
Abstract
Study Design
Systematic review and meta-analysis.
Objective
Compilation of complication outcomes data from the surgical management of severe rigid kyphoscoliosis patients using VCR-based vs non-VCR-based corrective maneuvers is lacking. This meta-analysis aimed to compare complication outcomes between those classified osteotomy approaches.
Methods
Thorough literature review and meta-analysis were conducted between January 2000 and September 2021. The selection criteria were studies: i) reporting major curve Cobb angle of ≥80° and flexibility of <25% or 30%; ii) comparing VCR or ≥ Type V Schwab osteotomy defined as VCR-based vs [non-VCR-based] techniques, (any osteotomy or technique other than VCR); iii) published in English with ≥10 patients; iv) reporting complication rates; and v) having minimum of 2-year follow-up. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Significance level was set at (P < .05).
Results
Of the 174 patients included, 52.30% (n = 91) and 47.70% (n = 83) were VCR-based and non-VCR-based, respectively. The incidence of dural tears/nerve injuries/significant intraoperative-neuromonitoring changes was significantly higher; [OR = 6.78, CI= (1.75 to 26.17), I2 = 0%, (P = .006)] in the VCR-based group than the non-VCR-based group. The ‘overall surgical and medical’ complication rate was significantly higher in the VCR-based group, [OR = 1.94, CI= (1.02 to 3.67), I2 = 31%, (P = .04)].
Conclusion
Both VCR-based and non-VCR-based surgical techniques for management of severe rigid scoliosis and kyphoscoliosis patients pose comparable overall surgical complication rates, while a significantly higher perioperative neurological complication incidence was associated with VCR-based technique compared to the non-VCR-based techniques. The VCR-based technique was associated with 6.78 times higher incidence of neurological complications compared to non-VCR-based techniques.
Keywords
Introduction
In the spine literature, severe rigid scoliosis or kyphoscoliosis has been reportedly defined as severe spinal curves in the coronal plane with Cobb angle of ≥80° and angular curves in the sagittal plane of more than 50° and flexibility of <25% or 30%.1-7 Etiologies of these severe deformities include congenital, syndromic, neuromuscular, as well as idiopathic, the latter of which less commonly become severe.8-11 Regardless of the etiology of scoliosis or kyphoscoliosis, patients clinically presenting with acutely progressive or symptomatically severe rigid spinal deformities require timely surgical intervention to halt progression, achieve correction, restorate global spinal alignment, and improve back pain or neurological deterioration, as well as cosmetic and quality of life outcomes.12-15
Currently employed surgical approaches include posterior-only, antero-posterior, with various osteotomies or three-column osteotomies including resection of at least one full vertebra with its rostral and caudal intervertebral discs, otherwise known as vertebral column resection (VCR), while surgery may be staged or non-staged.10,16-19 During surgical planning and decision-making, surgical techniques for management of severe rigid scoliosis or kyphoscoliosis can be complex and clinically challenging. Most often, due to the rigidity and severity of these curves, aggressive surgical corrective cantilever maneuvers and osteotomy techniques are embraced to allow adequate and maximum correction of the scoliotic or kyphoscoliotic curves.6,20-26 The advancement of technology, anesthetic care, intraoperative neuromonitoring, and instrumentation systems have allowed for the advancement of complex osteotomy techniques in treatment of severe rigid spinal deformities.27-29
Vertebral column resection typically permits as much as 45 to 60° of curve correction usually at the apex of the major curve.30-32 Even though VCR-based technique acknowledges maximum correction amongst the osteotomy phenotypes, it is associated with a higher incidence of complications including neurological deterioration.33-35 There are non-VCR-based techniques for achieving satisfactory corrective and patient outcomes in severe rigid spinal deformity, including posterior column osteotomies (PCOs), also known as such as Smith-Petersen osteotomy (SPO) and Ponte osteotomy (PO), or pedicle subtraction osteotomy (PSO), bone-disc-bone osteotomy (BDBO), anterior release, internal distraction, among others.36,37 To assess the safety outcomes of VCR-based vs non-VCR-based surgical techniques, it is critical to identify comparative studies that compared complication outcomes of VCR-based and non-VCR-based surgical techniques in the surgical treatment of patients with severe rigid scoliosis or kyphoscoliosis.
Comparative studies discussing the perioperative complication outcomes of VCR-based vs non-VCR-based techniques for correction of severe rigid scoliosis or kyphoscoliosis have not been reported in the spine literature to date in a systematic comparison of the entirety of the literature. It is of pertinent importance that we identify and weigh the risks associated with these techniques and determine where the risk trade-offs may be unacceptable especially in cases in which lower complexity procedures resulting in reliable corrections are reported to be equivalent between either of these techniques when appropriately selected. 38
Our review team, therefore, aimed to conduct a systematic review and meta-analysis of perioperative complication rates reported in comparative studies of VCR-based and non-VCR-based surgical techniques in the management of severe rigid scoliosis or kyphoscoliosis.
Methodology
Search Strategy and Study Selection Criteria
This systematic review was performed and reported in observance to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement in addition to the current recommendations of the Cochrane Collaboration.39-41
Search Strategy
Relevant comparative studies comparing vertebral column resection, [VCR-based] and other corrective maneuvering or osteotomy, [non-VCR-based] techniques were acquired through a comprehensive electronic literature search from 5 electronic databases: PubMed, EMBASE, MEDLINE, Google Scholar, and Cochrane library databases from January 1st, 2000, until October 31st, 2021. The search terminology included “severe rigid scoliosis”, “severe rigid kyphoscoliosis”, “surgical management”, “vertebral column resection”, or “comparative study”.
Selection of Studies
Studies were selected by 4 independent authors who screened the titles and abstracts of the retrieved studies for their eligibility of inclusion and excluded any unrelated studies. In the case that eligibility could not be assessed from the title or abstract alone, the entire text of the respective study was retrieved and further reviewed for relevancy and eligibility on the premise of the study aim to ensure the best-formulated synthesis of data and information. Furthermore, the references of the studies were searched for other potential studies. If an article was deemed relevant, the full text was obtained for review and for potential consideration of inclusion through further screening.
Inclusion and Exclusion Criteria
Studies were considered qualified if they had fulfilled the following inclusion criteria: (1) patients diagnosed with severe rigid scoliosis or kyphoscoliosis defined with average Cobb angle of ≥80° and flexibility of <25% or 30%, and with or without sagittal plane deformities; (2) patients primarily managed with only VCR or ≥ Type V Schwab osteotomy (defined as VCR), [VCR-based] vs any osteotomy types or corrective techniques other than VCR, [non-VCR-based]; (3) studies published English that included at least 10 patients; (4) studies reporting perioperative complication rate outcomes; (5) studies with 2-year minimum follow-up period. Conversely, articles were mutually culled and excluded if they met any of the following exclusion criteria: (1) if article compared between any 2 VCR-based techniques; (2) if article included modified VCR-based technique; (3) if article included etiology of global-only kyphosis or infection-induced kyphosis in the [VCR-based] vs [non-VCR-based] compared patient cohorts, and (4) if the etiology in each of the compared group was degenerative. We did not apply a criterion for screening the level of evidence and whether a study was randomized controlled trial, prospective or retrospective in nature with the sole aim to maximize the patient pool. Discussions between the 4 main authors resolved any disagreements about inclusion and exclusion criteria.
Outcome Measures
The main outcome measures were generally reported perioperative medical and surgical complication rate outcomes between [VCR-based] vs [non-VCR-based] techniques for the surgical treatment of rigid scoliosis or kyphoscoliosis. These perioperative complications included compilation of cardio-pulmonary complications; dural tear/nerve injury/significant intraoperative neuromonitoring changes; surgical site infections/wound complications; implant/cage-related issues; postoperative intensive care unit (ICU) admission; re-operation within 2-years following corrective surgery; and overall surgical complication outcomes reported across the 4 included studies.
Data Extraction
Data extraction was conducted in adherence to a custom data extraction table created for documenting all relevant details from the included articles. The 4 main authors were tasked to independently extract data from each article, including the first author’s name, publication year, patient demographics, severe rigid scoliosis or kyphoscoliosis diagnosis, baseline characteristics, type of surgical intervention, thus comparing VCR or ≥ Type V Schwab osteotomy defined as [VCR-based] vs [non-VCR-based] techniques, (any osteotomy or technique other than VCR), follow-up period, results on perioperative complication outcome of interest, and the quality assessment score of each included study. Our initial goal was to screen for Level I or II comparative studies inclusion, but if no published reports were found, we intended to further screen for Level III comparative studies inclusion as a strategy to maximize the captured patient pool due to the rarity of reported comparative studies outcomes on corrective techniques in severe rigid scoliosis or kyphoscoliosis patients.
Quality and Risk of Bias Assessment
The 4 main authors independently evaluated the quality and risk of bias of each included comparative study in accordance with the Methodological Index for Non-Randomized Studies (MINORS) tool, and the McGuinness and Higgins’ Risk-of-bias VISualization (robvis) tool, which includes the following criteria: bias resulting from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in outcome measurement, and bias in selecting the reported result. 42
In each included comparative article, every criterion was classified as among low risk, with some concerns, or high risk of bias. The quality of each study was classified into 1 of 3 levels: “low risk of bias” (all items were classified as low risk), “some concerns of risk of bias” (at least 1 item was classified with some concerns), or “high risk of bias” (at least 1 item was classified as high risk). Any conflicts pertaining to the risk of bias assessment were solved by discussion between the 4 main authors.
Statistical Analyses
For each study, outcomes included in our analysis were effective number. Data were reported as odds ratios, (ORs) and 95% confidence intervals (CIs). Statistical heterogeneity was evaluated by the I2 test. If the I2 value was >25%, the random effects model was employed. Conversely, if the I2 value was <25%, the fixed-effects model was used. Any potential explanations for heterogeneity were initially investigated by a random-effects model of the meta-analysis. The meta-analysis significance level was set at (α = .05). Stata version 17.0 (Stata Corp LLC, College Station, TX) and RevMan version 5.4.1 statistical software packages were utilized for all meta-analyses.
Results
Search Results and Study Selection
The literature search resulted in 1216 publications related to the treatment of severe rigid scoliosis. Out of them, 455 articles were identified as eligible for inclusion, then 432 were excluded due to duplicate records, nonconformity, or non-comparative nature of studies, leaving 23 full-text studies that were further screened for satisfying the specific qualitative criteria for this systematic review and meta-analysis. A total of 4 comparative studies were finally observed.6,43-45 All four (4) comparative studies were included in the qualitative analysis according to PRISMA guidelines (Figure 1). They were comparative studies that related [VCR-based] vs [non-VCR-based] techniques for the surgical treatment of patients with severe rigid scoliosis or kyphoscoliosis. These 4 studies also assessed the perioperative medical and surgical complication incidence of treated patients between [VCR-based] and [non-VCR-based] approaches. PRISMA Flow diagram of the search strategy and the yield of eligible studies.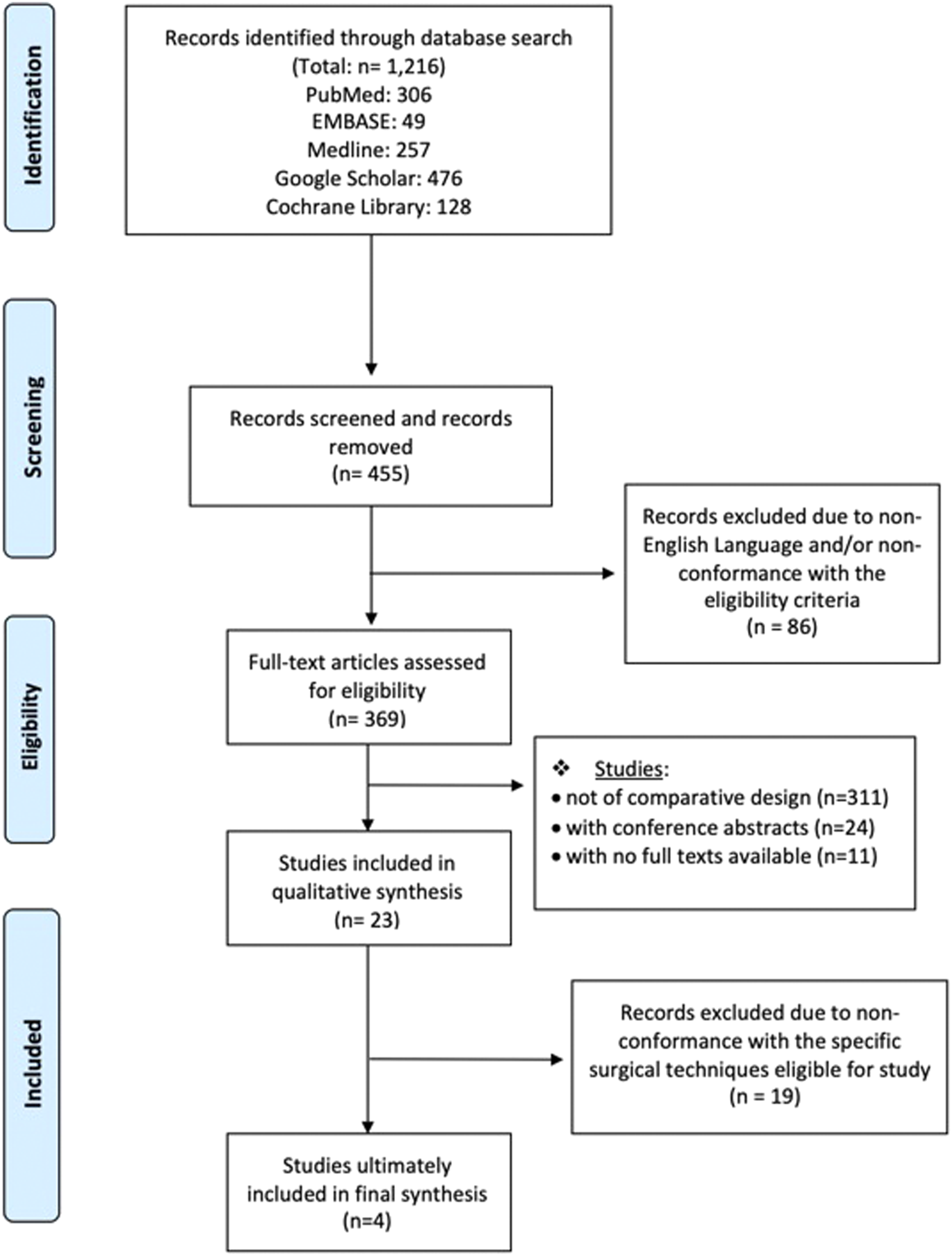
Characteristics of Included Studies
Characteristic Features of Included Comparative Studies.
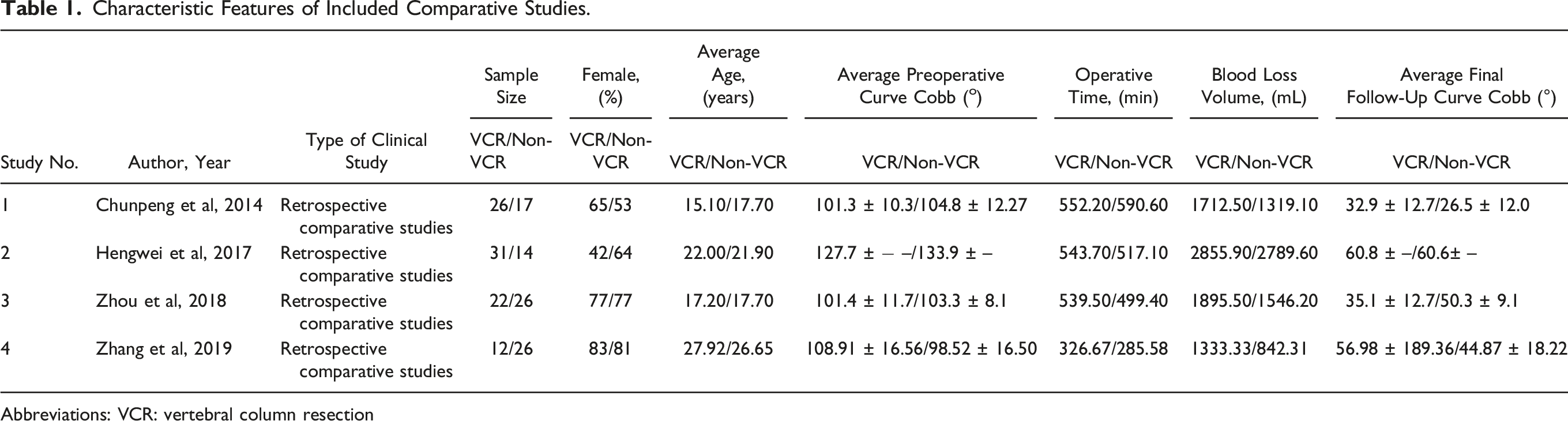
Abbreviations: VCR: vertebral column resection
Methodologic Quality and Risk of Bias Estimation
All the 4 comparative cohorts of the included studies had patients who were allocated to either VCR-based or non-VCR-based surgical techniques. Comparative studies were considered of high quality, and the risk of bias across and within all the included studies was determined to be low based on Cochrane collaboration, ‘McGuinness and Higgins’ Risk-of-bias VISualization (robvis),
42
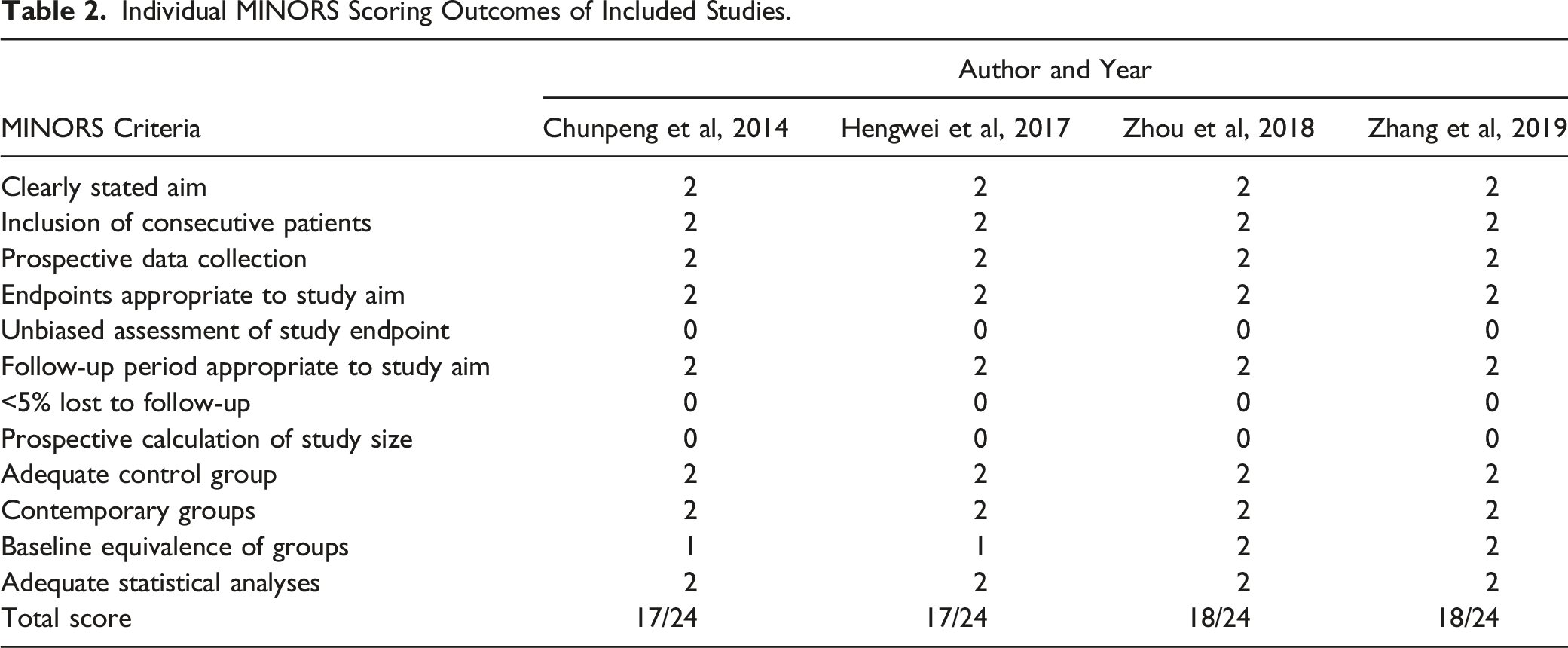
(Figure 2) and MINORS assessment tools (Table 2), respectively.
46
Risk of bias assessment. Individual MINORS Scoring Outcomes of Included Studies.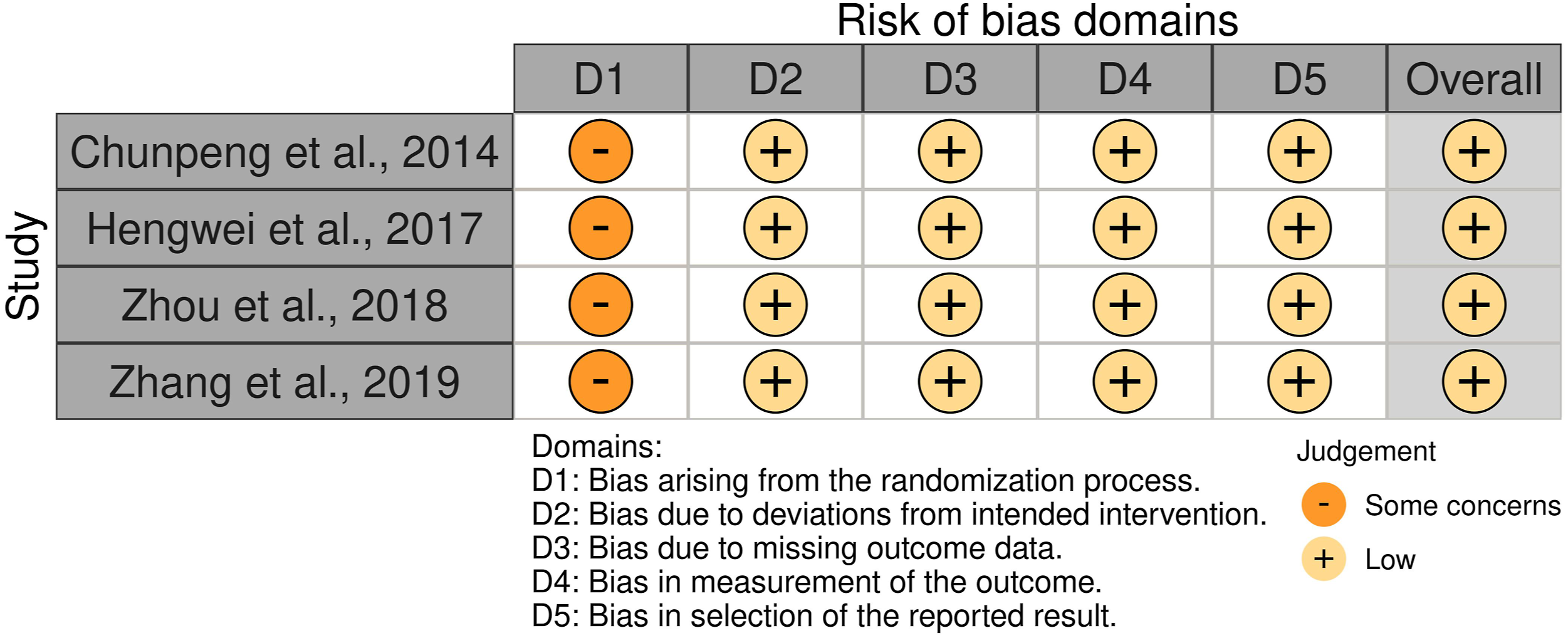
Medical Complications
There were 2 generally reported perioperative medical complications, which were a) cardiopulmonary complications and b) non-routine surgical intensive care unit (SICU) admission. All four (4) comparative studies6,43-45 reported on cardiopulmonary complications, but only2; Chunpeng et al
43
and Zhou et al
45
reported on non-routine SICU admission outcomes, (Figure 3). Generally reported postoperative complications.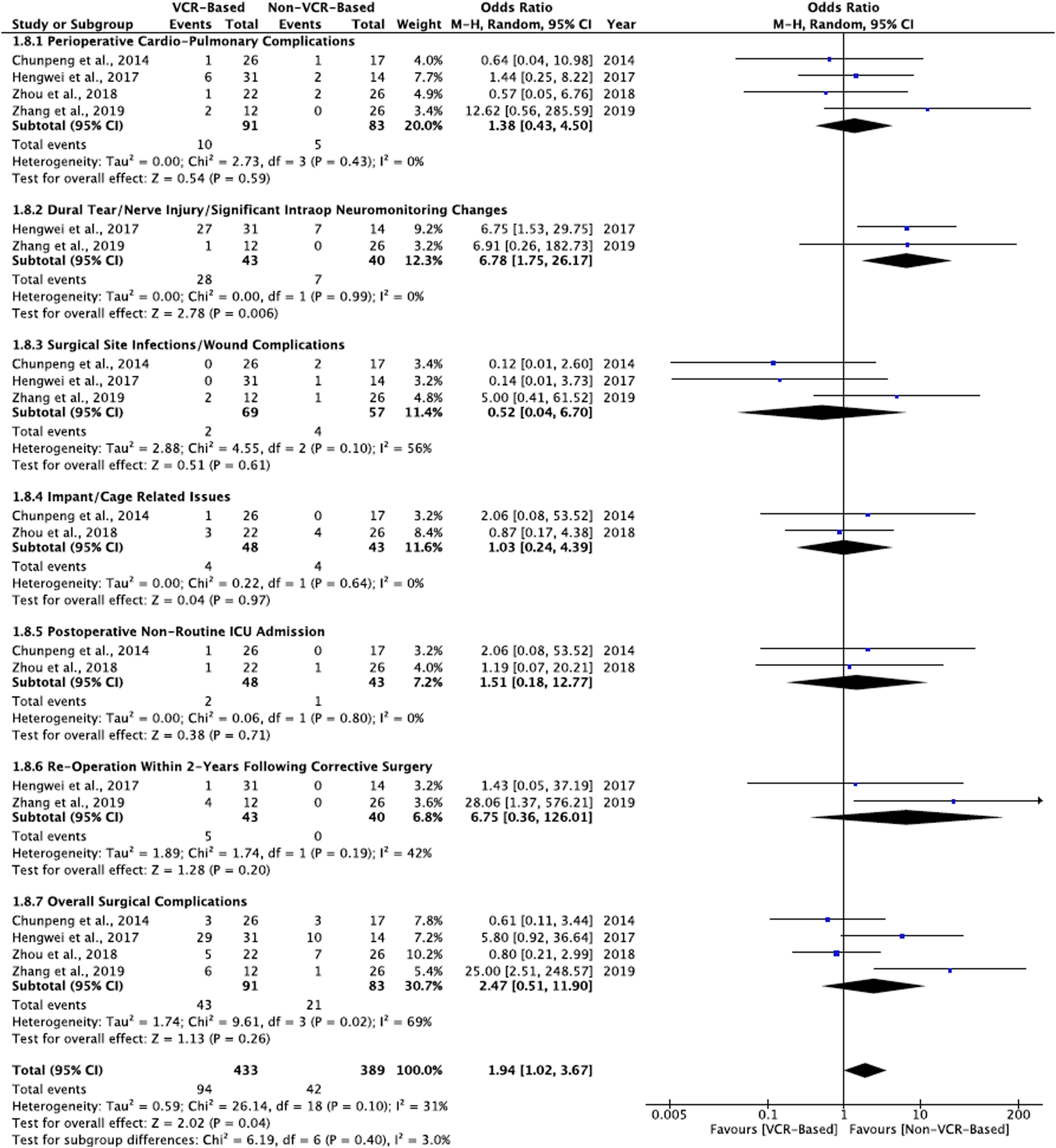
Cardiopulmonary Complications
There was n = 10/91 (11.0%) vs n = 5/83 (6.0%) incidence of cardiopulmonary events observed between the VCR-based vs non-VCR-based patient groups, respectively, from all four (4) studies,6,43-45 and no statistical significance was observed, [OR = 1.38, CI= (.43 to 4.50), I2 = 0%, (P = .59)], (Figure 3).
Surgical Intensive Care Unit Admissions
There was n = 2/48 (4.2%) vs n = 1/43 (2.3%) incidence of non-routine SICU admissions observed between the VCR-based and non-VCR-based patient groups, respectively, from two (2) studies: Chunpeng et al 43 and Zhou et al, 45 and no statistical significance was observed, [OR = 1.51, CI= (.18 to 12.77), I2 = 0%, (P = .71)], (Figure 3).
Surgical Complications
There were 4 generally reported perioperative surgical complications, which were: 1) dural tears/nerve injury/significant intraoperative neuromonitoring changes; 2) surgical site infections/wound complications; 3) implants/cage-related issue; and 4) re-operation within 2 years of index corrective surgery.
Dural Tears/Nerve Injury/Significant Intraoperative Neuromonitoring Changes
There was n = 28/43 (65.12%) vs n = 7/40 (17.5%) incidence of durotomy, nerve injury, or significant neuromonitoring changes observed from two (2) studies: Hengwei et al 44 and Zhang et al 6 between the VCR-based vs non-VCR-based patient groups, respectively, and was statistically significant, [OR = 6.78, CI = (1.75 to 26.17), I2 = 0%, (P = .006)], (Fig. 3).
Surgical Site Infections/Wound Complications
There was n = 2/69 (2.9%) vs n = 4/57 (7.0%) incidence of surgical site infections/wound complications respectively observed between the VCR-based vs non-VCR-based patient groups from three (3) studies: Chunpeng et al 43 reported 2 patients with wound complications in their non-VCR-based cohort, Hengwei et al 44 reported 1 patient with deep surgical site infection (SSI) in their non-VCR-based patient cohort, and Zhang et al 6 reported 2 patients with deep SSI in the VCR-based cohort and 1 patient with superficial SSI in the non-VCR-based patient cohort, while no statistical significance was observed, [OR = .52, CI= (.04 to 6.70), I2 = 0%, (P = .61)], (Fig. 3).
Implants/Cage-Related Issues
There was n = 4/48 (8.3%) vs n = 4/43 (9.3%) incidence of implants/constructs-related issues observed between the VCR-based and non-VCR-based patient groups, respectively, from two (2) studies: Chunpeng et al 43 reported one incidence of pedicle screw mispositioning in 1 patient in the VCR-based group. Zhou et al 45 reported 1incidence of pedicle screw mispositioning in 1 patient and titanium mesh cage mispositioning in 2 patients in the VCR-based group while 4 patients were detected with a screw breech each on postoperative postero-anterior radiographs, and no statistical significance was observed, [OR = 1.03, CI= (.24 to 4.39), I2 = 0%, (P = .97)], (Fig. 3).
Re-Operation Within 2 years of Following Corrective Surgery
There was n = 5/43 (11.6%) vs n = 0/40 (.0%) incidence of re-operation within 2 years of primary corrective surgery observed from two (2) studies: Hengwei et al 44 reported 1 case of re-operation within 2 years due to rod breakage in the VCR-based group and Zhang et al 6 reported 4 total cases of re-operation the VCR-based patient groups (2 patients for deep incisional debridement, 1 patient for internal fixation adjustment, and 1 patient for thoracoplasty, and no statistical significance was observed between VCR-based vs non-VCR-based group, [OR = 6.75, CI= (.36 to 126.01), I2 = 42%, (P = .20)], (Fig. 3).
Overall Surgical Complications
All four (4) comparative studies6,43-45 reported complication outcomes between the VCR-based vs non-VCR-based patient groups. Overall, n = 43/91 (47.3%) vs n = 21/83 (25.3%) surgical complication incidence was observed between the 2 techniques, but no statistical significance was observed, [OR = 2.47, CI= (.51 to 11.90), I2 = 69%, (P = .26)], however, we found significant difference between VCR-based and non-VCR-based techniques for ‘overall combined medical and surgical’ complication incidence, [OR = 1.94, CI= (1.02 to 3.67), I2 = 31%, (P = .04)], (Fig. 3).
Risk of Bias Across Studies
The risk of bias outcomes between the included studies were as follows: the comparisons of anteroposterior VCR [APVCR] vs anterior release plus posterior spinal fusion [AR+PSF] in Chunpeng et al.’s 43 study demonstrated a MINOR score of 17/24; of non-extended VCR [Non-Ext_VCR] vs extended pedicle subtraction osteotomy [Ext_PSO] in Hengwei et al.’s 44 study demonstrated a MINOR score of 17/24; of anteroposterior VCR [APVCR] vs anteroposterior spinal fusion [APSF] in Zhou et al.’s study 45 demonstrated a MINOR score of 18/24; and of posterior-only VCR [PVCR] vs multiple asymmetrical Ponte osteotomy [MAPO] in Zhang et al.’s 6 study demonstrated a MINOR score of 18/24, (Table 2).
Discussion
The authors of this meta-review study sought to compare perioperative complication incidence in comparative studies of VCR-based vs non-VCR-based techniques utilized in surgical treatment of severe rigid scoliosis or kyphoscoliosis. In cases of severe rigid spinal deformities, VCR-based surgery is an effective corrective technique; nevertheless, it is also associated with a noteworthy risk of major perioperative morbidity and neurological complications.34,35 This practically means that VCR-based spinal surgery is a technically demanding skill that even the most experienced surgeons find challenging. It is seldom utilized in most spinal deformity patients and should be utilized only when other safer and less technically demanding osteotomy techniques are rather considered not plausible. Our study, the first meta-analysis of comparative studies assessing complications in VCR-vs non-VCR-based procedures for spinal deformity, points to the higher rates of neurological injury associated with VCR.
Surgical maneuvers other than VCR for correcting severe rigid spinal deformities to accomplish spinal alignment, curve correction, and satisfactory patient outcomes do exist.6,36,37,47,48 Due to the very high risk of perioperative and neurologic complications associated with VCR-based technique,34,35 outcomes of aggregated studies on the premise of VCR-based vs non-VCR-based surgery would serve as a basis of reference in assessing safety during surgical technique and decision making and to enhance value-based outcomes of severe deformity patients. In 2007, Lenke et al 49 reported a 20.0% complication rate in a study of 43 adult and pediatric PVCR patients. Also in 2013, Lenke et al 15 reviewed a large VCR-based multicenter case series of 147 spinal deformity patients that comprised of circumferential VCRs (including staged and non-staged procedures) and the authors observed 68 intraoperative events and 43 postoperative events with an overall 58.5% complication incidence.
In other published studies, Ayvaz et al, 50 reviewed 18 adolescent congenital kyphoscoliosis patients with curves ranging from 31° to 116°, in which the surgeons applied posterior all-pedicle screw instrumentation combined with multiple posterior column (SRS-grade-2) osteotomies and concave rib resections. No neurological complications were observed in their cohort of non-VCR-based procedures. They observed perioperative complication incidence of only 11.1% (1 pneumothorax and 1 pneumonia) and achieved satisfactory corrective outcomes. More recently, Sacramento-Dominiguez et al, 51 reviewed 72 patients with severe rigid curves >100°, who were safely treated with multiple posterior column osteotomies (MPCOs) and posterior fusion following halo-gravity traction while reporting an overall perioperative complication rate of 22.2%. They also attained satisfactory results in their patient cohort. These complication rates were low and consistently comparable with the overall complication rate of 25.3% observed in the non-VCR-based cohort. It is becoming more evident that utilization of milder osteotomy grades, such as PCOs, in the management of severe rigid spinal curves when feasible results in lower complication rates. Nevertheless, the ultimate decision of choice of osteotomy technique is solely reliant on the nature of the pathology, the surgeon’s armamentarium in terms of training and experience, and comfort with the osteotomy technique, and other clinical and patient factors that dictate perioperative clinical outcomes.
In this current study, we observed a significant overall complication incidence of 47.3% associated with the VCR-based technique compared to a 25.3% overall complication incidence in non-VCR-based patient group. Albeit comparison between the 2 techniques was statistically insignificant regarding the overall surgical complication rates, an overview of each perioperative event stemming from the VCR-based surgeries compared against that of the non-VCR-based surgeries in this study is certain to demonstrate higher overall perioperative complication rates in the VCR-based surgeries in these severe rigid scoliosis or kyphoscoliosis patients. Clearly, we observed significantly higher rates of incidence of ‘dural tears/nerve injury/significant neuromonitoring changes’ in the VCR-based patient group and those patients were 6.78 times at risk higher than the non-VCR-based patient group. These findings corroborate evidence from cohort studies surrounding neurological complication rates following VCR-based procedures.34,52,53 In the service of minimizing complications while optimizing outcomes and advancing value-based care in healthcare delivery, it is of great importance that safety is prioritized during surgical decision-making, especially when non-VCR-based options may be efficacious in managing these severe rigid spinal deformity patients. The premise of clinical safety and value-based outcomes in surgical approaches to spinal deformity correction is rapidly becoming a global trend and concern in spine practice. 38
Strengths and Limitations
To our knowledge, this is the first ever reported study on comparison of complication incidence between VCR-based and non-VCR-based techniques in the surgical treatment of severe rigid scoliosis or kyphoscoliosis. Although the value of approaches not involving VCR are suggested by this review, this study is also undoubtedly limited by the lack of included prospective or randomized controlled studies and hence may reflect underreported complication incidence. Further, the total pool of patients within each comparative group or subset is small with a limited number of studies to choose from (4). Another limitation is that one of the included studies, thus, Hengwei et al 44 compared patient outcomes that included pedicle subtraction osteotomy (PSO) or a Schwab-SRS grade 3-4 in the non-VCR group vs VCR (grade 5-6). Essentially this is a comparison of greater and lesser complexity three-column osteotomies (3COs). 36 This may cloud the delineation between complications associated with lesser grade PCOs and true VCR (grade 5-6 osteotomies). We believe in order to decisively inform the spinal deformity practice; it would be beneficial to study the complication-reported outcomes of each type of 3CO [grades 3-6] to weigh the risks associated with extended or non-extended application of the type of 3CO. This study niche is under feasibility evaluation by our study team.
Conclusion
The evidence generated from this study indicates that the overall surgical complication rate surrounding non-VCR-based surgical techniques appears comparable to rates observed in VCR-based patient groups for the treatment of severe rigid spinal deformities. In this current meta-review, we ultimately observed that severe rigid scoliosis or kyphoscoliosis patients managed by VCR-based surgical techniques are 6.78 times significantly at higher risk of incidence of ‘dural tears/nerve injury/significant neuromonitoring changes’ compared to patients managed with non-VCR-based surgical techniques. The outcome of this study conclusively warrants the spine practice to employ lesser grades of corrective osteotomies and perhaps in combination with halo-gravity traction (HGT) in these severe rigid scoliosis or kyphoscoliosis patients when feasible, especially when comparable and satisfactory major curve corrective outcomes can be achieved.
Footnotes
Authors’ Contributions
N.V. and Y.H. conceptualized and designed the study; N.V., N.N.A., K.M., M.K.M., W.H.H., W.C.C., M.B.M., Z.Y.Y., N.R.S., Y.P.Z., A.X.P., K.G., and X.Y.C., acquired data; N.V., N.N.A., M.K.M., K.G., N.R.S., Y.P.Z., K.M., and Y.H. analyzed and interpreted data; N.V. and B.L. drafted the article; N.N.A., K.M., M.K.M., Y.P.Z., A.X.P., S.S.K., A.A., B.L., Y.H., and N.V. critically revised the article; all authors reviewed submitted version of the article; A.A., B.L., Y.H., and N.V. approved the final version of the article; N.V., K.M., N.N.A., K.G., M.B.M., W.C.C., W.H.H., Z.Y.Y. and N.R.S. provided technical and material support. Y.H. and N.V. spearheaded the study and Y.H., A.A., and B.L. supervised the entire study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.