
Abstract
Study Design:
Retrospective chart review.
Objectives:
Chiari malformation (CM) is characterized by a downward displacement of the cerebellar tonsils through the foramen magnum. This tonsillar herniation may sometimes be accompanied by syringomyelia and/or basilar invagination (BI). In this study, we examined the surgical outcomes of patients by underwent C1-2 reduction + fixation (C1-2RF), which is a new method defined by Goel, in the literature.
Methods:
Between 2015 and 2018, 21 patients (mean age and duration of follow-up: 39 years and 20 months, respectively) with CM were treated with atlantoaxial fixation. We found syringomyelia in all patients and BI in 9 of them. In all cases, radiography, computed tomography, and magnetic resonance imaging were performed radiologically. C1-2RF was performed in all patients. Preoperative and postoperative clinical Japanese Orthopaedic Association scores were obtained. Syrinx size and cerebrospinal fluid flow rate were compared radiologically.
Results:
All patients were treated with C1-2RF. None of the patients underwent foramen magnum decompression or intervention for the syrinx. Occipital bone and subaxial spinal structures were not included in the fixation. In addition to significant clinical improvement, significant improvement in syringomyelia and cerebrospinal fluid flow rate was seen on the radiographs of all patients.
Conclusions:
Although posterior fossa decompression and/or duraplasty is a common treatment modality in CM, we propose that the C1-2RF method described by Goel is a radiologically and clinically effective treatment method, whether or not BI and/or syringomyelia in CM are present. This article is the first article of central and axial atlantoaxial dislocation, except for Goel’s writings in the literature.
Introduction
Chiari malformation (CM) is characterized by a downward herniation of the cerebellar tonsils through the foramen magnum. CM is often associated with basilar invagination (BI) and syringomyelia.1-11 There are many proposed theories for CM pathogenesis, including molecular, hydrodynamic, and mechanicalaetiologies. 12 A reduced posterior fossa volume, which is associated with genetic syndromes but is more commonly idiopathic, leads to the displacement of the cerebellar tonsils into the spinal canal. 13 Type1 CM is the most common type and occurs in 1 in every 1000 births.14-16 Neurologic signs and symptoms may occur by 2 mechanisms. The first is due to the compression effect on the neural structures around the spinal canal and foramen magnum, and the second is due to neurological damage caused by the development of syrinx cavities inside the spinal cord or brain stem.
The primary treatment for CM is restoration of cerebrospinal fluid (CSF) flow at the craniovertebral junction and elimination of compression on the nervous system structures. Therefore, treatment protocols are widely identified as follows11,17-22: Posterior fossa decompression (PFD) PFD + duraplasty (currently the most widely used method) PFD+ duraplasty and tonsil resection PFD + duraplasty with syringosubarachnoid shunt PFD+ excision of the outer leaf of the dura Atlantoaxial(C1-2) reduction + fixation (C1-2 fix)
It is clearly seen in the literature that there is no definitive surgical treatment modality in CM.14,23-25
In this study, we examine both clinically and radiologically 21 cases on which we performed the atlantoaxial reduction plus fixation method, as described by Goel.
Material and Methods
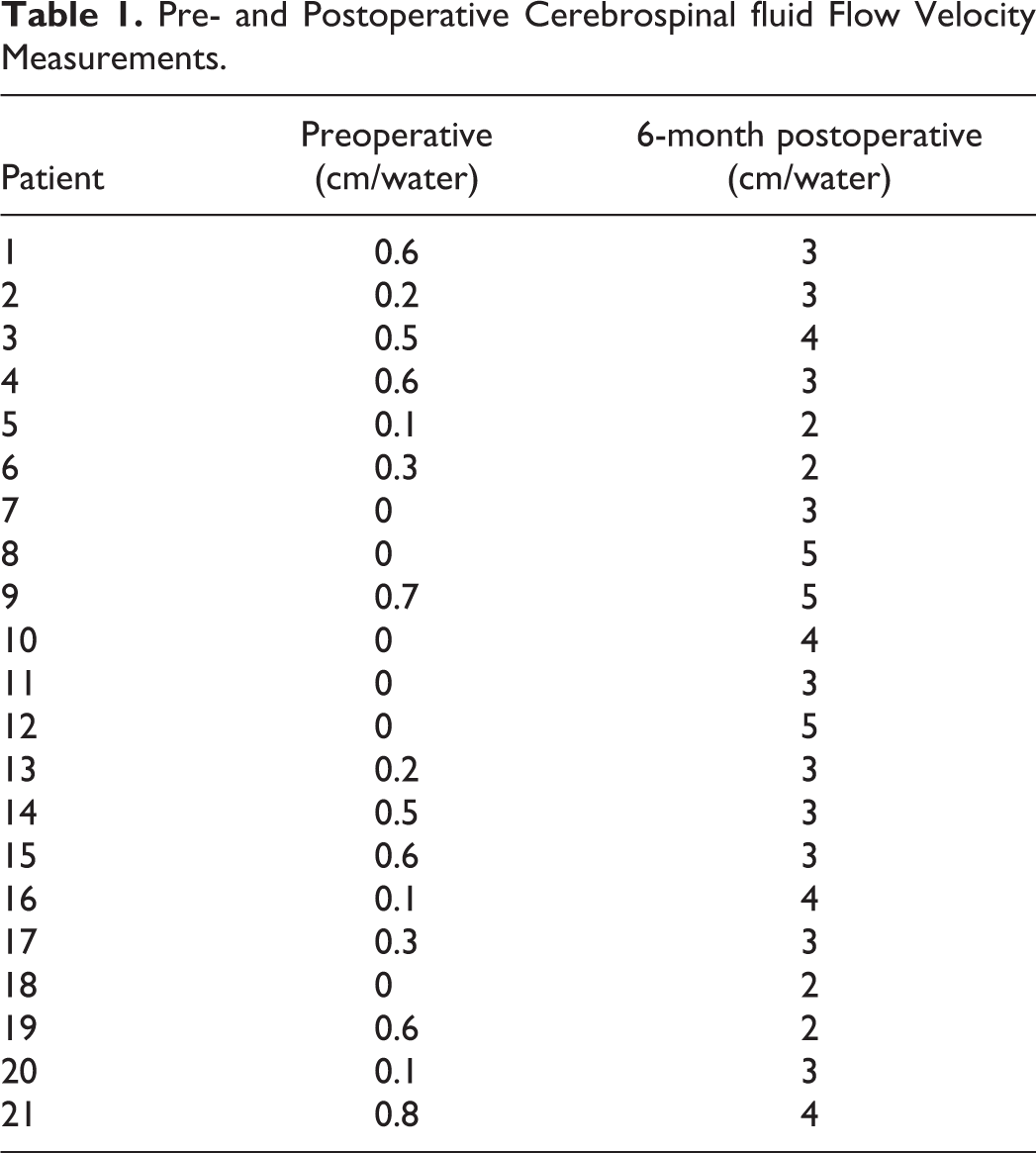
Institutional review board approval was obtained for this study. Eight patients with CM were treated with atlantoaxial stabilization in our department between 2015 and 2018. The patients comprised 13 men and 8 women. The mean age of the patients was 39 years (range, 13-64 years). We found syringomyelia in all patients and BI in 9 of them. Patients with any spinal abnormality, such as spina bifida, brain tumours or hydrocephalus, skull bone anomaly, infections, or connective tissue disorder, were excluded. None of the patients had known syndromic disease (eg, Down, Morquio, or Ehlers-Danlos syndrome). All patients underwent dynamic computed tomography (CT) and magnetic resonance imaging (MRI) with the head in the neutral, flexion, and extension positions. All patients underwent cine MRI for trapping of the CSF flow at the craniovertebral junction for CM. The CSF flow rate was absent or decreased in all patients (Table 1).
Pre- and Postoperative Cerebrospinal fluid Flow Velocity Measurements.
There are 3 types of atlantoaxial dislocations: type 1, anterior atlantoaxial instability; type 2, posterior atlantoaxial instability; and type 3, central atlantoaxial instability (no radiologically demonstrable evidence of instability, which is diagnosed during surgery). On sagittal CT imaging, 7 of our patients had type 1, 6 patients had type 2, and 8 patients had type 3 atlantoaxial dislocation (Figures 2, 3, and 4).
During postoperative follow-up, MRI was performed radiologically on the first day, at 1 month, and at 6 months. The CSF flow rates were examined at 6 months. Preoperative and postoperative clinical modified Japanese Orthopaedic Association (mJOA) and visual analogue scale (VAS) scores were obtained. The mean duration of follow-up was 20 months.
Surgical Method
All patients underwent the atlantoaxial stabilization technique as described by Goel.1,2,26 The patients were placed on the surgical table in the Concorde position, and the head of the operating table was raised to 30°. Traction with Gardner-Wellstongs was applied at a weight appropriate for the age and bodyweight of the patient. Cervical traction was used only intraoperatively and was performed after induction of anesthesia. The purpose of the traction was to stabilise the head in the optimal surgical position. The direction of traction was chosen with the aim of decreasing or eliminating direct compression to the face and eyes.
The main purpose of the surgery was to expose (at this stage, the articular space is mostly exposed after dissecting the C2 nerve roots) and open the atlantoaxial joint. After the articular surfaces were widely decorticated with osteotomes and curettes, bone grafts harvested from the iliac crest were placed in the PEEK (polyetheretherketone) cage (Piron Medical Design; Figure 1) and in the joint cavity. Lateral mass screws were then placed in the C1, and peduncular screws (Piron medical design) were placed in the C2. Reduction and fixation were ensured with rods. Foramen magnum decompression or syrinx intervention was not performed in any patient. Occipital bone and subaxial spinal structures were not included in the fixation. The patients were mobilized with a cervical corset on the first postoperative day.
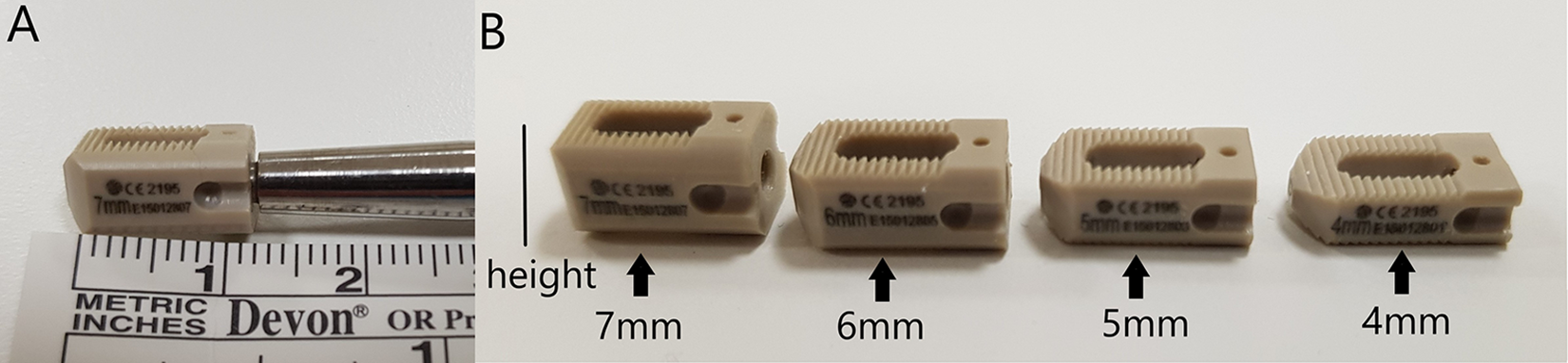
(A) Polyetheretherketone (PEEK) cage size. (B) PEEK cage types.
Results
All patients demonstrated significant clinical improvement in the early postoperative period. The mean duration of follow-up was 20 months. The mJOA of the patients increased from 13.28 to 15.14. The VAS score decreased from 8.42 to 1.9 (Table 2).
Patients’ Pain and Neurological Status Assessment.
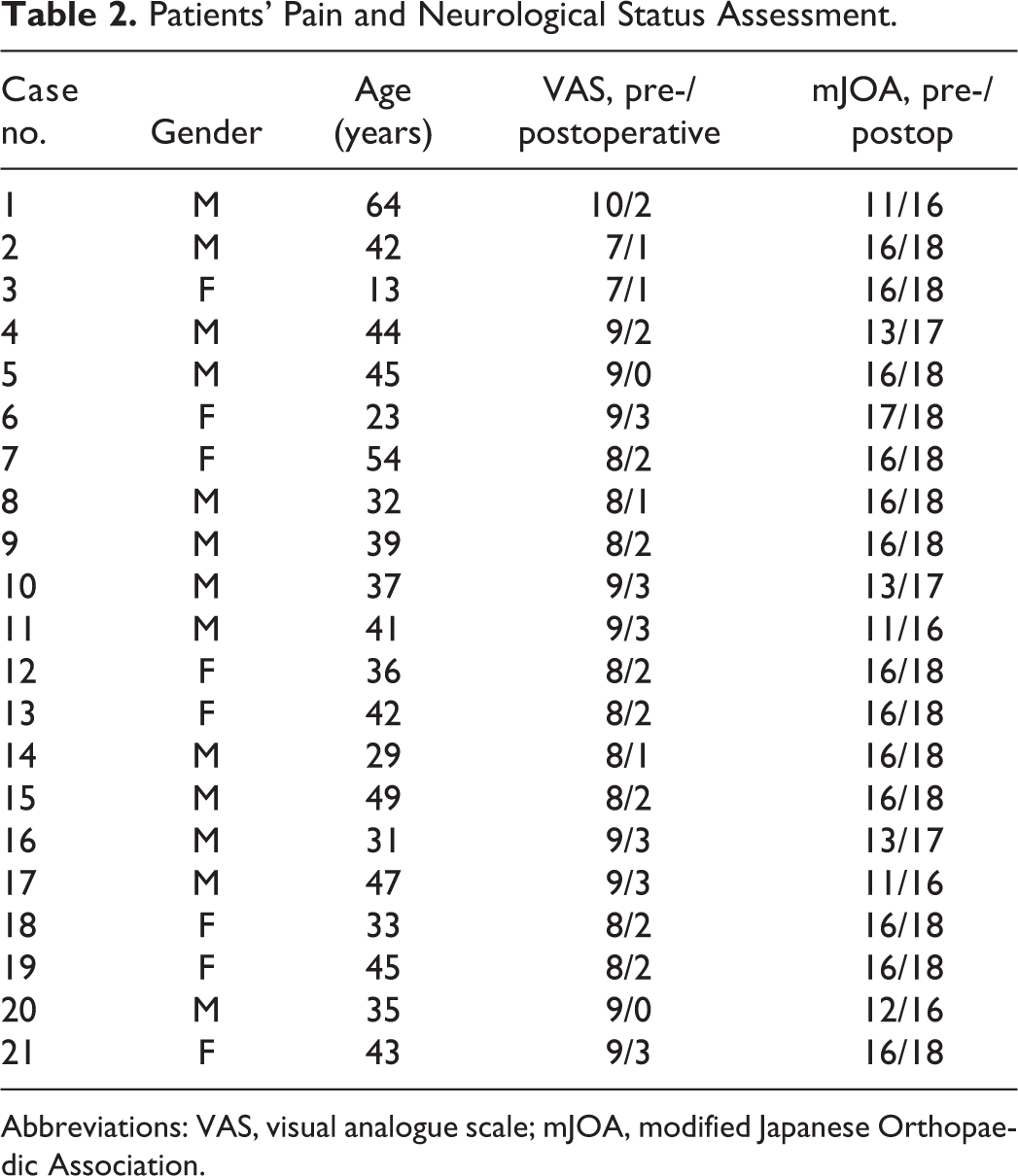
Abbreviations: VAS, visual analogue scale; mJOA, modified Japanese Orthopaedic Association.
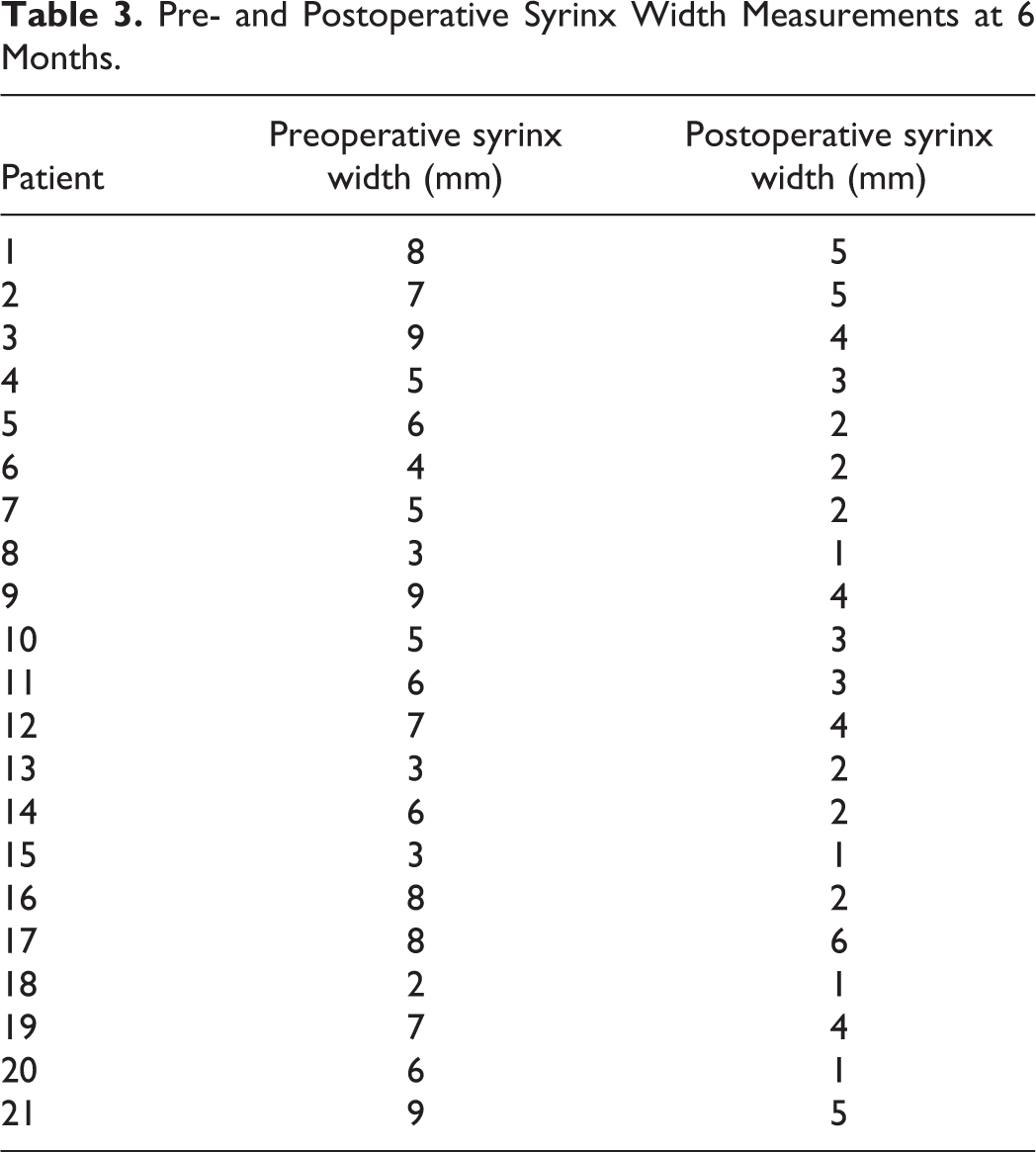
A significant reduction was observed radiologically in the syrinx cavity measurements (Table 3) on the patients’ postoperative MRIs (Figures 2, 3, and 4).
Pre- and Postoperative Syrinx Width Measurements at 6 Months.
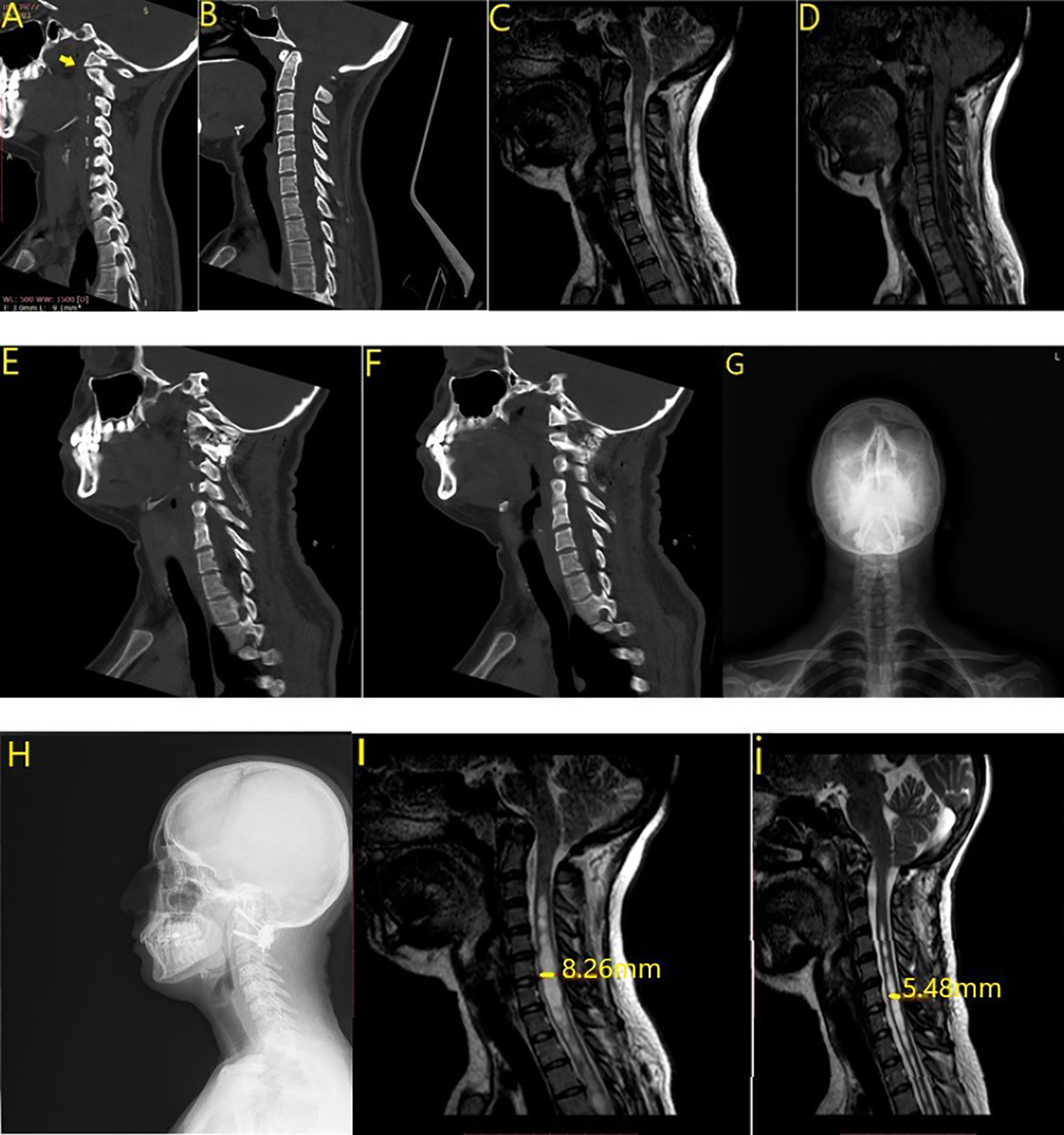
Case 1. (a) Type 1 atlantoaxial dislocation. (b) Preoperative computed tomography (CT). (c, d) Preoperative magnetic resonance imaging (MRI). (e, f) Postoperative CT. Cage and screws. (g, h) Postoperative radiograph. (l, i) Early (after 1 day) and 6-month postoperative MRI.
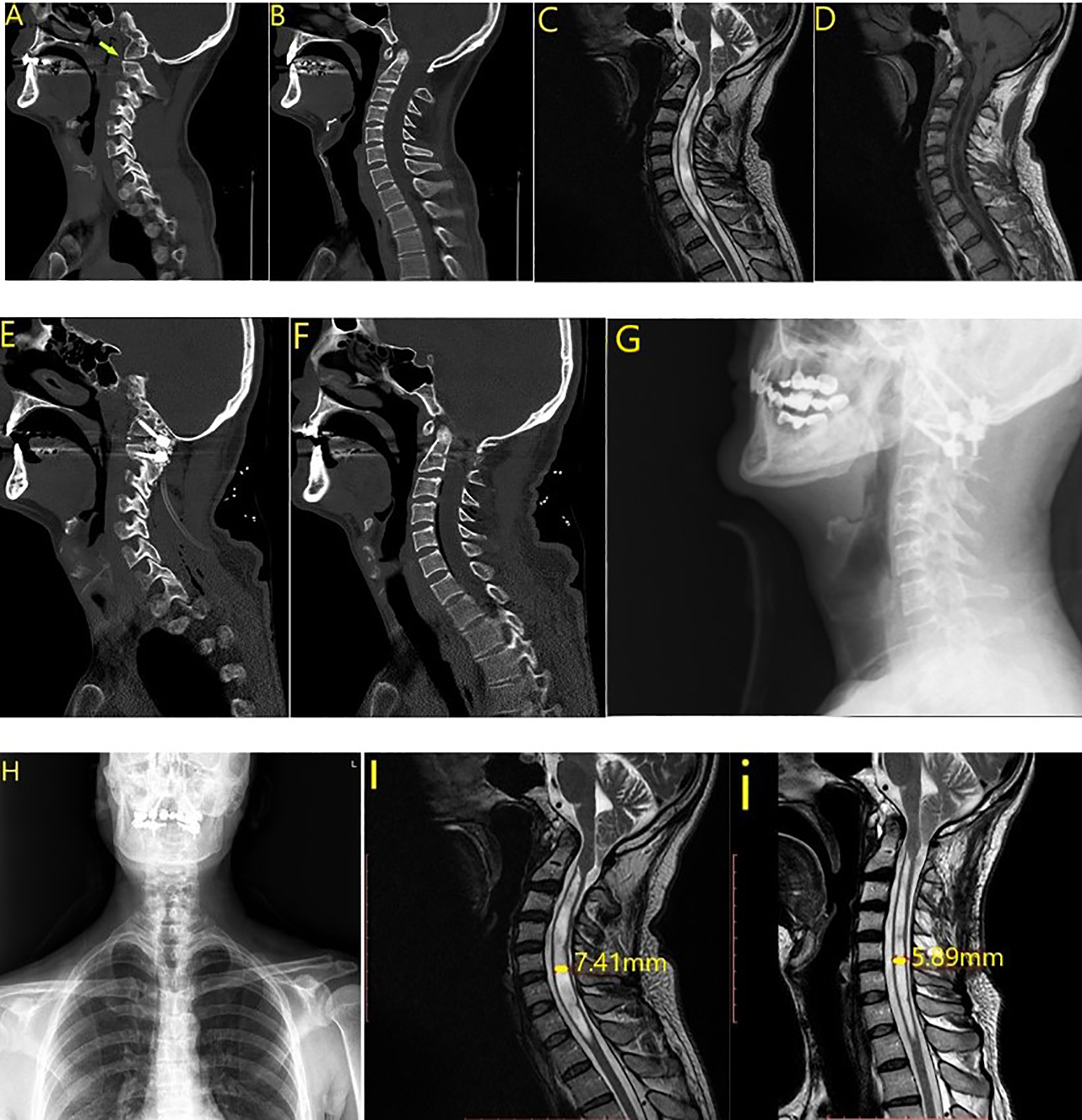
Case 2. (a) Type 2 atlantoaxial dislocation. (b) Preoperative computed tomography (CT). (c, d) Preoperative magnetic resonance imaging (MRI). (e, f) Postoperative CT. Cage and screws. (g, h) Postoperative radiograph. (l, i) Early (after 1 day) and 6-month postoperative MRI.
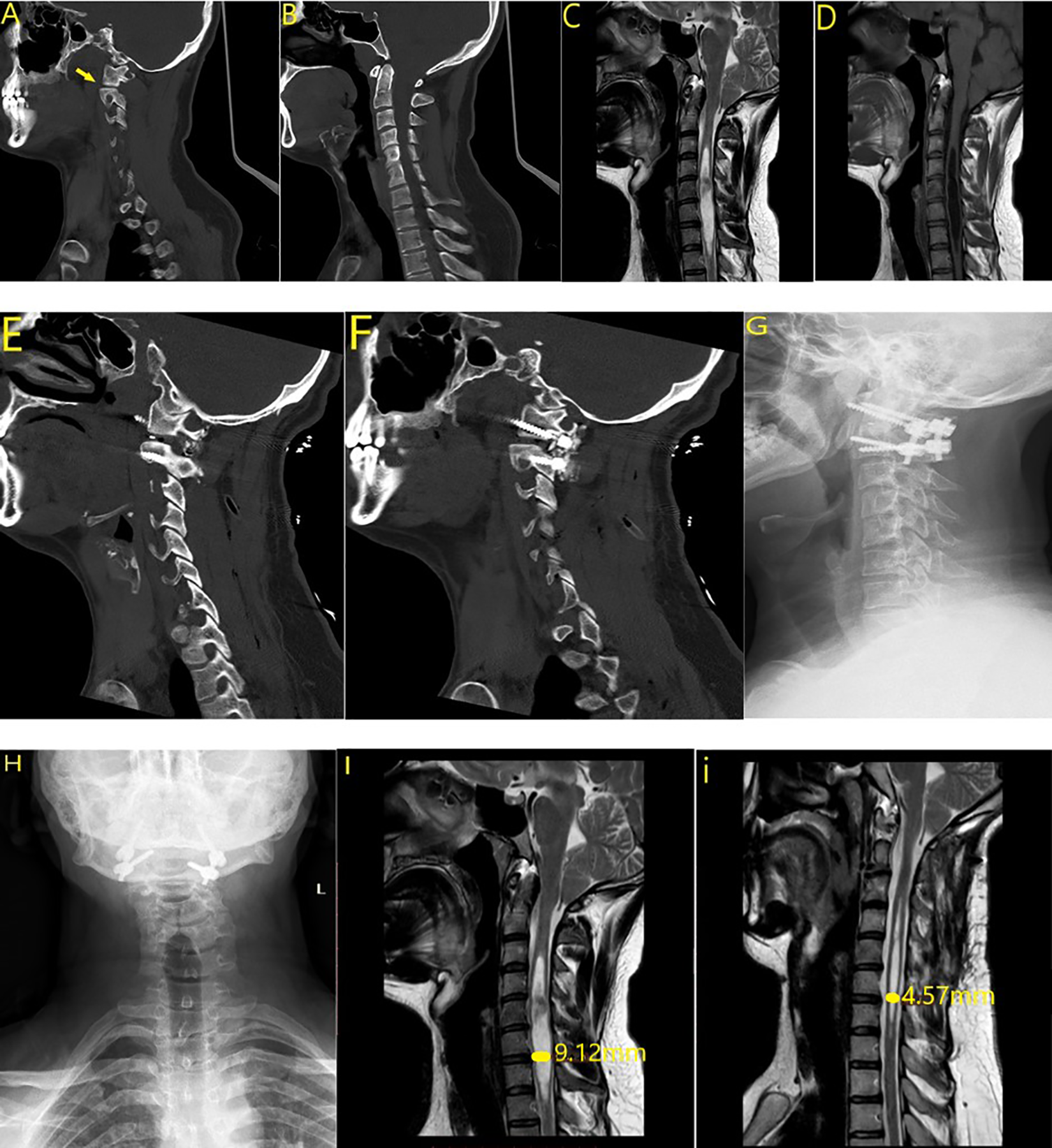
Case 3. (a) Type 3 atlantoaxial dislocation. (b) Preoperative computed tomography (CT). (c, d) Preoperative magnetic resonance imaging (MRI). (e, f) Postoperative CT. Cage and screws. (g, h) Postoperative radiograph. (l, i) Early (after 1 day) and 6-month postoperative MRI.
No patients developed infection or neurologic complications. No additional surgical intervention was required during the postoperative follow-up period in any patient after deterioration. CT and MRI revealed that successful distraction was achieved using the C1-2 PEEK cage in all patients, and partial or almost complete improvement was observed in BI.
Discussion
The primary treatment for CM is to restore CSF flow at the craniovertebral junction and to eliminate compression on the nervous system structures, and current treatment protocols are designed to achieve this goal. The most commonly used surgical technique is PFD with or without duraplasty. Studies in the literature have reported the success rate of this technique to be approximately 70% to 80%. 27 However, 20% to 30% of patients do not benefit from this surgical method. We believe that this is likely because the etiopathogenesis of CM is still not fully understood. Because we believe that the etiopathogenesis of CM is due to the atlantoaxial instability, as mentioned by Goel, we observed a significant improvement in all cases in whom we performed the surgery. We had no failed cases.
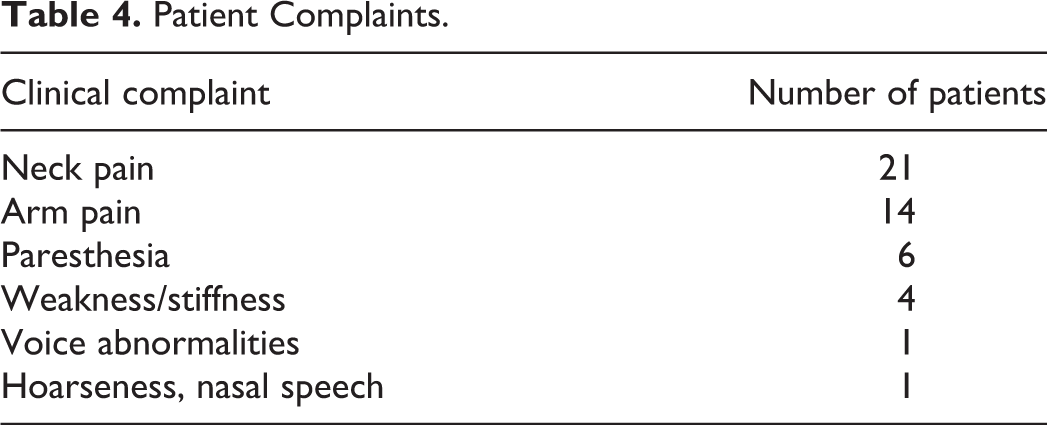
The most common symptoms associated with CM are suboccipital headache and neck pain (80%). These symptoms are exacerbated by the Valsalva maneuver. Other common symptoms include ocular disorders, otoneurologic symptoms (dizziness, hearing loss), gait ataxia, and general fatigue. Rare signs are isolated limb pain or weakness. Myelopathy is classically manifested by dissociative sensory loss (ie, loss of pain and temperature sensation, preserved fine touch, and proprioception) and motor weakness.15,16,28 Sleep apnea may occur in CM patients due to weakness of the pharyngeal muscles resulting from compression of the brain stem, upper spinal cord, or lower cranial nerve. The most common complaint in our patients was neck pain radiating to the head followed by pain and paresthesia radiating to the arms. The patients’ clinical symptoms are detailed in Table 4. Significant improvement was observed in the clinical complaints of all patients in whom we performed the surgery.
Patient Complaints.
Syringomyelia accompanies 30% to 70% of CM type 1 cases radiologically. This association is mentioned in many articles. There are many theories for the pathogenesis of syringomyelia (eg, Gardner hydrodynamic theory, Ball and Dayan’s pulsatile CSF theory, Williams’s craniospinal pressure dissociation theory, Oldfield’s tonsillar piston theory, Welch’s CSF leakage theory, Aboulker’s theory of blockage at the cisterna magna level). 29 As seen here, the possible etiopathological factors of syringomyelia are controversial. We believe that syringomyelia is the clinical manifestation of atlantoaxial instability in CM; therefore, we link the improvement of syringomyelia after surgery to this in all cases.
BI is associated radiologically with CM type 1 in 25% to 30% of cases. 11 Although many surgical techniques have been described in the literature for the treatment of BI, the most frequently recommended surgical technique is craniovertebral junction fixation with our without anterior decompression.10,17-19 Although neurologic improvement may be observed after anterior decompression alone, serious potential morbidities such as neurologic deterioration or respiratory problems may occur.17,21 In addition, recurring dislocation toward the cranial and recurrent compression are potential dangers in patients who undergo only anterior decompression without strong internal fixation. 22 Since we assumed that the association between CM and BI is due to the same etiological origin (atlantoaxial instability), we associated the improvement in 9 cases (42%) with CM and BI with this in our series.
According to the theory of atlantoaxial joint instability described by Goel in 2009, there are 3 types of atlantoaxial instability
30
: Type 1: anterior atlantoaxial instability Type 2: posterior atlantoaxial instability Type 3: central atlantoaxial instability (no radiologically demonstrable evidence of instability—it is diagnosed during surgery)
At the same time, with regard to the classification reported by Goel in 2019, 27 the atlantodental space may not change abnormally in atlantoaxial facetal instability in types 2 and 3, and there may be no neural or dural compression with the odontoid process. For these reasons, Goel referred to type 2 and 3 atlantoaxial facetal instability as “central” or “axial” atlantoaxial instability.
Goel purported that CM, BI, and syringomyelia are not congenital malformations. Rather, he stated that all of these are clinical reflections of atlantoaxial joint instability and that they manifest as syringomyelia, BI, and CM depending on the type and severity of joint instability. He emphasized that syringomyelia actually plays the role of a protective airbag for neural structures. In addition, Goel highlighted that surgical treatment in patients with CM, syringomyelia, and BI results in the elimination of this instability.
After foramen magnum decompression, the neural structures that are under compression due to narrowed or obstructed CSF are relieved, resulting in clinical and radiologic improvement of the patient. However, this situation is temporary, as patients eventually return to their former clinical and radiologic conditions, and their condition may even worsen as a result of the underlying atlantoaxial instability. According to Goel, this resembles the deflation of an airbag, and in the long term, the balloon becomes inflated again, causing a recurrence of the previous clinical condition. 31
In his series of 65 CM patients, Goel 26 reported a significant improvement in JOA and VAS scores. The clinical mJOA scores of the patients in whom we performed surgery increased from 13.28 preoperatively to 15.14 after surgery, on average. The VAS score decreased from 8.42 preoperatively to 1.9 after surgery. In conclusion, patients’ pain decreased significantly, and their clinical function increased.
The limitations of this study include the small number of patients and the short duration of the follow-up period.
Conclusion
Our article is the first study in the literature after Goel’s publication showing central or axial C1-2 dislocation in CM pathogenesis, and the dramatic clinical and radiologic improvement of CM patients after surgery supports the hypothesis that there is an underlying atlantoaxial instability, as Goel mentioned. Although PFD and/or duraplasty is a common treatment modality in CM, the radiologic and clinical results of the C1-2 fixation method described by Goel were found to be favorable in CM treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB: 691, Date: January 15, 2020) of Adana City Education and Research Hospital approved this study.