
Abstract
Study Design
Systematic review and meta-analysis.
Objective
This meta-analysis aimed to evaluate the learning curve in endoscopic spinal surgery, including the time to mastery and challenges faced by novice surgeons, to improve learning and surgical outcomes.
Methods
Data extraction included the learning curve period and a comparison of surgeons with more experience or late period of the learning curve (late) and surgeons with less experience and in the early period of the learning curve (early) with respect to demographic, surgical, hospitalization, functional, and complication variables. Statistical analysis was performed using Review Manager 5.4.1 software.
Results
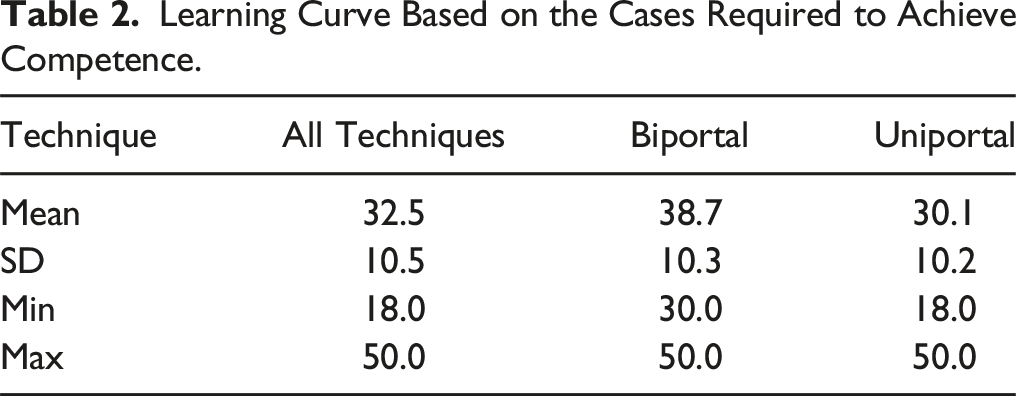
This meta-analysis included 16 studies (n = 1902). The average number of cases required to reach the learning curve was 32.5 ± 10.5. The uniportal technique required fewer cases (30.1 ± 10.2) than biportal technique (38.7 ± 10.3). There were no significant differences in demographic variables, operation level, or duration of symptoms between the advanced and novice surgeons. Advanced surgeons showed better outcomes in VAS leg pain at less than 6 months (SMD 0.18, 95% CI 0.01-0.34) and >6 months (SMD 0.14, 95% CI 0.02-0.27), as well as VAS back pain at > 6 months (SMD 0.16, 95% CI 0.04-0.29). The incidence of total complications was significantly higher in the novice surgeon group. The specific complications did not differ significantly between the 2 groups.
Conclusions
The average number of cases required to reach the learning curve was 32.5 ± 10.5. Experienced surgeons had shorter surgery and fluoroscopy times, better outcomes in leg and back pain, and a lower incidence of complications than novice surgeons.
Introduction
Spinal surgery is a complex and challenging field that requires technical skill and experience to achieve optimal outcomes. 1 As surgeons delve into this field, they encounter a learning process known as the “learning curve in spinal surgery.” This curve represents the trajectory of skill acquisition and improvement in surgical outcomes as surgeons gain experience and mastery of the specific techniques used in spinal interventions. There are as many learning curves as there are surgical techniques.
Currently, there is growing interest in the use of spinal endoscopy as a less invasive alternative to open spinal surgery. 2 Spinal endoscopy has shown promising results in terms of shorter surgical times, reduced blood loss, decreased postoperative pain, shorter hospital stay, and lower rates of revision surgery. 2 However, this technique requires experience and training to become familiar with and accustomed to endoscopic visualization.
The learning curve is a recurrent topic in the literature on spinal endoscopy and has been mentioned as one of the key aspects in mastering this technique.3-7 However, there is no adequate consensus on the number of cases required to achieve proficiency in spinal endoscopy.3-7 Some studies suggest that approximately 20 cases are needed for posterior cervical foraminotomy 3 and 34 cases for lumbar intervertebral fusion. 4 Other reports indicate that more experienced surgeons perform the procedures in a third less time than in the early stages of their learning. 5 In addition to the reduction in surgical time, other advantages associated with mastering spinal endoscopy have also been observed. These include a lower rate of complications 8 and reduced postoperative pain measured using a Visual Analog Scale (VAS). 9
For those taking their first steps in spinal endoscopy, specific challenges have been identified, such as lack of support and fear of potential complications. 10 Addressing these challenges comprehensively in a scientific article could provide valuable insights for novice surgeons and help to alleviate their concerns.
Quantifying and understanding the learning curve in spinal surgery is crucial as this information will be useful in guiding and measuring the progress of novice surgeons. Therefore, the aim of this study was to evaluate the time required to achieve mastery in spinal endoscopic surgery, specifically focusing on uniportal and biportal techniques, and to identify the most common challenges encountered by surgeons in the early stages compared to experienced surgeons. This knowledge is expected to contribute to better learning and improvement in surgical outcomes in the field of spinal surgery.
Methods
Eligibility Criteria
The protocol for this meta-analysis was registered in the PROSPERO (CRD42024541636). The PRISMA guidelines 11 and PICOS search strategy were followed. Patients included in the study underwent biportal, or uniportal endoscopic surgery for spinal stenosis. The intervention group consisted of surgeons who were in the early period of the learning curve or had less experience, with the term “early” defined differently in each study based on the operative time. The comparator group consisted of surgeons with more experience or who were in the late period of the learning curve. The main outcomes assessed were the time required for the learning curve and the differences in efficacy and safety outcomes between novice and experienced surgeons. Comparative studies or series that established a period for the learning curve and compared 2 types of surgeons were included in the analysis.
Exclusion criteria were applied to ensure the quality and relevance of the studies included in our manuscript. Duplicate studies, case reports, and letters to editors were excluded to avoid redundancy and prioritize comprehensive research findings. Studies published >10 years ago were also excluded, as recommended by experts in the field, considering the potential changes in endoscopic standards over time that could influence the results. Additionally, techniques, such as tubular endoscopy and microscopy, were excluded to maintain homogeneity in the study sample. Studies lacking relevant variables or with incomplete or missing data were also excluded to ensure data reliability and completeness.
Information Sources and Search Methods for Identification of Studies
A comprehensive search was conducted in the PubMed, Embase, Scopus, and Cochrane Library databases to identify relevant studies. No language restrictions were applied, and a filter was applied to include articles published within the last 10 years based on expert recommendations in the field. The search terms are detailed in Supplemental File 1. Two authors independently screened studies for eligibility. In cases of discrepancies, a third author was involved in the decision-making process to reach consensus.
Data Extraction and Data Items
Data extraction was performed by 2 authors, and a third author was involved in resolving discrepancies to reach a consensus. The extracted characteristics of the included studies encompassed several aspects. The primary variable of interest was the learning curve, which was evaluated based on the number of cases required to gain experience. Demographic variables included sex, mean age, BMI, number of patients who smoked, operation level, and duration of symptoms; surgical and hospitalization variables encompassed surgery time, length of hospital stay (LOS), and fluoroscopy time. Functional outcomes were assessed using the visual analog scale (VAS) for leg pain, VAS for back pain, and Oswestry Disability Index (ODI). Complications were also collected to evaluate safety outcomes.
Assessment of Risk of Bias in Included Studies
The risk of bias in the included studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) (Supplemental Table 1 12). The MINORS tool consists of 12 items with a maximum score of 24 for comparative studies and 16 for non-comparative studies. For non-comparative studies, scores ranging from 0 to 4, 5-7, 8-12, and ≥13 were categorized as very low, low, fair, and high quality, respectively. In comparative studies, scores ranging from 0 to 6, 7 to 10, 11 to 15, and ≥16 were categorized as very low, low, fair, and high, respectively. 12
In clinical trials, the Cochrane Review Manager tool was used to assess the risk of bias. This tool allows for the assessment of various domains of bias, including randomization, allocation concealment, blinding of participants and outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias. Each domain is evaluated and categorized as having a “low risk of bias,” “uncertain risk of bias,” or “high risk of bias” based on the information provided in the study.
Assessment of Results
Statistical analysis was conducted using the Review Manager 5.4 software. For continuous outcomes, the mean differences with 95% confidence intervals were calculated. Dichotomous outcomes were analyzed using odds ratios (ORs) with 95% confidence intervals. Heterogeneity among studies was evaluated using the Chi2 and I2 tests. I2 values greater than 25%, 50%, and 75% were considered indicative of low, moderate, and high heterogeneity, respectively. A fixed-effects model was used when no significant heterogeneity was detected, whereas a random-effects model was used in the presence of heterogeneity. To extract data from the figures, WebPlotDigitizer version 4.5 was utilized to ensure accurate data acquisition. In cases of missing data, guidelines provided in the Cochrane Handbook were followed to address this issue appropriately. 13
Risk of Bias Across the Studies
Publication bias was assessed using funnel plot asymmetry analysis conducted using Review Manager software. The effect estimate is plotted on the x-axis, while the standard error is plotted on the y-axis. A visual inspection of the funnel plot was performed to examine potential asymmetry, indicating potential publication bias. Formal statistical tests were not performed to assess publication bias.
Additional Analyses
Subgroup analyses were conducted regarding the follow-up time for the VAS and ODI variables to obtain preoperative results at less than 6 months and at more than 6 months.
In the sensitivity analyses, the methodology involved removing studies with the highest weight to evaluate the impact on the results. This approach allows an examination of the robustness and sensitivity of the findings by assessing how the exclusion of influential studies affects the overall outcome.
Results
Study Selection
The initial database search yielded a total of 410 results. After excluding case reports, letters to editors, protocols, duplicates, and studies published less than 10 years ago, 154 studies were removed, resulting in 256 remaining studies. Upon reviewing the titles and abstracts, 217 studies were excluded because they did not focus on endoscopy, utilized tubular endoscopy, or were not centered on the learning curve, leaving 39 studies. After a thorough examination of the full text, 23 studies were eliminated because they did not focus on the learning curve, did not share relevant variables, or contained incomplete or missing data, resulting in 16 studies. No additional studies were included in the reference lists. Ultimately, 16 studies were included in the meta-analysis (Figure 1).5,7,9,10,14-25 Study selection flow diagram (Preferred reporting items for systematic reviews and meta-analyses).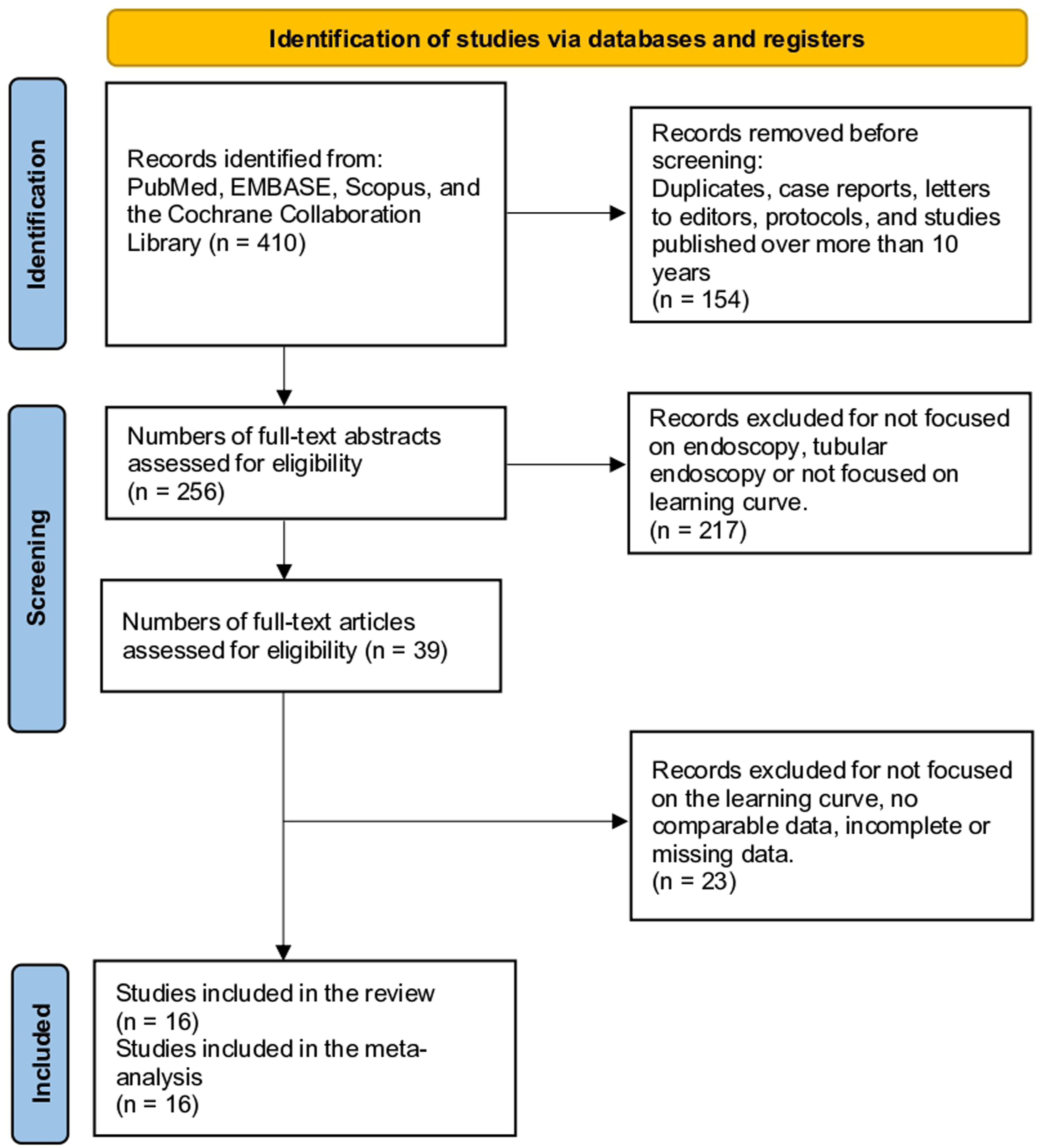
Study Characteristics
Main Baseline Characteristics of the Included Studies.
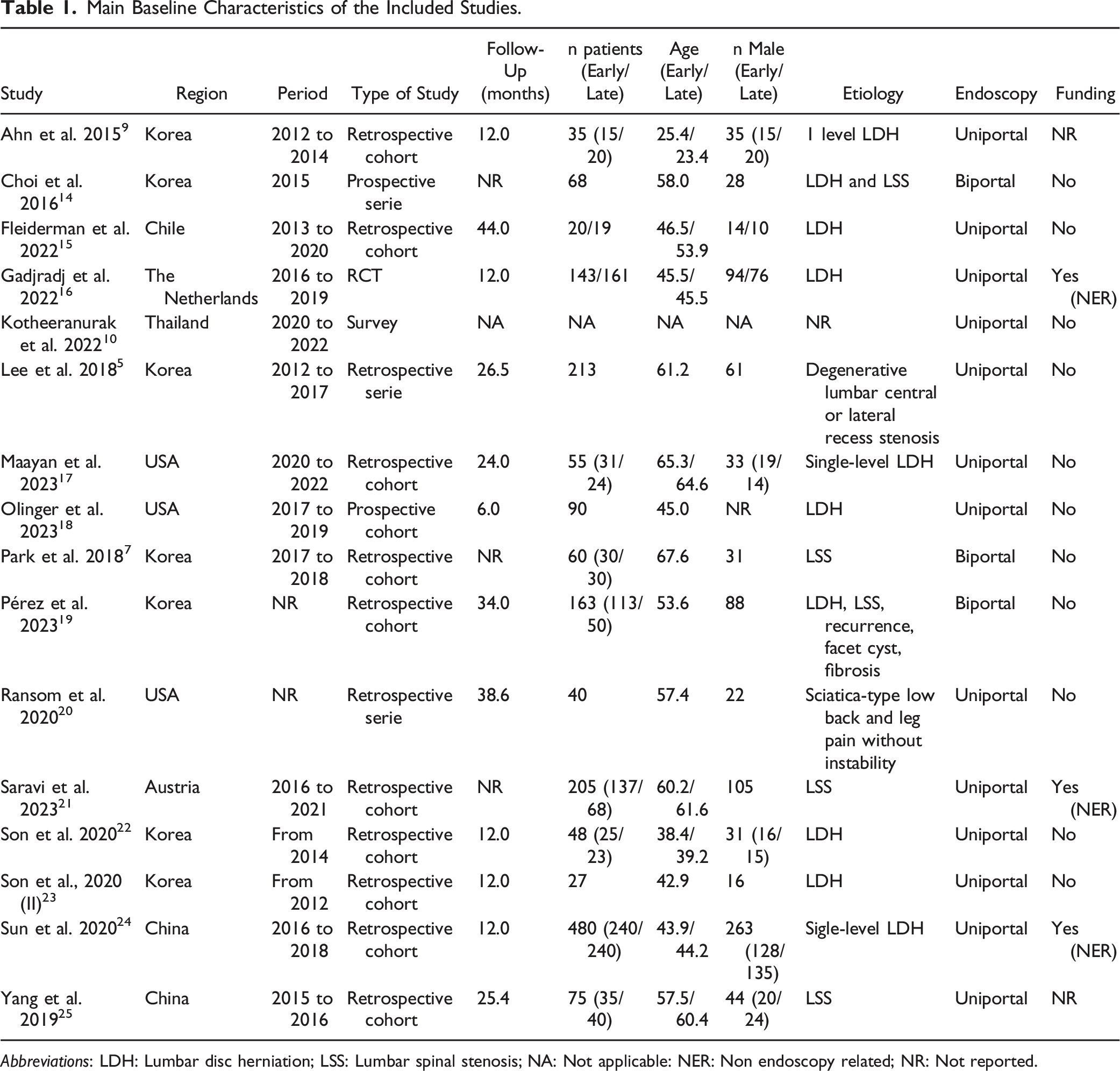
Abbreviations: LDH: Lumbar disc herniation; LSS: Lumbar spinal stenosis; NA: Not applicable: NER: Non endoscopy related; NR: Not reported.
Learning Curve
Learning Curve Based on the Cases Required to Achieve Competence.
Demographic Outcomes
Regarding whether different demographic variables were more frequent in 1 group or another, there were no significant differences in terms of sex (OR 1.03, 95% CI 0.80 to 1.32; participants = 1036; studies = 7; I2 = 0%) (Figure 2A), average age (MD −0.69, 95% CI −2.43 to 1.04; participants = 981; studies = 6; I2 = 7%) (Figure 2B), BMI (MD -0.32, 95% CI −1.19 to 0.55; participants = 1092; studies = 5; I2 = 46%) (Figure 2C), or smoking status (OR 1.37, 95% CI 0.93 to 2.03; participants = 556; studies = 6; I2 = 1%) (Figure 2D). There were also no significant differences in terms of the operation level between the groups (OR 1.21, 95% CI 0.75 to 1.97; participants = 556; studies = 6; I2 = 33%). The duration of symptoms also did not show any significant differences (SMD 0.11, 95% CI −0.02 to 0.25; participants = 832; studies = 3; I2 = 0%). The sensitivity analysis did not result in changes in the direction of the studies. Forest plots showing the comparison between “early” vs “late” surgeons with respect to demographic variables. There were no significant differences in sex (A), age (B), BMI (C), or smoking status (D).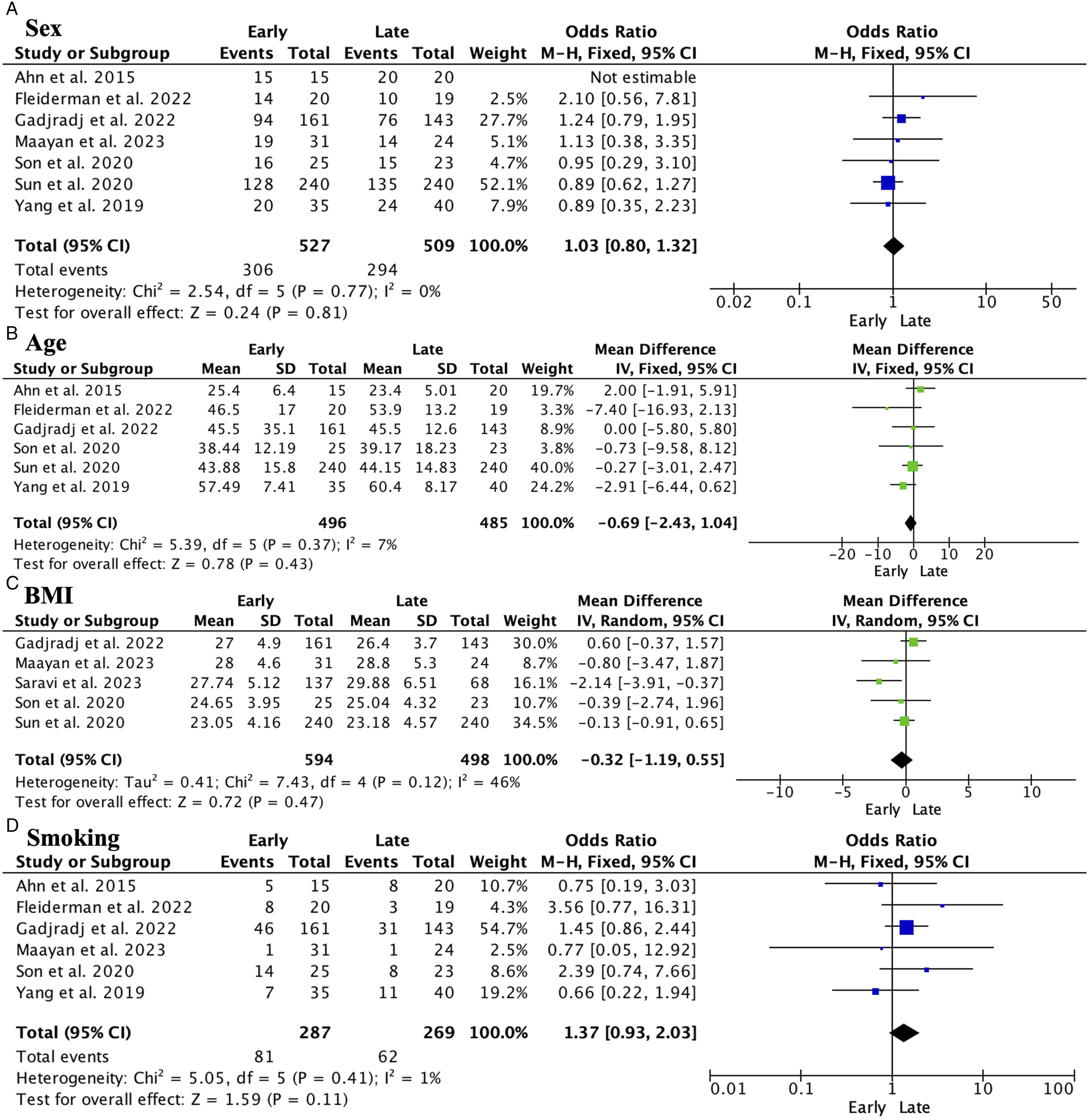
Surgery and Hospitalization Outcomes
The surgery time was significantly shorter in the advanced stage group (MD 28.51, 95% CI 12.19 to 44.83; participants = 1464; studies = 10; I2 = 99%) (Figure 3A). There were no significant differences in terms of stay (LOS) (SMD 0.17, 95% CI −0.03 to 0.36; participants = 443; studies = 5; I2 = 21%) (Figure 3B). Fluoroscopy time was significantly shorter in the advanced group (SMD: 0.54, 95% CI 0.37 to 0.70; participants = 610; studies = 3; I2 = 11%) (Figure 3C). The sensitivity analysis did not result in changes in the direction of the studies. Forest plots showing surgical and hospitalization variables. “Late” surgeons had significantly shorter surgery time (A). There were no significant differences in the length of the hospital stay (B). Fluoroscopy time was significantly shorter in the “late” surgeons (C).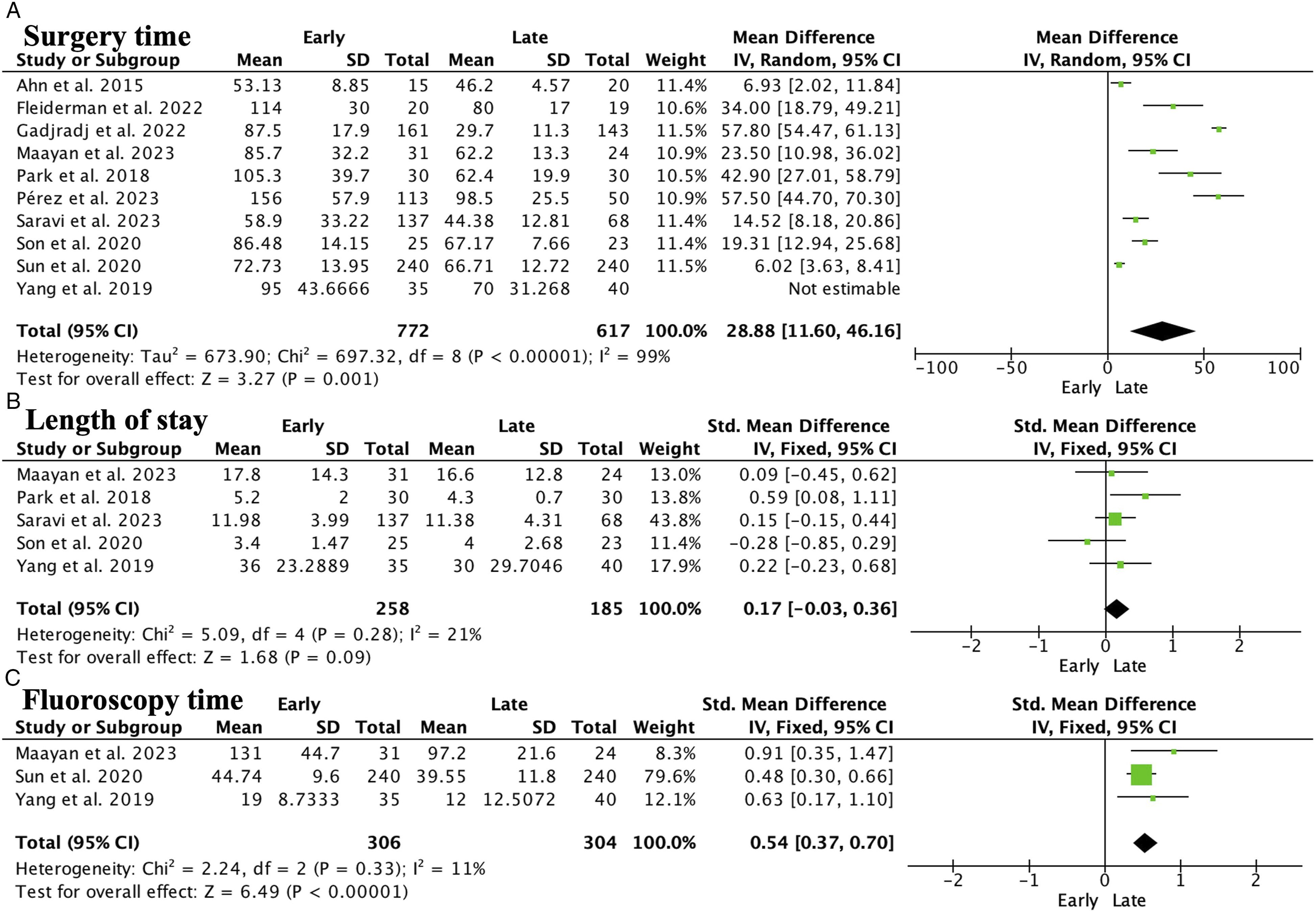
Visual Analogue Scale and Oswestry Disability Index
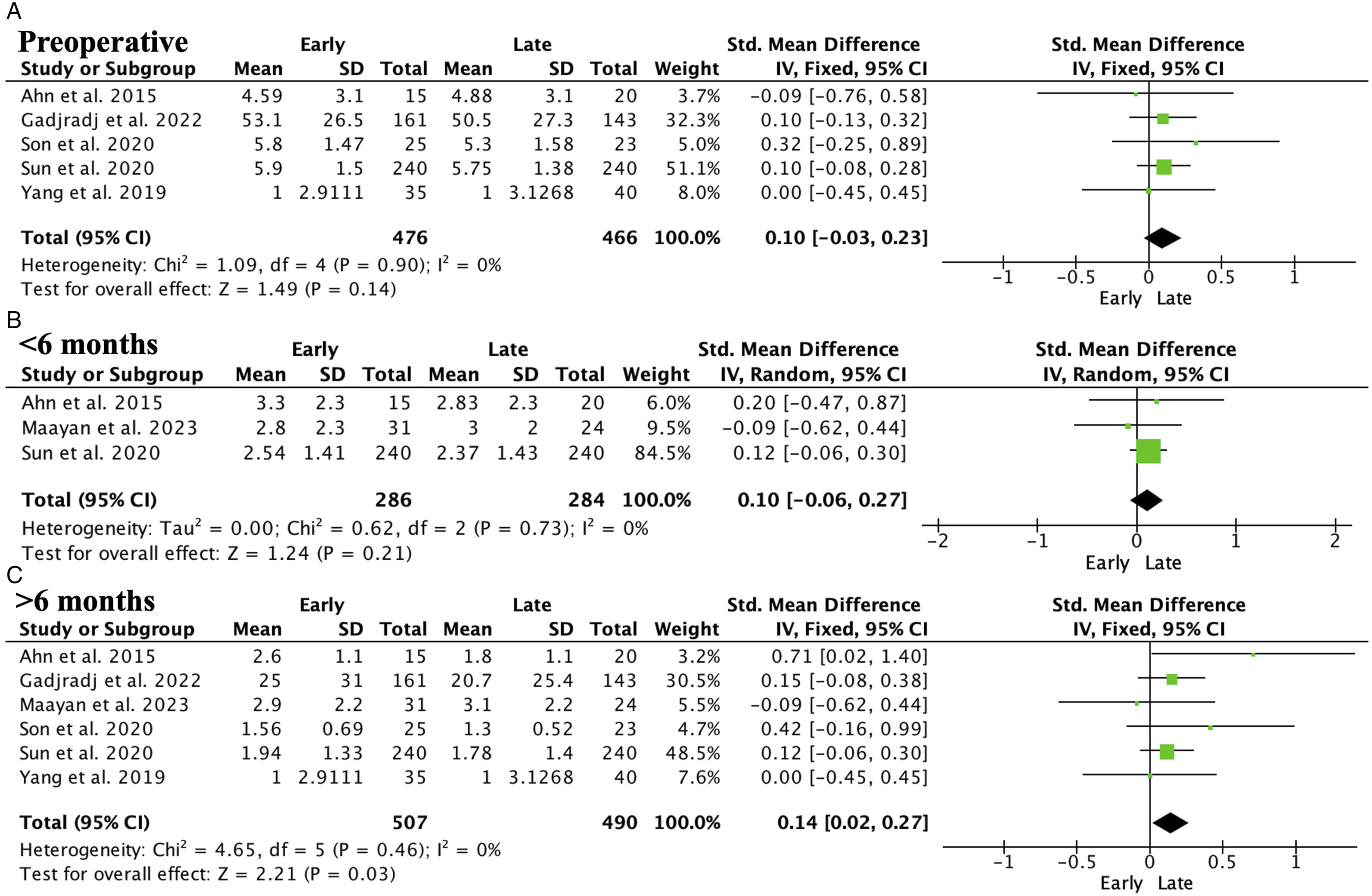
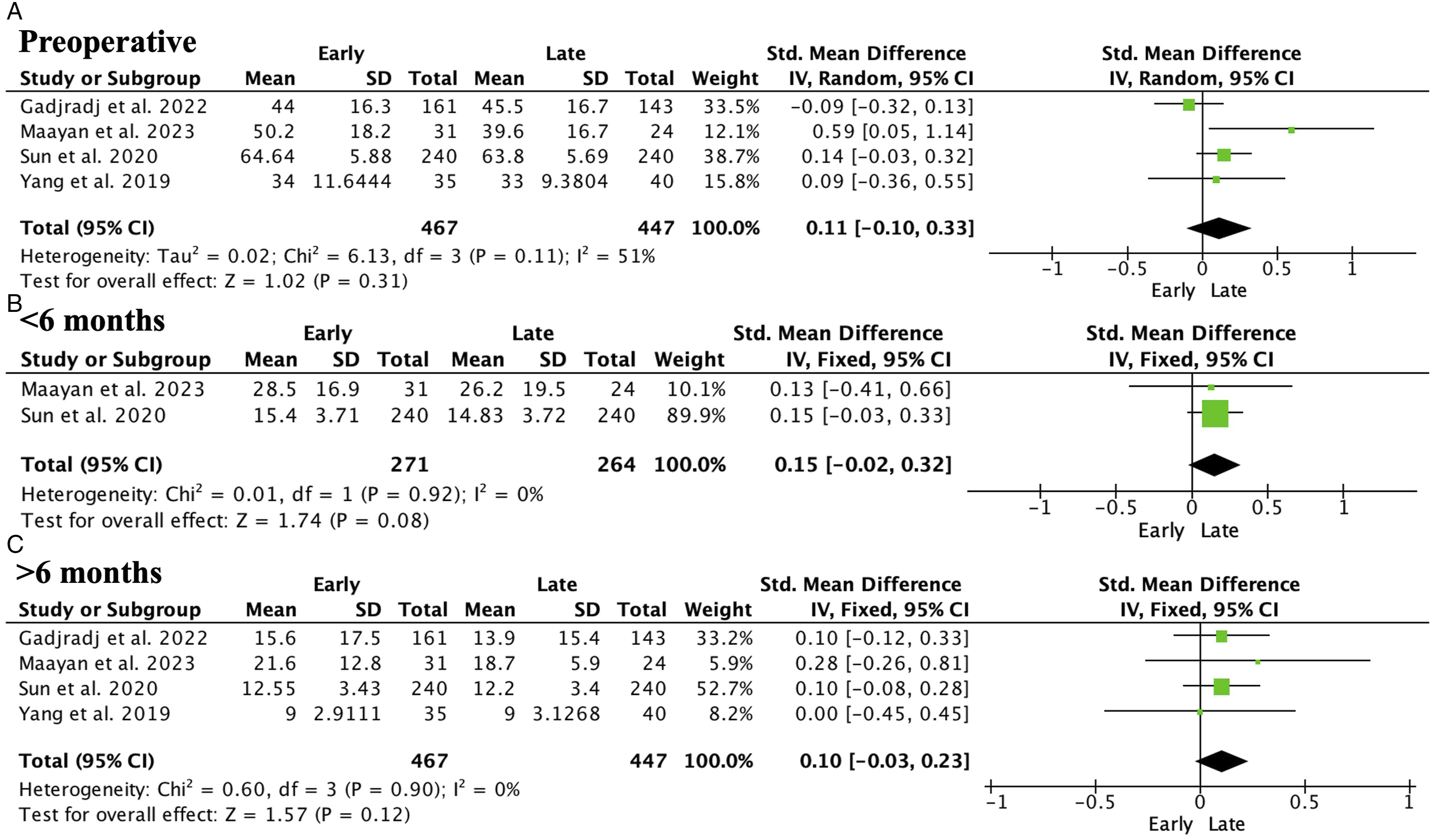
There were no significant differences in preoperative VAS leg pain (SMD 0.10, 95% CI −0.03 to 0.23; participants = 942; studies = 5; I2 = 0%) (Figure 4A). However, the advanced group with more experience showed significantly better outcomes in VAS leg pain at less than 6 months (SMD 0.18, 95% CI 0.01 to 0.34; participants = 570; studies = 3; I2 = 44%) (Figure 4B) and at more than 6 months (SMD 0.14, 95% CI 0.02 to 0.27; participants = 997; studies = 6; I2 = 0%) (Figure 4C). VAS back pain did not show significant differences preoperatively (SMD 0.10, 95% CI −0.03 to 0.23; participants = 942; studies = 5; I2 = 0%) (Figure 5A) or at less than 6 months (SMD 0.10, 95% CI −0.06 to 0.27; participants = 570; studies = 3; I2 = 0%) (Figure 5B). However, at more than 6 months, the group with more experience showed significantly better results (SMD 0.16, 95% CI 0.04 to 0.29; participants = 997; studies = 6; I2 = 23%) (Figure 5C). The sensitivity analysis revealed inconsistencies in the VAS leg pain results but not in the VAS back pain results. In contrast, the preoperative Oswestry Disability Index (ODI) did not show significant differences (SMD 0.11, 95% CI −0.10 to 0.33; participants = 914; studies = 4; I2 = 51%) (Figure 6A). There were no significant differences at less than 6 months (SMD 0.15, 95% CI -0.02 to 0.32; participants = 535; studies = 2; I2 = 0%) (Figure 6B) or >6 months (SMD 0.10, 95% CI −0.03 to 0.23; participants = 914; studies = 4; I2 = 0%) (Figure 6C). Sensitivity analysis did not change the direction of the studies. Forest plots showing VAS leg pain. Late surgeons showed no significant differences preoperatively (A), but instead showed significantly better results at less than 6 months (B) and >6 months (C). Forest plots showing VAS back pain. Late surgeons showed no significant differences preoperatively (A) or at less than 6 months (B) but showed significantly less pain at more than 6 months (C). Forest plot showing ODI. There were no significant differences preoperatively (A), at less than 6 months (B), or at > 6 months (C).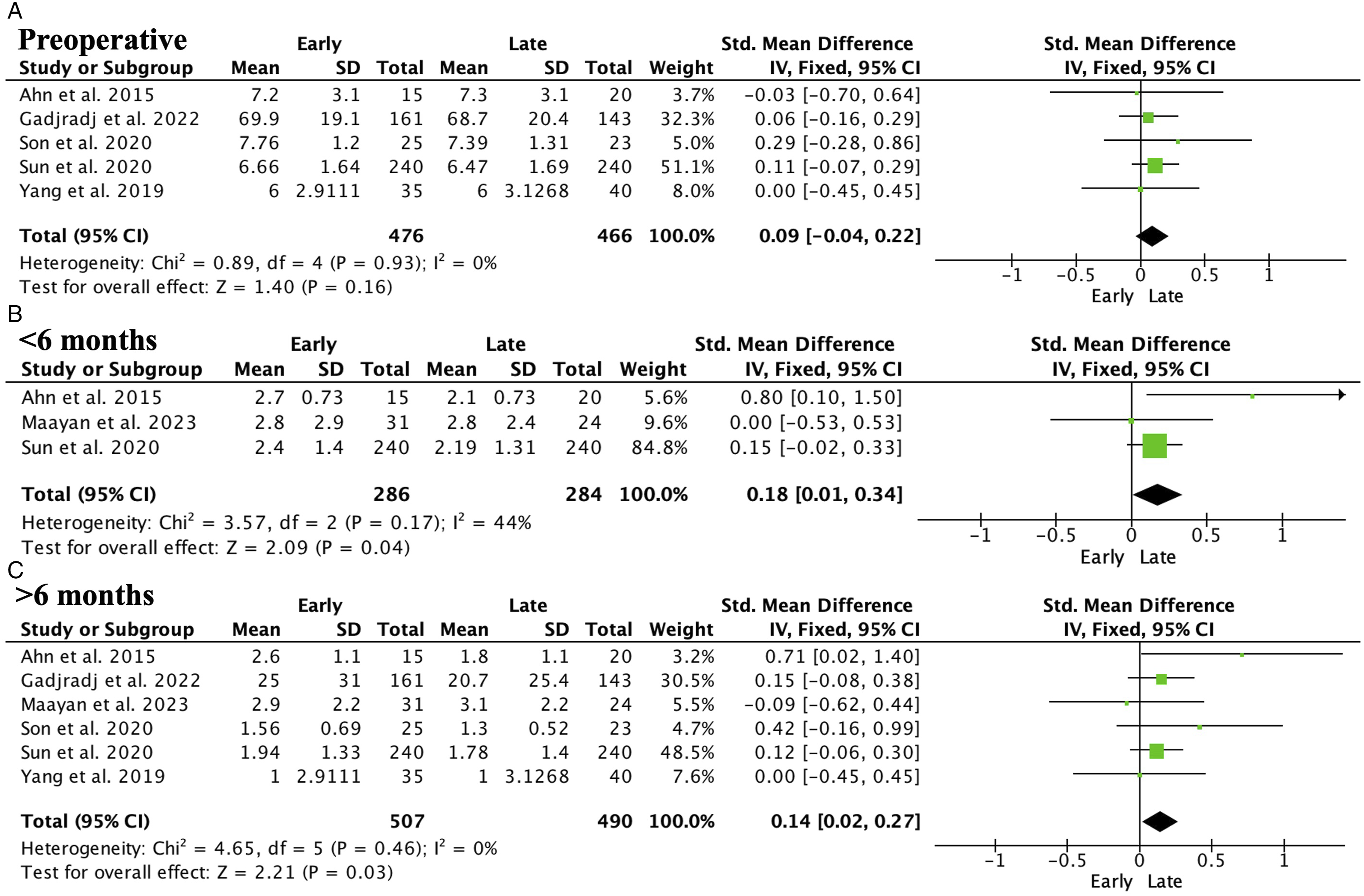
Complications
Complications.
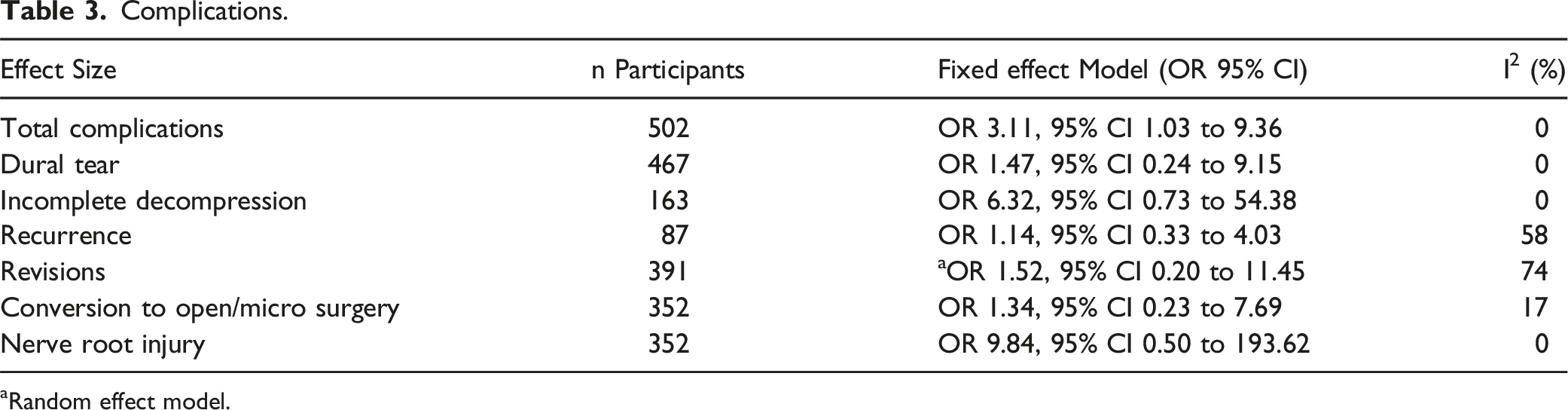
aRandom effect model.
Publication Bias
No publication bias was observed in the main variables (Figure 7). Funnel plot assessing publication bias.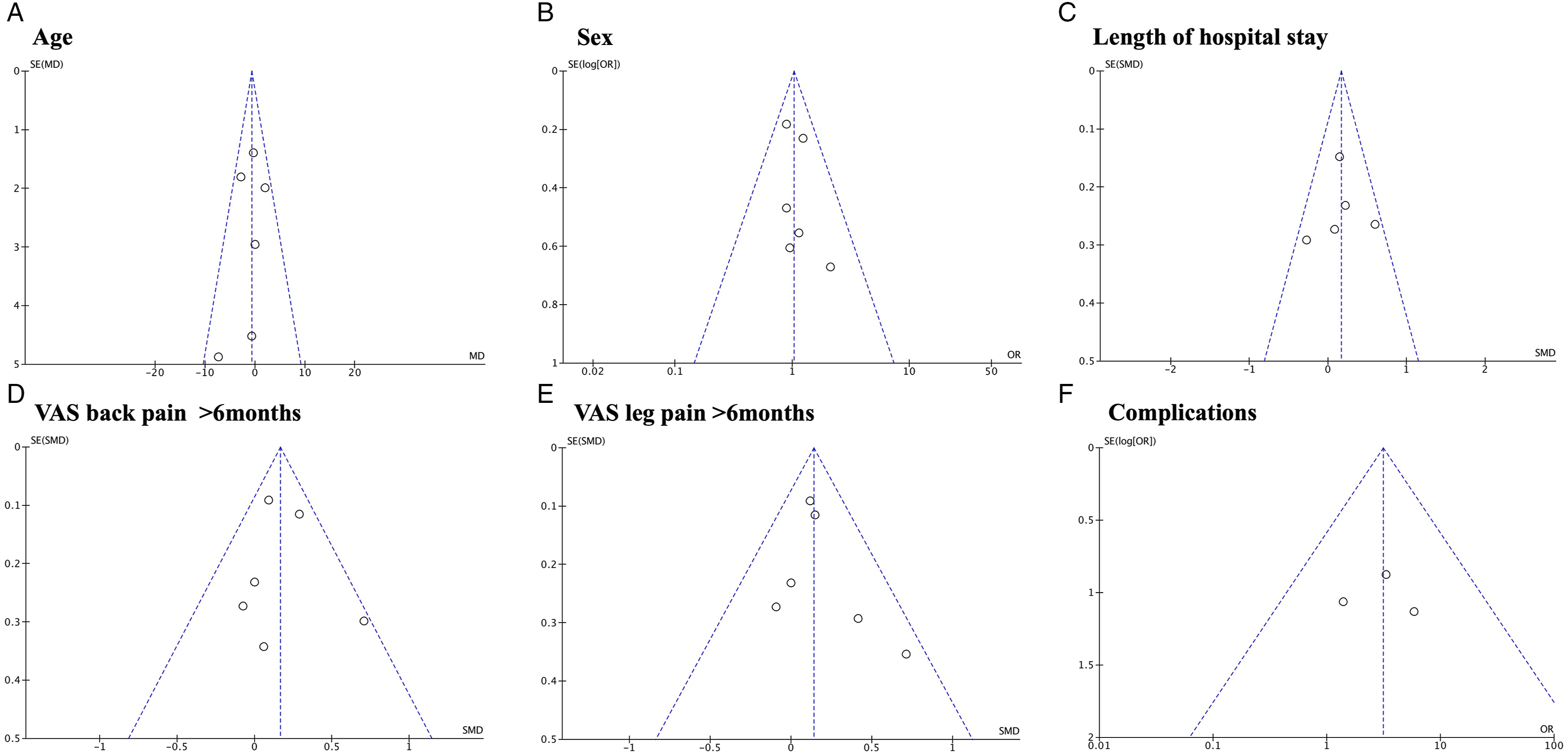
Discussion
This study analyzed the learning curve of endoscopic spinal surgery and compared the results between groups with different levels of experience. The uniportal technique required fewer cases to acquire experience. In addition, the group with more experience had shorter surgical times and better results in terms of pain. The less experienced group had a higher overall incidence of complications. It is important to highlight that all but 2 of the studies, which did not report their funding, were conducted without any financial support from the industry.
According to the literature, a learning curve was observed in other minimally invasive techniques, such as unilateral microscopic laminectomy surgery, with an average of approximately 29 cases required to acquire experience. 26 Minimally invasive surgery (MIS) techniques generally require 20-30 cases to reach the learning curve, highlighting the importance of proper case selection during the initial period. 27 In the transforaminal lumbar interbody fusion (TLIF) technique, approximately 31.3 cases were required to reach the learning curve. 28 Compared to data reported in the literature on microscopic surgery, our study found a similar learning time to achieve mastery in endoscopic surgery.29,30
The evolution of uniportal endoscopic surgery has been remarkable, with significant advancements in the development of specialized instruments and enhanced transfer of experience from master’s to trainee. This increased experience and technological improvements have contributed to a considerable reduction in the learning curve of the surgeons. In comparison, biportal surgery has also made progress, but it has a shorter history and less accumulated experience than uniportal surgery. However, it is important to note that biportal surgery has been primarily indicated for cases of spinal canal stenosis, a more challenging pathology to manage than hernias, which have been more commonly treated with uniportal surgery according to original studies.
This study focused on the last 10 years of research on the learning curve of endoscopic spinal surgery. When examining studies spanning a longer period of time, it was found that this learning curve can extend up to case number 72, according to a study by Morgenstern et al in 2007. 31 Additionally, another study conducted by Hsu et al in 2013 identified that approximately 33 cases were required to reach the learning curve. 32 It is important to note that this study specifically focused on endoscopic lumbar spinal surgery. However, when considering studies that focused on the cervical spine, a slightly lower learning curve was observed, with an average of 20-28 cases, according to the limited available studies.3,33
Overall, significantly higher complications were observed in the group of surgeons with less experience than in the group of experienced surgeons, although the complication rates were low in both groups (5% vs 2%, respectively). Existing complications, such as incidental dural tears or nerve root injuries, were mostly mild and did not have negative consequences for the patients. No significant differences were found in other complications, although their frequency was very low, and the statistical power to detect differences may be limited owing to the small sample size and the lack of inclusion of these variables in most studies. It is important to highlight the significance of meta-analysis in evaluating complications, as individual articles present low complication rates, but when combined, the power of the analysis increases. However, the complication rate was significantly lower in the experienced surgeons group. However, no significant differences were observed regarding specific complications separately, probably because of the small sample size, as few studies included these variables. In addition, novice surgeons may encounter challenges when it comes to identifying and fully removing structures such as the contralateral ligamentum flavum or structures in the proximal region during endoscopic spinal surgery. These findings emphasize the significance of establishing a proper learning curve and the importance of thorough training and education to minimize complications associated with this technique. It is worth noting that within the first 100 endoscopies, a failure rate of approximately 10% has been observed, including instances of residual disc fragments leading to early reherniation and requiring reintervention. 34
In this study, significant differences were found in terms of visual analog scale (VAS) pain scores less than or more than 6 months after endoscopic spinal surgery. These differences may be attributed to longer operative times or more intense manipulation of the nerve root during surgery, as surgeons need to familiarize themselves with the anatomy to achieve better visualization. 35 Another approach used by some surgeons is the application of lidocaine to the disc annulus at a volume of 1-2 cm³ to alleviate pain. 6 However, in our study, no significant differences were found in terms of symptomatology measured by the VAS scale and Oswestry Disability Index (ODI) at the preoperative level between the surgeon groups. It is possible that patients with more pronounced symptoms should be operated upon by surgeons with more experience, taking this into account. Additionally, no significant differences were observed in the symptom duration between the groups. However, experienced surgeons were able to significantly reduce pain compared with surgeons in the early stages of their training. However, no significant differences were found in terms of ODI, which assesses function. This could indicate that patients operated on by less experienced surgeons experienced more pain; however, this pain did not significantly affect their ability to perform daily activities.
Recommendations for Beginners in Endoscopic Spine Surgery.
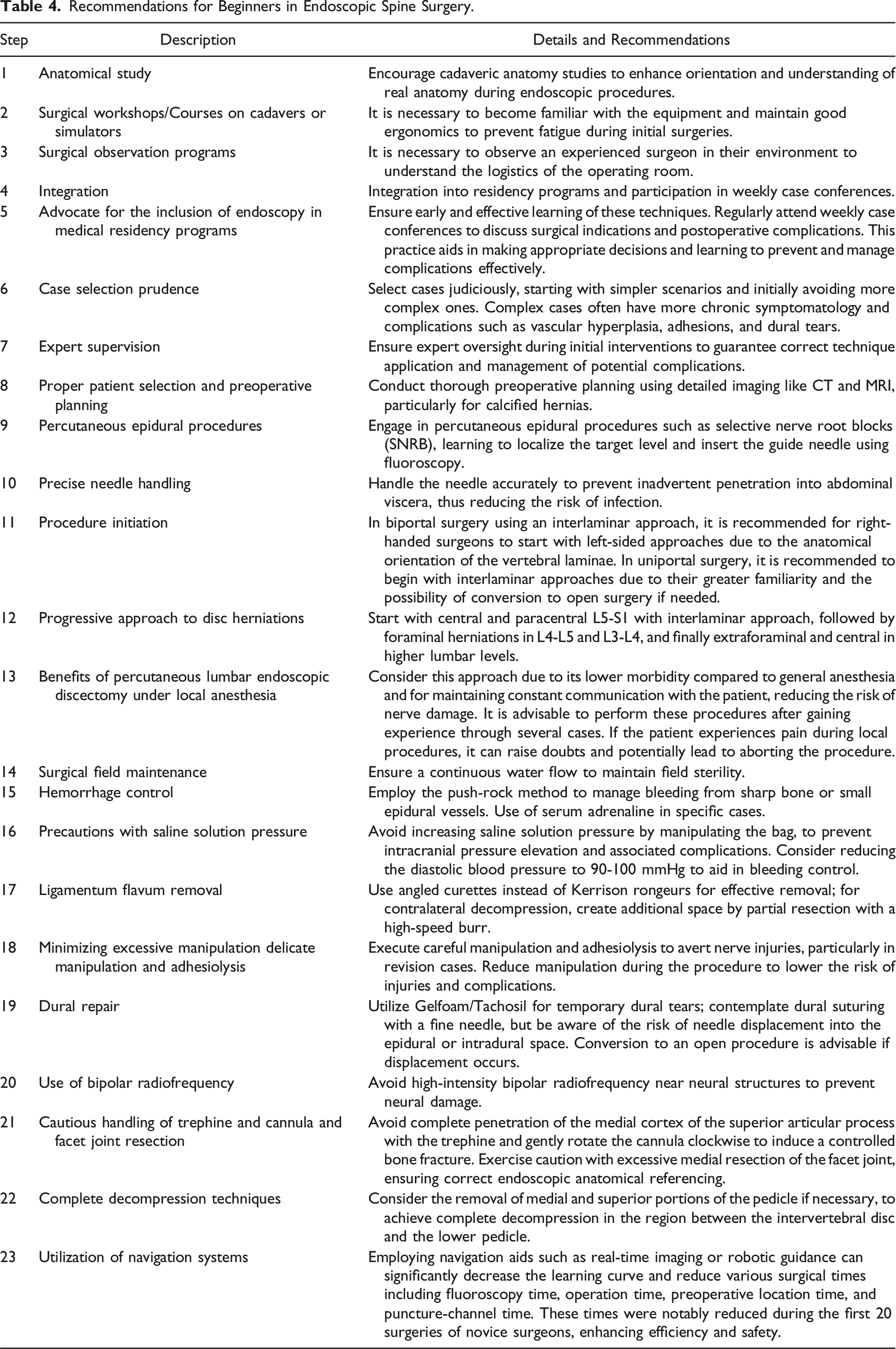
The use of navigation systems significantly reduces the learning curve and decreases various surgical times, including fluoroscopy, operation, preoperative localization, and puncture channel times. These times were notably reduced during the first 20 surgeries performed by surgeons. 36 Fluoroscopy and initial puncture can be challenging due to various logical factors, but navigation helps define the trajectory. Accurate needle insertion is crucial for avoiding nerve and blood vessel damage. The navigation system assisted in predefining the trajectory, resulting in a 36.11% reduction in puncture channel time, a 17.01% reduction in operation time, and a 34.09% reduction in fluoroscopy times.
When interpreting the study findings, it is important to acknowledge potential biases that could affect the results. For example, the possibility of complex cases being reserved for open surgery may overestimate the learning curve and underestimate the duration. However, the study found no significant differences between experienced and novice surgeons in terms of preoperative VAS or ODI scores, symptom duration, or patient age, indicating that case complexity did not differ between the groups. It is also important to consider the obstacles identified in endoscopy, as a survey conducted in Thailand revealed that personal motivations and lack of support are common challenges. 10 Furthermore, surgical time can be a valuable measure of competence as it can impact efficacy and safety variables. 38 Therefore, it is important to consider that novice surgeons may take longer during surgery, which could contribute to the lack of differences in certain complications observed in some studies.
This study had some important limitations that should be considered when interpreting the results. First, efforts were made to standardize the follow-up times among the included studies; however, there were still variations in the duration of these periods. Additionally, the limited number of available studies for many analyzed variables made it challenging to perform subgroups and divisions to assess the influence of factors, such as case etiology, techniques used, and learning times. Also, our analysis did not categorize outcomes based on different etiologies nor did they consistently differentiate outcomes between uniportal and biportal. As such, variations in surgical time and complications related to the extent of decompression were not directly comparable. Recognizing this limitation is crucial, as it highlights the need for future research to systematically address these distinctions to enhance the comparability and applicability of the study findings. Another significant limitation was the presence of different definitions of the learning curve in various articles, with some studies using longer periods and others using shorter periods. Another limitation was the lack of differentiation between the interlaminar and transforaminal techniques within the uniportal approach, as well as the lack of distinction between the paraespinal and interlaminar methods in the biportal approach. However, it is essential for an endoscopic spine surgeon to be proficient in all these techniques to ensure comprehensive clinical competency. Furthermore, the heterogeneity in case etiologies may also have influenced the results, making a more precise and detailed comparison difficult.
Conclusions
According to the study results, it was determined that, on average, 32.5 cases are required to reach the learning curve in endoscopic spine surgery, with a minimum range of 18 cases and a maximum of 50 cases. The uniportal technique was found to require a lower number of cases to gain experience, followed by the biportal technique. Additionally, as surgeons gained more experience, improvements were seen in surgical outcomes, such as shorter surgery times, reduced fluoroscopy time, and better results in terms of leg and back pain both in the short and long term. It was also found that the group with less experience had a significantly higher incidence of complications than the more experienced group. These findings are highly relevant for spine surgeons performing endoscopic surgery as they provide valuable information about the number of cases needed to achieve an optimal learning curve in this technique. Knowing the approximate number of cases required to reach this learning curve can assist surgeons in planning their training and developing realistic expectations regarding their progress in the endoscopic spine technique.
Supplemental Material
Supplemental Material - Meta-Analysis of Learning Curve in Endoscopic Spinal Surgery: Impact on Surgical Outcomes
Supplemental Material for Meta-Analysis of Learning Curve in Endoscopic Spinal Surgery: Impact on Surgical Outcomes by Juan Álvarez de Mon-Montoliú, Juan Castro-Toral, César Bonome-González, and Manuel González-Murillo in Global Spine Journal
Supplemental Material
Supplemental Material - Meta-Analysis of Learning Curve in Endoscopic Spinal Surgery: Impact on Surgical Outcomes
Supplemental Material for Meta-Analysis of Learning Curve in Endoscopic Spinal Surgery: Impact on Surgical Outcomes by Juan Álvarez de Mon-Montoliú, Juan Castro-Toral, César Bonome-González, and Manuel González-Murillo in Global Spine Journal
Footnotes
Author Contributions
Conception and design: J.A.d.M.-M., J.C.-T.., C.B.-G., M.G.-M.; Analysis and interpretation of the data: J.A.d.M.-M., J.C.-T.., C.B.-G., M.G.-M.; Drafting of the article: J.A.d.M.-M., J.C.-T.., C.B.-G., M.G.-M.; Critical revision of the article for important intellectual content: J.A.d.M.-M., J.C.-T.., C.B.-G., M.G.-M.; Final approval of the article: J.A.d.M.-M., J.C.-T.., C.B.-G., M.G.-M.; Statistical expertise: J.A.d.M.-M. and M.G.-M.; Obtaining of funding: N/A.; Administrative, technical, or logistic support: N/A.; Collection and assembly of data: J.A.d.M.-M., J.C.-T.., C.B.-G., M.G.-M.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.