
Abstract
Study Design
A systematic review and meta-analysis.
Objective
This study aimed to determine whether rheumatoid arthritis (RA) is associated with clinical outcomes following spinal surgery for lumbar spinal disorders.
Methods
MEDLINE, Embase, the Cochrane Library, and the International Clinical Trials Registry Platform were comprehensively searched for observational studies comparing clinical outcomes after lumbar spine surgery in patients with and without RA (>18 years). Quality assessment was conducted using the Quality in Prognosis Studies assessment tool. Pooled odds ratios (ORs) and hazard ratios were calculated for reoperation and surgical site infection by using a random effects model. Subgroup analyses were conducted to examine the effect of surgery type.
Results
Seven studies with 72,969 patients, including 7518 patients with RA, were analyzed. All studies had a moderate risk of bias. Patients with RA had a significantly higher odds of reoperation (OR: 5.57; 95% confidence interval [CI]: 1.10-28.26; I2 = 92%; P = 0.04) and higher odds of surgical site infection (OR: 1.47; 95% CI: 1.28-1.69; I2 = 2%; P < 0.01). No statistically significant difference was found in reoperation-free survival between patients with RA and those without RA (hazard ratio: 1.15; 95% CI: 0.94-1.40; I2 = 100%; P = 0.16). Patients with RA had higher complication rates, with incidence rates ranging from 13.5% to 57%, compared with those without RA.
Conclusion
Compared with patients without RA, patients with RA may be more likely to undergo reoperations and suffer from complications following surgery for lumbar spine lesions.
Introduction
Lumbar spinal disorders in patients with rheumatoid arthritis (RA) are complex and challenging, with the disease often affecting the facet joints and discovertebral junctions.1-3 Severe lumbar lesions have serious detrimental effects on the quality of life of patients with RA. 4 Patients with RA often develop osteoporotic vertebral fractures. 5 A correlation between disease activity and spinal malalignment was reported. 6 In a recent longitudinal analysis, we demonstrated that the disease activity of RA contributes to the deterioration of spinal sagittal alignment. 7
Surgical intervention is a key treatment modality for patients with RA with lumbar lesions refractory to conservative treatment. For these lesions, lumbar fusion or decompression surgery is mainly performed. 8 However, evidence regarding the association between RA and postoperative outcomes in patients with lumbar spinal disorders is lacking. Several studies suggest that RA has a negative effect on postoperative outcomes, whereas others argue that its effect is limited.9-11 In addition, systematic reviews on spinal surgery-related complications in patients with RA often integrate cervical and lumbar lesion outcomes.12,13 Given the distinct pathologies of cervical and lumbar spine lesions, a separate analysis should be conducted.
Therefore, we aimed to elucidate the association between RA and surgical outcomes by conducting a systematic review and meta-analysis focused on lumbar lesions. Our objective was to determine the incidence of reoperation, surgical site infection (SSI), and other complications after surgery in patients with RA compared with those without RA. This study aimed to contribute to the development of treatment strategies to mitigate the risks in patients with RA undergoing lumbar spine surgery.
Methods
Study Reporting and Protocol Registration
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplemental Appendix S1). 14 The requirement for informed consent from the study participants was waived because of the study design. The study protocol was registered on the Open Science Framework (https://osf.io/5t7jp/).
Study Eligibility
The review question posed was as follows: Does RA affect the clinical outcomes (reoperations and complications) of patients with lumbar spinal disorders who underwent lumbar spine surgery? We included all observational studies that reported clinical outcomes after lumbar spine surgery for lumbar spinal disorders in patients with RA (exposure) and those without RA (control) (≥18 years), including randomized controlled trials, prospective and retrospective cohort studies, case-control studies, and cross-sectional studies. Non-English language studies were included if appropriate translations could be obtained. Lumbar spinal disorders included degenerative conditions, such as spinal stenosis, disc herniation, spondylolisthesis, and spondylolysis, as well as inflammatory conditions associated with RA activity, such as synovitis and erosive changes at the facet joints and discovertebral junctions. The types of surgery included decompression surgery (laminectomy, discectomy, and laminoplasty) and lumbar fusion surgery (intervertebral fusion using any approach and posterior lateral fusion without a dynamic stabilization procedure). RA was defined based on the criteria used in each original study, including the American College of Rheumatology criteria, the European League Against Rheumatism criteria, and database codes such as the International Classification of Diseases. We excluded case series and studies that included patients who underwent prior lumbar spine surgery, long spinal fusion from the pelvis to thoracic spine, or spinal osteotomy, as well as patients diagnosed with ankylosing spondylitis.
Outcome of Interest
The primary outcomes assessed in this study were reoperation (survival outcomes) and SSI after lumbar surgery. For survival outcomes, odds ratios (OR) were calculated using the number of events observed in the RA and control groups. Hazard ratios (HR) were calculated if relevant data were available. Reoperation incidence was measured over the entire follow-up period. However, if data were available at several time points, the data closest to 2 years postoperatively were adopted. For SSI, we used the number of event data points. The definition of SSI was based on original studies, using database codes and clinical diagnoses. We reported outcome measures that were adjusted for potential confounding variables over the reported estimates that were not adjusted for potential confounding. The secondary outcome was the incidence of all adverse events related to the index surgery reported in the original study.
Data Screening and Extraction
We performed a comprehensive search of MEDLINE, Embase, the Cochrane Library, and the International Clinical Trials Registry Platform from inception until August 4, 2023. The database-specific search strategies are presented in Supplemental Appendix S2. Two independent reviewers (SH and MS) screened the titles and abstracts of the listed articles. Subsequently, they reviewed the complete texts of potentially included articles. Other relevant studies were identified by manually searching the reference lists of the included studies. Data were extracted by independent reviewers using a pre-piloted data extraction form. Any disagreements were resolved by consensus. We attempted to contact the authors of the included studies to clarify any relevant information or request additional data as necessary.
Quality Assessment
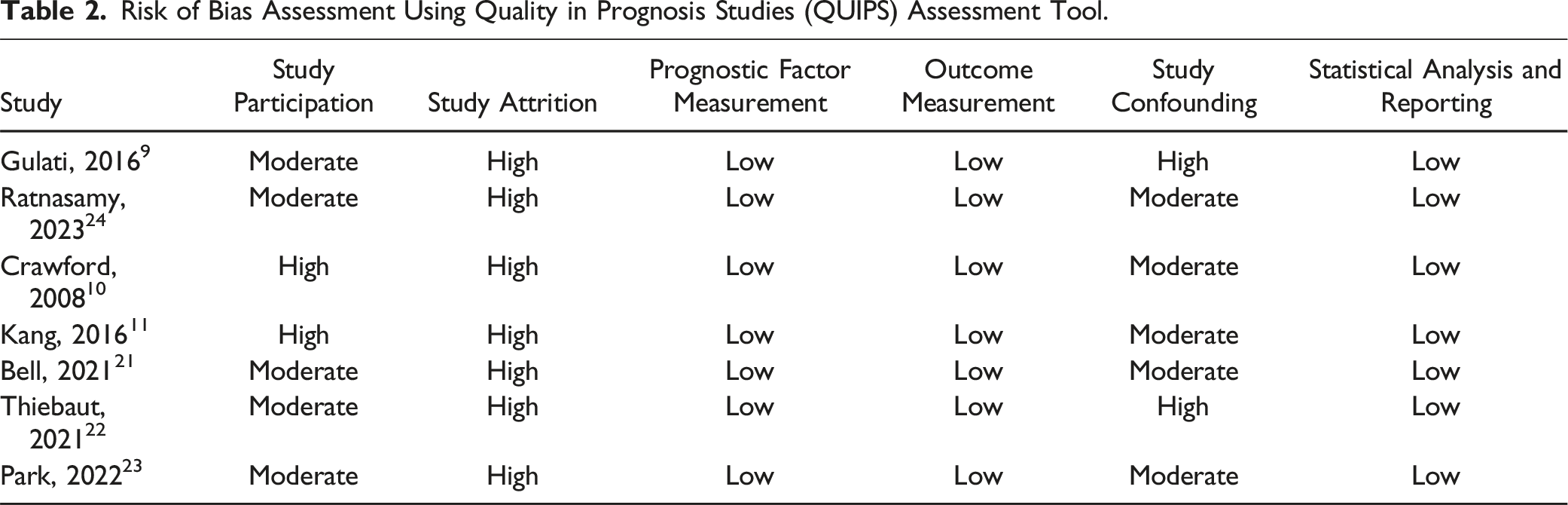
The quality of each included article was assessed by two reviewers using the Quality in Prognosis Studies (QUIPS) assessment tool (Supplemental Appendix S3). 15 To assess the confounding domain of the study, we predefined the following clinically relevant confounders: age, sex, body mass index, 16 smoking, 17 osteoporosis, 18 and comorbidity. 17 If all these confounders were adjusted for in the original study, we rated the study as having a low risk of bias in the confounding domain. The overall risk of bias was rated low if all QUIPS domains were rated low, moderate if one or two domains had an unclear or high risk of bias, and high if three or more domains had an unclear or high risk of bias. During the entire review process, disagreements between the two reviewers were resolved through discussions.
Data Synthesis
Statistical analyses were performed using R (version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria) and RevMan for Macintosh (version 5.4; The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). Heterogeneity among the studies was quantified using I2 statistics. We considered an I2 value of <25% to represent low heterogeneity and an I2 value of >75% to indicate high heterogeneity. 19 The Mantel–Haenszel method with a random-effects model was used to calculate the pooled ORs for reoperation and SSI. The inverse variance method with a random-effects model was used to calculate the pooled HRs for reoperation-free survival. If the author did not report the coefficients and variance of the Cox regression model, the HR and variance were estimated using the P-value of the log-rank test. 20 Forest plots were constructed to illustrate the outcomes of each study. To elucidate the influence of effect modifiers on the results, we conducted subgroup analyses of the primary outcomes according to the type of surgery: fusion surgery vs decompression surgery. If data were insufficient, data were qualitatively reviewed. Publication bias was not assessed using funnel plots and the Egger’s test because fewer than 10 studies were included for each outcome. Statistical significance was set at P < 0.05.
Results
Study Characteristics and Patient Demographics
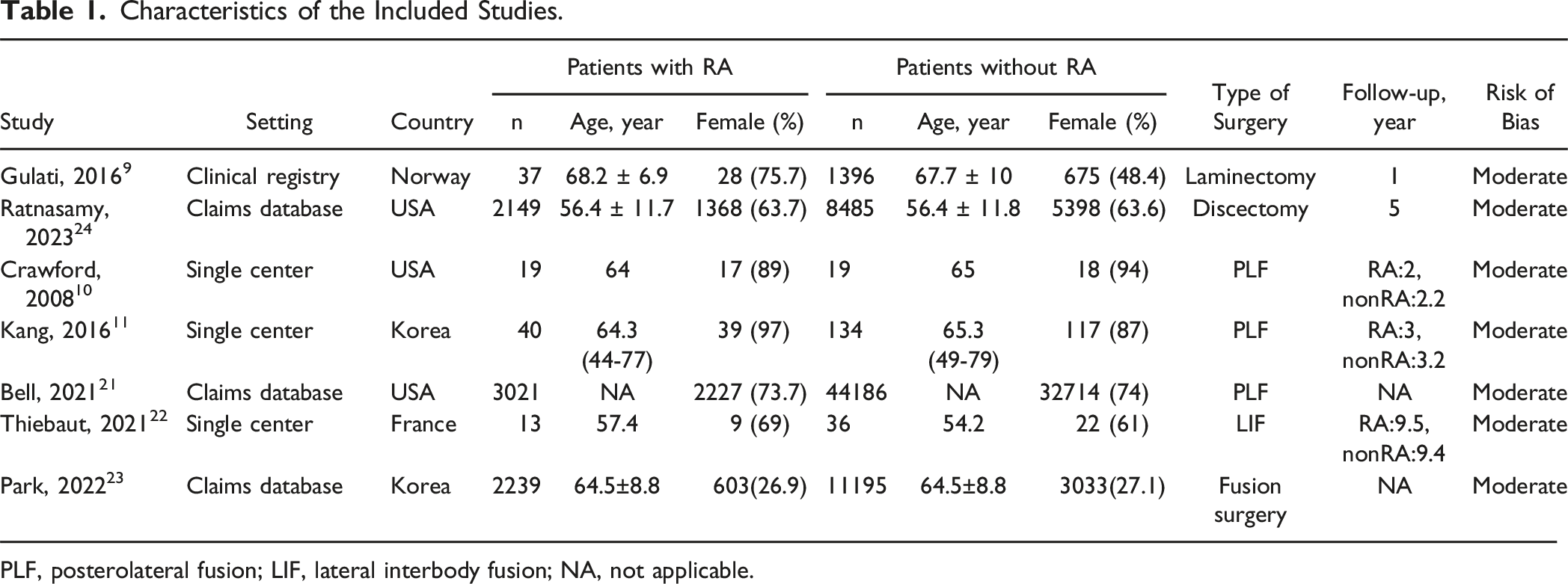
After eliminating duplicates, we screened 384 studies. Subsequently, we incorporated seven studies following the application of the exclusion criteria, as illustrated in Figure 1. Table 1 summarizes the characteristics of the included articles.9-11,21-24 All the included studies were retrospective cohort studies. The seven studies included 72,969 patients with lumbar spinal disorders who underwent lumbar spinal surgery, comprising 7518 (10%) patients with RA and 65,451 (90%) patients without RA. The mean or median age among the analyzed patients with RA ranged from 56.4 to 68.2 years, whereas that of patients without RA varied from 54.2 to 67.7 years. Among the seven studies, two included patients undergoing decompressive surgery, while the remaining five focused on patients after fusion surgery; three involved posterolateral fusion, one pertained to lumbar interbody fusion, and one included any type of fusion surgery. Table 2 shows that all studies had a moderate risk of bias, mainly due to insufficient study attrition and unadjusted confounders. Flow diagram. ICTRP: International Clinical Trials Registry Platform. Characteristics of the Included Studies. PLF, posterolateral fusion; LIF, lateral interbody fusion; NA, not applicable. Risk of Bias Assessment Using Quality in Prognosis Studies (QUIPS) Assessment Tool.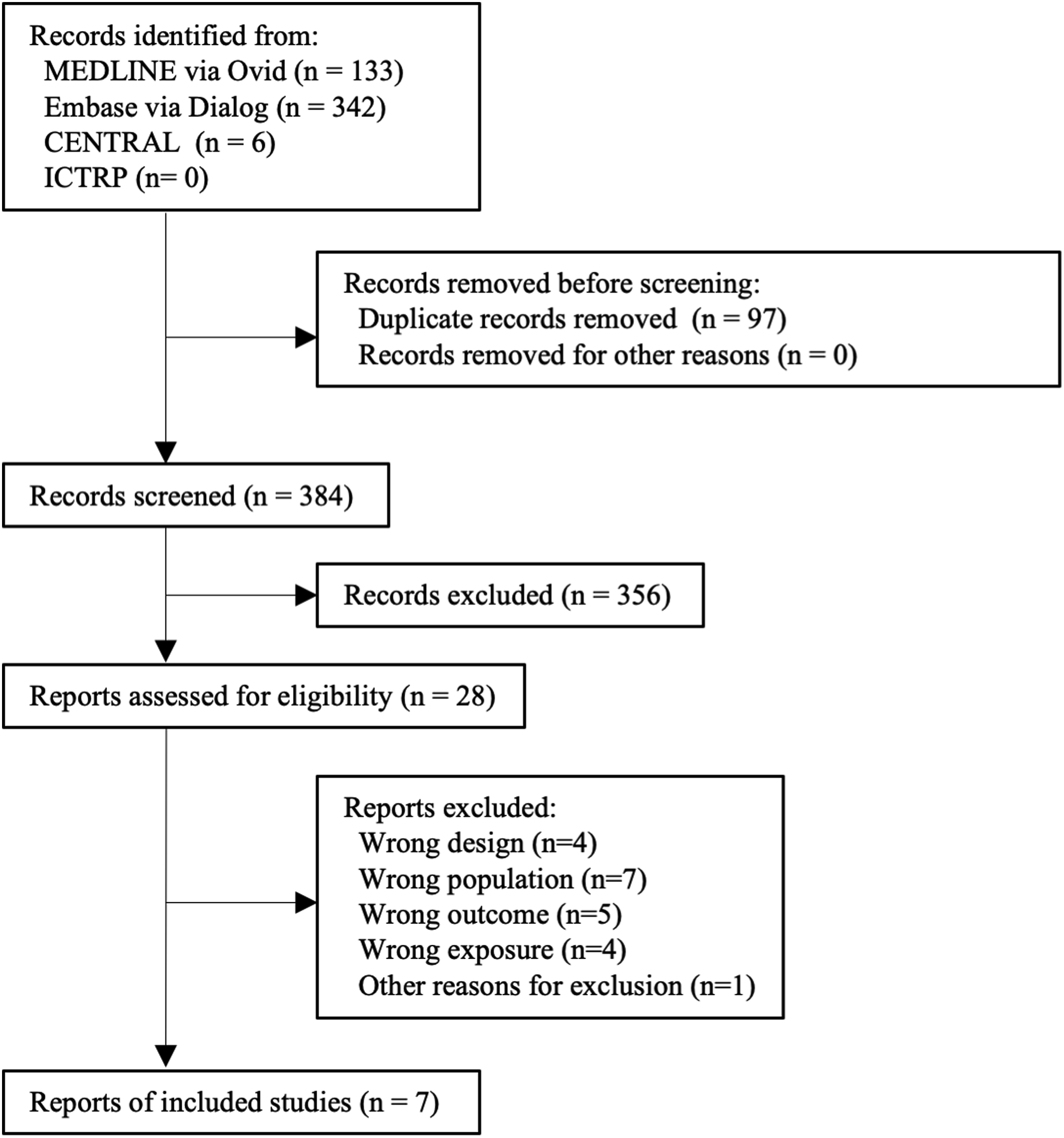
Reoperation
Five studies reported survival outcomes. Of these, three studies showed that the crude number of reoperations comprising 290 of 2292 patients with RA and 1000 of 11365 patients without RA at their mean follow-up ranged from 3 to 9.5 years.10,22,23 All the patients in these studies underwent lumbar fusion surgery. A statistically significant difference was observed in favor of patients without RA (OR: 5.57; 95% confidence interval [CI]: 1.10-28.26; I2 = 92%; P = 0.04, moderate risk of bias; Figure 2A). Among the five studies, two reported unadjusted survival data. One study only reported the result of the log-rank test at a follow-up of 5 years
24
; thus, the log HR was estimated from the P-value of the log-rank test. Another study reported the log-rank statistic at a 2-year follow-up,
21
so we calculated the log HR using these values, following the recommendations of the Cochrane Handbook.
25
No statistically significant difference was found in survival data (HR: 1.15; 95% CI: 0.94-1.40; I2 = 100%; P = 0.16, moderate risk of bias; Figure 2B). We did not perform sensitivity or subgroup analyses because of the small size of the included studies. Comparison between patients with rheumatoid arthritis (RA) and patients without RA (control). Outcome: reoperation. (A) The odds ratios (ORs) were determined using the Mantel–Haenszel method with a random effects model. (B) SE indicates standard error. The hazard ratios (HRs) were determined using a random effects model weighted by the inverse variance estimate. Square data markers represent ORs or HRs, with marker size reflecting the statistical weight of the study. Horizontal lines represent 95% confidence intervals (CIs). Diamond represents overall ORs or HRs, and 95% CIs for the outcome of interest.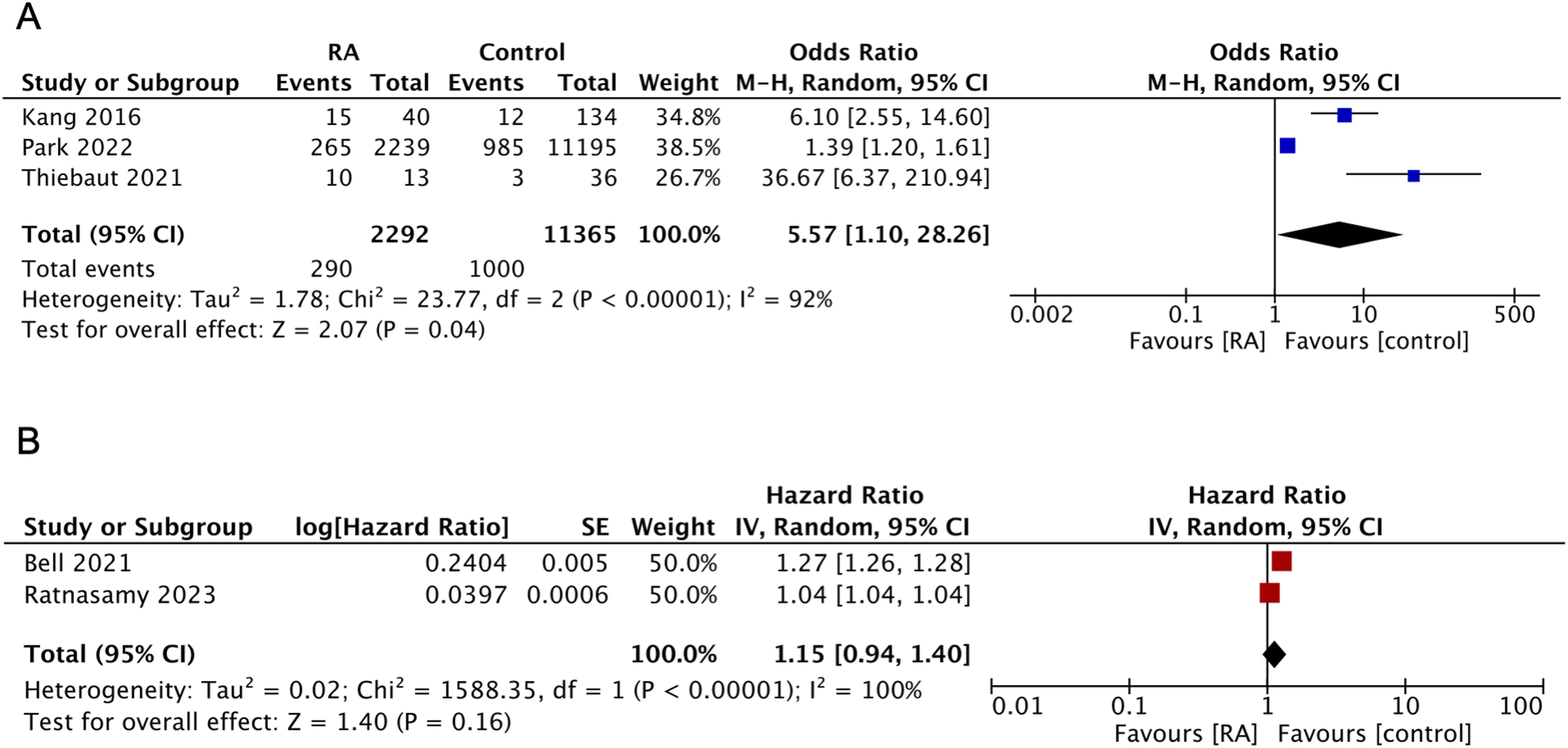
SSI
Six studies reported the incidence of SSI. Figure 3 shows a statistically significant difference in favor of patients without RA in total samples (OR: 1.47; 95% CI: 1.28-1.69; I2 = 2%; P < 0.01, moderate risk of bias). The pooled ORs for both surgical procedures showed a trend toward fewer SSIs in patients without RA. A subgroup analysis of the types of surgery was performed, and the test for subgroup differences revealed minimal heterogeneity between the types of surgery (P = 0.52). Comparison between patients with rheumatoid arthritis (RA) and patients without RA (control). Outcome: surgical site infection. The odds ratios (ORs) were determined using the Mantel–Haenszel (M-H) method with a random effects model. Square data markers represent ORs, with marker size reflecting the statistical weight of the study. Horizontal lines represent 95% confidence intervals (CIs). Diamond represents subgroup and overall ORs, and 95% CIs for the outcome of interest.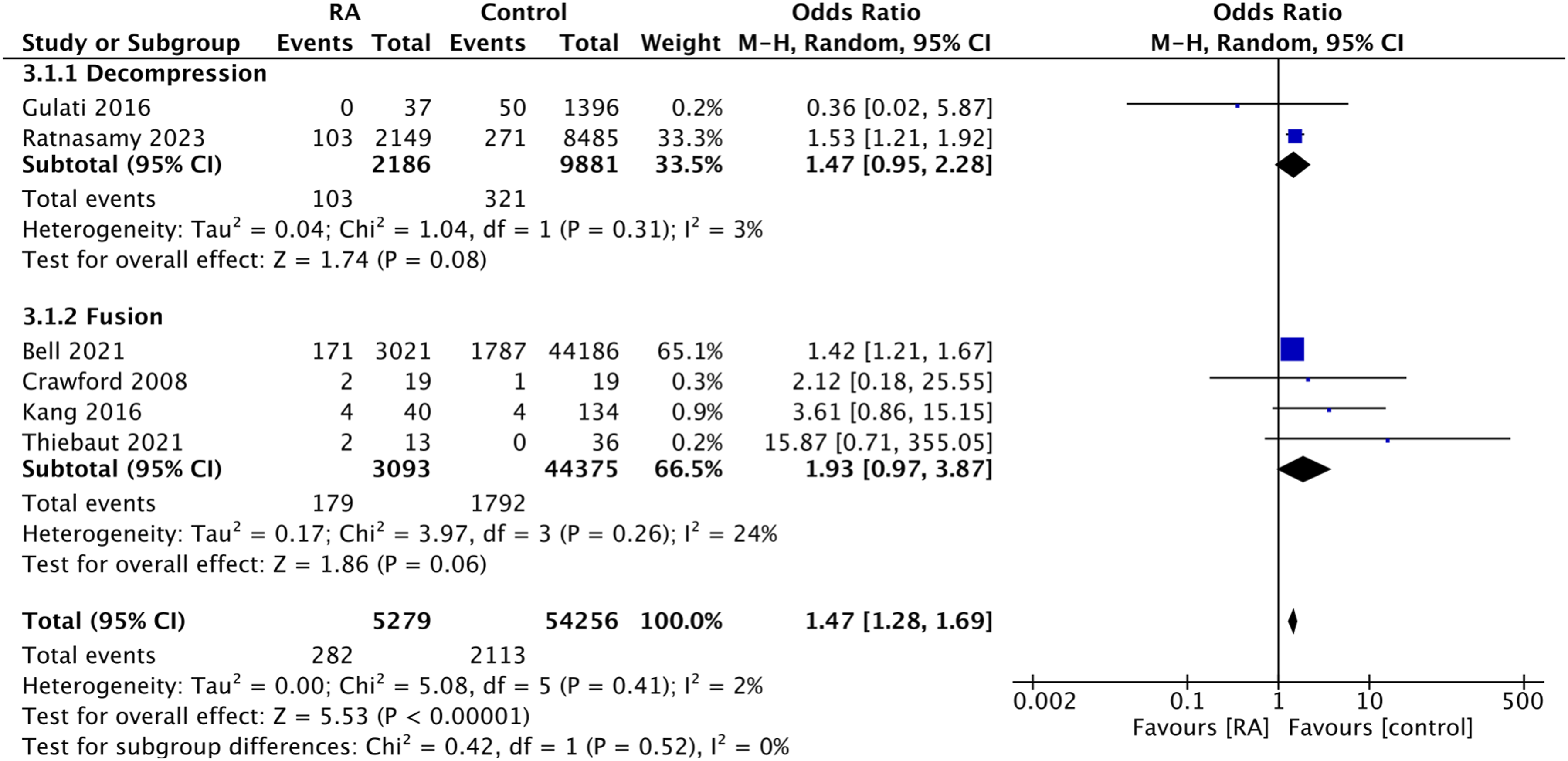
Other Complications
Details of Complications Following Surgery.
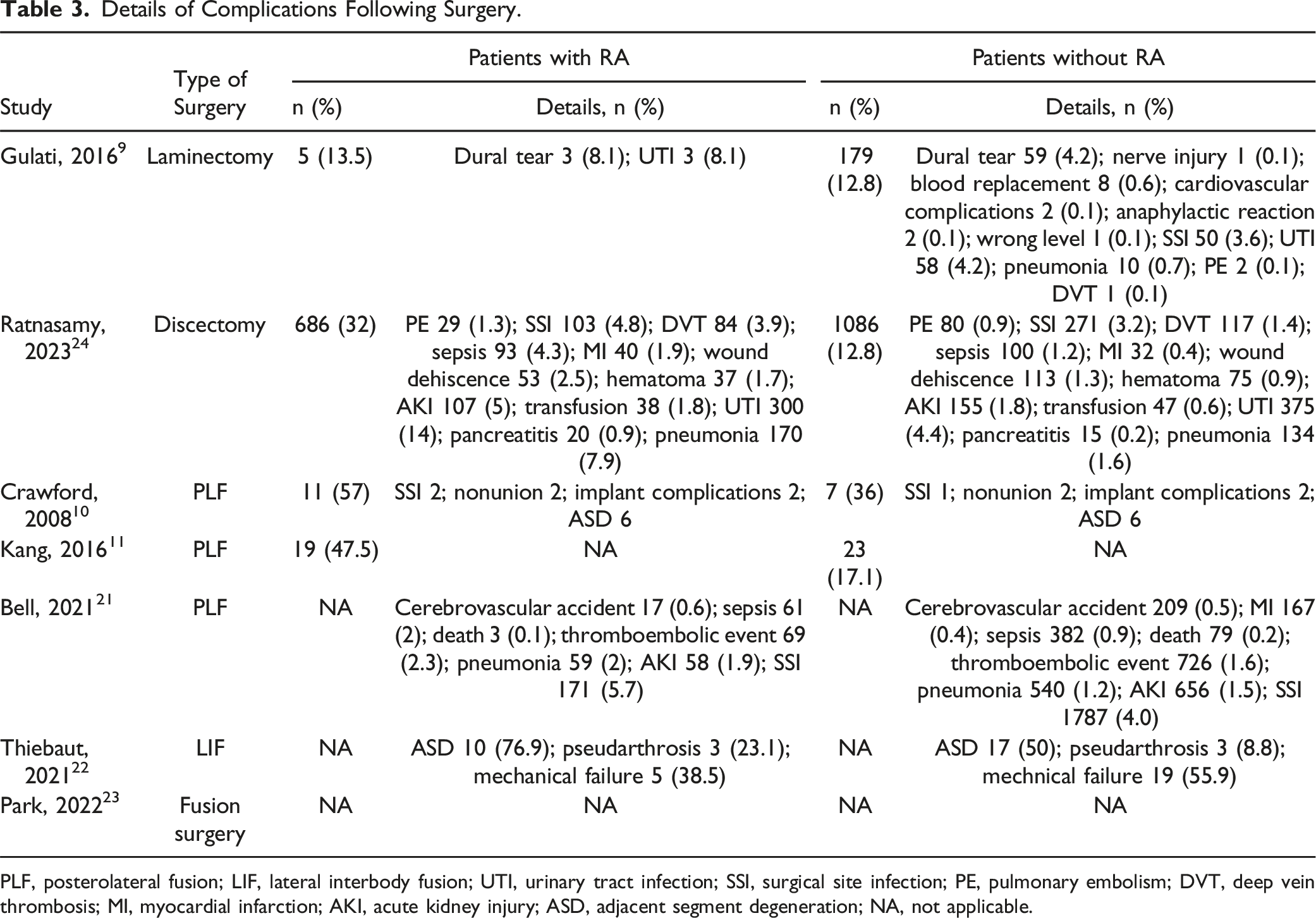
PLF, posterolateral fusion; LIF, lateral interbody fusion; UTI, urinary tract infection; SSI, surgical site infection; PE, pulmonary embolism; DVT, deep vein thrombosis; MI, myocardial infarction; AKI, acute kidney injury; ASD, adjacent segment degeneration; NA, not applicable.
Discussion
Lumbar spine lesions in patients with RA have been previously reported.1,2 However, evidence of the clinical outcomes following spine surgery is lacking. Our meta-analysis included a large sample of 72,969 patients, 10% of whom (7518 patients) were diagnosed with RA. These findings indicate that patients with RA had higher odds of undergoing reoperation and experienced more postoperative complications. Spine surgeons should properly understand the risks associated with lumbar spine surgery in patients with RA and perform comprehensive perioperative management to improve clinical outcomes.
Reoperation
The finding of a higher incidence of reoperation in patients with RA, indicated by a pooled OR of 5.57 (95% CI: 1.10-28.26), suggests that patients with RA were more likely to undergo reoperation than those without RA. The significant heterogeneity (I2 = 92%) in these results may reflect variations in surgical technique, perioperative care, and patient selection across the included studies. However, the consistently higher odds across these studies cannot be disregarded. Conversely, the HR for reoperation-free survival did not show a statistically significant difference (HR: 1.15, 95% CI: 0.94-1.40), which might suggest that the long-term risk of reoperation may not be as pronounced as initially indicated by the ORs. One of the two studies that provided survival data had a 5-year follow-up and found that patients with RA consistently exhibited higher reoperation rates in the first 2 years, with the survival curve crossing at approximately 2 years. Another study concluded that reoperation-free survival was significantly lower in patients with RA at the 2-year follow-up. These results indicate that reoperation within 2 years of lumbar spine surgery is likely common among patients with RA.
One study that examined outcomes after lumbar fusion surgery identified the reasons for reoperation. 11 Among patients with RA, six cases out of 40 reported implant failure. By contrast, implant failure occurred in three out of 134 patients without RA. Patients with RA are more susceptible to osteoporosis and sarcopenia,5,26 which may contribute to a higher incidence of reoperation.
SSI
The analysis also highlighted a lower incidence of SSI in patients without RA across all surgical types, demonstrating minimal heterogeneity (I2 = 2%) and indicating a consistent pattern across studies. Subgroup analysis of surgical techniques showed no statistically significant differences between decompression and fusion surgeries. The incidence of SSI was found to be high in patients with RA undergoing spinal surgery, including procedures on the cervical and thoracic spines. 13 Similar results were obtained when the data and analysis were restricted to the lumbar spine. These findings could reflect the systemic effects of RA, such as chronic inflammation and the use of immunomodulatory medications. 27 These factors could potentially increase susceptibility to infections regardless of the type of surgery performed.
Other Complications
Complications are more prevalent in patients with RA, which is aligned with the systemic nature of RA and its potential to complicate postoperative recovery. The variance in complication rates between patients with RA and those without RA (13.5%-57% vs 12.8%-36%, respectively) also indicates a multifactorial risk profile in patients with RA undergoing spine surgery.
For example, the incidence of dural tears in patients with RA undergoing laminectomy is noteworthy. A study analyzing a database of spinal surgeries for non-cervical lesions also reported that dural tears were more common in patients with RA. 28 Although these complications were relatively less frequent in patients without RA, the increased percentage in patients with RA could be attributed to dural adhesions resulting from chronic inflammation. Interestingly, when examining more detailed complications, such as adjacent segment degeneration, the data revealed that these are prevalent postoperative issues, particularly in patients with RA. Magnetic resonance imaging of lumbar lesions in patients with RA indicates that erosion of the lumbar endplates and facets is prevalent. 29 Chronic inflammation associated with RA may contribute to the increased incidence of adjacent segment degeneration. Although managing disease activity is a standard approach for treating RA, particular consideration may be required for patients who have undergone lumbar fusion surgery.
Table 3 also highlights the systemic nature of complications in patients with RA, with a broad spectrum of events ranging from cerebrovascular accidents to sepsis and myocardial infarction. This underscores the necessity for a multidisciplinary approach to perioperative care in patients with RA, encompassing not only surgical intervention but also the management of potential cardiovascular and thromboembolic complications.
Practical Considerations for Clinical Management
Based on our meta-analytic findings and previous reports, several practical considerations for managing patients with RA undergoing lumbar spine surgery are suggested. Preoperative medical optimization is essential: careful control of RA disease activity and comorbidities (e.g., chronic obstructive pulmonary disease, obesity, diabetes) can help reduce perioperative complications. 30 The decision to continue, modify, or temporarily discontinue biological disease-modifying antirheumatic drugs and/or glucocorticoids should be made in collaboration with rheumatologists, weighing the risk of RA flare against the risk of SSI. From a surgical standpoint, a meticulous technique to minimize tissue damage and operative time is crucial, especially given the predisposition of patients with RA to wound-healing problems. Extended postoperative antibiotic prophylaxis, although debated, may be considered in selected cases to mitigate infection risks. In prosthetic joint surgery, a 7-day extended course of antimicrobial therapy after surgery has been shown to reduce the incidence of periprosthetic joint infections in high-risk patients, including those with RA. 31 Nutritional optimization addressing hypoalbuminemia also appears beneficial for this group. Finally, close postoperative monitoring, including regular imaging and early intervention when implant loosening or infection is suspected, is paramount to reducing the likelihood of reoperation. These recommendations, although not yet backed by high-level evidence specific to patients with RA, may help guide more tailored, multidisciplinary care aimed at improving surgical outcomes.
Limitations
Although this meta-analysis offers important insights, it has several limitations. First, all the included studies were retrospective and with a moderate risk of bias. Most studies adjusted for confounders through patient matching, but they could not address all our pre-defined confounders. Future prospective cohort studies addressing these issues are necessary to confirm our findings. Second, the high heterogeneity observed in the data regarding reoperation and survival necessitates careful interpretation of the results. Nonetheless, the consistent direction of the effect sizes across studies suggests that RA may influence the primary outcome. Third, no studies have addressed disease activity in RA, and the effect of RA on postoperative outcomes has not been considered. A comparative study of patients with RA with and without well-controlled disease activity could clarify the underlying mechanisms.
Conclusion
This meta-analysis demonstrated an association between RA and increased postoperative complications, including reoperation and SSI, in patients undergoing lumbar spine surgery. These results underscore the importance of comprehensive perioperative management for improving clinical outcomes.
Supplemental Material
Supplement Material - Effect of Rheumatoid Arthritis on Postoperative Outcomes in Patients with Lumbar Spinal Disorders: A Systematic Review and Meta-Analysis
Supplemental Material for Effect of Rheumatoid Arthritis on Postoperative Outcomes in Patients with Lumbar Spinal Disorders: A Systematic Review and Meta-Analysis by Shintaro Honda, Koichi Murata, Masaki Sakamoto, Akihiro Shiroshita, Natsumi Saka, Bungo Otsuki, Takayoshi Shimizu, Takashi Sono, Soichiro Masuda, Koichiro Shima, and Shuichi Matsuda in Global Spine Journal
Footnotes
Author Contributions
Shintaro Honda, Akihiro Shiroshita and Natsumi Saka contributed to the study conception and design. Material preparation and data collection were performed by Shintaro Honda, Masaki Sakamoto and Akihiro Shiroshita. The first draft of the manuscript was written by Shintaro Honda Akihiro Shiroshita and Natsumi Saka, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Department of Advanced Medicine for Rheumatic Diseases is supported by Nagahama City, Shiga, Japan; Toyooka City, Hyogo, Japan; and two pharmaceutical companies (Asahi Kasei Pharma Corp., and AYUMI Pharmaceutical Co.). The stated companies had no role in the study design, data collection or analysis, manuscript writing, or the decision to submit the manuscript for publication. KM received speaking and/or consulting fees from AbbVie GK, Eisai Co., Ltd., Pfizer Inc., Chugai Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Pfizer Inc., Bristol-Myers Squibb, Daiichi Sankyo Co. Ltd., and Asahi Kasei Pharma Corp. SMatsuda received research grants and/or speaker fees from Astellas Pharma Inc., Daiichi Sankyo Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Eisai Co., Ltd., Takeda Pharmaceutical Company Limited, Chugai Pharmaceutical Co. Ltd, Pfizer Inc., and Asahi Kasei Corporation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.