
Abstract
Study Design
Systematic Review.
Objective
This meta-analysis systematically evaluates the safety and effectiveness of endoscopic techniques in the treatment of lumbar disc herniation (LDH).
Methods
A comprehensive computerized search was conducted on PubMed, Embase, Cochrane Library, China National Biomedical Literature Database (CBM), VIP Database, China National Knowledge Infrastructure (CNKI) and Wanfang Database. Randomized controlled trials (RCTs) comparing endoscopic techniques with non-endoscopic techniques for the treatment of LDH were identified. Meta-analysis was performed using RevMan 5.4 software.
Results
Seventeen RCTs involving 1748 LDH patients were analyzed. The meta-analysis revealed that, compared to the non-endoscopic discectomy (NED) group, the endoscopic discectomy (ED) group exhibited significantly lower intraoperative blood loss [MD = −74.45 mL, 95% CI (−124.88, −24.02), P = .004], shorter hospitalization duration [MD = −4.07 days, 95% CI (−6.67, −1.48), P = .002], lower Visual Analogue Scale (VAS) pain scores at the last follow-up [MD = −.35, 95% CI (−.63, −.07), P = .01], and a lower incidence of complications [RR = .35, 95% CI (.25, .48), P < .00001]. Moreover, the ED group exhibited a higher ratio of excellent and good therapeutic effects postoperatively [RR = 1.05, 95% CI (1.01, 1.10), P = .01]. However, there were no statistically significant differences between the 2 groups in terms of the Oswestry Disability Index (ODI) scores at the last follow-up [SMD = −.49, 95% CI (−1.14, .17), P = .14] and operation time [MD = −10.17 min, 95% CI (−27.05, 6.71), P = .24].
Conclusion
Endoscopic techniques in the treatment of LDH exhibit significant superiority in intraoperative blood loss, hospitalization duration, postoperative pain, complication rates, and postoperative therapeutic effects. This provides patients with a safer and more effective treatment option.
Introduction
In the field of spinal medicine, LDH has attracted considerable attention as a prevalent intervertebral disc disorder. The complexity of its symptoms and its notable impact on patients’ quality of life make the search for more effective and safe treatment methods an urgent need.1-3 In recent years, the development of minimally invasive techniques has provided a new approach to the treatment of LHD, with endoscopic surgery being a representative technology that has attracted widespread attention. With the application of endoscopic techniques, the medical community has shown a keen interest in their superiority in the treatment of LHD. Compared to traditional surgical methods, endoscopic surgery is believed to reduce surgical trauma, shorten recovery time, and thereby enhance the overall treatment experience for patients.4-6 However, existing research conclusions regarding the differences in treatment outcomes between endoscopic and non-endoscopic techniques are inconsistent. While some studies have conducted related meta- analysis,7-10 these analyses only included English literature and involved non-randomized controlled trials, potentially limiting the reliability and generalizability of the results. Against this research backdrop, we conducted the current meta-analysis. Through a comprehensive search of both English and Chinese RCTs, we compared endoscopic techniques with non-endoscopic techniques on key indicators such as intraoperative blood loss, operation time, hospitalization duration, VAS pain scores at the last follow-up, ODI scores at the last follow-up, complication rates, and the ratio of excellent and good therapeutic effects postoperatively. We systematically and comprehensively assessed the safety and effectiveness of endoscopic techniques in treating LHD, utilizing the GRADE system to evaluate the outcome indicators. The aim is to provide a safer and more effective treatment option for patients with LHD and to guide the further development of minimally invasive techniques in this field.
Material and Methods
This systematic review was executed and reported in accordance with the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Protocols. 11 The registration code assigned to this review is INPLASY2022410095.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Study Participants: Patients definitively diagnosed with LHD, aged 18 years or older, and of any gender. (2) Intervention: The experimental group received treatment for LHD using endoscopic techniques, while the control group underwent non-endoscopic treatments, such as traditional open surgery. (3) Study Design: RCTs, with publications in either Chinese or English. (4) Outcome indicators: intraoperative blood loss, operation time, hospitalization duration, VAS pain scores at the last follow-up, ODI scores at the last follow-up, complication rates, and the ratio of excellent and good therapeutic effects postoperatively. The complications considered in this study include: nerve root injury, vascular injury, postoperative infection, cerebrospinal fluid leakage, spinal cord injury, lumbar deformation, aggravated pain, and dystasia.
Exclusion Criteria
(1) Non-RCTs; (2) Non-clinical research literature; (3) Literature not in Chinese or English; (4) Review articles or studies classified as systematic reviews; (5) Studies focusing on recurrent LHD; (6) Literatures for which the full text is inaccessible or data extraction is not feasible.
Retrieval Strategy
We conducted a computerized search of PubMed, Embase, Cochrane Library, CBM, VIP Database, CNKI and Wanfang Database. The search terms included LHD, percutaneous transforaminal endoscopic discectomy, percutaneous endoscopic lumbar discectomy, percutaneous endoscopic transforaminal discectomy, percutaneous endoscopic interlaminar discectomy, full-endoscopic transforaminal lumbar discectomy, full-endoscopic interlaminar lumbar discectomy, randomized controlled trial, and RCT. The search period extended from the inception of the databases to December 25, 2023. Additionally, we retrieved references from the included literature to identify potentially relevant studies that met the inclusion criteria.
Literature Screening and Data Extraction
Two researchers independently conducted literature screening and data extraction in accordance with the inclusion and exclusion criteria. In case of discrepancies, these were resolved through discussion or consultation with a third party. Extracted data included the first author, publication year, country, sample size, age, surgical methods, time of follow-up and outcome indicators.
Quality Assessment
The quality of the included studies was evaluated using the Cochrane 5.1.0 bias risk assessment tool. This tool assesses 7 aspects, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other sources of bias. Each criterion was judged and categorized as high risk of bias, low risk of bias, or unclear. 12
Statistical Analysis
Meta-analysis was conducted using RevMan 5.4 statistical software. For categorical data, risk ratios (RR) with 95% confidence intervals (CI) were employed, while continuous data were expressed as mean differences (MD) or standardized mean differences (SMD) with their corresponding 95% CIs. Heterogeneity among studies was assessed using the χ2 test, and when no statistically significant heterogeneity was observed (I2 ≤ 50%), a fixed-effects model was applied. In cases of substantial heterogeneity among studies (I2 > 50%), a random-effects model was utilized. 13 In instances where significant heterogeneity was identified, and after confirming the accuracy of data extraction, subgroup analysis or sensitivity analysis was performed to identify the source of heterogeneity. If the source of heterogeneity could not be determined or if studies could not be quantitatively pooled, a descriptive analysis was conducted. Egger’s test was employed to assess publication bias for indicators with more than ten included studies. 14 A P-value less than .05 was considered statistically significant.
Quality Assessment of Evidence
The GRADEprofiler 3.6 was employed to assess the quality of evidence for each outcome indicator. Results were categorized into 4 levels: high, moderate, low, and very low based on 5 aspects, including the risk of bias, consistency, indirectness, imprecision, and publication bias. 15
Results
Literature Retrieval Results
Characteristics of the Studies Included in This Meta-Analysis.
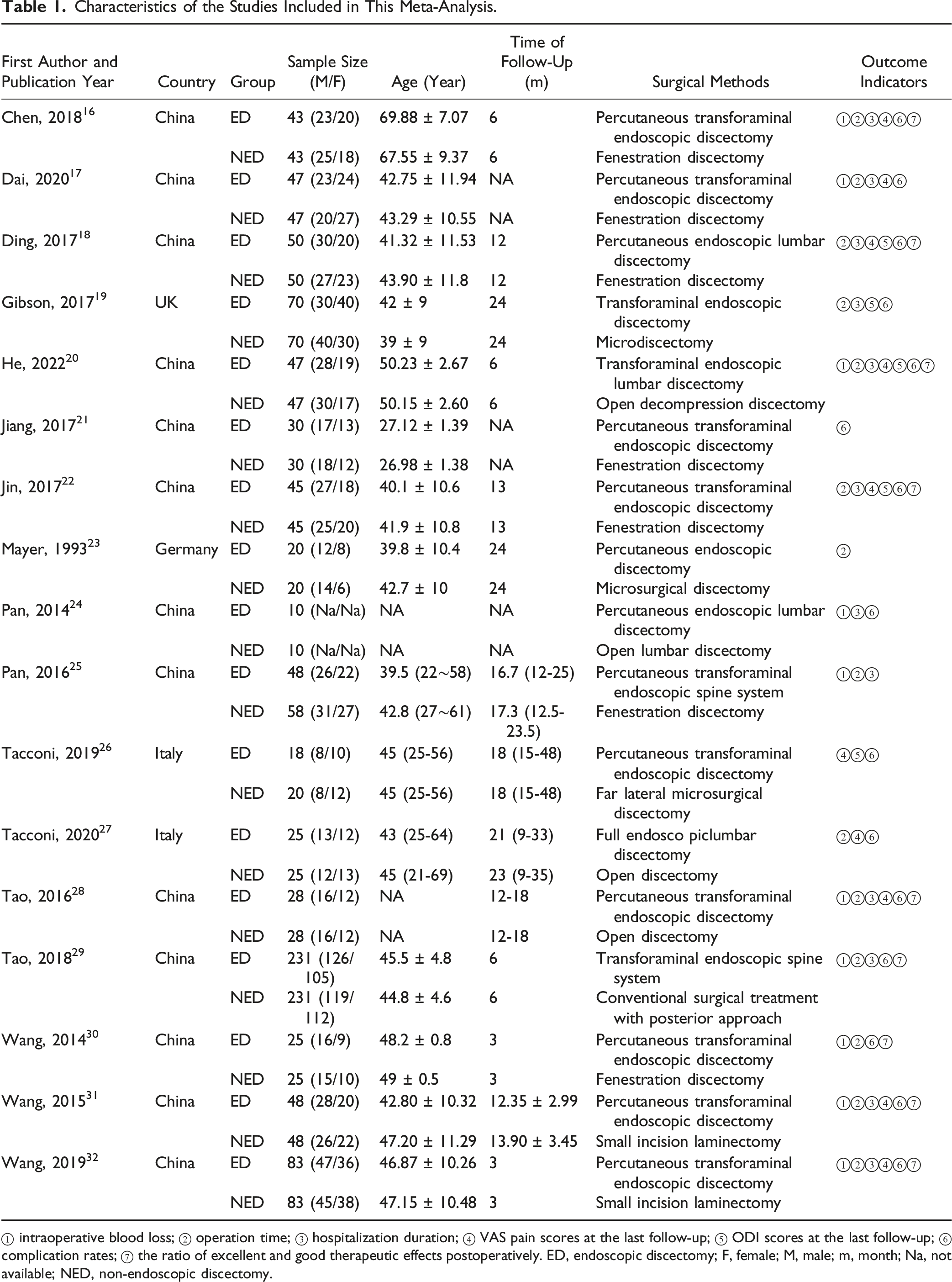
① intraoperative blood loss; ② operation time; ③ hospitalization duration; ④ VAS pain scores at the last follow-up; ⑤ ODI scores at the last follow-up; ⑥ complication rates; ⑦ the ratio of excellent and good therapeutic effects postoperatively. ED, endoscopic discectomy; F, female; M, male; m, month; Na, not available; NED, non-endoscopic discectomy.
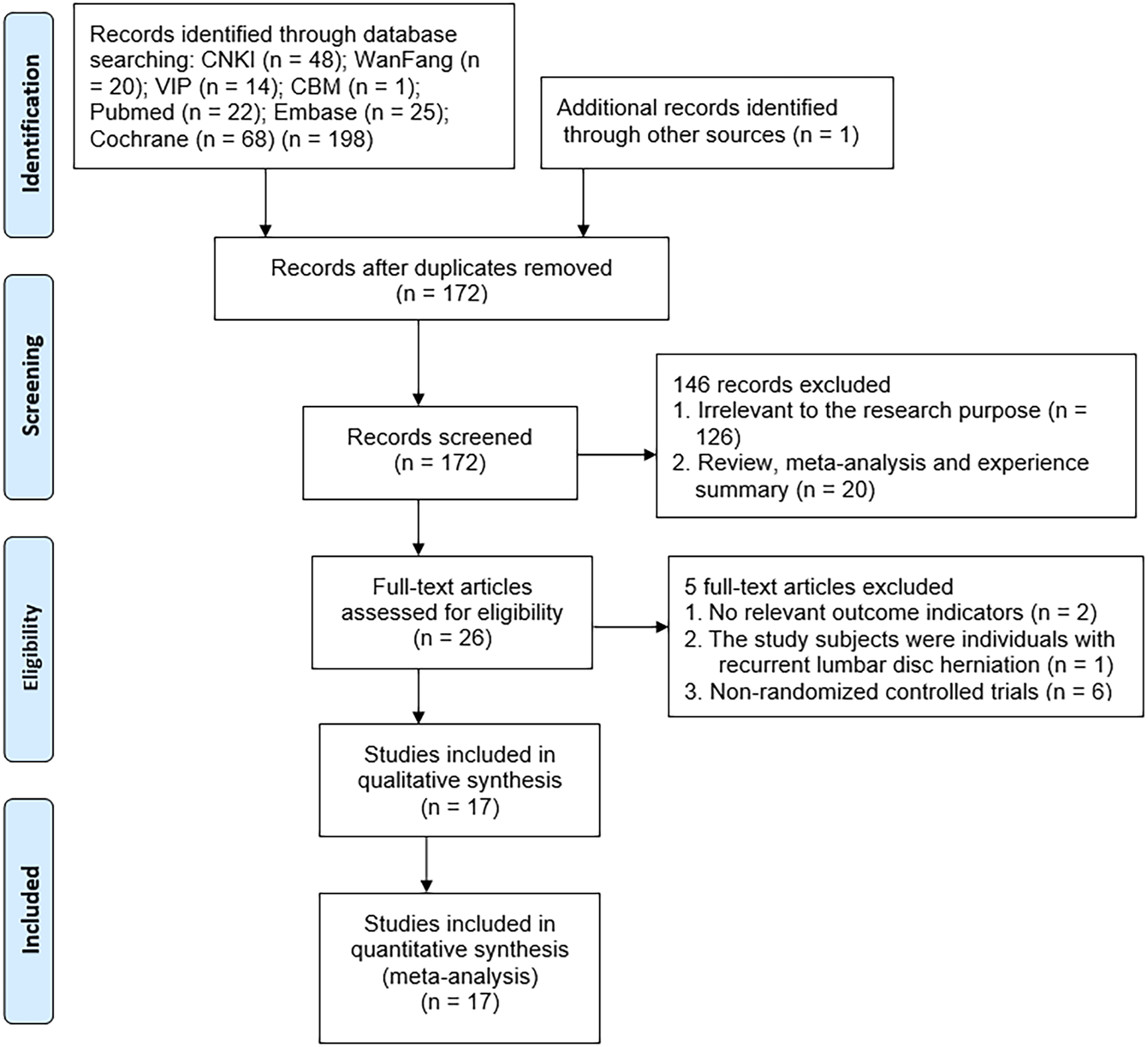
Study selection.
Results of Literature Quality Assessment
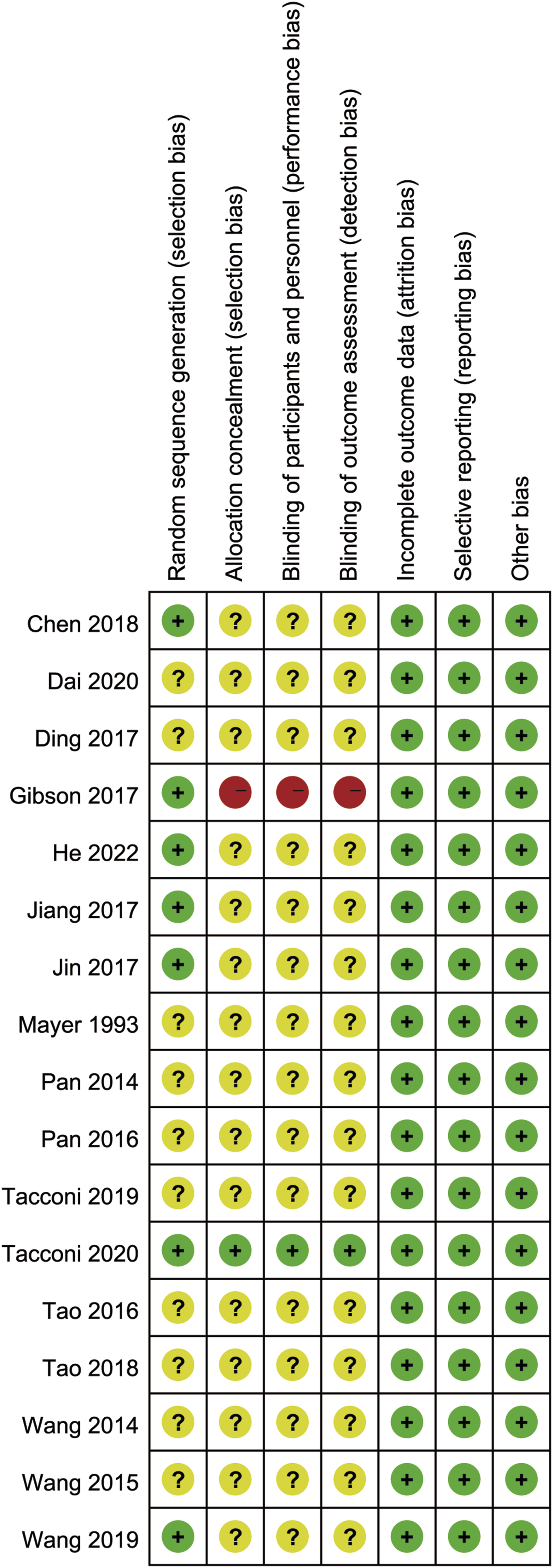
All 17 studies were RCTs.16-32 Among them, 7 studies16,19-22,27,32 described the randomization methods used. One study
27
utilized concealed allocation, implemented blinding for both participants and implementers, and employed blinding for outcome ssessors. No studies exhibited missing outcome data, selective outcome reporting, or other biases. As shown in Figures 2 and 3. Risk of bias graph for RCTs included in this study. Summary of the risk of bias analysis for the RCTs included in this study.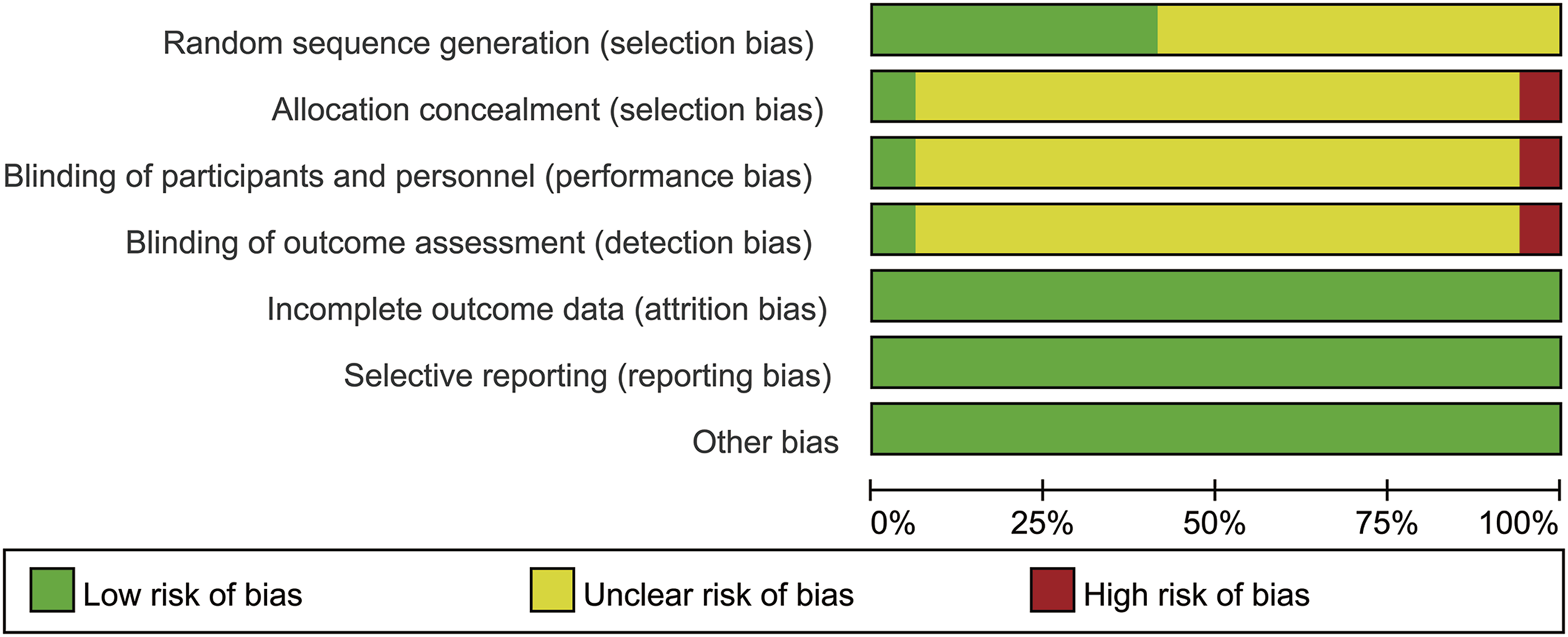
Meta Analysis Results
Intraoperative Blood Loss
Ten studies16,17,20,24,25,28-32 (1230 patients with LHD) reported intraoperative blood loss. The mean intraoperative blood loss in the ED group was 21.99 mL, while in the NED group it was 148.05 mL. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 100%). A random-effects model was employed to combine the effect sizes for the meta-analysis, revealing that the ED group had significantly less intraoperative blood loss compared to the NED group [MD = −74.45 mL, 95% CI (−124.88, −24.02), P = .004]. Based on the different endoscopic surgical techniques within the experimental group, we divided the studies into the Percutaneous Transforaminal Endoscopic Discectomy (PTED) subgroup and other ED subgroup. Six studies in the PTED subgroup16,17,28,30-32 (548 patients with LHD) reported intraoperative blood loss. The mean intraoperative blood loss in the ED group was 29.29 mL, while in the NED group it was 85.04 mL. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 95%). A random-effects model was used to combine the effect sizes for the meta-analysis, indicating that the ED group had significantly lower intraoperative blood loss than the NED group [MD = −51.20 mL, 95% CI (−61.93, −40.46), P < .00001]. Sensitivity analysis, conducted by systematically excluding each study, demonstrated that the direction of the combined effect sizes remained consistent, suggesting the stability of the subgroup results. Four studies in the other ED subgroup20,24,25,29 (682 patients with LHD) reported intraoperative blood loss. The mean intraoperative blood loss in the ED group was 16.04 mL, while in the NED group it was 173.58 mL. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 100%). A random-effects model was utilized to combine the effect sizes for the meta-analysis, revealing no statistically significant difference in intraoperative blood loss between the ED group and the NED group [MD = −108.67, 95% CI (−234.39, 17.06), P = .09]. Sensitivity analysis, performed by systematically excluding each study, showed that after excluding the study by He et al.
20
or Tao et al.,
29
intraoperative blood loss in the ED group was lower than the NED group, indicating relatively poor stability of the subgroup results. As shown in Figure 4. Forest plot of meta-analysis comparing intraoperative blood loss between the 2 groups.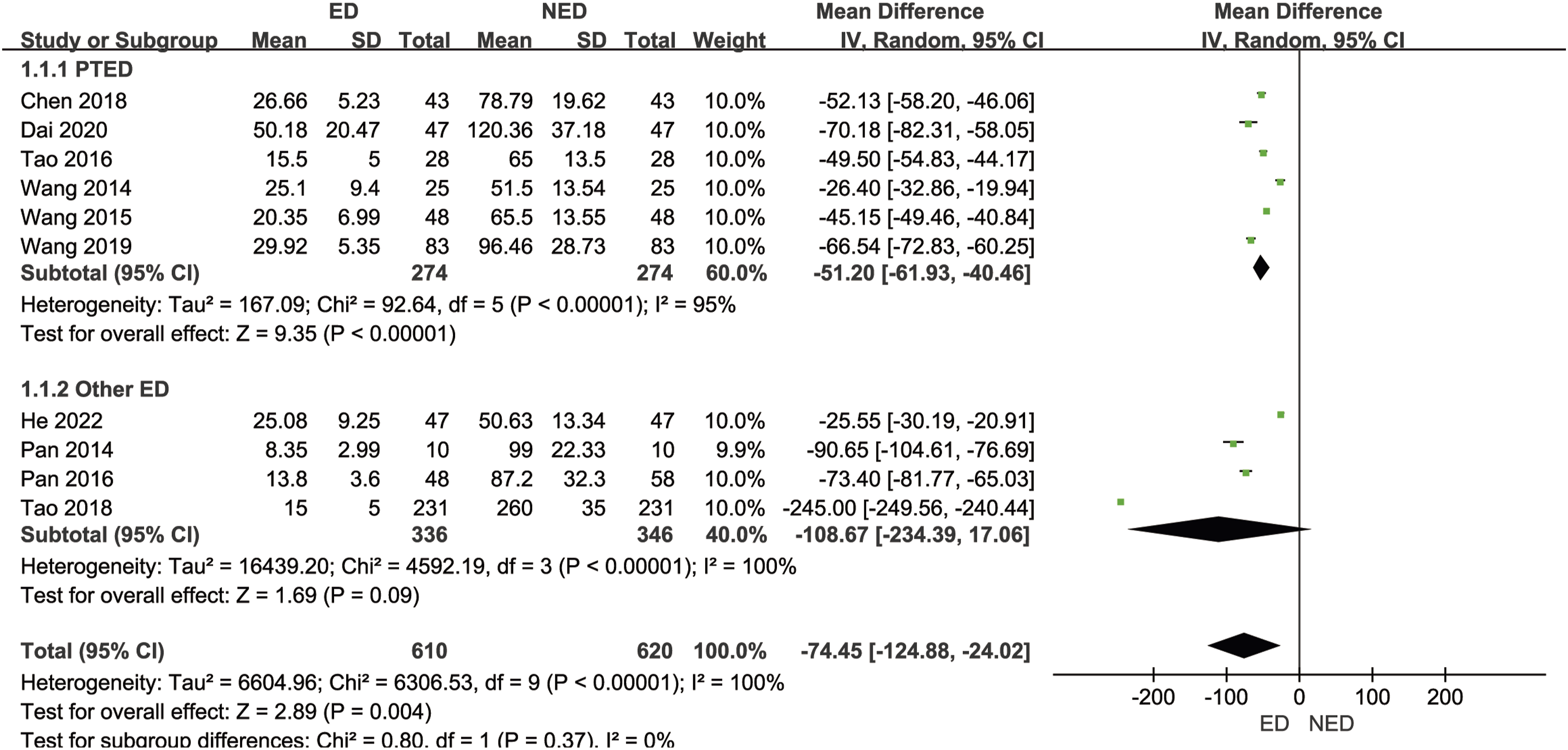
Operation Time
Fifteen studies16-20,22,23,25-32 (1668 patients with LHD) reported on operation time. The mean operation time in the ED group was 63.95 min, while in the NED group it was 87.52 min. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 99%). A random-effects model was employed to combine the effect sizes for the meta-analysis, revealing no statistically significant difference in operation time between the ED group and the NED group [MD = −10.17 min, 95% CI (−27.05, 6.71), P = .24]. Based on the different endoscopic surgical techniques within the experimental group, we divided the studies into the PTED subgroup and other ED subgroup. Eight studies in the PTED subgroup16,17,22,26,28,30-32 (676 patients with LHD) reported operation time. The mean operation time in the ED group was 66.41 min, while in the NED group it was 79.11 min. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 97%). A random-effects model was utilized to combine the effect sizes for the meta-analysis, indicating that the ED group had significantly shorter operation time than the NED group [MD = −11.69 min, 95% CI (−22.67, −0.71), P = .04]. Sensitivity analysis, systematically excluding each study, demonstrated that after excluding Dai et al.,
17
Tacconi and Giordan,
26
and Wang et al,
31
there was no statistically significant difference in operation time between the 2 groups, suggesting relatively poor stability of the subgroup results. Seven studies in the other ED subgroup18-20,23,25,27,29 (992 patients with LHD) reported operation time. The mean operation time in the ED group was 62.26 min, while in the NED group it was 93.20 min. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 100%). A random-effects model was used to combine the effect sizes for the meta-analysis, revealing no statistically significant difference in operation time between the ED group and the NED group [MD = −8.64 minutes, 95% CI (−45.13, 27.86), P = .64]. Sensitivity analysis, systematically excluding each study, showed that after excluding each study, the direction of the combined effect sizes remained consistent, indicating the basic stability of the subgroup results. As shown in Figure 5. Forest plot of meta-analysis comparing operation time between the 2 groups.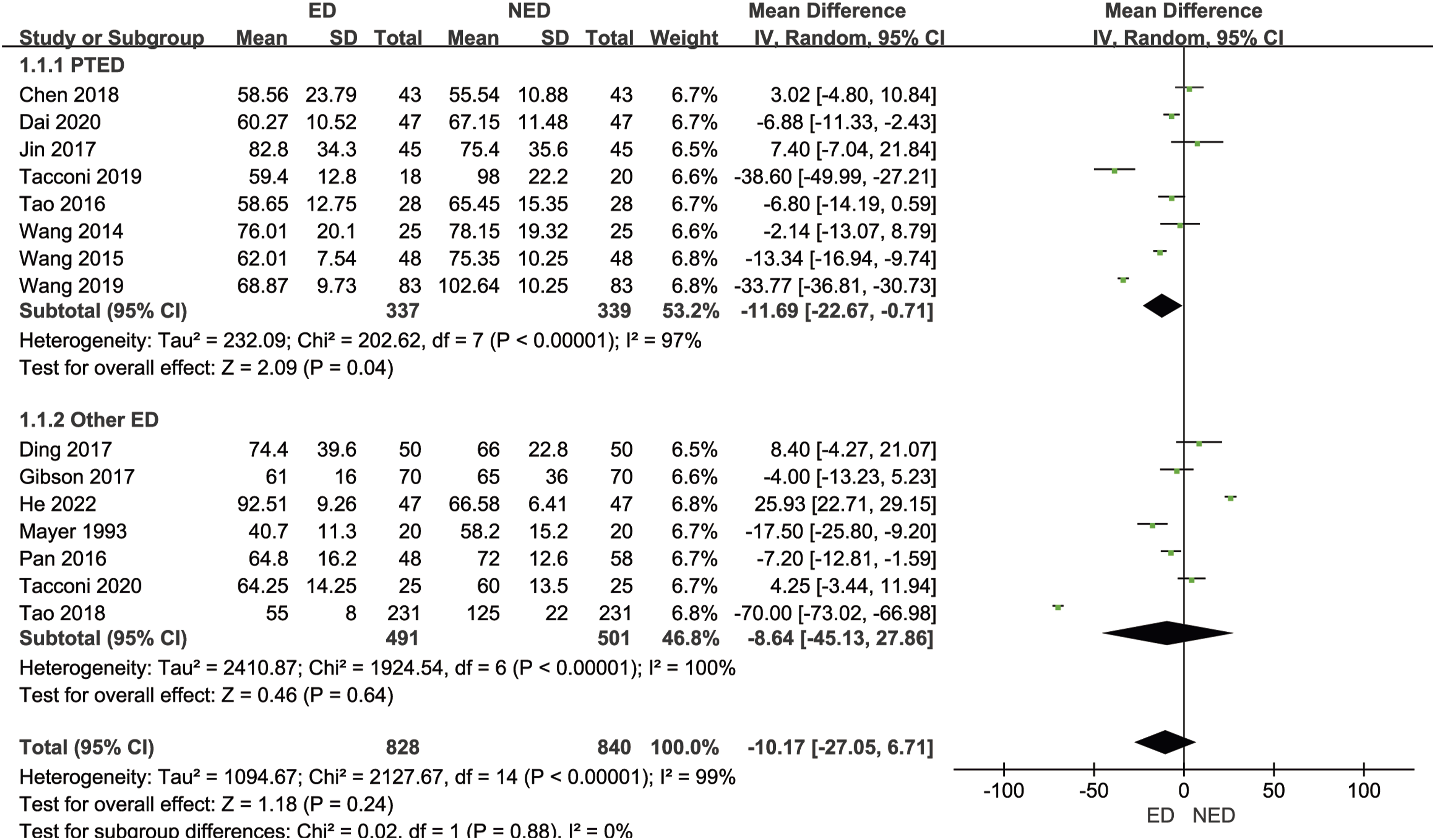
Hospitalization Duration
Twelve studies16-20,22,24,25,28,29,31,32 (1510 patients with LHD) reported on the hospitalization duration. The mean hospitalization duration in the ED group was 4.71 days, while in the NED group it was 10.47 days. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 100%). A random-effects model was employed to combine the effect sizes for the meta-analysis, revealing that the ED group had a significantly shorter hospitalization duration than the NED group [MD = −4.07 days, 95% CI (−6.67, −1.48), P = .002]. Based on the different endoscopic surgical techniques within the experimental group, we divided the studies into the PTED subgroup and other ED subgroup. Six studies in the PTED subgroup16,17,22,28,31,32 (598 patients with LHD) reported the hospitalization duration. The mean hospitalization duration in the ED group was 5.72 days, while in the NED group it was 9.31 days. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 84%). A random-effects model was utilized to combine the effect sizes for the meta-analysis, indicating that the ED group had a significantly shorter hospitalization duration than the NED group [MD = −3.46 days, 95% CI (−4.28, −2.63), P < .00001]. Sensitivity analysis, systematically excluding each study, demonstrated that after excluding each study, the direction of the combined effect sizes remained consistent, indicating the basic stability of the subgroup results. Six studies in the other ED subgroup18-20,24,25,29 (922 patients with LHD) reported the hospitalization duration. The mean hospitalization duration in the ED group was 4.03 days, while in the NED group it was 11.20 days. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 100%). A random-effects model was used to combine the effect sizes for the meta-analysis, revealing no statistically significant difference in the hospitalization duration between the ED group and the NED group [MD = −4.74 days, 95% CI (−9.47, −.01), P = .05]. Sensitivity analysis, systematically excluding each study, showed that after excluding Gibson et al.,
19
Pan et al.,
24
or Tao et al.,
29
the ED group’s hospitalization duration was significantly shorter than the NED group, suggesting relatively poor stability of the subgroup results. As shown in Figure 6. Forest plot of meta-analysis comparing hospitalization duration between the 2 groups.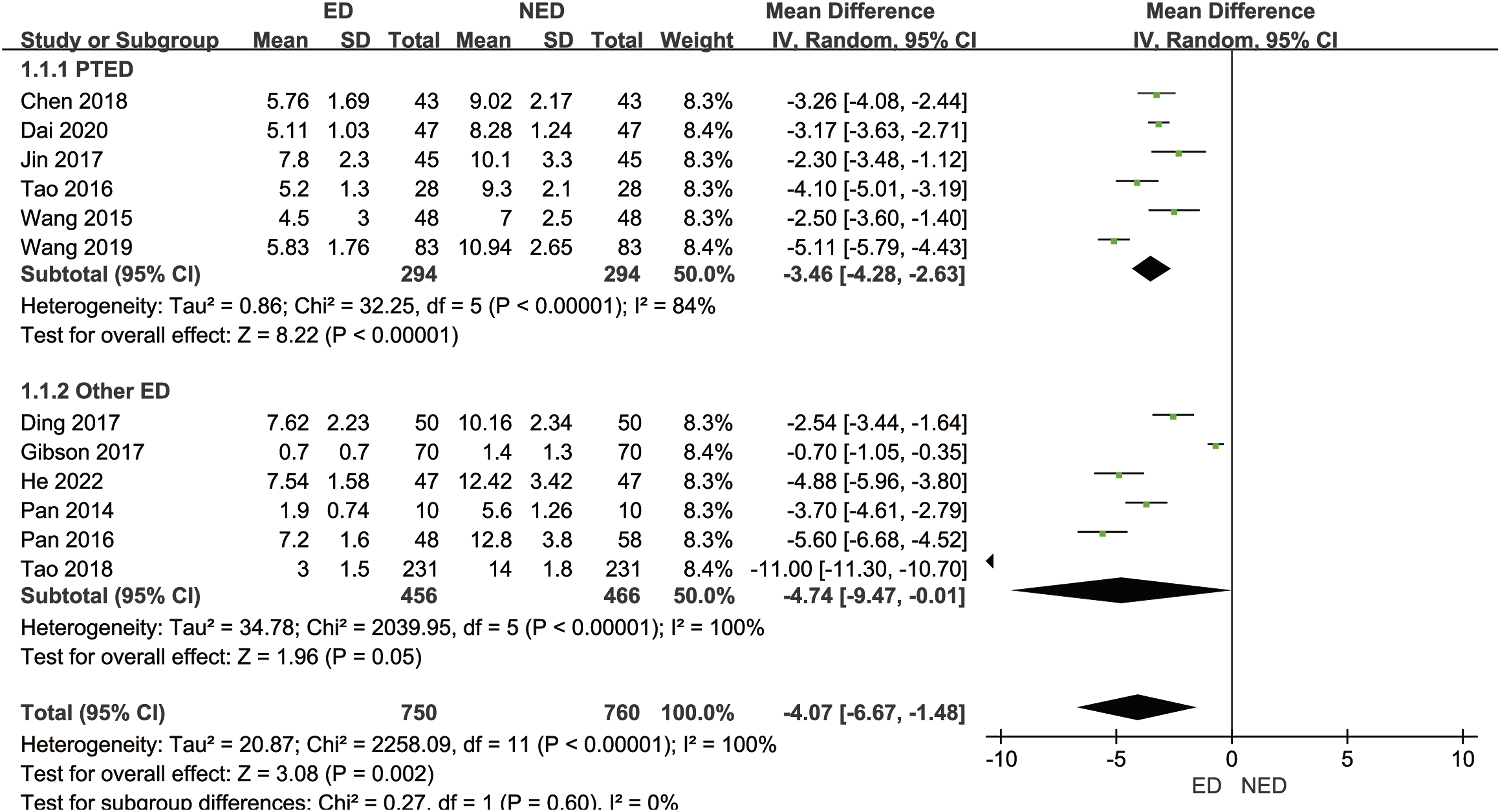
VAS Pain Scores at the Last Follow-Up
Ten studies16-18,20,22,26-28,31,32 (870 patients with LHD) reported the VAS pain scores at the last follow-up. The mean VAS pain scores at the last follow-up in the ED group was 1.29, while in the NED group it was 1.69. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 93%). A random-effects model was employed to combine the effect sizes for the meta-analysis, indicating that the ED group had significantly lower VAS pain scores at the last follow-up than the NED group [MD = −.35, 95% CI (−.63, −.07), P = .01]. Based on the different endoscopic surgical techniques within the experimental group, we divided the studies into the PTED subgroup and other ED subgroup. Seven studies in the PTED subgroup16,17,22,26,28,31,32 (626 patients with LHD) reported the VAS pain scores at the last follow-up. The mean VAS pain scores at the last follow-up in the ED group was 1.33, while in the NED group it was 1.76. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 94%). A random-effects model was used to combine the effect sizes for the meta-analysis, indicating no statistically significant difference in VAS pain scores at the last follow-up between the ED group and the NED group [MD = −.38, 95% CI (−.79, .02), P = .06]. Sensitivity analysis, systematically excluding each study, demonstrated that after excluding Dai et al.,
17
Tacconi and Giordan,
26
or Tao et al.,
28
the VAS pain scores at the last follow-up for the ED group were lower than the NED group, suggesting relatively poor stability of the subgroup results. Three studies in the other ED subgroup18,20,27 (244 patients with LHD) reported the VAS pain scores at the last follow-up. The mean VAS pain scores at the last follow-up in the ED group was .56, while in the NED group it was 1.51. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 100%). A random-effects model was employed to combine the effect sizes for the meta-analysis, indicating no statistically significant difference in VAS pain scores at the last follow-up between the ED group and the NED group [MD = −.26, 95% CI (−.92, .40), P = .44]. Sensitivity analysis, systematically excluding each study, showed that after excluding each study, the direction of the combined effect sizes remained consistent, indicating the basic stability of the subgroup results. As shown in Figure 7. Forest plot of meta-analysis comparing VAS pain scores at the last follow-up between the 2 groups.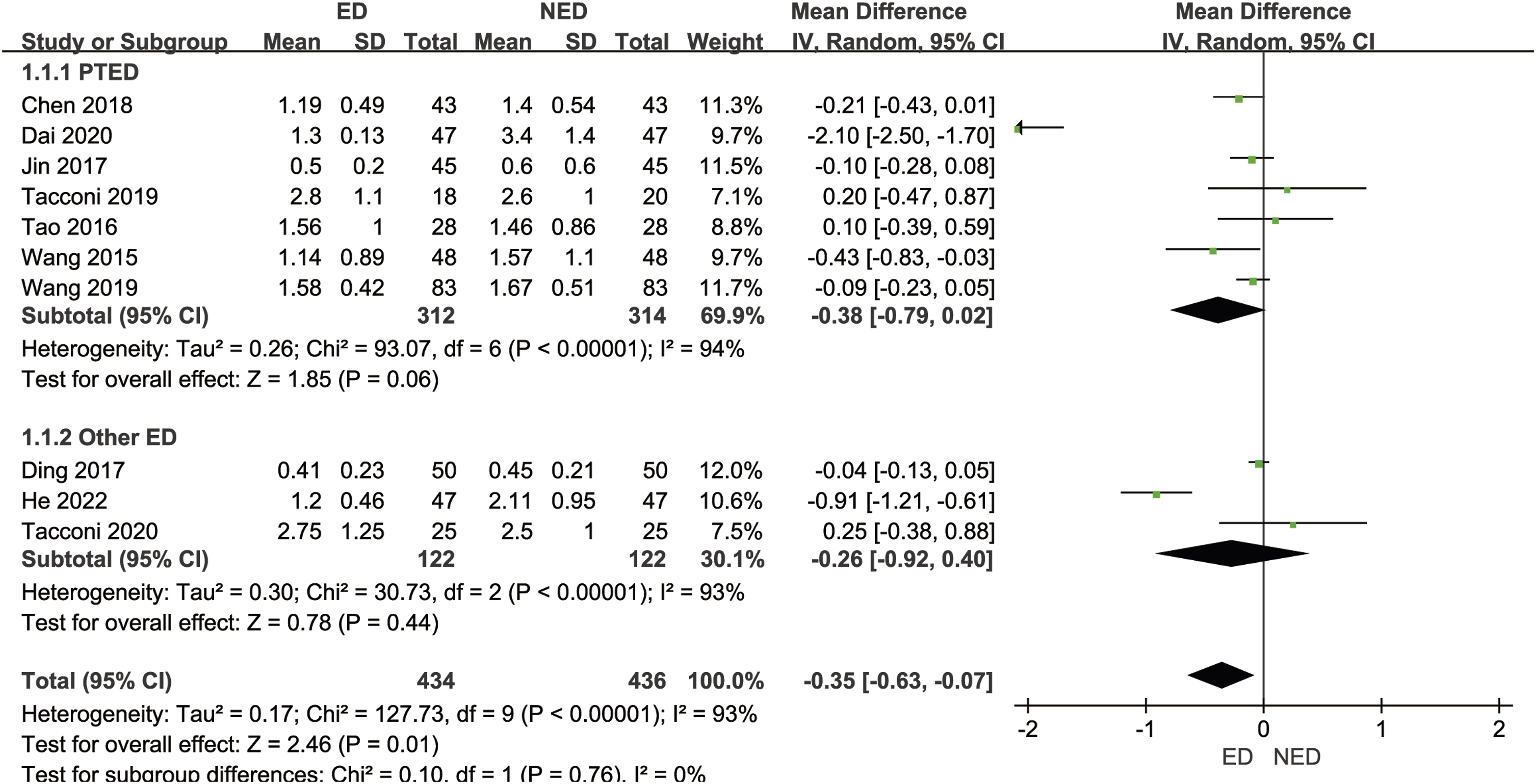
ODI Scores at the Last Follow-Up
Five studies18-20,22,26 (462 patients with LHD) reported the ODI scores at the last follow-up. The mean ODI scores at the last follow-up in the ED group was 10.22, while in the NED group it was 12.52. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 91%). A random-effects model was employed to combine the effect sizes for the meta-analysis, indicating no statistically significant difference in ODI scores at the last follow-up between the ED group and the NED group [SMD = −.49, 95% CI (−1.14, .17), P = .14]. Based on the different endoscopic surgical techniques within the experimental group, we divided the studies into the PTED subgroup and other ED subgroup. Two studies in the PTED subgroup22,26 (128 patients with LHD) reported the ODI scores at the last follow-up. The mean ODI scores at the last follow-up in the ED group was 9.20, while in the NED group it was 9.90. There was no statistically significant heterogeneity among the studies (P = .49, I2 = 0%). A fixed-effects model was used to combine the effect sizes for the meta-analysis, indicating no statistically significant difference in ODI scores at the last follow-up between the ED group and the NED group [SMD = −.16, 95% CI (−.50, .19), P = .38]. Three studies in the other ED subgroup18-20 (334 patients with LHD) reported the ODI scores at the last follow-up. The mean ODI scores at the last follow-up in the ED group was 10.60, while in the NED group it was 17.40. There was significant statistical heterogeneity among the studies (P < .00001, I2 = 95%). A random-effects model was employed to combine the effect sizes for the meta-analysis, indicating no statistically significant difference in ODI scores at the last follow-up between the ED group and the NED group [SMD = −.73, 95% CI (−1.79, .33), P = .18]. Sensitivity analysis, systematically excluding each study, demonstrated that after excluding each study, the direction of the combined effect sizes remained consistent, indicating the basic stability of the subgroup results. As shown in Figure 8. Forest plot of meta-analysis comparing ODI scores at the last follow-up between the 2 groups.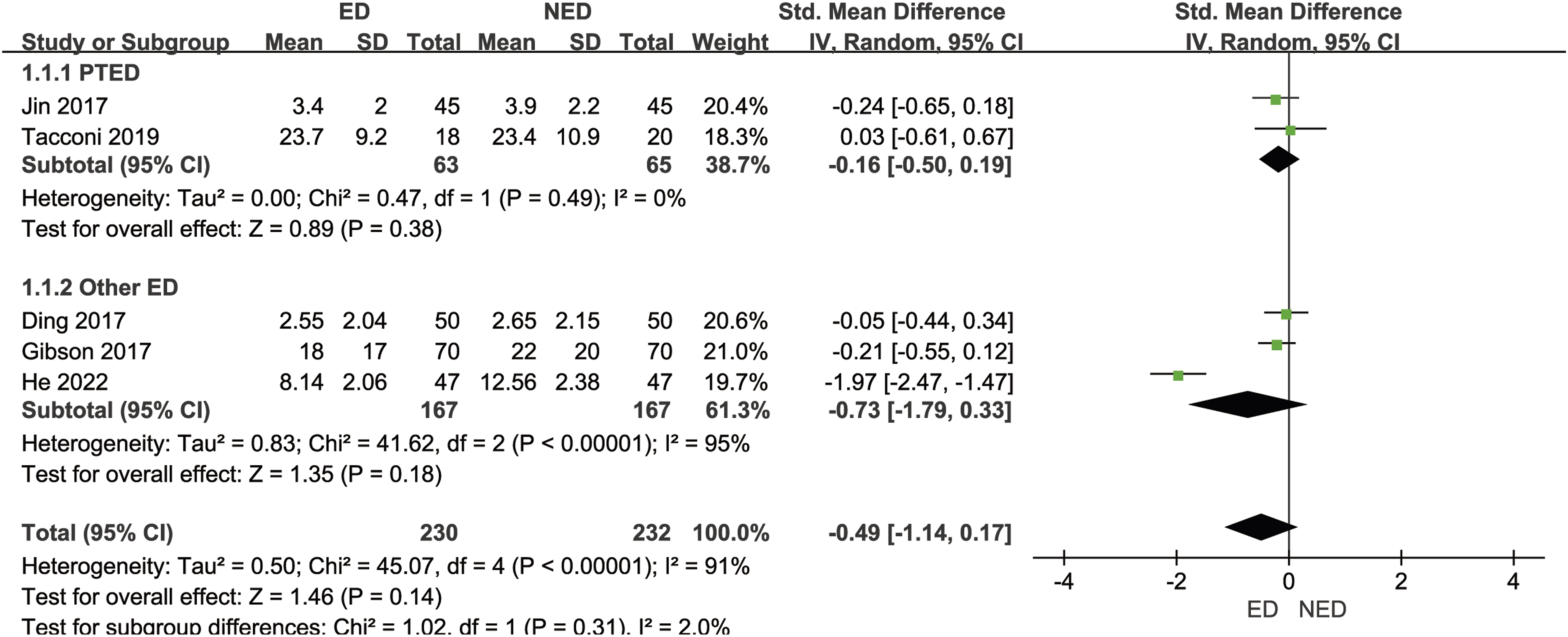
Complication Rates
Sixteen studies16-22,24-32 (1708 patients with LHD) reported the complication rates. In the ED group, the complication rate was 41/848 (4.8%), while in the NED group, the complication rate was 123/860 (14.3%). There was no statistically significant heterogeneity among the studies (P = .42, I2 = 3%). A fixed-effects model was used to combine the effect sizes for the meta-analysis, indicating that the ED group had a lower complication rate compared to the NED group [RR = .35, 95% CI (.25, .48), P < .00001], with a statistically significant difference. As shown in Figure 9. Forest plot of meta-analysis comparing complication rates between the 2 groups.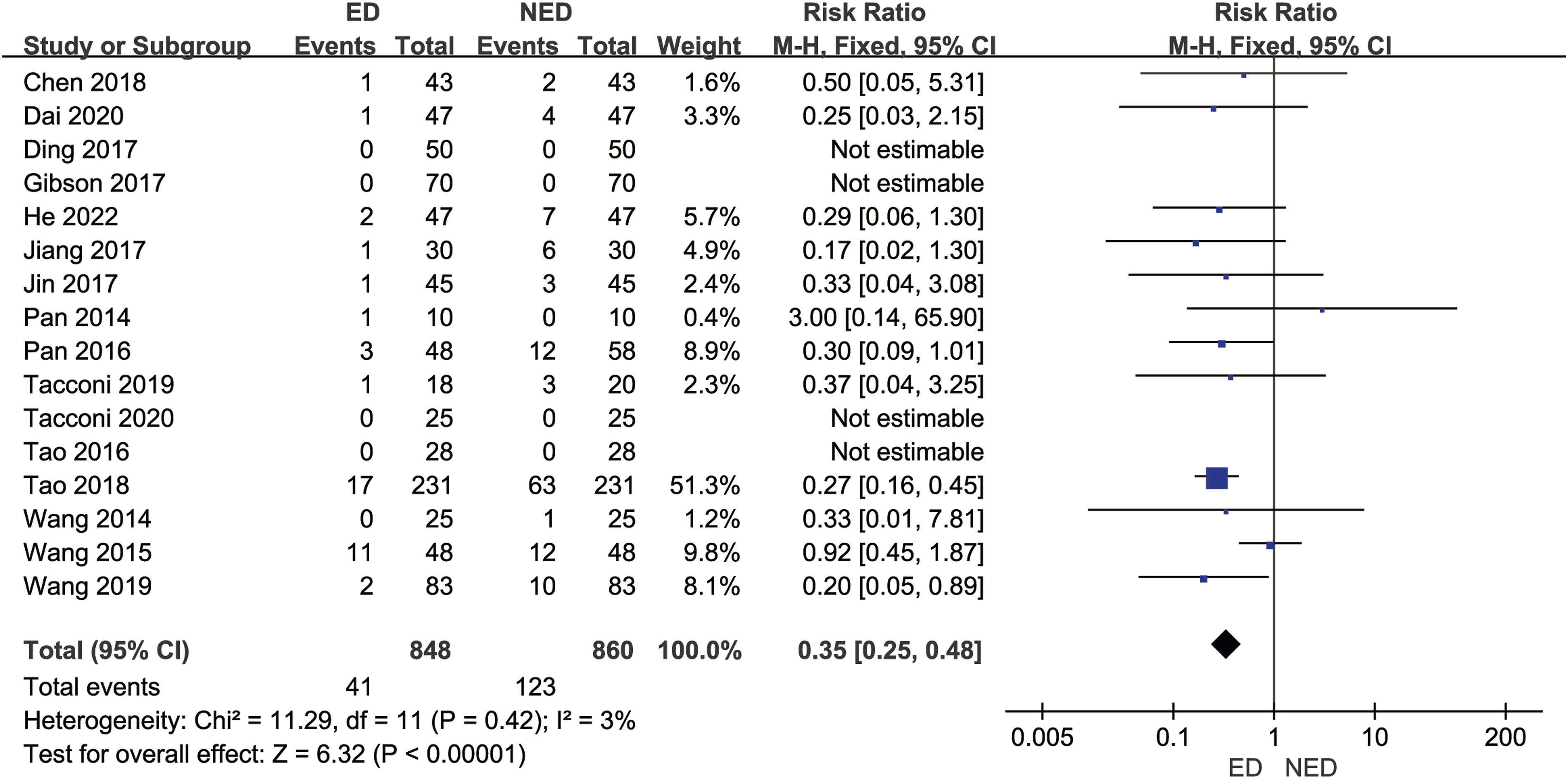
Ratio of Excellent and Good Therapeutic Effects Postoperatively
Nine studies16,18,20,22,28-32 (1200 patients with LHD) reported the ratio of excellent and good therapeutic effects postoperatively. In the ED group, the ratio of excellent and good therapeutic effects postoperatively was 41/848 (90.3%), while in the NED group, it was 514/600 (85.6%). There was no statistically significant heterogeneity among the studies (P = .34, I2 = 11%). A fixed-effects model was used to combine the effect sizes for the meta-analysis, the results indicated a higher ratio of excellent and good therapeutic effects postoperatively in the ED group compared to the NED group [RR = 1.05, 95% CI (1.01, 1.10), P = .01], with a statistically significant difference. As shown in Figure 10. Forest plot of meta-analysis comparing the ratio of excellent and good therapeutic effects postoperatively between the 2 groups.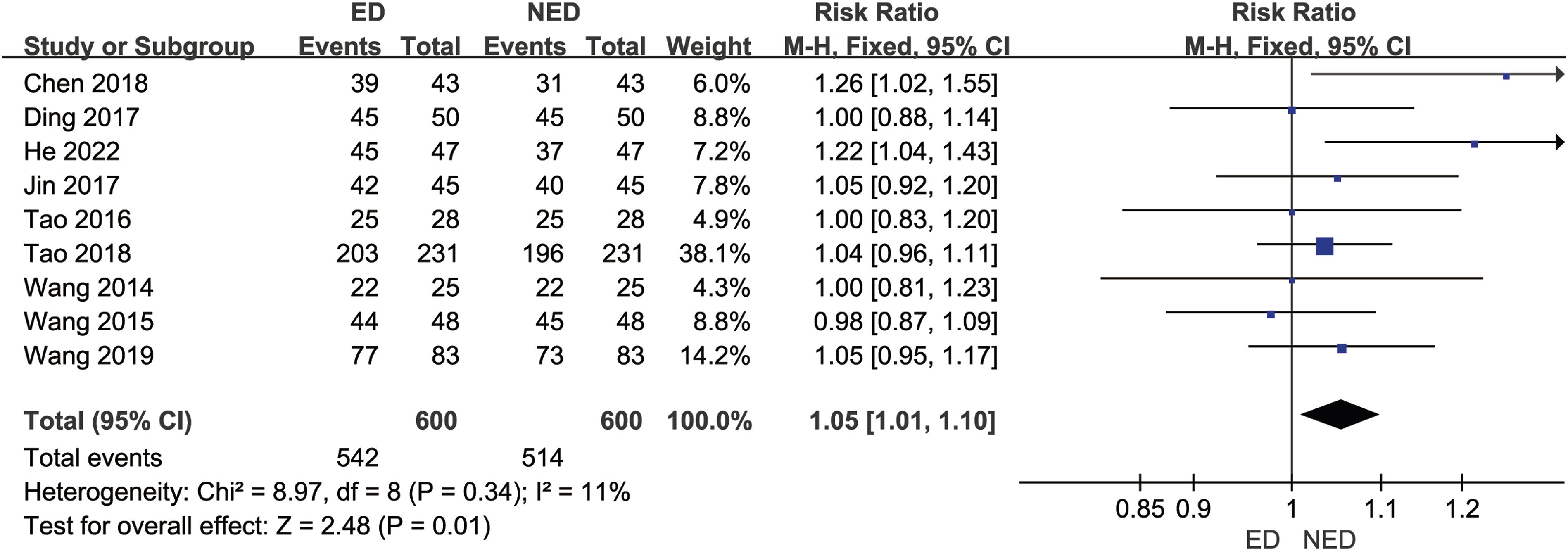
Publication Bias Analysis
Egger’s tests were conducted with intraoperative blood loss, operation time, hospitalization duration, VAS pain scores at the last follow-up, and complication rates as indicators. The results yielded P-values of .728, .329, .307, .222, and .947, respectively. These findings suggest a minimal likelihood of publication bias in our study.
GRADE Evidence Quality Grading Results
GRADE Assessment of Outcome Indicators.
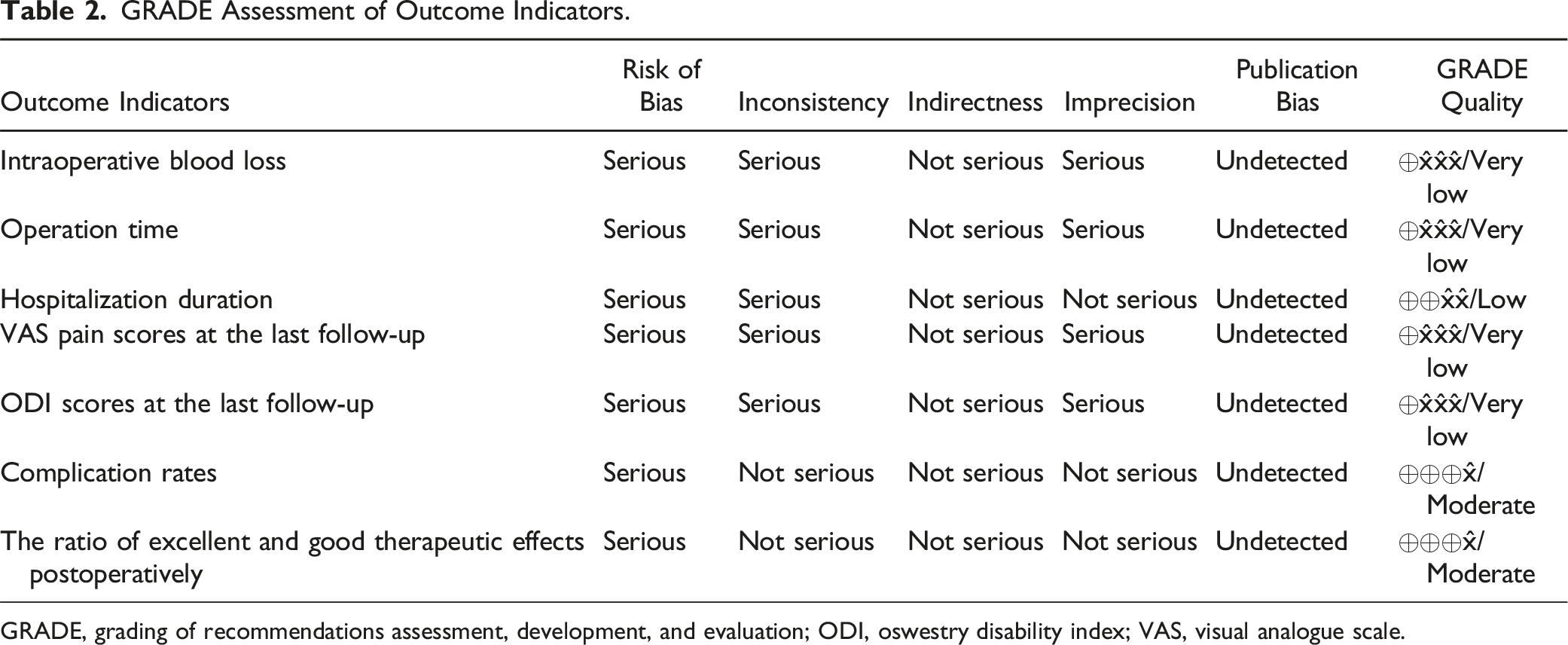
GRADE, grading of recommendations assessment, development, and evaluation; ODI, oswestry disability index; VAS, visual analogue scale.
Discussion
Traditional treatment methods for LHD primarily involve non-endoscopic techniques, such as open surgery. While these methods have shown certain effectiveness in alleviating patient symptoms, they come with notable drawbacks. Conventional open surgeries typically require large incisions, resulting in significant trauma. Patients may experience prolonged postoperative pain, bleeding, and recovery periods, leading to a considerable impact on their quality of life.17,27 With the advancements in minimally invasive techniques, endoscopic technology has emerged as a prominent approach in treating LHD. Endoscopic procedures, characterized by smaller incisions, a clear visual field, and more precise operations, provide patients with a gentler treatment option.33,34 However, a comprehensive and systematic comparison of the safety and effectiveness of endoscopic techniques vs traditional non-endoscopic techniques in treating LHD is currently lacking. Despite numerous studies focusing on endoscopic technology for LHD treatment, the existing evidence exhibits heterogeneity among different studies, and local research results are relatively dispersed.16-32 Therefore, conducting a systematic review and meta-analysis based on the PRISMA guidelines can integrate the results of existing studies, providing more reliable evidence for clinical practice and offering clearer treatment options for both physicians and patients. The aim of this study is to perform a comprehensive meta-analysis of RCTs that compare endoscopic and non-endoscopic techniques for treating LHD. Our objective is to systematically assess the safety and effectiveness of both treatment approaches, and we aim to provide evidence-based insights into the realm of clinically effective minimally invasive treatments.
The endoscopic surgery group demonstrated a significant advantage in terms of intraoperative blood loss, which is likely the result of several contributing factors. First, compared to traditional non-endoscopic surgeries, the minimally invasive nature of endoscopic techniques involves smaller and more precise incisions, reducing interference and damage to the patient’s tissues, which in turn minimizes vascular injury and leads to a significant reduction in intraoperative blood loss. Second, endoscopic surgery provides a high-definition visual field, allowing surgeons to observe the surgical site more clearly and perform more intuitive operations. This visual clarity facilitates precise tissue handling, reducing the likelihood of inadvertent vascular injury and further decreasing blood loss. Additionally, endoscopic techniques are often equipped with advanced auxiliary tools such as vascular coagulators and high-frequency electrocoagulation devices, which can effectively control intraoperative bleeding, enhancing the overall safety of the procedure.34-37 However, while there was a statistically significant difference in blood loss between the endoscopic and non-endoscopic groups, it is important to note that the average blood loss in both groups was relatively low, and its clinical significance may be limited. Since lumbar disc herniation surgeries typically do not involve significant vascular injury, the blood loss in traditional surgeries is generally not substantial enough to significantly impact patient recovery. Therefore, despite the statistical difference, the actual effect on clinical outcomes may be limited. Furthermore, continuous saline irrigation is a routine part of endoscopic surgery, helping to maintain a clear visual field and reduce small vessel bleeding. However, this irrigation process also presents challenges for accurately measuring intraoperative blood loss. In traditional surgery, blood loss can be directly measured using a suction device, whereas in endoscopic surgery, the actual blood loss may be underestimated or difficult to quantify due to the saline irrigation. Thus, the clinical relevance of blood loss differences should be interpreted with caution, and future research should consider more precise methods for assessing blood loss to improve the accuracy of the data.
The hospitalization duration for patients in the ED group was significantly shortened, indicating that endoscopic technology holds promise for providing patients with a more rapid recovery and early discharge. Several factors may contribute to this outcome, including the minimally invasive nature leading to swift recovery, fewer postoperative complications, and lower postoperative pain levels. The VAS pain scores at the last follow-up in the ED group demonstrated a significant decrease, reflecting the effective control of postoperative pain by endoscopic technology. The advantages of minimally invasive surgery lie in the lesser postoperative pain experienced by patients, contributing to increased postoperative satisfaction and improved recovery outcomes. The reduction in VAS pain scores may also be related to the finer protection of neural structures provided by endoscopic technology, reducing traction and damage to neural tissues.17,19 Additionally, the ED group exhibited a significantly lower complication rate, reflecting the enhanced safety profile of endoscopic technology during surgery. The small incisions, intuitive operations, and more precise procedures associated with minimally invasive surgery contribute to the reduction of surgery-related complications. This outcome is crucial for patients, as a lower complication rate implies lower risks and a shorter recovery time. However, the variation in complication reports across studies is likely related to differences in how each study defines complications. The types of complications range from mild postoperative pain to more severe issues like spinal cord injury, with clearly differing clinical impacts. Therefore, we recommend that future studies standardize the definition of complications to provide more clinically meaningful results. Lastly, the ED group exhibited a higher ratio of excellent and good therapeutic effects postoperatively, further highlighting the significant advantages of endoscopic technology in treating LHD. The increased ratio of excellent and good therapeutic effects postoperatively may be associated with factors such as reduced intraoperative blood loss, decreased pain scores, and reduced complications, reflecting the comprehensive effect of endoscopic technology in improving the overall postoperative condition of patients.
However, no statistically significant differences were observed between the 2 groups in terms of ODI scores at the last follow-up and operation time. Firstly, the lack of significant differences in ODI scores at the last follow-up may be attributed to the comprehensive nature of ODI as a composite index, encompassing various aspects such as patient function, quality of life, and pain. Even with significant advantages in other indicators, the ODI results are influenced by a variety of factors, including individual patient recovery rates and levels. 38 Therefore, no significant statistical differences were observed at the last follow-up due to the combined effects of these factors. Secondly, the results regarding operation time also did not demonstrate statistically significant differences. Operation time is influenced by factors such as surgical complexity, surgeon experience, and patient anatomy. While endoscopic technology is generally believed to enhance surgical efficiency, individual variations and unexpected circumstances during surgery can lead to fluctuations in operation time. Thus, the lack of statistically significant differences may be attributed to the significant randomness of these factors in this study. Despite the absence of statistically significant differences, it is noteworthy that the ED group showed a trend towards lower ODI scores and shorter operation time, suggesting a potential advantage of endoscopic technology in patient recovery and surgical outcomes. This may be influenced by limitations in the study sample, individual variations, and other potential factors not included in the analysis. Future research can further explore the reasons behind these trends and validate these findings through larger samples and more rigorously designed RCTs.
This study has several limitations: (1) Some of the included studies had small sample sizes, and there were unclear descriptions of randomization methods, blinding, and allocation concealment in most studies. These issues may impact the internal validity of the results and limit the reliability of the conclusions. (2) There was considerable heterogeneity among the included studies, arising from variations in study design, sample sizes, and methodologies. These variations made it difficult to fully compare outcomes across studies. Although subgroup analysis was performed, it did not significantly reduce the heterogeneity, and poor stability was observed in some subgroups. This heterogeneity complicates the interpretation of results and may limit the generalizability of the findings. (3) Although all studies compared the outcomes of endoscopic and non-endoscopic surgeries, there were significant differences in the types of endoscopic techniques used. Due to variations in surgical approaches, access routes, and the instruments used, these different techniques may result in varying postoperative outcomes. (4) The non-endoscopic surgery group in this study includes various surgical techniques, which may differ in terms of invasiveness, operation time, and blood loss. These differences could potentially affect the results. (5) Variability in follow-up durations across studies may lead to heterogeneity in the final outcomes, such as pain scores and ODI scores. Some studies reported relatively short follow-up periods, which may not fully capture the long-term efficacy of the treatments. (6) The majority of outcome indicators were rated as having low quality according to the GRADE system, which raises concerns about the reliability of the results and conclusions. This limitation highlights the need for future research to focus on improving the quality of evidence by using more rigorous study designs, larger sample sizes, and standardized methodologies to ensure more reliable and robust outcomes. (7) The study is limited to articles published in English and Chinese, potentially excluding relevant studies published in other languages. This may limit the diversity of evidence considered and could potentially affect the generalizability of the findings. (8) Although this study aimed to compare the safety and effectiveness of endoscopic vs non-endoscopic surgeries, the lack of high-quality comparative studies limited the ability to conduct a comprehensive, systematic evaluation. Future research should focus on conducting robust, well-designed comparative studies to better assess the differences in outcomes between these 2 surgical techniques.
In conclusion, the findings of this study support endoscopic technology as a safe and effective option for treating LHD, providing a solid evidence base for minimally invasive treatments. However, further evaluation is needed through high-quality, large-sample, multicenter RCTs to improve reliability. Future research should also focus on standardizing surgical techniques and follow-up durations to reduce heterogeneity, assessing long-term impacts on quality of life and functional recovery, and including studies in multiple languages to enhance evidence diversity.
Footnotes
Author Contributions
Bo-Tao Cai and Fan Yang conceptualized and designed the study, Deng-Chao Wang executed the search strategy. Data collection was carried out by Bo-Tao Cai and Fan Yang, with Deng-Chao Wang performing a subsequent data validation. Analysis was conducted by Bo-Tao Cai and Fan Yang, which was later verified by Deng-Chao Wang. Quality assessment of the studies was undertaken by Bo-Tao Cai and Fan Yang, with Deng-Chao Wang providing a secondary review. Bo-Tao Cai authored the manuscript, and Deng-Chao Wang provided editorial input. All authors contributed to the manuscript’s review and revision process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Involving Human Participants and/or Animals
This article did not include any studies involving human participants or animals performed by any of the authors.
Clinical Trial Registration
The registration number is INPLASY2022410095.