Abstract
Study Design
Prospective Randomized Controlled Trial.
Objectives
To investigate the effect of combined motor control and isolated lumbar strengthening exercise (MC + ILEX) vs general exercise (GE) on upper lumbar paraspinal muscle volume and composition, strength and patient outcomes in individuals with chronic low back pain (LBP).
Methods
50 participants with nonspecific chronic LBP were randomly allocated (1:1) to each group (MC + ILEX or GE) and underwent a 12-week supervised intervention program 2 times per week. Magnetic resonance imaging was performed at baseline, 6-weeks and 12-weeks to examine the impact of each intervention on multifidus (MF) and erector spinae (ES) muscle volume (cm3) and fatty infiltration (%FI) at L1-L2, L2-L3 and L3-L4.
Results
Our results revealed no significant between-groups findings for MF and ES %FI and volume, and patient-reported psychosocial measures. However, both groups had significant within-groups decreases in MF %FI at L1-L2, L2-L3 and L3-L4, with concomitant decreases in MF volume at L1-L2 and L2-L3, and at L3-L4 in the GE group. Each group displayed significant improvements in Kinesiophobia, while only MC + ILEX had significant improvements in pain catastrophizing, anxiety, depression and sleep. Lastly, significant correlations were found between change in Kinesiophobia and upper lumbar MF %FI, and between change in strength and lower lumbar MF and ES size.
Conclusions
Both exercise interventions may help reduce upper lumbar MF %FI in individuals with chronic LBP, while MC + ILEX could significantly improve important patient outcomes. Our results support the idea that improvements in paraspinal muscle health associate with better patient outcomes. Further high-quality imaging studies are needed to explore these relationships.
Keywords
Introduction
Low back pain (LBP) is a well-recognized and significant public health concern.1-3 The healthcare-related cost for chronic LBP and social consequences are substantial for society.2,4 In addition, impairments in strength,5,6 flexibility,7,8 endurance, 9 and obesity 10 are well documented in individuals with chronic LBP. Fatty infiltration (FI), muscle atrophy, and asymmetry in the lumbar paraspinal muscles, especially in the multifidus (MF), are associated with LBP.11-14 Poor motor control, reduced muscle activation, and fatigue are possible mechanisms leading to degenerative paraspinal muscle changes. More specifically, inefficient motor coordination could result in repetitive mechanical stress on adjacent structures and potentially instability, joint overloading, and pain. 15 Therefore, many exercise interventions focus on activating paraspinal muscles.16-18
There is growing evidence that exercise is effective at treating LBP.19,20 Exercise therapy is currently the most widely used form of conservative treatment for chronic LBP, however the best kind of exercise is unclear. While it is a recognized non-operative modality and part of any post-operative spine surgery, the protocols are variable. Still, exercise therapy is recommended as a first-line treatment for people with chronic LBP, 21 with improvements in pain, quality of life, depression and functional status.16-18,21-23 Motor control (MC) is a specific kind of exercise that emphasizes coordination and control of the trunk muscles. It includes the isolated activation of deep trunk muscles and the integration of superficial muscles with the goal of retraining control and function restoration. 24 While the effects of MC on pain and disability are promising,24-26 literature regarding its effectiveness on improving paraspinal muscle morphology is scarce.27,28 A recent systematic review showed very low- to low-quality evidence that MC exercise alone was superior than general physiotherapy in increasing lumbar MF cross-sectional area (CSA), and that MC exercise is similar to other interventions in increasing resting lumbar MF thickness, in chronic LBP. 29 In the same study, low-quality evidence proposed there was no relationship between MF morphological changes from MC exercise and LBP-related disability. While MC exercises may improve lumbar MF morphology in people with chronic LBP, it remains unclear whether the observed morphological changes are related to clinical outcomes. 29
Studies have also utilized targeted strengthening exercises to enhance lumbar muscle strength and recommended using pelvic restraints to limit the activity of other large muscles of the posterior chain (e.g., gluteus and hamstrings), such as isolated lumbar extension exercise (ILEX).16,30 Since most exercises interventions do not involve pelvic stabilization it is possible that the absence of paraspinal muscle morphological changes may be due to the compensation of the other posterior chain muscles. 30 Pelvic stabilization during extension exercises is potentially able to efficiently target the lumbar extensors and lead to significant morphological and functional changes. It is unclear if paraspinal muscle adaptations from exercise interventions will lead to improvements in patient-related outcomes.27,28,31,32 An ILEX program did not result in significant muscle morphological changes in patients with chronic LBP. 28 However, a significant correlation was still found between improvements in muscle size and composition, and improvements in disability, anxiety/depression, and strength. Based on their findings, the authors suggested that muscle health improvements may lead to larger functional improvements. 28
Our recent work stemming from the same trial as this study, compared the effects of combined MC and ILEX vs general exercise on paraspinal muscle morphology at the two lower lumbar spinal levels (L4-L5 and L5-S1). 33 Results showed a significant between-groups difference in MF and ES CSA, with only the MC + ILEX group demonstrating a significant increase in size at both levels. Furthermore, only the MC + ILEX group demonstrated a significant decrease in ES %FI at L5-S1. Finally, both groups had significant improvements in pain, disability, and quality of life. While this previous work focused on the lower lumbar levels, the current study’s aim is to assess the effect of both interventions on paraspinal muscle health at the upper lumbar spinal levels (e.g., L1-L2, L2-L3 and L3-L4) and their association with patient-reported outcome measures. Due to greater weight-induced stress and spinal pathology,34-36 the lower lumbar levels typically undergo more degenerative changes (increased atrophy and FI) compared to the upper levels.34,37,38 Consequently, the upper lumbar levels have been less frequently investigated. Interestingly, one recent study found an association between LBP and paraspinal muscle FI at every lumbar level, with severe FI in the upper ES muscle. 39 Thus, LBP may develop as a result of FI-related diminished quality of upper paraspinal muscles, which warrants further attention. Specifically, the purpose of this study was to investigate the effect of a combined MC and ILEX strengthening vs a general exercise (GE) group on 1) paraspinal muscle size, composition (e.g. FI) at the upper spinal levels, and strength, and the association of these changes with 2) pain, disability, quality of life, and psychosocial factors (including: kinesiophobia, catastrophizing, anxiety, depression, and sleep) in individuals with chronic LBP.
Methodology
Study Design
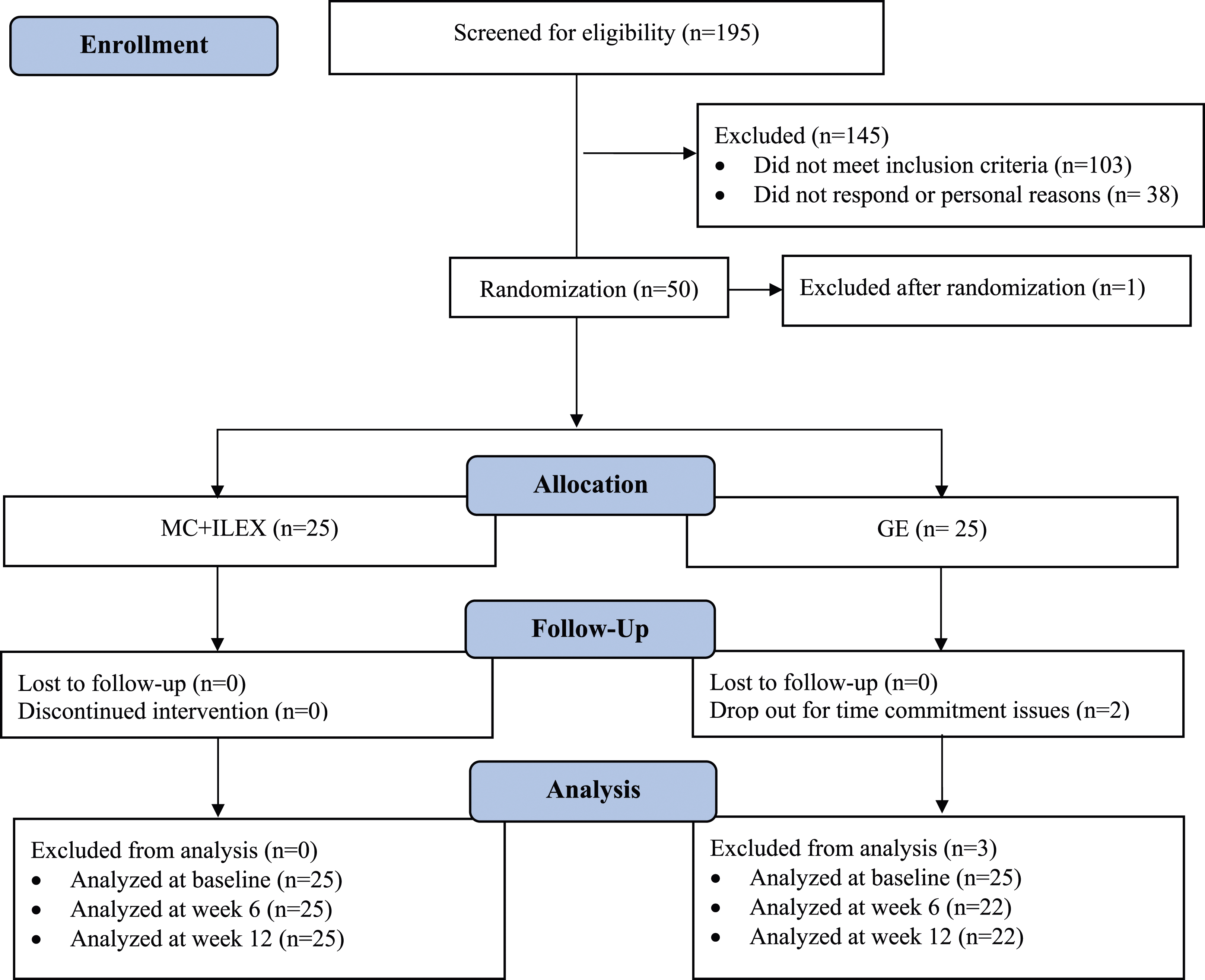
This study was a two-arm prospective randomized controlled trial (RCT), with outcomes collected at baseline, 6 and 12 weeks follow-up (refer to Figure 1 in the Appendix).
Study Setting
This study was conducted at the School of Health, Concordia University (registration trial NTCT04257253). The study was approved by the Central Ethics Research Committee of the Quebec Minister of Health and Social Services (# CCER-19-20-09) and the protocol has been published. 40 All participants signed a consent form before beginning the study.
Participants
Participants were recruited from the School of Health Athletic Therapy clinic and through poster and media advertising (e.g. email blast by the School of Health) which our lab has used before. 40 If individuals expressed interest in participating in the trial, a member of the research team contacted them to discuss the study further to confirm eligibility, obtain consent, and enroll them. Participants were recruited according to the following criteria. Inclusion: 1) chronic non-specific LBP (>3 months), defined as pain in the region between the lower ribs and gluteal folds, with or without leg pain; 2) currently seeking care for LBP; 3) aged between 18 to 65 years old; 4) English or French speakers; 5) have a score of “moderate” or “severe” disability on the modified Oswestry Low Back Pain Questionnaire; 6) do not currently engage in sports or fitness training specifically for the lower back muscles (3 months prior the beginning of the trial). Exclusion: 1) evidence of nerve root compression or reflex motor signs deficits (e.g. weakness, reflex changes, or sensory loss with same spinal nerve); 2) previous spinal surgery or vertebral fractures; 3) other major lumbar spine structural abnormalities (e.g. spondylolysis, spondylolisthesis, or lumbar scoliosis >10°); 4) comorbid health conditions that would prevent active participation in exercise programs (e.g. screened with Physical Activity Readiness Questionnaire).
Randomization and Blinding
Following written informed consent, participants were randomly assigned to treatment groups (1:1). Random allocation was conducted by an individual not involved in the study who created consecutive numbered sealed opaque envelopes (e.g., computer-generated randomization sequence with permuted blocks). Participants were informed of their allocation by the therapists. Only the assessor was blinded to participants’ characteristics, since blinding of therapists and participants is normally not feasible in exercise interventions. 41
Procedure
The intervention period was 12 weeks, with a frequency of 2 times per week and about 45 minutes per session for each group. This frequency of training was chosen over more frequent training as there is a potential for overtraining when lumbar extensor muscles are isolated. 42 Moreover, additional weekly session offers no further improvements in symptomatic patients.43,44 The period of 12 weeks was chosen since strength improvements from training mainly occurs within that time period. 45 A graduate student in Exercise Science supervised the GE training sessions and a certified athletic therapist supervised the MC + ILEX sessions (i.e. 1 student assigned to each group). Both groups were encouraged to follow home exercise programs 2-3 times per week during and after the intervention period. All exercise sessions took place on the School of Health conditioning floor.
Exercise Interventions
Each intervention has been reported in detail in previous publications.33,40 Therefore, only the main components of both interventions will be described in the current paper.
General Exercise Group (Control Intervention)
Participants in this group performed a generalized exercise program comprising a 10 minute aerobic warm-up (e.g. walking or cycling program), resistance training exercises, and finishing with trunk-leg stretching exercises. 23 The machine-based resistance exercise program was separated into 2 days (non-consecutive days) with a focus on different muscle groups each day. Three sets were completed for each exercise. The level of difficulty was progressed gradually based on a study protocol created by Iversen et al. 46 targeting the following repetition format: week 1-2, 15-20 repetitions; week 3-5, 12-15 repetitions; week 6-8, 10-12 repetitions; week 9-12, 8-10 repetitions. Weights were increased by 5% once the participants were able to perform 2 or more repetitions than the number assigned for that period. The purpose of the control intervention was to restore patients to the normal activities of daily living (e.g. rising, bending, lifting, walking) by improving lower-body strength and flexibility. Such generalized exercise programs have been shown to be beneficial for the rehabilitation of patients with non-specific LBP by decreasing pain and enhancing function, 23 but are not intended, nor expected to have an impact on paraspinal muscle morphology. 27
Combined Motor Control and Isolated Lumbar Extension Exercise Group (MC + ILEX)
Patients in this group performed MC training which was based on a variety floor exercises in different starting positions (e.g. supine/crook lying, side-lying, prone) intended to directly activate the MF and transversus abdominus in a co-contraction. 47 The goal of these exercises is to enhance neuromuscular control and dynamic stability of the spine in a functional way. The first phase (cognitive) aimed to correct muscle patterns by increasing the activation of deep trunk muscles (e.g., MF and transverse abdominus muscles) and reducing the activity of the superficial muscles while having normal breathing patterns. The second phase (autonomous activation) included the addition of low load to the muscle by means of leverage through the limbs first into static positions and then into dynamic positions. 48 The aim was to progress to automatic activation of deep trunk muscles with coordination of superficial muscles. Lumbar extensor muscle strengthening exercises was performed in parallel to the MC exercises using the MedX Lumbar Extension Isokinetic Dynamometer. This machine allows for isolated testing and strengthening of the lumbar extensors through a unique pelvic stabilization system, which removes the activation of synergistic and compensatory muscles. Participants performed 2 sets of 15-20 repetitions of lumbar extension in the flexion-extension plane of movement at a resistance load of 55% of their one repetition maximum at 24°. The resistance load was increased by 5% at the next session 49 or once the participant was able to complete 15-20 repetitions before failure.
Data Collection
All outcomes were obtained at baseline for both intervention groups. All baseline assessments (e.g. MRI, strength, questionnaires) were repeated at 6- and 12-weeks follow-up. Self-reported questionnaires were completed in-person using paper forms. Magnetic resonance imaging (MRI) outcomes and lumbar extensor muscle assessments (e.g., strength) were obtained at the School of Health, Concordia University. Demographic characteristics were obtained via self-reported questionnaires at baseline, after the randomization.
Outcome Measures
Primary Outcome Measures
1) Multifidus muscle 3D volume and FI at the L1-L2, L2-L3 and L3-L4 levels.
Secondary Outcome Measures
1) Erector spinae 3D volume and FI at the L1-L2, L2-L3 and L3-L4 levels, 2) kinesiophobia, 3) catastrophizing, 4) depression/anxiety, 5) sleep quality, 6) pain, 7) disability, 8) quality of life, and 9) lumbar extension strength.
Measurement Tools
MRI Assessment of Paraspinal Muscle Morphology
All participants underwent baseline routine lumbosacral MRI evaluation prior to the beginning of the exercise intervention using the School of Health’s 3-tesla GE machine. Axial T2-weigthed and DIXON (Lava-flex, 2 echo sequence) were obtained from L1 to L5 to assess the paraspinal muscle morphology and composition. Bilateral manual segmentation of regions of interest (ROI) representing the CSA of each muscle were acquired on axial T2-weighted slices at L1-L2, L2-L3, and L3-L4 to calculate the summative 3D volume of the right and left side (more accurate assessment than single slice). More specifically, measurements were acquired across 5 slices for each level, from the lower endplate of the above vertebra to the upper endplate of the below vertebra. Dixon axial water and fat images were used to calculate the percent fat-signal fraction: %FSF=(Signalfat/[Signalwater + SignalFat]x100) of each muscle at every spinal level. The Horos DICOM viewer software was used for imaging analysis. Right and left volume and %FI measurements were averaged for each level, and used in the analyses.
Segmentation Method
The MF muscle’s medial border was defined from the spinous process’ most superficial to deep portion where it connects to the lamina. The MF muscles’ anterior and deep border was outlined between the lateral portion of the lamina to the anterior portion of the mammillary process and zygapophyseal joint. It connected with the ES muscle’s anterior and deep border where it continued through the lateral portion of the transverse process. The ES muscle’s posterior border was outlined by the fascial plane, which included the epimuscular “fat-filled tent” between the longissimus and iliocostalis muscles when present. Epimuscular fat tents that were lateral to the iliocostalis muscle and beneath the lumbosacral fascia were also included in the ROI.50,51
To test the reliability for MF and ES muscle measurements (Volume and %FI), the MR images of 10 participants were randomly selected by the rater (B.R.) and measured independently. After at least 5 days, the same measurements were repeated.
Lumbar Extensor Muscle Strength
Lumbar extensor isokinetic muscle strength was assessed using the MedX Lumbar Isokinetic Dynamometer (MedX, Ocala, FL). The MedX allows for complete stabilization of the pelvis, which eliminates the activation of the gluteal and hamstring muscles which is a key element to isolate the lumbar spinal musculature during strength testing and therapeutic training, hence the name Isolated Lumbar Extension (ILEX). Due to equipment failure with the load cell of the machine, strength data was unavailable for some participants for a short period of time, limiting our sample size to 26 participants who completed the strength tests at all timepoints. More details of the procedure are described in the published protocol. 40
Questionnaires
Pain, disability, quality of life, pain-related fear (catastrophizing and Kinesiophobia), depression, anxiety, and sleep quality were assessed by self-reported questionnaires. Participants were asked to complete the Short-Form 12 Item Survey questionnaire (SF-12), modified Oswestry Low Back Pain Disability Index (ODI) and numerical pain rating scale to measure patients’ quality of life, disability/functional status and related pain, respectively. The Pain Catastrophizing Scale (PCS) and the Tampa Scale of Kinesiophobia (TSK) were used to measure pain-related fear. The Hospital Anxiety and Depression Scale (HADS) were used to assess depression and anxiety, and the Insomnia Severity Index (ISI) was used to assess sleep disturbances. All questionnaires have previously demonstrated a good level of test-retest reliability and have been validated in individuals with chronic LBP.52-60
Sample Size Justification
A total of 50 patients were recruited (25 in each group). An a priori sample size was calculated by using the effect size (e.g. significant increase in MF muscle size measurements after a MC intervention) from an earlier study. 61 Therefore, sample size estimation was calculated, using G*power software (version 3.1), by using a mean effect size of 0.90, 80% power and a significance level of alpha 0.05, and allowing for a 10% buffer for potential loss to follow-up and 10% treatment non-adherence.
Statistical Analysis
Primary and secondary outcome measures were first analyzed using descriptive statistics. Intra-class correlation coefficients (ICCs) were used to assess intra-rater reliability of the paraspinal muscle measurements; ICC(2,1) were calculated using a 2-way random-effects model, single-measurement, and absolute agreement and the following agreement interpretation guidelines (i.e., <0.50 = poor, 0.50-0.75 = moderate, 0.75-0.90 = good, and > 0.90 = excellent). 62 Between- and within-subjects repeated measures analysis of variance (ANOVA) were used to assess the change in all outcomes for all time points. Changes in paraspinal muscle measurements of interest were adjusted for baseline values. Pearson correlations were used to evaluate the association between changes in paraspinal muscle morphology and changes in pain, disability/function status, quality of life, pain related fear, depression, anxiety, and sleep quality. Crude Pearson correlations and partial correlations adjusted for BMI and age were used to evaluate the association between changes in paraspinal muscle morphology and changes in strength. Associations between muscle morphology and strength were calculated for the combined upper lumber levels (L1-L2, L2-L3 and L3-L4) and compared to the combined lower lumbar levels (L4-L5 and L5-S1), which we previously investigated 33 but did not reported on. Strength of correlation was defined according to Cohen’s guidelines. The strength of correlation coefficients (r) were interpreted as 0.1 to 0.2, 0.3 to 0.5, and >0.5 indicating small/weak, medium/moderate and large/strong correlations, respectively. 63 All statistical analyses were performed using IBM SPSS version 28.0 (IBM Corp., Armonk, NY, USA); a P-value of <0.05 was considered statistically significant.
Results
Participants
Participants’ Baseline Characteristics.
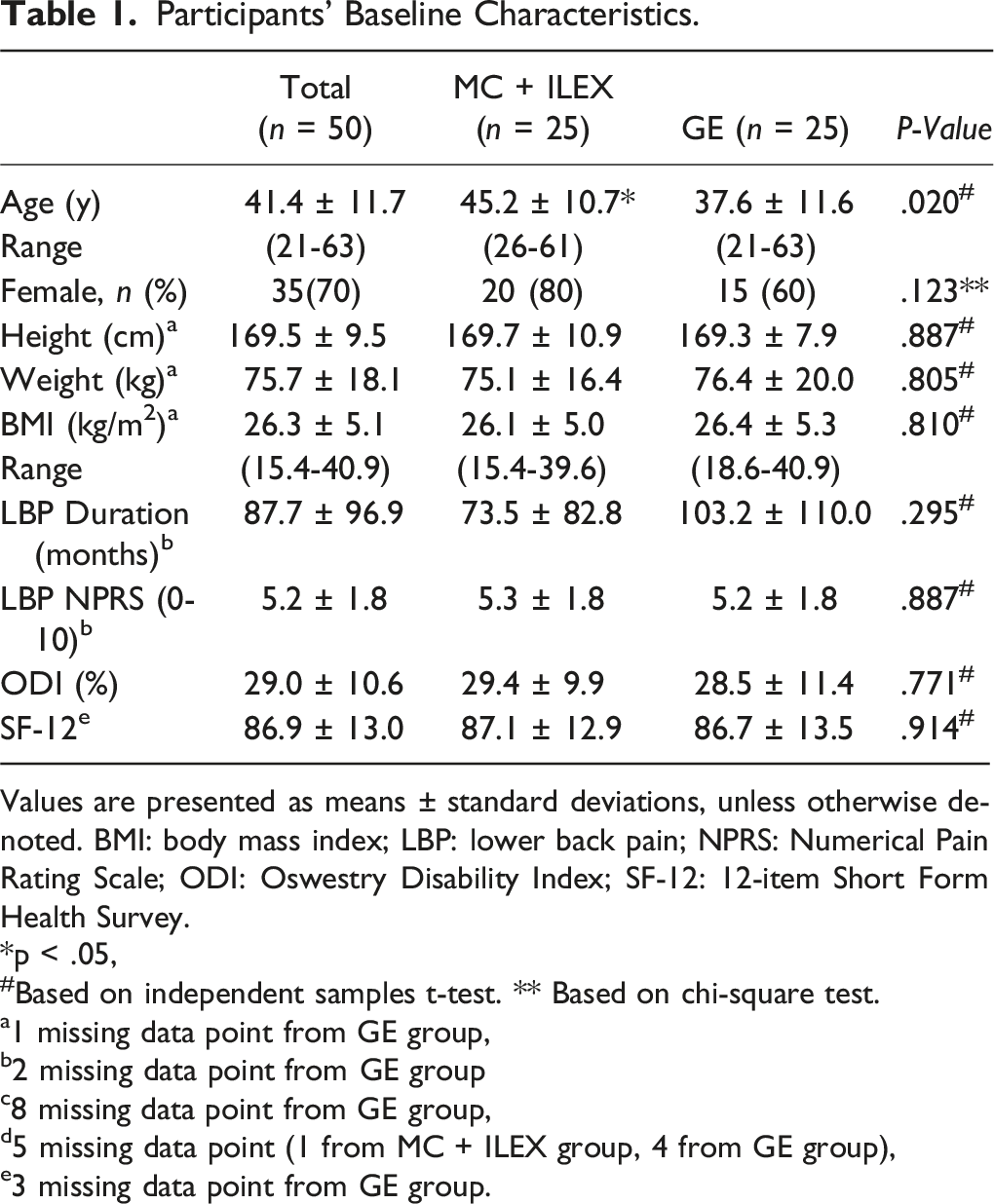
Values are presented as means ± standard deviations, unless otherwise denoted. BMI: body mass index; LBP: lower back pain; NPRS: Numerical Pain Rating Scale; ODI: Oswestry Disability Index; SF-12: 12-item Short Form Health Survey.
*p < .05,
#Based on independent samples t-test. ** Based on chi-square test.
a1 missing data point from GE group,
b2 missing data point from GE group
c8 missing data point from GE group,
d5 missing data point (1 from MC + ILEX group, 4 from GE group),
e3 missing data point from GE group.
Reliability
As seen in Table A1 in the Appendix, excellent intra-rater reliability (ICCs > 0.90) was observed for volume and %FI, with the exception of left MF volume at L1-L2 (ICC = 0.874).
Effect of MC + ILEX and GE on Fatty Infiltration (% Fat Infiltration)
Adjusted Multifidus and Erector Spinae Muscle % Fatty Infiltration Means in the MC + ILEX and GE Groups.
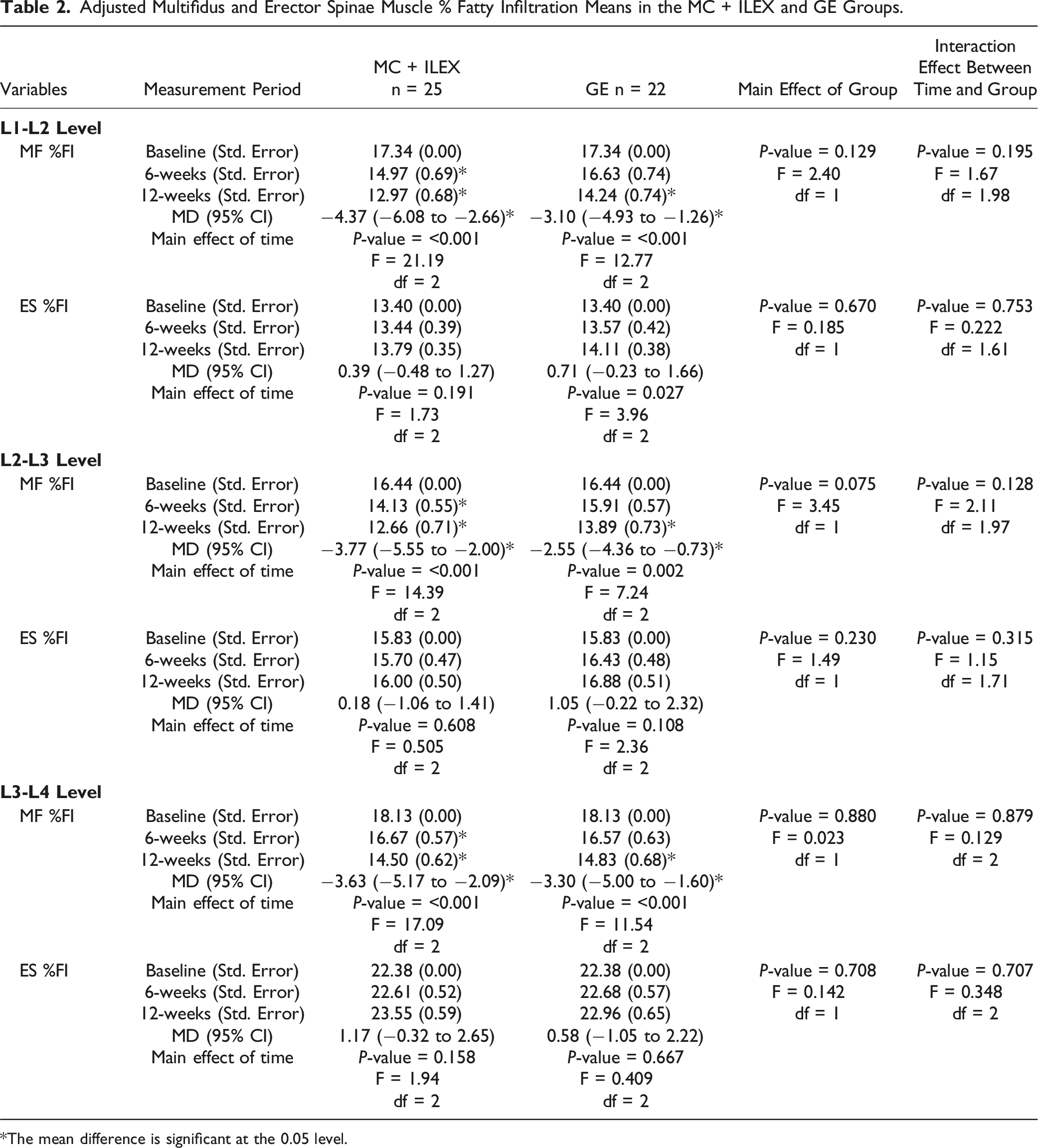
*The mean difference is significant at the 0.05 level.
Effect of MC + ILEX and GE on Muscle Volume
Adjusted Multifidus and Erector Spinae Muscle Volume Means in the MC + ILEX and GE Groups.
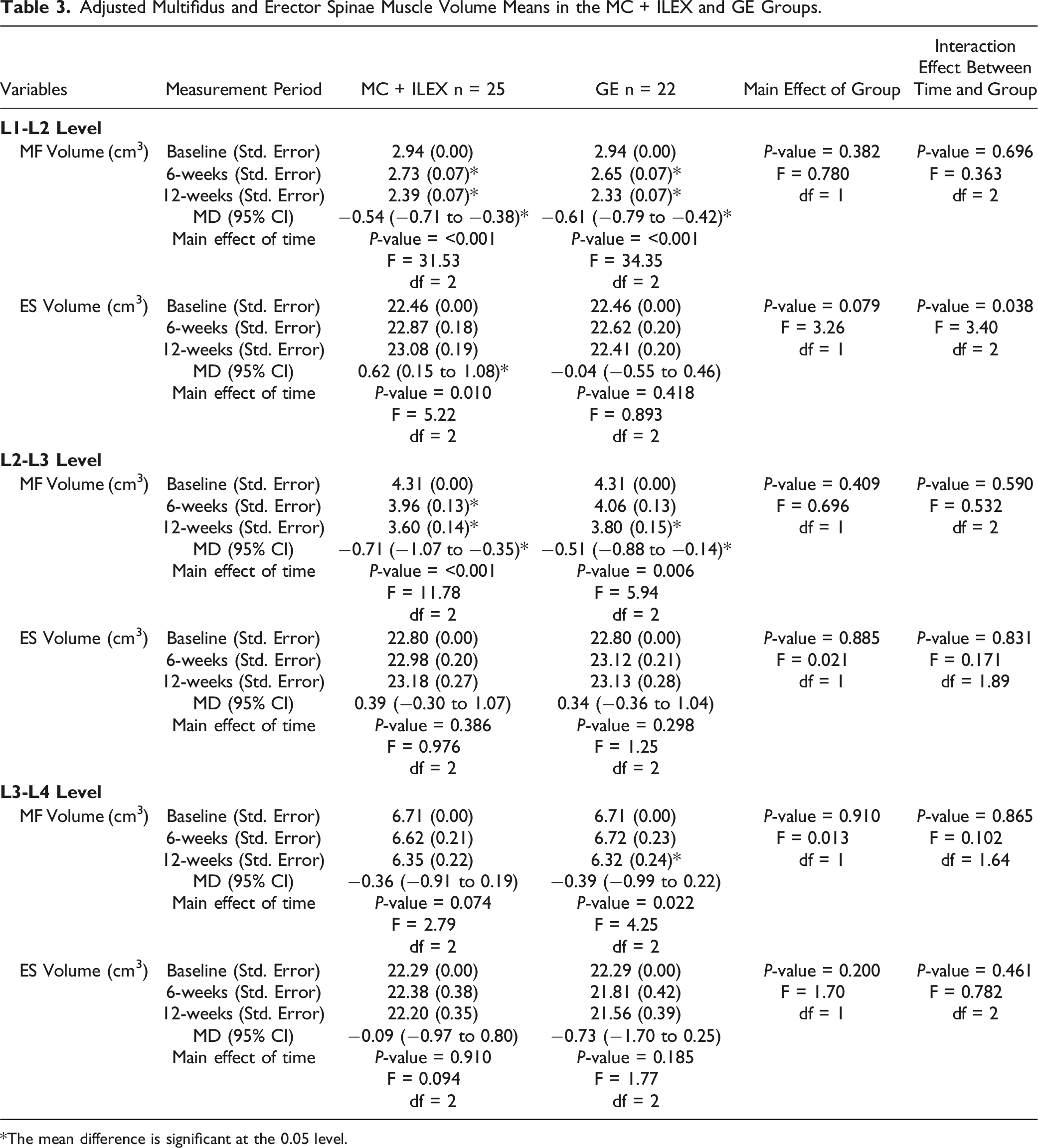
*The mean difference is significant at the 0.05 level.
Patient-Reported Outcome Measures
The effect of both interventions on pain, disability, and quality of life have been reported in a previous related publication. 33
Comparison of Psychosocial Factors (e.g. Catastrophizing, Kinesiophobia, Anxiety, Depression, and Sleep) in the MC + ILEX and GE Groups.
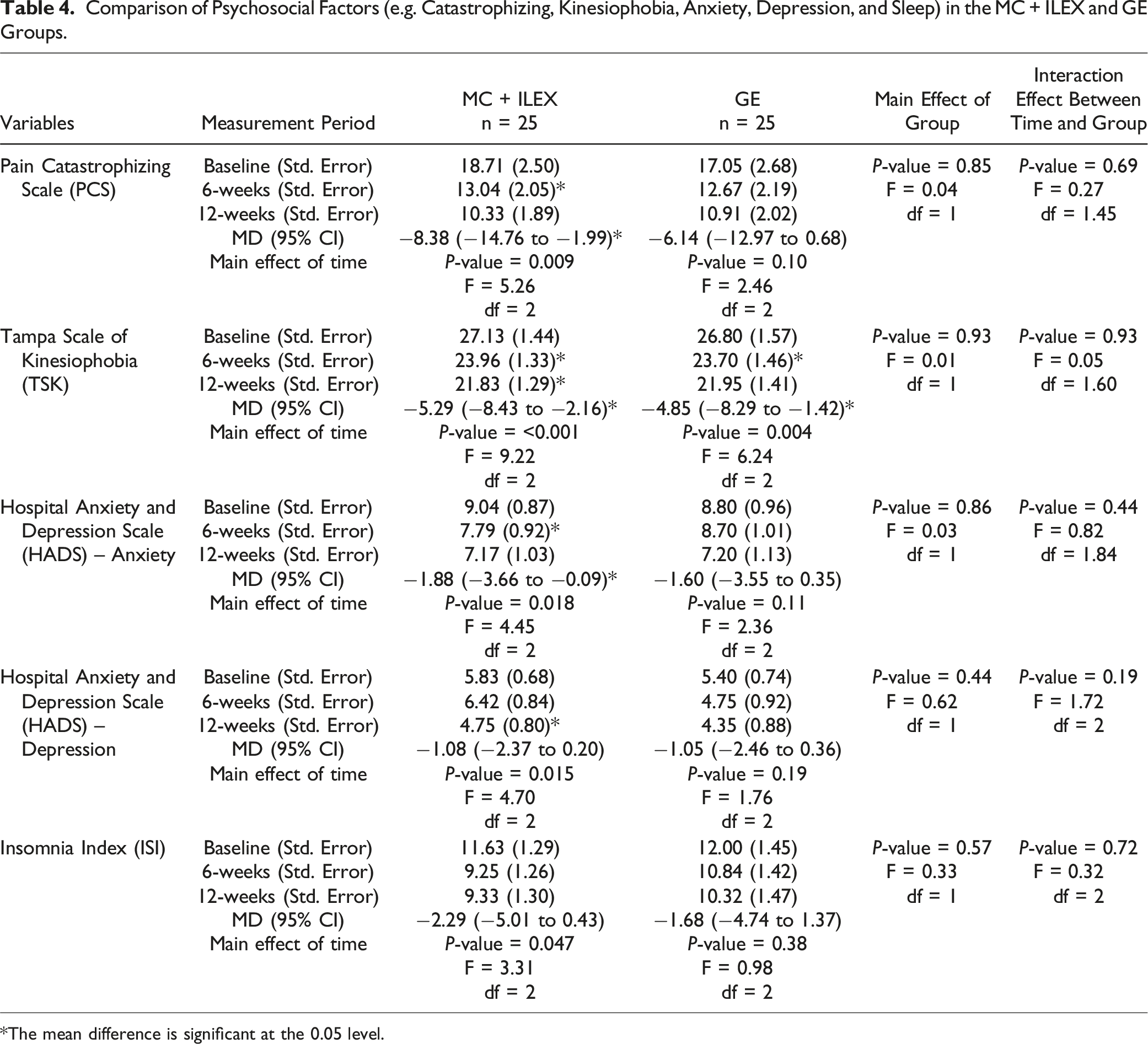
*The mean difference is significant at the 0.05 level.
Correlation Between Changes in Muscle Morphology and Patient-Reported Outcome Measures
Correlations Between Changes in the Muscle Morphology (L1-L2, L2-L3 and L3-L4 Levels Combined) and Changes in Pain, Disability and Quality of Life.
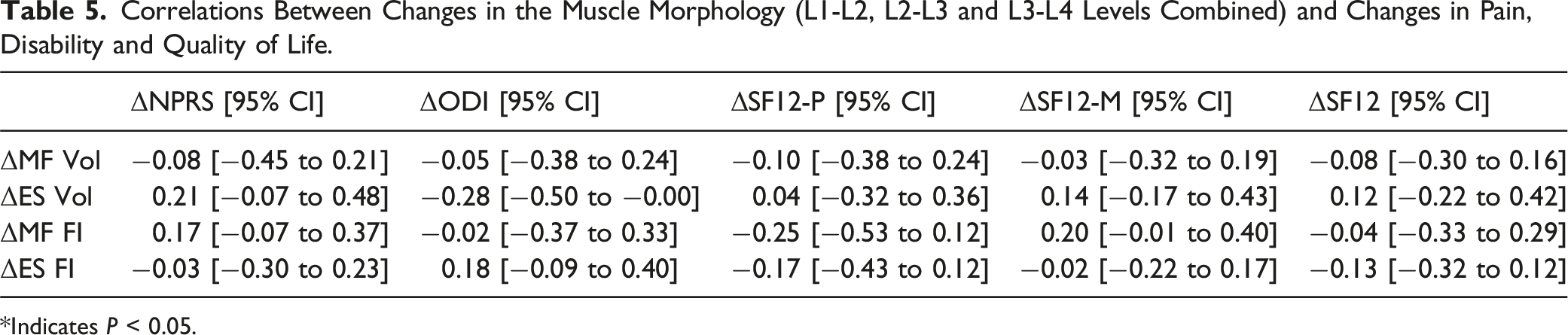
*Indicates P < 0.05.
Correlations Between Changes in the Muscle Morphology (L1-L2, L2-L3 and L3-L4 Levels Combined) and Changes in Psychosocial Factors (e.g. Catastrophizing, Kinesiophobia, Anxiety, Depression, and Sleep).
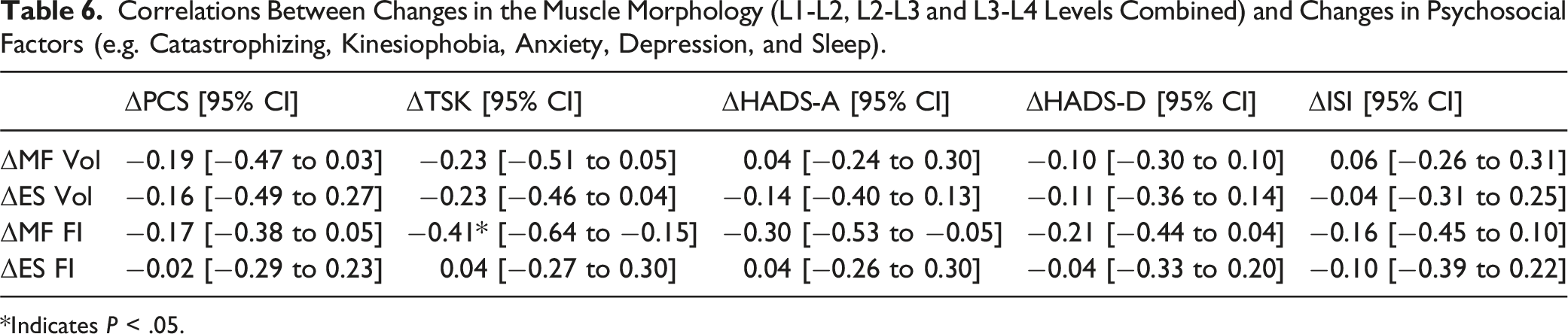
*Indicates P < .05.
Correlation Between Changes in Muscle Morphology and Strength
Crude and Adjusted Partial Correlations Between Changes in the Muscle Morphology (Upper and Lower Levels Combined) and Change in Mean and Max (36°) Strength.
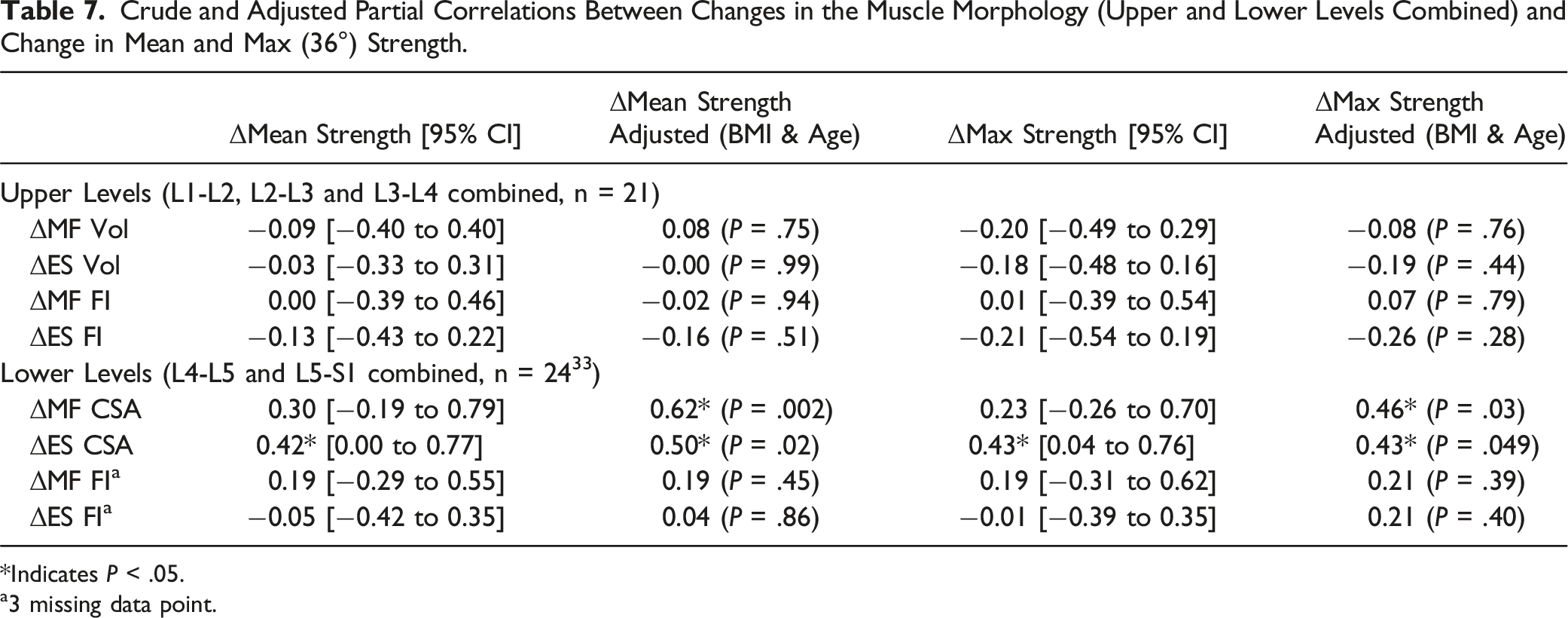
*Indicates P < .05.
a3 missing data point.
Discussion
Summary of Findings
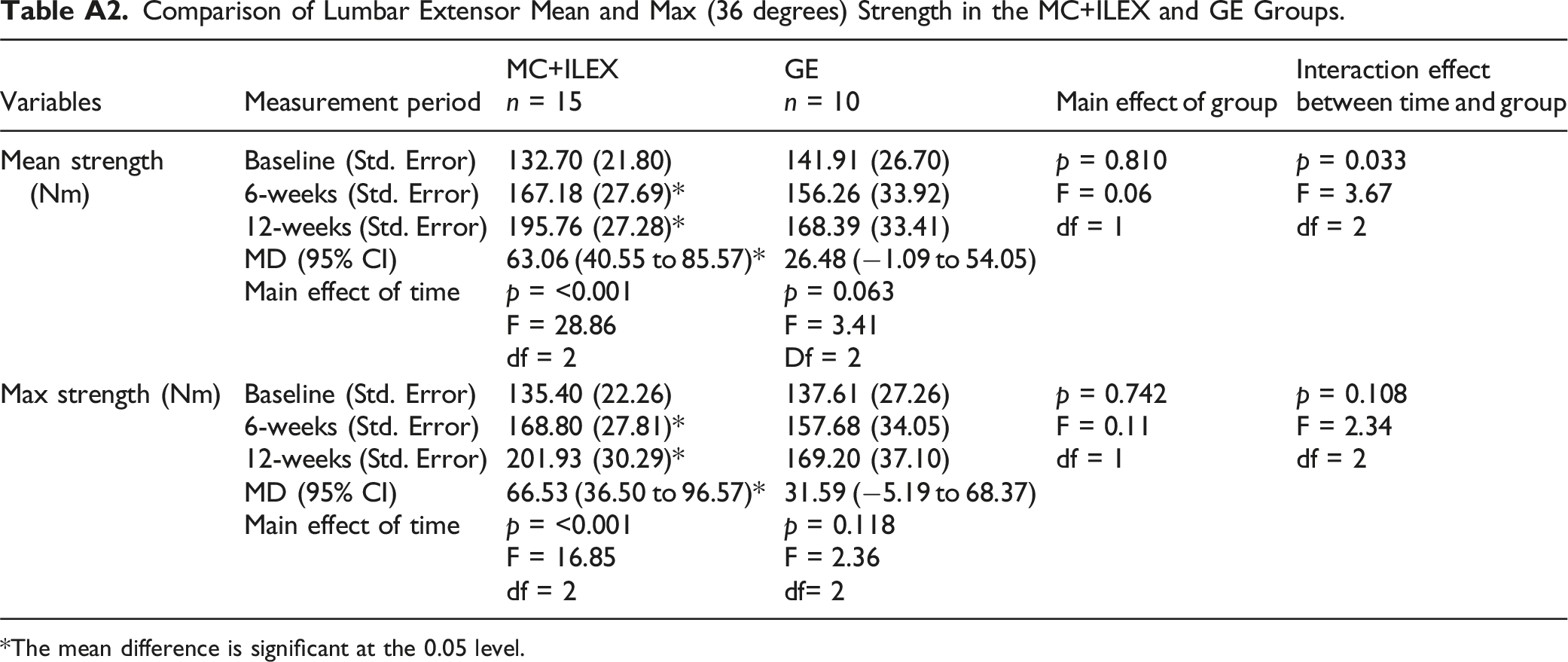
This study provides novel findings about the effect of two different exercise interventions on upper lumbar paraspinal muscle morphology, which is understudied but has been implicated in the development of LBP, 39 and its association with patient-reported outcomes. Our results revealed no significant between-groups findings for MF and ES %FI and volume. Notably, each group displayed significant within-groups decreases in MF %FI at L1-L2, L2-L3 and L3-L4, with concomitant within-groups decreases in MF volume at L1-L2 and L2-L3, and at L3-L4 in the GE group. Our results also showed a significant within-groups increase in ES %FI in the GE group and in ES volume in the MC + ILEX group, both at L1-L2. An analysis of patient-reported outcomes showed no significant between-groups findings, but each group displayed significant improvements in Kinesiophobia, while only MC + ILEX had significant improvements in catastrophizing, anxiety, depression and sleep. Furthermore, MC+ILEX displayed significant improvements in lumbar strength at both 6-weeks and 12-weeks follow-up. Lastly, significant correlations were found between change in upper lumbar MF %FI and Kinesiophobia, and between change in lower lumbar paraspinal muscle CSA and strength.
Effect of MC + ILEX and GE on Fatty Infiltration (%FI) and Muscle Volume
Both a 12-week MC + ILEX or GE intervention had a significant effect on FI in the upper lumbar levels. A significant decrease in MF %FI in both groups was seen at L1-L2, L2-L3 and L3-L4 (all above the minimal detectable changes – Table 2) in the MC + ILEX group, with an increase in ES %FI in the GE group at L1-L2. Our study also revealed a significant concomitant decrease in MF volume in both groups at L1-L2 and L2-L3, and in the GE group at L3-L4, which were all below the minimal detectable changes. Snodgrass et al. investigated cervical muscle volume and FI in people with chronic idiopathic neck pain compared to age and sex-matched asymptomatic controls, 64 and reported greater cervical MF volume and FI in participants with chronic pain as compared to the controls, with similar relative volume. Indeed, higher levels of FI in the MF may be a contributor to or a sign of the development or persistence of LBP. 64 In a recent study, the same authors again investigated people with and without chronic idiopathic neck pain, but analyzed recovery patterns 6 months later. 65 Supporting our findings, results showed that while neck muscle FI increased in the not recovered group, FI and volume decreased in the recovered group and the asymptomatic group, especially in the MF. Although the authors investigated the cervical spine, this still may explain why our study observed a concomitant decrease in muscle volume with an exercise induced decrease in %FI in the lumbar MF, as FI could decrease along with volume during recovery but increase when pain persists. Of note, in our previous work investigating the lower lumbar spinal levels, the MC + ILEX intervention led to a significant increase in MF CSA with no change in FI at L4-L5 and L5-S1, while no MF morphological changes were observed in the GE group. 33 This suggests important differences in paraspinal muscle physiological adaptations in response to exercise interventions between the upper and lower spinal levels, emphasizing the importance of analyzing levels separately. 66 A large body of evidence clearly demonstrates that paraspinal muscle FI is markedly greater at the lower lumbar levels (as compared to the upper levels) in individuals with and without LBP,37,38 with a 15-year longitudinal also reporting greater changes in paraspinal muscle morphology (increased atrophy and FI) at L5-S1 relative to L3-L4 over time. 34 Most bodyweight is tolerated at the L5-S1 level, inducing larger stress at that level. 34 Therefore, it is not surprising that the lower lumbar levels are the levels most associated in failure, with a greater incidence of spinal pathology and degenerative changes.35,36 Since a high amount of intramuscular FI may be more resilient to morphological changes, 32 the greater amount of fat at the lower lumbar levels compared to the upper levels could partly explain our findings. 37 Reversing FI through means of exercise at the lower lumbar levels likely require a larger force, with more frequent and longer training sessions at higher muscle loads. While the proper exercise prescription for decreasing FI still remains unclear,67,68 at least 8 weeks of exercise training has led to clear changes in the homeostatic myocellular setting, 69 which could take longer in untrained people. 70 In accordance with a recent systematic review, 67 previous exercise interventions were likely too short and used insufficient intensities to result in paraspinal compositional changes at the lower lumbar levels, which are most commonly investigated levels. Indeed, only one study has investigated the effect of an exercise intervention on paraspinal muscle morphology both at the upper and lower spinal levels. 71 For example, a high-intensity resistance-based exercise program reported no significant compositional (FI) changes in the ES or MF at the midlevel of the L4 vertebrae in patients with chronic LBP, 28 but the effect of the intervention at the upper spinal levels was not investigated. However, the upper lumbar levels require further investigation as LBP has been shown to be associated with paraspinal muscle FI at every lumbar level, with severe FI of the upper ES muscle possibly being a feature of LBP. 39
In terms of muscle composition, we are only aware of one study that reported a reduction in paraspinal muscle FI following a 16-week free-weight-based resistance training program. 32 Though, they only investigated the lower levels of the lumbar spine and used sub-optimal paraspinal muscle measurements. With regards to muscle size, the current study also showed a significant interaction effect between time and group in L1-L2 ES volume, in which only the MC + ILEX group had a significant increase. Motor control interventions focus on efficient trunk muscle activation, 24 while targeted strengthening exercises enhance lumbar muscle strength and limit global muscle involvement of the posterior chain (e.g., gluteus and hamstrings) when used with pelvic restraints.16,30 Again, pelvic stabilization during extension exercises could assist in ILEX and lead to morphological changes, especially when MC ensures proper recruitment of targeted muscles. Therefore, it is not surprising that only the MC + ILEX group demonstrated an increase in ES volume and strength. While exercise studies investigating paraspinal morphology in the upper lumbar spinal levels are limited, the studies investigating the lower levels have shown mixed results in improving lumbar paraspinal muscle size.28,29,33 Tagliaferri et al. investigated the effects of 6 months of MC exercise with spinal manual therapy vs general strength and conditioning (involving components of lumbar strengthening) on combined muscle volume (L1-L5) in 40 chronic LBP patients. 71 They reported no change in MF, ES, psoas major and quadratus lumborum total volume (L1 to L5) at 6 months, except for a significant increase in MF volume in the general strength and conditioning group only. Changes in muscle composition (e.g., FI) were not investigated. Interestingly, however, when performing analysis separately for each spinal level (e.g., middle 3 slices for each spinal level) the authors reported a significant increase in MF CSA at L3, L4 and L5 in the general strength and conditioning group at 6-months, and a significant decrease in MF CSA at L1 in the motor control group at 3-months, which was nearly significant (P = 0.05) at L2 as well. Therefore, the results of Tagliaferri et al. 71 are in accordance our findings both from our previous published work 33 and the current study as whole-body general strength program, which included lumbar strengthening, improved MF size at the lower lumbar levels and that MC training led to a similar decrease in MF size at the upper lumbar levels. This further suggest that changes in paraspinal muscle morphology could be muscle and level dependent.
Finally, variations in segmentation methods and imaging sequences also contribute to inconsistent paraspinal muscle morphological findings, and complicate direct comparison between studies. Current imaging studies use different segmentation methods, which are often not thoroughly described and either “include” or “exclude” the epimuscular fat, when present, in the ROI of lumbar paraspinal muscles. Including epimuscular fat in the ROI does have an impact on CSA and %FI measurements. 50 While there is no clear consensus whether epimuscular fat should be included or excluded from ROIs, a recent study does suggest that epimuscular is more common at the lower lumbar levels (e.g., L4-L5 and L5-S1) and in subjects with chronic LBP. 72
Psychosocial Factors (Catastrophizing, Kinesiophobia, Anxiety, Depression, and Sleep)
As previously reported, both interventions were successful to improve pain, disability and quality of life (36). While Kinesiophobia improved in both groups, significant improvements in catastrophizing, anxiety, depression and sleep quality were only observed in the MC + ILEX. Psychological and social factors influence pain, and therefore could influence clinical outcomes in people living with chronic musculoskeletal pain. 73 A systematic review found strong evidence of a correlation between higher levels of Kinesiophobia with higher levels of pain and disability in people with chronic musculoskeletal pain. 74 Another systematic review and meta-analysis of RCTs reviewed the effectiveness of exercise training compared to non-exercise comparators on fear avoidance in pain and pain-free individuals. 75 Exercise was more effective than non-exercise comparators in improving fear avoidance or Kinesiophobia in both LBP and chronic LBP. This is a possible explanation why both our interventions led to similar significant improvements in pain, disability, and Kinesiophobia. Participation in exercise therapy could encourage patients with LBP to confront their fear of performing movements or valued activities of daily living. 75
Motor control training has beneficial effects on pain-related fear in people with chronic LBP.76-78 Eight weeks of patient education with MC exercise and MC exercise alone led to significant improvements in fear-avoidance beliefs and pain catastrophizing in adults with chronic LBP. 76 Even two sessions of a pain neurophysiology education program with therapeutic exercise, which included lower back MC exercises, and therapeutic exercise alone led to improvements in catastrophizing and Kinesiophobia in patients with chronic LBP. 77 Perhaps the gradual exposure and progression of our study’s MC training was similar to graded exercise exposure, which has been seen to improve pain-related fear and avoidance behaviors in people with chronic musculoskeletal pain. 79 Additionally, a decrease in pain was correlated with decreases in fear-avoidance beliefs and catastrophizing in people with LBP. 80 The MC + ILEX group may have developed a more resilient and positive perception towards their pain condition during the intervention. This could have been achieved through an exercise induced improvement in self-efficacy, 81 a key factor in the management of chronic pain, defined as an individual’s confidence in their ability to establish and accomplish actions necessary to reach specific performance goals. 82 In terms of pain, pain self-efficacy is as an individual’s confidence in their functional ability despite their painful state. 83 Therefore, low self-efficacy could result in increased catastrophizing, anxiety, depression and ultimately a poor self-perception of one’s pain condition. 84 Our results suggest that the combination of MC and ILEX may have provided a way for individuals with chronic LBP to feel as though they are efficiently taking control of their condition, providing them important feelings of self-improvement. Supporting our findings, a 10-week high-intensity general resistance exercise program did not significantly improve anxiety or depression in people with LBP. 28 It is also proposed that depressive symptoms are significant moderators of the relationship between sensorimotor exercise training and improvement in pain in chronic LBP. 85 Further depressive mood and anxiety significantly moderated the effect of sensorimotor exercise on disability. 85 Therefore, psychosocial outcomes, such as depression and anxiety, could moderate the relationship between MC exercise induced changes in chronic LBP. This could also explain the inconsistent results seen across studies investigating the effects of different types of exercise in chronic LBP, and highlights the importance of identifying psychosocial risk factors to personalize treatments. Overall, the participants’ cognitive representation of their condition may have been steered toward a more constructive representation. The cumulative results of improved pain, function and self-efficacy encouraged participants to partake in valued activities again, leading to a sense of fulfilment and a concomitant improvement in catastrophizing, anxiety, and depression.
Correlation Between Changes in Muscle Morphology and Changes in Patient-Reported Outcomes
Previous literature supports the fact that higher paraspinal muscle FI is associated with higher disability in patients with lumbar spine conditions, including chronic LBP,86-89 and could predict greater disability after lumbar spinal surgery. 87 In addition, a recent systematic review found strong evidence of an association between poorer pre-operative paraspinal muscle quality (atrophy and FI) and post-operative complications after lumbar surgery. 90 In terms of patient-reported outcomes, higher disability has been shown to be a significant independent factor of LBP severity, 91 and is significantly correlated with pain in patients with spinal disorders. 92 There is also evidence to support that patients with severe disability (ODI>41) have greater pain following lumbar surgery.93,94 Altogether, considering the severity of disability and paraspinal muscle quality among patients with lumbar conditions is essential, as it has important clinical implications. Though, very few studies have investigated the correlations between temporal paraspinal muscle changes, especially in volume, and patient-reported outcomes.
Our findings between muscle morphology and patient-reported outcomes revealed a significant moderate correlation between change in MF %FI and Kinesiophobia, supporting the idea that changes in muscle morphology may relate to improvements in patient outcomes. Pinto et al. found low-quality evidence of no relationship between MF morphological changes from MC exercise and LBP-related disability. 29 Altogether, the authors concluded that MC exercises may improve lumbar MF morphology in people with chronic LBP, but these alterations may not be related to clinical outcomes. As mentioned previously, a high-intensity resistance-based exercise program did not result in ES or MF morphological changes in patients with LBP. 28 Interestingly, in those that did demonstrate an improvement in muscle size (CSA) and composition (FI), a correlation was seen with their improvements in disability and anxiety/depression. This demonstrates a correlation between improvements in muscle morphology and greater functional improvements. Of note, one study did find a significant association between ES FI and physical activity fear-avoidance beliefs, which remained significantly moderate after correcting for covariates. 95 This finding corroborates with ours as pain-related fear or avoidance behaviors during physical activity may lead to compositional changes from disuse of muscles. Again, while MC and strengthening exercises have specific basis for their mechanisms of action and support of their efficacy to improve patients’ pain and symptoms from RCTs and systematic reviews,16,27,96,97 it cannot be assumed that the improvement in clinical outcomes is a direct result of improvements in specific muscle deficits targeted by exercise. It is therefore suggested that exercise for chronic LBP should be tailored to the individual, due to individual variations in morphological and functional changes in paraspinal muscles. 98 This gives rise to a unique opportunity to identify subgroups of patients with LBP who will better respond to specific exercise interventions.28,98
Correlation Between Changes in Muscle Morphology and Changes in Strength
As a continuation of our previous work, 33 our findings revealed significant moderate to strong correlations between change in parapsinal CSA and strength, despite having wide confidence intervals, at the combined lower level of the lumbar spine (L4-L5 and L5-S1). This finding supports the theory that improvements in paraspinal muscle size could positively influence muscle strength and could partially explain the significant improvement in lumbar extensor strength in the MC+ILEX group. However, studies investigating this relationship remain limited. While Tagliaferri et al. compared the effects of MC exercise with spinal manual therapy vs a general strength and conditioning intervention in chronic LBP, the correlation between paraspinal muscle morphology and strength was not assessed. 71 However, the general strength group did demonstrate simultaneous significant improvements in MF CSA, isometric trunk extension and flexion endurance. In addition, a high-intensity resistance-based exercise program in patients with LBP did find a correlation between improvements in strength in those that demonstrated an improvement in muscle size. 28 In accordance to our findings, the authors propose that muscle health improvements could lead to larger functional improvements. Though, the MC group in Tagliaferri et al.’s study had a significant improvement in trunk extension endurance, without any notable improvements in muscle size. 71 While some studies support the idea that morphological changes in paraspinal muscles can influence muscle recruitment and lead to LBP related motor control dysfunction,99-104 there are limited studies and mixed findings examining the converse relationship, making it difficult to draw conclusions. Surprisingly, we found no correlation between change in paraspinal muscle FI (e.g., quality) and strength, and studies assessing this relationship are scarce. LBP is correlated with FI in the lumbar MF, which may result in lumbar dysfunction, 105 decreased muscle performance106-109 or reduced range of motion. 105 We are aware of only one study reporting a significant association between ES FI and relative back extensor strength, 107 but this study was performed with healthy individuals (without any LBP). The association between paraspinal muscle morphology and strength in individuals with chronic LBP warrants further attention.
Limitations
This study had some limitations. Participant recruitment occurred during COVID-19, which led our facility to have limited hours and capacity restrictions. Therefore, the selection of participants was limited to those who heard about the opportunity via word of mouth or through Concordia University connections, as oppose to from multiple sources. Of note, the participants were aware of which group they were randomized in due to the nature of the interventions given, and therefore blinding of the participants was not possible. Additionally, our sample was primarily composed of female participants.
Conclusions
This study provided preliminary evidence that both exercise interventions may be effective to reduce MF muscle FI at the upper spinal levels in participants with chronic LBP. Additionally, the MC + ILEX intervention led to significant improvements in several important patient-reported outcome measures, especially psychological, and should be considered for the non-operative and post-operative exercise treatment of patients with LBP. Notably, our findings further supported the notion that improvements in overall paraspinal muscle health are associated with concomitant improvements in clinical outcomes, including Kinesiophobia and strength.
Footnotes
Author Contributions
All authors have made substantial contributions to the conception or design of the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agree to be accountable for all aspects of the work ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fonds de Recherche du Québec en Santé (FRQS) grant number 283321, 295685, and 309200, and Multidisciplinary Research Project Grant from the School of Health, Concordia University.
Ethical Statement
Informed Consent
Informed consent was obtained from all participants involved in this study. Written informed consent was obtained from the participants to publish this paper.
Trial registration
NTCT04257253.
Appendix
Intra-Rater Reliability of MF and ES Volume and % Fatty Infiltration. CI: confidence interval; ES: erector spinae; ICC: intraclass correlation coefficient; MDC: minimal detectable change; MF: multifidus; SEM: standard error measurement. Comparison of Lumbar Extensor Mean and Max (36 degrees) Strength in the MC+ILEX and GE Groups. *The mean difference is significant at the 0.05 level.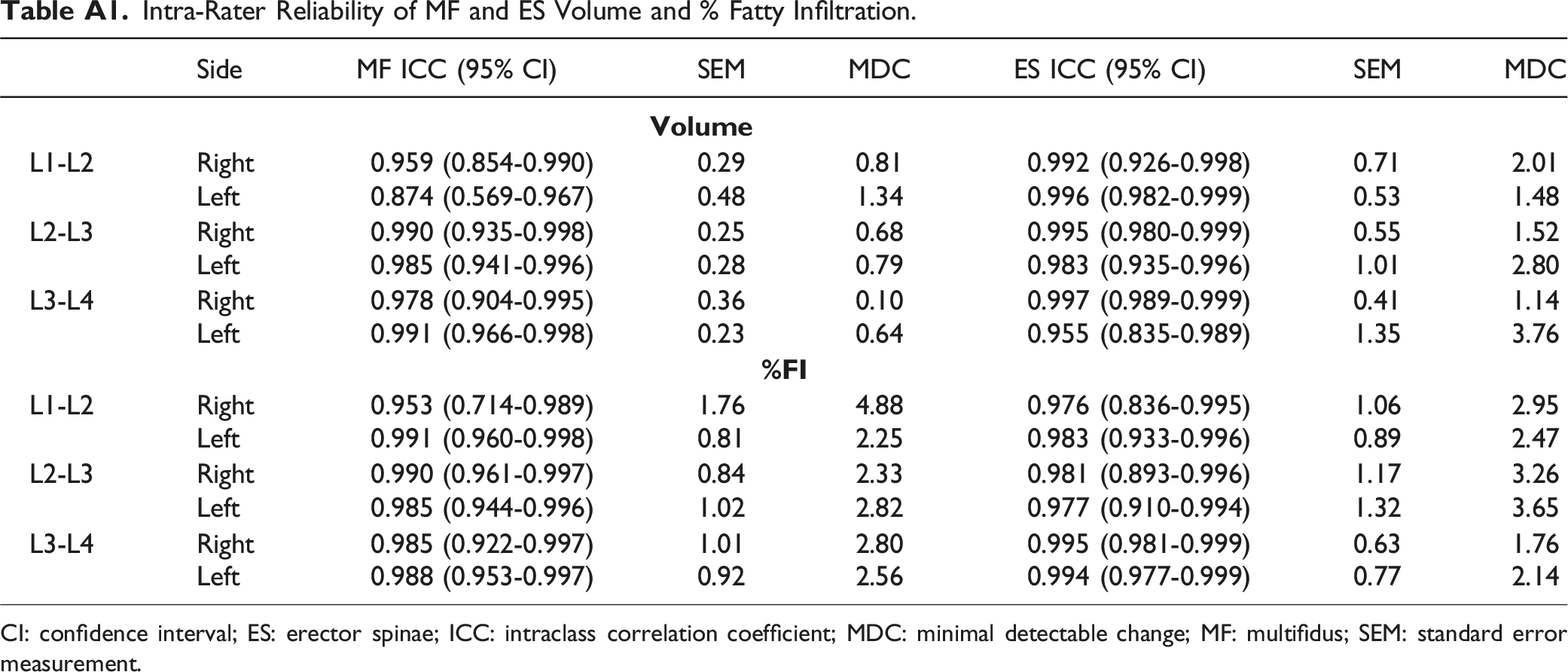
Side
MF ICC (95% CI)
SEM
MDC
ES ICC (95% CI)
SEM
MDC
L1-L2
Right
0.959 (0.854-0.990)
0.29
0.81
0.992 (0.926-0.998)
0.71
2.01
Left
0.874 (0.569-0.967)
0.48
1.34
0.996 (0.982-0.999)
0.53
1.48
L2-L3
Right
0.990 (0.935-0.998)
0.25
0.68
0.995 (0.980-0.999)
0.55
1.52
Left
0.985 (0.941-0.996)
0.28
0.79
0.983 (0.935-0.996)
1.01
2.80
L3-L4
Right
0.978 (0.904-0.995)
0.36
0.10
0.997 (0.989-0.999)
0.41
1.14
Left
0.991 (0.966-0.998)
0.23
0.64
0.955 (0.835-0.989)
1.35
3.76
L1-L2
Right
0.953 (0.714-0.989)
1.76
4.88
0.976 (0.836-0.995)
1.06
2.95
Left
0.991 (0.960-0.998)
0.81
2.25
0.983 (0.933-0.996)
0.89
2.47
L2-L3
Right
0.990 (0.961-0.997)
0.84
2.33
0.981 (0.893-0.996)
1.17
3.26
Left
0.985 (0.944-0.996)
1.02
2.82
0.977 (0.910-0.994)
1.32
3.65
L3-L4
Right
0.985 (0.922-0.997)
1.01
2.80
0.995 (0.981-0.999)
0.63
1.76
Left
0.988 (0.953-0.997)
0.92
2.56
0.994 (0.977-0.999)
0.77
2.14
Variables
Measurement period
MC+ILEX
GE
Main effect of group
Interaction effect between time and group
Mean strength (Nm)
Baseline (Std. Error)
132.70 (21.80)
141.91 (26.70)
p = 0.810
F = 0.06
df = 1p = 0.033
F = 3.67
df = 2
6-weeks (Std. Error)
167.18 (27.69)*
156.26 (33.92)
12-weeks (Std. Error)
195.76 (27.28)*
168.39 (33.41)
MD (95% CI)
63.06 (40.55 to 85.57)*
26.48 (−1.09 to 54.05)
Main effect of time
p = <0.001
p = 0.063
F = 28.86
F = 3.41
df = 2
Df = 2
Max strength (Nm)
Baseline (Std. Error)
135.40 (22.26)
137.61 (27.26)
p = 0.742
F = 0.11
df = 1p = 0.108
F = 2.34
df = 2
6-weeks (Std. Error)
168.80 (27.81)*
157.68 (34.05)
12-weeks (Std. Error)
201.93 (30.29)*
169.20 (37.10)
MD (95% CI)
66.53 (36.50 to 96.57)*
31.59 (−5.19 to 68.37)
Main effect of time
p = <0.001
p = 0.118
F = 16.85
F = 2.36
df = 2
df= 2
Consort Flow Diagram.