) and BMD of 0.876 g/cm2 in the affected area of the spine. The prescribed treatment was subcutaneous injection of denosumab 60 mg (Prolia; Amgen, Inc., Thousand Oaks, CA, USA) every 6 months and supplementation with calcium carbonate 600 mg + vitamin D3 400 mg twice a day. The patient was followed up at 10 months and 13 months. After two denosumab injections, her BMD significantly increased and her back pain decreased in severity. BMD measurements determined by DXA revealed increases in the lumbar spine T-score to −0.9 and Z-score to −0.9, representing 15.7% increases compared with baseline.

Magnetic resonance imaging examination of the lumbar spine revealed L2, L3, and L4 vertebral body compression fractures. The collapsed vertebral bodies showed hypointensity on (a) T1-weighted imaging and hyperintensity on (b) T2-weighted imaging and (c) short-TI inversion recovery imaging.
Biochemical markers before treatment.

ALP, alkaline phosphatase; iPTH, intact parathyroid hormone; N-MID, N-osteocalcin (N-MID fragment); CTX, type I collagen carboxy-terminal peptide; PINP, type I procollagen amino-terminal peptide.
The patient’s clinical presentation had significantly improved, and she decided to terminate the treatment with denosumab. Two months later, her back pain worsened and she underwent a DXA examination. BMD measurements showed that the lumbar spine T-score and Z-score were −2.1 and −2.1, respectively, representing a −2% decrease in each score. The femoral neck BMD had decreased from 0.791 to 0.709 g/cm2, representing a decrease of −10.4%. The patient resumed treatment with denosumab, and her back pain was rapidly relieved. Two additional courses of denosumab were administered, and DXA was performed at 23 months and 29 months to examine the changes in BMD. Compared with baseline, the BMD of the lumbar spine had increased by 7.7% at 29 months (Table 2). At the time of this writing, the patient was continuing treatment with denosumab.
Changes in BMD parameters after denosumab treatment.

BMD, bone mineral density; H-BMD, hip BMD; IR, increasing rate.
The patient provided verbal informed consent for treatment and written consent for publication of this case report. Ethics committee approval was not required because of the nature of this study (case report). The reporting of this study conforms to the CARE guidelines. 4
Discussion
PO is a rare condition that was first described approximately 60 years ago. 2 During adulthood, an imbalance between osteoblasts and osteoclasts can cause reductions in BMD that lead to an increased risk of fractures. 3 Several possible mechanisms underlying the link between pregnancy and PO have been suggested. The maternal physiological calcium requirements are remarkably high during the second and third trimesters of pregnancy, when rapid mineralization of the fetal skeleton occurs. The rate of calcium absorption doubles secondary to elevated levels of calcitriol and parathyroid hormone-related peptide as well as the direct intestinal effects of estrogen. 5 The degree of BMD reduction during pregnancy ranges from 2% to 4%. 6 During lactation, the average loss of calcium in breast milk is approximately 210 mg/day, and marked decreases in BMD are frequently observed. 7 Patients who are pregnant or have PO can expect these parameters to return to normal at 6 to 12 months after cessation of breastfeeding. 8
The most common sites of PO are the vertebrae. PO is characterized by the occurrence of vertebral fragility fractures, most commonly at the lower thoracic and/or lumbar levels. The main clinical symptoms are severe and prolonged back pain and height loss. 8 Osteoporosis and fractures can also occur in other locations, such as the sacrum, superior and inferior pubic bones, ischiopubic arch, pubic body, proximal femoral diaphysis, femoral neck, subcapital hip region, and ribs. 9
Vertebral compression fractures related to PO can be attributed to several factors, including bone loss mainly at the trabeculae and mechanical effects on the spine such as weight gain and increased lumbar lordosis. 10 Unlike other types of osteoporotic vertebral fractures, PO-related fractures tend to involve multiple vertebrae; in one study, the mean number of fractures was 4.4 per patient. 11 Bonacker et al. 12 reported eight vertebral fractures in a single patient. Few patients have a vertebral fracture at a single level. The thoracolumbar region is the most commonly affected area, and the most vulnerable levels appear to be T11 to L4. The present case of PO involved multiple lumbar segments from L2 to L4. Magnetic resonance imaging is recommended to examine the condition of the thoracic and lumbar vertebrae to avoid a missed diagnosis of fractured vertebrae in patients with suspected PO. Height decreases are common in patients with PO because of the multiple vertebral fractures. The height of the present patient had decreased by 1 cm since delivery.
No consensus on how to treat PO has been reached. The treatment options are limited to those described in previous case reports. Treatment should be focused on increasing BMD and preventing the occurrence of fragility fractures. The documented medical treatments include calcium and vitamin D supplementation, bisphosphonates, TPT, calcitonin, strontium ranelate, and denosumab. In a recent study, the two most frequently used treatments were denosumab and bisphosphonates. 13
Adequate levels of calcium and vitamin D are important for all women with PO, regardless of whether other pharmacological treatments are offered. 10
Numerous clinical case reports have described women with PO who received bisphosphonate treatment, either orally or intravenously. These reports generally indicated reductions in bone pain, improvements in mobility, and sequential improvements in lumbar spine BMD. O’Sullivan et al. 14 reported a series of patients with PO and noted that those who received bisphosphonate treatment exhibited spinal BMD increases of 17% at 1 year and 23% at 2 years, which were significantly higher than those in patients without bisphosphonate treatment (2% at 1 year and 11% at 2 years). Li et al. 15 demonstrated that bisphosphonates were effective for reducing bone turnover markers in patients with PO.
Treatment with TPT is beneficial in terms of both efficacy and safety. 16 TPT has a short half-life of 1 hour and undergoes rapid elimination. Therefore, TPT treatment for PO is associated with an absence of complications and abnormalities during subsequent gestation and delivery. 17 Unlike bisphosphonates, TPT is not stored in the bone matrix for years; therefore, patients should receive TPT if they are anticipating future pregnancies because this drug has been assigned to pregnancy category C by the Food and Drug Administration. 9 Winarno et al. 18 described a patient with PO in whom TPT effectively increased the BMD after failed treatment with oral and intravenous bisphosphonates and adequate calcium and vitamin D supplementation. Additionally, Lampropoulou-Adamidou et al. 19 found that TPT therapy provided clinical improvement of back pain.
Denosumab is a human monoclonal antibody that binds to receptor activator of nuclear factor κB-ligand (RANKL) and inhibits the activation of osteoclasts and osteoclast precursors. This inhibition leads to suppression of bone turnover in patients with osteolytic bone disease, and a curative effect has been reported in postmenopausal women. 20 The first report of denosumab for treatment of PO was published in 2016 by Sánchez et al., 21 who described two patients treated with bisphosphonates and denosumab. To date, 10 patients with PO who were treated with denosumab, including the patient in the present case, can be found in the English-language literature (Table 3). Of these 10 patients, 1 received treatment with nasal calcitonin and strontium ranelate for 1 year, but their lumbar BMD remained unchanged. Therefore, the treatment was switched to subcutaneous denosumab. After two injections, the lumbar spine BMD had increased by 14%. 21 Another patient was treated with TPT and denosumab, and their BMD had significantly increased at 6 months. However, the patient requested an alternative treatment to avoid the frequent injections; therefore, the TPT was switched to subcutaneous injection of denosumab. 22 The remaining eight patients received treatment with denosumab only. In all 10 patients, the treatment with denosumab markedly improved the bone microarchitecture and increased the BMD. The present patient received oral calcium and vitamin D supplementation throughout the course of treatment. After the first course of denosumab, the BMD gradually increased and the pain significantly improved. After the second course of denosumab, the patient discontinued treatment because of the increase in BMD and improvement in pain. However, the BMD decreased again thereafter. The patient then accepted two additional treatments with denosumab, and her BMD increased and back pain improved.
Published articles on vertebral fractures in patients with postpartum osteoporosis treated with denosumab.
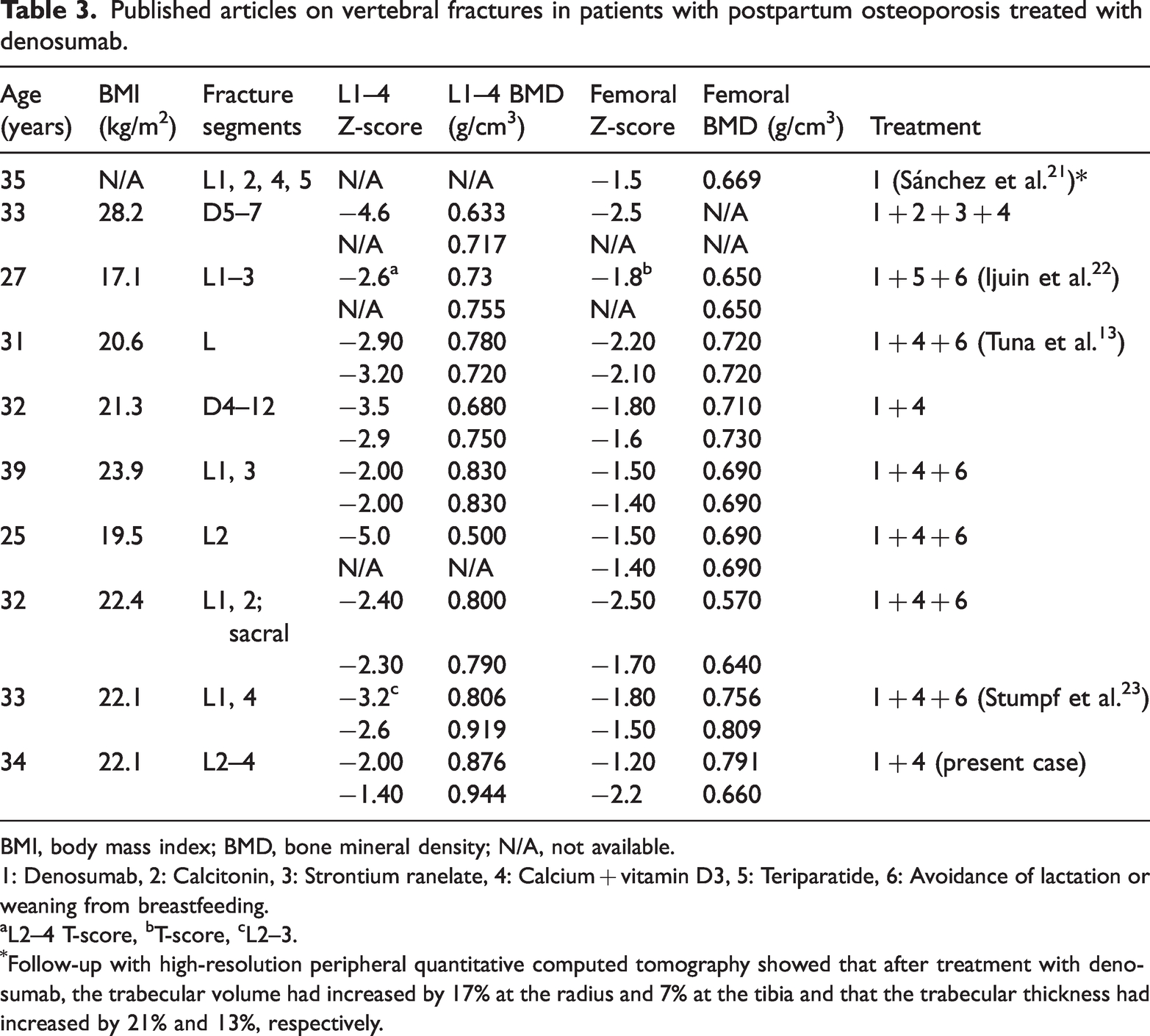
BMI, body mass index; BMD, bone mineral density; N/A, not available.
1: Denosumab, 2: Calcitonin, 3: Strontium ranelate, 4: Calcium + vitamin D3, 5: Teriparatide, 6: Avoidance of lactation or weaning from breastfeeding.
L2–4 T-score, bT-score, cL2–3.
Follow-up with high-resolution peripheral quantitative computed tomography showed that after treatment with denosumab, the trabecular volume had increased by 17% at the radius and 7% at the tibia and that the trabecular thickness had increased by 21% and 13%, respectively.
Conclusion
Denosumab can be used in the treatment of PO with a good safety profile and positive results in terms of increasing BMD and reducing pain. However, further evidence regarding its long-term safety is needed.
Footnotes
Acknowledgements
The authors thank the hospital staff for their cooperation.
Author contributions
Study design: Guan-xi Wang and Jin-hua Han
Literature search: Rui-zhi Zhou
Writing of the original draft: Jin-hua Han and Rui-zhi Zhou
Literature review and editing: Chuan-ping Gao
All the data supporting the findings in this study are included in the published manuscript.
Data availability statement
The data are available upon reasonable request from the corresponding author.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.