
Abstract
Objective
This study aimed to systematically analyze the effectiveness and safety of the local application of vancomycin powder to prevent surgical site infection (SSI) after spinal surgeries and provide guidance for clinical practice.
Methods
Two researchers independently searched PubMed, Web of Science, Elsevier, and China National Knowledge Infrastructure using the MeSH terms “spinal surgery,” “vancomycin,” “local,” “topical,” “prophylactic,” “surgical site infection,” and “SSI” to identify studies published between January 2010 and January 2020 on the local application of vancomycin powder for preventing SSI after spinal surgeries. The outcome assessment indicators were analyzed using RevMan 5.3 software.
Results
Three randomized controlled trials, two prospective studies, and 26 retrospective studies were included in the current research. The results of the meta-analysis revealed significant differences between the vancomycin and control groups (non-vancomycin group) concerning the incidence of SSI (risk ratio = 0.39, 95% confidence interval = 0.28–0.55, Z = 5.46), indicating that local application of vancomycin powder can significantly reduce the incidence of SSI.
Conclusion
Local application of vancomycin powder is an effective and safe method to prevent SSI after spinal surgeries.
Keywords
Background
Surgical site infection (SSI) is one of the most common complications of spinal surgery, occurring at an incidence of 0.3% to 20.0%.1,2 In spinal surgeries, SSI could result in the development of pseudoarthrosis, spinal cord and neural injury, pyemia, and even patient death. Multiple surgeries and the usage of antibiotics lead to extended hospital stay and increased healthcare costs.3,4 More than 60% of SSIs are reported to be caused by Staphylococcus aureus and coagulase-negative Staphylococcus, both of which can be controlled by vancomycin. Since its first application in 2011, vancomycin has been used locally to prevent SSI in many surgical centers.5,6 However, the effects of the local application of vancomycin are not consistent. The current meta-analysis aimed to clarify whether local vancomycin application is an effective and safe method for preventing SSI after spinal surgeries.
Methods
Search of the literature
Two researchers independently searched PubMed, Web of Science, Elsevier, and Chinese National Knowledge Infrastructure using the keywords “spinal surgery,” “vancomycin,” “local,” “surgical site infection,” and “SSI” to identify randomized controlled trials (RCTs), half-randomized studies, prospective cohort studies, and retrospective studies of the local application of vancomycin powder for preventing SSI. Considering the relatively short period of local application of vancomycin in spinal surgeries, only studies published between January 2010 and January 2020 were included in the research. The incidence of SSI was used as the main outcome assessment parameter. Case reports, studies that only reported the outcome of prophylactic vancomycin use, and studies that only compared biochemical test results such as C-reaction protein or procalcitonin levels or the erythrocyte sedimentation rate were excluded from this study. Ethics approval was not required for this meta analysis.
Extraction of data
Two researchers independently extracted information such as the duration of study follow-up, patient age, methods of randomization, vancomycin dosage, method of drug application, and incidence of SSI.
Quality assessment
The quality of the included studies was assessed using the instructions provided by the Cochrane Handbook and Newcastle–Ottawa scale. 7 The criteria used in the current study include the method of randomization, blinding, and the integrity of data.
Statistical analysis
The outcome assessment indicators were analyzed using RevMan 5.3 software. A fixed-effects model was applied when I2 ≤ 50%, and a random-effects model was used when I2 > 50%. Subgroup analysis was performed when necessary.
Results
In total, 992 studies were screened by title, and 31 studies8–38 were included in the final meta-analysis. The 31 studies included a total of 17,708 patients. Among those patients, 7627 patients were treated with vancomycin after spinal surgeries to prevent SSI, and the remaining 10,081 patients were included as controls (Figure 1, Table 1).

Schematic chart of study inclusion.
Demographic characteristics of the included studies

SSI, surgical site infection; RCT, randomized controlled trial; N/A, not available
The 31 studies included three RCTs, two prospective cohort studies, and 25 reported retrospective case series. The studies were conducted from 2011 to 2019, and most of the studies were published between 2013 and 2015. Despite the retrospective nature of most of the included studies, the level of evidence was II to III for most studies, and the Newcastle–Ottawa scale was 5 to 7. A random-effects model was used for the overall analysis of the efficacy of vancomycin for preventing SSI because I2 = 54%. The overall risk ratio (RR) was 0.39 (95% confidence interval [CI] = 0.28–0.55), indicating a significantly lower incidence of SSI in the vancomycin group than in the control group (P < 0.001, Figure 2).
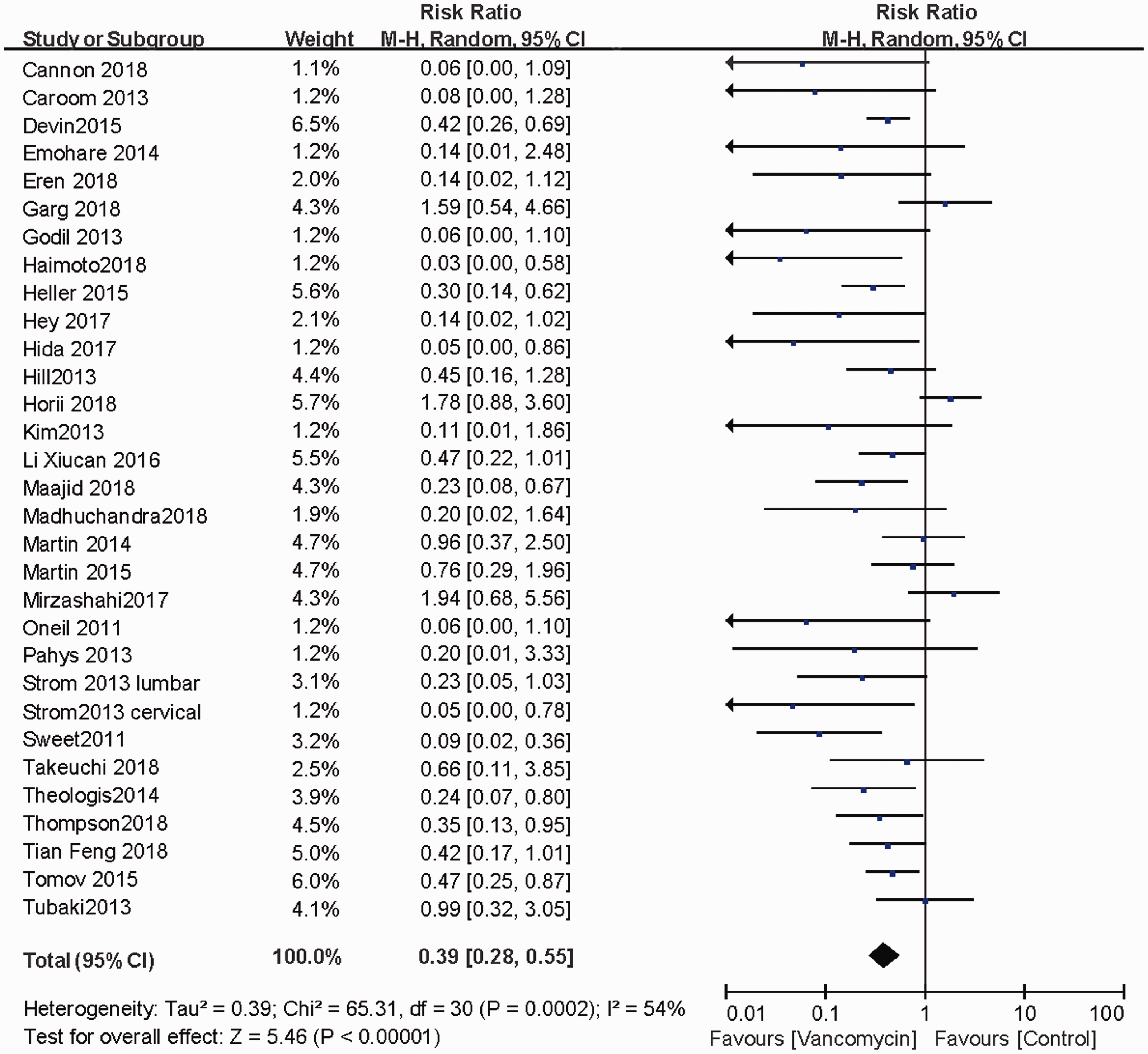
Overall meta-analysis of all included studies. CI, confidence interval.
RCTs normally have little patient selection bias and better repeatability than retrospective studies. Thus, in this study, we separately analyzed the results of RCTs and retrospective cohort studies. The three RCTs included in the meta-analysis reported the results for a total of 1517 patients, including 742 patients in the vancomycin group and 775 patients in the control group. The overall RR was 1.22 (95% CI = 0.62–2.40), indicating no significant difference between the two groups (P = 0.48, Figure 3). Meanwhile, data from the remaining 28 prospective and retrospective studies including 16,656 patients (7094 in the vancomycin group and 9562 in control group) revealed a significantly lower incidence of SSI in the vancomycin group than in the control group (RR = 0.33, 95% CI = 0.23–0.47, P < 0.01, Figure 3).

Subgroup analysis according to study design. CI, confidence interval.
Spinal surgeries with internal fixation usually require more time and result in a higher level of intraoperative hemorrhage. Together with foreign body implantation, patients who undergo internal fixation are more likely to experience SSI than non-instrumented cases. In the current study, 19 studies involving 8015 patients (3533 patients in the vancomycin group and 4482 patients in the control group) reported the results of surgeries with internal fixation. The meta-analysis illustrated that the incidence of SSI was significantly decreased by the local application of vancomycin (RR = 0.30, 95% CI = 0.18–0.48, P < 0.01, Figure 4).
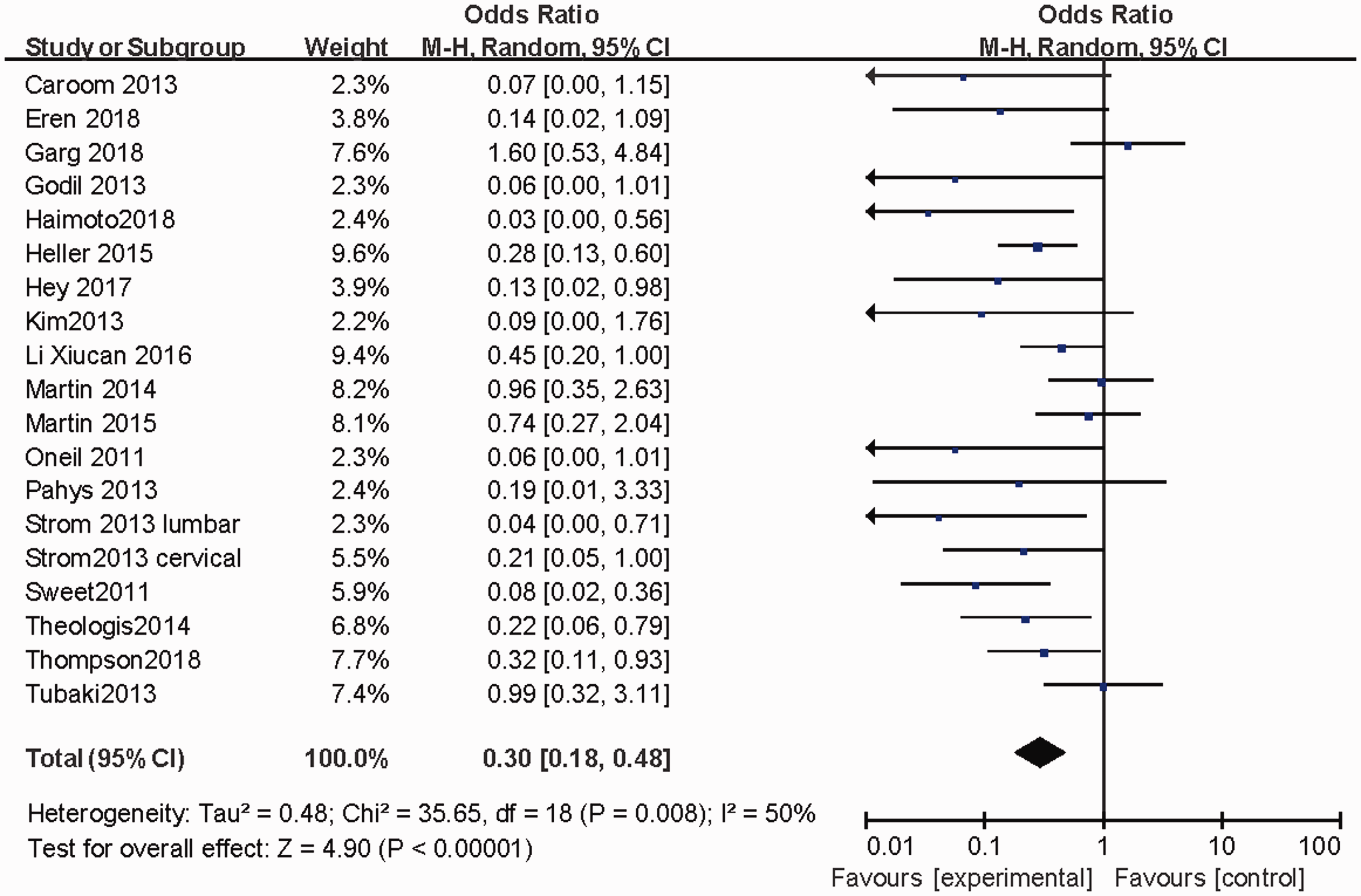
Meta-analysis of studies only including patients who underwent internal fixation.
Discussion
Vancomycin is a type of glycopeptide antibody. It was initially used to treat inflammation caused by S. aureus that cannot be controlled by penicillin because of patient allergy or bacterial resistance. 39 The drug adheres to the bacterial cell wall and causes various defects, including changes in the permeability of the bacterial cell membrane and selective inhibition of the formation of several RNAs. The local application of vancomycin ensures that a high concentration of antibiotics accumulates at the surgical site while maintaining low drug concentrations in the blood, killing Gram-positive bacteria in the surgical site while causing little harm to internal organs. One of the first reports of vancomycin locally applied as a means for SSI prevention in spinal surgery was that by Sweet et al. 31 They used 2 g of vancomycin, with 1 g applied to the bone graft and 1 g applied directly on the incision, and the incidence of infection was 0.2%, which was significantly lower than the control rate of 2.6%. After spinal injury or surgery, blood flow is usually disrupted, which makes the intravenous delivery of antibiotics to the injured site difficult. The local administration of vancomycin guarantees that a sufficient antibiotic concentration is achieved at the injured site while avoiding the side effects of high drug concentrations in the circulation system. Most studies identified in our meta-analysis revealed that this strategy significantly reduced the risk of SSI.
Although the local application of vancomycin proved to be generally effective in reducing the incidence of SSI, our results indicated that local delivery may not affect the incidence of SSI in patients with no internal fixation. This could be explained by the already significantly lower ratio of SSI after spinal surgeries with no internal fixation. As presented in Table 1, patients in different studies underwent different surgical procedures ranging from more invasive thoracolumbar deformity correction and tumor removal12,25,26,33,34 to less invasive decompression and fracture stabilization.8,27–30 For example, the incidence of SSI was as high as 5.2% among patients undergoing deformity correction in the study by Martin et al., 25 versus less than 1% among patients undergoing posterior cervical spine surgeries. 28
Despite the significantly lower risk of SSI in the vancomycin group than in the control group in most retrospective studies, all three RCTs26,32,37 reported no significant differences of the SSI risk between the groups. However, one of the RCTs used another locally applied antibiotic, and the other two RCTs were hampered by weak study designs and unreliability. Two of the three RCTs provided no trial registration number, and none of the RCTs was a multi-center study. One RCT compared vancomycin with the antibiotic ampicillin. The repeatability of these RCTs is questionable.
Safety is the main concern regarding the preventative application of vancomycin. The intravenous administration of vancomycin can lead to thrombophlebitis, eosinophilia, “red man syndrome,” ototoxicity, and nephrotoxicity. 40 When 1 g of vancomycin powder was administered to a female patient after corpectomy caused by breast cancer metastasis in a study by Mariappan, 41 an allergic reaction and circulatory collapse occurred. Youssef 42 identified an epidural seroma 6 weeks after the local application of 2 g of vancomycin in a female patient undergoing lumbar spine surgery. These are the only reports in the current literature of serious adverse effects associated with locally applied vancomycin. Edin et al. 43 found that when the concentration of vancomycin is lower than 1000 μg/mL, it has little effect on osteoblasts. In a study of Gans et al., 44 87 children undergoing surgical intervention for spinal deformity received 500 mg of vancomycin powder locally, and the blood serum concentration of vancomycin was not significantly different from that of patients in the control group. In the study by Armaghani, the serum vancomycin concentration was 2.5 μg/mL immediately after surgery and 1.1 μg/mL 2 days after surgery, which were significantly lower than the concentration that can be toxic to cells (10,000 μg/mL). Meanwhile, the corresponding concentrations in the drainage fluid at these time points were 403.0 and 115.0 μg/mL, respectively. 45 The current meta-analysis included no reports on the adverse effects of local vancomycin application on vital organs.
Although most studies confirmed that vancomycin can significantly decrease the incidence of SSI, there is no consensus on the effective vancomycin dose for this purpose. The vancomycin dose has varied from 500 mg to 6 g in different studies, with most studies using doses of 1 to 2 g. The site at which the vancomycin should be applied is also under dispute. There is no consensus regarding whether the drug should be applied in deep or superficial fascia, directly to the bone graft, or on the host bone. Further animal and human studies are needed to study the effect of vancomycin in each of those scenarios.
In addition to safety, drug resistance is another important subject concerning the application of antibiotics. Considering that vancomycin is one of the last effective measures against surgical infections, whether local application can lead to vancomycin-resistant bacterial infection is one of the main concerns in the preventive application of this antibiotic. It can be concluded from the current meta-analysis of nearly 20,000 patients that the local application of vancomycin powder during spinal surgery does not increase the incidence of vancomycin-resistant bacterial infection.
Other authors such as Bakhsheshian 46 and Texakalidis et al. 47 conducted meta-analyses of studies investigating the effect of vancomycin powder on the incidence of SSI after spinal surgery. Considering that several studies on this subject are newly published, we included larger numbers of studies in patients in our meta-analysis. The current study, despite our comprehensive literature search and inclusion of a large number of patients, has certain disadvantages. First, only three of the included studies were RCTs, which had the opposite result as the overall data, and the remaining studies were reports from retrospective patient series. Second, most studies included relatively small number of patients, which may have led to patient selection bias. However, most studies had relatively high quality, and because of the large overall patient base, the results of this meta-analysis can be used as a reference for decision making in spinal clinics.
Increasing numbers of authors agree that the local application of vancomycin is a cost-effective and safe strategy for preventing SSI in spinal clinics. However, the pharmacokinetics of this process is unclear, and all three RCTs indicated that vancomycin provided insignificant advantages over control treatments. More high-quality RCTs involving larger numbers of patients are needed before this method can be recommended as a routine modality in clinical practice.
Conclusions
Based on the current literature, the incidence of SSI after spinal surgeries can be significantly decreased by the local application of vancomycin powder. However, more high-quality RCTs should be conducted to further validate this conclusion.