
Abstract
Study Design
Case series.
Objective
Posterior percutaneous endoscopic cervical diskectomy (PECD) can preserve the disk in patients with a foraminal disk herniation. However, progressive angulation at the operated segment is a concern, especially for patients with cervical lordosis < 10 degrees. The change in cervical lordosis after posterior PECD was analyzed.
Methods
Medical records were reviewed of 32 consecutive patients (22 men, 10 women; mean age, 49 ± 12 years) who had single-level foraminal soft disk herniation. The operation levels were as follows: C4–5 in 1 patient, C5–6 in 12, C6–7 in 18, and C7–T1 in 1. All patients were discharged the day after the operation, and neck motion was encouraged. All patients were followed for 30 ± 7 months (range, 24 to 46 months), and 21/32 patients (66%) had radiographs taken at 25 ± 11 months (range, 12 to 45 months). Radiologic parameters were assessed, including cervical curvature (C2–7), segmental Cobb's angle (SA), and anterior and posterior disk height (AH and PH, respectively) at the operative level.
Results
At the last follow-up, 29/32 patients (91%) had no or minimal pain, and 3/32 patients had occasional pain. SA, AH, and PH were not significantly changed. Cervical lordosis < 10 degrees was present in 10/21 patients preoperatively and in 3/21 patients at the last follow-up. For patients with cervical lordosis < 10 degrees, cervical curvature changed from −2.5 ± 8.0 to −11.3 ± 9.3 degrees (p = 0.01). For patients with cervical lordosis ≥ 10 degrees, cervical curvature changed from −17.5 ± 5.8 to −19.9 ± 5.7 degrees (p = 0.24).
Conclusions
Cervical curvature does not worsen after posterior PECD.
Introduction
Anterior cervical diskectomy and fusion (ACDF) is currently the standard treatment for cervical disk disease. However, there are problems associated with fusion, such as limitation of motion and the potential for adjacent segment pathology. 1 , 2 Although artificial disk replacement (ADR) was introduced to address these issues, artificial disks may not alter the natural history of degeneration. Various problems associated with artificial cervical disks, such as heterotopic ossification, mechanical failure, and spontaneous fusion, have been reported. 3 , 4 , 5 , 6 There are several surgical techniques for disk preservation that utilize the natural cervical disk itself to address the problems associated with instrumentation in fusion or disk replacement for patients with foraminal disk herniations, such as anterior or posterior foraminotomy and diskectomy. 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 However, one concern with posterior foraminotomy is progressive angulation at the operative segment, especially for patients with cervical lordosis < 10 degrees. 15 Posterior foraminotomy and diskectomy can be performed using endoscopic techniques, and the soft tissue trauma from bone removal can be minimized with magnification and fine endoscopic instruments. 9 The application of posterior percutaneous endoscopic cervical diskectomy (PECD) for patients with decreased cervical lordosis may be controversial, because surgery may worsen cervical lordosis by injuring facet joint/muscles, but cervical lordosis may be improved by reduced pain and muscle spasm. 16 , 17 In the present study, we evaluated change in cervical sagittal curvature after posterior PECD.
Materials and Methods
Patients
This study was approved by the institutional review board at the Seoul National University Hospital (H-1210-078-434). The medical records were reviewed of 32 consecutive patients (22 men, 10 women; mean age, 49 ± 12 years; range, 26 to 73 years) who underwent single-level PECD between March 2009 and November 2011. During this period, 104 cervical spine surgeries were performed for single-level cervical degenerative disk disease. We considered posterior PECD for patients whose main symptom was arm pain due to foraminal soft disk herniation without spinal cord compression and facet degeneration. Disk degeneration was evaluated with T2-weighted sagittal magnetic resonance (MR) imaging as described by Pfirrmann et al, 18 and grades I, II, and III (inhomogeneous structure of the disk with intermediate gray signal intensity and preserved disk height) were acceptable for posterior PECD, if indicated. Conventional ACDF, ADR, or microforaminotomy was performed for patients with central disk herniation, cervical myelopathy, or foraminal bony stenosis due to spur or facet joint hypertrophy (Table 1). Preoperatively, MR imaging, computed tomography (CT), and anteroposterior and lateral plain radiographs were taken. Patients were asked to stand up and look straight ahead during radiography. All patients filled out a questionnaire to determine the neck disability index (NDI; 50 possible points) 19 and visual analog pain (VAS) score for the neck (10 possible points) and arm (10 possible points). All operations were performed with completely endoscopic techniques by two surgeons at two different institutions. The operative levels were C4–5 in 1 patient, C5–6 in 12 patients, C6–7 in 18 patients, and C7–T1 in 1 patient. All patients were discharged the day after the operation without a neck collar, and free neck motion was encouraged. The patients were scheduled to visit the outpatient clinic at 1, 3, 6, and 12 months postoperatively, as well as yearly thereafter. At each visit, the patients were asked to fill out the same questionnaire, and plain radiographs of the cervical spine (standing anteroposterior and lateral) were taken at 6 months, 12 months, and yearly thereafter with the same protocol. We followed all patients through either outpatient clinic visits or telephone interviews. Clinically, all patients were followed for 30 ± 7 months (range, 24 to 46 months). Not all of the patients had radiographs at every visit, and 21 of the 32 patients (66%) had follow-up radiographs at a mean 25 ± 11 months (range, 12 to 45 months).
Summary of surgeries for single-level cervical degenerative disk disease from March 2009 to November 2011
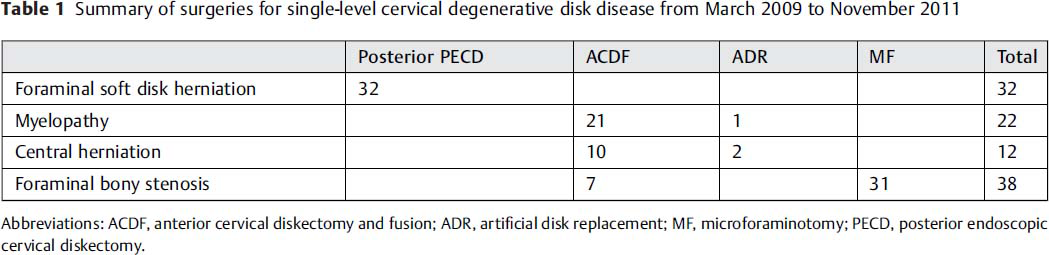
Abbreviations: ACDF, anterior cervical diskectomy and fusion; ADR, artificial disk replacement; MF, microforaminotomy; PECD, posterior endoscopic cervical diskectomy.
Surgical Methods
The surgical methods were similar to those previously reported. 9 , 20 , 21 All operations were performed under general anesthesia in a prone position with three-point pin fixation devices with a table-mounted holder (Mayfield system, Intergra, Plainsboro, New Jersey, United States) or craniocervical traction with a Gardner-Wells tongs skeletal fixation system (Fig. 1). The neck was flexed to widen the interlaminar window and to reduce overlapping of the facet joints. Normal saline was hung ∼1.5 m above the patient and connected to endoscopic equipment for continuous irrigation (Fig. 1). After a skin incision of 8 mm was made above the medial junction of the inferior and superior facet joint (V-point, Fig. 2), which was identified with an intraoperative orthogonal fluoroscopic image, the obturator (6.9 mm outer diameter) was introduced. The tip of the obturator was placed at the V-point under fluoroscopic guidance, and the boundaries of the inferior lamina, superior lamina, and medial margin of the facet joint were palpated with the obturator. The oblique-type working channel (7.9 mm outer diameter) was introduced on the obturator, and the endoscope (Vertebris, Richard Wolf GmbH, Knittlingen, Germany) was introduced. The entire operation was performed under visual control and continuous irrigation with normal saline. 9 , 20 The opened bevel of the working channel was directed toward the medial side to avoid accidentally compressing the spinal cord. After clearing out the soft tissue around the V-point, the drilling of the bone was performed from the medial margin of the interlaminar space; the inferior lamina was drilled first (Fig. 2). The size of the bony drilling depended on the size and location of the herniated disk material, usually within a 3- to 4-mm radius around the V-point (Fig. 2). The ligamentum flavum was removed, and the lateral margins of the dura and exiting nerve root were visualized. During the operation, vessels were coagulated to control bleeding, and soft tissues around nerve root and disk were coagulated for preparation of the annulus. Ruptured fragments were identified from axillar or shoulder or nerve root and removed after making an incision on the annulus. Decompression was confirmed by both visualization and palpation from points either inferior or superior to the nerve root. After the operation, a closed suction drain was inserted through the working channel if epidural bleeding was a concern (18/32 patients, 56%), and it was removed the next day.
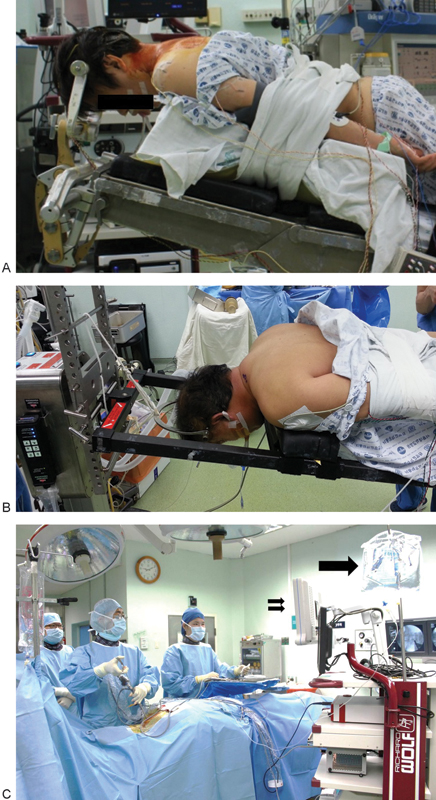
Operation room setup. Skeletal fixation is performed with either Mayfield head-holder (Intergra, Plainsboro, New Jersey, United States) (A) or Gardner-Wells tongs (B). Reverse Trendelenburg position is taken to reduce venous pressure (C). Irrigation saline (arrow) is hung ∼1.5 m above the patient to prevent high water pressure (C). The entire procedure was performed under direct visualization on the monitor (double arrows).
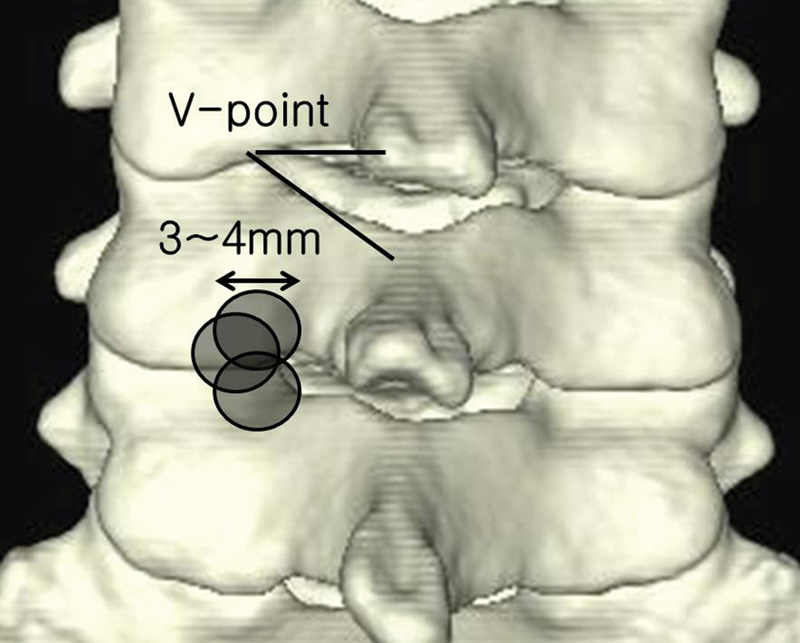
V-point and extent of bony removal. The V-point included the inferior margin of the cephalic lamina, the medial junction of the inferior and superior facet joints, and the superior margin of the caudal lamina. Bone drilling was started from the V-point. The shaded areas show the extent of bony removal. The diameter of the endoscopic instruments is usually 3 to 4 mm, and the size of bony removal was assessed with reference to the diameter of the instrument.
Radiologic Measurements
Radiologic parameters, including cervical curvature (C2–7, tangential method), segmental Cobb's angle at the operative level (SA), and actual anterior/posterior height from the superior end plate of the cephalic vertebra to the inferior end plate of the caudal vertebra (AH and PH, respectively) were compared (Fig. 3). 22 Negative angles indicate lordosis. Actual AH and PH length were calculated using CT scans, using the formula actual length = measured length on plain radiograph × (measured length of superior end plate of cephalic vertebra on CT scan / measured length of superior end plate of cephalic vertebra on plain radiograph).
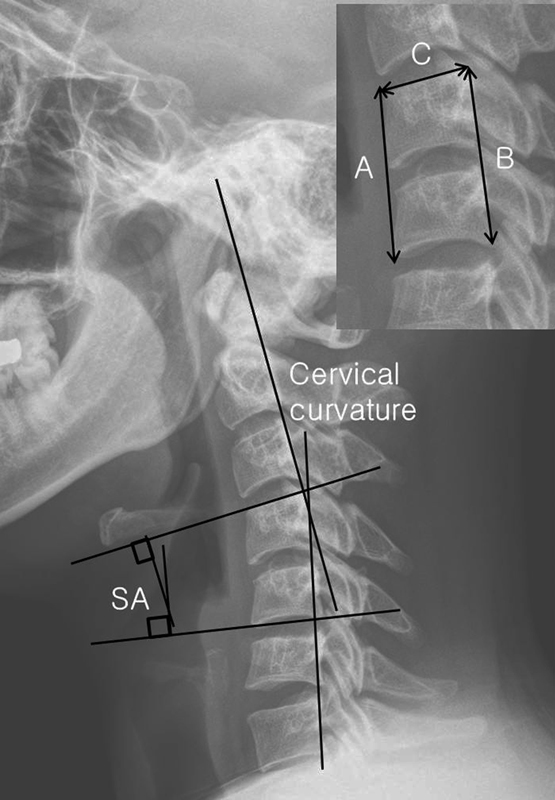
Radiologic measurements. Cervical curvature is measured using the tangential method from C2 to C7. The segmental angle (SA) is measured from the superior end plate to the inferior end plate of the cephalic and caudal vertebra using Cobb's method. To calculate the anterior (AH) and posterior height (PH) between the cephalic and caudal vertebra, the length between the anterior/superior corner and anterior/inferior corner of the cephalic and caudal vertebrae was measured (A) from plain radiographs. Similarly, the length from the posterior/superior to the posterior/inferior corner of the vertebrae was measured (B) from plain radiographs. The length of the superior end plate of the cephalic vertebra was measured from plain radiographs (C) and computed tomography scans (actual C). The actual lengths of A (AH) and B (PH) were measured using the following formula: AH = A × (actual C/C); PH = B × (actual C/C).
Statistical Analysis
Preoperative clinical parameters (NDI, neck VAS, and arm VAS) and radiologic parameters (cervical curvature, SA, AH, and PH) were compared with those obtained at the last follow-up visit. Mann-Whitney U test was used for analysis. All statistical analyses were performed using SPSS (version 17.0, SPSS, Chicago, Illinois, United States), and statistical significance was defined as p < 0.05 (two-sided).
Results
Ruptured fragments were identified in 26/32 (81%) patients, and these were removed through the axilla of the root in 25/26 patients. In 6/32 patients, the bulged annulus compressed the nerve root and was decompressed with a radiofrequency coagulator. After the operation, decompression was confirmed using MR imaging in all patients. Conversion to open surgery was not necessary in any patient. Postoperatively, two patients complained of transient thumb hypesthesia for a week. Although not definitive, we suspected thermal injury as the cause of transient hypesthesia in one patient. Dural injury occurred in one patient during drilling, but the size was ∼2 mm and the arachnoid membrane was intact. After diskectomy, the wound was closed without repairing the dura mater. Hypesthesia disappeared 1 week later without permanent sequela.
At the last follow-up, 29/32 patients (91%) had no or minimal arm pain (excellent or good outcome according to the Macnab criteria), and 3/32 patients had occasional pain (fair outcome). Preoperatively, the NDI, neck VAS, and arm VAS were 22.1 ± 7.4, 6.7 ± 2.9, and 7.6 ± 2.4, respectively, and the postoperative NDI, neck VAS, and arm VAS significantly decreased to 2.9 ± 3.8, 1.7 ± 1.9, and 1.5 ± 2.0, respectively (p < 0.05, Table 2). Cervical lordosis significantly changed from −10.7 ± 9.4 to −15.7 ± 8.7 degrees (p < 0.01, Fig. 4). Cervical lordosis was <10 degrees in 10/21 patients preoperatively and in 3/21 patients at the last follow-up. For patients with cervical lordosis < 10 degrees, cervical curvature changed from −2.5 ± 8.0 to −11.3 ± 9.3 degrees (p = 0.01). For patients with cervical lordosis ≥ 10 degrees, cervical curvature changed from −17.5 ± 5.8 to −19.9 ± 5.7 degrees (p = 0.24). Cervical kyphosis was present in 2 patients (16 and 7.2 degrees) and changed to 1 and −8.7 degrees at 12 months. The preoperative AH, PH, and SA were 31.8 ± 3.9 mm, 32.2 ± 3.5 mm, and −1.7 ± 4.4 degrees, and the postoperative AH, PH, and SA were 31.6 ± 3.9 mm, 32.0 ± 3.5 mm, and −2.6 ± 2.6, respectively. Postoperative values were not significantly different from preoperative ones (p = 0.24, 0.43, and 0.07, respectively). During the follow-up, there were no recurrences or reoperations at either index or adjacent levels.
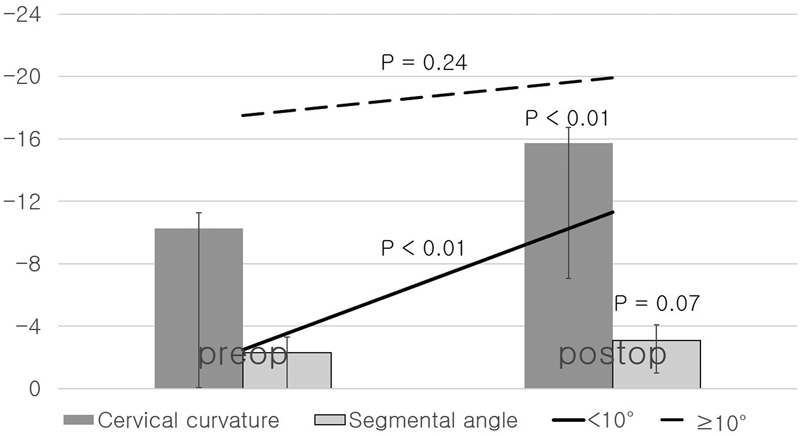
Radiologic outcome. The mean values are represented with bar graphs, and standard deviations are indicated with line graphs. The results of the statistical analysis are shown above the lines. Negative values denote lordosis. The results of patients with cervical lordosis < 10 degrees and patients with cervical lordosis ≥ 10 degrees are presented with line graphs. The cervical curvature and segmental angle are expressed in degrees, and the anterior and posterior heights are expressed in millimeters. Cervical lordosis was significantly changed from −10.7 ± 9.4 to −15.7 ± 8.7 degrees (p < 0.01). For patients with cervical lordosis < 10 degrees, cervical curvature was changed from −2.5 ± 8.0 to −11.3 ± 9.3 degrees (p = 0.01). For patients with cervical lordosis ≥ 10 degrees, cervical curvature was changed from −17.5 ± 5.8 to −19.9 ± 5.7 degrees (p = 0.24).
Neck disability index (NDI) a
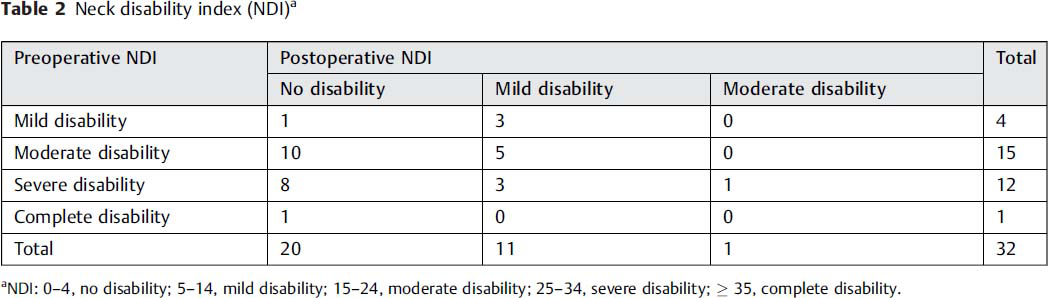
NDI: 0–4, no disability; 5–14, mild disability; 15–24, moderate disability; 25–34, severe disability; ≥ 35, complete disability.
Case Report
A 27-year-old man presented with 6-month duration of right arm pain, which was intractable to medication and several epidural injections. His NDI, neck VAS, and arm VAS were 17/50, 3/10, and 7/10, respectively. His symptoms were accompanied by mild right bicep weakness (manual motor power test grade IV/V). The MR image showed a foraminal disk herniation at C5–6 on the right side (Fig. 5A). Plain cervical lateral radiographs showed cervical kyphosis of 7.2 degrees and an SA of 10.8 degrees (Fig. 5B). AH and PH were 31.0 and 33.1 mm, respectively. Posterior PECD was performed, and the ruptured disk material was removed with minimal facetectomy (Fig. 5C and D). Decompression was confirmed with a postoperative MR image (Fig. 5E). He was followed for 26 months, at which point the NDI, neck VAS, and arm VAS were 0/50, 0/10, and 0/10, respectively. Plain radiographs obtained 12 months postoperatively showed improved cervical lordosis (−8.7 degrees, Fig. 5F). SA, AH, and PH were 0.9 degrees, 30.9 mm, and 33.0 mm, respectively.
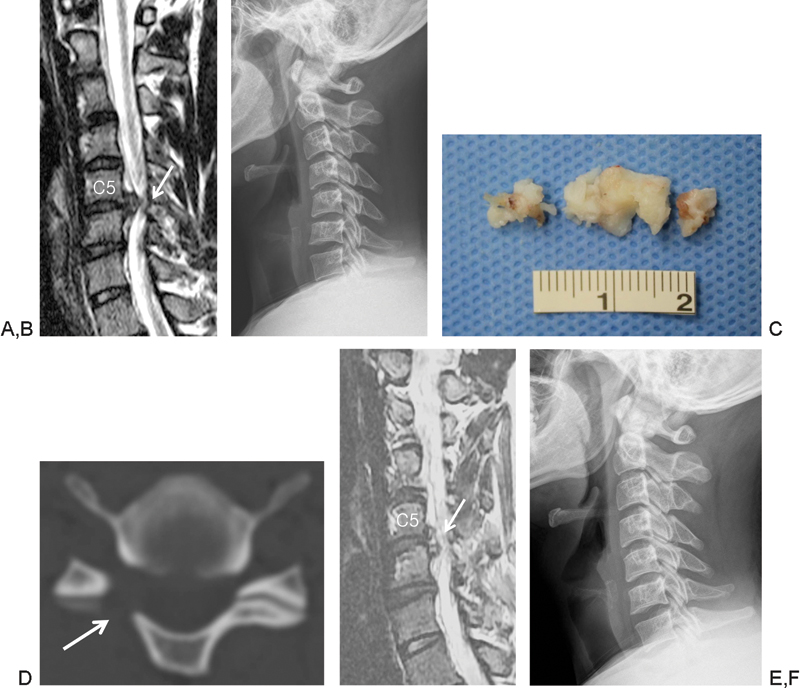
Preoperative T2-weighted sagittal magnetic resonance (MR) image showed a herniated disk at C5–6 (A, arrow) in the case reported. Plain cervical lateral radiographs showed cervical kyphosis of 7.2 degrees and SA of 10.8 degrees (B). A large disk fragment was removed during the operation (C). Postoperative computed tomography scan showing that the medical facet was minimally removed (D, arrow). Successful removal of the ruptured disk fragment was confirmed with postoperative T2-weighted sagittal MR images (E, arrow). Plain radiographs obtained 12 months postoperatively showed improved cervical lordosis of −8.7 degrees (F).
Discussion
Because segmental motion is preserved with posterior PECD, progressive angulation at the operated segment is a concern, especially for patients with cervical lordosis < 10 degrees. In the present study, we analyzed cervical sagittal curvature after posterior PECD. Cervical lordosis was not worsened for patients with lordosis ≥ 10 degrees and improved for patients with lordosis < 10 degrees. The height of the disk and the segmental angle at the operative segment were preserved. Clinically, 91% of patients exhibited favorable outcomes for more than 2 years, and the results were similar to previous findings. 9 , 20
Posterior foraminotomy and diskectomy is an alternative option for select patients with arm pain, and clinical improvement and reoperation rates are comparable to those of standard ACDF. 11 , 12 , 14 , 15 , 23 , 24 Moreover, the preservation of a mobile segment is a great advantage over fusion surgery with respect to cost and the progression of adjacent segment pathology. In fact, it has been suggested that 30% of fusion surgeries could be replaced by foraminotomy. 1 , 14
Cervical kyphosis can be divided into reducible and irreducible types. 17 Reducible kyphosis is mostly related to local disk prolapse, pain, or muscular weakness, but irreducible kyphosis is always associated with significant cervical degeneration or congenital bone malformation. 17 In cases of soft disk herniation at the neural foramen, cervical arthroplasty is one surgical option, and cervical kyphosis has been reported to be reversed with improvement in symptoms if no significant cervical spine degeneration was present. 17 However, the artificial disk is not a true substitute for the native disk, and issues of heterotopic ossification, spontaneous fusion, and adjacent segment pathology have not been completely resolved. 5 , 6 , 17 Therefore, a disk-preserving surgery may be preferable for select patients. However, the progression of kyphosis and decreased disk heights after anterior foraminotomy or anterior PECD have been reported in the literature. 7 , 10 , 25 After anterior PECD, 12% of patients showed a progression of kyphosis of approximately 5 degrees during a 2-year follow-up. Moreover, these patients exhibited significantly decreased disk height. 25
Although the progression of angulation at the operative segment can be a problem after open posterior foraminotomy, 15 changes in the cervical curvature after posterior PECD may be different due to less damage to the muscle and facet joint than open microforaminotomy (Fig. 2). Moreover, posterior PECD is primarily used in patients with soft disk herniation without significant cervical degeneration, 9 , 13 , 20 , 26 and we may expect spontaneous recovery of cervical lordosis by removing the ruptured disk material. Ruetten et al published their surgical outcomes after posterior PECD, and neither increased kyphosis nor decreased disk height was detected in any of the patients. 20 In the present study, indication of posterior PECD was the same as previous recommendations. Bony removal was minimized, and the patients were encouraged to move and extend their neck starting on the first postoperative day. The cervical curvature, disk height, and segmental angle were not worsened. Interestingly, cervical kyphosis was reversed to lordosis in one patient (Fig. 5). Normal cervical lordosis was reported to be 20 to 30 degrees, but cervical lordosis was not significantly correlated with neck pain. 27 , 28 , 29 Moreover, 17% of patients without neck pain showed a kyphotic segmental angle of >4 degrees. 27 Although we showed improved cervical lordosis for some patients, it may be a coincidental finding for selected patients. Mild kyphosis or decreased cervical lordosis may be a normal finding in many individuals. Nonetheless, it appears that posterior PECD does not worsen cervical sagittal alignment.
Limitations
In the present study, we showed that cervical sagittal alignment was not worsened after posterior PECD in selected patients. This result was based on an analysis of a small group, which increases the chance of type I statistical error. Moreover, although the patients were asked to look straight ahead during the radiograph, their neck position was not standardized. In addition, without a control group (such as an open foraminotomy group), the superiority of posterior PECD cannot be assessed. Long-term analysis of a large group is required. Second, the indications for posterior PECD are limited and cannot be applied for all types of cervical degenerative disk disease. For example, this procedure is not optimal for the removal of a centrally located pathology, hard disk, or bony spur. 8 , 9 We performed posterior PECD for 31% (32/104) of patients with single-level cervical degenerative disk disease, but the proportion should not be generalized. Some patients with soft disk herniation at the neural foramen searched for spine endoscopic surgeons; therefore, the proportion of indicated patients would be different from that in the other hospitals and countries. Third, in the present study, we referred to CT scan to differentiate hard disk from soft disk herniation. However, it may be better differentiated with MR image, and CT scans need to be restricted for selected patients. Finally, posterior PECD is not a familiar surgical technique, and surgeons have to be accustomed to various endoscopic techniques and instruments. 21 , 30 , 31 , 32 Despite these shortcomings, posterior PECD may be a good alternative for select patients, considering that it preserves the natural disk using a minimally invasive technique.
Conclusions
The gold standard technique for the treatment of cervical disk herniation is ACDF. A disk-preserving surgery with an endoscopic technique for patients with foraminal soft disk herniation may be an alternative surgical option, and it appears that cervical sagittal curvature does not worsen after posterior PECD.
Disclosures
Chi Heon Kim, Consultant: Richard Wolf GmbH
Kyung-Hyun Shin, user of the endoscopic equipment of Richard Wolf GmbH
Chun Kee Chung, user of the endoscopic equipment of Richard Wolf GmbH
Sung Bae Park, user of the endoscopic equipment of Richard Wolf GmbH
Jung Hee Kim, none
Footnotes
Acknowledgments
This work was supported by the Global Frontier R&D Program on Human-centered Interaction for Coexistence funded by the National Research Foundation of Korea grant funded by the Korean Government (MEST) (NRF-2012M3A6A3055889).